Back to Journals » Clinical Ophthalmology » Volume 20
Risk-Stratified Postoperative Follow-Up After Uncomplicated Cataract Surgery: Real-World Outcomes and Implications for Remote Care
Authors Bratos Rubio P ![]() , Arnalich-Montiel F, Mingo-Botin D, Muñoz Negrete FJ
, Arnalich-Montiel F, Mingo-Botin D, Muñoz Negrete FJ ![]()
Received 21 January 2026
Accepted for publication 5 March 2026
Published 1 April 2026 Volume 2026:20 597819
DOI https://doi.org/10.2147/OPTH.S597819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Pablo Bratos Rubio,1,2,* Francisco Arnalich-Montiel,1– 3,* David Mingo-Botin,1,2 Francisco J Muñoz Negrete1– 3
1Department of Ophthalmology, Ramón Y Cajal University Hospital, Madrid, Spain; 2Instituto Ramón y Cajal de Investigación Sanitaria (IRYCIS), Madrid, Spain; 3Department of Ophthalmology, Universidad de Alcalá, Madrid, Spain
*These authors contributed equally to this work
Correspondence: Pablo Bratos Rubio, Department of Ophthalmology, Ramón Y Cajal University Hospital, Ctra. de Colmenar Viejo km 9.1, Madrid, 28034, Spain, Tel +34 692398444, Email [email protected]
Background: To evaluate the clinical value of postoperative examinations at 24 hours and 30 days following uncomplicated phacoemulsification, and to identify subgroups who may safely benefit from remote or simplified follow-up pathways.
Methods: A retrospective observational study was conducted, including all patients who underwent uncomplicated phacoemulsification at a high-volume tertiary public hospital during September 2024. Demographic data, ophthalmologic history, surgical characteristics, day-1 and day-30 findings, visual outcomes, and emergency visits were extracted from electronic medical records. Postoperative complications associations were evaluated using bivariate tests and multivariate binomial logistic regression.
Results: Of 296 patients, the most common 24-hour complication was transient intraocular pressure elevation (13.2%). Overall, 20.9% showed a postoperative finding on day 1, and 14.2% required unplanned reassessment. At 30 days, complications occurred in 6.7% of cases, mainly cystoid macular edema (3.6%). In multivariate analysis, 24-hour complications (P=0.028) and ophthalmologic comorbidities (P=0.010) independently predicted 30-day complications. Patients without ophthalmologic history, without 24-hour complications, and with early visual improvement had a markedly lower risk of adverse outcomes. Applying a risk-based follow-up strategy could reduce approximately 50% of routine 30-day in-person reviews and relieve up to 300 hours of annual clinical workload.
Conclusion: This risk-stratified postoperative model may improve service efficiency in high-volume public hospitals, support the sustainability of ophthalmic care, and may be transferable to other public health systems. Low-risk patients could be safely monitored remotely without compromising clinical outcomes. Prospective studies are required to confirm these findings.
Keywords: cataract, phacoemulsification, postoperative complications, follow-up, telemedicine, risk stratification
Introduction
Cataract surgery is one of the most frequently performed surgical procedures worldwide. The increasing prevalence of cataracts associated with demographic ageing has intensified the workload of ophthalmology departments, particularly in public healthcare systems such as Spain’s. Advances in phacoemulsification techniques have substantially improved surgical safety, reduced recovery times, and minimized the incidence of severe postoperative complications. Nevertheless, postoperative follow-up protocols remain variable and resource demanding.1,2
International clinical guidelines show considerable heterogeneity. The American Academy of Ophthalmology (AAO) recommends an early examination within the first 48 hours, followed by refractive evaluation during the first postoperative month.3 Conversely, the European Society of Cataract and Refractive Surgeons (ESCRS) and the Royal College of Ophthalmologists (RCOphth) consider that a mandatory in-person review at 24 hours is not always necessary in the absence of intraoperative complications and may be replaced by structured telephone calls or telemedicine-based assessments conducted by ophthalmologists, optometrists, or trained nurses.4 Likewise, the second monthly follow-up visit may be performed in person or remotely and does not necessarily require the direct participation of a specialist.5
The growing adoption of telemedicine across multiple medical fields, together with the need to alleviate clinical burden, has stimulated interest in alternative follow-up strategies after cataract surgery.6 However, evidence supporting these approaches is limited, particularly in patients with pre-existing ocular disease or other risk factors, who are often excluded from clinical trials.7,8 Although the absence of ocular comorbidities and intraoperative complications is generally considered indicative of a low-risk profile, this definition relies mainly on expert consensus and trial exclusion criteria, with limited evidence supporting structured risk-stratified follow-up pathways.3,8 Real-world data from tertiary hospitals are therefore essential to determine whether a risk-stratified postoperative pathway can maintain patient safety while optimizing resource allocation.
