Back to Journals » International Journal of Women's Health » Volume 18
Metabolic Syndrome Predicts Chemotherapy Resistance and Poor Prognosis in Epithelial Ovarian Cancer: A Retrospective Observational Cohort Study
Authors Deng J, Cheng L, Xiang G, Yang Z, Li C, He Y, Chen X ![]()
Received 3 April 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:18 614197
DOI https://doi.org/10.2147/IJWH.S614197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jie Deng,1,* Li Cheng,2,* Guiting Xiang,3 Zhiling Yang,4 Chanyu Li,4 Ying He,2 Xiaofeng Chen4
1Department of Gynecology, Xindu Hospital of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Department of Rheumatology and Immunology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 3Department of Gynecology and Obstetrics, The Third People’s Hospital of Xindu District, Chengdu, Sichuan, People’s Republic of China; 4Department of Gynecology and Obstetrics, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaofeng Chen, Department of Gynecology and Obstetrics, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China, Email [email protected] Ying He, Department of Rheumatology and Immunology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Objective: This study aimed to evaluate the association between metabolic syndrome and chemotherapy resistance, as well as its prognostic significance in patients with epithelial ovarian cancer.
Materials and Methods: This single-center retrospective observational cohort study analyzed clinical data from 513 patients with histologically confirmed epithelial ovarian cancer who underwent cytoreductive surgery followed by standard platinum-based chemotherapy at The First Affiliated Hospital of Chengdu Medical College between January 2019 and December 2021. Metabolic syndrome was diagnosed according to the International Diabetes Federation criteria. Follow-up data were collected through outpatient visits and telephone interviews, and overall survival and progression-free survival were recorded. Survival outcomes were evaluated using Kaplan–Meier analysis. Multivariable Cox proportional hazards regression models were employed to identify independent prognostic factors after adjustment for clinically relevant confounders, including age, histological subtype, FIGO stage, surgical completeness, chemotherapy response, and maintenance therapy.
Results: Among the 513 included patients, 180 (35.09%) were diagnosed with metabolic syndrome. Patients with metabolic syndrome had significantly higher body mass index, advanced FIGO stages, higher prevalence of diabetes, hypertension, dyslipidemia, and higher rates of chemotherapy resistance compared to those without metabolic syndrome. Kaplan–Meier analysis showed that patients with metabolic syndrome had significantly shorter overall survival and progression-free survival compared with patients without metabolic syndrome. In multivariable Cox regression analysis, metabolic syndrome remained independently associated with poorer overall survival and progression-free survival after adjustment for potential confounding factors.
Conclusion: Metabolic syndrome is significantly associated with chemotherapy resistance and poor prognosis in patients with epithelial ovarian cancer. These findings suggest that metabolic syndrome may serve as a useful clinical indicator for risk stratification. However, because this was a single-center retrospective observational study, causal relationships cannot be established. Further prospective multicenter studies are warranted to validate these findings.
Keywords: metabolic syndrome, chemotherapy resistance, ovarian cancer, overall survival, progression-free survival
Introduction
Ovarian cancer remains the most lethal gynecological malignancy, characterized by a poor prognosis primarily attributable to late diagnosis and high recurrence rates following initial therapy.1–3 The standard treatment involves cytoreductive surgery followed by platinum-based chemotherapy; however, approximately 70–80% of patients who initially respond to chemotherapy eventually develop resistance, significantly compromising survival outcomes.4,5 Chemotherapy resistance and recurrence represent critical clinical challenges in ovarian cancer management, underscoring the urgent need to identify novel prognostic factors and therapeutic targets to enhance clinical decision-making and patient outcomes.6,7
Metabolic syndrome is characterized by a cluster of interrelated factors, including central obesity, dyslipidemia, hypertension, insulin resistance, and elevated fasting glucose levels. It has emerged as a significant global health concern due to its rising prevalence and its association with multiple malignancies.8–10 Accumulating evidence from human studies indicates that metabolic syndrome and its individual components are not only associated with increased cancer incidence but may also adversely affect treatment response and survival outcomes.11–13 For instance, hyperglycemia, insulin resistance, and dyslipidemia have been linked to reduced chemotherapy sensitivity and poorer prognosis in several solid tumors, potentially through mechanisms involving chronic inflammation, oxidative stress, and activation of insulin-like growth factor–related signaling pathways.14–16 However, despite these findings, the impact of metabolic syndrome on chemotherapy resistance and survival outcomes in epithelial ovarian cancer remains unclear.
Recent studies have investigated the association between metabolic syndrome and ovarian cancer; however, the available evidence remains limited and inconsistent.17,18 Previous research has largely focused on the role of metabolic syndrome in cancer risk and tumor progression, with relatively few studies examining its impact on chemotherapy response and long-term survival in patients with epithelial ovarian cancer.19–21 Furthermore, most existing studies have not comprehensively evaluated whether metabolic syndrome independently predicts chemotherapy resistance and prognosis in epithelial ovarian cancer after controlling for confounding factors. Therefore, the present study aimed to evaluate whether metabolic syndrome was independently associated with chemotherapy resistance and adverse survival outcomes in patients with epithelial ovarian cancer after adjustment for clinically relevant confounding factors. This study may extend previous work and provide more robust clinical evidence to clarify the prognostic and therapeutic relevance of metabolic syndrome in ovarian cancer, thereby facilitating individualized treatment approaches.
Materials and Methods
Study Population
A total of 745 ovarian cancer patients treated at the Department of Obstetrics and Gynecology, The First Affiliated Hospital of Chengdu Medical College, between January 2019 and December 2021. At last, 513 patients were included in the study based on the following inclusion and exclusion criteria, and the patient enrollment process was displayed in Figure 1. Inclusion criteria were as follows: (1) confirmed diagnosis of epithelial ovarian cancer through pathological assessment; (2) presence of metabolic syndrome at the time of enrollment; (3) treatment involving cytoreductive surgery followed by standard platinum-based chemotherapy; and (4) availability of complete medical records and follow-up data. Patients were excluded if they had other coexisting malignancies or failed to complete chemotherapy due to severe complications. Written informed consent was obtained from all participants before the commencement of the study. This study was conducted following the ethical principles of the Declaration of Helsinki and received approval from the Ethics Committee of The First Affiliated Hospital of Chengdu Medical College (No. 23463457).
 |
Figure 1 The flow chart of patient enrollment. |
Patient Treatment and Data Collection
All included patients underwent cytoreductive surgery followed by 6–8 cycles of platinum-based chemotherapy, and some of them received maintenance therapies. Preoperative fasting venous blood samples were collected 1–3 days before surgery and analyzed within 2 hours. Demographic data, clinicopathological parameters, and preoperative laboratory test results were extracted from medical records.
