Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Machine Learning-Based Prediction of Prolonged Mechanical Ventilation After Stanford Type A Aortic Dissection Surgery
Authors Wei Z, Zhou J, Li X, Liu H, Leng H, Zheng Y, Zhou S, Cheng T, Cai Z
Received 22 April 2026
Accepted for publication 21 June 2026
Published 29 June 2026 Volume 2026:19 617194
DOI https://doi.org/10.2147/JMDH.S617194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Zhanhua Wei,1,* Jiali Zhou,2,* Xing Li,1,* Huafen Liu,2 Huijun Leng,3 Yao Zheng,3 Sisi Zhou,4 Tong Cheng,1 Zhongxiang Cai1
1Department of Nursing, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 2Department of Cardiology, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 3Department of Cardiovascular Surgery, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 4Department of Cardiovascular Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhongxiang Cai, Department of Nursing, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China, Email [email protected]
Purpose: Stanford type A aortic dissection (TAAD) is a life-threatening cardiovascular emergency associated with high morbidity and mortality. Prolonged mechanical ventilation (PMV) remains a common postoperative complication and is associated with delayed recovery and increased resource use. Although several logistic regression–based prediction models for PMV after TAAD surgery have been reported, evidence comparing conventional regression with machine learning approaches remains limited. This study aimed to develop and internally validate three prediction models, namely logistic regression, support vector machine (SVM), and extreme gradient boosting (XGBoost), for assessing the risk of PMV after TAAD surgery.
Patients and Methods: A total of 511 patients with TAAD from Renmin Hospital of Wuhan University and Tongji Hospital affiliated with Tongji Medical College of Huazhong University of Science and Technology were retrospectively enrolled and randomly divided into a training set (75%) and a test set (25%). PMV was defined as invasive mechanical ventilation > 48h from the end of surgery to the first successful extubation. Risk factors for PMV were screened by univariate analysis and least absolute shrinkage and selection operator (LASSO) regression. Predictive models were then constructed using logistic regression, SVM, and XGBoost. Model performance was evaluated using AUC, sensitivity, specificity, accuracy, recall, and F1-score, and assessed by calibration curves and decision curve analysis (DCA). SHAP analysis was performed for the final model.
Results: PMV occurred in 159 patients, with an incidence of 31.1%. LASSO regression identified six predictors: preoperative lactate, cardiopulmonary bypass time, peak postoperative creatinine, postoperative plasma transfusion, lactate at the end of surgery, and pulmonary complications. In the test set, the AUCs of the SVM, logistic regression, and XGBoost models were 0.820, 0.805, and 0.784, respectively. Although SVM achieved the highest numerical AUC and showed relatively favorable calibration and clinical net benefit, the differences in AUC among the three models were not statistically significant. Therefore, SVM was selected for SHAP interpretation based on its balanced overall performance rather than statistical superiority in discrimination.
Conclusion: The three models demonstrated acceptable internal performance for predicting PMV after TAAD surgery, with SVM showing a numerically higher AUC and favorable overall performance in discrimination, calibration, and decision curve analysis. The identified predictors are clinically interpretable, and the current value of these models may mainly lie in perioperative risk stratification and postoperative dynamic assessment, thereby providing potential support for postoperative respiratory management. However, because postoperative variables were included and external validation was not performed, the findings should be interpreted as preliminary and require prospective multicenter validation before routine clinical use.
Keywords: perioperative care, respiratory management, risk stratification, machine learning, postoperative complications
Introduction
Cardiovascular diseases are the leading cause of death and disability worldwide, accounting for approximately one-third of all deaths.1 Among them, aortic dissection is a life-threatening cardiovascular emergency that often results in poor prognosis and even death.2 Aortic dissection is characterized by a tear in the aortic intima, allowing blood to enter the medial layer of the aortic wall and create a separation between the true and false lumens.3 Stanford type A aortic dissection (TAAD), which involves the ascending aorta or aortic arch, is an acute and rapidly progressing condition with a mortality rate increasing by approximately 1% per hour after onset and reaching up to 50% within 48 hours.4,5 Surgical repair remains the only definitive treatment, and although significant advancements have been achieved, patient outcomes remain poor.6 Postoperative complications are common in TAAD patients, including neurological dysfunction, acute kidney injury, and respiratory failure.7
Among these complications, the incidence of respiratory failure is as high as 51.6%, and the recovery of postoperative respiratory function directly determines the duration of mechanical ventilation.8 Prolonged mechanical ventilation (PMV) is closely associated with poor outcomes, with its incidence after TAAD surgery ranging from 28.9% to 73.3%.7,9 Studies have shown that extended mechanical ventilation may impair cardiopulmonary function, increase the burden on other organs, prolong hospitalization, raise healthcare costs, and elevate patient mortality by 2.3% to 17.0%.10,11 Therefore, accurate identification of patients at increased risk of PMV is important for perioperative risk stratification, postoperative respiratory management, and optimization of intensive care resources.
With the integration of computer science and mathematical algorithms, data processing and mining have become more efficient and accurate.12 Machine learning not only has the capacity to handle large datasets but can also extract complex and hidden relationships, thereby potentially improving the accuracy and personalization of predictions.13 These methods rely on patients’ clinical test results and monitoring data to support risk assessment and clinical decision-making.14 Support vector machine (SVM) is a high-performance supervised learning algorithm commonly used for data classification by determining the optimal hyperplane.15 This method may offer advantages when handling data in high-dimensional feature spaces and is particularly suitable for complex datasets with unclear class boundaries or nonlinear separability.16 Extreme gradient boosting (XGBoost) is characterized by its efficiency and flexibility in handling missing data and integrating weak predictive models.17 Its predictive performance and potential clinical utility can be assessed using the area under the receiver operating characteristic curve (AUC) and decision curve analysis (DCA), respectively.17 Compared with conventional logistic regression, machine learning algorithms may offer greater flexibility in capturing nonlinear relationships and complex interactions among perioperative variables. This may be relevant to PMV after TAAD surgery, because the duration of mechanical ventilation may be influenced by the combined effects of preoperative status, intraoperative factors, and postoperative conditions. However, increased model complexity does not necessarily translate into clinically meaningful improvement. Therefore, direct comparison between conventional logistic regression and machine learning models remains necessary.