This study evaluates the utility of 24-hour and 30-day postoperative examinations after uncomplicated phacoemulsification, identifies predictors of early and late complications, and explores whether selected patient profiles could be safely managed with remote or simplified follow-up strategies. We hypothesized that absence of ophthalmologic comorbidity, absence of 24-hour complications, and early visual improvement would identify a low-risk group in whom routine 30-day in-person review could potentially be simplified or replaced by remote follow-up.
Materials and Methods
This retrospective observational study was conducted at a tertiary public academic center in Madrid, Spain. All consecutive patients who underwent cataract surgery between 1 and 30 September 2024 were screened. Eligible cases were those in which standard phacoemulsification with intraocular lens implantation was completed without intraoperative complications. Intraoperative complications included posterior capsule rupture, vitreous loss, zonular dialysis, or other unplanned events requiring deviation from standard phacoemulsification. Combined glaucoma or retinal surgery and procedures with any intraoperative complications were excluded. Patients lacking complete postoperative evaluations at 24 hours or 30 days were also excluded.
Data were obtained from the hospital’s electronic medical record system and anonymized before analysis. The study received approval from the Institutional Review Board and the Institutional Ethics Committee. The study was conducted in accordance with the Declaration of Helsinki. Extracted variables included demographic characteristics, systemic comorbidities, and relevant ophthalmologic history such as glaucoma, pseudoexfoliation, pathological myopia, age-related macular degeneration, or previous vitreoretinal or glaucoma surgery. Surgical details included the operated eye (first or second), cataract density according to the LOCS III classification, level of surgeon experience (resident or attending), and intraocular lens type and power. Standard practice at our center includes postoperative examinations at 24 hours and 30 days, along with a regimen of topical antibiotics and a tapering course of topical corticosteroids. Postoperative information included reported symptoms at 24 hours and 30 days, intraocular pressure (IOP) measurements, best corrected visual acuity before surgery and at both follow-ups, incision integrity, and documented complications. The need for unplanned reviews, emergency visits, surgical re-intervention, and the final postoperative status (discharge, continuation in routine follow-up, or referral to specialized clinics) was also recorded. Clinically significant complications were defined as those requiring a change in postoperative treatment. Early IOP elevation was defined as IOP >26 mmHg at 24 hours and late IOP elevation as IOP >21 mmHg at 30 days, based on our institutional protocols and current literature;9 cystoid macular edema was diagnosed based on OCT findings.
Descriptive statistics were used to summarize the dataset. Categorical variables were expressed as absolute numbers and percentages, while continuous variables were described using means and standard deviations. Associations between clinical variables and postoperative complications were evaluated using chi-square tests for categorical variables and Student’s t-test or one-way ANOVA for continuous variables, depending on distribution normality determined by the Kolmogorov–Smirnov test. Multivariate binomial logistic regression was conducted to identify variables independently associated with 30-day complications, incorporating those clinical factors most likely to influence postoperative outcomes based on univariate results (P < 0.05) or strong clinical rationale. Statistical significance was set at p < 0.05. All statistical analyses were performed using SPSS (IBM Corp., Armonk, NY).
Results
A total of 296 patients fulfilled the inclusion criteria (Table 1). The mean age was 75.5 ± 8.3 years, and 65.8% were women. Systemic hypertension was the most prevalent comorbidity. Among male patients, 28 individuals (9.5%) were receiving treatment for prostatic disease. Regarding ophthalmologic conditions, 6.4% had glaucoma, 6.1% had pathological myopia, 3.7% had exudative age-related macular degeneration, and 3.5% presented pseudoexfoliation syndrome. Seven operated eyes had undergone previous vitrectomy, and two had previously undergone non-penetrating deep sclerectomy. Surgical activity was balanced between the first and second eyes, and residents performed 44.6% of the cases under direct supervision. Cataract density was predominantly nuclear, with a mean LOCS III scale density of 2.76, and the mean intraocular lens power implanted was 20.9 diopters.
