Back to Journals » International Journal of General Medicine » Volume 19
Non-HDL/HDL Cholesterol Ratio as a Protective Factor for Functional Recovery Following Intracerebral Hemorrhage: A Prospective Cohort Study
Authors Gu T, Yu C, Zha Z, Rao C ![]() , Zhang X
, Zhang X ![]() , Wen M
, Wen M ![]() , Huo Y, He C
, Huo Y, He C ![]() , Zhu L
, Zhu L ![]()
Received 2 December 2025
Accepted for publication 7 March 2026
Published 24 March 2026 Volume 2026:19 585980
DOI https://doi.org/10.2147/IJGM.S585980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Woon-Man Kung
Tong Gu,1 Chuanqin Yu,1 Zhiwen Zha,1 Chen Rao,1 Xuke Zhang,1 Meihai Wen,1 Yucheng Huo,2 Chen He,1 Lei Zhu1
1Department of Neurology, The First Hospital of Anhui University of Science & Technology, Huainan, Anhui, People’s Republic of China; 2Obstetrics and Gynecology, The First Hospital of Anhui University of Science & Technology, Huainan, Anhui, People’s Republic of China
Correspondence: Lei Zhu, Department of Neurology, The First Hospital of Anhui University of Science & Technology, Huainan, Anhui, People’s Republic of China, Email [email protected]
Purpose: Whether lipid profiles influence functional recovery after intracerebral hemorrhage (ICH) is unclear. This study investigated the association between the non-high-density lipoprotein to high-density lipoprotein cholesterol ratio (NHHR) and 90-day functional outcomes in patients with ICH.
Patients and Methods: This single-center, prospective, observational cohort study enrolled 200 patients with acute ICH. Fasting blood samples were collected within 24 hours of admission for lipid profiling, and NHHR was calculated as (total cholesterol high-density lipoprotein cholesterol [HDL-C])/HDL-C. The primary outcome was functional status at 90 days, assessed using the modified Rankin Scale (mRS). Based on the mRS scores, patients were classified into two groups: favorable outcome (mRS ≤ 2, functional independence) and poor outcome (mRS > 2, functional dependence or death).
Results: Of the 200 patients, 81 (40.5%) had poor outcomes at 90 days. The poor outcome group exhibited significantly lower baseline NHHR compared to the favorable outcome group (2.54 vs. 2.75, P = 0.002). After multivariable adjustment, a higher NHHR remained independently associated with reduced odds of poor outcome (adjusted odds ratio = 0.608; 95% confidence interval: 0.401– 0.921; P = 0.019). As a standalone predictor, NHHR exhibited high sensitivity (85.2%) but low specificity (39.5%) for predicting poor outcome, with an optimal cutoff of ≤ 3.185. Its discriminative ability was modest (area under the curve [AUC] = 0.590; 95% CI: 0.510– 0.670; P = 0.03 2). However, combining NHHR with the NIHSS score substantially improved prognostic performance (AUC = 0.863; 95% CI: 0.804– 0.923; P < 0.001), an effect that remained stable after internal validation (bootstrap-corrected AUC = 0.851; 95% CI: 0.789– 0.914).
Conclusion: A higher baseline NHHR independently predicts favorable 90-day outcomes after ICH, supporting a “protective lipid paradox” distinct from ischemic stroke. As a simple and readily available biomarker, NHHR offers complementary prognostic information to established clinical scales and may aid early risk stratification.
Keywords: intracerebral hemorrhage, prognosis, lipid paradox, non-HDL/HDL cholesterol ratio, biomarker
Introduction
Intracerebral hemorrhage (ICH) remains the most devastating stroke subtype, with one-year mortality exceeding 50% and most survivors left permanently disabled.1 Within one month, more than 40% of patients die or become functionally dependent. Survivors also face a two- to three-fold higher risk of recurrent stroke, cognitive decline, and major adverse cardiovascular events.2,3 These outcomes highlight the need for early prognostic tools to guide clinical decisions and improve recovery.
The role of lipid metabolism in ICH prognosis remains controversial. Unlike in ischemic stroke (IS), where cholesterol promotes atherosclerosis, epidemiological data suggest an inverse relationship between cholesterol levels and ICH outcomes—termed the “lipid paradox”.4 Some studies have linked lower low-density lipoprotein cholesterol (LDL-C) and a lower LDL-C/high-density lipoprotein cholesterol (HDL-C) ratio to increased mortality and poor functional recovery after ICH.5,6 However, these findings are inconsistent, and the mechanisms underlying this paradox remain unclear. This uncertainty has gained clinical relevance in the current era of intensive LDL-C lowering for cardiovascular prevention.7
The non-HDL to HDL cholesterol ratio (NHHR) reflects the balance between pro-atherogenic particles (LDL-C, very-low-density lipoprotein cholesterol [VLDL-C]) and anti-atherogenic HDL-C. Compared with single lipid parameters, NHHR provides a more comprehensive view of lipid metabolism and its associated inflammatory and oxidative stress.8,9 Although NHHR predicts outcomes in cardiovascular disease and has been linked to acute kidney injury in ICH,10 its association with functional recovery after ICH has not been prospectively studied.
We hypothesized that a higher baseline NHHR independently predicts favorable functional outcome (modified Rankin Scale [mRS] ≤ 2) at 90 days after ICH. This hypothesis suggests a protective lipid profile in ICH, distinct from the pro-atherogenic profile in IS. Accordingly, this prospective cohort study was designed to: (1) investigate the independent association between baseline NHHR and 90-day functional outcome; and (2) determine whether adding NHHR to the National Institutes of Health Stroke Scale (NIHSS) provides incremental prognostic value.
Materials and Methods
Study Design and Population
This was a single-center, prospective, observational cohort study conducted at the Department of Neurology, The First Affiliated Hospital of Anhui University of Science and Technology, between February 2024 and February 2025. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all participants or their legal representatives.
Eligibility criteria were as follows:
Inclusion criteria:
- Radiologically confirmed spontaneous ICH via computed tomography (CT) or magnetic resonance imaging (MRI);
- Age 18–80 years;
- Symptom onset within 24 hours prior to admission, and completion of both cranial CT and blood sampling within 24 hours of onset;
- Complete clinical documentation.
Exclusion criteria:
- Secondary hemorrhage etiologies (eg., intracranial tumors, traumatic hemorrhage, subarachnoid hemorrhage);
- Significant systemic diseases (cardiac/hepatic/renal insufficiency, hematologic disorders, autoimmune diseases, and malignancies);
- Active infections at onset (acute/chronic infections, hepatitis, tuberculosis);
- Pre-ICH mRS score >2, indicating pre-existing disability;
- Incomplete clinical or laboratory data required for the primary analysis.
