Back to Journals » International Journal of Women's Health » Volume 15
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Authors Gebremichael MA ![]() , Lema TB
, Lema TB
Received 3 April 2023
Accepted for publication 30 August 2023
Published 4 September 2023 Volume 2023:15 Pages 1383—1395
DOI https://doi.org/10.2147/IJWH.S415615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Elie Al-Chaer
Mitsiwat Abebe Gebremichael,1 Tefera Belachew Lema2
1Public Health Department, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 2Population and Family Health Department, Human Nutrition Unit, College of Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia
Correspondence: Mitsiwat Abebe Gebremichael, Public Health Department, College of Medicine and Health Sciences, Ambo University, P. O. Box 19, Ambo, 00251, Ethiopia, Email [email protected]
Introduction: Evidence has demonstrated that knowledge and attitudes are indicators of nutrition and health modification among pregnant women. As a result, the objective of this study was to assess the prevalence and predictors of knowledge and attitudes about optimal nutrition and health among pregnant women in their first trimester of pregnancy.
Methods: A community-based cross-sectional study design was conducted between April 1 and June 1, 2018 among 750 pregnant women and sampled using the multi-stage sampling technique in the Ambo district of the West Shoa Zone, Ethiopia. Using a pre-tested, semi-structured questionnaire, data were gathered and analyzed using SPSS version 23. First, descriptive statistics were used, then bivariate and, finally, multivariable logistic regression analysis was used to assess the association of the predictors with the outcome variables.
Results: Overall, 33.3% and 31.3% of pregnant women had good knowledge and favorable attitudes about optimal nutrition and health, respectively. Residence, the woman’s and her husband’s educational status, having > five household members, being in rich households, taking distance to reach a health institution, being multiparous, having information, and receiving counseling were significantly associated with pregnant women’s knowledge on optimal nutrition and health. Also, a favorable association was found between a woman’s attitude toward optimal nutrition and health and her and her husband’s educational status, household wealth status, and the distance traveled to a health facility.
Conclusion: The nutrition and health knowledge and attitudes of pregnant women in the study area were suboptimal. Improving knowledge and attitude during the first trimester of pregnancy is essential for suggesting nutrition and health-related behavior in the succeeding periods of pregnancy, which predominantly determine the pregnancy’s outcomes.
Keywords: knowledge, attitude, optimal nutrition and health, pregnant women, Ethiopia
Corrigendum for this paper has been published.
Introduction
The promotion of community and pregnant women’s health depends heavily on nutrition.1 Pregnant women should consume a variety of foods that are high in energy, protein, vitamins, minerals, and water because women have increased physiological needs for energy and nutrients to support fetal growth and development.2 A person must be well-nourished in order to be healthy, and nutritional status can be impacted by bad health.3
The main elements of optimum nutrition and health are encouraging a supportive lifestyle and care, micronutrient supplementation (commonly iron and folate), disease prevention and treatment measures (top priorities for malaria and deworming), and consumption of a variety of foods from both plant and animal origins. Additionally, eating more frequently and in larger quantities with gestational age, using iodized salt for the entire family, and avoiding any foods due to taboos are also important.4,5
For women’s health and the health of their offspring, they must consume the proper quantity of food.6 The requirements for practically all nutrients increase from 8 to 63% compared to non-pregnant and/or non-lactating women, while the demand for a few micronutrients, including vitamin D, vitamin E, vitamin K, calcium, and phosphorus, remains the same throughout pregnancy.7 Women who are pregnant need a wide variety of foods and at least one more meal per day than women who are not pregnant, as well as plenty of clean water. For the mother and fetus to grow, iron-rich meals, iodized salt, and a reduction in heavy workloads are all necessary.3,4
The likelihood of having newborns of small gestational age (SGA) decreases by around 31% when pregnant women provide a balanced diet.8 The WHO has set a goal of reducing anemia in women of reproductive age by 50% and low birth rates by 30% by providing appropriate nutrition throughout pregnancy in order to lower death rates over the following five years.5,9 In Ethiopia, anemia affected about 17% of women in the reproductive age group and 22% of pregnant women.10 Only 11% of women, however, took iron supplements for 90 days or longer.11
Disease prevention and treatment procedures place a high priority on the prevention and treatment of malaria, deworming, and hygiene as part of best health practices.12–14 The pregnant woman, the fetus, and the newborns are all at risk from malaria infection. It commonly comes with consequences like low birth weight and transplacental parasitemia, as well as anemia and intrauterine growth restriction (IUGR).15 The pregnant women and their fetus will be protected against malaria if insecticide-treated bed nets (ITN) are given at the initial point of contact.16 In Ethiopia, though, more than 40% of pregnant women lack access to ITN.17
One of the public health issues that has an impact on pregnant women’s and their unborn children’s health is soil-transmitted helminthes (STHs).18 These infections infected roughly 70% of pregnant women in Ethiopia.19 The World Health Organization (WHO) recommended that, to mitigate the impact of STH-induced anemia and its associated consequences, deworming medications coupled with hygiene education be used during pregnancy.20 However, a multilevel analysis carried out in Ethiopia revealed that just 7.8% of them used deworming medicine while pregnant.21
Work load, rest during pregnancy, and the capacity of pregnant women to make decisions at home are all aspects of optimal health practices that have an impact on pregnant women’s optimal nutrition practices, either directly or indirectly.5 These factors fall under the category of supportive lifestyle and care components. Women who lack energy can conserve it by avoiding strenuous activities, setting reasonable work hours, and getting enough rest.4,5
Due to their social status, women in some cultures may be less able to acquire resources and decide how to use them to improve their health and nutrition, especially during pregnancy.12,22 Approximately 65.4% of pregnant married women had made decisions either alone or with their husbands in all three decision-making parameters (ie, own health care, making large household purchases, visits to her family or relatives), according to a study conducted in sub-Saharan Africa using a multi-country analysis of 25 countries.23
In order to ensure that pregnant women receive adequate nutrition and proper health, nutrition knowledge is crucial.24 Malnutrition and poor health are said to be caused immediately by a lack of knowledge and attitude.25 Evidence has demonstrated that attitudes and knowledge about nutrition and health are indicators of dietary habit modification and are one of the elements that go into having a healthier nutritional practice. Therefore, pregnant women are expected to have the necessary knowledge and attitude to maintain optimal nutrition and health during pregnancy.24,26
The Ethiopian Ministry of Health (MoH) has employed a variety of strategies, such as social media-based nutrition education. Similarly, health extension workers (HEWs) have been working to address the lack of dietary knowledge and attitudes among women.27 The government also recommends nutrition and health counseling for pregnant women, both at health institutions and in the community28 because improving maternal nutrition and health is the most appealing and long-lasting strategy for promoting maternal and child health.29 However, only 47% of women were knowledgeable about the need to eat a varied and balanced diet.30 Similarly, only 27%, 48.4%, and 34.5% of respondents to a study carried out in Addis Ababa, Ethiopia, were found to have adequate knowledge, a favorable attitude, and appropriate practices for maternal nutrition, respectively.26
Pregnant women’s’ knowledge of and attitude toward optimal nutrition and health practices are influenced by a number of variables. These include the respondent’s type of work, the respondent’s mother’s educational level, her monthly income, the number of her pregnancies, her ANC visits, the size of her family, being a rural resident and her marital status.31,32
Suboptimal dietary and health practices among pregnant women in Ethiopia have been documented.33–36 This might be because there are difficulties putting nutritional and health advice into reality because of the knowledge, attitude, and cultural norms that exist in a given society.