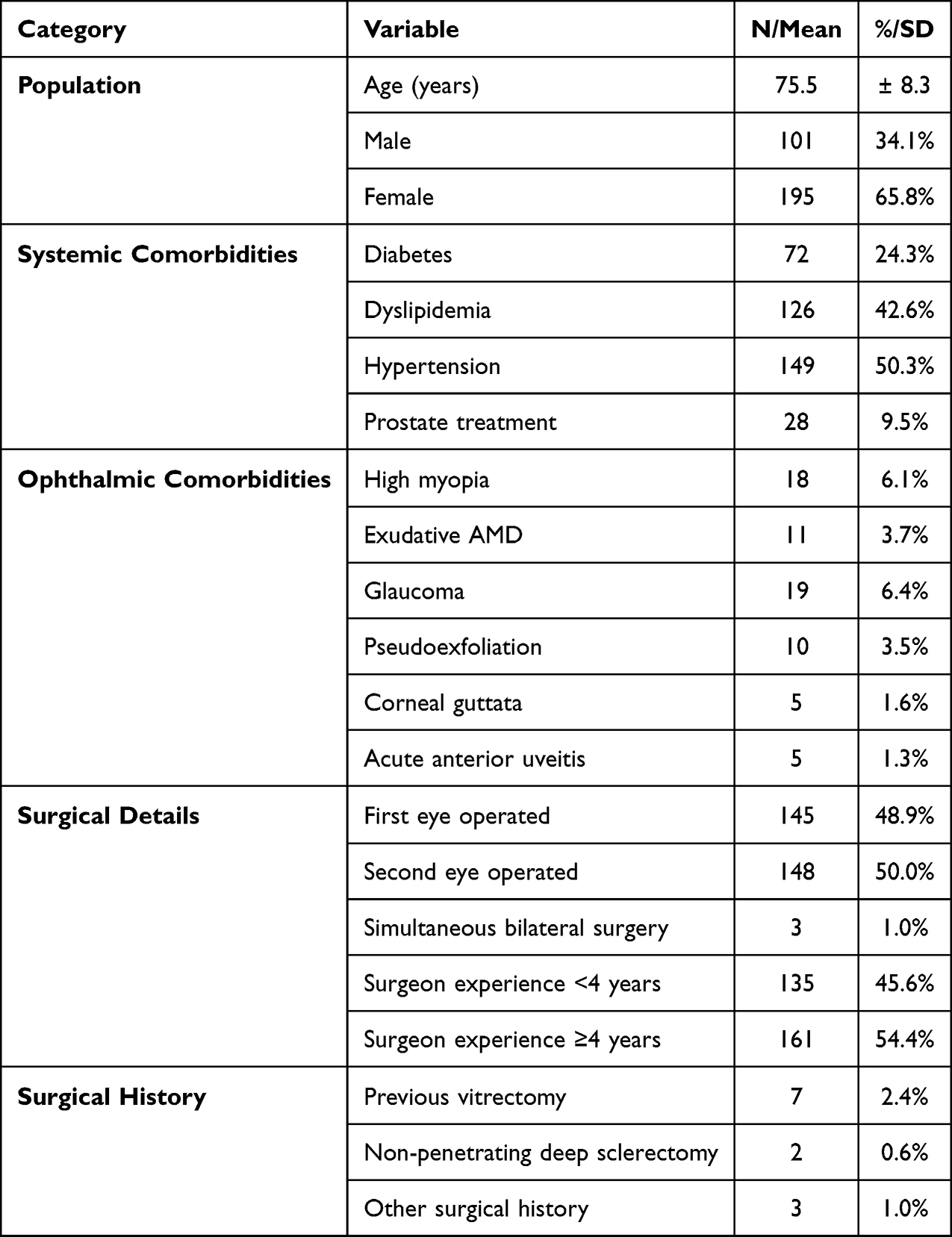 |
Table 1 Baseline Characteristics and Surgical Details |
At the 24-hour assessment, eleven patients reported symptoms such as ocular pain, blurred vision, or foreign body sensation (Table 2). Seven of the symptomatic patients exhibited postoperative complications, with a mean intraocular pressure of 37 mmHg. Transient IOP elevation was the most frequent objective finding. IOP spikes >26 mmHg occurred in 13.2% of eyes (n=39). The overall mean IOP at the 24-hour visit (including uncomplicated cases) was 20.75 ± 1.8 mmHg. Corneal incision leakage occurred in 5.7% of eyes; all were managed conservatively and showed good clinical evolution. Altogether, 20.9% of eyes presented at least one postoperative finding at 24 hours, and 14.2% of patients required a scheduled unplanned in-person reassessment, most commonly due to IOP spikes. Two patients required surgical re-intervention: one for haptic reposition and the other for retained cortex removal. Pseudoexfoliation syndrome was the only preoperative factor significantly associated with higher intraocular pressure at 24 hours (p = 0.046). No statistically significant differences in early complications were observed between surgeries performed by residents and those conducted by attending surgeons.