A total of 214 patients with acute ICH were screened for eligibility. After excluding 14 patients who met the exclusion criteria, 200 patients were enrolled in this prospective cohort study. For enrolled patients, ICH etiologies were retrospectively classified using the modified Boston criteria (version 2.0).11 Patients were categorized as probable hypertensive ICH (HTN-ICH), probable cerebral amyloid angiopathy-related ICH (CAA-ICH), or indeterminate etiology based on neuroimaging findings and clinical history. Classification was performed independently by two neurologists, with disagreements resolved by consensus. The detailed patient enrollment process is presented in the CONSORT-style flowchart (Figure 1).
 |
Figure 1 Study recruitment profile. |
Demographic and Clinical Information
Baseline demographic and clinical data were collected, including age, sex, vascular risk factors (hypertension, diabetes, coronary artery disease, atrial fibrillation, prior stroke), pre-admission medications (antihypertensive drugs, antidiabetic drugs, statin, and anticoagulants), and admission blood pressure. A history of dyslipidemia was recorded only when explicitly documented in medical records.
Fasting venous blood samples were collected on the first morning after hospital admission, with all laboratory assessments performed within 24 hours of symptom onset. All samples were analyzed in the hospital’s central laboratory using Mindray automated analyzers for hematology, coagulation, and biochemical assays (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China), with strict adherence to routine internal quality control and calibration protocols.
The following laboratory parameters were measured:
Complete blood count: white blood cells (WBC, ×109/L), red blood cells (RBC ×1012/L), neutrophils (NEUT ×109/L), lymphocytes (LYM, ×109/L), platelet count (PLT, ×109/L);
Coagulation profile: prothrombin time (PT, s), international normalized ratio (INR), activated partial thromboplastin time (APTT, s);
Liver and renal function markers: alanine aminotransferase (ALT, U/L), aspartate aminotransferase (AST, U/L), albumin (ALB, g/L), cystatin C (Cys-C, mg/L);
Metabolic and lipid panel: blood glucose (Glu, mmol/L), homocysteine (Hcy, μmol/L), total cholesterol (TC, mmol/L), high-density lipoprotein cholesterol (HDL-C, mmol/L), low-density lipoprotein cholesterol (LDL-C, mmol/L), triglycerides (TG, mmol/L), apolipoprotein A1 (ApoA1, g/L), and apolipoprotein B (ApoB, g/L);
Non-high-density lipoprotein cholesterol (non-HDL-C) was calculated as TC minus HDL-C. Subsequently, the following derived lipid indices were calculated:
Non-HDL-C to HDL-C ratio (NHHR): non-HDL-C/HDL-C;
Remnant cholesterol (RC): TC – HDL-C – LDL-C;
Apolipoprotein B to A1 ratio (ApoB/ApoA1): ApoB/ApoA1.
Outcome Measures
The primary outcome of this study was functional status at 90 days (±7 days) after symptom onset, assessed using the mRS. To ensure unbiased assessment, trained research personnel who were blinded to all baseline data—including clinical information, laboratory results (specifically NHHR levels), and neuroimaging findings—conducted structured telephone or in-person interviews to obtain 90-day mRS scores. For the primary analysis, mRS scores were dichotomized according to a prespecified, clinically validated threshold: favorable outcome was defined as mRS ≤ 2 (indicating functional independence), and poor outcome as mRS > 2 (indicating moderate to severe disability, dependence, or death).
Secondary outcomes included early neurological deterioration (END) and hematoma expansion (HE). According to the definition from the TICH-2 randomized controlled trial,12 END was defined as an increase of ≥4 points in NIHSS score or a decrease of ≥2 points in the Glasgow Coma Scale (GCS) score within 48 hours after admission. HE was defined as an absolute increase in hematoma volume of >6 mL or a relative increase of >33% from baseline to 24-hour follow-up CT scan, according to standard criteria.13 Both END and HE were assessed by investigators blinded to clinical and laboratory data.
Imaging Evaluation
All patients underwent two non-contrast cranial CT scans: one on admission and one within 24 hours after admission. Hematoma volume was calculated using the ABC/2 method: Volume = 0.5 × A × B × C, where A is the maximum longitudinal diameter, B is the perpendicular diameter, and C is the hematoma thickness (scan slice thickness: 0.5 cm).
ICH location and hematoma volume and the presence of intraventricular hemorrhage (IVH) were independently assessed by at least two experienced neurologists blinded to all clinical and laboratory data. Inter-rater reliability for hematoma volume measurement was evaluated using the intraclass correlation coefficient (ICC).
Statistical Analyses
Data were analyzed using SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), and categorical variables as frequency (percentage). Between-group comparisons were performed using the Student’s t-test, Mann–Whitney U-test, chi-square test, or Fisher’s exact test, as appropriate.
Variable Selection and Model Specification
Multivariable logistic regression was used to identify factors independently associated with 90-day functional outcome. A hybrid variable selection strategy was employed. First, key covariates with established prognostic value in ICH—age, sex, admission NIHSS score, hematoma volume, and intraventricular extension—were forced into the model as a priori confounders.14 Second, other potential predictors (all laboratory parameters and additional clinical features) were screened using univariate logistic regression; variables with P < 0.10 were considered candidates. Third, a backward stepwise elimination procedure (exit criterion P ≥ 0.10) was applied to the candidate variables, while the a priori covariates were retained regardless of their P value. The full list of candidate variables is provided in Supplementary Table S1.
Model Building and Assessment
An initial multivariable model was fitted containing all forced covariates and candidate variables. A backward stepwise elimination procedure (exit criterion P ≥ 0.10) was then applied to the candidate variables, with the a priori covariates retained. Multicollinearity was assessed using variance inflation factors (VIF), with VIF > 5 indicating significant multicollinearity.
Diagnostic Accuracy Assessment and Internal Validation
Bootstrap internal validation with 1000 resamples was performed to assess model stability. Effect modification of NHHR by ICH etiology (HTN-ICH vs. CAA-ICH) was examined via an interaction term. Prognostic discriminative ability was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) with 95% confidence intervals (CIs) was calculated using the DeLong method. Optimal cut-off values were determined by maximizing Youden’s index. The 95% CIs for sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were estimated using the exact binomial method (Wilson score interval) and confirmed by bootstrap resampling (1000 iterations).
A two-sided P < 0.05 was considered statistically significant for all inferential analyses.
Results
Study Population and Baseline Characteristics
Between February 2024 and February 2025, 214 consecutive patients with spontaneous ICH were screened for eligibility. After applying the prespecified criteria, 200 patients were enrolled in this prospective cohort (Figure 1). Based on the 90-day mRS assessment, 119 patients (59.5%) were classified as having a favorable outcome (mRS ≤ 2) and 81 patients (40.5%) as having a poor outcome (mRS > 2). According to the modified Boston criteria (version 2.0), 118 patients (59.0%) were classified as probable HTN-ICH, 8 patients (4.0%) as probable CAA-ICH, and the remaining 74 patients (37.0%) as indeterminate etiology.