Previous studies have explored risk factors and developed logistic regression–based models for delayed extubation or PMV after TAAD surgery.18–20 These studies have provided important evidence for identifying patients at increased risk, but several issues remain. First, existing studies have varied in the definition of PMV and the selection of candidate predictors, which may limit comparability and generalizability. Second, conventional regression models may have limited flexibility in capturing nonlinear relationships and complex interactions among perioperative variables. Third, direct comparisons between conventional regression and machine learning models within the same TAAD-associated PMV cohort remain limited. Evaluating discrimination alone may also be insufficient. Calibration, clinical net benefit, and model interpretability should also be considered when assessing the potential value of a prediction model.
Despite their predictive flexibility, machine learning models are often difficult to interpret. Black-box predictions may be challenging to translate into clinical practice unless clinicians can understand which variables contribute most to the predicted risk and how these variables influence model output. Explainable artificial intelligence methods, such as SHapley Additive exPlanations (SHAP), provide a way to quantify the contribution of individual predictors to model predictions, thereby improving transparency and interpretability.21
Accordingly, this two-center retrospective study aimed to: (1) investigate factors associated with PMV after TAAD surgery; and (2) develop and internally validate three prediction models, including logistic regression, support vector machine (SVM), and extreme gradient boosting (XGBoost). By comparing conventional regression with machine learning approaches using the same cohort and selected predictors, and by evaluating discrimination, calibration, decision curve analysis, and SHAP-based interpretability, this study sought to explore whether machine learning models could provide additional predictive or explanatory value for perioperative risk stratification and postoperative respiratory management. Given the inclusion of postoperative variables and the absence of external validation, the proposed models should be interpreted as preliminary tools for perioperative or postoperative dynamic risk assessment rather than as standalone early preoperative prediction models.
Material and Methods
Study Design, Participants, and Setting
Using convenience sampling, a retrospective analysis was conducted among patients diagnosed with TAAD who underwent surgery at Renmin Hospital of Wuhan University between November 2021 and November 2024, and at Tongji Hospital affiliated with Tongji Medical College of Huazhong University of Science and Technology between November 2022 and November 2024. A total of 511 patients were included in this study. The participant selection process is shown in Supplementary Figure S1. Inclusion criteria were as follows: (1) diagnosis of TAAD confirmed by aortic computed tomography angiography (CTA); (2) age ≥18 years; (3) successful completion of surgery with safe transfer to the cardiothoracic intensive care unit (ICU) for postoperative monitoring and treatment; and (4) requirement for continued mechanical ventilation after surgery. Exclusion criteria were as follows: (1) known severe preoperative respiratory diseases; (2) severe preoperative dysfunction of major organs; (3) hematologic disorders, active inflammatory diseases (such as autoimmune diseases and infections), or long-term oral glucocorticoid therapy; (4) preexisting psychiatric disorders; (5) preexisting neurological disorders; and (6) missing clinical data exceeding 10%. Ethical considerations were strictly followed throughout the study in accordance with the latest version of the Declaration of Helsinki. This study was approved by the Ethics Committee of Renmin Hospital of Wuhan University (Approval No. WDRY2025-K047) and the Ethics Committee of Tongji Hospital affiliated with Tongji Medical College of Huazhong University of Science and Technology (Approval No. TJ-IRB202504004). Due to the retrospective nature of the study, the requirement for informed consent was waived by both ethics committees. All patient data were anonymized before analysis, and personal identifying information was removed to ensure patient confidentiality throughout the study.
Baseline Data
Based on a review of the literature and preliminary group discussions, the following data were collected, including patients’ demographic characteristics, preoperative, intraoperative, and postoperative information. General demographic data included age, sex, body mass index (BMI) and smoking history. Preoperative data included time from symptom onset to surgery, white blood cell count, platelet count, blood lactate, blood glucose, D-dimer, troponin I, interleukin-6, preoperative shock, cerebral hypoperfusion, cardiac tamponade, limb ischemia, and preoperative analgesia. Intraoperative data included cardiopulmonary bypass (CPB) time, deep hypothermic circulatory arrest (DHCA), aortic cross-clamp time, blood transfusion volume, red blood cell transfusion volume, ascending aortic diameter, concomitant coronary artery bypass grafting (CABG), and other concomitant cardiac procedures. Postoperative data included serum albumin, serum creatinine, transfused plasma and platelets, stroke, and lactate level at the end of surgery.
Delphi Expert Consultation and Determination of Candidate Variables
Based on a systematic literature review, a preliminary pool of candidate predictors for PMV after surgery for TAAD was developed. Two rounds of Delphi expert consultation were subsequently conducted to refine and screen these candidate variables. A total of 15 experts from relevant fields participated in the consultation. Expert engagement was assessed by the questionnaire response rate, expert authority by the authority coefficient, and the concentration and consistency of expert opinions by the mean importance score, coefficient of variation, and Kendall’s coefficient of concordance. Items with a mean importance score <3.5 or a coefficient of variation >0.25 were considered for deletion or revision. After the first round, items were deleted, added, or revised according to expert feedback, and a second-round questionnaire was then developed. After two rounds of consultation, 30 candidate variables were retained. Subsequently, a pilot investigation was performed to further assess the availability and completeness of these variables, based on which the final set of variables for subsequent statistical analysis was determined. The Delphi process was intended to establish and optimize the candidate predictor pool rather than to serve as the final statistical selection procedure. The final retained variables were entered into the univariate analysis, and those with statistical significance were subsequently included in the LASSO regression for final predictor selection.
Diagnostic Criteria for Prolonged Mechanical Ventilation (PMV)
At present, there is no universally accepted definition of PMV after surgery for TAAD. Although the Society of Thoracic Surgeons defines prolonged postoperative mechanical ventilation as ventilation lasting more than 24h, a threshold of >48h has been more commonly used in studies on delayed extubation after aortic dissection surgery.22 Accordingly, in this study, PMV was defined as invasive mechanical ventilation lasting >48h from the end of surgery to the first successful extubation. Only the duration of the initial postoperative invasive mechanical ventilation period was included, whereas ventilation time after reintubation was excluded. Patients who underwent tracheostomy before the first successful extubation were classified as having PMV if the duration of invasive mechanical ventilation exceeded 48h. Noninvasive ventilation was not considered in the definition of PMV. Although patients were enrolled from two centers, postoperative mechanical ventilation management and extubation decisions were guided by similar clinical principles at both institutions, as detailed below. Before extubation, patients were required to meet the following criteria: hemodynamic stability, absence of active bleeding, normal body temperature, clear consciousness, adequate recovery of muscle strength, and no significant acid-base imbalance. In addition, the following respiratory parameters had to be satisfied: tidal volume >6mL/kg, respiratory rate 10–30 breaths/min, and arterial partial pressure of carbon dioxide (PaCO2) <50mmHg.7,23 Extubation was performed only after comprehensive clinical assessment by the attending physicians. Operational definitions of several study variables are provided in Supplementary Table S1.