Diagnosis of Metabolic Syndrome
Metabolic syndrome was assessed at the time of admission, prior to the initiation of ovarian cancer treatment. As defined by the International Diabetes Federation (IDF), a diagnosis of Metabolic Syndrome requires the presence of central obesity in combination with any two of the following four criteria: (1) elevated triglyceride levels, equal to or exceeding 1.7 mmol/L (150 mg/dL); (2) decreased high-density lipoprotein (HDL) levels which are less than 1.03 mmol/L (40 mg/dL) in men and less than 1.29 mmol/L (50 mg/dL) in women, or undergoing specific treatment for dyslipidemia; (3) increased blood pressure, indicated by a systolic reading of at least 140 mmHg or a diastolic reading of at least 90 mmHg, or current use of antihypertensive medication; and (4) elevated fasting plasma glucose levels of 5.6 mmol/L (100 mg/dL) or more, or a previous diagnosis of type 2 diabetes mellitus.9 Central obesity was defined using ethnicity-specific IDF thresholds for Asian populations, with waist circumference ≥90 cm in men and ≥80 cm in women.
Definition of Variables
Metabolic syndrome was treated as a binary variable (present vs absent) based on the International Diabetes Federation criteria. Chemotherapy response was categorized as chemotherapy-sensitive versus chemotherapy-resistant according to standard clinical definitions (recurrence ≤6 months). Other covariates, including age and BMI, were analyzed as continuous variables, while clinicopathological characteristics such as FIGO stage, histological subtype, and surgical completeness were included as categorical variables. Surgical completeness was categorized according to the degree of cytoreduction, complete cytoreduction: no macroscopic residual disease; optimal cytoreduction: residual disease ≤1 cm; suboptimal cytoreduction: residual disease >1 cm.
Patient Follow-Up
Patient follow-up was conducted through telephone interviews and outpatient consultations. Assessments during follow-up included physical examinations, imaging studies such as computed tomography, and evaluation of tumor markers as clinically indicated. Overall survival was defined as the duration from the date of diagnosis until death from any cause or the date of the last follow-up. Progression-free survival was measured from the initiation of treatment until disease recurrence, as confirmed by imaging studies or elevated serum tumor marker levels. The last follow-up ended in January 2025, and the median follow-up time was 58 months. The chemotherapy responses were assessed following the guidance of the Response Evaluation Criteria in Solid Tumors.22 Patients were categorized as chemotherapy-sensitive if they demonstrated a significant response to initial platinum-based chemotherapy, achieved clinical remission, or experienced disease recurrence more than six months after treatment completion. Conversely, chemotherapy resistance was defined as disease progression or relapse within six months after completion of initial chemotherapy, despite an initially favorable response.22
Statistical Analysis
Statistical evaluations were conducted using SPSS software (SPSS Inc., Chicago, IL, USA). Data were expressed as frequencies and percentages for categorical variables, and as means with standard deviations (mean ± SD) for continuous variables. The Chi-square test or Fisher’s exact test was applied for analyzing categorical data, whereas the Student’s t-test or Mann–Whitney U-test was used for continuous data, depending on the distribution.
To identify prognostic indicators, both univariate and multivariate analyses were carried out using the Cox proportional hazards model. Covariates included in the multivariable Cox proportional hazards regression models were selected based on clinical relevance and previously established prognostic importance in epithelial ovarian cancer, including age, histological subtype, FIGO stage, surgical completeness, chemotherapy response, and maintenance therapy. Multicollinearity among candidate variables was assessed using variance inflation factors, and no substantial multicollinearity was observed. The proportional hazards assumption was evaluated for all variables included in the Cox models by inspection of log-minus-log survival plots. We performed a post hoc power assessment for the Cox proportional hazards models using Schoenfeld’s method. Overall survival and progression-free survival were estimated using the Kaplan–Meier method, and differences between groups were assessed with the Log rank test. Statistical significance was defined as a two-tailed p-value less than 0.05.
Results
Patient Characteristics
A total of 513 patients diagnosed with epithelial ovarian cancer were included in this study. Patient demographics and clinical characteristics are summarized in Table 1. The median age at diagnosis was 53 years old, and the median body mass index (BMI) was 27 kg/m2. Among participants, 128 (24.95%) had a history of diabetes, 191 (37.23%) had hypertension, and 116 (22.61%) had dyslipidemia. Metabolic syndrome was identified in 180 patients, representing 35.09% of the study cohort.
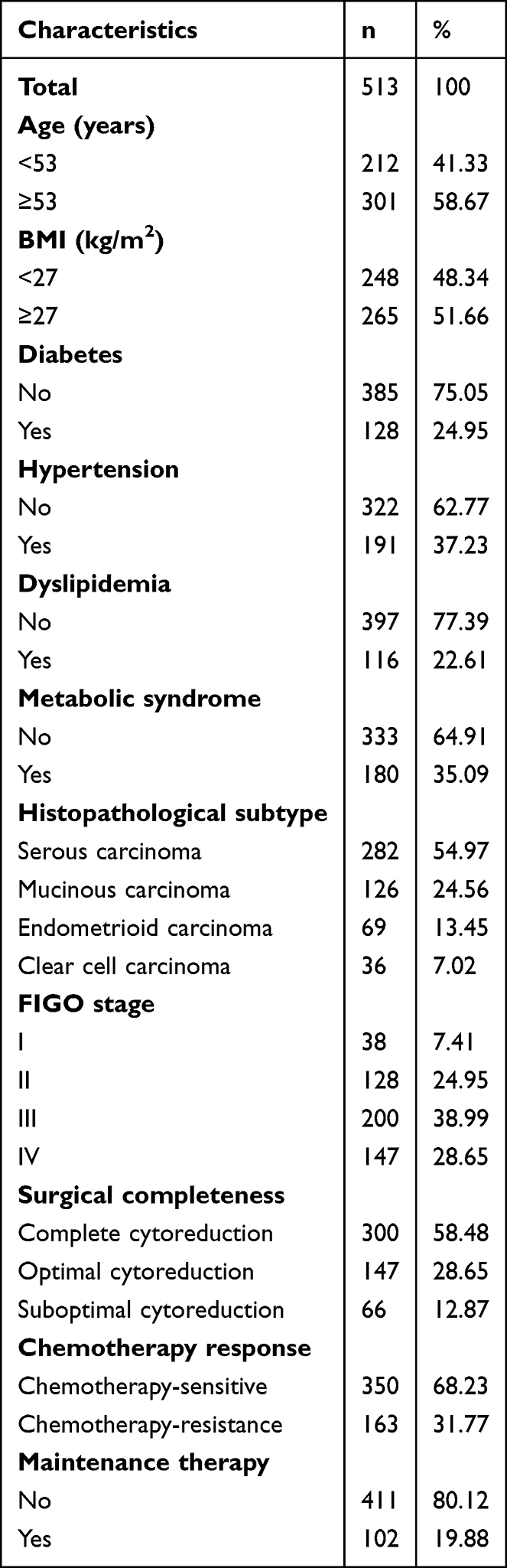 |
Table 1 Patient Characteristics |
Histopathological analysis showed that 282 patients (54.97%) had serous carcinoma, 126 (24.56%) had mucinous carcinoma, 69 (13.45%) had endometrioid carcinoma, and 36 (7.02%) had clear cell carcinoma. According to FIGO staging, 38 (7.41%) patients were classified as stage I, 128 (24.95%) as stage II, 200 (38.99%) as stage III, and 147 (28.65%) as stage IV. Surgical completeness included complete cytoreduction in 300 patients (58.48%), optimal cytoreduction in 147 (28.65%), and suboptimal cytoreduction in 66 (12.87%). Regarding chemotherapy response, 350 (68.23%) patients were classified as chemotherapy-sensitive, while 163 (31.77%) patients demonstrated chemotherapy resistance. A total of 102 (19.88%) patients received maintenance therapy, while 411 (80.12%) patients did not receive maintenance therapy.