The magnitude of undernutrition increased with increasing gestational age, especially in the third trimester of pregnancy,37 despite the fact that Ethiopian pregnant women’s dietary habits were similar to those they had before becoming pregnant. Similarly, disease prevention and treatment procedures like the prevention and treatment of malaria, deworming, and hygiene, and supportive lifestyles like work load, rest during pregnancy, and the capacity of pregnant women to make decisions were the health aspects of pregnant women that needed due attention during pregnancy and affected the outcome of both the mother and their offspring.4,5
This study differs from other studies since it was conducted during the first trimester of pregnancy, whereas most studies have not done so at this stage of pregnancy. Moreover, this study tried to use standardized tools and procedures (like the WHO Essential Nutrition Action Guidelines and the frameworks from the Manoff group that were used to promote maternal nutrition and health in developing countries) in measuring knowledge and attitudes toward optimal nutrition and health. This study also differs from the other studies in that it incorporates both nutritional and health aspects of pregnant women related to knowledge and attitude one at a time, rather than other studies that focus only on nutritional aspects. Therefore, assessing knowledge and attitude during the first trimester of pregnancy is crucial for advising nutrition and health-related behavior in the following phases of pregnancy, which primarily affect the pregnancy’s outcomes.
To develop evidence-based, successful intervention methods, it is crucial to assess the prevalence and predictors of knowledge and attitudes about optimal nutrition and health among pregnant women in their first trimester of pregnancy. In order to improve the nutritional and health practices and nutritional status of pregnant women, it can be important to inform policymakers, planners, researchers, programmers, and health professionals in Ethiopia to pay due attention in the first trimester of pregnancy. Therefore, the purpose of this study was to assess the prevalence and predictors of knowledge and attitudes about optimal nutrition and health among pregnant women in their first trimester of pregnancy.
Materials and Method
Study Setting and Period
The study was conducted in the Ambo district from April 1 to June 1, 2018. Ambo district is located in the West Shoa Zone, Oromia Regional State, and west-central Ethiopia. Ambo, one of 22 districts in the west Shoa Zone, is divided into 39 kebeles (Ethiopia’s smallest administrative divisions), 6 of which are urban and 33 of which are rural, and is situated at 8°59′ N and 37°51′ E. The district has a total population of 152,143, according to the Central Statistics Agency’s (CSA) 2007 national census report. Of this number, 75,668 are men, and the remaining 76,475 are women.38 Based on 2017 district health office data, it has 37,454 and 6976 reproductive age groups and pregnant women, respectively. There are 6 health posts, 8 health centers, and 2 public hospitals in the district (West Shoa Zone Health Bureau Report, personal communication, June, 2017).
Study Design
A community-based cross-sectional study was employed.
Source Population and Study Population
The source population consisted of all pregnant women in their first trimester of pregnancy living in Ambo district, while the study population consisted of randomly selected pregnant women in their first trimester of pregnancy from the selected kebeles.
Inclusion Criteria
Pregnant women between the ages of 18 and 49 who lived in the study kebeles for at least six months were included in this study. Moreover, a laboratory test was done to confirm pregnancy, and then the last menstrual period was calculated to assure the woman was in her first trimester of pregnancy.
Exclusion Criteria
Pregnant women who were unable to respond to the questions were excluded.
Sample Size Determination and Sampling Technique
This study was part of a larger one entitled Effect of behavior change communication through the health development army on optimal nutrition and health practices of pregnant women in Ambo district, Oromia, Ethiopia: A cluster randomized controlled community trial registered at Pan African Clinical Trials as PACTR201805003366358. The sample size was calculated using the G Power 3.1.9.2 program based on the following assumptions: α error probability = 0.05; power = 0.8; an effect size of 0.5; allocation ratio (N1/N2) = 1; design effect of 2; and 10% loss to follow-up. According to the study done in Guto Gida Woreda, East Wollega Zone, Ethiopia, the proportion of pregnant women with optimal nutritional practices (P1) was 0.34%,39 while P2 was 0.49, assuming a difference of 15.4% between P1 and P2,40,41 and the final sample size was 770 pregnant women.
The study’s pregnant women were selected using a multi-stage sampling technique. The entire kebele in the Ambo district was divided into rural and urban sectors. Out of the 39 kebeles (6 urban and 33 rural) that were already in existence, 12 were selected through simple random sampling (SRS) using the lottery technique, with two being urban and 10 being rural. A computer-generated random number that was proportional to the size allocation of each kebele was used to select the eligible households using simple random sampling from among the chosen kebele. The number of pregnant women required was then selected using a computer-generated simple random sampling technique from among the identified eligible pregnant women in each kebele.
Data Collection Tools and Procedures
A pre-tested, English-language, semi-structured questionnaire was used to collect the data. To maintain consistency, language experts translated the questionnaire into two regional languages (Afan Oromo and Amharic) before returning it to English. Before the actual data collection, the questionnaire was pretested on 39 (5%) of the overall sample size that were excluded from the final main sample in order to detect any ambiguity, length, completeness, consistency, or acceptability. Prior to data collection, some alterations and skip patterns were addressed.
Eight diploma nurses were recruited to gather the data. The study’s objective and relevance, information confidentiality, respondent rights, informed consent, and interviewing techniques were all covered in the training given to the data collectors. Every day, the investigator and four supervisors with BScs in nursing verified the completed questionnaires for consistency and completeness. The questionnaire had 73 questions and asked about sociodemographic and economic information like family size, education, occupation, and wealth index; maternal characteristics, such as years of marriage, parity, gravidity, and ANC history; and health and nutrition information, as well as knowledge and attitudes about nutrition and health among pregnant women. “Supplementary Figure 1” The interview lasted 35–40 minutes.
The household wealth index was evaluated using the wealth constructs from the Ethiopian Demographic and Health Survey.34 The principal component Analysis was used in order to determine the wealth score. The wealth score was developed to divide households into poor, medium, and rich categories. Eight questions that assessed the decision-making power of women were taken from the Ethiopian Demographic and Health Survey questionnaire. Using the mean, women’s decision-making abilities were categorized.42
Questions about knowledge and attitude were adapted from the Manoff group’s formative research to improve maternal nutrition and health in developing countries and the WHO’s essential nutrition action framework.4,5
To assess pregnant women’s knowledge of optimum health and nutrition, 26 questions were used. A participant’s knowledge score was determined based on how many of the knowledge assessment questions they were able to correctly respond to. Each right response was worth 1, while each wrong response was worth 0. Tercile (three equal parts) were made by adding the factor scores. A pregnant woman was considered to have poor knowledge of nutrition and health if she scored in the first or second tercile, and good knowledge of nutrition and health if she scored in the highest tercile (ie, the third tercile).36
The attitude toward health and nutrition was evaluated using 20 Likert-scale questions. Tercile (three equal parts) were made by adding the factor scores. A pregnant woman was regarded as having an unfavorable attitude if she scored in the first or second tercile and a favorable attitude if she scored in the third tercile.36
Data Processing and Analysis
Before being entered, the data were thoroughly reviewed for accuracy and consistency throughout data gathering. Then it was entered into EPI data version 3.1 and exported to SPSS for Windows version 23 for cleaning and analysis. The variables were summarized using descriptive statistics like frequency, percentage, mean, and standard deviation. Continuous variables were normally distributed and assessed using the Kolmogorov–Smirnov test.