Statistical Analysis
The required sample size was determined according to the events per variable (EPV) principle.24 The sample size for this study was determined after establishing a pool of potential influencing factors through literature review and expert consultation. Initially, 30 independent variables were identified from the literature, with 10 samples allocated per variable. According to previous studies, the incidence of delayed extubation ranged from 28.9% to 73.3%. Considering possible data inefficiency, an additional 10% was added to the estimated sample size. Thus, the required sample size was calculated as 10×30 ÷ (28.9%–73.3%) × (1 + 10%) = 450–1142. Based on this estimation, the inclusion of 511 patients in the present study met the sample size requirement. The cohort was then randomly divided into a training set and a testing set at a ratio of 7.5:2.5.
During data preprocessing, some variables contained missing values in a subset of cases. To minimize the reduction in effective sample size and information loss associated with direct deletion of incomplete cases, missing data were handled according to the proportion of missingness at the case level. Cases with a missingness proportion of ≥10% were considered to have incomplete key information and were excluded from further analysis. For cases with a missingness proportion of <10%, missing values were imputed according to variable type. Within a multiple imputation framework, continuous variables were imputed using predictive mean matching, whereas categorical variables, if missing, were imputed using logistic regression.25 No missing values were observed in categorical variables in the present study. The proportion of missingness for variables with missing data has been summarized in Supplementary Table S2. To avoid data leakage, the dataset was first divided into training and testing sets, and the imputation model as well as other preprocessing procedures were fitted using the training set only and then applied to the testing set.
Statistical analyses were performed using R version 4.4.2 and SPSS version 25.0. Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed variables are presented as mean±standard deviation (SD), and comparisons between groups were performed using the independent-samples t test. Non-normally distributed variables are expressed as median and interquartile range (IQR), and comparisons were conducted using the Mann–Whitney U-test. Categorical variables are presented as frequencies and percentages, and comparisons between groups were performed using the chi-square test or Fisher’s exact test, as appropriate. PMV after TAAD surgery was used as the outcome variable. Univariate logistic regression was performed to screen candidate variables, and variables with statistical significance in the univariate analysis were entered into least absolute shrinkage and selection operator (LASSO) regression analysis. The optimal λ value was determined by 10-fold cross-validation. All tests were two-sided, and a P value < 0.05 was considered statistically significant.
The dataset was divided into training and testing sets using the R package “caret”. Univariate logistic regression was performed using the R package “glm”, and LASSO regression was conducted using the R package “glmnet”. Model development was based on the tidymodels framework, including the “recipes”, “parsnip”, “workflows”, “tune”, “rsample”, and “yardstick” packages. Logistic regression (engine = glm), support vector machine (SVM; engine = kernlab), and extreme gradient boosting (XGBoost; engine = xgboost) models were developed separately. Five-fold cross-validation was performed using the “rsample” package, and hyperparameter tuning was conducted using the “tune” package. Model discrimination was evaluated using ROC curves, AUC, accuracy, sensitivity, specificity, recall, and F1-score. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test and calibration curves. The Hosmer-Lemeshow test was implemented using the “ResourceSelection” package, and calibration curves were generated using the “rms” package. ROC curves and DCA curves were generated using the “yardstick”, “dcurves”, and “ggplot2” packages. Interpretability analysis of the final model was performed using the “fastshap” package to calculate SHAP values and visualize variable importance. SHAP summary plots and feature importance plots were generated using “ggplot2”, and beeswarm plots were produced using the “ggbeeswarm” package.
Model development and hyperparameter tuning were performed exclusively within the training set using five-fold cross-validation, with AUC as the primary selection criterion. For the SVM model, an RBF kernel was applied, and the cost and rbf_sigma parameters were optimized using regular grid search. The search ranges were 2−5 to 25 for cost and 10−4 to 10−1 for rbf_sigma. The optimal parameter combination was cost = 32 and rbf_sigma = 0.00316, with a mean cross-validated AUC of 0.834. For the XGBoost model, random grid search was used to tune mtry, min_n, tree_depth, learn_rate, loss_reduction, and sample_size within predefined ranges. Considering that six predictors were included in the final model, the search range for mtry was restricted to 2–6. The other search ranges were min_n = 5–20, tree_depth = 1–3, learn_rate = 10−3–10−1, loss_reduction = 10−3–10°, and sample_size = 0.8–1.0.
Results
Results of the Delphi Expert Consultation
A total of 15 experts participated in two rounds of Delphi consultation, with a 100% response rate in both rounds. The expert authority coefficient was 0.848 in both rounds. The Kendall’s coefficients of concordance (W) for the two rounds were 0.417 and 0.359, respectively, both reaching statistical significance (both P < 0.001), indicating good consensus among the experts. After the first round, items were deleted, added, and revised based on the predefined screening criteria and expert feedback, and the second-round questionnaire was then developed. Following the two rounds of consultation, 30 candidate variables were generated. In the pilot investigation, interleukin-6 and intraoperative fluid balance were removed after group discussion because of excessive missing data. Finally, 28 factors were retained for subsequent statistical analysis, and all were entered into the univariate analysis. The item importance ratings and coefficients of variation in the first and second rounds of expert consultation are presented in Supplementary Tables S3 and S4.
Baseline Characteristics
A total of 511 patients were included in this study, comprising 352 in the non-prolonged mechanical ventilation (non-PMV) group and 159 in the prolonged mechanical ventilation (PMV) group, with an incidence of 31.1%. Significant differences were observed between the PMV and non-PMV groups after TAAD surgery (P < 0.05). Detailed information is presented in Table 1.