Associations Between Patient Characteristics and Metabolic Syndrome
Based on the presence or absence of metabolic syndrome, the study patients were divided into two groups: the metabolic syndrome group and the non-metabolic syndrome group. Table 2 summarizes the patient characteristics associated with metabolic syndrome. Compared to patients without metabolic syndrome, those with metabolic syndrome exhibited significantly higher BMI (p < 0.0001) and more advanced FIGO stages (p < 0.0001). Additionally, metabolic syndrome was significantly associated with diabetes (p < 0.0001), hypertension (p = 0.035), dyslipidemia (p < 0.0001), and chemotherapy response (p = 0.032). However, no significant associations were found between the two groups regarding age (p = 0.623), tumor histological subtype (p = 0.432), surgical completeness (p = 0.397), or maintenance therapy (p = 0.329).
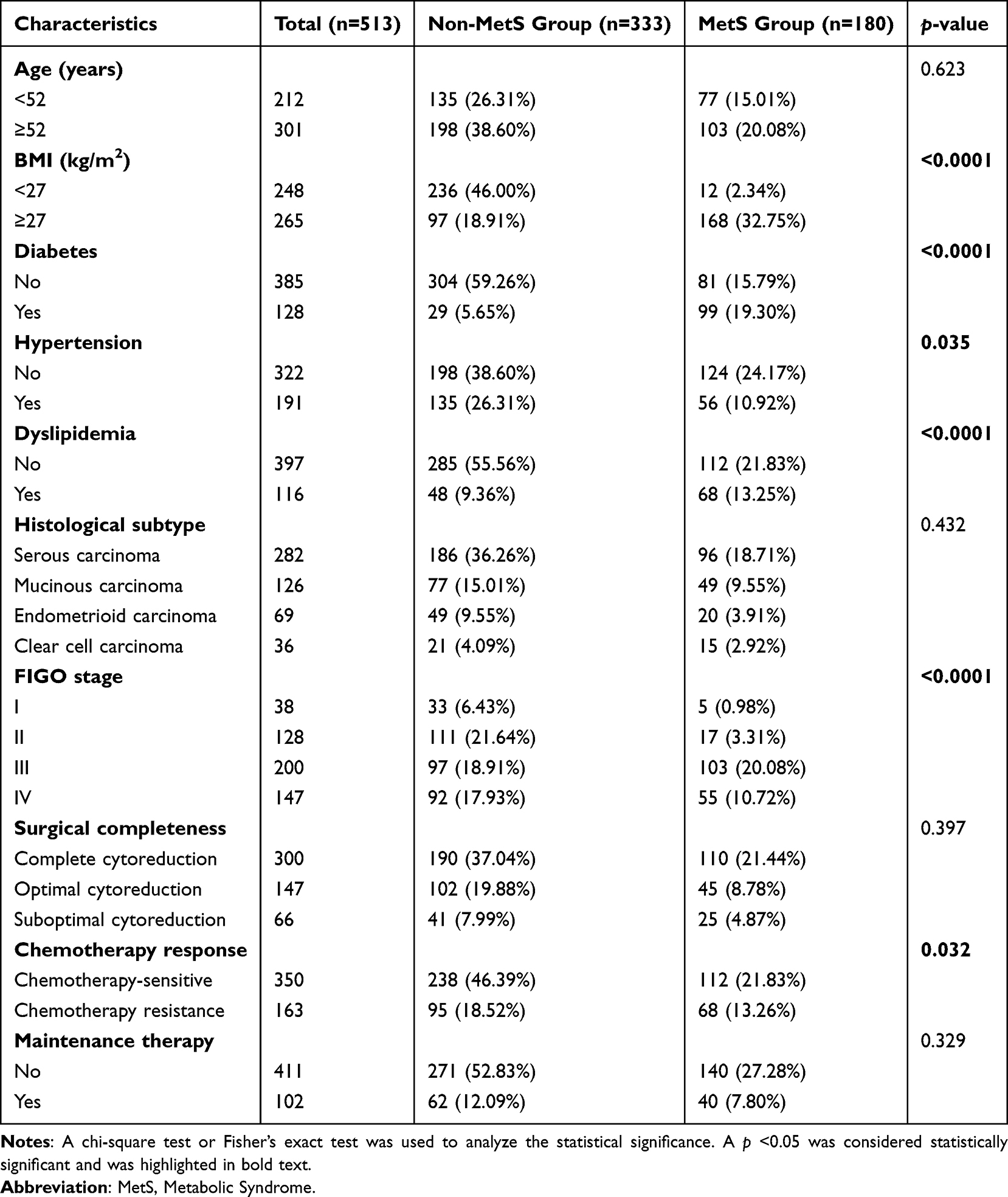 |
Table 2 Associations Between Patient Characteristics and Metabolic Syndrome |
Associations Between Patient Characteristics and Chemotherapy Response
The study cohort was categorized into two groups, including the chemotherapy-resistant group and the chemotherapy-sensitive group based on chemotherapy response. The results indicated that metabolic syndrome (p = 0.032), histological subtype (p < 0.0001), FIGO stages (p < 0.0001), surgical completeness (p = 0.0002), and maintenance therapy (p = 0.0014) were significantly associated with chemotherapy response (Table 3). However, no significant associations were found between the two groups regarding age (p = 0.302), BMI (p = 0.271), diabetes (p = 0.610), hypertension (p = 0.297), or dyslipidemia (p = 0.348) (Table 3).