To evaluate factors, bivariate and multivariable logistic regression analyses were performed. The Hosmer-Lemeshow goodness-of-fit statistic is used to assess a model’s fitness. The correlation between independent variables was examined using the Pearson Correlation Coefficient. To demonstrate the crude effect that every factor has on knowledge and attitude, a bivariable logistic analysis was performed. It was obtained for their odds ratios (OR), 95% confidence intervals (CI), and p-values. Variables with a P-value of <0.25 in the bivariable analyses were entered into multivariable logistic regression analyses. To evaluate the strength of the association, an odds ratio (OR) with a 95% confidence interval (CI) was computed. In the multivariable analyses, a p-value < 0.05 was utilized to denote statistical significance.
Data Quality Control
The pretested questionnaire was modified using standard data collection tools. The Cronbach's alpha value of the questionnaire was checked, and it was found to be > 0.7 (ie, 0.81 for knowledge and 0.9 for attitude), indicating that it is appropriate for use in the study. Three days were allocated to training for data collectors and supervisors. To aid in respondent comprehension, the questionnaire was also translated into the two main languages of the research district (Afan Oromo and Amharic). The data collection process was thoroughly monitored by supervisors and the investigator. Every day, completed surveys were verified for completeness, and any errors or missing information were fixed. Using the established procedures, key assumptions were verified.
Results
Socio Demographic and Economic Characteristics
With a 97.4% response rate, 750 pregnant women in total were interviewed. Six hundred eight pregnant women from rural kebeles made up the majority of the sample (81.1%), while 142 were from urban kebeles (18.9%). Pregnant women’s ages ranged from 18 to 38, and respondents’ mean (± standard deviation) age was 27 (± 4.4). A total of 286 pregnant women (38.1%) and 219 (29.2%) of their husbands had no formal education. Four hundred fifty-seven of the pregnant women’s husbands (60.9%) were farmers, while 618 of them (82.4%) were housewives or daily workers. About 24% of pregnant women, or 180 of them, had more than five family members, with a mean (±SD) family size of 4.5 (±1.6) individuals (Table 1).
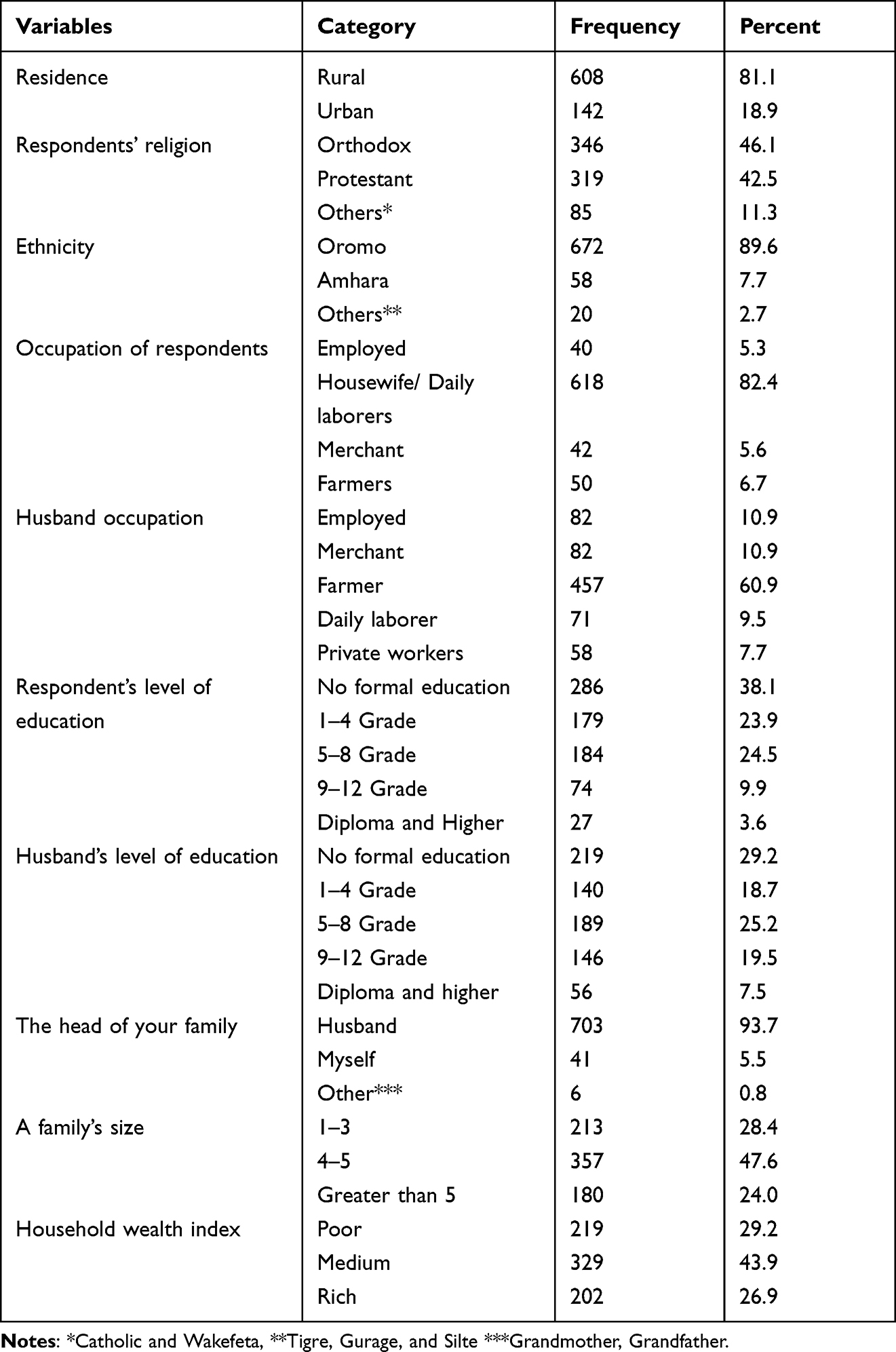 |
Table 1 Socio-Demographic and Economic Characteristics of the Pregnant Women in Ambo District, Ethiopia, 2018, (n =750) |
Maternal and Obstetric Characteristics
The mean (±SD) age of the respondents at marriage was 19.8 ± 2.4. More than half of mothers (58.1%) had previously had an ANC visit, and the majority (70.5%) of women got information on health and nutrition. The majority of responders (69.4%) were multiparous, 84.0% were multigravida, and 83.3% had a pregnancy interval of less than three years (Table 2).
