Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Knowledge and Perceptions of Nurse Practitioners on Adverse Events Following Immunization and Barriers to Reporting in the Central Region, Eritrea: A Cross-Sectional Study
Authors Abdu N ![]() , Mosazghi A, Yehdego T, Tesfamariam EH
, Mosazghi A, Yehdego T, Tesfamariam EH ![]() , Russom M
, Russom M ![]()
Received 24 February 2022
Accepted for publication 12 July 2022
Published 25 July 2022 Volume 2022:14 Pages 125—134
DOI https://doi.org/10.2147/DHPS.S363925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender Aparasu
Nuru Abdu,1 Asmerom Mosazghi,1 Tedros Yehdego,2 Eyasu H Tesfamariam,3 Mulugeta Russom4– 6
1Department of Medical Sciences, Pharmacy Unit, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 2Expanded Program on Immunization, Family and Community Health Division, Department of Public Health, Asmara, Eritrea; 3Biostatistics and Epidemiology Unit, Department of Statistics, Mai-Nefhi College of Science, Mai-Nefhi, Eritrea; 4Eritrean Pharmacovigilance Centre, National Medicines and Food Administration, Ministry of Health, Asmara, Eritrea; 5Department of Medical Informatics, Erasmus Medical Centre, Rotterdam, the Netherlands; 6European Program for Pharmacovigilance and Pharmacoepidemiology, University of Bordeaux, Bordeaux, France
Correspondence: Nuru Abdu, Department of Medical Sciences, Pharmacy Unit, Orotta College of Medicine and Health Sciences, Asmara, Eritrea, Tel +291 7-262928, Email [email protected]
Background: Though vaccines are generally considered extremely safe and effective, they have been associated with some serious adverse events following immunization (AEFIs). AEFIs might be related to either the vaccine, immunization error, anxiety related to immunization, and/or coincidental events. If they are not reported and investigated in timely fashion, they can create rumors and confidence gaps. In the last few years, reporting AEFIs in the Central Region of Eritrea, compared to other regions, has been found to be very low, with the root cause for this variation unknown, making intervention strategies challenging. This study was conducted to assess nurse practitioners’ knowledge and perceptions on AEFI surveillance and barriers to reporting in the region.
Methods: An analytical cross-sectional study was conducted among all nurse practitioners who were directly or indirectly involved in immunization services working in all health facilities of the region. Data were collected between October 2019 and February 2020 using an interview-based questionnaire. Percentages and medians (IQR) were used as descriptive statistics, and Mann–Whitney and Kruskal–Wallis tests were used as inferential tools.
Results: A total of 130 respondents with a median age of 40 (IQR 23) years were included in the study. The overall median (IQR) knowledge score of the respondents on AEFI surveillance was 87.50 (19) out of 100. Furthermore, median (IQR) comprehensive perception score was 70 (20) out of 100 (range 40– 95). Shortage of motivation and not knowing how to report were identified as the main barriers to reporting AEFIs.
Conclusion: Knowledge and perceptions of nurse practitioners in the Central Region on AEFI surveillance were generally encouraging. They should however need to be further trained on the basics of AEFI surveillance to bridge the identified barriers to reporting.
Keywords: adverse event following immunization, nurse practitioners, knowledge, perception, barriers, Eritrea
Background
Immunization is one of the most effective and successful public health interventions for protecting individuals and the general public from vaccine-preventable diseases.1 Annually, immunization averts an estimated 2–3 million deaths that from diphtheria, pertussis, tetanus, and measles in all age-groups.2 The diseases targeted by routine immunization are all preventable and among the leading causes of childhood morbidity and mortality. Therefore, immunization needs to be offered at every opportunity with the aim of eliminating these vaccine-preventable diseases.3
Despite the remarkable progress in the prevention of vaccine-preventable deaths, immunization-related safety issues have been a subject of medical debate in the literature and media. Currently, many vaccine-preventable diseases, such as smallpox, polio, and measles, are being eradicated/eliminated and public memory of these deadly diseases is fading. The introduction of several vaccines aimed at tackling other unaddressed public health issues are also of concern to the public. Consequently, alleged vaccine-safety issues have been among the derailing medical debates and jeopardized the uptake of vaccinations, ultimately ending up with disease outbreaks in some countries.3
This behooves public health programs and regulators to establish vaccine-safety surveillance systems to detect, report, investigate, assess, and communicate adverse events following immunization (AEFIs), actual or perceived, at the earliest possible time before creating major concern and/or outrage in the public. As the term indicates, AEFIs are not only vaccine-product or vaccine quality-related, but they also include all events, such as immunization errors, immunization-related anxiety, and coincidental events that follow immunization.2 An AEFI may be any unfavorable or unintended sign, abnormal laboratory finding, symptom, or disease encountered after vaccination.4
The efforts of improving the quality of immunization services should therefore be augmented with establishing a functional vaccine-safety surveillance system which is a pivotal element of vaccine deployment. Taking the aforementioned facts into consideration, the Expanded Program on Immunization (EPI) in collaboration with the Eritrean Pharmacovigilance Centre have been conducting massive sensitization campaigns across the country. The main aim of the campaign is to equip health-care professionals (HCPs) with knowledge and skills on detecting, reporting, investigating, and assessing AEFIs.