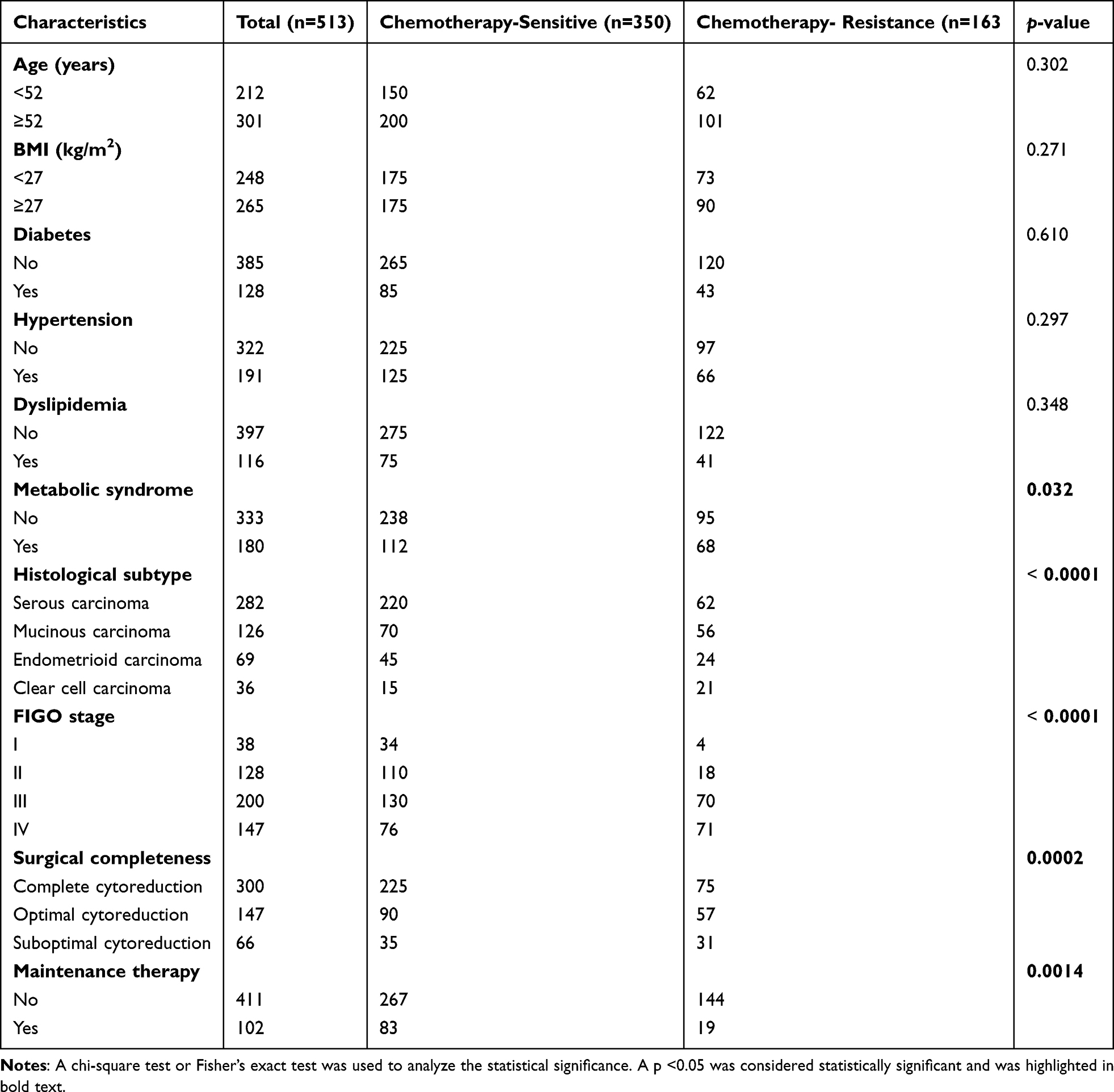 |
Table 3 Associations Between Patient Characteristics and Chemotherapy Response |
Identification of Risk Factors for Overall Survival and Progression-Free Survival of Ovarian Cancer Patients
To identify prognostic factors for ovarian cancer patients, univariate and multivariate Cox proportional hazards regression models were employed. The univariate analysis revealed that metabolic syndrome, tumor FIGO stage, surgical completeness, chemotherapy response, and maintenance therapy were all significantly associated with overall survival (Table 4). In the subsequent multivariate analysis, adjusted for potential confounding variables including age, histological subtype, FIGO stage, surgical completeness, and maintenance therapy, it identified metabolic syndrome (HR = 3.16; 95% CI: 2.11–5.24; p = 0.002) and chemotherapy resistance (HR = 4.83; 95% CI: 2.42–6.03; p < 0.0001) as independent risk factors for overall survival (Table 4). Additionally, progression-free survival was evaluated, it also identified metabolic syndrome (HR = 3.31; 95% CI: 2.02–5.53; p = 0.001) and chemotherapy resistance (HR = 2.95; 95% CI: 2.13–5.47; p < 0.0001) as independent risk factors for progression-free survival (Table 5).
