Back to Journals » Nursing: Research and Reviews » Volume 12
Knowledge, Attitude, Perceived Responsibilities, and Associated Factors Regarding Colostomy Care Among Nurses Working in Surgical Units at Amhara Region General and Referral Hospitals, Ethiopia: A Mixed Method Study
Authors Tiruneh TE ![]() , Alem G
, Alem G ![]() , Taddele M, Tizazu ZM, Minale FK
, Taddele M, Tizazu ZM, Minale FK ![]() , Alemu KD
, Alemu KD ![]()
Received 8 April 2022
Accepted for publication 22 September 2022
Published 13 October 2022 Volume 2022:12 Pages 191—206
DOI https://doi.org/10.2147/NRR.S367050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Natasha Hodgkinson
Tsegaye Eneyew Tiruneh,1 Girma Alem,2 Mekuanint Taddele,3 Zewedu Minewey Tizazu,1 Fasil Kefale Minale,1 Kasaye Demeke Alemu4
1Department of Nursing, Debre Markos Comprehensive Specialized Hospital, Debre Markos, Ethiopia; 2Department of Nursing College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 3Departments of Public Health College of Health Sciences, Injibara University, Debre Markos, Ethiopia; 4Department of HIV/AIDS Prevention Care and Treatment, International Center for AIDS Care Program/ICAP, Bahir Dar, Ethiopia
Correspondence: Tsegaye Eneyew Tiruneh, Tel +251920273593, Email [email protected]
Background: Colostomy is one of the commonest lifesaving procedures worldwide with aims of decompression of an obstructed colon or diversion of feces. Colostomy care is important to improve the quality of life of the patient, yet information is scarce concerning knowledge, attitude, and role of nurses on colostomy care in Ethiopia generally and in Amhara region specifically.
Objective: This study aimed to assess knowledge, attitude, perceived responsibility, and associated factors regarding colostomy care among nurses working in surgical units at Amhara region general and referral hospitals, Ethiopia.
Methods: A cross-sectional, mixed method study was conducted from March 1 to 30, 2020 using a census method. The data were collected using semi-structured, self-administered questionnaire and in-depth interview. Analytic schemes including bivariable and multivariable logistic regression were computed considering P-value < 0.05 to identify statistically significant factors. Qualitative data were analyzed with thematic content analysis.
Results: In the current study, the adequate knowledge of nurses was found to be 40.4% (95% CI: 35.4– 45.8). Clinical experience, colostomy care guidelines, gave care for colostomy patient, ever received colostomy care training, and read professional literature regularly were significantly associated with adequate knowledge. Favorable attitude of nurses was found to be 49.6% (95% CI: 45– 54.5). Presence of colostomy care guidelines, gave care for colostomy patients, and adequate knowledge were significantly associated with favorable attitude. Nurses have a strong professional perception of caring for colostomy patients but lack of training, inadequate supplies, and lack of professional perquisite are barriers identified.
Conclusion: In the present study, nearly half of nurses had only adequate knowledge and favorable attitude, but the majority of nurses perceived their responsibilities towards colostomy care. Therefore, taking part in care, developing guidelines, providing training and fulfilling nurses’ perquisite are needed to enhance the knowledge, attitude, and responsibility of nurses towards colostomy care.
Keywords: colostomy care, knowledge, attitude, perceived responsibility
Background
According to the colostomy guide, colostomy is an artificial opening in the abdominal wall that is made during surgery so stools are able to pass and drain outside the body via an opening.1 Colostomy is the most common ostomy type.1 It’s usually needed because a problem is causing the colon to not work properly due to obstructions or perforation of the intestine and rectum, congenital malformations, medical problems such as rectal cancer, diverticular disease, trauma affecting the colon and incontinence and it needs to be removed.1,2
Colostomy can be temporary or permanent. The temporary colostomy is reversed and normal bowel movements are restored. Whereas, permanent colostomy provides an exit for stool but will not be closed in the future. The types of colostomies are usually identified by the location of the stoma: ascending, transverse, descending/sigmoid. Colostomy differs in types which are loop, end and loop end stoma. The appearance of the stoma depends on individual differences in the human body and the type of colostomy. While the stoma may be quite large at first, it will shrink gradually and attain its final size in six to eight weeks.1,3
The colostomy operation is known worldwide as an efficient method of life saving, but it may cause various physical, social, and psychological disorders4,5 which including flatus odor, fecal leakage, peristomal skin problems, fatigue, anorexia, dyspepsia, nausea, diarrhea, constipation, and pain.1 Nursing care is significant to improve the quality of life of the patient by preventing these complications and to minimize the psychological and physiological adjustment to the created colostomy.4
Nurse and other health-care providers’ knowledge, attitude and responsibilities have a significant role for colostomy care5,6 that can change the attitude of a patient and their family agreement about colostomy.7 However, fulfilling this role successfully can be determined merely when nurses are supported by the requisite knowledge, attitude, and skills. Nursing care that is provided to a colostomy patient can be depending on the type of colostomy.5
Nurses should be sensitized and counseled about colostomy care to be mentally prepared before surgery and give care and train the patient how to care for themselves after surgery. Nurses should also educate the patient about colostomy bags, i.e. that they have no effect on eating habits and if cared for properly have no smell and it is even difficult to notice someone who uses them. In Aga Khan University Hospital there is a support group for stoma and cancer patients that regularly meets to sensitize about the condition.8
Nurses should assess patients’ physical, social, and emotional factors that may have an impact on the ability to carry out colostomy care. Patients may have comorbidities that obstruct coordination and function, such as post amputation, post-stroke weakness, Parkinson’s disease, or severe arthritis and other infirmities. Plan of care should be evaluated for patient taking into account visual acuity. Self-colostomy care may be overwhelming for the infirm and fatigue may mean a patient is too weak to perform it.6 In broad, colostomy is a way of treatment for some diseases and needs knowledge, appropriate attitude, and perceived responsibilities to perform the care. Nurses have enormous input in providing the colostomy care and educating a patient with a colostomy.
Studies have reported that approximately 750 thousand colostomy surgery done in the United States in the age range from newborn to 90 years.1 It is estimated that over 10 to 21 thousand new ostomies are created each year in the UK.9 Similarly in Ethiopia, colostomy surgery is a prevalent procedure which was reported 253 colostomies were done in Addis Ababa within two years.10
Colostomy is a global public health issue which leads to a variety of social, economic, and psychological health impacts, markedly in sub-Saharan Africa where impacts are highly increased compared with high-income countries.11 It needs safety and precision nursing care to reduce the negative impact of colostomy and improve patients’ quality of life.12
Despite the aim of colostomy being to relieve patients’ pain and discomfort, in cases of inadequate and inappropriate colostomy care it causes early complications such as skin irritation, erosion, and ulceration (25–34%) and late complication of stoma prolapse (8–75%), and 19% of initially temporary colostomies become permanent, therefore it is believed to pose huge economic and social impacts on individuals, society, and the nation at large.13 Impacts also affect caregivers, where over 47% of spouses had left their family and 93% had left their jobs to care for a patient with a stoma.11,14
Colostomy leads to changes in a patient’s body image and also affects the self-esteem negatively in general and experience of negative feeling and fear in particular.15 Colostomy intensely influences the quality of life, indicated by more anxious symptoms, feeling of disabilities and lower adjustment to new life. Patients who receive appropriate education and guidance during the preoperative period had a better adaptation to the situation.16 In addition, patients with colostomy may also experience embarrassment, feeling of uncleanness and feeling of disgust with the ostomy appliance so patients should have appropriate nursing counseling services to adjust their lives with colostomy.17
In spite of the fact that nurses are vanguard health professionals who play a key role in caring of patients with colostomy, conversely a descriptive cross sectional study in Turkey shows that 74% of nurse did not perceive colostomy care as a responsibility.6
Yet an adequate knowledge and favorable attitude are essential components in the delivery of colostomy care.18,19 Nurses are frontline health professionals, who provide colostomy care in the surgical unit. However, studies show that there was lack of knowledge and unfavorable attitude among nurses towards colostomy care.20,21 Another study revealed that 79.3% of nurses had inadequate knowledge22 and 70% of nurses had unfavorable attitude towards colostomy care.5
To the best of researchers’ knowledge, there is limited study regarding knowledge, attitude, perceived responsibilities and factors regarding colostomy care among nurses in Ethiopia. Therefore, understanding knowledge, attitude, perceived responsibilities and their factors is important to improve the colostomy care process, and would help hospitals in providing a basis for planning and integrating the necessary involvement to solve the identified factors.