Notably, a formal diagnosis of dyslipidemia was explicitly documented in the medical records of only 2 patients (1.0%) in the entire cohort; therefore, this variable was not included in the multivariable analyses. Baseline demographic, clinical, and laboratory characteristics stratified by outcome group are summarized in Table 1.
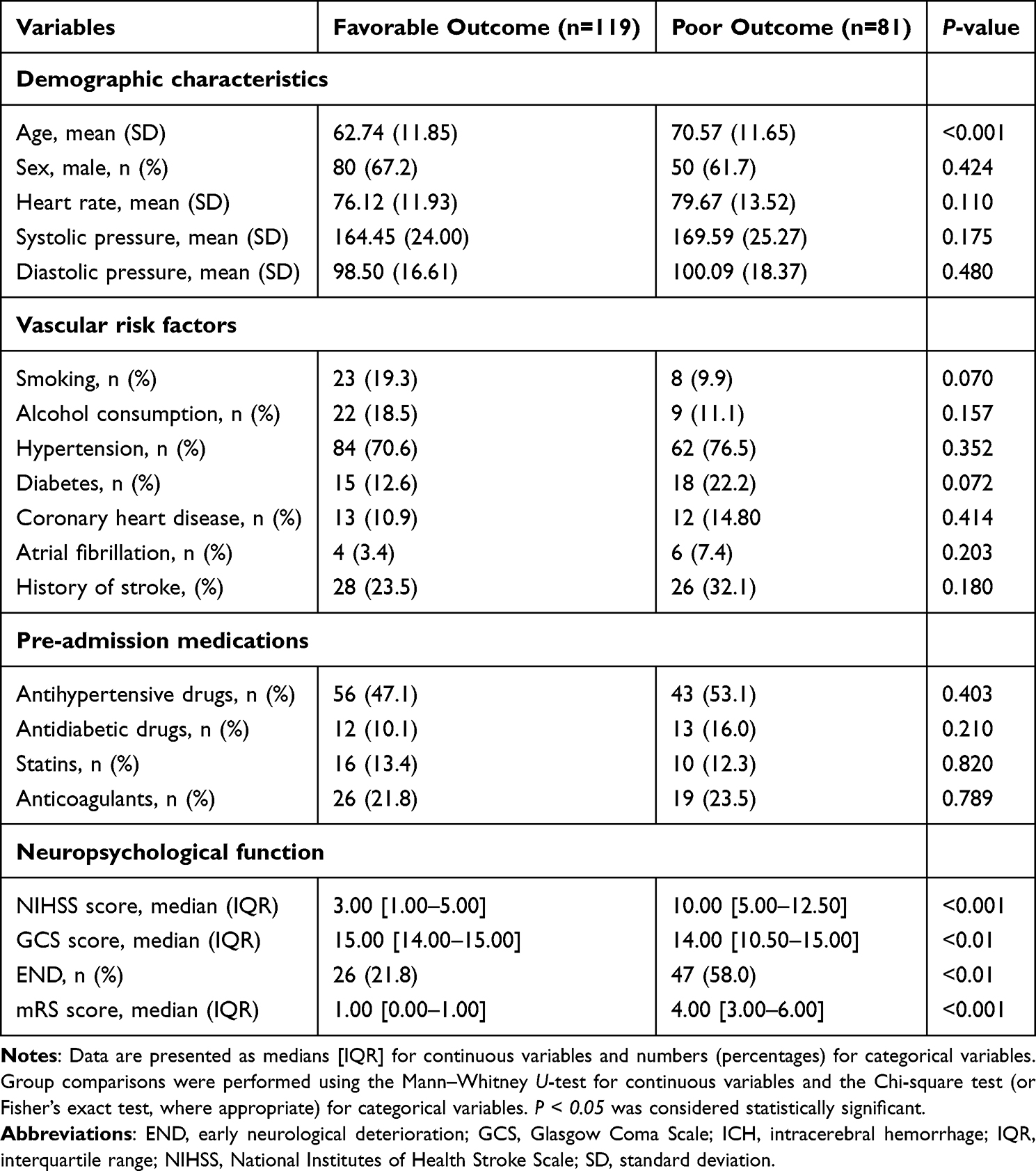 |
Table 1 Baseline Characteristics of Patients with ICH Stratified by 90-Day Functional Outcome |
Patients with poor outcomes, compared to those with favorable outcomes, were significantly older and presented with higher baseline NIHSS scores, higher 90-day mRS scores, and a greater incidence of END, while their admission GCS scores were significantly lower (all P < 0.05). No significant differences were observed in other baseline characteristics, including sex, vascular risk factors, and pre-admission medications (Table 1).
Imaging and Laboratory Parameters at Admission
Neuroimaging Parameters
Inter-rater reliability for hematoma volume measurement was excellent (ICC = 0.92; 95% CI: 0.88–0.95). As presented in Table 2, patients with poor 90-day functional outcomes had significantly larger baseline hematoma volumes, higher rates of intraventricular extension and hematoma expansion, and a predominance of deep hemorrhage location compared to those with favorable outcomes (all P < 0.05).
