Back to Journals » Journal of Pain Research » Volume 15
Non-Surgical and Rehabilitative Interventions in Patients with Frozen Shoulder: Umbrella Review of Systematic Reviews
Authors de Sire A, Agostini F ![]() , Bernetti A, Mangone M, Ruggiero M
, Bernetti A, Mangone M, Ruggiero M ![]() , Dinatale S, Chiappetta A, Paoloni M, Ammendolia A, Paolucci T
, Dinatale S, Chiappetta A, Paoloni M, Ammendolia A, Paolucci T
Received 20 April 2022
Accepted for publication 5 August 2022
Published 19 August 2022 Volume 2022:15 Pages 2449—2464
DOI https://doi.org/10.2147/JPR.S371513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Alessandro de Sire,1 Francesco Agostini,2 Andrea Bernetti,2 Massimiliano Mangone,2 Marco Ruggiero,2 Stefano Dinatale,2 Alessandro Chiappetta,2 Marco Paoloni,2 Antonio Ammendolia,1 Teresa Paolucci3
1Department of Medical and Surgical Sciences, University of Catanzaro “Magna Graecia”, Catanzaro, Italy; 2Department of Anatomical and Histological Sciences, Legal Medicine and Orthopedics, Sapienza University, Rome, Italy; 3Department of Medical, Oral and Biotechnological Sciences, G. D’Annunzio University of Chieti-Pescara, Chieti, Italy
Correspondence: Francesco Agostini, Department of Anatomical and Histological Sciences, Legal Medicine and Orthopedics, Sapienza University, Rome, Italy, Email [email protected]
Background: Frozen shoulder (FS) is a painful condition characterized by progressive loss of shoulder function with passive and active range of motion reduction. To date, there is still no consensus regarding its rehabilitative treatment for pain management.
Purpose: The aim of this umbrella review of systematic reviews was to analyze the literature, investigating the effects of non-surgical and rehabilitative interventions in patients suffering from FS.
Patients and Methods: A review of the scientific literature was carried out from 2010 until April 2020 using the following search databases: PubMed, Medline, PEDro, Scopus and Cochrane Library of Systematic Reviews. A combination of terms was used for the search: frozen shoulder OR adhesive capsulitis AND systematic review OR meta-analysis AND rehabilitation NOT surgery NOT surgical intervention. We included systematic reviews that specifically dealt with adults with FS, treated with non-surgical approaches. All the systematic reviews and meta-analyses included in the study that met the inclusion criteria were assessed using the Assessment of Multiple Systematic Reviews as a quality assessment tool.
Results: Out of 49 studies, only 14 systematic reviews respected the eligibility criteria and were included in this study. Their results showed an important heterogeneity of the studies and all of them agree on the lack of high-quality scientific work to prove unequivocally which rehabilitative treatment is better than the other. Due to this lack of gold standard criteria, there may be also a heterogeneity in the diagnosis of the reviews analyzed.
Conclusion: Non-surgical and rehabilitative interventions are undoubtedly effective in treating FS, but there is no evidence that one approach is more effective than the other regarding the methods reported. Future high-quality RCTs are needed to standardize the treatment modalities of each physiotherapy intervention to provide strong recommendations in favor.
Keywords: adhesive capsulitis, frozen shoulder, pain control, pain management, rehabilitation, non-surgical interventions
Introduction
Frozen shoulder (FS), also known as adhesive capsulitis, is a painful condition characterized by progressive loss of shoulder mobility. The American Shoulder and Elbow Society produced a consensus regarding FS, in which it is defined as a condition characterized by progressive functional restriction of shoulder movement with active and passive range of motion (ROM) reduction and without significant radiographic alterations of the glenohumeral joint.1–3 The prevalence of primary FS is estimated to range between 2% and 5% in the general population4 and between 10% and 38% in patients with diabetes mellitus (with no difference between type 1 diabetes mellitus-DM or type 2 DM) and thyroid diseases which can be considered the main risk factors for secondary FS.5,6 The incidence of FS is higher in patients aged between 40 and 65 years and affects predominantly women and the non-dominant shoulder.7–9
To date, the pathogenetic mechanisms are still uncertain, but it is accepted that FS is a consequence of inflammation of the synovium that precedes capsular fibrosis just as pain precedes mobility limitations.10,11
Patients usually report pain, initially in extreme degrees of ROM, for at least a month and later onset of joint limitation that is predominant in flexion, abduction (at average and extreme degrees) and external rotation (specially between 45 and 90 degrees of abduction) and interferes with activities of daily life.1–10
Articular shoulder pain might be provoked by sensitization of structures containing Aδ, Aβ, and C-fibers, proved to be also present in the joint tissue, in the earliest phases.12 However, with persistent pain and chronic inflammation, pain is associated with hyperexcitability of spinal nociceptive neurons, provoking central sensitization and increasing neurotransmitters release in the joint.13 Indeed, chronic shoulder pain in literature is associated with detrimental consequences in terms of impact on health, work capability and quality of life, and even causing temporal gyrus brain modification and orbitofrontal cortex.14
There are no absolute diagnostic criteria defining the exact degree of joint restriction for the diagnosis of FS, but according to the guidelines of the American Physical Therapy Association, a loss of ROM greater than 25% in two planes of motion and loss of passive external rotation greater than 50% compared to the uninvolved shoulder or an external rotation of less than 30° would be characteristic of FS.4,15 Additionally, the commonly referenced clinical findings include painful stiff shoulder for at least 4 weeks; severe shoulder pain that interferes with activities of daily living or work; night pain; painful restriction of both passive and active shoulder ROM (elevation <100, external rotation >50% restriction); normal radiological appearance.8
FS often progresses in three different stages: 1) the freezing (with pain), 2) frozen (adhesive) and 3) thawing phases. In the first stage (2–9 months), there is a gradual onset of severe and diffuse shoulder pain (typically worsens at night). During the second (4–12 months) stage, the pain will begin to subside with a characteristic progressive loss of shoulder ROM. During the third stage (about 5–26 months), the patient experiences a gradual return of ROM.16
A sensitive clinical test for FS appears to be the Shoulder Shrug Sign, which evaluates the patient’s ability to abduct in the frontal plane up to 90°, without compensation. It has a sensitivity of 95% and a specificity of 50%.17,18 Another study proposes a pathognomonic provocative palpation test for FS, the Coracoid Pain Test. It is performed by exerting digital pressure at the level of the acromioclavicular joint, on the anterolateral subacromial area and on the coracoid process; the test is positive when the score was 3 points or higher on pressure in the coracoid area compared with the other two areas according to the Visual analogue scale (VAS).19
The pressure is exerted during the test on the rotator cuff interval which is one of the areas most affected by the pathogenic process. Compared to the control group (healthy people), the test showed a sensitivity of 99% and a specificity of 98%; instead, compared to other shoulder diseases, it has a sensitivity of 96% and a specificity of 87%. However, the study has various limitations such as analyzing only one group, not blinded, of patients and also no reliability index is reported.19
For the evaluation of FS there are various shoulder-specific outcome measures, such as the Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH), Shoulder Pain and Disability Index (SPADI), Constant-Murley Shoulder Score (CSS), Simple Shoulder Test (SST), Penn Shoulder Score, American Shoulder and Elbow Surgeon score (ASES) and the Shoulder Rating Questionnaire (SRQ).8
Several therapeutic approaches to mitigating pain and restore shoulder ROM in FS have been proposed. Drug treatment is based on the oral administration of steroids or NSAIDs and on the use of intra-articular or subacromial infiltrations of corticosteroids, collagenase, hyaluronic acid or physiological solution.20–22
Administration of corticosteroids, whether oral or infiltrative, yields rapid benefits on pain and joint recovery in the short term, mainly in the early stages,4 although there is no evidence of long-term efficacy.7 The infiltrations of hyaluronic acid seem to reduce synovial inflammation by acting at the level of cytokines, consequently reducing pain and improving functional activity. In the literature, however, there is conflicting evidence regarding the actual effectiveness of this treatment.23 Hydrodilatation is a technique that involves the injection of physiological solution and anesthetic with or without corticosteroids inside the joint with the aim of decreasing intra-articular pressure by breaking the capsular adhesions and consequent expansion of the joint space. In the literature, there is no consensus on the dosage and volume of the injection or if capsular rupture was related to the better outcome and moreover, although it is often recommended to administer corticosteroids in hydrodilatation, there are no reliable data that confirm the greater effectiveness of this technique compared to simple steroid infiltration.24
Although it is not possible to define a univocal protocol to date, rehabilitation treatments play a pivotal role in the management of FS, and comprise patient education, stretching exercises, joint mobilization, and manual therapy.4,25–27
Physical modalities such as low-level laser therapy (LLLT), magnetotherapy, ultrasound (US) therapy, and transcutaneous electrical nerve stimulation (TENS) are also commonly used.28–30
Manipulation under anesthesia (MUA) is another possible procedure which involves scapular stabilization with subsequent flexion, extension, abduction, adduction, internal and external rotation of the shoulder until reaching the final degrees of movement following anesthesia. Today it is considered a routine procedure, but the evidence supporting the MUA is equivocal. No differences have been reported in the literature at 1, 3, 6 and 12 months between MUA and conventional physiotherapy exercises, and iatrogenic damage including haemarthrosis, SLAP lesions, partial thickness tears of subscapularis, osteochondral defects and labral detachment may also be found following manipulation.31
In the event that there are no satisfactory results with conservative treatment, open capsular release surgery or arthroscopy can be used.7
In light of these considerations, the purpose of this umbrella review of systematic reviews was to investigate the effects of non-surgical and rehabilitative interventions in patients suffering from FS with reference to specific rehabilitation protocols and techniques.