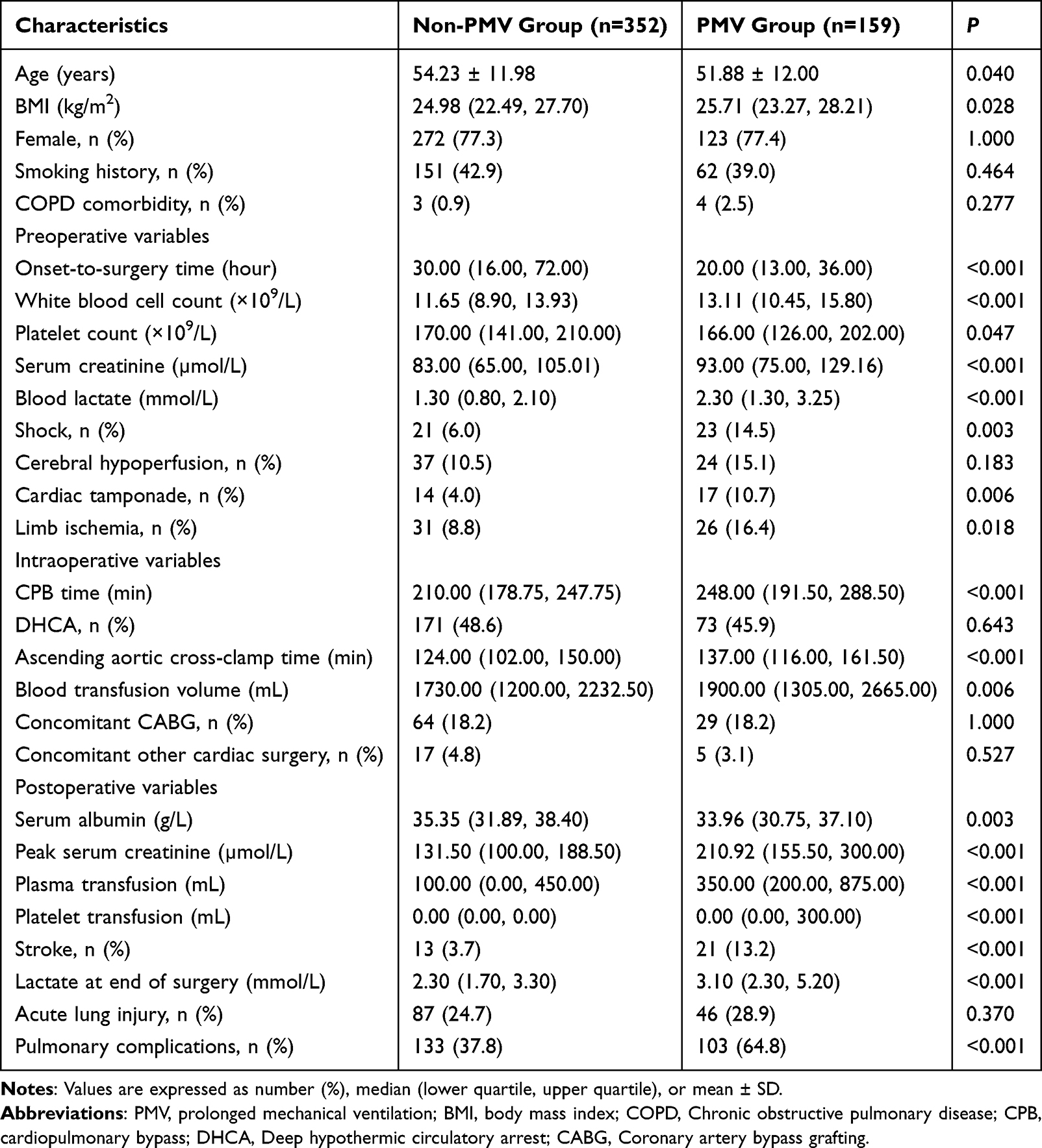 |
Table 1 Characteristics of Patients with Stanford Acute Type A Aortic Dissection |
Univariate Analysis of Variable Selection
Univariate analysis showed that onset-to-surgery time, white blood cell count, platelet count, blood lactate, shock, cardiac tamponade, limb ischemia, CPB time, ascending aortic cross-clamp time, serum albumin, peak serum creatinine, plasma transfusion, platelet transfusion, lactate at the end of surgery, and pulmonary edema or pulmonary infection comorbidity were significantly associated with PMV after surgery for TAAD (P < 0.05, Table 2).
 |
Table 2 Univariate Analysis of Risk Factors for Prolonged Mechanical Ventilation After Surgery for Stanford Type A Aortic Dissection |
LASSO Regression for Variable Selection
Fifteen variables identified as statistically significant in the univariate analysis were further analyzed using LASSO regression with 10-fold cross-validation to determine the optimal penalty parameter λ. Cross-validation identified the λ value that minimized prediction error while also considering λ within one standard error (λ.1se), thereby achieving a balance between model accuracy and predictive performance.
In this study, the final model was constructed using the λ.1se criterion (λ = 0.07191526). At this penalty level, six variables retained non-zero coefficients and were selected as predictors. These variables included preoperative blood lactate, CPB time, peak postoperative serum creatinine, postoperative plasma transfusion, lactate at the end of surgery, and pulmonary complications. The exact coefficients of these variables are presented in Supplementary Table S5. The selection process is illustrated in Figures 1 and 2.
 |
Figure 1 Feature Selection Process Using LASSO Regression. |
 |
Figure 2 Optimal Lambda Selection via Cross-Validation. |
Model Construction and Comparison of Predictive Performance
Three prediction models were constructed and compared, including logistic regression, SVM, and XGBoost. All three models were developed using the same six selected predictors. During model validation, the dataset was randomly split into a training set and a test set at a ratio of 7.5:2.5, and cross-validation was performed within the training set. The training process was repeated five times to reduce randomness. Hyperparameter combinations were determined through cross-validation and then used to train the final models.Model performance was evaluated using the area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, recall, and F1-score. Calibration curves, the Hosmer–Lemeshow test, and decision curve analysis (DCA) were used to assess model calibration and clinical net benefit. SHAP analysis was subsequently performed for the model selected for interpretation.
Tables 3 and 4 present the performance metrics of the three models in the training and test sets, respectively, including AUC, accuracy, sensitivity, specificity, recall, and F1-score. The ROC curves of the individual models are shown in Figures 3–5, and the comparative ROC curves on the test set are shown in Figure 6.
 |
Table 3 Performance of Three Models on the Training Set |
 |
Table 4 Performance of Three Models on the Test Set |
 |
Figure 3 ROC Curves of Logistic. |
 |
Figure 4 ROC Curves of SVM. |
 |
Figure 5 ROC Curves of XGBoost. |
 |
Figure 6 ROC Curves of the Three Models. |
In the test set, the SVM model achieved the numerically highest AUC, followed by logistic regression and XGBoost. However, DeLong tests showed that the differences in AUC among SVM, logistic regression, and XGBoost were not statistically significant (all P > 0.05). Detailed pairwise comparison results are presented in Supplementary Table S6.