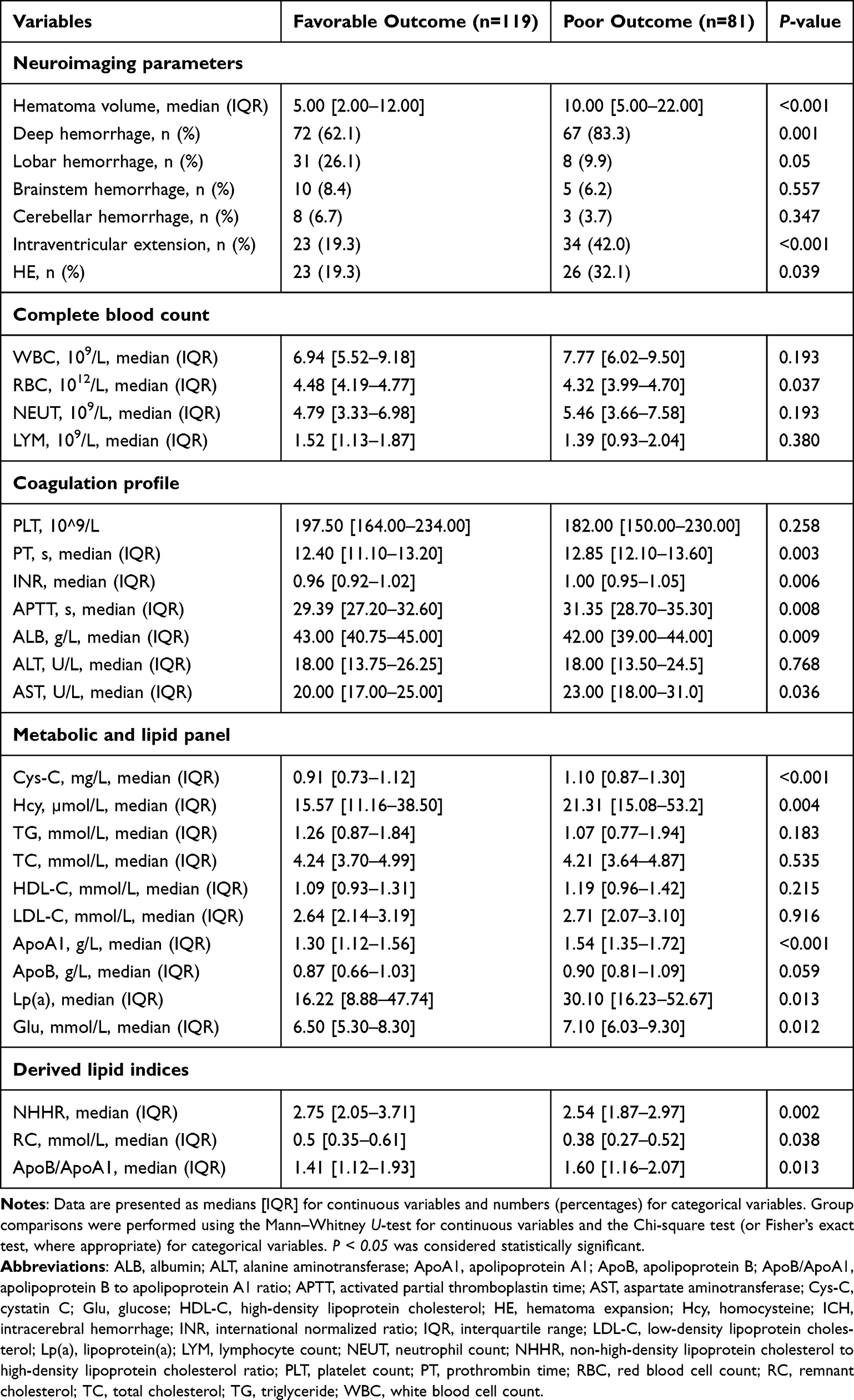 |
Table 2 Comparison of Imaging and Laboratory Findings at Admission in Patients with ICH Stratified by 90-Day Functional Outcome |
Laboratory Parameters
Significant between-group differences were observed in admission laboratory parameters (Table 2). Patients in the poor outcome group exhibited a distinct laboratory profile, characterized by lower RBC counts, ALB levels, and a lower NHHR (P = 0.002). This was accompanied by elevated levels of AST, Cys-C, Hcy, ApoA1, Lp(a), Glu, and ApoB/ApoA1 (all P < 0.05). Additionally, coagulation profiles were prolonged in the poor outcome group, as indicated by significantly higher PT, INR, and APTT (all P < 0.01).
Multivariate Logistic Regression and Robustness Assessment
The final multivariable logistic regression model included the pre-specified clinical covariates (age, sex, NIHSS score, hematoma volume, and IVH) and two laboratory variables retained after stepwise selection: ApoA1 and NHHR (see Supplementary Table S1 for candidate variables).
The final multivariable logistic regression model (Table 3) identified several factors independently associated with poor 90-day functional outcome. A higher NIHSS score was an independent risk factor (adjusted odds ratio [aOR] = 1.151; 95% CI: 1.066–1.242; P < 0.001). Intraventricular extension was also confirmed as an independent risk factor (aOR = 5.46; 95% CI: 1.62–16.67; P = 0.006). Conversely, both a higher baseline NHHR (aOR = 0.608; 95% CI: 0.401–0.921; P = 0.019) and a higher level of ApoA1 (aOR = 0.234; 95% CI: 0.080–0.684; P = 0.008) were independently associated with a reduced odd of poor outcome. Other markers that were significant in univariate analyses, including Cys-C, Glu, and RC, did not retain statistical significance in the final multivariable model.
 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Poor 90-Day Functional Outcome After ICH |
Sensitivity analyses confirmed the robustness of these findings. No significant interaction was observed between NHHR and ICH etiology (P for interaction = 0.288). When a stricter variable entry criterion (P < 0.05) was applied, NHHR was no longer retained in the model, and the primary model showed better fit (lower AIC; Supplementary Table S3).
Correlation Analyses
Correlations between specific laboratory markers and key clinical/radiological parameters were assessed using Spearman or Pearson tests, as appropriate (Table 4).
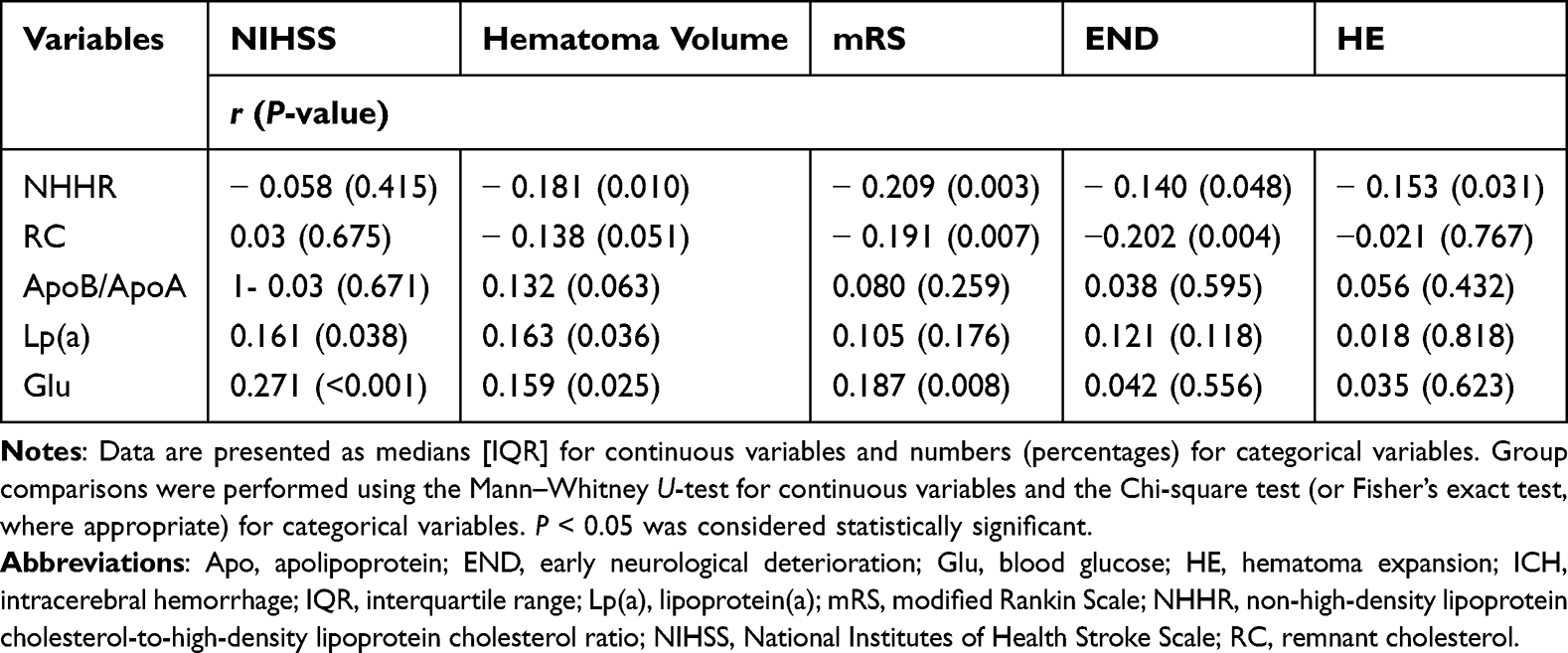 |
Table 4 Correlation Analysis Between Lipid Metabolic Indices and Clinical Severity/Outcome Indicator |
Several significant correlations were observed. NHHR exhibited significant negative correlations with hematoma volume (r = −0.181, P = 0.010), while RC showed a trend toward a negative correlation (r = −0.138, P = 0.051). Both NHHR and RC were negatively correlated with mRS score (r = −0.209, P = 0.003 and r = −0.191, P = 0.007, respectively), END (r = −0.140, P = 0.048 and r = −0.202, P = 0.004), and HE (r = −0.153, P = 0.031 and r = −0.202, P = 0.004). In contrast, Lp(a) and Glu showed significant positive correlations with baseline NIHSS score and hematoma volume (all P < 0.05). The ApoB/ApoA1 ratio did not correlate significantly with any of the severity or outcome indicators (all P > 0.05).