Methods
Study Setting
The study was conducted in Amhara region public general and referral hospitals. An institutional based mixed method study design was conducted from March 1 to 30, 2020. Amhara region is one of the nine regional states in Ethiopia which has thirteen zones and holds six referral and three general public hospitals which are distributed throughout eight zones. University of Gonder, Tibeb Ghion, Debremarkos, Debrebirhan, Felegehiwot, and Dessie Referral Hospitals are found 748 km, 564 km, 299 km, 130 km, 564 km, and 400 km, respectively and Debretabor, Injibara and Weldiya General Hospitals are found 667 km, 447 km, and 520 km, respectively from the capital of Ethiopia. There were 49, 48, 55, 68, 75, 37, 38, 34, and 28 nurses working in surgical wards of Debrebirhan, Debremarkos, Dessie, Felegehiwot, Gondar, Tibeb Ghione, Debretabor, Weldiya, and Injibara hospitals, respectively.
Population
In this study, the source population were all nurses who were working in surgical units and available during the data collection period at Amhara region general and referral hospitals surgical units. Among these, those who did not wish to participate were excluded from the study.
Sample Size and Sampling Procedures
Quantitative Part
The sample size was determined by using a single population proportion formula by considering population proportion (p) (51.3%) of knowledge towards colostomy care among nurses which was taken from a study conducted in Addis Ababa, Ethiopia,23 Z σ/2 = 1.96 = at 95% confidence level, 5% margin of error (d).

The minimum number required was calculated as 383, and 10% added to compensate non-response rate. Then final sample size was [383+ (383x10%)] 421 nurses. Therefore, all 432 nurses who were working in the surgical ward at Amhara Region General and Referral Hospitals were included in the census method (Table 1).
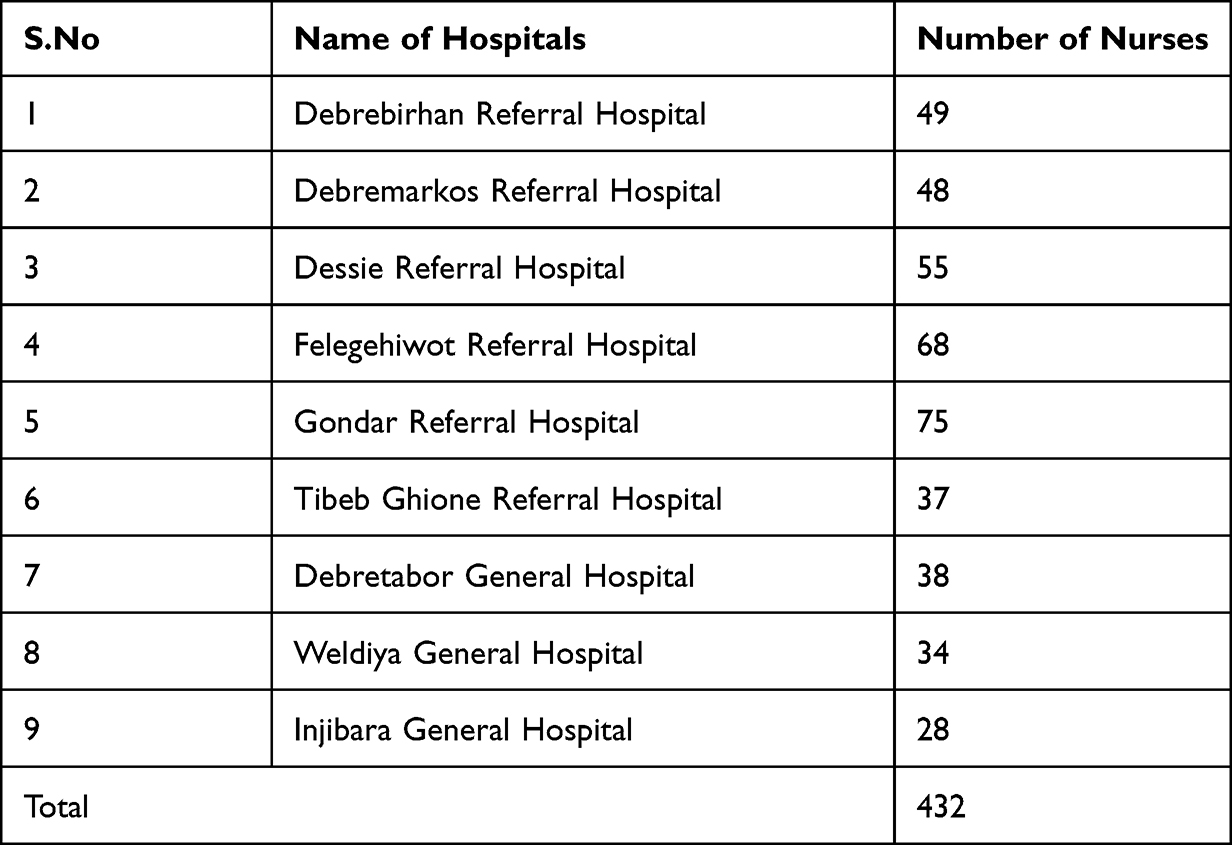 |
Table 1 Number of Nurses Who Work in Surgical Unit in Amhara Region General and Referral Hospitals That Was Sample of This Research, 2020 |
Qualitative Part
Purposive sampling was used to select participant nurses by their experience and willingness to participate24 and data were collected from three randomly selected referral hospitals at Amhara region for in-depth interview. Thirteen BSc nurses were involved in the in-depth interview. The recruitment process continued until data saturation was reached; this was when no new data emerged during interviews.
Study Variables
Dependent Variable
Knowledge, attitude and perceived responsibilities about colostomy nursing care.
Independent Variables
Socio-demographic factors (age, sex, religion, marital status, income, educational status, and institution where nurses obtained their educational award), Managerial/work-related factors (current working hospital, specialty of hospital, surgical unit experience, total clinical experience, presence of colostomy care guidelines and use of colostomy care guidelines), Professional related factors (taking colostomy training/meeting within 6–8 months, ever attended colostomy training/meeting, taking colostomy care lesson during their study, referred literatures on colostomy care within 6 months, read professional literature on colostomy care regularly and care of patients with colostomy).
Operational Definition
Adequate Knowledge
Nurses who answered the mean and above of the knowledge questions (53%).7,23
Inadequate Knowledge
Those nurses who answered less than the mean of the knowledge questions.
Favorable Attitude
Those nurses who scored the mean and above of the attitude questions (57.6%).7
Unfavorable Attitude
Those nurses who scored less than the mean of the attitude questions.
Data Collection Tools and Procedures
Quantitative Part
A pre-tested semi-structured, self-administered questionnaire was adapted from different previous works of literature and guidelines.1,6,7,20,23 The questionnaire consists of socio-demographic characteristics, work and professional related data, nurses’ knowledge towards colostomy care (8 true false and 17 multiple choice items with a total range of 0–25) and nurses’ attitude towards colostomy care (9 questions with 5 point Likert scale: from “strongly agree = 5” to “strongly disagree = 1” with a total score range of 9–45). For this purpose, nine BSc nurses participated as data collectors. Furthermore, continuous follow-up was also made by research team members throughout the data collection period.
Qualitative Part
In-depth interviews were taken in face-to-face semi-structured interview guide questions.24 The guide was developed after literature review.1,6,7,20,23 It was first developed in English and then translated to the local language (Amharic) to facilitate communication with participants. The interview questions focused on nurses’ perceived responsibility and barriers encountered to perform colostomy care. All interviews were taken by audio recorder and notes were taken during interviews. The principal investigator who conducted the interview started with an introduction and explanation of the purpose of the study and confidentiality. Data were transcribed and grouped under selected themes then translated to English by a language expert to analyze. Coded data were sorted and matched to identify similarities and differences. Finally, the data were summarized and narrated manually.