Calibration analysis on the test set showed acceptable agreement between predicted and observed outcomes for all three models, as indicated by the Hosmer–Lemeshow test results (all P > 0.05). Logistic regression and SVM showed relatively better calibration than XGBoost (Figures 7–9). Decision curve analysis further showed that logistic regression and SVM provided a higher and more stable net benefit than XGBoost across a wide range of threshold probabilities (Figures 10–12).
 |
Figure 7 Calibration Curve of Logistic. |
 |
Figure 8 Calibration Curve of SVM. |
 |
Figure 9 Calibration Curve of XGBoost. |
 |
Figure 10 Decision Curve Analysis of Logistic. |
 |
Figure 11 Decision Curve Analysis of SVM. |
 |
Figure 12 Decision Curve Analysis of XGBoost. |
The three models showed different sensitivity-specificity profiles on the test set. XGBoost showed relatively higher sensitivity, indicating that it classified more PMV cases as high risk at the selected threshold. In contrast, SVM showed higher specificity, indicating fewer false-positive classifications. Considering discrimination, calibration, clinical net benefit, and the balance between sensitivity and specificity, the SVM model was selected for SHAP-based interpretation rather than because of a statistically significant superiority in AUC. SHAP analysis was used to further explore the contribution of each predictor to the SVM model output and to improve model transparency. The SHAP results are shown in Figures 13 and 14.
 |
Figure 13 SHAP-based Feature Importance Ranking. |
 |
Figure 14 SHAP Value Analysis of Each Feature and Their Impact on the Model Output. |
Discussion
This two-center retrospective study developed and compared three prediction models for PMV after surgery for TAAD using the same set of selected predictors. Six perioperative variables were identified through univariate analysis and LASSO regression, including preoperative blood lactate, CPB time, peak postoperative serum creatinine, postoperative plasma transfusion, lactate at the end of surgery, and pulmonary complications. These variables capture information from preoperative physiological status, intraoperative surgical burden, transfusion requirements, and postoperative organ function, reflecting the multifactorial nature of respiratory recovery after TAAD surgery. Among the three models, SVM achieved the highest numerical AUC in the test set and showed relatively balanced performance in discrimination, calibration, clinical net benefit, and specificity. Although the AUC difference among the models was not statistically significant, the direct comparison of conventional regression and machine learning approaches using the same cohort and predictor set provides useful evidence for understanding the potential role of flexible modeling strategies in PMV risk assessment after TAAD surgery.
Several previous studies have investigated PMV or delayed extubation after TAAD surgery using conventional statistical approaches. Yu et al19 conducted a retrospective analysis of 452 patients diagnosed with TAAD, identified risk factors for PMV after surgery, and constructed a logistic regression model. Luo et al18 categorized mechanical ventilation duration into <12 h, 12 h to <24 h, 24 h to <48 h, 48 h to <72 h, and ≥72 h, compared the clinical characteristics and outcomes among these groups, performed multivariate logistic regression analysis, and developed a logistic regression model. Another retrospective study collected data from 381 TAAD patients, identified nine relevant risk factors, and established a logistic regression model.20 These studies provided important evidence for risk assessment of delayed extubation or PMV after TAAD surgery. Compared with previous regression-based studies, the present study evaluated logistic regression, SVM, and XGBoost within the same analytical framework and further assessed discrimination, calibration, decision curve analysis, and SHAP-based interpretability. This approach allows a more comprehensive evaluation of model performance and transparency than discrimination-based assessment alone.
Postoperative plasma transfusion was selected as one of the predictors associated with PMV. Surgery for TAAD is typically complex and prolonged, and many patients require postoperative transfusion of blood products to maintain circulation, correct coagulation abnormalities, and manage anemia.26 The association between plasma transfusion and PMV may reflect greater surgical complexity, bleeding tendency, coagulation dysfunction, or more severe perioperative illness. In addition, transfusion-related inflammatory responses may contribute to postoperative pulmonary dysfunction. The “two-hit” hypothesis is widely used to explain transfusion-related acute lung injury.27 According to this hypothesis, blood components may directly or indirectly activate neutrophils, injure pulmonary capillary endothelium, and promote acute lung injury. During blood storage, changes in red blood cell function, electrolyte imbalance, coagulation abnormalities, platelet aggregation, and inflammatory mediator release may further affect pulmonary and systemic responses.28,29 Previous studies have suggested that autologous blood transfusion may improve short-term outcomes in TAAD repair and reduce postoperative mechanical ventilation time and hospital stay.30 These findings support the importance of refined perioperative transfusion management in patients undergoing TAAD surgery.
Prolonged CPB time was also associated with PMV after TAAD surgery, which is consistent with previous research.23 Compared with other major cardiac surgeries, aortic dissection procedures are associated with longer CPB durations.31 During CPB, inflammatory cells, including neutrophils and lymphocytes, may be activated, leading to the release of inflammatory mediators and amplification of systemic inflammatory responses. These responses are associated with postoperative dysfunction of organs such as the heart, lungs, and kidneys.32 Increased pulmonary vascular permeability and peripheral vascular resistance during CPB may also contribute to lung tissue injury, pulmonary edema, hypoxemia, and multi-organ dysfunction.33 Studies have shown that the use of hemoperfusion devices during CPB can effectively attenuate the intraoperative systemic inflammatory response and reduce the risk of lung tissue injury.34 Therefore, optimization of CPB management, reduction of unnecessary CPB duration, and application of lung-protective strategies may be clinically relevant for postoperative respiratory management in TAAD patients.
Postoperative pulmonary complications, such as pulmonary infection, pulmonary edema, and atelectasis, are common after cardiac surgery.35 Patients with TAAD are particularly susceptible to these complications due to factors such as surgical techniques, anesthesia protocols, and the use of blood products, especially the application of CPB.35 These complications can impair gas exchange, worsen oxygenation, and delay weaning from mechanical ventilation.36 In addition, microbubbles or microthrombi generated during CPB may enter the pulmonary circulation, obstruct the pulmonary microvascular bed, and cause ventilation-perfusion mismatch, thereby further compromising oxygenation.37 Moreover, cold saline infusion into the pericardial cavity during cardiac arrest may injure the phrenic nerve, resulting in postoperative diaphragmatic elevation or paralysis and further impairing pulmonary ventilation.38 Previous studies have shown that patients who develop pulmonary complications after TAAD surgery require significantly longer durations of mechanical ventilation.39 In this study, the identification of pulmonary complications as an important predictor highlights the need for early postoperative pulmonary assessment, prevention of infection, optimization of fluid balance, and timely respiratory support.