Despite the efforts of a massive sensitization campaign, detection and reporting of AEFIs in the Central Region was found to be negligible. For example, during the measles and rubella vaccination campaign in 2018, only about 1% (ten of 916) of the documented AEFIs were from the Central Region. The root cause for this variation was unknown, making intervention strategies challenging. As poor knowledge and perceptions of HCPs on monitoring AEFIs have previously been associated with failures of several immunization programs,5,6 identifying possible factors and/or barriers to reporting is vital in strategizing future interventions. This study was thus conducted to assess knowledge, perceptions, and barriers to reporting of AEFIs in the Central Region.
Methods
Study Design and Setting
This was a cross-sectional analytical study conducted in the Central Region (Zoba Maekel) using a quantitative approach. The study was conducted in all health facilities of the region that provide immunization services. In the region during the study period, there were 34 health facilities in the region (three community hospitals, five health centers, and 26 health stations). The total number of nurse practitioners working in the region was 655. Only 142 were involved in immunization-related services.
Source and Study Population
All nurse practitioners directly or indirectly involved in immunization services working in all health facilities of the region and willing to participate were the source population for this study. Those who had experience of working in immunization services <6 months and other categories of HCP were excluded.
Sample Size and Sampling Technique
A census approach was employed, as the number of nurses working in the immunization services of the region were few in number. As a sampling technique was not practical due to power limitations, this study included all nurse practitioners that were eligible for the study in all health facilities of the region.
Data-Collection Tools and Procedures
A self-designed structured and interview-based questionnaire (Additional file 1) based on similar studies3,7,8 was used to collect data. The questionnaire had four components: respondents’ sociodemographic characteristics, their experiences, knowledge and perceptions, as well as barriers to reporting AEFIs. To ensure face and content validity of the questionnaire, it was subjected to peer review by selected experts in the fields of pharmacy, medicine, and public health. It was then modified based on the comments provided and further pretested (conducted in four health facilities in Anseba Region). The pretesting was aimed at checking the questionnaire’s suitability, comprehensiveness, flow of questions, and skip patterns, as well as familiarization of data collectors, estimation of time for completion, and accuracy of the questions.
Actual data collection was conducted between October 2019 and February 2020. After approval to conduct the study had been obtained from heads of the health facilities, all actively working nurse practitioners in the respective facilities were asked for consent to participate. Once eligibility and willingness had been secured, questionnaires were filled with a face-to-face interview. The interview was chosen to avoid misunderstanding of the questions, filling the questionnaires by discussing with their colleagues, or reading material that could enhance their knowledge and perception. In cases where nurse practitioners were not available during data collection, efforts were made to reach them by all possible means, and those who could not be reached or seemed highly hesitant to take part were considered nonrespondents. To ensure consistency, two pharmacists (NA and AM) were selected and oriented to conduct the interview-based data collection. To avoid information bias, data collectors that had no managing role in the EPI and the Eritrean Pharmacovigilance Centre were selected.
Variable Measurement
Knowledge was measured using 16 items. A score of 1 was given for correct answers and 0 for wrong answers. Then, the assigned scores were added, divided by 16, and multiplied by 100 to get composite knowledge scores. Perception was measured with four items using a 5-point Likert scale ranging from strongly agree to strongly disagree. For descriptive analysis, merging was performed for “strongly agree” and “agree” as one category and, “disagree” and “strongly disagree” as another, leaving “neutral” as the third category. Responses for a negatively worded item were at first reverted to get a composite perception score. Perception scores were computed from the original responses of the participants, with an ideal minimum of 4 and maximum of 20.
Reliability
Scales with fewer items are generally assessed using mean inter-item correlations, rather than Cronbach’s α. These correlations are expected to fall somewhere between 0.15 and 0.50, because values >0.15 indicate that the scale is too broad of a construct, while anything >0.50 would indicate redundancy of items on the scale.9 In this study, the mean inter-item correlations for knowledge (16 items) and perception (four items) were 0.576 and 0.150 respectively, showing acceptable values.
Statistical Analysis
Data were entered and analyzed using CSPro 7.0 and SPSS 26 respectively. All descriptive statistics, means, medians, percentages, and frequencies were computed as appropriate. Normality of the knowledge and perception scores was assessed using the Kolmogorov–Smirnov test. After confirming abnormality, nonparametric Mann–Whitney U or Kruskal–Wallis tests were used to make comparisons of the knowledge and perception scores across the categories of selected independent variables. P<0.05 was considered statistically significant.
Ethics
Approval to conduct the study was obtained from the Ministry of Health research ethics and protocol review committee. Permission was also obtained from the Zonal Medical Officer of the Central region and heads of the respective health facilities prior to data collection. Written informed consent to participate in the study was obtained from all the study participants, all personal information was deidentified, and only aggregated information is reported.
Operational Definitions
Knowledge
Information acquired through experiences and/or education by nurse practitioners’ on AEFI.
Perception
Sensible understanding of nurse practitioners’ on AEFI.
Barriers
Obstacles or challenges to nurse practitioners’ in reporting AEFI.
Results
The total number of HCPs working in the EPI in 34 health facilities of the Central Region was 142. However, the data collectors approached only 130 participants, as the rest were not available in their working areas for different reasons.