Data Quality Control
The tool was checked for completeness, clarity, and content validity by an expert and pre-tested in 5% of the total sample at Finote Selam hospital. Based on the findings, unclear questions and ambiguous words were modified. Data collectors and supervisors were trained for a day on the data collection tool and data collection process. The internal consistencies of questionnaire items were very good as evidenced by the overall Cronbach’s Alpha of 0.87. Data were checked for completeness throughout the data collection by the supervisor and the principal investigator daily and the necessary corrective feedback was given to data collectors.
Statistical Data Management and Analysis
Quantitative Part
Data were coded and entered into EpiData version 3.1 and checked for completeness, cleaned to check for frequencies, accuracy, consistencies, outliers, missed values, and variables. The data were exported to Statistical Package for Social Science (SPSS) version 25 for analysis. Descriptive statistics such as frequency, percentage, tables, charts, were used depending on the nature of the variable. The assumption of the logistic regression mode was checked using a Hosmer and Lemeshow goodness of fit test. Binary logistic regression analysis was computed to assess the associations of the independent variables. In the bivariable analysis variables with p-value < 0.25 were entered into the multivariable logistic regression. Variables with a p-value of <0.05 at multivariable analysis were considered as significantly associated with the outcome variable. The strength of association between independent and outcome variable was assessed using adjusted odds ratio (AOR) with 95% confidence interval (CI).
Qualitative Part
All the interviews were transcribed verbatim. Transcripts and translations were cross checked for accuracy and consistency. Translated notes were read and re-read by researchers to review the codes and discussed the categories and themes to ensure that the participants’ perspectives are accurately and appropriately represented. Identification codes were developed based on each participant’s current order of interview in order to label verbatim quotes without breaking confidentiality. The researcher identified themes and sub-themes from the data and thematic analysis was used to identify themes and sub-themes by grouping related codes.
Results
Study Participants’ Characteristics
A total of 413 participants were included in this study with a response rate of 97.6%. About 54.5% of respondents were females. The mean (±SD) age of the participants was 28.25 (±3.38) years and the majority (88.9%) were orthodox Christian. Regarding marital status 49.2% were married, nearly two-thirds (71.7%) had >5000 birr income, similarly nearly two-thirds (70.5%) were educated at a governmental institution (Table 2).
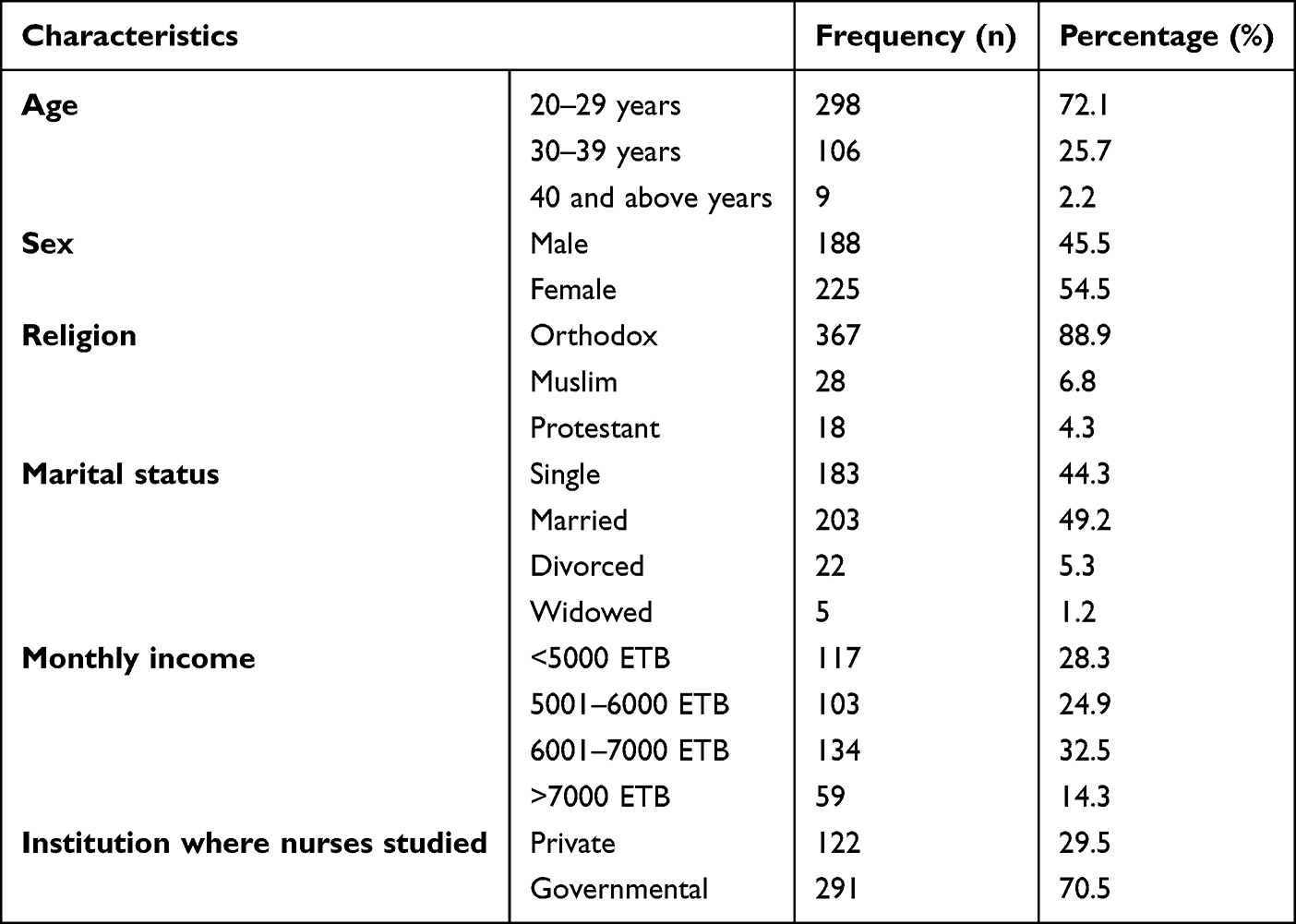 |
Table 2 Socio-Demographic Characteristics of the Study Participants at Amhara Region General and Referral Hospitals (n = 413), 2020 |
More than three-quarters (94.4%) of respondents were bachelor’s degree holders (Figure 1).
 |
Figure 1 The bar graph of the nursing qualification level of knowledge, attitude, perceived responsibilities and associated factors regarding to colostomy care among nurses working in surgical unit at Amhara region general and referral hospitals, Amhara, Ethiopia, 2020 (n = 413). |
Managerial/Work Related Factors
Three-quarters (74.3%) of respondents were from non-teaching hospitals, among these 77.2% were at referral hospitals, and 17.7% were from Gonder referral hospital. Nearly half (47.2%) of respondents had greater than 6 years of clinical experience and 40% of respondents responded positively regarding presence of colostomy care guidelines and only 13.3% of them used colostomy care guidelines in their work area (Table 3).