Lactate is commonly used to assess tissue perfusion and cellular metabolic status. Elevated preoperative lactate levels in patients with TAAD may be associated with cardiac dysfunction, inadequate tissue perfusion, or organ failure, all of which can contribute to the development of PMV after surgery.40,41 Xie et al20 also reported that elevated preoperative lactate is a risk factor for PMV, consistent with the findings of this study. Therefore, timely correction of acid–base imbalance and maintenance of normal lactate levels in such patients may help reduce the risk of PMV.
Serum creatinine, an important biochemical marker reflecting glomerular filtration function, is widely used in clinical practice to assess and monitor renal function status.42 Elevated postoperative serum creatinine may lead to renal insufficiency or even renal failure. Renal dysfunction disrupts normal metabolic homeostasis, resulting in the accumulation of nitrogenous metabolites such as creatinine in the body. These metabolic disturbances can further trigger pulmonary inflammatory responses, promote the development of hypoxemia, and ultimately contribute to PMV.43 On the other hand, injury to vital organs such as the kidneys can disrupt water and electrolyte balance, leading to severe postoperative hypoxemia and consequently PMV.44 Therefore, postoperative fluid management should be optimized, including balancing therapeutic factors and patient-related parameters such as urine output and fluid infusion, to maintain overall fluid homeostasis and preserve renal function.
This study confirmed that elevated lactate levels at the end of surgery are a risk factor for PMV after TAAD, consistent with previous findings.7 Hyperlactatemia frequently occurs during cardiac surgery and can lead to postoperative complications such as prolonged mechanical ventilation and increased risk of mortality.45,46 The development of hyperlactatemia may be associated with the interplay of multiple intraoperative factors, including impaired renal function, anesthesia management strategies, and the effects of CPB. Meanwhile, persistent postoperative organ hypoperfusion and hypoxia may further exacerbate lactate accumulation.46 Therefore, future perioperative management should emphasize dynamic monitoring of serum lactate levels and optimization of circulatory and oxygen metabolic support to help reduce postoperative mechanical ventilation time.
From a modeling perspective, this study also illustrates the balance between predictive flexibility and clinical interpretability. SVM and XGBoost may capture nonlinear relationships and complex feature interactions, whereas logistic regression is simpler, more transparent, and easier to interpret. In the present study, logistic regression showed performance close to that of SVM, while SVM demonstrated the highest numerical AUC and relatively balanced overall performance. These findings suggest that model selection should not rely solely on AUC, but should also consider calibration, clinical net benefit, sensitivity-specificity balance, interpretability, and feasibility of implementation. SHAP analysis was incorporated to improve the transparency of the SVM model by quantifying the contribution of each predictor to model output. Although the SHAP results did not aim to establish new biological mechanisms, they provide a clinically understandable explanation of how the selected variables contributed to PMV risk estimation in this cohort.
An important feature of the present model is that the final predictors included preoperative, intraoperative, and postoperative variables. The postoperative variables included in the model were recorded before the confirmation of delayed extubation or PMV; therefore, they were not derived from information obtained after outcome determination. This temporal relationship supports the use of the model for dynamic reassessment of respiratory risk during the perioperative and early postoperative period. Rather than serving as a purely preoperative prediction model, the proposed model may be more appropriately positioned as a perioperative or postoperative dynamic risk assessment tool, particularly for supporting risk evaluation before extubation decisions and for guiding postoperative respiratory management.
In future clinical practice, after adequate external validation, such a model could potentially be embedded into an electronic medical record system or ICU information platform. After early postoperative laboratory results and complication assessments become available, the model could generate updated PMV risk estimates and assist clinicians in identifying patients who may benefit from closer monitoring, individualized ventilatory strategies, or early multidisciplinary intervention. Different thresholds may be selected according to the intended clinical purpose: lower thresholds may be useful for screening patients requiring closer observation, whereas higher thresholds may help reduce false-positive alerts and unnecessary interventions. This workflow-oriented application may provide a practical direction for translating prediction models into postoperative ICU management.
In summary, this study developed and internally validated three prediction models for PMV after TAAD surgery and compared their performance using the same predictor set. The SVM model showed the highest numerical AUC and relatively balanced performance. The incorporation of SHAP analysis enhanced model interpretability and provided insight into the contribution of perioperative variables to PMV risk estimation. These findings support the feasibility of using prediction models for perioperative or postoperative dynamic risk assessment after TAAD surgery. Further external validation and prospective multicenter studies are needed before clinical implementation.
Limitation
Despite its strengths, this study has several limitations. First, as a retrospective study, it may be subject to missing data, selection bias, and residual confounding, which could affect the reliability of the results. Second, although data from 511 participants across two hospitals were included, the sample size remained relatively limited and no large-scale dataset was available. In particular, while the sample size was justified based on the events-per-variable (EPV) principle, the number of outcome events may still have been relatively limited for more complex machine learning models such as XGBoost. This may increase the risk of model instability and overfitting. Although five-fold cross-validation, hyperparameter tuning within the training set, and an independent test set were used to reduce overfitting, the robustness of the models still requires further evaluation in larger external cohorts. In addition, the relatively better performance of XGBoost in the training set but lower performance in the test set suggests that overfitting cannot be completely excluded. Third, although stratified sampling was used to preserve a similar outcome distribution between the training and test sets, no dedicated class-imbalance handling strategy, such as class weighting, oversampling, undersampling, or SMOTE, was applied during model development. Given that the PMV incidence was 31.1%, the class imbalance was moderate rather than severe. However, its potential influence on threshold-dependent performance metrics, particularly sensitivity and specificity, cannot be completely excluded. Fourth, the present study performed internal validation only and lacked external validation using geographically or temporally independent cohorts; therefore, the generalizability of the models to other institutions or populations remains to be further confirmed. Fifth, the final model included several postoperative variables, including postoperative pulmonary complications, peak postoperative serum creatinine, and lactate at the end of surgery, which were assessed after surgery but before confirmation of PMV. Although these variables were collected before the study endpoint and were intended to support peri-extubation or early postoperative risk reassessment, their temporal proximity to prolonged mechanical ventilation may limit causal interpretation and reduce the applicability of the model for a true early prediction scenario based solely on preoperative and intraoperative information. Future studies should adopt prospective, multicenter designs with larger sample sizes and external validation, and may also incorporate additional machine learning algorithms, imbalance-adjustment strategies, and separate models restricted to preoperative and intraoperative variables to further improve predictive performance, robustness, and clinical applicability.
Conclusion
This study developed and compared logistic regression, SVM, and XGBoost models for predicting PMV after surgery for TAAD. The models showed acceptable internal predictive performance within the present dataset, with supportive evidence from discrimination, calibration, and decision curve analyses. SVM achieved the highest numerical AUC and showed relatively balanced overall performance. Given the inclusion of postoperative variables, these models should be interpreted as perioperative or postoperative dynamic risk assessment tools rather than standalone early preoperative prediction models. External validation and prospective multicenter studies are required before clinical implementation.