Materials and Methods
Search Strategy
A review of the scientific literature was carried out from 2010 until April 2020 using the following search databases: PubMed, Medline, PEDro, Scopus and Cochrane Library of Systematic Reviews. A combination of terms was used for the search: frozen shoulder OR adhesive capsulitis AND systematic review OR meta-analysis AND rehabilitation NOT surgery NOT surgical intervention.32
The first version of this article was made in 2020, taking into consideration the articles related to the previous 10 years.
Selection Process
After the manual removal of duplicates, two reviewers independently screened all papers for eligibility. In case of disagreement, a consultation of a third reviewer allowed a consensus. Articles were considered eligible if responding to the questions defined by the following PICO model:
A population (P) of men and women over 18 years of age with a diagnosis of FS was selected. The intervention (I) was rehabilitation treatment, including manipulations under anesthesia, Mulligan or Maitland manipulations, passive, active-assisted or active mobilizations, ROM exercise, hydrodilatation, physical modalities, proprioceptive neuromuscular facilitations (PNFs), stretching exercises, acupuncture, both oral and intra-articular corticosteroid, suprascapular nerve block and occupational therapy. Comparison (C) between different rehabilitative approach and with other types of interventions, such as surgical or medical conservative therapy, was taken into account. Studies that included at least one of the following outcomes (O) were considered eligible: pain assessment by scales; ROM measurement by electronic or traditional goniometer; evaluation of shoulder function and related disability using scales such as the Shoulder Pain and Disability Index (SPADI), Constant-Murley Shoulder Score (CSS), American Shoulder and Elbow Surgeons (ASES) or the Simple Shoulder Test (SST); quality of life, assessed with specific validated questionnaires; strength assessment.
All the systematic reviews and meta-analyses of the last 10 years that had FS or frozen shoulder as the main topic were included. We excluded 1) studies with other design; 2) studies written in a language different from English; 3) full-text unavailability; 4) studies not mentioning a physiotherapy treatment; and 5) studies where FS or adhesive capsulitis or was not the main topic.
Data Extraction
Two reviewers independently extracted data from included studies using a customized data extraction on a Microsoft Excel sheet. In case of disagreement, the consensus was achieved through a third reviewer.
The information obtained included 1) date of publication; 2) research period; 3) characteristics of the studies included and participants in the studies; 4) interventions; 5) main outcomes; 6) main results; and 7) limitations.
Quality Assessment
All the systematic reviews and meta-analyses included in the study that met the inclusion criteria were assessed using the Assessment of Multiple Systematic Reviews (AMSTAR) as a quality assessment tool.33 AMSTAR checklist comprehends 11 questions, with a yes/no answer, investigating the overall quality of a systematic review. Evidence was interpreted based on the AMSTAR score of each individual article (see Table 1 for further details).
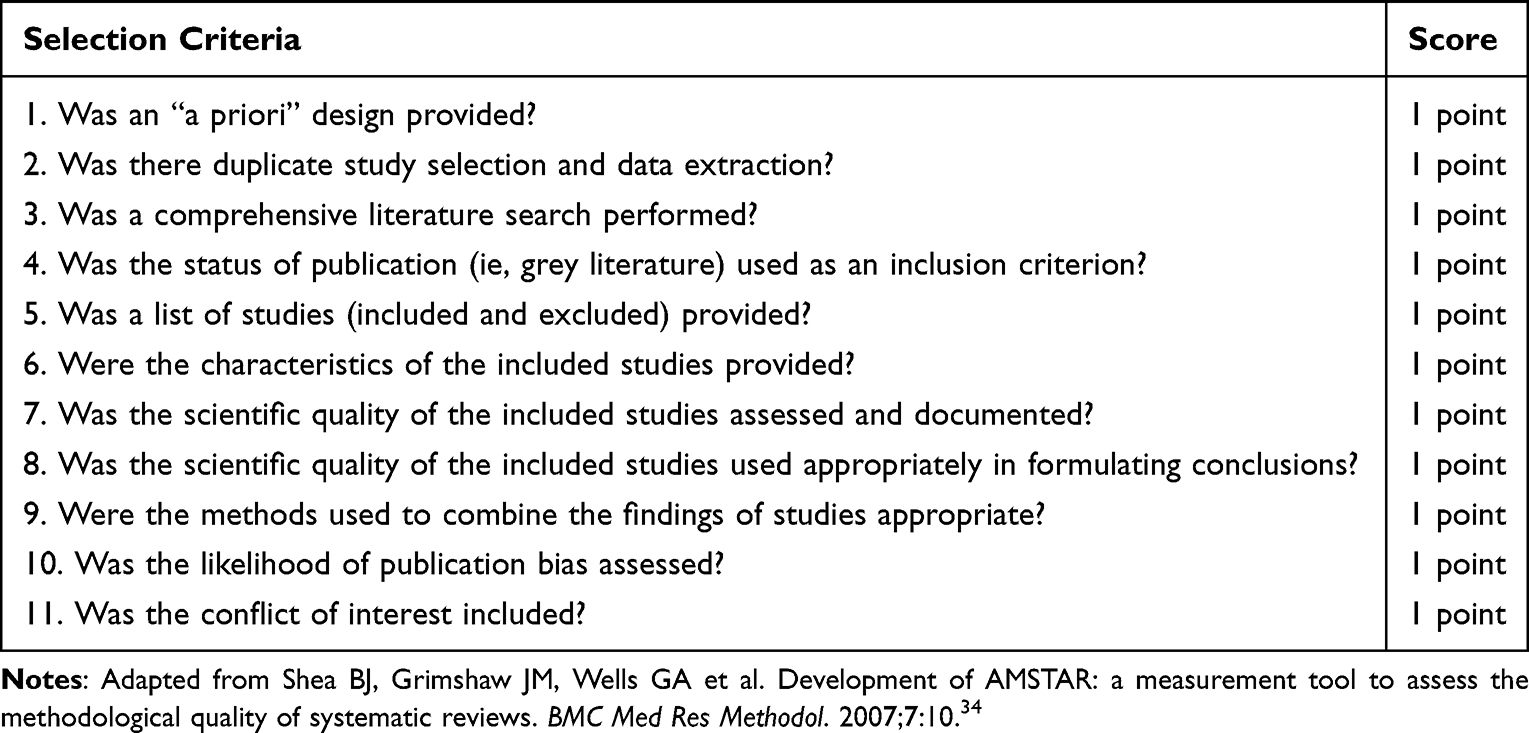 |
Table 1 Assessment of Multiple Systematic Reviews (AMSTAR) Criteria for the Quality Scoring of the Systematic Review Included |
Results
Fourteen systematic reviews were included in this umbrella review, as shown by the PRISMA flow chart in Figure 1. The characteristics of these studies are detailed in Table 2. The included studies29,34–42 have been published between 2010 and 2019. Thirteen studies assessed pain with VAS scale,29,34–37,39–46 11 investigated shoulder ROM,29,34–40,42–45 10 evaluated shoulder function and disability with specific scales (DASH, SPADI, Constant, SST, ASES and SRQ).29,34–36,39,40,42,44–46 AMSTAR score of the included SR ranged from 5/11 to 10/11.