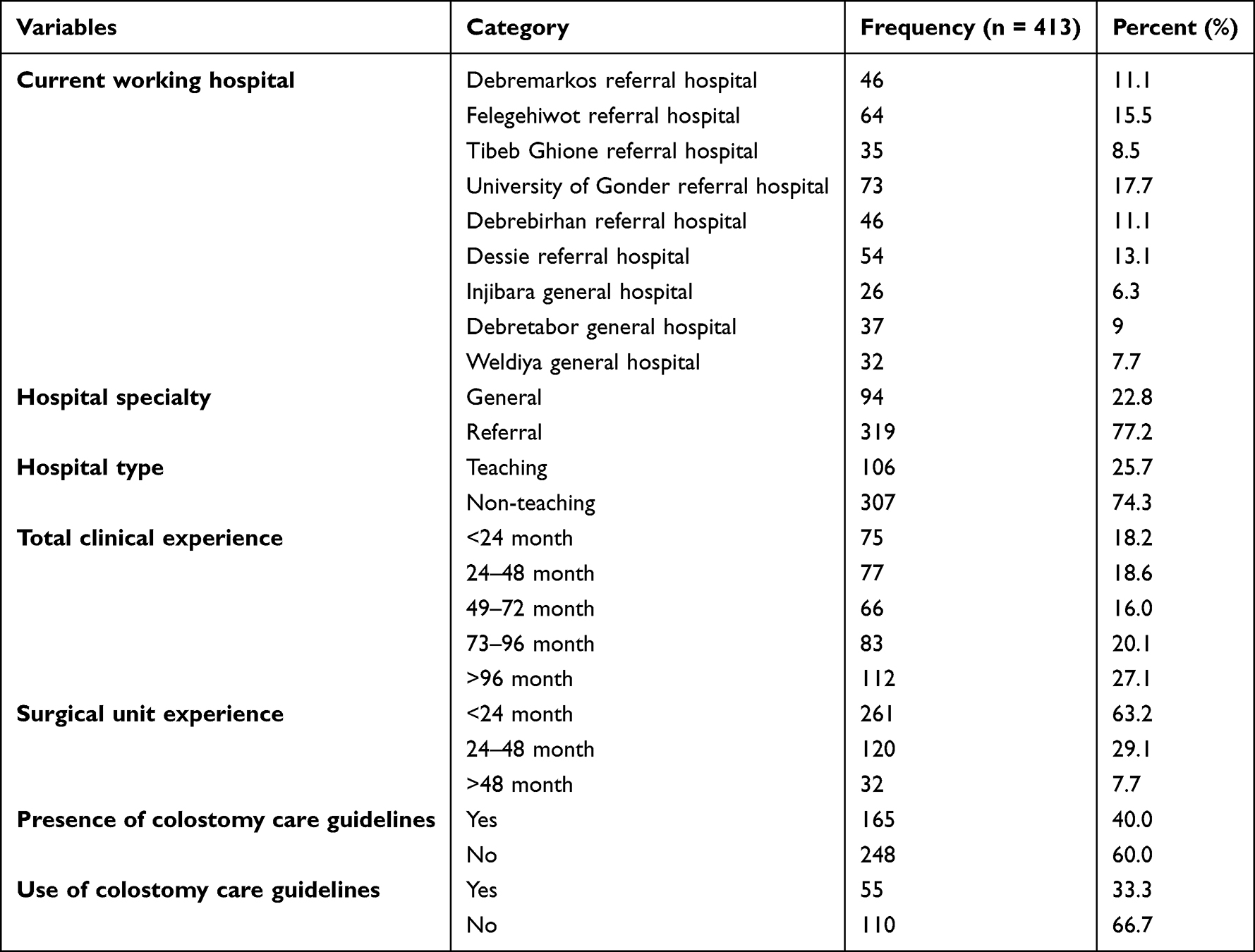 |
Table 3 Managerial/Work Related Characteristics of the Study Participants at Amhara Region General and Referral Hospitals (n = 413), 2020 |
Professional Related Factors
One-third (32.2%) of respondents have not learnt formal colostomy care in their nursing qualification study. Only 42.1% of study participants had cared for less than five patients in the last six months. Less than one-quarter (16%) of respondents had received training on colostomy care within the last six to eight months. Seventy-one (17.2%) respondents had ever attended training/meetings on colostomy care during their service period. Almost three-quarters (73.1%) of nurses have not referred to literature on colostomy care within the last six months and 62.7% of nurses also have not read professional literature regularly (Table 4).
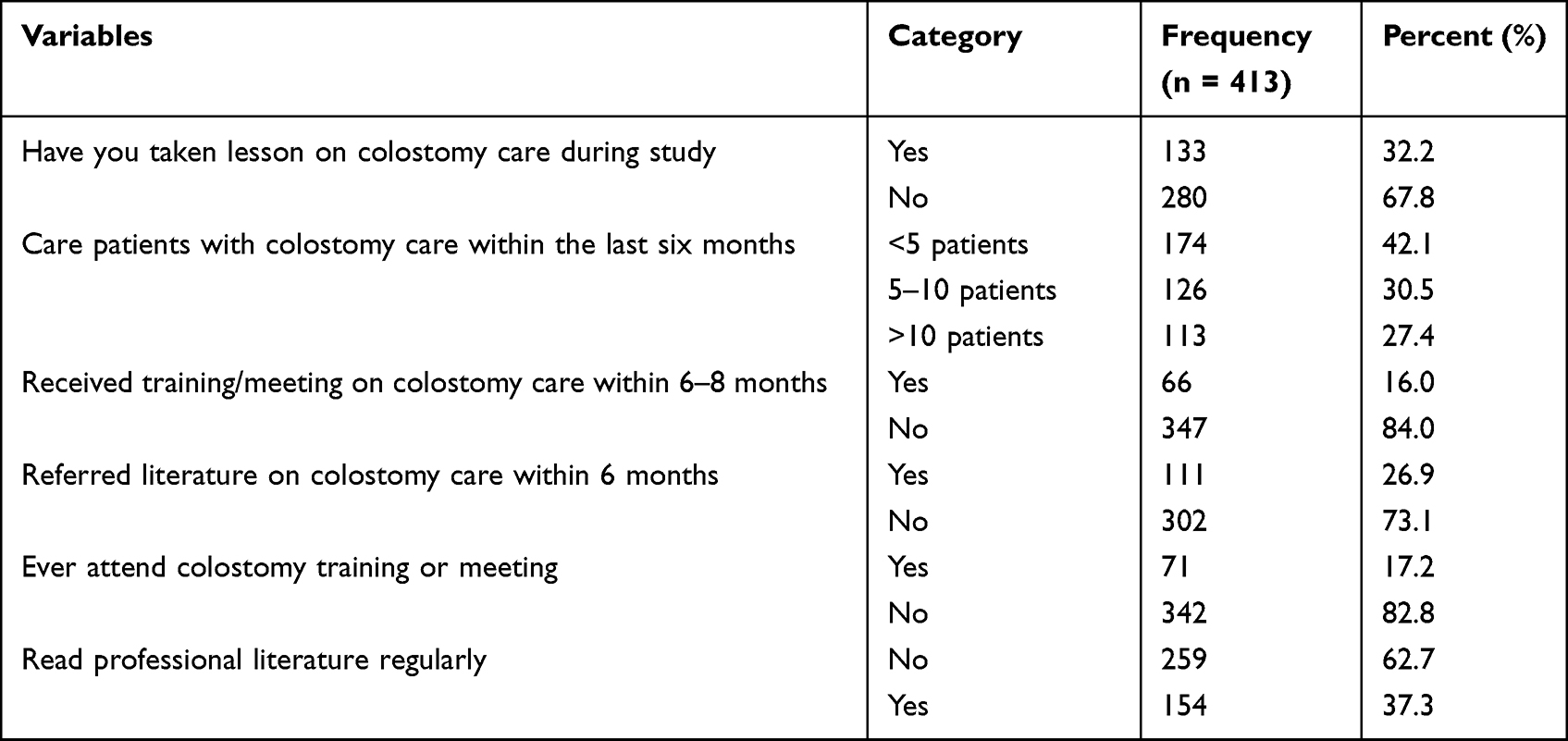 |
Table 4 Professional Related Characteristics of the Study Participants at Amhara Region General and Referral Hospitals (n = 413), 2020 |
Knowledge of Nurses Towards Colostomy Care
Nearly two-thirds of participants (69.5%) correctly answered the time of return to previous activities after colostomy surgery. From participants, 45.3% answered correctly on how location of colostomy affects colostomy output and bathing with colostomy. More than half (55%) of participants correctly respond about temporary colostomy, whereas 62% of participants knew about colostomy surgery. Regarding to the use of odor reduction filter to an ostomy bag to release the gas, 57.6% of nurses answered correctly (Table 5).
 |
Table 5 Frequency and Percentage Distribution of Knowledge (True/False) Item Questions About Colostomy Care at Amhara Region General and Referral Hospitals (n = 413), 2020 |
The majority (72.9%) of participants knew the use of colostomy opening and only 35.8% of the nurses correctly expected the fecal output from a colostomy (Table 6).