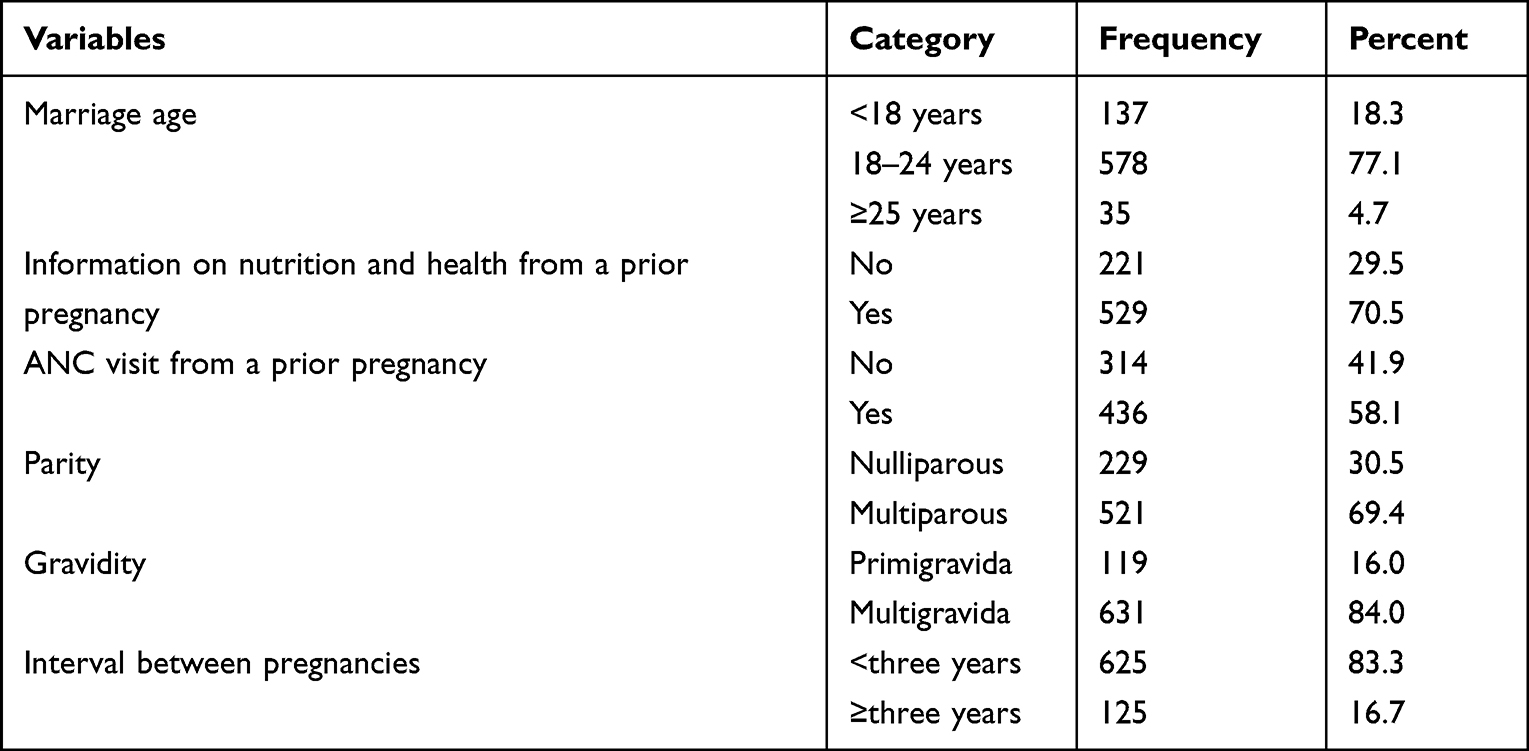 |
Table 2 Maternal and Obstetric Characteristics of the Pregnant Women in Ambo District, Ethiopia, 2018, (n =750) |
Pregnant Women’s Knowledge of Optimal Nutrition and Health Issues
Three hundred twenty-five respondents (43.3%) were well-informed about eating more frequently and increasing portion size as gestational age increased. Five hundred and sixteen of the sampled pregnant women (68% of the total) had good awareness of the variety of diets (of both plant and animal origin) that can be consumed while pregnant. Likewise, 241 (32.1%) of the survey respondents had good awareness of issues pertaining to iron and folate tablets. Three-quarters (75.2%) of participants had a good understanding of supportive lifestyle and care-related topics, while about 30% of participants had a good understanding of questions related to disease prevention and treatment. Overall, 250 participants in the survey (33.3%) had good knowledge on nutrition and health-related issues during this pregnancy (Table 3).
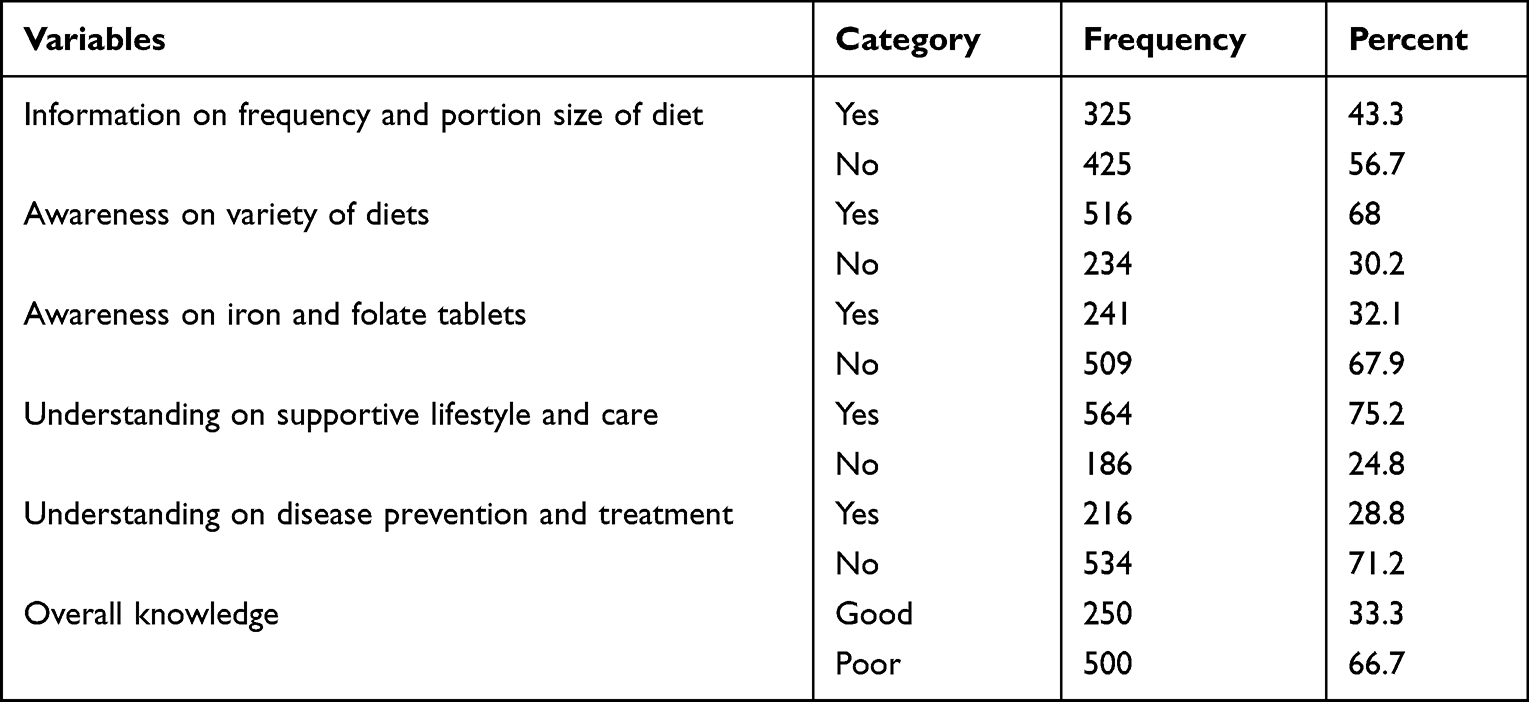 |
Table 3 Knowledge of Pregnant Women on Optimal Nutrition and Health Related Issues in Ambo District, Ethiopia, 2018, (n =750) |
Pregnant Women’s Attitude Toward Optimal Nutrition and Health Issues
As shown in Table 4, for each subtheme of nutrition and health-related questions during pregnancy, about 108 (14.4%), 192 (25.6%), 422 (56.3%), 276 (36.8%), and 308 (41.1%) pregnant women had a favorable attitude, respectively. In this study, the overall favorable attitude of pregnant women was 31.3% (Table 4).