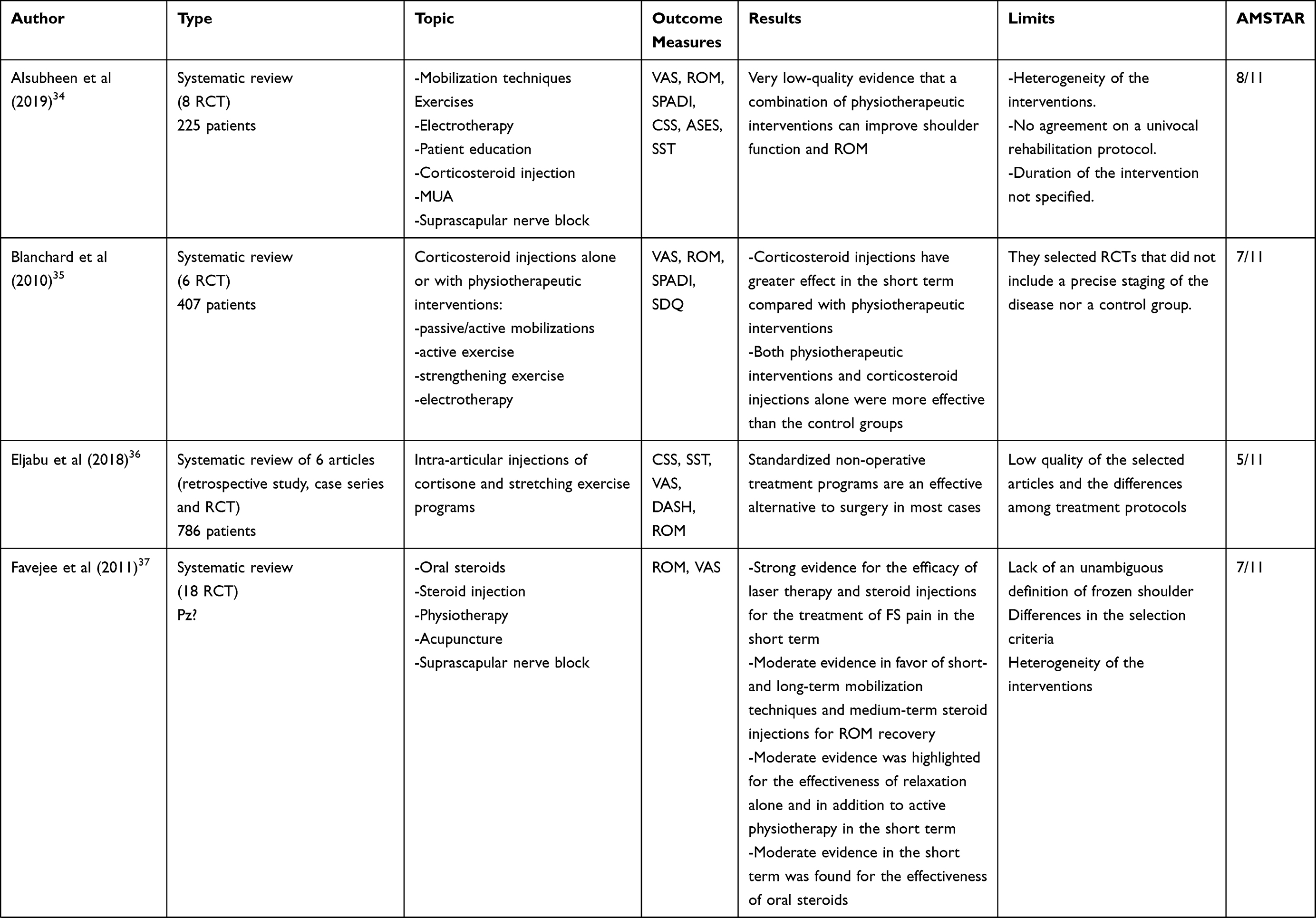 | 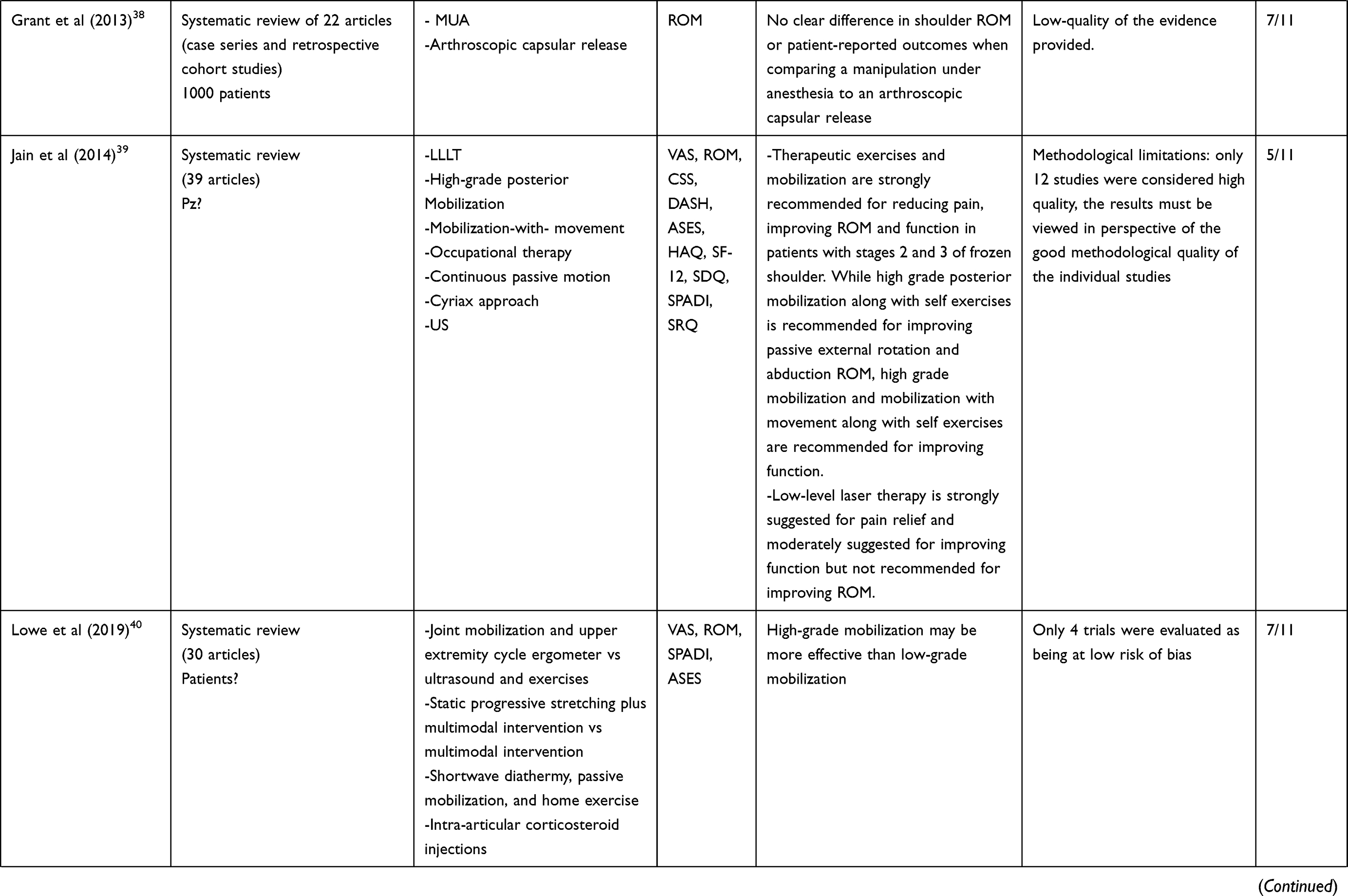 | 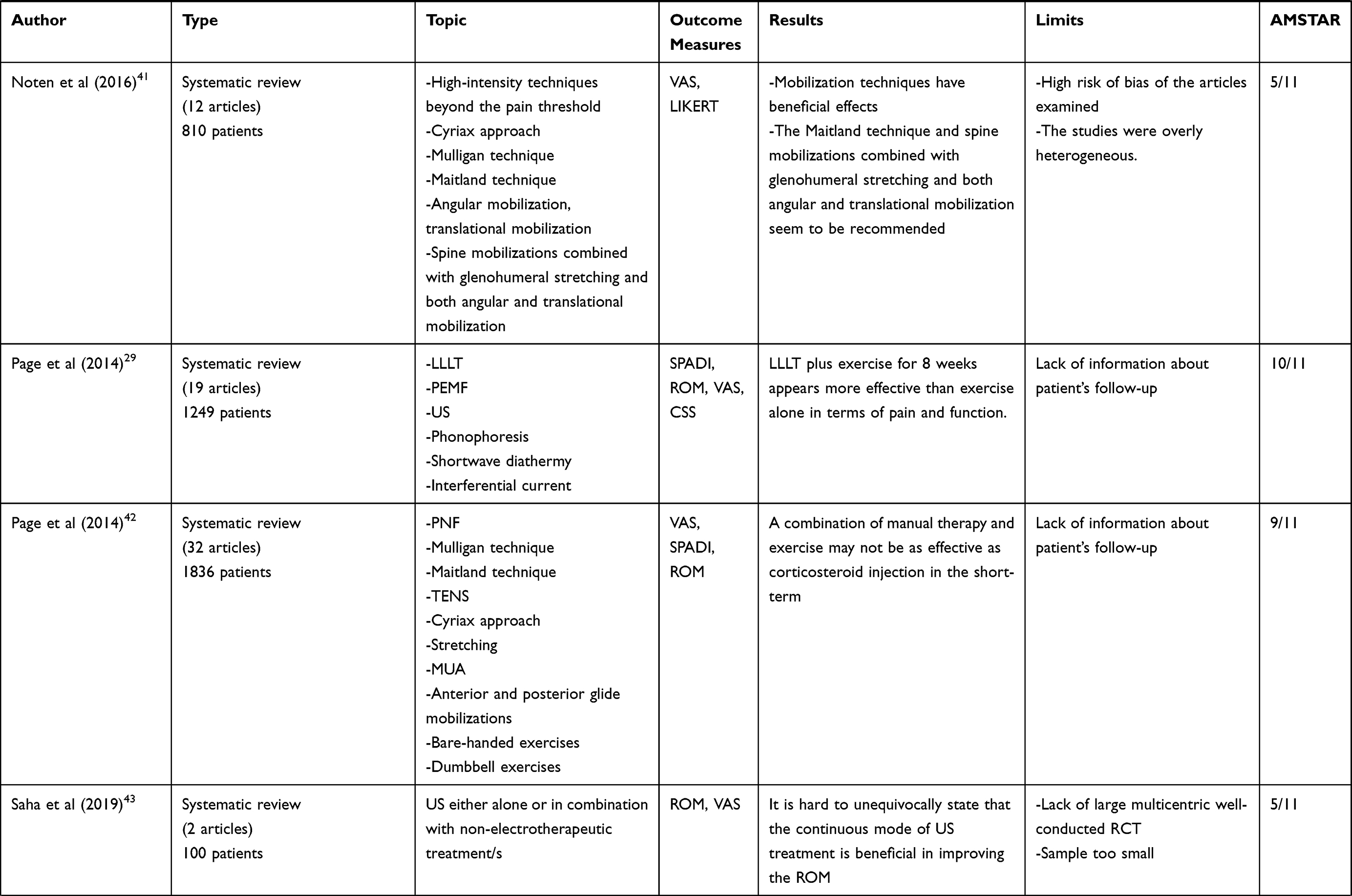 | 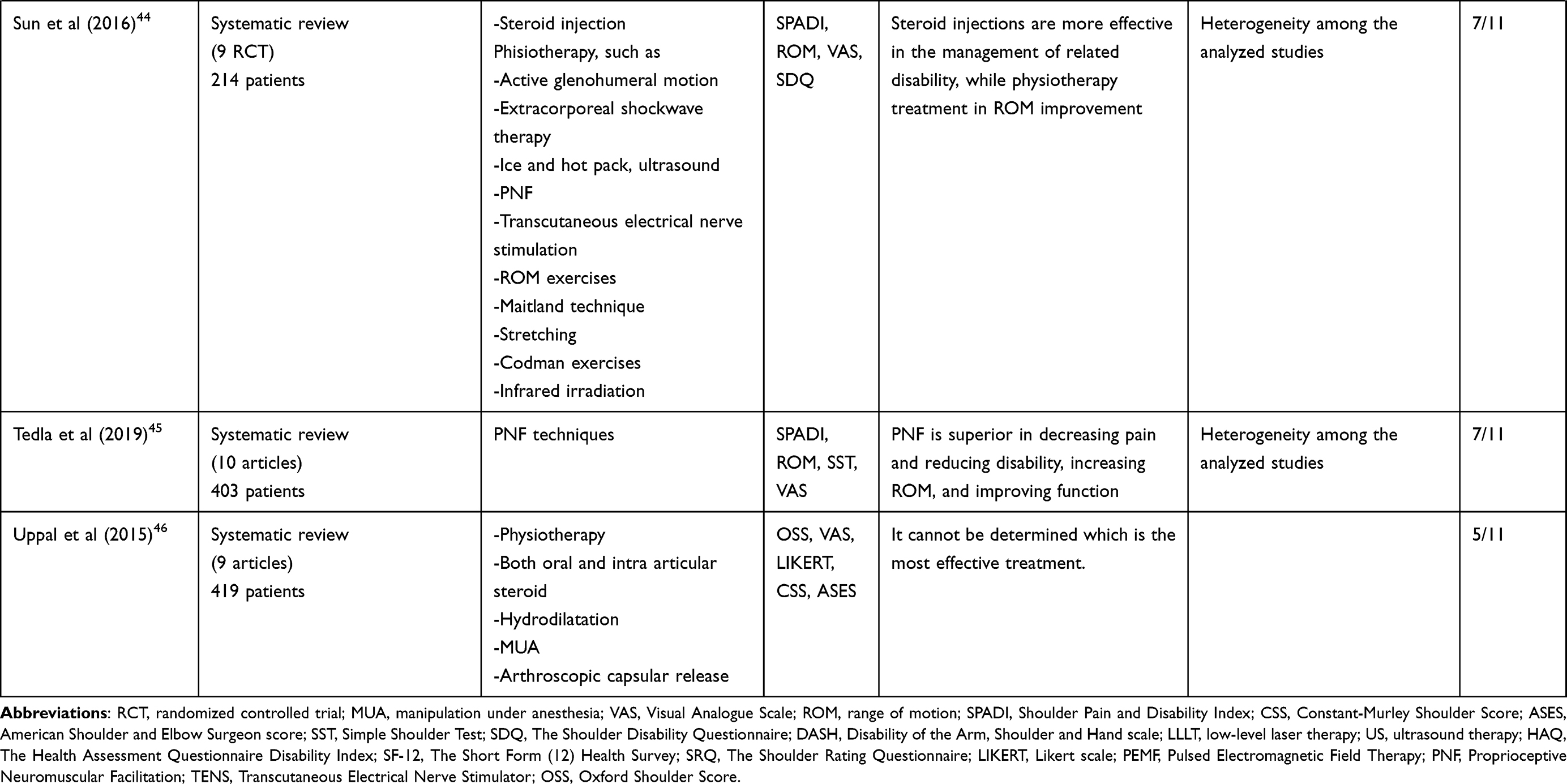 |
Table 2 Main Characteristics of the Included Systematic Reviews |
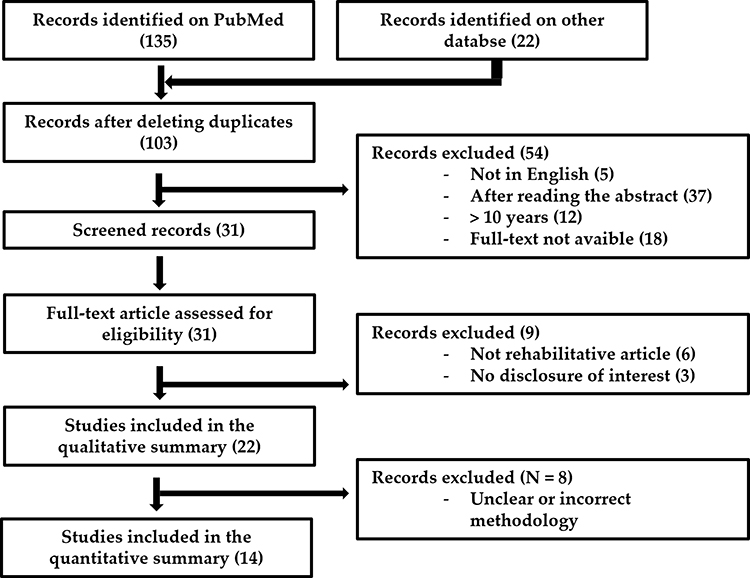 |
Figure 1 PRISMA study flow chart. Notes: PRISMA figure adapted from Page MJ, Moher D, Bossuyt PM et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021 Mar 29;372:n160. Creative Commons.32 |
Alsubheen et al34 published a metanalysis (AMSTAR score of 8/11) of eight randomized controlled trials (RCT), assessed through the GRADE (Grading of Recommendations, Assessment, Development and Evaluations), that included one or a combination of nonsurgical interventions in adult patients with diabetes: physiotherapeutic interventions (including mobilization techniques, exercises, electrotherapy, and patient education), corticosteroid injection, MUA, hydrodilatation, and suprascapular nerve block. Pain, shoulder ROM and function were the outcome measures. This study has some limitations due to the heterogeneity of the interventions and to the very limited literature on the effectiveness of physiotherapeutic interventions, corticosteroids injection, and other nonsurgical interventions for the treatment of FS in patients with diabetes. Moreover, there is no agreement on a univocal rehabilitation protocol or on exercise programs shared between the RCT analyzed, nor information on the duration of the intervention. In detail, joint mobilization plus exercises, continuous passive motion with