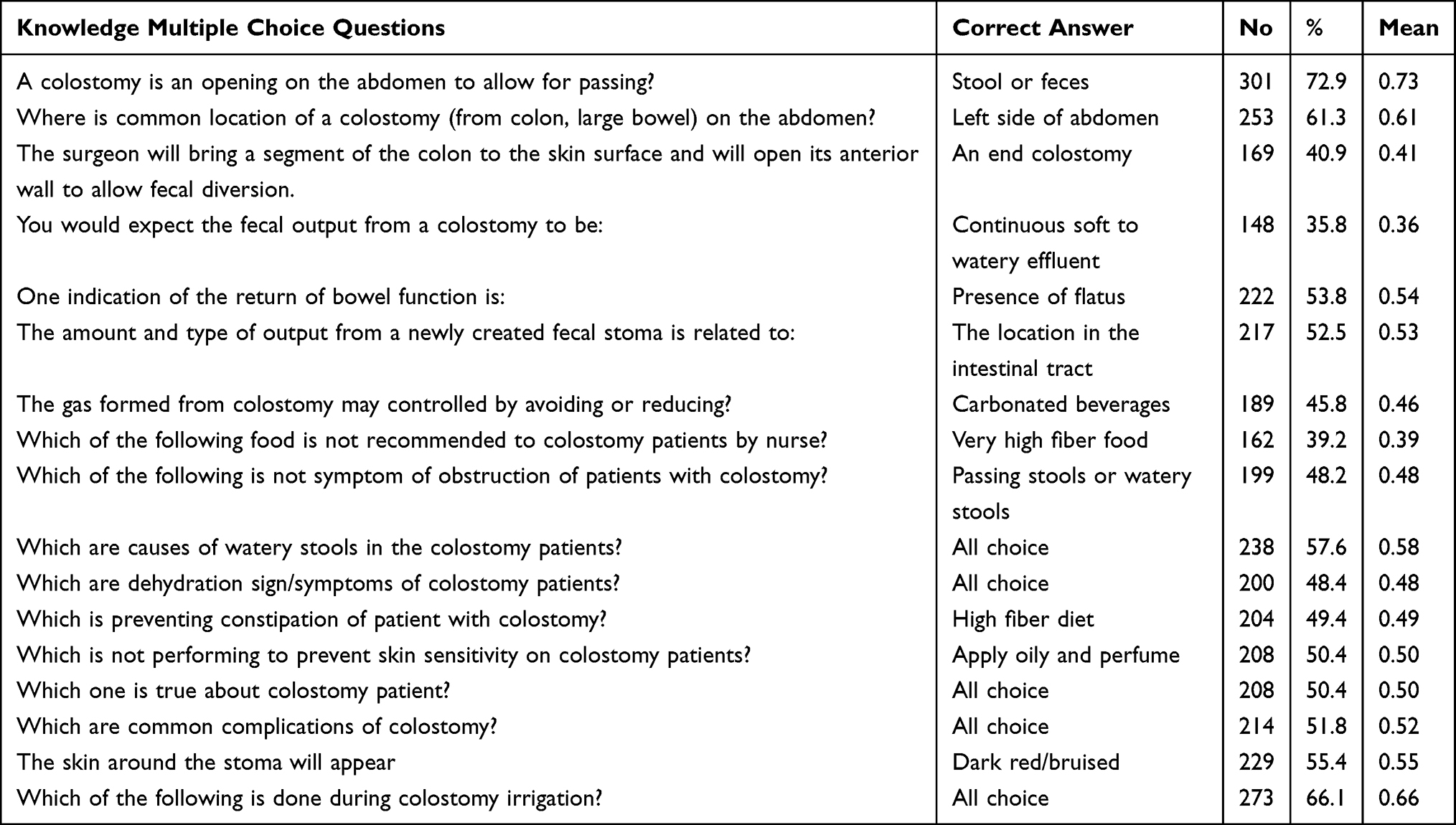 |
Table 6 Frequency and Percentage Distribution of Knowledge (Multiple Choice) Questions About Colostomy Care at Amhara Region General and Referral Hospitals (n=413), 2020 |
The mean score for knowledge was 0.53 with a standard deviation of 0.112. Study participants who scored more than and equal to the mean value were regarded as having adequate knowledge, whereas participants who scored less than the mean value were regarded as having inadequate knowledge. Among 413 participants, 40.4% (95% CI: 35.4–45.8) had adequate knowledge and 59.6% had inadequate knowledge about colostomy care.
Factors Related with Knowledge of Nurses Regarding to Colostomy Care
In binary logistic regression analysis, age, marital status, educational status, total clinical experience, surgical unit experience, presence of colostomy care guidelines, care for patients with colostomy within six months, receiving colostomy care training within the last six to eight months, ever attending a colostomy care training/meeting, and read professional literature regularly had an association with adequate knowledge of colostomy care. In the multivariable analysis, only five variables were identified as significantly associated factors of adequate knowledge.
In this study, the odds of adequate knowledge on colostomy care were almost three times higher among nurses who had greater than 96 months clinical experience than among nurses who had less than 24 months clinical experience (AOR: 2.99, 95% CI: 1.54–5.84). The odd of adequate knowledge on colostomy care were 2.3 times higher among nurses with guidelines for colostomy care than among nurses without guidelines for colostomy care (AOR: 2.25, 95% CI: 1.45–3.49). Similarly nurses who gave care for more than ten patients within six months were 2.2 times more likely to have adequate knowledge about colostomy care than nurses who gave care for fewer than five patients within the last six months (AOR: 2.24, 95% CI: 1.37–3.81). The odds of adequate knowledge on colostomy care were almost two times higher among nurses who had ever had training on colostomy care than among nurses who had not ever had training on colostomy care (AOR: 1.94, 95% CI: 1.10–3.43). Nurses who read professional literature regularly were two times more likely to have adequate knowledge about colostomy care than those who did not read professional literature regularly (AOR: 2.07, 95% CI: 1.33–3.22) (Table 7).
 |
Table 7 Multivariable Logistic Regression Analysis of Factors Associated with Nurses Knowledge of Colostomy Care in Amhara General and Referral Hospitals, Amhara, Ethiopia, 2020 (n=413) |
Attitude of Nurses Towards Colostomy Care
One-third (32%) of participants agreed that providing stoma care would maintain their skills and one-third (32.7%) of respondents agreed that lack of confidence does not avert from stoma care. From the respondents, 18.6% were agreed that there were adequate staff to care for colostomy patients and 10.2% of respondents agreed that there is adequate access to written information to teach their patients. Only 9.4% of respondents agreed that they knew who will answer their colostomy care questions (Table 8).
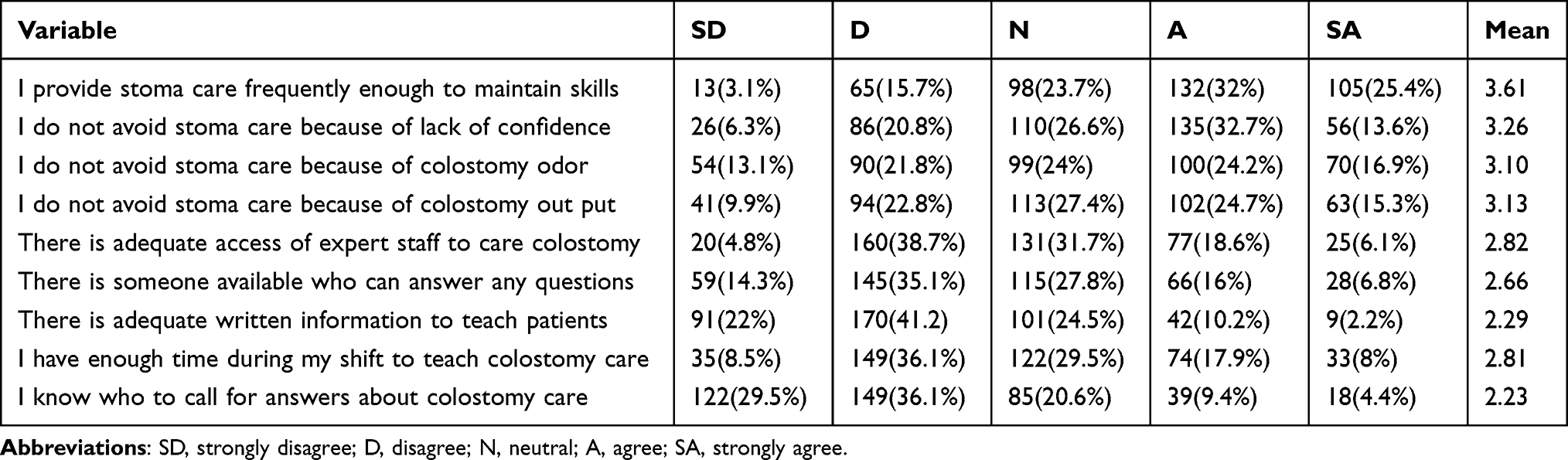 |
Table 8 Attitude of Nurses About Colostomy Care at Amhara Region General & Referral Hospitals, Amhara, Ethiopia, 2020 |
The mean score for attitude was 2.88 with a standard deviation of 0.642. The overall result of this study showed that nearly half (49.6%) (95% CI: 45–54.5) had favorable attitude, whereas 50.4% had unfavorable attitude towards colostomy care.