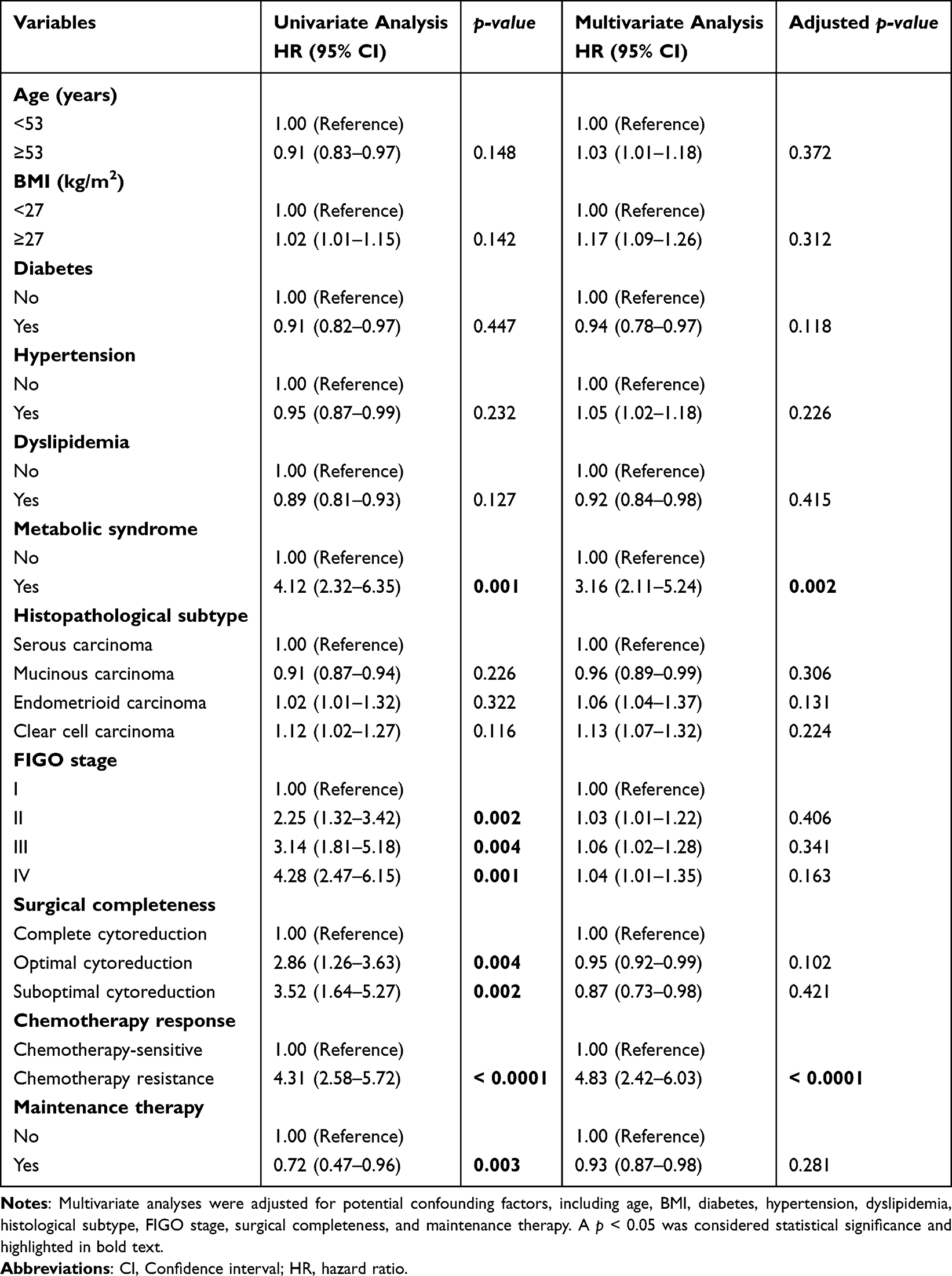 |
Table 4 Identification of Risk Factors for Overall Survival Using Univariate and Multivariate Cox Proportional Hazards Regression Model |
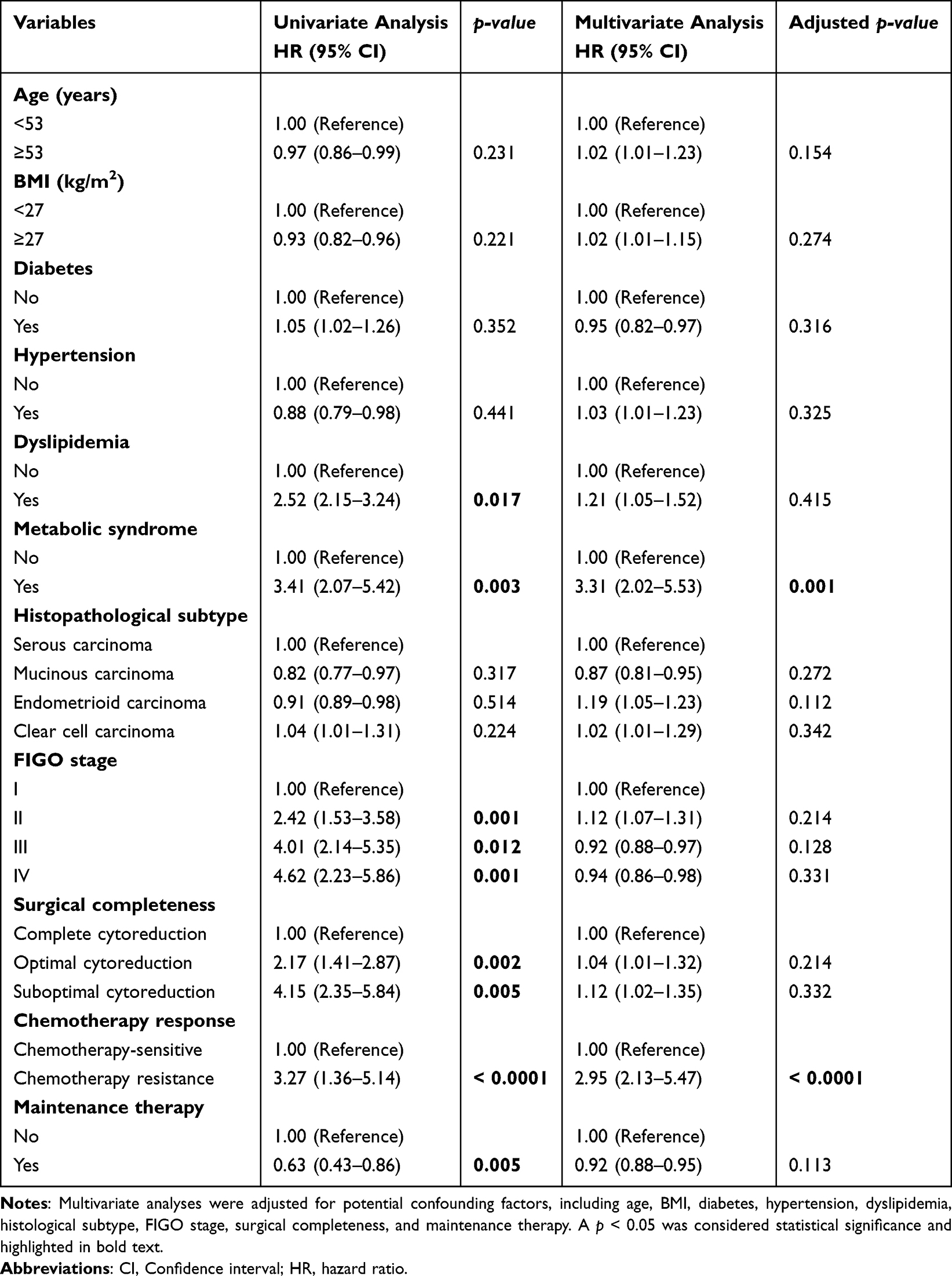 |
Table 5 Identification of Risk Factors for Progression-Free Survival Using Univariate and Multivariate Cox Proportional Hazards Regression Model |
Ovarian Cancer Patients with Metabolic Syndrome Exhibit Reduced Overall and Progression-Free Survival
Kaplan–Meier analyses were performed to compare survival outcomes between ovarian cancer patients with and without metabolic syndrome (Figure 2). The results demonstrated that patients with metabolic syndrome had significantly decreased overall survival (HR = 4.13; 95% CI: 2.32–6.25; p = 0.002) and progression-free survival (HR = 3.54; 95% CI: 1.27–5.68; p = 0.001) compared to those without metabolic syndrome (Figure 2).