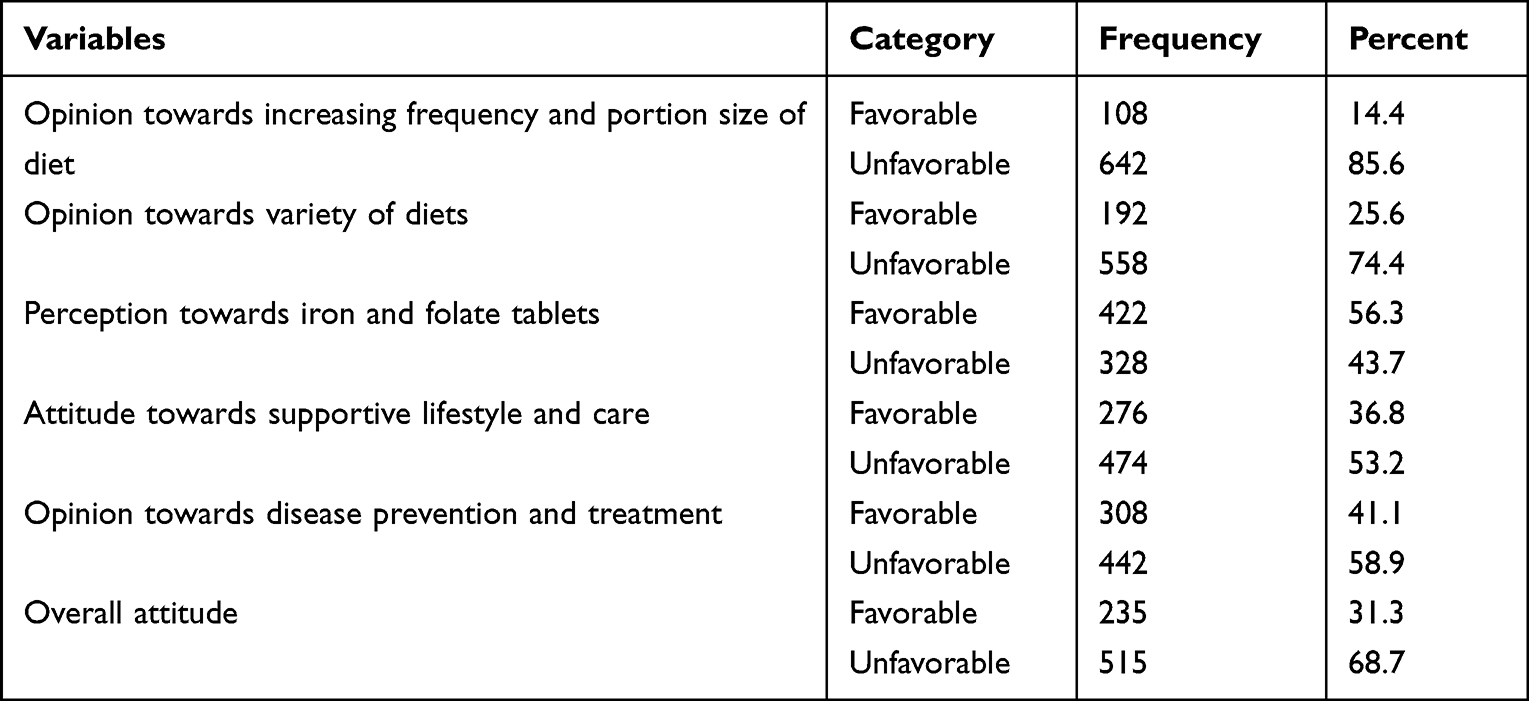 |
Table 4 Attitude of Pregnant Women Towards Optimal Nutrition and Health Related Issues in Ambo District, Ethiopia, 2018, (n =750) |
Predictors of Mothers’ Knowledge and Attitude on Optimal Nutrition and Health
On multivariable logistic regression analysis, residence [AOR=1.7; 95% CI: 1.01–2.88], women’s educational status (primary education [AOR=4.23; 95% CI: 2.36–7.55], and secondary and above education [AOR=5.80; 95% CI: 2.63–12.81]), husband’s educational status (primary education [AOR=3.19; 95% CI: 1.60–6.35], secondary and above education [AOR=4.64; 95% CI: 2.16–9.97], having greater than five family size [AOR=2.13; 95% CI: 1.09–4.14], being in the rich household [AOR=1.93; 95% CI: 1.11–3.38], less than 30 minutes to get to health institution [AOR=1.78; 95% CI: 1.05–3.00], less than or equal to one live birth [AOR=2.96; 95% CI: 1.18–7.40], having nutrition and health information [AOR=1.89; 95% CI: 1.17–3.05] and having counseling on nutrition and health [AOR=1.63; 95% CI: 1.10–2.41] were significantly associated with pregnant women knowledge on optimal nutrition and health.
Likewise, being in the secondary and above education of pregnant women [AOR=3.12; 95% CI: 1.47–6.61], husband educational status (being in the primary education [AOR=4.13; 95% CI: 2.16–7.89], and secondary education and above [AOR=7.65; 95% CI: 3.63–16.13]) being in the medium and rich households [AOR=0.37; 95% CI: 0.23–0.60], and [AOR=0.41; 95% CI: 0.24–0.69], respectively, getting to the health institution takes less than 30 minutes [AOR=2.24; 95% CI: 1.35–3.73], and getting to the health institution within 30–60 minutes [AOR=1.98; 95% CI: 1.28–3.06] were positively associated with an attitude towards optimal nutrition and health of pregnant women (Table 5).
 |
Table 5 A Multivariable Binary Logistic Regression Model Predicting Pregnant Women’s Knowledge and Attitudes Towards Optimal Nutrition and Health in the Ambo District of Ethiopia, 2018 |
Discussion
Good knowledge and a favorable attitude increased the likelihood of adopting appropriate dietary habits and improving health compared to poor knowledge and an unfavorable attitude.43–46 This study assesses the prevalence and predictors of knowledge and attitude of pregnant women about optimal nutrition and health. The results of the study could be used as input for health and nutrition policymakers in order to build evidence-based and effective intervention strategies to improve nutrition and health behaviors and, therefore, nutritional status and birth outcomes.
Overall, 33.3% of the pregnant women in this study were knowledgeable about nutrition and health. This result was higher than the study done in Addis Ababa, Ethiopia (27%),26 but lower than the result found in southern Ethiopia (61.0%).32 This might be because the outcome variables were different—this study focused on the composite variable nutrition and health, whereas the other two studies concentrated on nutritional knowledge—or because the study designs were different—ours was a community-based study, whereas the Addis Abeba study was facility-based. Health care providers and planners should give due attention since more than two-thirds of the pregnant women had poor knowledge. Malnutrition and its adverse impact on both maternal and fetal outcomes are said to have as their immediate source a lack of knowledge about appropriate nutrition and health.32,47
Overall, 31.3% of the pregnant women in this study had a favorable attitude toward optimal nutrition and health, which was consistent with the study conducted in Ethiopia (33.5%),26 lower than the study done in Addis Ababa, Ethiopia (40.5%)32 and (67%) in the Manzini Region of Swaziland.48 The parameter used to measure it and the nature of the outcome variable, the research period, the study design, and sociocultural factors may all be the sources of this variation. Like knowledge, more than two-thirds of the pregnant women had an unfavorable attitude towards nutrition and health. This implies that health care providers, including health extension workers, community health agents, and planners, should work to change the attitudes of pregnant women.