Factors Related with Attitude of Nurses Regarding to Colostomy Care
In binary logistic regression analysis nurses’ total clinical experience, surgical unit experience, presence of colostomy care guideline, taken colostomy care lesson during study, care of patients with colostomy within six months, ever attend colostomy care training/meeting and knowledge of nurse towards colostomy care had an association with favorable attitude of colostomy care. In the multivariable analysis, only three variables were identified as significantly associated factors of favorable attitude.
In this study, the odds of favorable attitude on colostomy care were almost two times higher among nurses with guidelines for colostomy care than among nurses without guidelines for colostomy care (AOR: 2.13, 95% CI: 1.32–3.43). Similarly the odds of favorable attitude on colostomy care were two times higher among nurses who gave care for five to ten patients within the last six months than among nurses who gave care to fewer than five patients within the last six months (AOR: 2.03, 95% CI: 1.17–5.52). Also the odds of favorable attitude on colostomy care were 9.8 times higher among nurses who had adequate knowledge towards colostomy care than among nurses who had inadequate knowledge toward colostomy care (AOR: 9.76, 95% CI: 5.94–16.03) (Table 9).
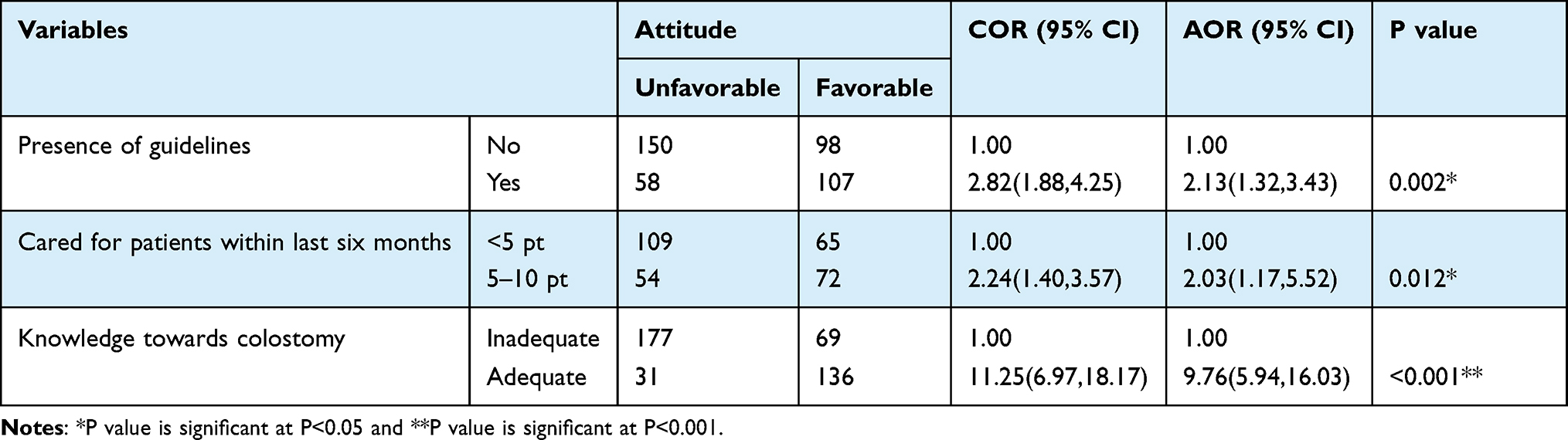 |
Table 9 Factors Associated with Nurses’ Attitude of Colostomy Care in Amhara General and Referral Hospitals, Amhara, Ethiopia, 2020 (n=413) |
Perceived Responsibilities Findings
A total of 15 nurses working in surgical wards in three referral hospitals (Felegehiwot, Debremarkos, and Tibeb Ghione) at Amhara region were invited to take part in the study and 13 of these agreed to participate. The analysis recognized two main themes and four sub-themes under the main themes related to the perceived responsibilities of nurses about colostomy care (Table 10).
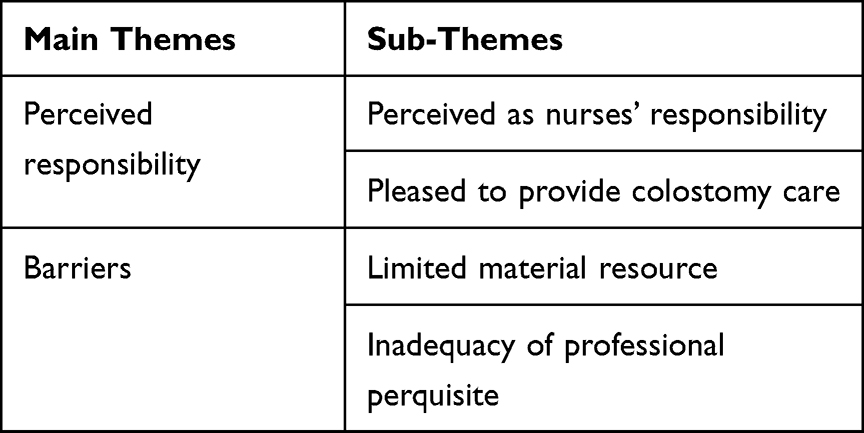 |
Table 10 Main Themes with Corresponding Sub-Themes in the Content Analysis |
Perceived Responsibility
These themes emerged from the nurses’ descriptions of how they perceived their colostomy care responsibilities in working as a nurse in the surgical ward and this is illustrated by the two sub-themes: perceived as nurses’ responsibility and pleased to provide colostomy care.
Nurses stated that they should be primarily responsible for colostomy care. Eight nurses expressed that nurses should be aware of patients’ stress, condition, and progress to give high quality colostomy care:
I believe that responsibility of colostomy care is for nurses, and we are closer to patients than other caregivers to understand their problems and assess frequently and reassure about colostomy … and it creates satisfaction to us … all nurses have a duty to be one of colostomy care giver in the ward … we nurses are frontline of colostomy care …. (nurse 1)
Another participant illustrated that responsibility for colostomy care should be for both nurses and physicians. There are diverse job descriptions between nurse and physician in general and also for colostomy care specifically so all healthcare providers should fulfill their role:
All professionals working in the department are responsible. Because the division of labor is different for each of them, I believe the patient would benefit from it. (nurse 13)
On the other hand, nurses express the roles of nurses, physicians, attendants, and patients themselves in colostomy care; patients and attendants should be active listeners and apply what nurses and physicians had told them to do; nurses do formal nursing colostomy care and physicians also perform diagnosis and treatment options according to a patient’s condition:
I believe that it is better to be given the colostomy care responsibility for all nurses, physicians, patients, and caregivers. I know I am also responsible for colostomy care as one nurse. (nurse 10)
Three nurses expressed that colostomy care responsibility in their hospitals was for both nurses and attendants. As we know colostomy alters patients’ social relation and dissatisfaction with one’s physical appearance and families have negative attitudes towards it:
Colostomy care should be given by a nurse. Although it is usually embarrassing, very uncommon and uncomfortable for patients and caregivers and not well known to the community. For the sake of patient, we have to take responsibility. But, in our working hospital care is often given by attendants, which is incorrect …. (Nurse 9)
But other participants stated
It is nurses’ responsibility and we should perceive that. It is also done by nurses at our hospital …
Whatever their perception all participants had performed colostomy care for 8 to 26 patients in their experience
Yes, I do care for patients with colostomy. Because patients with colostomy have a lot of confusion about it, I feel that we should treat them more closely … (All nurses)
Many of the participants explored the varied role of working in the surgical department as a nurse. For example: psychological reassurance, health education about colostomy, frequently clean and follow conditions:
because patients have confusion and question about colostomy; I feel that we should offer psychological reassurance, health education as well as early intervention …. (nurse10)
Some of the participants illustrate that monitoring their diet. frequent assessment and positioning were day to day performing skills:
cares we give them are monitor their diet; output, sign of infection, positioning and consultation if necessary are some of … (nurse 2)
Barriers
This theme reflects on the challenge and limitations that participants faced when working in the surgical ward. This is described by the two sub-themes: limited material resources and inadequacy of professional perquisite.