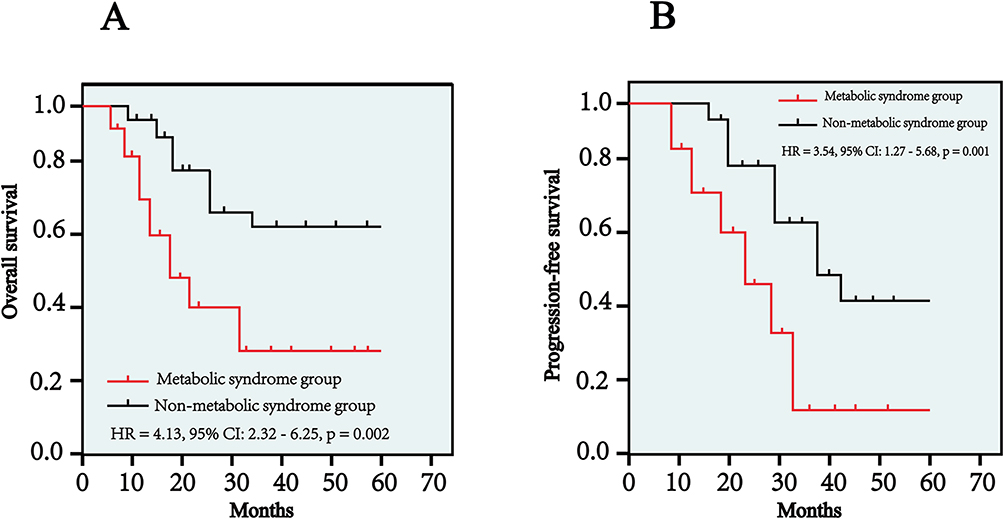 |
Figure 2 Kaplan–Meier curves for overall survival (A) and progression-free survival (B) of ovarian cancer patients with metabolic syndrome and without metabolic syndrome. The statistical differences between groups were assessed by the Log rank test and a p-value less than 0.05 was determined as statistical significance. |
Discussion
In the present study, we demonstrated a significant association between metabolic syndrome and chemotherapy resistance, as well as poor prognosis, in patients with epithelial ovarian cancer. Specifically, our findings indicated that ovarian cancer patients with metabolic syndrome exhibited significantly shorter overall and progression-free survival, and chemotherapy resistance compared to patients without metabolic syndrome. These results underscore the clinical relevance of metabolic syndrome as a potential prognostic marker and therapeutic target for ovarian cancer management, suggesting it may be considered to integrate metabolic evaluation into clinical practice.
Metabolic syndrome is characterized by central obesity, hypertension, dyslipidemia, insulin resistance, and hyperglycemia, and has increasingly been recognized as a contributor to cancer initiation and progression.23–26 Epidemiological evidence consistently suggests that metabolic syndrome and its individual components substantially elevate the risk of various malignancies, including breast, colorectal, and pancreatic cancers.26–28 Mechanistic studies further support these observations, implicating chronic inflammation, oxidative stress, insulin-like growth factor (IGF) signaling alterations, and disruptions in lipid metabolism associated with metabolic syndrome as potential drivers of tumorigenesis and progression.
Our findings align with prior research on the influence of metabolic syndrome on ovarian cancer progression, as evidenced by advanced tumor FIGO stages. A case-control study by Ying Chen et al reported that metabolic syndrome significantly increased the risk of ovarian cancer, advanced disease stages, and tumor aggressiveness, underscoring the complex interaction between metabolic syndrome and cancer progression.17 Similarly, studies of lipid metabolism have shown that lipid-related indices may be associated with chemoresistance and prognosis in epithelial ovarian cancer.19 In contrast, a recent meta-analysis summarized by Ziyu Chen et al found no statistically significant association between metabolic syndrome and ovarian cancer risk; however, their analysis included only five studies, potentially introducing selection bias and limiting generalizability.18 Collectively, these studies, alongside our own, emphasize the importance of metabolic syndrome as a contributing factor in tumorigenesis and ovarian cancer progression.
In this study, we also observed a significant correlation between metabolic syndrome and chemotherapy resistance which is an essential determinant of clinical outcomes in ovarian cancer. The mechanism underlying this association likely involves multiple interconnected pathways. Elevated insulin and IGF-1 levels, common in insulin-resistant states, activate oncogenic signaling cascades such as the phosphoinositide 3-kinase PI3K/Akt pathway, enhancing cell proliferation, promoting survival, and inhibiting apoptosis, thus contributing to chemotherapy resistance.29–31 Additionally, dyslipidemia in metabolic syndrome may alter cell membrane fluidity and drug uptake, thereby influencing the intracellular drug accumulation and efficacy of chemotherapies.32 Consistent with this hypothesis, previous studies indicated that patients with disrupted lipid metabolism experienced poorer responses to platinum-based chemotherapy, highlighting the potential therapeutic value of addressing metabolic disturbances in conjunction with conventional chemotherapy.
Furthermore, obesity-related chronic inflammation which is characterized by elevated pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP) that may exacerbate tumorigenesis and chemotherapy resistance.33 Inflammatory signaling pathways, including the NF-κB pathway, have been documented to upregulate multidrug resistance genes and anti-apoptotic mechanisms, consequently diminishing chemotherapy efficacy.34 Therefore, the chronic inflammatory environment promoted by obesity and metabolic syndrome likely constitutes an additional critical factor underlying the observed association between metabolic syndrome and chemotherapy resistance in ovarian cancer.
Our multivariate analyses identified metabolic syndrome as an independent predictor of poorer overall survival and progression-free survival, even after adjusting for established confounders, such as age, histological subtype, FIGO stage, surgical completeness, and maintenance therapy. These results support the hypothesis that metabolic syndrome independently modulates treatment responses and clinical outcomes. Early identification and management of metabolic syndrome may thus potentially improve treatment responses and survival outcomes in ovarian cancer patients through personalized therapeutic strategies combining metabolic interventions with conventional oncological treatments.