Sociodemographic and Background Characteristics
A total of 130 respondents with a median age of 40 (IQR 23) years were included in the study. A majority (88.5%) were female and with a certificate level of nursing education (76.2%). Most had prior training in AEFI (64.6%) and participated (83.1%) in the measles and rubella campaign conducted in 2018. Detailed sociodemographic characteristics of the study population are provided in Table 1.
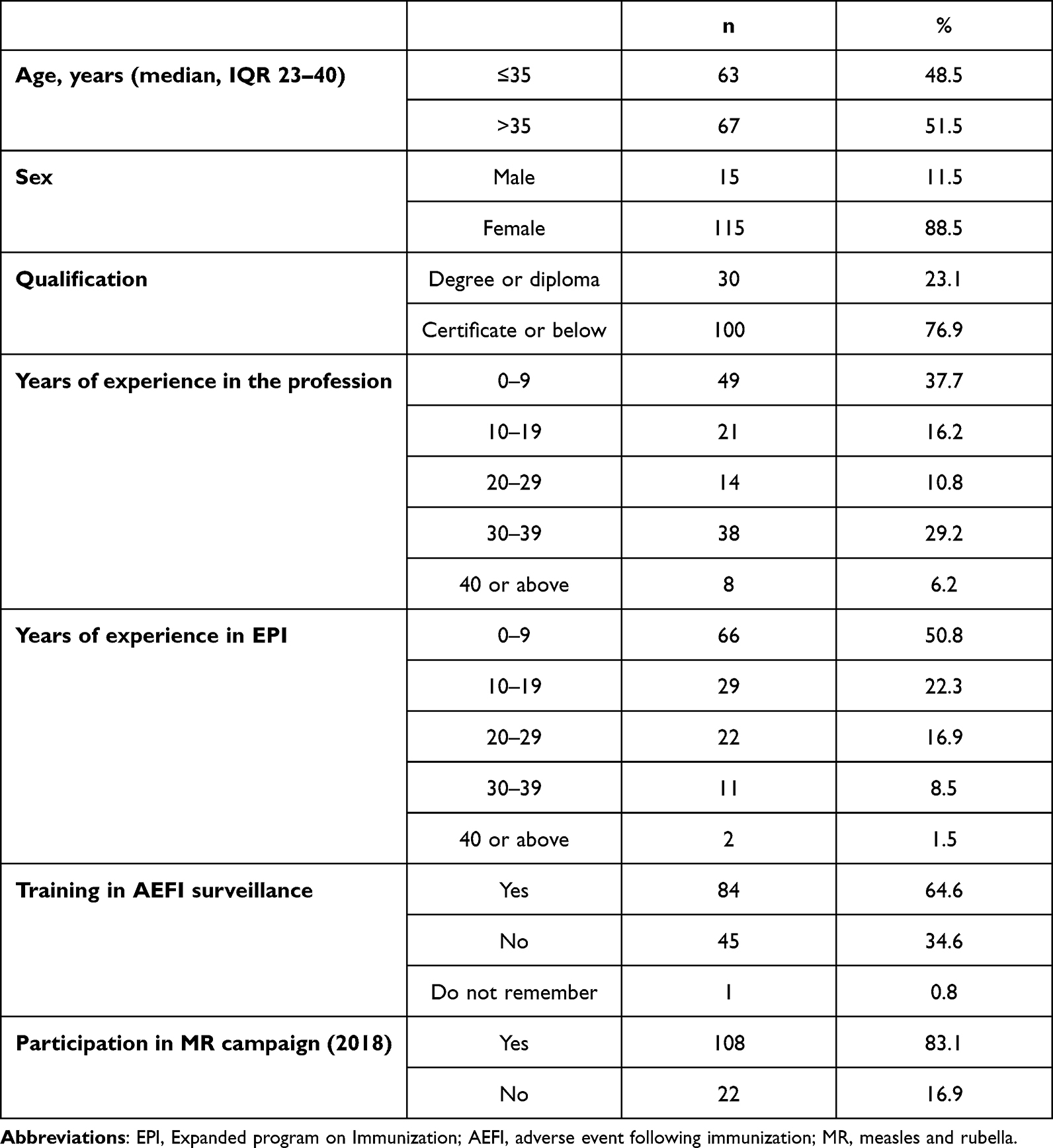 |
Table 1 Sociodemographics and background characteristics (n=130) |
Knowledge of Nurse Practitioners on AEFI Surveillance and Its Associated Factors
A majority of the respondents (78.1%) correctly identified the causes of AEFI. “Immunization error can be a result of inappropriate route of administration” and “Immunization surveillance aims at early detection and response to AEFI” were the highest correctly responded items (each by 97.7% of the nurses). On the other hand, the lowest correctly responded (by only 50% of the nurses) item was “HCPs should report an AEFI when they are not confident about the diagnosis” (Table 2).