In Ethiopia, a number of factors may have an influence on pregnant women’s knowledge of and attitudes regarding nutrition and health. These factors include women’s educational status, household wealth, access to healthcare facilities, employment status, parity, place of residence, antenatal care visits, and place of delivery.26,32,34 Research carried out in Kenya and India revealed that pregnant women’s knowledge and attitudes toward dietary and health practices were influenced by counseling and health information provided by health professionals during visits to health institutions.31,49
In this study, compared to pregnant women with no formal education, pregnant women with primary and secondary education and above were more likely to have good knowledge and a favorable attitude regarding optimal nutrition and health. This concurs with research conducted in Addis Abeba, southern Ethiopia, and Malaysia.26,32,50 This may be because educated pregnant women are better able to utilize written information resources like articles and other educational materials that are published online, in newspapers, on flyers, and in books. A better understanding and perspective of health and nutrition may result from this, empowering them to fend off outside influences and interference.
Similarly, husbands of pregnant women who had completed primary and secondary education or higher were more likely than those with no formal education to have knowledge of and a favorable attitude towards nutrition and health. This finding is in congruence with the studies done in Ethiopia,51 Cameroon,52 and Ghana.53 One possible explanation for this is that higher husband education may be associated with current knowledge and attitudes about nutrition and health issues, better communication with wives, and lending a higher degree of communication to their wives, which facilitates the sharing of optimum nutrition and health-related issues.
Compared to pregnant women who resided in rural areas, pregnant women from urban areas were more likely to be knowledgeable about optimal nutrition and health. This outcome is consistent with other related research done in southwest Iran.54 This may be due to the fact that people from urban areas were more likely to have access to health facilities where they could obtain knowledge on nutrition and other aspects of health, in addition to from social media and mainstream media. The third reason might be that rural-dwelling women have limited decision-making power and, as a result, little influence over their nutrition and health decisions.55
Pregnant women who traveled the least amount of time (ie, less than 30 minutes and 30–60 minutes) to reach a health facility were more likely to have good knowledge and a favorable attitude regarding optimal nutrition and health than those who traveled more than 60 minutes. This is in line with other research conducted in sub-Saharan African nations.55–57 This may be because households with limited financial resources find it difficult to acquire knowledge about nutrition and health issues and change their unfavorable attitudes because they cannot afford to pay for transportation when receiving a referral or when a medical facility is located far from home.
Pregnant women from rich households were more likely to have good knowledge of optimal nutrition and health than those from poor households. This is supported by studies showing that pregnant women from poor households are less likely to use health facility services because of financial hardship, which challenges families to pay even for nominal fees, transport fees, and compensating the gap left at home to care for children.58,59 The other possible reason could be that those with a higher level of wealth had the opportunity to buy broadcasting materials like radio and television to get better opportunities for nutrition and other health-related information and education. Contrary to this, pregnant women from middle- or upper-wealth families were less likely to have a favorable attitude than those from low-wealth families. For a possible explanation, we might need further studies, especially qualitative and other analytical research, which is recommended.
The odds of having good knowledge about optimal nutrition and health were higher among pregnant women who had more than five household members as compared to those who had less than or equal to three household members. This result was similar to the findings in the Manzini Region of Swaziland48 and Addis Ababa, Ethiopia.51 This might be due to sharing nutrition and health information within the family based on each family member’s preferences, or it might also result from the previous pregnancy experience.
In the present study, the odds of nutrition and health knowledge among multiparous women were higher than those among nulliparous women. This finding is congruent with a previous study conducted in an urban community in Ghana and a rural community in Punjab.53,60 Multiparous mothers are repeatedly exposed to nutrition and health information throughout antenatal follow-up, compared to nulliparous women.
The odds of having good knowledge about optimal nutrition and health were higher among pregnant women who had nutrition and health information as compared to those who had no nutrition and health information. This significant association can be explained by the fact that nutrition and health information have a direct contribution to enhancing women’s optimal nutrition and health knowledge. Similarly, pregnant women who received nutrition and health counseling from health professionals had a significant association with optimal nutrition and health knowledge. This was supported by the study done in Eastern Ethiopia.61 The likely reason for this could be that since clients perceive health professionals as highly credible sources of information, their reinforcement is an important aspect of nutrition and health compliance.
Strength and Limitation of the Study
The strength of this study includes the fact that it was done in the first trimester of pregnancy, which most studies have not done at this gestational age. Furthermore, this study used a tool such as the WHO Essential Nutrition Action (ENA) framework and guidance from formative research for promoting maternal nutrition conducted in developing countries, which is most importantly used to assess pregnant women’s knowledge and attitudes about nutrition and health at this age. The limitations of this study are: First, the knowledge and attitude questions in this study may have been subject to information bias, which may have caused participants to report more favorable responses out of a fear of being judged. Secondly, the cross-sectional study design used did not show causal relationships between variables.
Conclusions
Pregnant women in the study area had suboptimal nutritional and health knowledge and attitudes because more than two-thirds of pregnant women had poor knowledge and an unfavorable attitude towards optimal nutrition and health. Residence, women’s educational status, husband’s educational status, family size, household wealth index, time traveled to reach a health institution, parity, having nutrition and health information, and having counseling on nutrition and health were significantly associated with knowledge on optimal nutrition and health. Likewise, women’s and husbands’ levels of education, household wealth index, and the time required to reach a health institution were positively associated with an attitude toward optimal nutrition and health.
Hence, behavior change communications should be delivered to enhance pregnant women’s knowledge and change their attitudes toward optimal nutrition and health. Further, the Authors recommend that those identified factors need to be further researched with a strong study design, like a follow-up and qualitative study, to show causation (knowledge accumulation, attitudinal change, and impact on health behaviors later).
Data Sharing Statement
Raw SPSS Data will be supplied by the corresponding author upon request.
Ethical Approval and Consent
The institutional Review Board of Jimma University approved the study (ref no. RPGC/40724/2016). Permission to conduct the study in the respective kebeles was granted by Ambo District Health Offices (ref no. ADHO/134/2018), and written informed consent was obtained from participants. Personally identifiable information will not be used in any form in the presentation of the findings. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We are extremely grateful to Jimma University for arranging transportation for the researchers and data collectors. The West Shoa zone and Ambo district staff, as well as the supervisor and data collectors who worked diligently during the study period, are also acknowledged by the authors for allowing the study to take place. Also, we would like to thank all the authors who gave us their published works so that we could evaluate the literature. Finally, we’d like to express our gratitude to the study participants who voluntarily participated in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Jimma University supported the authors for the transportation of researchers, data collectors, and perdium for data collectors.
Disclosure
The authors declare that they have no competing interest in this work.
References
1. Montasser NAE, Helal RM, Megahed WM, et al. Egyptian women’s satisfaction and perception of antenatal care. Int J Trop Dis Health. 2012;2(2):145–156. doi:10.9734/IJTDH/2012/1312
2. World Health Organization, UNICEF. Healthy food and nutrition for women and their families, training course for health professionals; 2019. Available from: http://www.who.dk.