Acknowledgments
We thank all the individuals who participated in this study.
Funding
This study was approved by the Wuhan University Clinical Nursing Master’s Research Cultivation Fund Project (LCHL202316).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–19. doi:10.1016/j.jacc.2020.11.010
2. Evangelista A, Isselbacher EM, Bossone E, et al. Insights from the international registry of acute aortic dissection: a 20-year experience of collaborative clinical research. Circulation. 2018;137:1846–1860. doi:10.1161/CIRCULATIONAHA.117.031264
3. Hagan PG, Nienaber CA, Isselbacher EM, et al. The international registry of acute aortic dissection (IRAD): new insights into an old disease. JAMA. 2000;283:897–903. doi:10.1001/jama.283.7.897
4. Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the international registry of acute aortic dissection. J Am Coll Cardiol. 2015;66:350–358. doi:10.1016/j.jacc.2015.05.029
5. Milewicz DM, Ramirez F. Therapies for thoracic aortic aneurysms and acute aortic dissections. Arterioscler Thromb Vasc Biol. 2019;39:126–136. doi:10.1161/ATVBAHA.118.310956
6. Elsayed RS, Cohen RG, Fleischman F, et al. Acute type a aortic dissection. Cardiol Clin. 2017;35:331–345. doi:10.1016/j.ccl.2017.03.004
7. Jin M, Ma WG, Liu S, et al. Predictors of prolonged mechanical ventilation in adults after acute type-a aortic dissection repair. J Cardiothorac Vasc Anesth. 2017;31:1580–1587. doi:10.1053/j.jvca.2017.03.036
8. Wan JH, Li XS, Han C, et al. Research progress on nursing interventions for acute respiratory dysfunction after surgery in patients with type A aortic dissection. Chin J Nurs. 2020;55(4):553–557. doi:10.3761/j.issn.0254-1769.2020.04.018
9. Fan FD, Zhou Q, Ge M, et al. Analysis of risk factors for delayed tracheal extubation after surgery for Stanford type A aortic dissection. J Cardiovasc Surg. 2014;4:181–184. doi:10.3760/cma.j.issn.1674-1588.2014.04.008
10. Clendenen N, Weitzel N. Predictors of prolonged mechanical ventilation in adults after acute type-a aortic dissection repair-implications for the future. J Cardiothorac Vasc Anesth. 2017;31:1562–1563. doi:10.1053/j.jvca.2017.05.022
11. Wang D, Abuduaini X, Huang X, et al. Development and validation of a risk prediction model for postoperative pneumonia in adult patients undergoing Stanford type a acute aortic dissection surgery: a case control study. J Cardiothorac Surg. 2022;17:22. doi:10.1186/s13019-022-01769-y
12. Bulten W, Balkenhol M, Belinga JA, et al. Artificial intelligence assistance significantly improves gleason grading of prostate biopsies by pathologists. Mod Pathol. 2021;34:660–671. doi:10.1038/s41379-020-0640-y
13. Zhang S, Bamakan S, Qu Q, et al. Learning for personalized medicine: a comprehensive review from a deep learning perspective. IEEE Rev Biomed Eng. 2019;12:194–208. doi:10.1109/RBME.2018.2864254
14. Han B, Chen H, Yao Y, et al. Genetic and non-genetic factors associated with the phenotype of exceptional longevity & normal cognition. Sci Rep. 2020;10:19140. doi:10.1038/s41598-020-75446-2
15. Rezvani S, Wu J. Handling multi-class problem by intuitionistic fuzzy twin support vector machines based on relative density information. IEEE Trans Pattern Anal Mach Intell. 2023;45:14653–14664. doi:10.1109/TPAMI.2023.3310908
16. Davenport MA, Baraniuk RG, Scott CD. Tuning support vector machines for minimax and neyman-Pearson classification. IEEE Trans Pattern Anal Mach Intell. 2010;32:1888–1898. doi:10.1109/TPAMI.2010.29
17. Hou N, Li M, He L, et al. Predicting 30-days mortality for MIMIC-III patients with sepsis-3: a machine learning approach using XGboost. J Transl Med. 2020;18:462. doi:10.1186/s12967-020-02620-5
18. Yuanxi L, Li Z, Jiang X, et al. A novel nomogram for predicting prolonged mechanical ventilation after acute type a aortic dissection surgery: a retrospective study investigating the impact of ventilation duration on postoperative outcomes. Ann Med. 2024;56:2392871. doi:10.1080/07853890.2024.2392871
19. Yu Y, Wang Y, Deng F, et al. Construction of a nomogram risk prediction model for prolonged mechanical ventilation in patients following surgery for acute type a aortic dissection. Front Cardiovasc Med. 2024;11:1335552. doi:10.3389/fcvm.2024.1335552
20. Xie LF, Han X, Xie YL, et al. A predictive model for prolonged mechanical ventilation after triple-branched stent graft for acute type a aortic dissection. J Surg Res. 2024;296:66–77. doi:10.1016/j.jss.2023.12.007
21. Nohara Y, Matsumoto K, Soejima H, et al. Explanation of machine learning models using shapley additive explanation and application for real data in hospital. Comput Methods Programs Biomed. 2022;214:106584. doi:10.1016/j.cmpb.2021.106584
22. Diaz-Castrillon CE, Brown JA, Navid F, et al. The impact of prolonged mechanical ventilation after acute type a aortic dissection repair. J Thoracic Cardiovasc Surg. 2024;167:1672–1679. doi:10.1016/j.jtcvs.2022.07.007
23. Ge M, Wang Z, Chen T, et al. Risk factors for and outcomes of prolonged mechanical ventilation in patients received DeBakey type i aortic dissection repairment. J Thorac Dis. 2021;13:735–742. doi:10.21037/jtd-20-2736
24. Wynants L, Bouwmeester W, Moons KG, et al. A simulation study of sample size demonstrated the importance of the number of events per variable to develop prediction models in clustered data. J Clin Epidemiol. 2015;68:1406–1414. doi:10.1016/j.jclinepi.2015.02.002
25. Heymans MW, Twisk JWR. Handling missing data in clinical research. J Clin Epidemiol. 2022;151:185–188. doi:10.1016/j.jclinepi.2022.08.016
26. Xie Q, Li C, Zhong Y, et al. Blood transfusion predicts prolonged mechanical ventilation in acute Stanford type a aortic dissection undergoing total aortic arch replacement. Front Cardiovasc Med. 2022;9:832396. doi:10.3389/fcvm.2022.832396
27. Tung JP, Chiaretti S, Dean MM, et al. Transfusion-related acute lung injury (TRALI): potential pathways of development, strategies for prevention and treatment, and future research directions. Blood Rev. 2022;53:100926. doi:10.1016/j.blre.2021.100926
28. Semple JW, Rebetz J, Kapur R. Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood. 2019;133:1840–1853. doi:10.1182/blood-2018-10-860809