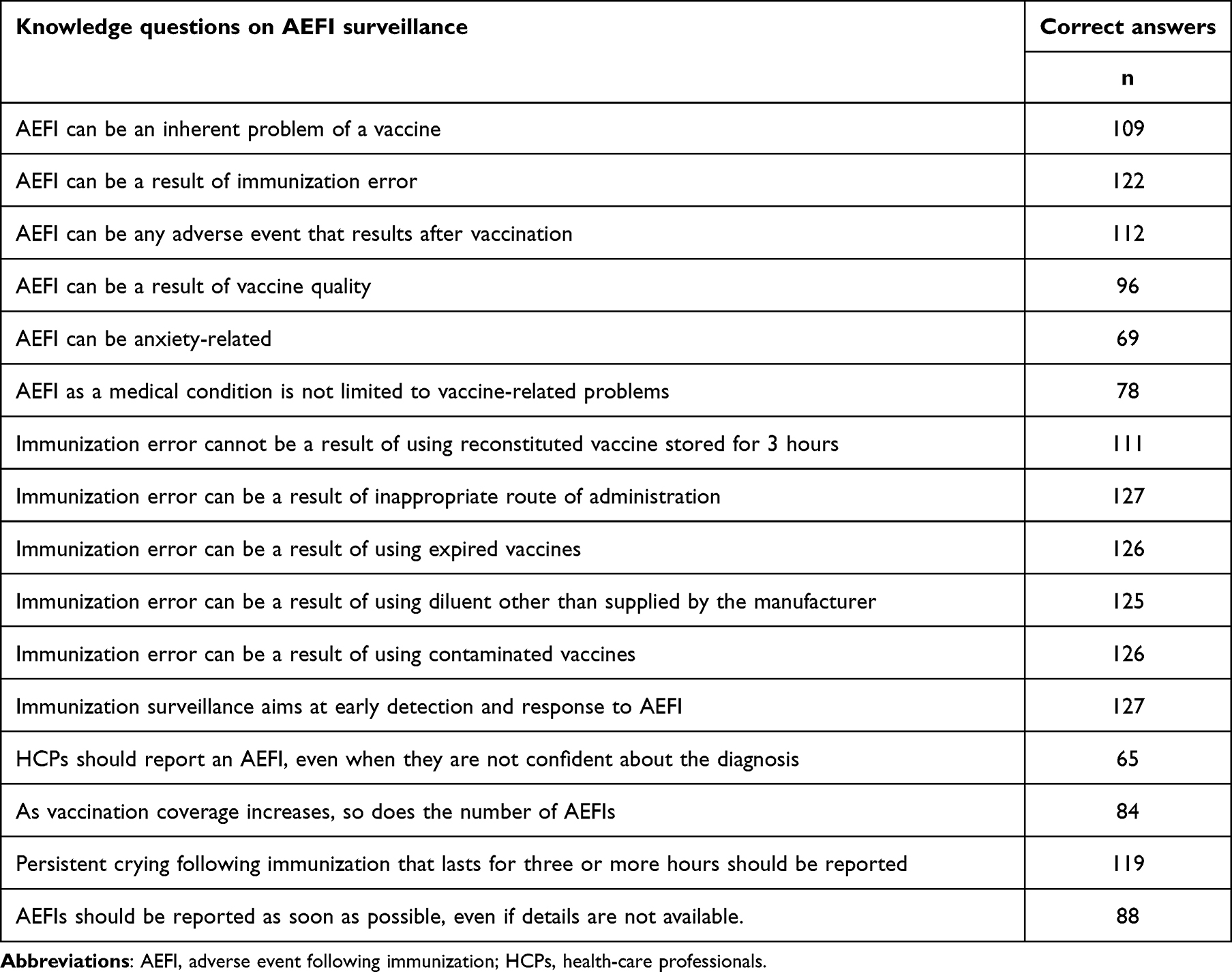 |
Table 2 Proportion of nurses with correct answers on knowledge questions (n=130) |
The overall median (IQR) knowledge score of the respondents on AEFI surveillance was 87.50 (19) out of 100. Mann–Whitney U tests revealed that there was no significant difference in knowledge scores for the categories of age (p=0.622), sex (p=0.191), qualification (p=0.172), and any history of training on AEFI surveillance (p=0.936). Similar insignificant knowledge differences were also observed for the categories of years of overall work experience (p=0.536) and years of work experience in EPI (p=0.349) using the Kruskal–Wallis test (Table 3).