electrotherapy, and LLLT showed greater effects (better outcomes) on pain, ROM, and function than other physiotherapeutic interventions. In addition, corticosteroids plus exercise were found to reduce pain, improve shoulder function and ROM when compared to NSAIDs plus exercise. A meta-analysis of 3 RCTs with severe heterogeneity revealed a short-term effect of corticosteroids over joint mobilization plus exercises on pain, ROM, and function. Similarly, corticosteroid injection was found to provide small short-term benefits on pain when compared to joint mobilization, with poor evidence. However, joint mobilization plus exercises and LLLT were found to reduce pain and improve function in another systematic review with no formal meta-analysis or effect size calculations.30 Two systematic reviews with high-risk RCTs,31,32 which recommended the use of LLLT and corticosteroids to reduce pain and the use of joint mobilization to improve shoulder ROM and function, agree with the findings of the current review. Lastly, MUA did not show additional benefits over the use of other nonsurgical or surgical interventions. They conclude that there is very low-quality evidence that a combination of physiotherapeutic interventions (exercises, modalities, mobilization), NSAIDs, and/or corticosteroid injections can have negligible to major effects in improving shoulder function or disability, ROM, and pain levels in managing FS in patients with diabetes. In order to determine the best intervention for managing FS in patients with diabetes, future high-quality RCTs are needed.