29. Cho MS, Modi P, Sharma S. Transfusion-related acute lung injury. Blood. 2025;105(6):2266–2273.
30. Norton EL, Kim KM, Fukuhara S, et al. Autologous blood transfusion in acute type a aortic dissection decreased blood product consumption and improved postoperative outcomes. JTCVS Open. 2022;12:20–29. doi:10.1016/j.xjon.2022.07.005
31. Uimonen M, Olsson C, Jeppsson A, et al. Cardiopulmonary bypass time during surgery for acute type a aortic dissection and mid-term survival. J Cardiovasc Dev Dis. 2025;12. doi:10.3390/jcdd12040139
32. Jufar AH, Lankadeva YR, May CN, et al. Renal and cerebral hypoxia and inflammation during cardiopulmonary bypass. Compr Physiol. 2021;12:2799–2834. doi:10.1002/cphy.c210019
33. Pak O, Sydykov A, Kosanovic D, et al. Lung ischaemia-reperfusion injury: the role of reactive oxygen species. Adv Exp Med Biol. 2017;967:195–225. doi:10.1007/978-3-319-63245-2_12
34. Yang J, Ji D, Zhu YQ, et al. Hemoperfusion with HA380 in acute type a aortic dissection patients undergoing aortic arch operation (HPAO): a randomized, controlled, double-blind clinical trial. Trials. 2020;21:954. doi:10.1186/s13063-020-04858-2
35. Fischer MO, Brotons F, Briant AR, et al. Postoperative pulmonary complications after cardiac surgery: the VENICE international cohort study. J Cardiothorac Vasc Anesth. 2022;36:2344–2351. doi:10.1053/j.jvca.2021.12.024
36. Nguyen LS, Estagnasie P, Merzoug M, et al. Low tidal volume mechanical ventilation against no ventilation during cardiopulmonary bypass in heart surgery (MECANO): a randomized controlled trial. Chest. 2021;159:1843–1853. doi:10.1016/j.chest.2020.10.082
37. Ding X, Zha T, Abudurousuli G, et al. Effects of regional cerebral oxygen saturation monitoring on postoperative cognitive dysfunction in older patients: a systematic review and meta-analysis. BMC Geriatr. 2023;23:123. doi:10.1186/s12877-023-03804-6
38. Laghlam D, Naudin C, Srour A, et al. Persistent diaphragm dysfunction after cardiac surgery is associated with adverse respiratory outcomes: a prospective observational ultrasound study. Can J Anaesth. 2023;70:228–236. doi:10.1007/s12630-022-02360-8
39. Chen P, Li H, Liu C, et al. Postoperative pulmonary complications in acute type a aortic dissection. BMC Surg. 2025;25:318. doi:10.1186/s12893-025-03062-w
40. Garcia-Alvarez M, Marik P, Bellomo R. Stress hyperlactataemia: present understanding and controversy. Lancet Diabetes Endocrinol. 2014;2:339–347. doi:10.1016/S2213-8587(13)70154-2
41. Garcia-Alvarez M, Marik P, Bellomo R. Sepsis-associated hyperlactatemia. Crit Care. 2014;18:503. doi:10.1186/s13054-014-0503-3
42. Jiang B, Zhen G, Yang H, et al. Normalization of elevated preoperative serum creatinine and acute kidney injury after cardiac surgery: a retrospective cohort study. Sci Rep. 2025;15:27933. doi:10.1038/s41598-025-13719-4
43. Marchiset A, Jamme M. When the renal (function) begins to fall: a mini-review of acute kidney injury related to acute respiratory distress syndrome in critically ill patients. Front Nephrol. 2022;2:877529. doi:10.3389/fneph.2022.877529
44. Sheng W, Yang HQ, Chi YF, et al. Independent risk factors for hypoxemia after surgery for acute aortic dissection. Saudi Med J. 2015;36:940–946. doi:10.15537/smj.2015.8.11583
45. Hajjar LA, Almeida JP, Fukushima JT, et al. High lactate levels are predictors of major complications after cardiac surgery. J Thorac Cardiovasc Surg. 2013;146:455–460. doi:10.1016/j.jtcvs.2013.02.003
46. Haanschoten MC, Kreeftenberg HG, Arthur BR, et al. Use of postoperative peak arterial lactate level to predict outcome after cardiac surgery. J Cardiothorac Vasc Anesth. 2017;31:45–53. doi:10.1053/j.jvca.2016.04.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Machine Learning Model Based on Health Records for Predicting Recurrence After Microwave Ablation of Hepatocellular Carcinoma
An C, Yang H, Yu X, Han Z, Cheng Z, Liu F, Dou J, Li B, Li Y, Li Y, Yu J, Liang P
Journal of Hepatocellular Carcinoma 2022, 9:671-684
Published Date: 28 July 2022
Machine Learning-Based Predictive Modeling of Diabetic Nephropathy in Type 2 Diabetes Using Integrated Biomarkers: A Single-Center Retrospective Study
Zhu Y, Zhang Y, Yang M, Tang N, Liu L, Wu J, Yang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1987-1997
Published Date: 10 May 2024
A Mortality Risk Prediction Model for Septic Shock in Patients Aged ≥50: Role of Norepinephrine Index and Procalcitonin
Li XL, Mi T, Liu C, Feng M
International Journal of General Medicine 2025, 18:3045-3062
Published Date: 10 June 2025
Risk-Stratified Postoperative Follow-Up After Uncomplicated Cataract Surgery: Real-World Outcomes and Implications for Remote Care
Bratos Rubio P, Arnalich Montiel F, Mingo-Botin D, Muñoz Negrete FJ
Clinical Ophthalmology 2026, 20:597819
Published Date: 1 April 2026
Machine Learning Model Predicts New-Onset Lower Extremity Deep Vein Thrombosis After Pelvic Fracture Surgery and Targeted Diagnosis
Fu H, Dong Q, Li G, Zhao K, Hou Z
Clinical Epidemiology 2026, 18:590414
Published Date: 7 May 2026