Predictive Performance of Individual and Combined Indicators
The diagnostic accuracy of individual variables and their combinations for predicting poor 90-day outcome was evaluated using ROC curve analysis. The NHHR, when combined with the NIHSS score, demonstrated the highest predictive performance among all tested models (Table 5, Figure 2). A comprehensive summary of all predictive metrics, including AUC, optimal cut-off values, sensitivity, specificity, PPV, and NPV, is provided in Supplementary Table S2.
 |
Table 5 Predictive Performance of Individual Variables and Combined Models for Poor 90-Day Outcome in Patients with ICH |
 |
Figure 2 Receiver operating characteristic (ROC) curves for predicting poor 90-day outcome. (A) ROC curves of all univariate predictors; the National Institutes of Health Stroke Scale (NIHSS) score shows the highest discriminatory ability. (B) ROC curve comparison of the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR), NIHSS score, and their combination. The combined model (NHHR + NIHSS) demonstrates superior predictive performance. Area under the curve (AUC) values are provided in Table 5. |
Among individual indicators (Table 5, Figure 2a), the NIHSS score showed the highest discriminative ability (AUC = 0.845; 95% CI: 0.773–0.917). Age and hematoma volume also showed moderate predictive value (AUC = 0.678 and 0.664, respectively; both P < 0.001). Among laboratory markers, Cys-C exhibited the highest AUC (0.685; 95% CI: 0.599–0.771), followed by RC and Glu. NHHR demonstrated a modest AUC of 0.590 (95% CI: 0.510–0.670; P = 0.032), with high sensitivity (85.2%) but low specificity (39.5%) at its optimal cutoff of ≤3.185.
Among bivariate combinations (Table 5, Figure 2b), the model integrating NHHR with the NIHSS score yielded the highest predictive performance (AUC = 0.863; 95% CI: 0.804–0.923; P < 0.001), with a sensitivity of 88.0% and specificity of 83.0%. This AUC was numerically higher than that of NIHSS alone (0.845) and substantially exceeded those of other NHHR-based combinations (eg., with age, Cys-C, or Glu; AUCs 0.622–0.710). Bootstrap internal validation confirmed the model’s stability (optimism-corrected AUC = 0.851; 95% CI: 0.789–0.914).
To visualize the association of NHHR with outcome, patients were stratified by NHHR quartiles (Figure 3). The proportion of patients with a favorable outcome increased with higher NHHR quartiles, from 56.0% in Q1 to 80.0% in Q4, consistent with its protective effect observed in multivariable analysis.
 |
Figure 3 Proportion of patients with favorable outcome stratified by NHHR quartiles. |
Discussion
In this single-center, prospective cohort study, a higher baseline NHHR was independently associated with favorable 90-day functional outcomes after ICH. In our multivariable model, each unit increase in NHHR corresponded to an estimated 39% reduction in the odds of poor outcome (adjusted odds ratio = 0.608; 95% CI: 0.401–0.921; P = 0.019), an effect that persisted after bootstrap internal validation. Furthermore, NHHR showed significant negative correlations with key radiographic and clinical endpoints, including hematoma volume (r = –0.181, P = 0.010), HE (r = –0.153, P = 0.031), and 90-day mRS score (r = –0.209, P = 0.003). The consistency of these associations across multiple outcomes suggests a mechanistic link between systemic lipid homeostasis and the attenuation of early hematoma growth, a critical determinant of ICH prognosis.
Previous studies on the lipid paradox in ICH have largely focused on isolated lipid parameters (eg., LDL-C or HDL-C), with inconsistent conclusions.15,16 By contrast, this study prospectively evaluated, for the first time, a composite lipid index—NHHR—in relation to functional recovery after ICH. By capturing the balance between atherogenic and atheroprotective lipid pools, NHHR offers a more integrated metabolic perspective. This approach revealed two key insights. First, lipid balance—rather than absolute levels of individual components—is independently associated with functional recovery. Second, this association appears to be mediated through pathways linked to hematoma expansion—a mechanistic insight that would not have been captured by analyzing isolated lipid fractions. These findings provide a potential explanation for the inconsistent results of previous studies, as the prognostic effect of one lipid fraction likely depends on the relative level of the other.
The contrasting roles of lipids in ICH versus ischemic stroke reflect fundamental differences in their underlying pathophysiology. In IS, elevated non-HDL-C promotes atherosclerotic plaque instability and thromboembolic risk, establishing lipid-lowering as a cornerstone of secondary prevention.17 In ICH, by contrast, the primary injury is not atherothrombotic but hemorrhagic, creating an acute demand for lipid substrates to support cellular membrane repair, hematoma containment, and vascular integrity18—biological processes that are not merely different in degree, but entirely distinct in kind from those operating in IS. Within this pathophysiological framework, NHHR acquires a distinct biological meaning. A higher NHHR reflects both an adequate supply of cholesterol for membrane repair (non-HDL-C) and preserved HDL-related vascular protective function.19 The observed association between higher NHHR and favorable recovery is therefore not paradoxical, but rather coherent with the unique metabolic demands of the hemorrhagic brain.