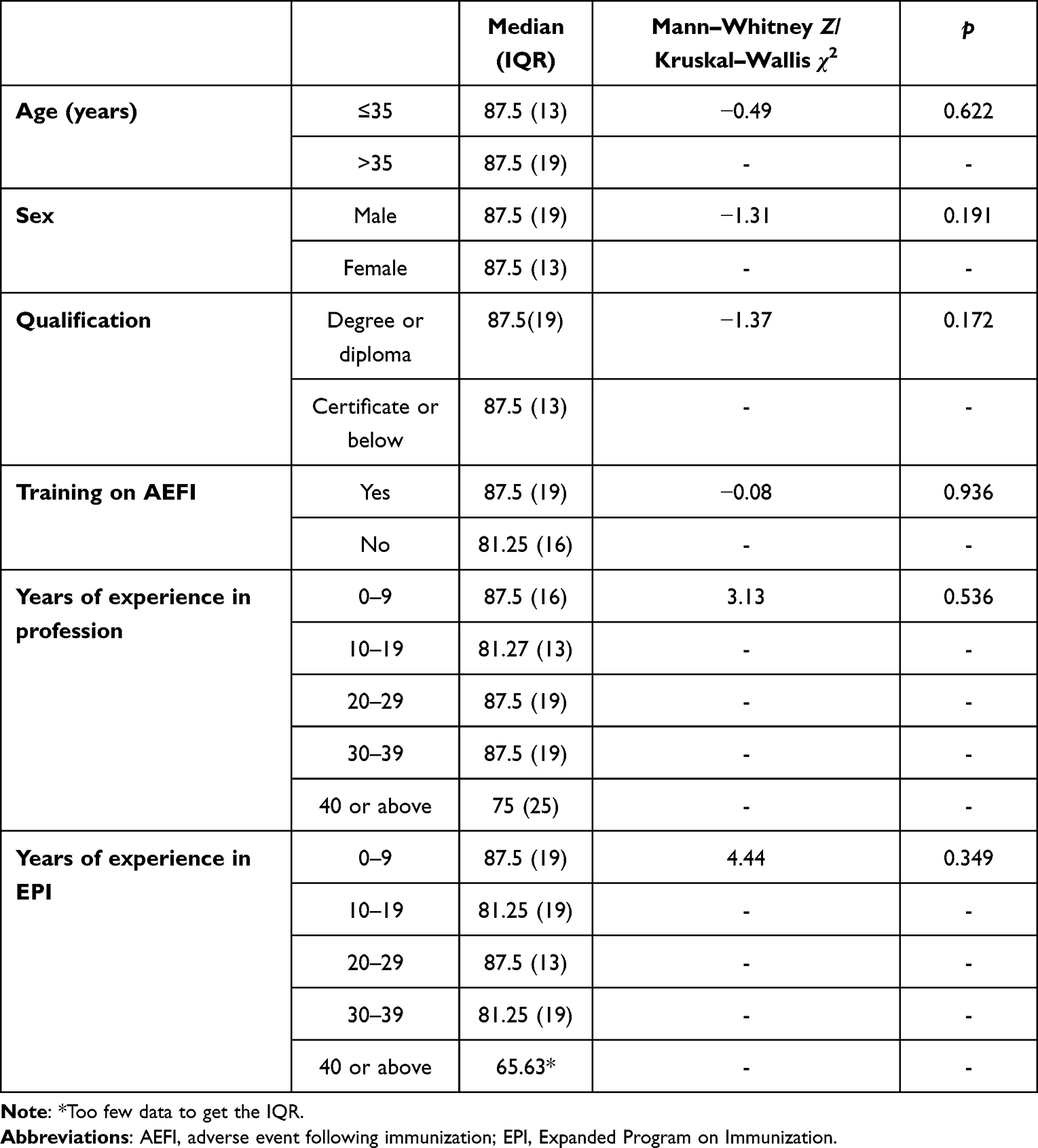 |
Table 3 Comparison of median knowledge scores across the categories of the independent variables |
The respondents showed the highest (98.5%) level of good perception by agreeing to “Enhancing surveillance of AEFI can help build public trust in the immunization program.” On the other hand, less than a quarter (23.8%) of the nurses had good perception on “Public tolerance towards AEFI is higher compared to adverse effects of drugs, as vaccines provide lifelong protection” (Table 4). Median (IQR) comprehensive perception score was 70 (20) out of 100, ranging from a minimum of 40 to a maximum of 95. Comparisons of the median perception scores across the categories of age (p=0.789), sex (p=0.415), qualification (p=0.403), and training on AEFI surveillance (p=0.602) revealed no significant differences. Neither the categories of years of experience in their profession (p=0.172) nor that of years of experience in EPI (p=0.238) had significantly different perception scores (Table 5).