All participants described that limitation and inadequacy they encountered in their everyday experience were mainly related to lack of training, lack of guidelines and inadequate supply such as gloves, adhesive plaster, cloth, gauze, colostomy bag, and wiper. One nurse stated:
Many times they only offer work to nurse, but they have forgotten the need of something to improve the quality of care. Like: Lack of professional perquisite, lack of training, absence of personnel protective equipment … (nurse 4)
Participants expressed that resource limitation they encounter was a barrier to provide adequate colostomy care and they felt an inadequacy to fulfill their perceived responsibilities. It is expressed as:
When giving care for patients with colostomy without guideline, training, colostomy bag and wiper, the care was compromised and not as good as we expected (nurse 8).
The equipment and supply are inadequate to give care for patient with colostomy:
we look patients who are heavily contaminated but we cannot help. It is a big challenge for us … (nurse 1).
Discussion
The result of this study showed that only 40.6% (95% CI: 35.4–45.8) of nurses had adequate knowledge about colostomy care. This finding is consistent with a study conducted in Nellore, India in which 46% of the respondents had adequate knowledge.5 Even though, there is a difference in socioeconomic status and level of health sector development, the possible reason of similarity between the current study and the study in India might be using a similar study population (staff nurse), study unit, and study design.
The result of this study is also lower than the study conducted in Addis Ababa, Ethiopia, 51.3%.23 The possible reason for this difference might be due to difference of study setting and data collection tool. In this study only nurses working in surgical wards were included and a tool with 25 knowledge questions was used; whereas in the study done in Addis Ababa the study subject included nurses working in surgical, ICU, and oncology units and used a tool with 17 knowledge questions.
However, the result of this study was higher than the study done in Turkey, 27.5%,6 in India, 13.8%,25 and in Iran, 22.2%.20 The possible justification might be due to differences in study design, differences in study setting, and differences in sample size, different tools used and the differences in result rating; for example, in the Iran study, the knowledge was rated as very high, high, low, and very low. As well, the result rating in India’s study is quite different, it was rated as poor, average, good, and very good. This may differ from the figurative interpretation of this study as adequate and inadequate knowledge.
Having clinical experience greater than 8 years (97 months) in nursing (AOR: 2.99: 95% CI: 1.54– 5.84) was significantly associated with adequate knowledge towards colostomy care. The finding was supported by a study conducted in Ethiopia23 and in Turkey.6 The finding might be justified as when nurses’ experience increases, they become familiar with the subject matter thereby acquire knowledge to carry out the procedure with safety and precision.
The finding of this study showed that having cared for more than ten patients with colostomy (AOR: 2.24, 95% CI: 1.37–3.81) was significantly associated with adequate knowledge towards colostomy care. The finding was supported by a study conducted in Ethiopia23 and in Turkey.6 The finding might be justified as when nurses care for more patients with colostomy, they become familiar with the problem thereby acquire knowledge to solve the problem of patients with colostomy professionally.
Similarly, nurses working in settings having colostomy care guidelines was significantly associated with nurses’ knowledge towards colostomy care (AOR: 2.25, 95% CI: 1.45–3.49). This result is in line with the research conducted in Jordan.18 This can be justified by the fact that the presence of guidelines will advocate the art and science of stoma nursing care.19 Availability of colostomy care guidelines is likely improving nurses’ knowledge and skill and providing continuity of quality care.
Nurses who ever attended colostomy training was significantly associated with nurses’ knowledge towards colostomy care (AOR: 1.94, 95% CI: 1.10–3.43). This finding was supported by a study done in Egypt12 and in Ethiopia.23 This might be justified as the fact that training is vital for acquiring new knowledge and skill for providing safe and precise colostomy care.
Another factor significantly associated with nurses’ knowledge towards colostomy care was reading professional literature regularly (AOR: 2.07, 95% CI: 1.33–3.22). This result was consistent with studies done in Addis Ababa, Ethiopia23 and in Ankara, Turkey.6 This might be because nurses who regularly read literature related to the subject matter can update their knowledge towards colostomy care to provide quality service.
Nearly half (205; 49.6%) with 95% CI (45–54.5) of participants had a favorable attitude towards colostomy care. This result was lower than the study conducted in New Delhi, 64%21 and in India, 66.7%.25 The possible justification might be due to difference in socioeconomic status, level of health sector development, study setting, study design, sample size, and difference in the tool used to rate the outcome.
On the other hand, this study finding was higher than a study done in Southern California, 30%22 of participants had a favorable attitude towards colostomy care. The reason behind this difference might be difference in sample size, difference in study setting and the difference in instrument (tool) used to assess nurses’ attitude about colostomy care.
Working in hospitals having colostomy care guidelines was significantly associated with nurses’ attitude towards colostomy care (AOR: 2.13; 95% CI: 1.32–3.43). This finding was supported by the United Kingdom national stoma care clinical guidelines18 and Jordan colostomy care policies and guidelines.19 This could be justified as the presence of guidelines for colostomy care may improve the knowledge of nurses that would develop optimistic attitude.
Similarly, nurses who had cared for more than five patients with colostomy within the last six months were significantly associated with nurses’ attitude towards colostomy care (AOR: 2.03, 95% CI: 1.17–5.52). This finding was supported by a study conducted in Southern California.22 This might be because as nurses’ experience of caring for patients with colostomy increased, they become familiar with the subject matter thereby improve attitude to carry out the procedure.
In addition, nurses who have adequate knowledge towards colostomy care were significantly associated with nurses’ attitude towards colostomy care (AOR: 9.76, 95% CI: 5.94–16.03). This fact is justified as nurses having adequate knowledge and greater understanding about the subject matter leads to more positive attitude.1,2 Nurses who understand the importance, complications, and impact of colostomy on patients’ physical, social, and emotional wellbeing might have a significant role in changing nurses’ attitude towards colostomy care.
The present findings reveal how 13 Amhara region general and referral hospitals surgical unit nurses perceived their responsibilities regarding colostomy care. Two main themes emerged from the interviews. The first indicates that they generally perceived colostomy care as nurses’ responsibility and were pleased to provide colostomy care. The second themes indicated that there were limited material resources and inadequacy of professional perquisite.
The result indicates that eight nurses perceived that colostomy care is their responsibility. Nurses expressed that they were proud of giving colostomy care to the patients to relieve their stress and maintain the physical and social wellbeing of patients. This finding was in line with the goal of the education of Ethiopian nurses and reflective of the value of the professional code of conduct of role description of nurses in the Federal Ministry of Health of Ethiopia.26 Moreover, the finding indicated that nurses were passionate and proud of their work. This is supported by nurse practice acts guidelines.27 According to the present study only one nurse did not consider colostomy care as a nurse responsibility and the other four nurses reported that the role to care patients with colostomy should be for all nurses and other caregivers such as physicians and attendants.
Many nurses stated that several challenges were present to give colostomy care such as lack of training, inadequate supplies, and lack of professional perquisite. However, these factors were beyond nurses’ control as indicated in this study. This was in line with studies conducted in New York28 and in Spain.29 The finding indicates that quality patient care depends on nurses’ perception towards care, availability of hospital resources, and necessary medical supplies and equipment.