In this cohort, baseline LDL‑C levels did not differ between the favorable and poor outcome groups (2.64 vs. 2.71 mmol/L, P = 0.916). By contrast, a higher NHHR was independently associated with favorable recovery (aOR = 0.608, P = 0.019). This dissociation suggests that, by capturing both non‑HDL‑C and HDL‑C, NHHR may reflect a broader metabolic phenotype—one that reflects both cholesterol availability for tissue repair and HDL‑related vascular protective function.
Apolipoprotein A1, the primary functional protein of HDL‑C, offers an indirect window onto this protective capacity. In our cohort, the poor prognosis group had significantly higher ApoA1 levels (1.54 vs. 1.30 g/L, P < 0.001) yet a lower NHHR (2.54 vs. 2.75, P = 0.002). This dissociation suggests that HDL function, rather than HDL cholesterol concentration per se, may be the more clinically relevant metric in acute ICH. Although ApoA1 facilitates reverse cholesterol transport and clearance of cerebral cholesterol,20,21 acutely elevated ApoA1 may signal HDL functional exhaustion rather than enhanced protection.
HE doubles the risk of death or severe disability after intracerebral hemorrhage, independent of baseline hematoma volume.22 A 2020 meta-analysis of 4310 patients confirmed that HE is the strongest modifiable determinant of poor functional outcome, with an odds ratio of 3.83 (95% CI: 2.51–5.85) for death or severe disability.23 Previous studies have also reported associations between low cholesterol levels and increased HE risk or poorer outcomes after ICH,24,25 consistent with our finding that lower NHHR—reflecting an unfavorable lipid profile—was associated with higher HE incidence. Our data show that lower admission NHHR was associated with higher HE incidence (r = –0.153, P = 0.031) and larger hematoma volume (r = –0.181, P = 0.010). This dose‑response relationship supports a potential mechanistic link between lipid profile and hematoma growth.
Our findings suggest three potential pathways by which an unfavorable lipid profile may increase HE risk.
First, platelet hemostatic function. Cholesterol is required for platelet membrane integrity. Hypocholesterolemia depletes membrane cholesterol, impairs aggregation, and prolongs bleeding time—documented in both genetic hypercatabolism and animal ICH models.26 Low NHHR may thus delay primary hemostasis at the vessel rupture site.
Second, endothelial barrier integrity. HDL‑C preserves endothelial function via SR‑BI‑mediated eNOS activation and tight junction maintenance. Disruption of this pathway increases microvascular fragility18,27 and predisposes to rebleeding under hemodynamic stress. The excess of deep hemorrhages in our poor‑outcome group (83.3% vs. 62.1%, P = 0.001) is consistent with impaired endothelial resistance.
Third, erythrocyte membrane stability. Erythrocyte deformability and osmotic resistance depend on membrane lipid composition. Higher RBC counts in the high‑NHHR group (4.48 vs. 4.32 × 1012/L, P = 0.037) suggest that a favorable lipid milieu stabilizes erythrocyte membranes,28 potentially attenuating hemolysis‑driven hemoglobin release, hydroxyl radical generation, and secondary blood–brain barrier disruption.
An unfavorable lipid profile may simultaneously impair clot formation, weaken the microvascular wall, and destabilize erythrocytes—three distinct mechanisms that collectively increase the likelihood of hematoma enlargement. It is important to acknowledge that these mechanistic interpretations, while biologically plausible and grounded in our correlational data, remain speculative. Our study was designed as a clinical prognostic investigation and did not include direct functional assays—such as measurements of platelet aggregation, endothelial tight junction proteins, or erythrocyte membrane fluidity—that would be required to empirically validate these pathways. Future translational studies incorporating such assessments are necessary to establish causality and move beyond association.
We further evaluated the predictive efficacy of NHHR for poor 90-day outcome. As a single predictor, NHHR achieved an AUC of 0.590 (95% CI: 0.510–0.670, P = 0.032) with an optimal cutoff of ≤3.185 (sensitivity, 85.2%; specificity, 39.5%). Given its high sensitivity but limited specificity, NHHR has restricted utility as a standalone screening tool and is better positioned as a complementary biomarker. Notably, the combination of NHHR and the NIHSS score yielded superior predictive performance (AUC = 0.863, 95% CI: 0.804–0.923, P <0.001), with a sensitivity of 88.0% and specificity of 83.0%. The complementary nature of NHHR and NIHSS likely reflects their distinct biological and clinical dimensions: NHHR captures systemic lipid metabolic status and tissue repair potential, whereas NIHSS quantifies the severity of established neurological deficits.29,30 Their combination thus integrates biochemical information with clinical manifestations, providing a more comprehensive prognostic assessment than either marker alone.
Importantly, the protective association of NHHR with favorable outcome appeared linear across the observed range, without evidence of a U‑shaped or threshold effect within our cohort. The optimal cutoff value of 3.185 identified by ROC analysis represents a classification threshold for risk stratification, not a biological “switch” beyond which protection is lost or reversed. Whether extremely high NHHR levels might confer different effects warrants investigation in larger, more diverse populations.
The protective effects of NHHR may vary across racial and sex subgroups. The optimal NHHR range differs between populations, with Chinese cohorts showing a higher beneficial range compared with Western populations.31 Genetic variations in lipid metabolism genes and dietary patterns may have contributed to these disparities.32 Additionally, the estrogen-mediated upregulation of SR-B1 receptors enhances HDL functionality, potentially amplifying the protective effects of NHHR in female patients with ICH.33 Future studies with larger, diverse populations and stratified analyses by race and sex are warranted to validate these interactions.
Limitations and Future Directions
This study has several limitations that merit consideration. These limitations, however, should be interpreted in light of the study’s primary aim—to establish the prognostic value of NHHR in a well-characterized prospective ICH cohort—and they provide clear directions for future research rather than diminishing the validity of our core findings.
First, the single-center design limits generalizability. While internal validation with bootstrap resampling (optimism-corrected AUC = 0.851) supports model stability within our cohort, external validation in independent, multi-center populations is essential. Model performance may vary across settings due to differences in case mix, clinical practices, and laboratory methodologies—a well-documented phenomenon in prognostic research. The observational design also precludes causal inference regarding NHHR and outcomes.
Second, despite adjustment for key confounders, including statin use and coagulation parameters, residual confounding from unmeasured factors remains possible. Data on pre-ICH dietary habits and physical activity were not collected, and comprehensive hemostatic function assessments (eg., platelet reactivity, fibrinogen levels) were unavailable. Additionally, a formal diagnosis of dyslipidemia was documented in only 2 patients (1.0%), reflecting under-documentation in acute care rather than true absence, and could not be adjusted for.