3. IFRC. International federation of red cross and red crescent societies; nutrition guidelines: saving lives, changing minds. Switzerland, Geneva; 2013.
4. MOG. Guidance for formative research on maternal nutrition: prepared for the infant and young child nutrition project; 2011.
5. World Health Organization. Essential nutrition actions: improving maternal, newborn, infant and young child health and nutrition. Geneva; 2013. Available from: https://apps.who.int/iris/handle/10665/84409.
6. Mugyia AS, Tanya AN, Njotang PN, Ndombo PK. Knowledge and attitudes of pregnant mothers towards maternal dietary practices during pregnancy at the Etoug-Ebe Baptist Hospital Yaounde. Health Sci Dis. 2016;17(2):1.
7. Potdar RD, Sahariah S, Gandhi M, et al. Improving women’s diet quality preconceptionally and during gestation: effects on birth weight and prevalence of low birth weight-a randomized controlled efficacy trial in India (Mumbai maternal nutrition project). Am J Clin Nutr. 2014;100(5):1257–1268. doi:10.3945/ajcn.114.084921
8. Imdad A, Bhutta ZA. Maternal nutrition and birth outcomes: effect of balanced protein-energy supplementation. Paediatr Perinat Epidemiol. 2012;26:178–190. doi:10.1111/j.1365-3016.2012.01308.x
9. World Health Organization. Essential nutrition actions: mainstreaming nutrition through the life-course; 2019.
10. EDHS. Ethiopia Mini Demographic and Health Survey in Ethiopia Demographic and Health Survey I, Ethiopia. Addis Ababa: Central Statistical Agency; 2014.
11. EMDHS. Ethiopian mini demographic and health survey, important profile; 2019.
12. ENGINE. Empowering new generations to improve nutrition and economic opportunities, reference manual; 2013.
13. McClure EM, Goldenberg RL, Dent AE, Meshnick SR. A systematic review of the impact of prevention of malaria in pregnancy on low birth weight and maternal anemia. Int J Gynec Obst. 2013;121(103):9. doi:10.1016/j.ijgo.2012.12.014
14. UN. Water global analysis and assessment of sanitation and drinking-water (GLAAS) 2017 report: financing universal water, sanitation and hygiene under the sustainable development goals. Geneva: World Health Organization; 2017.
15. World Health Organization. Global Technical Strategy for Malaria 2016–2030. Geneva: World Health Organization; 2015.
16. World Health Organization. Implementing Malaria in Pregnancy Programs in the Context of World Health Organization Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: World Health Organization; 2018.
17. Kassie GA, Adella GA, Gebrekidan AY, et al. Insecticide-treated bed net utilization and associated factors among pregnant women in Ethiopia: a systematic review and meta-analysis. Malar J. 2023;22(223):5. doi:10.1186/s12936-023-04655-7
18. World Health Organization. Health topics on Soil transmitted infections; 2023.
19. Feleke BE, Jember TH. Prevalence of helminthic infections and determinant factors among pregnant women in Mecha district, Northwest Ethiopia: a cross sectional study. BMC Infect Dis. 2018;18(1):1–6. doi:10.1186/s12879-018-3291-6
20. World Health Organization. Guideline: Preventive Chemotherapy to Control Soil-Transmitted Helminth Infections in at-Risk Population Groups. World Health Organization; 2017.
21. Bantie B, Kassaw Yirga G, Ayenew YE, et al. Deworming utilization among pregnant mothers with at least one antenatal care follow-up in Ethiopia: a multilevel analysis. PLoS One. 2022;18(1):6. doi:10.1371/journal.pone.0279967
22. Guyon AB, Quinn VJ. Essential Nutrition Action Frame Work. Training Guide for Health Workers. Washington DC: Core Group; 2011.
23. Zegeye B, Adjei NK, Olorunsaiye CZ, et al. Pregnant women’s decision-making capacity and adherence to iron supplementation in subSaharan Africa: a multi-country analysis of 25 countries. BMC Pregnancy Childbirth. 2021;21(822). doi:10.1186/s12884-021-04258-7
24. Mudor H, Bunyarit F. A prospective of nutrition intake for pregnant women in Pattani, Thailand. Procedia Soc Behav Sci. 2013;91:179–184. doi:10.1016/j.sbspro.2013.08.415
25. USAID. Multi-Sectoral Nutrition Strategy Technical Guidance Brief: Maternal Nutrition for Girls Women. Washington, DC: USAID; 2014:1–10.
26. Zelalem T, Erdaw A, Tachbele E. Nutritional knowledge, attitude and practices among pregnant women who attend antenatal care at public hospitals of Addis Ababa, Ethiopia. Int J Nurs Midwifery. 2018;10(7):81–89. doi:10.5897/IJNM2017.0289
27. Swanson V, Hart J, Byrne-Davis L, Merritt R, Maltinsky W. Enhancing behavior change skills in health extension workers in Ethiopia: evaluation of an intervention to improve maternal and infant nutrition. Nutrients. 2021;13(6):1995. doi:10.3390/nu13061995
28. Saldanha LS, Buback L, White JM, et al. Policies and program implementation experience to improve maternal nutrition in Ethiopia. Food Nutr Bull. 2012;33:S27–50. doi:10.1177/15648265120332S103
29. Hambidge KM, Krebs NF. Strategies for optimizing maternal nutrition to promote infant development. Reprod Health. 2018;15(87). doi:10.1186/s12978-018-0534-3
30. Zerfu TA, Biadgilign S. Pregnant mothers have limited knowledge and poor dietary diversity practices, but favorable attitude towards nutritional recommendations in rural Ethiopia: evidence from community-based study. BMC Nutrition. 2018;4(43). doi:10.1186/s40795-018-0251-x
31. Perumal N, Cole DC, Ouédraogo HZ, et al. Health and nutrition knowledge, attitudes and practices of pregnant women attending and not-attending ANC clinics in Western Kenya: a cross-sectional analysis. BMC Pregnancy Childbirth. 2013;13(146):1. doi:10.1186/1471-2393-13-146
32. Gezimu W, Bekele F, Habte G. Pregnant mothers’ knowledge, attitude, practice and its predictors towards nutrition in public hospitals of Southern Ethiopia: a multicenter cross-sectional study. SAGE Open Med. 2022;10:1–10. doi:10.1177/20503121221085843
33. Chakona G, Shackleton C. Food taboos and cultural beliefs influence food choice and dietary preferences among pregnant women in the Eastern Cape. South Afr Nutri. 2019;11(2668). doi:10.3390/nu11112668
34. CSA, ICF. Central Statistical Agency (CSA) [Ethiopia] and ICF, Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia, and Rockville, Maryland: CSA, ICF; 2016.