Conclusion
In the present study, nearly half of study participants had adequate knowledge and favorable attitude towards colostomy care. Clinical experience, presence of colostomy care guidelines, care of patient with colostomy, took training/meeting and read professional literature were factors towards colostomy care. The majority of nurses perceived that colostomy care was the responsibility of nurses. In addition, they have a strong commitment to serve and care for patients with colostomy. Therefore, policymakers and the health bureau should emphasize training opportunities for nurses, make available guidelines to carry out colostomy care and consider indisputable nurses’ perquisite. The administrator should arrange training for nurses who were assigned newly at surgical wards. Similarly, nurses should read updated literatures to enhance their knowledge and attitude on colostomy care.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odd ratio; DBRH, Debre Brehan Referral Hospital; DMRH, Debre Markos Referral Hospital; DRH, Dessie Referral Hospital; DTGH, Debre Tabor General Hospital; FHRH, Felege Hiwot Referral Hospital; FMOH, Federal Ministry of Health; GUSH, Gonder University specialist Hospital; IGH, Injibara General Hospital; SPSS, Statistical Package for Social Science; TGRH, Tibeb Gion specialist hospital; WGH, Weldiya general hospital.
Data Sharing Statement
All materials and data are available from the corresponding author without any restriction.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the ethical review committee of health science Debre Markos University with institutional research ethics review committee number of HSC/R/C/Ser/PG/Co/416/17/12. Permission was obtained from selected hospital administrators. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from each participant before their participation including publication of anonymous responses.
Acknowledgments
We would like to acknowledge Debre Markos University, Health Science College; department of nursing for facilitating all the requirements from beginning to the completion of this work. We are also equally indebted to all hospitals for giving permission to conduct this thesis. Finally, we extend our special thanks to all data collectors and respondents.
Author Contributions
TE; conception of the research protocol, literature review, study design, data analysis, interpretation, and drafting of the manuscript. All authors contributed to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hooper J, Gutman N. Colostomy guide. United Ostomy Associat Am. 2017;6:1–24.
2. Recalla SE, Nazarali K, Mayo R, et al. Ostomy care and management: a systematic review. J Wound Ostomy Continence Nurs. 2013;40(5):489–500. doi:10.1097/WON.0b013e3182a219a1
3. Bhattacharya U, Kumar A, Raju A. Permanent colostomy wound: aeromedical disposal. Indian J Aerospace Med. 2019;63(1):39–43. doi:10.25259/IJASM_2019_8
4. Karabulut HK, Dinç L, Karadag A. Effects of planned group interactions on the social adaptation of individuals with an intestinal stoma: a quantitative study. J Clin Nurs. 2014;23(19–20):2800–2813. doi:10.1111/jocn.12541
5. Rama Harika B, Elizebeth J, Betty Lebona IS. A study of assess the knowledge regarding care of ostomies among staff nurses and nursing students in Narayana medical college hospital, Nellore. IJAR. 2016;2(5):1086–1089.
6. Duruk N, Uçar H. Staff nurses’ knowledge and perceived responsibilities for delivering care to patients with intestinal ostomies: a cross-sectional study. J Wound Ostomy Continence Nurs. 2013;40(6):618–622. doi:10.1097/WON.0b013e3182a9a7ed
7. Sinasac PA. Residential aged care workers’ knowledge, attitudes and confidence in providing stoma care. IJNH. 2017;41:14–19.
8. English E. Kenya Australia WCET AASTN twinning project: report of 2015 Kenyan stoma wound and continence nursing education program (SWCNEP). J Stomal Ther Australia. 2016;36(2):18.
9. Porrett T, Frost S, Elcoat DBE C. High impact actions for stoma care. Gastrointestinal Nurs. 2010;8(5):6–7. doi:10.12968/gasn.2010.8.5.48572
10. Massenga ACA, Nuri A, Bugimbi M, et al. Indications for and complications of intestinal stomas in the children and adults at a tertiary care hospital in a resource-limited setting: a Tanzanian experience. BMC Gastroenterol. 2019;19(1):157. doi:10.1186/s12876-019-1070-5
11. Muzira AKN, Kisa P, Langer M, et al. The socioeconomic impact of a pediatric ostomy in Uganda: a pilot study. Pediatr Surg Int. 2018;34(4):457–466. doi:10.1007/s00383-018-4230-8
12. Hashem SF, Abusaad FE-S. Improving nurses’ knowledge and practices regarding the care of children with intestinal stomas; 2016.
13. Ambe PCK, Nitschke NR, Odeh C, et al. Intestinal ostomy: classification, indications, ostomy care and complication management. Dtsch Arztebl Int. 2018;115(11):182. doi:10.3238/arztebl.2018.0182
14. Sheetz KHW, Krell SA, Morris RW, et al. Complication rates of ostomy surgery are high and vary significantly between hospitals. Dis Colon Rectum. 2014;57(5):632. doi:10.1097/DCR.0000000000000038
15. Gao Y. New stoma patients’ experiences during post-operative nursing care; 2012.
16. Yang A-H, Yan M, Qin Y-H. The development status of specialized nursing in ostomy care both in China and abroad. Chin Nurs Res. 2016;3(3):117–120. doi:10.1016/j.cnre.2016.06.014
17. Shaffy SK, Karobi D, Gupta R. Psychosocial experience of the patients with colostomy/ilesotomy: a qualitative study. Indian J Soc Psychiatry. 2014;30(1–2):28–34.
18. UK AoSCN. ASCN stoma care national clinical guidelines; 2016.
19. Subih MM, Teresa M. Ostomy educational program for nurses in Jordan. Wound Clinic Business; 2016.
20. Bagheri M, Sharifan P, Behboudi Far A, Pouresmail Z, Kavousi F. Nurses’ knowledge about fecal intestinal ostomies’s care: a cross-sectional study. Jundishapur J Chronic Dis Care. 2017;6(2):e43345.
21. Andrews GR, Sharma A. Attitude of surgical oncology nurses towards ostomy care. Int J Nurs Educ. 2013;5(2):143–147. doi:10.5958/j.0974-9357.5.2.082
22. Gemmill RK, Ortiz K, Anderson M, et al. What do surgical oncology staff nurses know about colorectal cancer ostomy care? J Contin Educ Nurs. 2011;42(2):81–88. doi:10.3928/00220124-20101101-04
23. Geleta T. Assessment of knowledge and associated factors regarding colostomy care among staff nurses working in surgical, icu and oncology units at selected public hospitals, Addis Ababa, Ethiopia, 2017. Addis Ababa University; 2017.
24. Etikan I. Comparison of convenience sampling and purposive sampling. Am J Theor Appl Stat. 2016;5:1–4. doi:10.11648/j.ajtas.20160501.11
25. Kadam A, Shinde MB. Effectiveness of structured education on caregiver’s knowledge and attitude regarding colostomy care. IJSR. 20
26. Federal Republic of Ethiopia ministry of Health (FMoH), Ethiopian hospital reform implementation guideline. Addis Ababa.; 2017.
27. Russell KA. Nurse practice acts guide and govern nursing practice. J Nurs Regul. 2012;3(3):36–42. doi:10.1016/S2155-8256(15)30197-6
28. Deshpande R. Effectiveness of planned nursing intervention an knowledge and practice of selected aspects of care provided by care giver of children with colostomy admitted in hospitals of Mumbai. IJNH. 2015;1(2):151–556.
29. Nieves CB, Celdrán-Mañas DC, Morales-Asencio M, Hernández-Zambrano JM, Hueso-Montoro SM. Ostomy patients’ perception of the health care received. Rev Lat Am Enfermagem. 2017;11:25.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Gebremichael MA, Lema TB
International Journal of Women's Health 2023, 15:1383-1395
Published Date: 4 September 2023
Assessing Students’ Knowledge and Attitudes Regarding the Risks and Prevention of Consanguineous Marriage: A Cross-Sectional Online Survey
Jairoun AA, Al-Hemyari SS, Shahwan M, Karuniawati H, Zyoud SH, Abu-Gharbieh E, Zyoud SH, Al-Ani M, Habeb M, Jairoun M
Journal of Multidisciplinary Healthcare 2024, 17:1251-1263
Published Date: 20 March 2024