Third, the small number of CAA-ICH cases (n=8) limits conclusions for this subtype. Although an interaction test showed no significant difference by etiology (P for interaction = 0.288), this analysis is underpowered. Dedicated studies with larger CAA-ICH cohorts are needed to definitively determine whether the NHHR effect differs in this population.
Fourth, only baseline NHHR was measured. Serial measurements would clarify whether dynamic lipid changes post-ICH predict recovery and whether the protective lipid profile is sustained or transient. This represents an important direction for future investigation.
Fifth, mechanistic insights remain speculative. Our study did not include advanced lipoprotein characterization (eg., HDL subclasses, cholesterol efflux capacity) or functional assays of platelet aggregation, endothelial integrity, or erythrocyte membrane stability—key pathways implicated by our HE-focused findings. These measurements are essential for moving beyond correlation to mechanistic understanding.
These limitations directly inform three priorities for future research: (1) External validation: Multi-center cohorts spanning diverse geographical regions and ethnic populations are needed to confirm the generalizability of the combined NHHR-NIHSS model, using standardized protocols for lipid measurement and outcome assessment; (2) Mechanistic studies: Future investigations should incorporate serial lipid measurements, advanced lipoprotein profiling, and direct functional assays to elucidate the biological pathways linking NHHR to ICH outcomes. Serial measurements at standardized time points would help determine whether early changes in NHHR predict subsequent recovery and whether the protective lipid profile is sustained or transient; (3) Stratified analyses: Larger studies with sufficient statistical power are needed to explore effect modifications by sex, ethnicity, genetic background, and ICH etiology, enabling more personalized approaches to prognostication.
Conclusion
This study identifies baseline NHHR as a novel, independent, and readily accessible prognostic biomarker for 90-day functional recovery after ICH. A higher NHHR is consistently associated with smaller hematoma volume, reduced hematoma expansion, and lower odds of poor functional outcome, positioning it as a protective metabolic phenotype distinct from the atherogenic profile in ischemic stroke. Critically, the combination of NHHR with the NIHSS score substantially improves prognostic discrimination, achieving an AUC of 0.863. This simple, low-cost, and rapidly available multimodal approach may facilitate early risk stratification and individualized management in acute ICH settings.
These findings advance the paradigm of lipid profiling in ICH—from isolated components toward integrated metabolic signatures—and provide a testable framework for future mechanistic and translational investigations. External validation in multi-center cohorts and elucidation of HDL functional subphenotypes are the immediate next steps.
Abbreviations
ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; AUC, area under the receiver operating characteristic curve; CAA-ICH, cerebral amyloid angiopathy-related intracerebral hemorrhage; CT, computed tomography; Cys-C, cystatin C; END, early neurological deterioration; GCS, Glascow coma scale; Glu, glucose; HE, hematoma expansion; Hcy, homocysteine; HTN-ICH, hypertensive intracerebral hemorrhage; ICC, intraclass correlation coefficient; ICH, intracerebral hemorrhage; IS, ischemic stroke; MRI, magnetic resonance imaging; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; NHHR, non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio; NPV, negative predictive value; PPV, positive predictive value; RC, Remnant cholesterol; ROC, receiver operating characteristic; VIF, variance inflation factor.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and confidentiality concerns, but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This is an observational study. No clinical trial number is applicable. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of The First Hospital of Anhui University of Science and Technology (Approval No.: 2023-KY-B003-001). Informed consent was obtained from all individual participants involved in the study.
Acknowledgments
The authors would like to thank Xiaoling Guo and Changru Sang for their invaluable assistance with data collection. We also extend our gratitude to all the patients and their families for their participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was funded by the Anhui Science and Technology University (Grant No. YZ2023H1C001) and the Anhui Provincial Health Commission (Grant No. AHWJ2023A2016). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Barros G, Nistal D, Martini ML, Kellner CP, Levitt MR. Bilateral endoscopic intracerebral hemorrhage evacuations at two separate time points: a case report. Cureus. 2021;13(12):e20613. doi:10.7759/cureus.20613
2. Moisander A, Pamilo K, Eskelinen A, et al. Low incidence of clinically relevant bleeding complications after fast-track arthroplasty: a register study of 8,511 arthroplasties. Acta Orthop. 2022;93:348–16. doi:10.2340/17453674.2022.2207
3. Kumar R, Abu Bakar A, Thanabalan J, et al. Safety and use of MLC601/MLC901 (NeuroAiDTM) in primary intracerebral hemorrhage: a cohort study from the NeuroAiD safe treatment registry. Brain Sci. 2020;10(8):499. doi:10.3390/brainsci10080499
4. Lv S, Song Y, Zhang FL, et al. Early prediction of the 3-month outcome for individual acute ischemic stroke patients who received intravenous thrombolysis using the N2H3 nomogram model. Ther Adv Neurol Disord. 2020;13:1756286420953054. doi:10.1177/1756286420953054
5. Liu Y, Fu H, Wang Y, et al. Association between the low-density lipoprotein to high-density lipoprotein ratio and prognosis in critically ill intracerebral hemorrhage patients: a retrospective cohort study from the MIMIC-IV database. Lipids Health Dis. 2025;24(1):36. doi:10.1186/s12944-025-02459-z
6. Chang JJ, Katsanos AH, Khorchid Y, et al. Higher low-density lipoprotein cholesterol levels are associated with decreased mortality in patients with intracerebral hemorrhage. Atherosclerosis. 2018;269:14–20. doi:10.1016/j.atherosclerosis.2017.12.008
7. Di Giovanni G, Kataoka Y, Bubb K, Nelson AJ, Nicholls SJ. Impact of lipid lowering on coronary atherosclerosis moving from the lumen to the artery wall. Atherosclerosis. 2023;367:8–14. doi:10.1016/j.atherosclerosis.2023.01.017
8. Li L, Zhuang L, Xu Z, et al. U-shaped relationship between non-high-density lipoprotein cholesterol and cognitive impairment in Chinese middle-aged and elderly: a cross-sectional study. BMC Public Health. 2024;24(1):1624. doi:10.1186/s12889-024-19164-8
9. Huang X, Li J, Zhang L, Zhang C, Li C. The association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and non-alcoholic fatty liver disease in US adults: a cross-sectional study. Sci Rep. 2024;14(1):24847. doi:10.1038/s41598-024-76002-y
10. Wang J, Bian L, Wang A, et al. Liver fibrosis is associated with clinical outcomes in patients with intracerebral hemorrhage. Neuropsychiatr Dis Treat. 2022;18:2021–2030. doi:10.2147/NDT.S375532
11. Lee TC, Leung WC, Ho C, et al. Association of LDL-cholesterol <1.8 mmol/L and statin use with the recurrence of intracerebral hemorrhage. Int J Stroke. 2024;19(6):695–704.