35. Girma AT, Molla AK, Genetu AE. Dietary practice and associated factors among pregnant women at public health institution in Mizan-Aman Town, Southwest Ethiopia. Nutr Metab Insights. 2021;14. doi:10.1177/11786388211057796
36. Mulugeta YD, Degu GA, Belachew T. Dietary practices and associated factors among pregnant women in West Gojjam Zone, Northwest Ethiopia. BMC Pregnancy Childbirth. 2020;20(1):18. doi:10.1186/s12884-019-2702-z
37. Kedir H, Yemane B, Alemayehu W. Magnitude and determinant of malnutrtion among pregnant women in eastern Ethiopia. Evidence from rural, community based setting. Matern Child Nutr. 2016;12:51–63. doi:10.1111/mcn.12136
38. CSA. Population size by sex, area and density by Region, Zone and Wereda. 2022.
39. Daba G, Beyene F, Garoma W, Fekadu H. Assessment of nutritional practices of pregnant mothers on maternal nutrition and associated factors in Guto Gida Woreda, East Wollega Zone, Ethiopia. Sci Technol Arts Res J. 2013;2(3):105–113. doi:10.4314/star.v2i3.98748
40. Diddana TZ, Kelkay GN, Dola AN, Sadore AA. Effect of nutrition education based on health belief model on nutritional knowledge and dietary practice of pregnant women in Dessie town, Northeast Ethiopia: a Cluster Randomized Control Trial. J Nutr Metab. 2018;2018:1–10. doi:10.1155/2018/6731815
41. WestJr KP, Christian P, Labrique AB, et al. Effects of vitamin a or Beta carotene SupplementationonPregnancy-RelatedMortality and infant mortality in rural Bangladesh. A Cluster Randomized Trial. JAMA. 2011;305(19):1986–1995. doi:10.1001/jama.2011.656
42. CSA, ICF. Central Statistical Agency (CSA) [Ethiopia] and ICF, Ethiopia Demographic and Health Survey. Addis Ababa and Rockville: CSA and ICF; 2016.
43. Abel G, Amare G, Ermias A, Dawit G. Determinants of dietary practice among pregnant women at the public hospitals in Bench-Sheko and Kaffa Zones, Southwest Ethiopia. BMC Nutri. 2022;8(88). doi:10.1186/s40795-022-00588-7
44. Eni-Olorunda T, Akinbode OO, Akinbode AO. Knowledge and attitude of mothers on risk factors influencing pregnancy outcomes in Abeokuta South Local Government Area, Ogun State. Eur Sci J. 2015;11(11):1.
45. Yalewdeg M, Birhane M, Adissu Y. Dietary practices and their determinants among pregnant women in Gedeo Zone, Southern Ethiopia: a community-based cross-sectional study. Dove Press J. 2020;12:267–275. doi:10.2147/NDS.S267453
46. Nana A, Zema T. Dietary practices and associated factors during pregnancy in northwestern Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):183. doi:10.1186/s12884-018-1822-1
47. Ibikunle HA, Okafor IP, Adejimi AA. Pre-natal nutrition education: health care providers’ knowledge and quality of services in primary health care centres in Lagos, Nigeria. PLoS One. 2021;16(11):e0259237. doi:10.1371/journal.pone.0259237
48. Masuku SKS, Lan SJ. Nutritional knowledge, attitude, and practices among pregnant and lactating women living with HIV in the Manzini Region of Swaziland. J Health Popul Nutr. 2014;32(2):261–269. PMCID: PMC4216962.
49. Ghosh-Jerath S, Devasenapathy N, Singh A, Shankar A, Sodpey S. Ante natal care (ANC) utilization, dietary practices and nutritional outcomes in pregnant and recently delivered women in urban slums of Delhi, India: an exploratory cross-sectional study. Reprod Health. 2015;12(20). doi:10.1186/s12978-015-0008-9
50. Wong JL, Zhe Xin L, Ying Lim P, Keng SL. Knowledge of nutrition during pregnancy and associated factors among Antenatal mothers. Int J Public Health Clin Sci. 2018;5(1):1.
51. Tesfa S, Aderaw Z, Tesfaye A, Abebe H, Tsehay T. Maternal nutritional knowledge, practice and their associated factors during pregnancy in Addis Sub city health centers, Addis Ababa, Ethiopia. Int J Afr Nurs Sci. 2022;17(2):100482. doi:10.1016/j.ijans.2022.100482
52. Nchangmugyia AS, Nguti A, Tanya K, Njotang PN, Ndombo PK. Knowledge and attitudes of pregnant mothers towards maternal dietary practices during pregnancy at the Etoug- Ebe Baptist Hospital Yaounde. Health Sci Dis. 2016;17:24–29.
53. Appiah PK, Naa Korklu AR, Korklu N, Bonchel DA, Fenu GA, Wadga-Mieza Yankey F. Nutritional knowledge and dietary intake habits among pregnant adolescents attending antenatal care clinics in urban community in Ghana. J Nutr Metab. 2021;2021:8835704. doi:10.1155/2021/8835704
54. Naghashpour M, Mansouri S, Vadizadeh A, Cheraghian B, Fallahi R, Vaziri F. Determinants of nutritional knowledge, attitude, and practice among southwestern Iranian households: a community-based study. Nutr Health. 2020;26(2):93–102. doi:10.1177/0260106020905419
55. Kifle MM, Kesete HF, Gaim HT, Angosom GS, Araya MB. Health facility or home delivery? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. J Health Popul Nutr. 2018;37(22). doi:10.1186/s41043-018-0153-1
56. Moyer CA, Mustafa A. Drivers and deterrents of facility delivery in subSaharan Africa: a systematic review. Reprod Health. 2013;10(40). doi:10.1186/1742-4755-10-40
57. Aremu O, Lawoko S, Dalal K. Neighborhood socioeconomic disadvantage, individual wealth status and patterns of delivery care utilization in Nigeria: a multilevel discrete choice analysis. Int J Womens Health. 2011;3:167–174. doi:10.2147/IJWH.S21783
58. Muzaffar N. Maternal health and social determinants: a study in Jammu and Kashmir. Public Health Res. 2015;5(5):144–152. doi:10.5923/j.phr.20150505.04
59. Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK, Souza JP. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. 2015;12(6):e1001847. doi:10.1371/journal.pmed.1001847
60. Singh T, Deepti SS, Deepti SS. Knowledge, attitude, practice and determining factors regarding nutrition during pregnancy among females of rural Punjab. Int J Community Med Public Heal. 2019;6(7):2874. doi:10.18203/2394-6040.ijcmph20192818
61. Berhane A, Belachew T. Effect of Picture-based health education and counselling on knowledge and adherence to preconception Iron-folic acid supplementation among women planning to be pregnant in Eastern Ethiopia: a randomized controlled trial. J Nutr Sci. 2022;11(e58):1. doi:10.1017/jns.2022.51
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with Research knowledge and Attitude among Clinical Midwives Working at Public Health Facilities of Northwest Ethiopia, 2021: A Cross-Sectional Study
Gebresilassie KY, Wami SD, Baraki AG, Kassie BA
Advances in Medical Education and Practice 2022, 13:661-670
Published Date: 6 July 2022
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Comprehensive Knowledge, Attitudes, Behaviors, and Associated Factors of HIV/AIDS in Gondar City Public Health Facilities Among HIV Testing and Counselling Service Users, Northwest Ethiopia, 2022; an Ordinal Logistic Regression Analysis
Terefe B, Techane MA, Assimamaw NT
HIV/AIDS - Research and Palliative Care 2023, 15:713-726
Published Date: 7 December 2023
Sex Disparities: Couple’s Knowledge and Attitude Towards Obstetric Danger Signs and Maternal Health Care: in Rural Jimma Zone of Ethiopia
Shibeshi KA, Lemu YK, Gebretsadik LA, Gebretsadik AM, Morankar S
International Journal of Women's Health 2024, 16:987-1007
Published Date: 30 May 2024