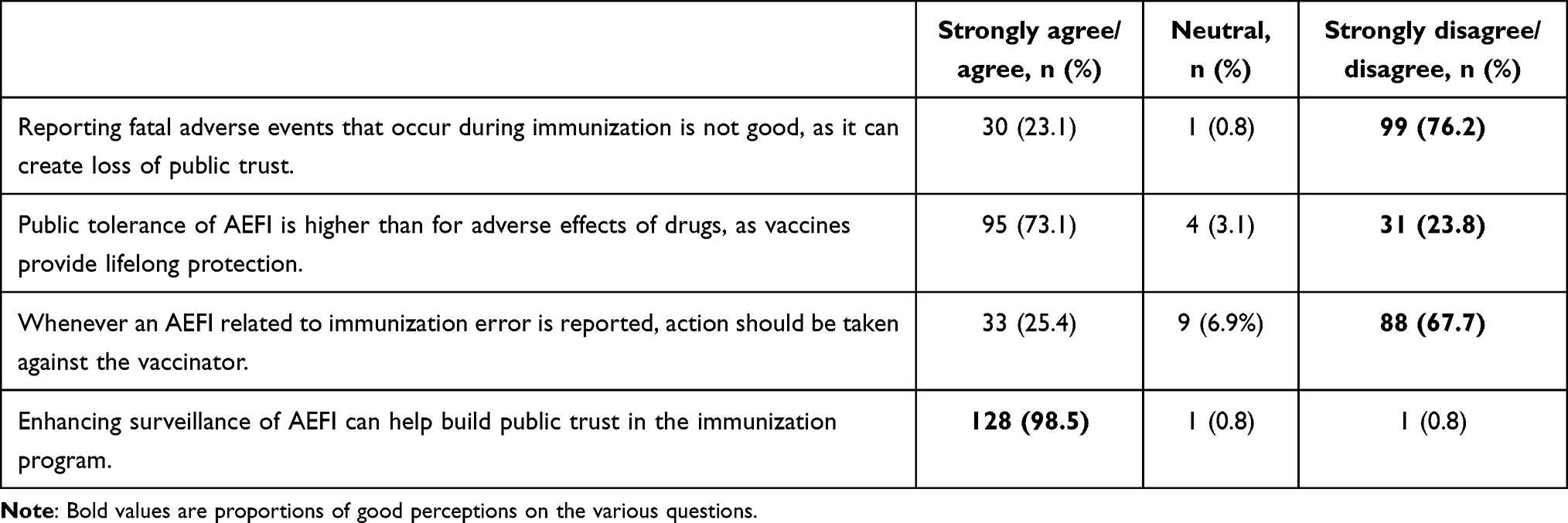 |
Table 4 Distribution of nurses on perceptions of AEFI |
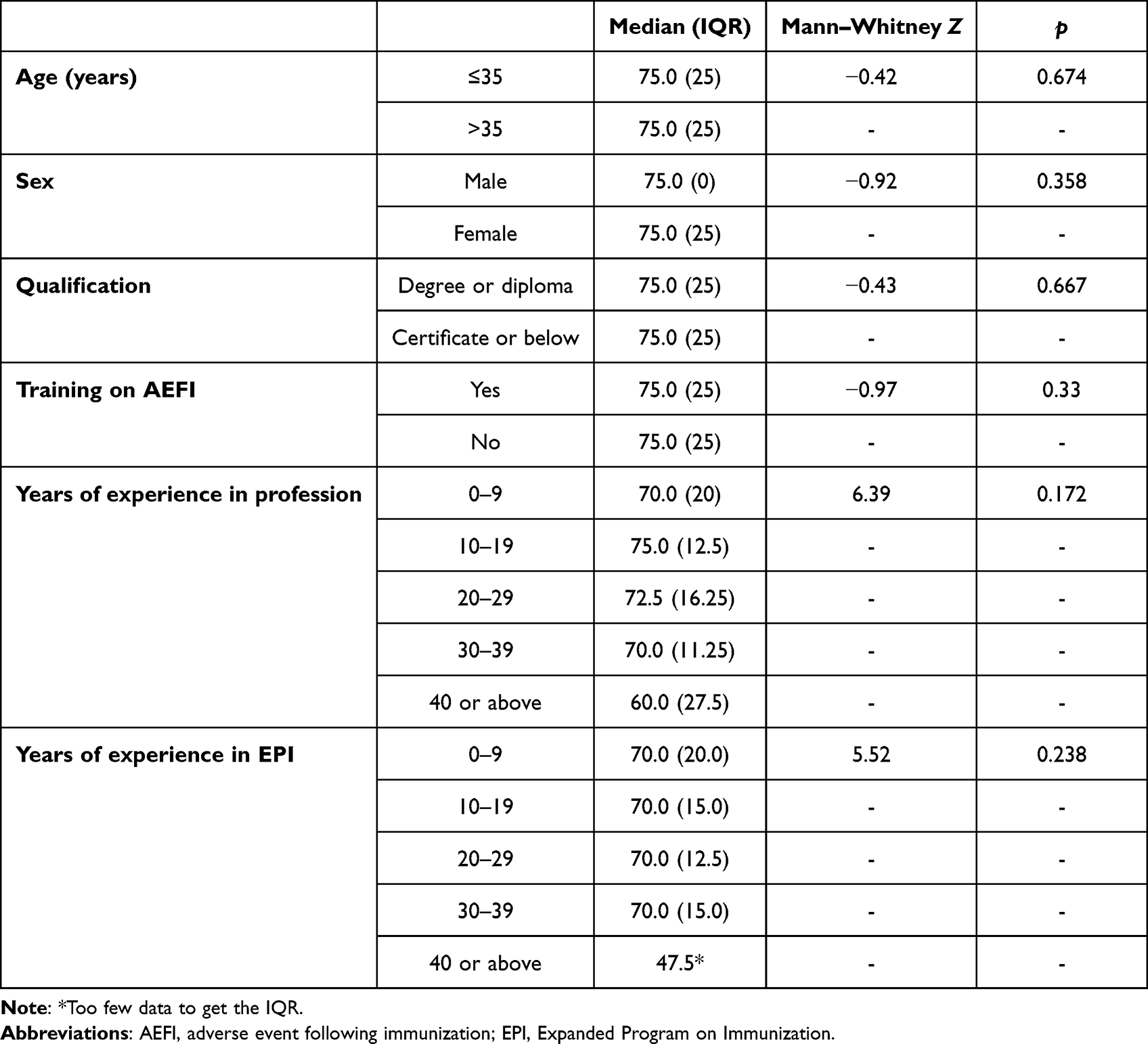 |
Table 5 Comparison of median perception scores among the independent variables |
Reporting AEFIs and Barriers to Reporting
Overall, the respondents claimed that 61.9% of the AEFIs they had encountered were reported to the EPI or the Eritrean Pharmacovigilance Centre. About a third (n=42) reported at least one barrier that hindered them in reporting AEFIs. Encountered AEFIs not being serious, not motivated to report, and not knowing how to report were found to be the main barriers (Figure 1). Of those who required motivation, training (15 of 16), reception of feedback (one of 16), impact of reported cases (one of 16), and payment (one of 16) were reported as possible kinds of motivation.