Our findings hold important implications for the management of ovarian cancer patients. Routine screening for metabolic syndrome at ovarian cancer diagnosis could provide clinicians with crucial prognostic information, facilitating more informed therapeutic decision-making. Furthermore, interventions targeting metabolic syndrome including lifestyle modifications and pharmacological therapies aimed at insulin resistance, obesity, hypertension, and dyslipidemia could potentially enhance chemotherapy sensitivity and improve clinical outcomes. For example, previous studies have demonstrated the beneficial effects of metformin in reducing ovarian cancer risk and improving prognosis in ovarian cancer patients through its insulin-sensitizing and anti-inflammatory properties.35,36
This study has several important strengths. First, we employed rigorous and standardized diagnostic criteria for metabolic syndrome, ensuring accurate characterization of metabolic disturbances in our patient population. Second, comprehensive multivariate analyses accounted for numerous potential confounders, robustly validating metabolic syndrome as an independent predictor of clinical outcomes. Lastly, our evaluation of both chemotherapy resistance and survival outcomes provides a holistic assessment of the clinical significance of metabolic syndrome in ovarian cancer.
Nevertheless, some limitations of this study should be acknowledged. Its retrospective design could introduce selection biases, limiting the ability to infer causality from our findings. Despite adjustment for related confounding factors in the multivariate analyses, residual confounding cannot be completely excluded. Furthermore, the relatively limited sample size from a single institution may restrict the generalizability of our conclusions to broader populations. Prospective, multicenter studies involving larger, diverse cohorts are therefore necessary to confirm and extend these observations. Additionally, although our study highlights significant associations, detailed mechanistic investigations are warranted to elucidate the precise biological pathways linking metabolic syndrome to chemotherapy resistance and poor prognosis in ovarian cancer.
Conclusion
In conclusion, this single-center retrospective observational study demonstrated that metabolic syndrome was significantly associated with chemotherapy resistance and poorer overall and progression-free survival in patients with epithelial ovarian cancer. These findings suggest that metabolic syndrome may have prognostic value and could help identify patients at increased risk of adverse prognostic outcomes. However, because of the observational study design, causal relationships cannot be established. Further prospective multicenter interventional studies are needed to validate these findings and to determine whether targeted metabolic management can improve chemotherapy response and survival in patients with epithelial ovarian cancer.
AI Statement
This article used artificial intelligence tool DeepSeek for language improvement.
Abbreviations
BMI, body mass index; CI, confidence interval; CRP, C-reactive protein; HDL, high-density lipoprotein; HR, hazard ratio; IDF, International Diabetes Federation; IGF, insulin-like growth factor; IL-6, interleukin-6; TNF-α, tumor necrosis factor-alpha.
Ethics Statement
This study was conducted following the ethical principles of the Declaration of Helsinki and received approval from the Ethics Committee of The First Affiliated Hospital of Chengdu Medical College (No. 23463457).
Acknowledgment
Jie Deng and Li Cheng contributed equally to this work and shared the first authorship.
Funding
This work was supported by grants from the Chengdu Medical Scientific Research Project (No. 2024087), Sichuan Provincial Medical and Health Promotion Association (No. KY2022QN0293), Sichuan Science and Technology Program (No. 2024NSFSC1903), and The High-level Talents Project of Chengdu Medical College (No. CYFY-GQ70).
Disclosure
We declare no conflict of interest.
References
1. Jiang L, Wang J. Downregulation of INPP4B is associated with poor prognosis in epithelial ovarian carcinoma. Int J Gen Med. 2024;17:1059–13. doi:10.2147/IJGM.S445491
2. Zheng M, Li S, Deng J, Huang C, Zhang H. Identification and clinical validation of high HSP60 expression predicts poor prognosis in patients with ovarian cancer. Int J Gen Med. 2025;18:103–111. doi:10.2147/IJGM.S499524
3. Su H, Liao D, Huang C, Liu Q, Yu L. Low serum cholinesterase levels predict poor prognosis in patients with ovarian cancer. Int J Gen Med. 2025;18:1023–1033. doi:10.2147/IJGM.S509718
4. Ashworth A, Balkwill F, Bast RC, et al. Opportunities and challenges in ovarian cancer research, a perspective from the 11th Ovarian cancer action/HHMT Forum, Lake Como, March 2007. Gynecol Oncol. 2008;108(3):652–657. doi:10.1016/j.ygyno.2007.11.014
5. Santaballa A, Barretina P, Casado A, et al. SEOM clinical guideline in ovarian cancer (2016). Clin Transl Oncol. 2016;18(12):1206–1212. doi:10.1007/s12094-016-1588-8
6. Huo X, Sun H, Liu S, et al. Identification of a prognostic signature for ovarian cancer based on the microenvironment genes. Front Genet. 2021;12:680413. doi:10.3389/fgene.2021.680413
7. Zhou HH, Chen X, Cai LY, et al. Erastin reverses ABCB1-mediated docetaxel resistance in ovarian cancer. Front Oncol. 2019;9:1398. doi:10.3389/fonc.2019.01398
8. Li F, Du H, Li S, Liu J. The association between metabolic syndrome and gastric cancer in Chinese. Front Oncol. 2018;8:326. doi:10.3389/fonc.2018.00326
9. Alberti KG, Zimmet P, Shaw J. Metabolic syndrome--a new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23(5):469–480. doi:10.1111/j.1464-5491.2006.01858.x
10. Motterle G, L DEZ, Zecchini G, et al. Metabolic syndrome and risk of prostate cancer: a systematic review and meta-analysis. Panminerva Med. 2022;64(3):337–343. doi:10.23736/S0031-0808.21.04507-9
11. Yang X, Li X, Dong Y, et al. Effects of metabolic syndrome and its components on the prognosis of endometrial cancer. Front Endocrinol. 2021;12:780769. doi:10.3389/fendo.2021.780769
12. Berrino F, Villarini A, Traina A, et al. Metabolic syndrome and breast cancer prognosis. Breast Cancer Res Treat. 2014;147(1):159–165. doi:10.1007/s10549-014-3076-6