Blanchard et al35 published a systematic review (AMSTAR score of 7/11) of 6 articles aimed to determine the effectiveness of corticosteroid injections compared with physiotherapeutic interventions for the treatment of FS. The primary outcomes were pain, external rotation, and shoulder disability/function. A limitation to the study design is that it selected RCTs that included neither a precise disease staging nor a control group. However, the study results suggest that corticosteroid injections have a greater short-term effect than physiotherapeutic interventions. This effect decreased over time, with only a small not statistically significant effect in favor of injections in the longer term. This review also showed that both physiotherapeutic interventions and corticosteroid injections alone were more effective than the control groups. Therefore, these findings suggest that both physiotherapists and medical practitioners should consider giving a corticosteroid injection as an initial treatment for this condition but should not overlook more traditional physiotherapeutic interventions.
Eljabu et al,36 in a systematic review (AMSTAR score of 5/11) of seven studies, evaluated different therapeutic options for the treatment of FS. They examined both surgical and non-surgical interventions, and among these oral and intra-articular injections of corticosteroids and stretching exercise program. The flaws of this review are the low quality of the selected articles and the differences among treatment protocols. Nevertheless, the reviewed studies suggest that spontaneous recovery to normal levels of function is possible and standardized non-operative treatment programs are an effective alternative to surgery in most cases. However, patients with high-risk factors such as diabetes mellitus, and those who have chronic symptoms or who are bilaterally affected, would benefit from early arthroscopic capsular release. These studies showed that development of symptoms is directly correlated to anatomical deterioration.
Favejee et al37 carried out an extensive review (AMSTAR score of 7/11) to provide an evidence-based overview regarding the effectiveness of conservative and surgical interventions to treat FS. Among others, 5 Cochrane reviews and 18 RCTs were included, studying the effectiveness of oral medication, injection therapy, physiotherapy, acupuncture, arthrography distension and suprascapular nerve block (SSNB). The first limitation is due to the lack of a unique definition of FS as there are important differences in the selection criteria (the authors used the definition of ROM restriction in all directions). Secondly, there are important differences among the study designs, mainly due to the heterogeneity of the interventions as well as the differences in the outcomes used in the various studies. In two high-quality studies analyzed by the author, there is strong evidence for the efficacy of LLLT and steroid injections for the treatment of FS pain in the short term. Another RCT showed moderate evidence in favor of short- and long-term mobilization techniques and medium-term steroid injections for ROM recovery. In particular, end-range mobilizations, compared to mid-range mobilizations, are more effective as regards the scapulohumeral rhythm. Moreover, moderate evidence was highlighted for the effectiveness of relaxation alone and in addition to active physiotherapy in the short term. Furthermore, moderate evidence in the short term was found for the effectiveness of oral steroids compared with no treatment or placebo and SSNB compared with acupuncture, placebo, or steroid injections. Another high-quality RCT showed that the combination of MUA and exercises is more effective than single exercises in terms of improving ROM after 3 months of follow-up. Most of the studies reported short-term results, whereas symptoms of FS may last up to 4 years. High-quality RCTs studying long-term results are clearly needed in this field.
Grant et al,38 in a systematic review (AMSTAR score of 7/11) including 22 studies, studied differences in the clinical effectiveness of arthroscopic capsular release compared to MUA in patients with recalcitrant idiopathic FS. The outcomes were as follows: shoulder ROM, patient-reported outcomes, and complications. This study has a number of limitations that are primarily related to the quality of the available evidence. In addition to one study that compared MUA to a capsular release performed only when MUA did not result in acceptable ROM, there were no studies that directly compared the outcomes of MUA to an arthroscopic capsular release in idiopathic or secondary-systemic FS patients. There is no clear difference in shoulder ROM or patient-reported outcomes when comparing a MUA to an arthroscopic capsular release for the treatment of recalcitrant idiopathic or secondary-systemic FS. A high-quality study is required to definitively evaluate the relative benefits of these procedures.
Jain et al,39 in their systematic review published (AMSTAR score of 5/11) including 39 studies, evaluated the best available evidence for the use of physical therapy interventions in treatment of FS. Therapeutic exercises and mobilization are strongly recommended for reducing pain, improving ROM and function in patients with stages two and three of FS. This study suffers from predominantly methodological limitations. Since only 12 studies were considered high quality, the results must be viewed in perspective of the good methodological quality of the individual studies. There is limited literature on the effectiveness of specific exercise regimen for the treatment of FS. LLLT is strongly suggested for pain relief and moderately suggested for improving function but not recommended for improving ROM. This article therefore provides a grade A recommendation for the use of LLLT for pain management, grade B for the recovery of shoulder function, while being unable to provide recommendations regarding ROM recovery. Corticosteroid injections can be used for stage 1 FS. Acupuncture with therapeutic exercises is moderately recommended for pain relief, improving ROM and function. Electro-therapy can help in providing short-term pain relief. Continuous passive motion is recommended for short-term pain relief but not for improving ROM or function. Diathermy can be used for pain relief and improving ROM. It is not yet possible to provide recommendations regarding the use of US for pain relief, improving ROM or function.
Lowe et al40 analyzed in a systematic review (AMSTAR score of 7/11), including 30 trials, the clinical effectiveness of non-surgical interventions for people with primary FS. The outcomes were as follows: adverse events, pain, range of shoulder joint motion, self-reported function and disability, strength, quality of life, recovery time to recreation and return to work. A limitation is that only four trials were evaluated as being at low risk of bias with different methods, interventions and outcomes used across the trials. As regards manual therapy, the authors find out that high-grade mobilization may be more effective than low-grade mobilization in a population of patients who have already had physiotherapy and/or steroid injection. The question whether the addition of a daily static stretching program plus multimodal treatment improves range of movement, DASH scores and pain when compared with the multimodal treatment program alone, still requires further investigation and longer-term follow-up. As regards injection therapy, they recommend the use of corticosteroids and a home-based exercise program for people with a duration of FS symptoms less than 6 months.
Noten et al41 compiled a systematic review published (AMSTAR score of 5/11) of 12 RCTs (810 participants), investigating the efficacy of different articular mobilization techniques in patients with primary FS of the shoulder. The outcomes were ROM and pain. The main limitation of this review is the risk of bias; most studies failed to achieve blinding of the patients, therapist and assessor and concealment of allocation items were often not attained. Additionally, the studies were overly heterogeneous. Inclusion criteria varied among several studies (eg, duration and classification of injury, magnitude of loss of ROM). Most of the mobilization techniques included patients in the stiff phase, whereas some studies did not specifically report the phase. Therefore, the timing of the therapy at specific times in the disease’s progress is an important issue for future research. Follow-up, total duration, and frequency of the therapy also varied among studies. In this review, the following seven types of mobilization techniques were evaluated: angular mobilization, translational mobilization, spine mobilizations combined with glenohumeral stretching and both angular and translational mobilization, high-intensity techniques beyond the pain threshold, Cyriax approach, Mulligan technique, and Maitland technique. It turned out that mobilization techniques have beneficial effects in patients with primary FS of the shoulder. Particularly, the Maitland technique and spine mobilizations combined with glenohumeral stretching and both angular and translational mobilization seem to be recommended at the moment.