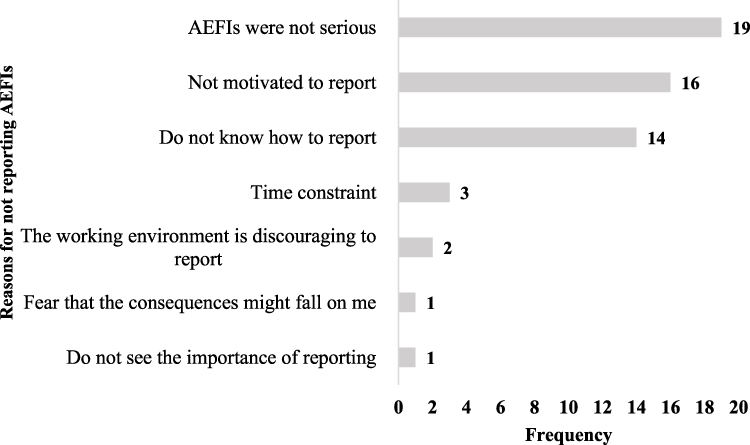 |
Figure 1 Barriers to study participants in reporting AEFIs (n=42). |
Discussion
Monitoring AEFI is of utmost importance for different reasons. It helps to identify immunization errors, serious AEFIs, and clusters of AEFIs, and documents rare but previously unknown AEFIs at the earliest possible time. In this study, the practice of the nurse practitioners’ on reporting AEFIs was satisfactory, as more than half (61.9%) claimed that they had reported AEFIs in the last 6 months prior to the initiation of the study. This is commendable and almost similar to the finding of a study conducted in Nigeria (56.7%),3 and much higher than another similar study conducted in Kenya, as only 2.3% of 274 nurses reported AEFIs they had encountered.7 Shortage of motivation and not knowing how to report were the main barriers identified to reporting AEFIs. To motivate reporters, the Eritrean Pharmacovigilance Centre provides acknowledgment letters for individual reports within 10 working days, as well as certificates and “Pharmacovigilante Awards” to the best reporters on annual basis. In the last few years, several safety signals of high public health importance have been identified by the Eritrean Pharmacovigilance Centre, which can also be another motivation for reporting AEFIs. Training on basics of AEFI surveillance, suggested as a motivation in this study, is the easiest thing the EPI and Pharmacovigilance Centre can offer HCPs. This can also be helpful in solving the second reported barrier. Enhancing the AEFI surveillance system is of utmost importance, as it helps to identify immunization errors, serious AEFIs, and clusters of AEFIs, and documents rare but previously unknown AEFIs at the earliest possible time. Subsequently, when required, they can be investigated and managed to ensure children’s safety and public confidence. Gaining a sound knowledge and perception on the subject matter by HCPs can be crucial for the success of various immunization programs.
In this study, the overall median knowledge score of the respondents on AEFI surveillance was commendable (87.5%). This result was much higher than studies conducted in Ghana (mean 5.9 out of 9.0),8 Albania (mean 21.66 out of 50),10 and Kenya (mean 7.62 out of 14.0).7 The fact that about two-thirds of the respondents had undertaken AEFI training helped them to acquire good knowledge on AEFI surveillance. Acquiring good knowledge of AEFI surveillance is helpful in improving HCPs’ vigilance and capacity in the detection and management of AEFIs, which is vital for enhancing public trust in immunization programs. Median comprehensive good perception scores reported in this study were lower than the study conducted in Kenya (mean 59.12 out of 70).7
The lowest knowledge level reported was for a question asking if HCPs should report an AEFI even when they are not confident about the diagnosis. The lowest perception level was for “Public tolerance toward AEFI is higher than adverse effects of drugs, as vaccines provide lifelong protection.” In upcoming trainings, emphasis should be made to encourage HCPs to report AEFIs, even if they are not confident in the diagnosis and have limited information. HCPs should be aware that vaccine-safety issues are more delicate and sensitive or intolerable compared to adverse drug reactions, as vaccines do not provide immediate benefits and are administered to healthy individuals. The reporting practices were satisfactory, but still require further improvement for all AEFI cases to be reported.
Neither of the selected sociodemographic and background characteristics (age, sex, profession, and training) were significantly associated with knowledge and perception. This result was inconsistent with a study conducted in Kenya, as having training on AEFI and level of education of the nurses were significantly associated with good knowledge and perception.7 Due to the cross-sectional nature of the study design, we could not confirm a cause–effect relationship. Also, this study was based in the Central Region only, and thus the results cannot be generalized to the whole country, and further nationwide study is required to get a complete picture.
Conclusion
The knowledge, perception, and practices of the nurse practitioners on AEFI surveillance in the Central Region were generally encouraging. To further increase reporting of AEFIs, the relevant regional programmers and health-facility managers should think of organizing continued training, including refreshers, on AEFI surveillance with emphasis on the weakest links to ensure all HCPs are well trained and equipped in reporting, managing, and investigating AEFIs.