12. Law ZK, Dineen R, England TJ, et al. Predictors and outcomes of neurological deterioration in intracerebral hemorrhage: results from the TICH-2 randomized controlled trial. Transl Stroke Res. 2021;12(2):275–283. doi:10.1007/s12975-020-00845-6
13. Li Z, You M, Long C, et al. Hematoma expansion in intracerebral hemorrhage: an update on prediction and treatment. Front Neurol. 2020;11:702. doi:10.3389/fneur.2020.00702
14. Toyoda K, Palesch YY, Koga M, et al. Regional differences in the response to acute blood pressure lowering after cerebral hemorrhage. Neurology. 2021;96(5):e740–e751. doi:10.1212/WNL.0000000000011229
15. Rodriguez-Luna D, Rubiera M, Ribo M, et al. Serum low-density lipoprotein cholesterol level predicts hematoma growth and clinical outcome after acute intracerebral hemorrhage. Stroke. 2011;42(9):2447–2452. doi:10.1161/STROKEAHA.110.609461
16. Cai B, Peng L, Wang ZB, Zhang M, Peng B. Association between serum lipid and hematoma expansion after spontaneous intracerebral hemorrhage in Chinese patients. J Stroke Cerebrovasc Dis. 2020;29(6):104793. doi:10.1016/j.jstrokecerebrovasdis.2020.104793
17. Wang C, Fu H, Xu H, et al. Non-traditional lipid biomarkers in atherosclerotic cardiovascular disease: pathophysiological mechanisms and strategies to address residual risk. Front Endocrinol. 2025;16:1576602. doi:10.3389/fendo.2025.1576602
18. Huang R, Pang Q, Zheng L, et al. Cholesterol metabolism: physiological versus pathological aspects in intracerebral hemorrhage. Neural Regen Res. 2025;20(4):1015–1030. doi:10.4103/NRR.NRR-D-23-01462
19. Arun AJ, Kaneki S, Baig M, Frishman WH, Aronow WS. High-density lipoprotein dysfunction and atherosclerotic cardiovascular disease: from quantity to quality. Cardiol Rev. 2025. doi:10.1097/CRD.0000000000001126
20. Yu Z, Zhang L, Zhang G, et al. Lipids, apolipoproteins, statins, and intracerebral hemorrhage: a Mendelian randomization study. Ann Neurol. 2022;92(3):390–399. doi:10.1002/ana.26426
21. Xie G, Jiang G, Huang L, et al. The role of APOA-I in Alzheimer’s disease: bridging peripheral tissues and the central nervous system. Pharmaceuticals. 2025;18(6):790. doi:10.3390/ph18060790
22. Pezzini D, Nawabi J, Schlunk F, et al. Predictors and prognostic impact of hematoma expansion in infratentorial cerebral hemorrhage. Neurocrit Care. 2024;40(2):707–714. doi:10.1007/s12028-023-01819-w
23. Wei Y, Zhu G, Gao Y, et al. Island sign predicts hematoma expansion and poor outcome after intracerebral hemorrhage: a systematic review and meta-analysis. Front Neurol. 2020;11:429. doi:10.3389/fneur.2020.00429
24. Magid-Bernstein J, Girard R, Polster S, et al. Cerebral hemorrhage: pathophysiology, treatment, and future directions. Circ Res. 2022;130(8):1204–1229. doi:10.1161/CIRCRESAHA.121.319949
25. Silva Marques J, Ennis G, Venade G, João Soares R, Monteiro N, Gomes A. Association of statins with functional outcome and 30-day mortality in patients with intracerebral hemorrhage. Cureus. 2021;13(4):e14421. doi:10.7759/cureus.14421
26. Siniscalchi C, Basaglia M, Meschi T, et al. Low LDL-cholesterol and hemorrhagic risk: mechanistic insights and clinical perspectives. Int J Mol Sci. 2025;26(12):5612. doi:10.3390/ijms26125612
27. Tapia VS, Withers SE, Zhou R, et al. The role of 25-hydroxycholesterol in the pathophysiology of brain vessel dysfunction associated with infection and cholesterol dysregulation. Dis Model Mech. 2025;18(9):dmm052145. doi:10.1242/dmm.052145
28. Wang Q, Wang D, Gao Y, et al. Impaired membrane lipids in ischemic stroke: a key player in inflammation and thrombosis. J Neuroinflammation. 2025;22(1):144. doi:10.1186/s12974-025-03464-w
29. Wang H, Wang J, Feng D, Wang L, Zhang J. Association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and cognitive impairment in patients with acute mild ischemic stroke. Eur J Med Res. 2025;30(1):430. doi:10.1186/s40001-025-02693-2
30. Lai Y, Jou E, Mofatteh M, et al. 7-Day National Institutes of Health Stroke Scale as a surrogate marker predicting ischemic stroke patients’ outcome following endovascular therapy. Transl Neurosci. 2023;14(1):20220307. doi:10.1515/tnsci-2022-0307
31. Luo X, Ye J, Xiao T, Yi T. Exploration of the association of a lipid-related biomarker, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR), and the risk of breast cancer in American women aged 20 years and older. Int J Surg. 2024;110(9):5939–5941. doi:10.1097/JS9.0000000000001700
32. Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab Syndr Obes. 2022;15:1677–1686. doi:10.2147/DMSO.S355980
33. Wang C, Yang N, Zhang Q, et al. Association between metabolic health indicators and cardiorespiratory fitness in urban young and middle-aged population: a retrospective cross-sectional study. Front Endocrinol. 2025;16:1489152. doi:10.3389/fendo.2025.1489152
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Risk Score (P-score) Based on a Three-Gene Signature, for Estimating the Risk of Prostate Cancer-Specific Mortality
Söderdahl F, Xu LD, Bring J, Häggman M
Research and Reports in Urology 2022, 14:203-217
Published Date: 11 May 2022
Serum NOX4 as a Promising Prognostic Biomarker in Association with 90-Day Outcome of Severe Traumatic Brain Injury
Jiang F, Chen Z, Hu J, Liu Q
International Journal of General Medicine 2022, 15:5307-5317
Published Date: 30 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Expression, Clinical Significance, Immune Infiltration, and Regulation Network of miR-3940-5p in Lung Adenocarcinoma Based on Bioinformatic Analysis and Experimental Validation
Lin Z, Huang W, Xie Z, Yi Y, Li Z
International Journal of General Medicine 2022, 15:6451-6464
Published Date: 6 August 2022
NUP62CL as an Immunological and Prognostic Biomarker of Oral Squamous Cell Carcinoma
Yu X, Xu L, Zhou Y, Zhou X, Yang L, Zhou Y
Journal of Inflammation Research 2023, 16:3799-3809
Published Date: 29 August 2023