Page et al,29 in a review (AMSTAR 10/11) of 19 trials (1249 participants), assessed through the GRADE, analyzed the evidence regarding the benefits and harms of electrotherapy modalities, delivered either alone or in combination with other interventions, for the treatment of FS. The most interesting findings were participant-reported pain relief of 30% or greater, overall pain, function, global assessment of treatment success, active shoulder abduction, quality of life, and the number of participants experiencing any adverse event. The weakness of this study is the lack of information about patient’s follow-up. Based upon low-quality evidence from one trial, LLLT for 6 days seems more effective than placebo in terms of global treatment success at 6 days. Based upon moderate quality evidence from another trial, LLLT plus exercise for 8 weeks appears more effective than exercise alone in terms of pain up to 4 weeks and function up to 4 months. It is unclear whether Pulsed electromagnetic field (PEMF) is effective than placebo, or whether other electrotherapy modalities are an effective adjunct to exercise. As for the US, in a study by Page’s review, US, “hot packs” and exercises are compared with US placebos, hot packs and exercises. There were no significant differences in pain, but only an improvement in function at 2 weeks and 3 months and in quality of life at 3 months. Given the low quality of the study, it is not possible to state the effectiveness of US compared to hot packs. With regard to the use of short-wave diathermy, this type of treatment was analyzed in a trial in the Page review, showing an improvement in function at 4 and 8 weeks and an improvement in ROM in particular in external rotation. However, the study is of low quality, hence no recommendations can be given on the use of diathermy in the treatment of FS. There are no studies in the literature that can recommend the use of TENS except in combination with other therapies, but these are poor quality studies. The effectiveness of this therapy in the treatment of FS remains to be fully ascertained. Further high-quality randomized controlled trials are needed to establish the benefits and harms of physical therapy interventions compared to interventions with evidence of benefit (eg, corticosteroid injection or arthrographic joint distension).
Page et al,42 in a subsequent review (AMSTAR 9/11) of 32 trials (1836 participants), assessed through GRADE, summarize available evidence regarding the benefits and harms of manual therapy and exercise, alone or in combination, for the treatment of patients with FS. The main findings were participant-reported pain relief of 30% or greater, overall pain (mean or mean change), function, global assessment of treatment success, active shoulder abduction, quality of life and the number of participants experiencing adverse events. The weakness of this study is the absence of indications about patient’s follow-up. The authors show that a combination of manual therapy and exercise may not be as effective as corticosteroid injection in the short-term. It is unclear whether a combination of manual therapy, exercise and electrotherapy is an effective adjunct to corticosteroid injection or oral NSAID. Following arthrographic joint distension with corticosteroid and saline, manual therapy and exercise may confer effects similar to those of sham US in terms of overall pain, function and quality of life, but may provide greater patient-reported treatment success and active range of motion.
Saha et al,43 in an extensive review (AMSTAR 5/11) including two RCTs, compared the therapeutic effects of the continuous mode of US either alone or in combination with non-electrotherapeutic treatment/s versus placebo and (or) non-electrotherapeutic treatment/s on shoulder joint ROM in primary FS patients. The quality of this study is limited by the reduced number of RCTs analyzed in a review dealing with studies carried out over 40 years (from 1979 to 2019) and by a lack of large multicentric well-conducted RCTs. In the first study, two groups were compared, the intervention group receiving hot packs, a continuous exercise and US program, and a control group receiving placebo US. In both groups, there was a significant improvement in ROM. In the second study, both groups (intervention and control) underwent physical exercises and stretching, the intervention group receivied US. Both groups had a significant increase in ROM, with no differences between groups. They conclude that it is hard to unequivocally state that the continuous mode of US treatment is beneficial in improving the ROM in different directions in primary FS patients due to the lack of rigorously conducted large multicentric trials of a relatively longer duration.
Sun et al,44 in a broad review (AMSTAR score of 7/11) of nine RCTs (453 participants), assessed using PEDro scale, compared the effect of steroid injection and physiotherapy (including active glenohumeral motion, extracorporeal shockwave therapy, ice and hot pack, ultrasound, and proprioceptive neuromuscular facilitation) for patients with FS. The primary outcome was functional improvement, and its main limitation is the heterogeneity among the analyzed studies. Sun38 examined only one study about PNF, which involved comparing steroid injections and PNF associated with Maitland mobilization and active exercises. From this study, it emerges that steroid injections are more effective in the management of related disability, while physiotherapy treatment in ROM improvement, particularly in external rotation at 6 weeks after treatment.
Tedla et al,45 in their review (AMSTAR 7/11) including 10 full-length articles, analyzed the effect of various PNF techniques applied to FS and to determine the effective treatment parameters. The additional aim of the study was to conduct a meta-analysis to ascertain the effectiveness of PNF on improving shoulder external rotation and abduction ROM and reducing pain in FS. However, the limitations of this study arise when combining RCTs with one partly experimental study, combining single-session studies with multiple session studies, and combining various methods of PNF treatments. In this review, nine RCTs showed that the PNF group is superior in decreasing pain and reducing disability, increasing ROM, and improving function. The meta-analysis not only showed a significant effect but also that the PNF is superior to conventional physical therapy in decreasing pain, increasing external rotation, and abduction ROM.
Uppal et al46 published a comprehensive review (AMSTAR score of 5/11), selecting nine studies, aimed to analyze the evidence of the available treatments for FS such as physiotherapy, both oral and intra-articular steroid, hydrodilatation, MUA and arthroscopic capsular release. Despite the quality of FS publications, it cannot be determined which is the most effective treatment.
Discussion
The purpose of this umbrella review of systematic reviews is to analyze the literature in order to investigate the effect of the different rehabilitation interventions in the management of patients suffering from FS. The scientific literature includes multiple studies, with a great variability of quality and objectives, relating to rehabilitation interventions concerning the most suitable treatment to be administered in patients with FS.
For the diagnosis, several authors report an acknowledged lack of specific diagnostic criteria for this condition.29,34,35,38,41,46 Due to this lack of gold standard criteria, there may be a heterogeneity in the diagnosis of the reviews analyzed. Some reviews specify that they included trials that selected participants suffering from pain and restriction in shoulder joint ROM in one or more planes32 or two or more planes.35,47 Several different interventions are used in the common clinical practice for treatment of FS, aimed at reducing pain and recovering ROM and function of shoulder joint with beneficial effects on the activities of daily living.1–3,5,7,8,24,29,34–46 In recent years, there has also been an increase in the diagnosis of FS, probably as a consequence of the change in the life and work habits of the general population and in addition to a clearer diagnostic path.48 In the past, there was a tendency to group different pathologies under an umbrella term as “scapulohumeral periarthritis”.49 Nowadays, different rehabilitation treatments have been proposed in the scientific literature.1,2,8 As often happens, it is difficult to make a comparison between rehabilitation interventions (as physiotherapy, physical agent modalities, infiltrative therapy, etc) in terms of safety and effectiveness in patients with FS.
Physical Therapies and Pain in FS
Firstly, we summarized the current evidence in the scientific literature on management of pain in FS, reporting the results of the above-mentioned systematic reviews, according to the following physical therapies:
Low-Level Laser Therapy (LLLT)
In the literature, a growing number of evidence are in favor of LLLT by virtue of its bio stimulating effects in terms of pain reduction compared to placebo. Among the physical therapies, it is the one that shows the most evidence of efficacy.29,39
Ultrasound
Based on the evidence analyzed, the use of ultrasound seems to lead to an improvement in ROM in the short term, as well as a slight effect on the reduction of pain.29,39,43
Pulsed Electromagnetic Field (PEMF)
The only review that analyzed this type of treatment did not report statistically significant results in terms of ROM, pain, and movement except for one study – of low quality – that reported an improvement in pain compared to placebo.29,42
Transcutaneous Electrical Nerve Stimulation (TENS)
There are no studies that can recommend the use of this therapy, except in combination with other therapies.29,34,35,42–44
Short Wave Diathermy
The studies analyzed have provided conflicting recommendations regarding the use of this therapy for FS, as it is of low quality. Therefore, no recommendations can be given on the use of diathermy in the treatment of FS.29,40
Rehabilitative Treatments and Pain in FS
The second question we asked ourselves was the following: What are the most used rehabilitation treatments, and which ones with the highest level of effectiveness?