13. Tao W, Yuan C, Kang B, et al. The effect of metabolic syndrome on colorectal cancer prognosis after primary surgery. Nutr Cancer. 2023;75(1):331–338. doi:10.1080/01635581.2022.2112243
14. Mili N, Paschou SA, Goulis DG, Dimopoulos MA, Lambrinoudaki I, Psaltopoulou T. Obesity, metabolic syndrome, and cancer: pathophysiological and therapeutic associations. Endocrine. 2021;74(3):478–497. doi:10.1007/s12020-021-02884-x
15. Bacalbasa N, Diaconu C, Iliescu L, et al. The influence of the metabolic syndrome on early postoperative outcomes of patients with advanced-stage endometrial cancer. Vivo. 2020;34(5):2913–2917. doi:10.21873/invivo.12120
16. Lee DY, Lee TS. Associations between metabolic syndrome and gynecologic cancer. Obstet Gynecol Sci. 2020;63(3):215–224. doi:10.5468/ogs.2020.63.3.215
17. Chen Y, Zhang L, Liu W, Wang K. Case-control study of metabolic syndrome and ovarian cancer in Chinese population. Nutr Metab. 2017;14(1):21. doi:10.1186/s12986-017-0176-4
18. Chen Z, Liu Z, Yang H, Liu C, Kong F. Metabolic syndrome and risk of ovarian cancer: a systematic review and meta-analysis. Front Endocrinol. 2023;14:1219827. doi:10.3389/fendo.2023.1219827
19. Li Y, Shang C, Liang H, Zhang K, Wu Y, Guo H. Associations of novel serum lipid index with epithelial ovarian cancer chemoresistance and prognosis. Front Oncol. 2023;13:1052760. doi:10.3389/fonc.2023.1052760
20. Huang GS, Brouwer-Visser J, Ramirez MJ, et al. Insulin-like growth factor 2 expression modulates Taxol resistance and is a candidate biomarker for reduced disease-free survival in ovarian cancer. Clin Cancer Res. 2010;16(11):2999–3010. doi:10.1158/1078-0432.CCR-09-3233
21. Ma Q, Liu Z, Wang T, et al. Resensitizing paclitaxel-resistant ovarian cancer via targeting lipid metabolism key enzymes CPT1A, SCD and FASN. Int J Mol Sci. 2023;24(22):16503. doi:10.3390/ijms242216503
22. Karmakar A, Kumtakar A, Sehgal H, Kumar S, Kalyanpur A. Interobserver variation in response evaluation criteria in solid tumors 1.1. Acad Radiol. 2019;26(4):489–501. doi:10.1016/j.acra.2018.05.017
23. Prasad H, Ryan DA, Celzo MF, Stapleton D. Metabolic syndrome: definition and therapeutic implications. Postgrad Med. 2012;124(1):21–30. doi:10.3810/pgm.2012.01.2514
24. Goodman E, Daniels SR, Dolan LM. Definition of metabolic syndrome. J Pediatr. 2007;150(4):e36. author replye36-7. doi:10.1016/j.jpeds.2006.11.057
25. Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. 2012;35(11):2402–2411. doi:10.2337/dc12-0336
26. Chlebowski RT, Aragaki AK, Pan K, et al. Breast cancer incidence and mortality by metabolic syndrome and obesity: the women’s health initiative. Cancer. 2024;130(18):3147–3156. doi:10.1002/cncr.35318
27. Chen H, Zheng X, Zong X, et al. Metabolic syndrome, metabolic comorbid conditions and risk of early-onset colorectal cancer. Gut. 2021;70(6):1147–1154. doi:10.1136/gutjnl-2020-321661
28. Zhong L, Liu J, Liu S, Tan G. Correlation between pancreatic cancer and metabolic syndrome: a systematic review and meta-analysis. Front Endocrinol. 2023;14:1116582. doi:10.3389/fendo.2023.1116582
29. Nwabo Kamdje AH, Seke Etet PF, Kipanyula MJ, et al. Insulin-like growth factor-1 signaling in the tumor microenvironment: carcinogenesis, cancer drug resistance, and therapeutic potential. Front Endocrinol. 2022;13:927390. doi:10.3389/fendo.2022.927390
30. Tufail M, Wan WD, Jiang C, Li N. Targeting PI3K/AKT/mTOR signaling to overcome drug resistance in cancer. Chem Biol Interact. 2024;396:111055. doi:10.1016/j.cbi.2024.111055
31. Cheaib B, Auguste A, Leary A. The PI3K/Akt/mTOR pathway in ovarian cancer: therapeutic opportunities and challenges. Chin J Cancer. 2015;34(1):4–16. doi:10.5732/cjc.014.10289
32. Peetla C, Vijayaraghavalu S, Labhasetwar V. Biophysics of cell membrane lipids in cancer drug resistance: implications for drug transport and drug delivery with nanoparticles. Adv Drug Deliv Rev. 2013;65(13–14):1686–1698. doi:10.1016/j.addr.2013.09.004
33. Lashinger LM, Rossi EL, Hursting SD. Obesity and resistance to cancer chemotherapy: interacting roles of inflammation and metabolic dysregulation. Clin Pharmacol Ther. 2014;96(4):458–463. doi:10.1038/clpt.2014.136
34. Koti M, Siu A, Clement I, et al. A distinct pre-existing inflammatory tumour microenvironment is associated with chemotherapy resistance in high-grade serous epithelial ovarian cancer. Br J Cancer. 2015;112(7):1215–1222. doi:10.1038/bjc.2015.81
35. Shi J, Liu B, Wang H, Zhang T, Yang L. Association of metformin use with ovarian cancer incidence and prognosis: a systematic review and meta-analysis. Int J Gynecol Cancer. 2019;29(1):140–146. doi:10.1136/ijgc-2018-000060
36. Kumar S, Meuter A, Thapa P, et al. Metformin intake is associated with better survival in ovarian cancer: a case-control study. Cancer. 2013;119(3):555–562. doi:10.1002/cncr.27706
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long Non-Coding RNAs ASB16-AS1 and AFAP1-AS1: Diagnostic, Prognostic Impact and Survival Analysis in Colorectal Cancer
Elabd NS, Soliman SE, Elhamouly MS, Gohar SF, Elgamal A, Alabassy MM, Soliman HA, Gadallah AA, Elbahr OD, Soliman G, Saleh AA
The Application of Clinical Genetics 2022, 15:97-109
Published Date: 1 August 2022
Efficacy of Bevacizumab in High-Grade Meningiomas: A Retrospective Clinical Study
Bai X, Liu X, Wen J
Neuropsychiatric Disease and Treatment 2022, 18:1619-1627
Published Date: 6 August 2022
Real-World Outcomes and Prognostic Factors Among Patients with Advanced Non-Small Cell Lung Cancer and High PD-L1 Expression Treated with Immune Checkpoint Inhibitors as First-Line Therapy
Ge W, Wu N, Jalbert JJ, Quek RGW, Liu J, Rietschel P, Pouliot JF, Harnett J, Hsu ML, Feliciano JL
Cancer Management and Research 2022, 14:3191-3202
Published Date: 16 November 2022
The Systemic Inflammation Score is Associated with the Survival of Patients with Prostate Cancer
Xie J, Xiao X, Dong Z, Wang Q
Journal of Inflammation Research 2023, 16:963-975
Published Date: 7 March 2023
Unveiling the Landscape of PD-L1 Expression and Tumor-Infiltrating Lymphocyte Subtypes in Advanced Triple-Negative Breast Cancer in Brazil
Dos Santos ALS, Da Silva JL, De Albuquerque LZ, Neto ALA, Da Silva CF, Cerva LAM, Small IA, Rodrigues FR, De Macedo FC, Marcelino CP, Batista PDM, Rego MADC, Borba MACSM, De Melo AC
Breast Cancer: Targets and Therapy 2025, 17:349-358
Published Date: 15 April 2025