Abbreviations
AEFI, adverse event following immunization; CSPro, Census and Survey Processing System; EPI, Expanded Program on Immunization.
Data Sharing
The data used in this study are available from the corresponding author and can be accessed upon reasonable request.
Ethics Approval and Consent to Participate
Ethics approval to conduct the study was obtained from the Ministry of Health research ethics and protocol review committee. Permission was also obtained from the Zonal Medical Officer of the Central Region and heads of the respective health facilities prior to data collection. Written informed consent to participate in the study was obtained from all study participants, all personal information was deidentified, and only aggregated information is reported.
Acknowledgments
The authors sincerely thank the study participants for their time and willingness to take part in the study. The authors also greatly acknowledge the support of Dr Tesfai Solomon, zonal medical officer, and all health-facility managers of the Central Region in facilitating the data-collection process.
Author Contributions
MR conceived the idea and EHT and NA analyzed the data. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
There was no source of funding for the study or manuscript preparation.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. World Health Organization. Global manual on surveillance of adverse events following immunization; 2014.
2. World Health Organization. Casualty Assessment of an Adverse Events Following Immunization: Users’ Manual for the Revised WHO Classification. Geneva: World Health Organization; 2013.
3. Lawal A, Mohammed AAA, Bilkisu B, Isa A. Knowledge, perception and reporting attitude of adverse effects following immunization among primary healthcare workers in sabon gari local government area Zaria, Kaduna state, Nigeria. Niger J Basic Clin Sci. 2018;15(1):81–86. doi:10.4103/njbcs.njbcs_18_17
4. Mehta UMJ, Duclos P, Fold P, Folb PI. Developing a national system for dealing with adverse events following immunization. Bull World Health Organ. 2000;78:170–178.
5. Netterlid EM, Håkansson A, Håkansson A. Surveillance of vaccine safety: comparison of parental reports with routine surveillance and a clinical trial. Vaccine. 2009;27:2042–2047. doi:10.1016/j.vaccine.2009.01.131
6. Gahunia J, Bigham M, Konrad S, Snow ME. Adverse events following immunization: evaluating an enhanced nursing role for PHNs. Can. Nurse. 2013;109:16–20.
7. Masika CWA, Atieli H, Were T. Knowledge, perceptions, and practice of nurses on surveillance of adverse events following childhood immunization in Nairobi, Kenya. BioMed Res Int. 2016;2016:1–10. doi:10.1155/2016/3745298
8. Peter Yamoah VB, Oosthuizen F, Oosthuizen F. Knowledge and perceptions of adverse events following immunization among healthcare professionals in Africa: a case study from Ghana. Vaccines. 2019;7:28. doi:10.3390/vaccines7010028
9. Clark LA, Watson D. Constructing validity: basic issues in objective scale development. Psychol Assess. 1995;7:309–319. doi:10.1037/1040-3590.7.3.309
10. IrsidaMehmeti E, Simaku A, Tomini E, Bino S, Bino S. Knowledge, practice and approaches of health professionals to adverse events following immunization and their reporting in Albania. Heliyon. 2017;3:e00331. doi:10.1016/j.heliyon.2017.e00331
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Centered Communication Among Pharmacy Professionals Working in Hospitals and Drug Retail Outlets in Asmara, Eritrea: Knowledge, Attitude, Self-Efficacy and Barriers
Michael E, Nurahmed A, Mihreteab H, Nurhussien M, Adem M, Goitom A, Mihreteab Siele S, Tesfamariam EH, Abdu N
Integrated Pharmacy Research and Practice 2022, 11:153-164
Published Date: 6 October 2022
Doctors’ and Nurses’ Knowledge and Perceived Barriers Regarding Acute Oxygen Therapy in a Tertiary Care Hospital in Nigeria
Desalu OO, Ojuawo OB, Adeoti AO, Oyedepo OO, Aladesanmi AO, Afolayan OJ, Ibraheem RM, Suleiman ZA, Opeyemi CM
Advances in Medical Education and Practice 2022, 13:1535-1545
Published Date: 19 December 2022
Knowledge, Attitudes, and Perceptions of Tuberculosis in Indonesia: A Multi-Center Cross-Sectional Study

Kaaffah S, Kusuma IY, Renaldi FS, Lestari YE, Pratiwi ADE, Bahar MA
Infection and Drug Resistance 2023, 16:1787-1800
Published Date: 28 March 2023
Knowledge, Perception, and Readiness of Indonesian Pharmacists for the Implementation of Telepharmacy-Based Pharmaceutical Services in Indonesia
Wathoni N, Lestari K, Iftinan GN, Rahayu SA, Nurlatifah A, Khairinisa MA, Elamin KM
Integrated Pharmacy Research and Practice 2023, 12:213-225
Published Date: 22 November 2023
Assessing Students’ Knowledge and Attitudes Regarding the Risks and Prevention of Consanguineous Marriage: A Cross-Sectional Online Survey
Jairoun AA, Al-Hemyari SS, Shahwan M, Karuniawati H, Zyoud SH, Abu-Gharbieh E, Zyoud SH, Al-Ani M, Habeb M, Jairoun M
Journal of Multidisciplinary Healthcare 2024, 17:1251-1263
Published Date: 20 March 2024