Mobilizations and Manual Therapy
Different rehabilitation methods were examined by the studies analyzed. The Mulligan method has been shown to be more effective than the Maitland method for ROM and shoulder function, although both are effective for the treatment of FS. Even compared to conventional stretching exercises, the long-term effectiveness is in favor of the Mulligan technique. On the other hand, continuous passive mobilization was found to be better in reducing pain when compared with active exercises.34–37,39–42,44,46
Manipulation Under Anesthesia (MUA)
The studies analyzed in this regard do not allow us to make recommendations concerning the use of this method. However, the combination of MUAs associated with a personalized exercise program is more effective than exercise alone.34,38,42,46
Proprioceptive Neuromuscular Facilitations (PNFs)
PNF treatment is superior to conventional physical therapy for pain reduction, ROM increase, improvement of function in patients with FS. In addition, albeit it shows lower efficacy in the management of related disability compared with steroids, it has greater efficacy in terms of ROM improvement, mainly due to extra rotation.42,44,46
From the analysis of the 14 reviews, an important heterogeneity of the treatments analyzed, the outcomes used, and the different treatment and follow-up times emerged as well as the importance of rehabilitation treatment in the reduction of pain and the improvement of function, such as therapeutic exercise, manual therapy, PNF physical modalities. Among the available evidence regarding physical modalities, LLLT seems to be the only one that leads to effective improvement, even if analyzed only in the short term, in particular for the reduction of pain and the increase in functionality, according to literature.29,31,39
Indeed, LLLT in FS is thought to induce pain reduction acting on several cellular mediators as prostaglandin E2, prostaglandin-endoperoxide synthase-2, interleukin 1-beta, tumor necrosis factor-alpha, and reducing oxidative stress and tissue edema.31
Regarding the other physical therapies examined by the reviews analyzed, given the poor quality and quantity of studies in the literature, no recommendations can be provided. Regarding the methods of mobilization and manual therapy, encouraging results have emerged, despite heterogeneity in the methods and timing of treatment, so that it is not possible to make recommendations. Most of the evidence regarding manual therapy techniques has compared manual therapy with corticosteroid injections. These showed greater efficacy in the short term, but not in the long term with no statistically significant differences in long term.34–37,39–42,44,46 The techniques of MUA, arthroscopic capsular release and corticosteroid injections have shown comparable efficacy to each other.34,38,42,46 Sun44 suggests manual therapy as the treatment of choice in patients with FS and DM, based on the results and low contraindications. In fact, corticosteroid injection may potentially affect the blood glucose; however, there are more evidence showing that the single injection may not have significant influence in patients with concomitant DM and FS.
The multidisciplinary management of these patients through professionals of medicine, surgery, physiotherapy allows the improvement of the functional outcomes and the quality of life of the patients.
Strength and Limitations of the Included Studies
All the studies agree on the lack of high-quality scientific work to prove unequivocally which treatment is better than the other.29,34–46 Various methods have been analyzed, also in combination, but none of them led to appreciable results in order to make recommendations with strong scientific evidence in favor.
Strength and Limitations of the Study
Surely, the strongest limitation is represented by the fact that our article is an umbrella review, which does not compare the results of the various articles included from a statistical point of view. Another limitation is that only articles published in the 10 years prior to 2020 were included.
Conclusions
Taken together, findings of this umbrella review of systematic reviews showed a lack of evidence of high-quality studies analyzing the effects of rehabilitative approaches on the management for FS, albeit they showed intriguing results. Further studies are needed to better assess the efficacy of the various rehabilitation interventions in patients with FS, starting from an adequate diagnosis.
Acknowledgments
We would like to thank Giuliano Alessio and Claudio Saulli.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
All authors have drafted or written, or substantially revised or critically reviewed the article.
All authors have agreed on the journal to which the article will be submitted.
All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
All authors agree to take responsibility and be accountable for the contents of the article.
Disclosure
The authors certify that there is no conflict of interest in any way with any financial organization regarding the material discussed in the manuscript.
References
1. Cho CH, Lee YH, Kim DH, Lim YJ, Baek CS, Kim DH. Definition, diagnosis, treatment, and prognosis of frozen shoulder: a consensus survey of shoulder specialists. Clin Orthop Surg. 2020;12(1):60–67. doi:10.4055/cios.2020.12.1.60
2. Ramirez J. Adhesive capsulitis: diagnosis and management. Am Fam Physician. 2019;99(5):297–300.
3. Neviaser AS, Neviaser RJ. Adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2011;19(9):536–542. doi:10.5435/00124635-201109000-00004
4. Kelley MJ, Shaffer MA, Kuhn JE, et al. Shoulder pain and mobility deficits: adhesive capsulitis. J Orthop Sports Phys Ther. 2013;43(5):A1–31. doi:10.2519/jospt.2013.0302
5. Brue S, Valentin A, Forssblad M, Werner S, Mikkelsen C, Cerulli G. Idiopathic adhesive capsulitis of the shoulder: a review. Knee Surg Sports Traumatol Arthrosc. 2007;15(8):1048–1054. doi:10.1007/s00167-007-0291-2
6. Lyne SA, Goldblatt FM, Shanahan EM. Living with a frozen shoulder - a phenomenological inquiry. BMC Musculoskelet Disord. 2022;23(1):318. doi:10.1186/s12891-022-05251-7
7. Ewald A. Adhesive capsulitis: a review. Am Fam Physician. 2011;83(4):417–422.
8. Kelley MJ, McClure PW, Leggin BG. Frozen shoulder: evidence and a proposed model guiding rehabilitation. J Orthop Sports Phys Ther. 2009;39(2):135–148.
9. Costantino C, Nuresi C, Ammendolia A, Ape L, Frizziero A. Rehabilitative treatments in adhesive capsulitis: a systematic review. J Sports Med Phys Fitness. 2022. doi:10.23736/S0022-4707.22.13054-9
10. Tamai K, Akutsu M, Yano Y. Primary frozen shoulder: brief review of pathology and imaging abnormalities. J Orthop Sci. 2014;19(1):1–5. doi:10.1007/s00776-013-0495-x
11. Zhang Y, Xue R, Tong Z, et al. The efficacy of manipulation with distension arthrography to treat adhesive capsulitis: a multicenter, randomized, single-blind, controlled trial. Biomed Res Int. 2022;2022:1562358. doi:10.1155/2022/1562358
12. Rau CL, Yang JL, Lin JJ, et al. Pain quality descriptors and sex-related differences in patients with shoulder pain. J Pain Res. 2018;11:1803–1809. doi:10.2147/JPR.S169006
13. Cinone N, Letizia S, Santoro L, et al. Intra-articular injection of botulinum toxin type A for shoulder pain in glenohumeral osteoarthritis: a case series summary and review of the literature. J Pain Res. 2018;11:1239–1245. doi:10.2147/JPR.S159700
14. Li JL, Yan CQ, Wang X, et al. Brain functional alternations of the pain-related emotional and cognitive regions in patients with chronic shoulder pain. J Pain Res. 2020;13:575–583. doi:10.2147/JPR.S220370
15. Li K, Bichoupan K, Gilchriest JA, Moosazadeh K. Real-world experience of treating frozen shoulder using active manipulation under local anesthetic: a retrospective study. Medicine. 2021;100(47):e27839. doi:10.1097/MD.0000000000027839
16. Chan HBY, Pua PY, How CH. Physical therapy in the management of frozen shoulder. Singapore Med J. 2017;58(12):685–689. doi:10.11622/smedj.2017107
17. Hegedus EJ, Goode AP, Cook CE, et al. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med. 2012;46(14):964–978. doi:10.1136/bjsports-2012-091066
18. Jia X, Ji JH, Petersen SA, Keefer J, McFarland EG. Clinical evaluation of the shoulder shrug sign. Clin Orthop Relat Res. 2008;466(11):2813–2819. doi:10.1007/s11999-008-0331-3
19. Carbone S, Gumina S, Vestri AR, Postacchini R. Coracoid pain test: a new clinical sign of shoulder adhesive capsulitis. Int Orthop. 2010;34(3):385–388. doi:10.1007/s00264-009-0791-4
20. Wilson J, Russell S, Walton M. The management of frozen shoulder. Curr Phys Med Rehabil Rep. 2015;3:181–187. doi:10.1007/s40141-015-0090-5
21. Karahan N, Ozdemir G, Kolukısa D, Duman S, Arslanoğlu F, Çetin M. Can collagenase be used in the treatment of adhesive capsulitis? Med Princ Pract. 2020;29(2):174–180. doi:10.1159/000503086
22. Khalil R, Tanveer F, Hanif A, Ahmad A. Comparison of Mulligan technique versus muscle energy technique in patients with adhesive capsulitis. J Pak Med Assoc. 2022;72(2):211–215. doi:10.47391/JPMA.1678
23. Lee LC, Lieu FK, Lee HL, Tung TH. Effectiveness of hyaluronic acid administration in treating adhesive capsulitis of the shoulder: a systematic review of randomized controlled trials. Biomed Res Int. 2015;2015:314120. doi:10.1155/2015/314120
24. Catapano M, Mittal N, Adamich J, Kumbhare D, Sangha H. Hydrodilatation with corticosteroid for the treatment of adhesive capsulitis: a systematic review. PM R. 2018;10(6):623–635. doi:10.1016/j.pmrj.2017.10.013
25. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an evaluation of three treatment regimens. Ann Rheum Dis. 1984;43(3):353–360. doi:10.1136/ard.43.3.353
26. Park C, An Y, Yoon H, et al. Comparative accuracy of a shoulder range motion measurement sensor and Vicon 3D motion capture for shoulder abduction in frozen shoulder. Technol Health Care. 2022;30(S1):251–257. doi:10.3233/THC-228024
27. Karabaş Ç, Talay Çalış H, Topaloğlu US, Karakükçü Ç. Effects of platelet-rich plasma injection on pain, range of motion, and disability in adhesive capsulitis: a prospective, randomized-controlled study. Turk J Phys Med Rehabil. 2021;67(4):462–472. doi:10.5606/tftrd.2021.6690
28. Zhang J, Zhong S, Tan T, et al. Comparative efficacy and patient-specific moderating factors of nonsurgical treatment strategies for frozen shoulder: an updated systematic review and network meta-analysis. Am J Sports Med. 2021;49(6):1669–1679. doi:10.1177/0363546520956293
29. Page MJ, Green S, Kramer S, Johnston RV, McBain B, Buchbinder R. Electrotherapy modalities for adhesive capsulitis (frozen shoulder). Cochrane Database Syst Rev. 2014;10:CD011324.
30. Ip D, Fu NY. Two-year follow-up of low-level laser therapy for elderly with painful adhesive capsulitis of the shoulder. J Pain Res. 2015;8:247–252. doi:10.2147/JPR.S84376
31. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;29(372):n160. doi:10.1136/bmj.n160
32. Lewis J. Frozen shoulder contracture syndrome - Aetiology, diagnosis and management. Man Ther. 2015;20(1):2–9. doi:10.1016/j.math.2014.07.006
33. Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. doi:10.1186/1471-2288-7-10
34. Alsubheen SA, Nazari G, Bobos P, MacDermid JC, Overend TJ, Faber K. Effectiveness of nonsurgical interventions for managing adhesive capsulitis in patients with diabetes: a systematic review. Arch Phys Med Rehabil. 2019;100(2):350–365. doi:10.1016/j.apmr.2018.08.181
35. Blanchard V, Barr S, Cerisola FL. The effectiveness of corticosteroid injections compared with physiotherapeutic interventions for adhesive capsulitis: a systematic review. Physiotherapy. 2010;96(2):95–107. doi:10.1016/j.physio.2009.09.003
36. Eljabu W, Klinger HM, von Knoch M. Prognostic factors and therapeutic options for treatment of frozen shoulder: a systematic review. Arch Orthop Trauma Surg. 2016;136(1):1–7. doi:10.1007/s00402-015-2341-4
37. Favejee MM, Huisstede BM, Koes BW. Frozen shoulder: the effectiveness of conservative and surgical interventions–systematic review. Br J Sports Med. 2011;45(1):49–56. doi:10.1136/bjsm.2010.071431
38. Grant JA, Schroeder N, Miller BS, Carpenter JE. Comparison of manipulation and arthroscopic capsular release for adhesive capsulitis: a systematic review. J Shoulder Elbow Surg. 2013;22(8):1135–1145. doi:10.1016/j.jse.2013.01.010
39. Jain TK, Sharma NK. The effectiveness of physiotherapeutic interventions in treatment of frozen shoulder/adhesive capsulitis: a systematic review. J Back Musculoskelet Rehabil. 2014;27(3):247–273. doi:10.3233/BMR-130443
40. Lowe CM, Barrett E, McCreesh K, De Búrca N, Lewis J. Clinical effectiveness of non-surgical interventions for primary frozen shoulder: a systematic review. J Rehabil Med. 2019;51(8):539–556. doi:10.2340/16501977-2578
41. Noten S, Meeus M, Stassijns G, Van Glabbeek F, Verborgt O, Struyf F. Efficacy of different types of mobilization techniques in patients with primary adhesive capsulitis of the shoulder: a systematic review. Arch Phys Med Rehabil. 2016;97(5):815–825. doi:10.1016/j.apmr.2015.07.025
42. Page MJ, Green S, Kramer S, et al. Manual therapy and exercise for adhesive capsulitis (frozen shoulder). Cochrane Database Syst Rev. 2014;8:CD011275.
43. Saha S, Saha S. Shoulder joint mobility in patients with primary adhesive capsulitis after treatment with continuous mode of ultrasound: a systematic review of randomized controlled trials. Med J Islam Repub Iran. 2019;33:144. doi:10.47176/mjiri.33.144
44. Sun Y, Lu S, Zhang P, Wang Z, Chen J. Steroid injection versus physiotherapy for patients with adhesive capsulitis of the shoulder: a PRIMSA systematic review and meta-analysis of randomized controlled trials. Medicine. 2016;95(20):e3469. doi:10.1097/MD.0000000000003469
45. Tedla JS, Sangadala DR. Proprioceptive neuromuscular facilitation techniques in adhesive capsulitis: a systematic review and meta-analysis. J Musculoskelet Neuronal Interact. 2019;19(4):482–491.
46. Uppal HS, Evans JP, Smith C. Frozen shoulder: a systematic review of therapeutic options. World J Orthop. 2015;6(2):263–268. doi:10.5312/wjo.v6.i2.263
47. Riccio I, de Sire A, Latte C, Pascarella F, Gimigliano F. Conservative treatment of traumatic shoulder instability: a case series study. Musculoskelet Surg. 2015;99(2):133–137. doi:10.1007/s12306-015-0373-0
48. Kingston K, Curry EJ, Galvin JW, Li X. Shoulder adhesive capsulitis: epidemiology and predictors of surgery. J Shoulder Elbow Surg. 2018;27(8):1437–1443. doi:10.1016/j.jse.2018.04.004
49. Gao M, Cong H, Li C, Qin X, An H, Jiang Z. Comparison of efficacy and safety of complementary and alternative therapies for scapulohumeral periarthritis: a protocol for Bayesian network meta-analysis. Medicine. 2021;100(18):e25769. doi:10.1097/MD.0000000000025769
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Description of Clinical Features and Diagnoses of 444 Cases with Neck-Shoulder-Upper Extremity Pain: A Single-Center Retrospective Review
Zhang H, Luo W, Li C, Zhao J, Zhang Q, Gu R
Journal of Pain Research 2022, 15:3483-3492
Published Date: 2 November 2022
Is Exercise Rehabilitation an Effective Adjuvant to Clinical Treatment for Myofascial Trigger Points? A Systematic Review and Meta-Analysis
Zhou Y, Lu J, Liu L, Wang HW
Journal of Pain Research 2023, 16:245-256
Published Date: 28 January 2023
The Importance of the Diaphragm in Neuromotor Function in the Patient with Chronic Obstructive Pulmonary Disease
Bordoni B, Escher A, Compalati E, Mapelli L, Toccafondi A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:837-848
Published Date: 11 May 2023
A Systematic Review and Meta-Analysis of the Effects of Rehabilitation Using Digital Healthcare on Musculoskeletal Pain and Quality of Life
Jang S, Lee B, Lee E, Kim J, Lee JI, Lim JY, Hwang JH, Jang S
Journal of Pain Research 2023, 16:1877-1894
Published Date: 31 May 2023
Frozen Shoulder and the Risk of Parkinson’s Disease: A Danish Registry-Based Cohort Study
Gadgaard NR, Veres K, Henderson VW, Pedersen AB
Clinical Epidemiology 2024, 16:447-459
Published Date: 27 June 2024