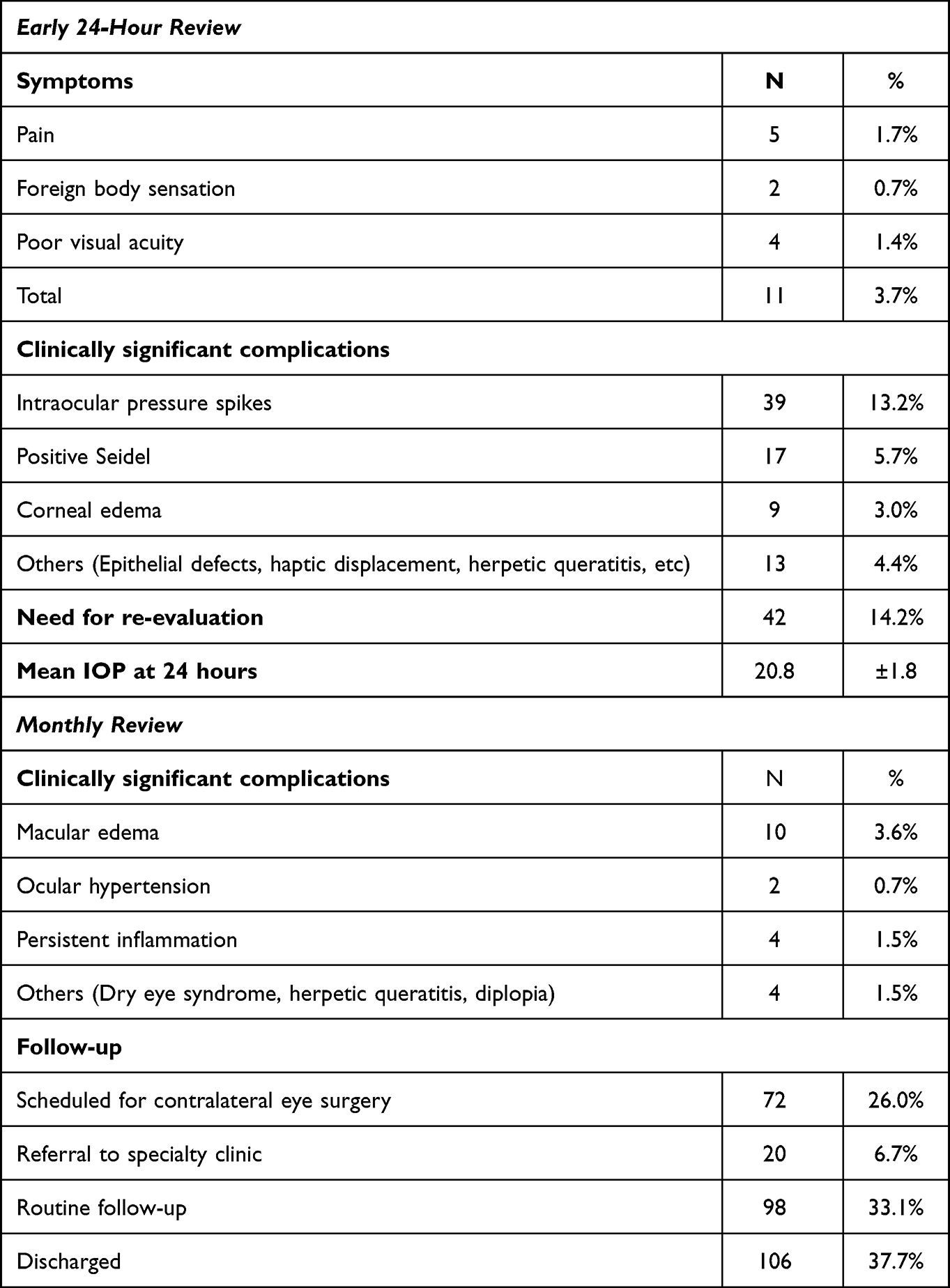 |
Table 2 Postoperative Reviews |
At the 30-day evaluation, postoperative complications were observed in 6.7% of eyes. Cystoid macular edema occurred in 3.6% of cases and was the most frequent late complication, followed by persistent inflammation in 4 eyes and elevated IOP in 2 eyes. By this time point, 37.7% of patients were discharged from follow-up, 33.1% continued routine care, and 6.7% were referred to specialized ophthalmology clinics. Visual outcomes were favorable overall: at 24 hours, more than two Snellen lines of improvement were already achieved in 37% of patients, and by 30 days, this improvement exceeded 60%. Twelve percent of patients experienced no visual improvement, primarily due to pre-existing retinal or optic nerve pathology.
Unplanned emergency visits occurred in 2.7% of cases, most commonly due to superficial punctate keratitis. One patient required surgical removal of retained cortex.
We conducted a univariate analysis and identified a significant association between ophthalmologic comorbidities and 30-day postoperative complications (p = 0.009) (Table 3). Complications detected at 24 hours were strong predictors of 30-day complications (p = 0.002). Early visual improvement was inversely associated with late postoperative complications (p = 0.038), suggesting its potential role as a marker for risk-stratified follow-up.
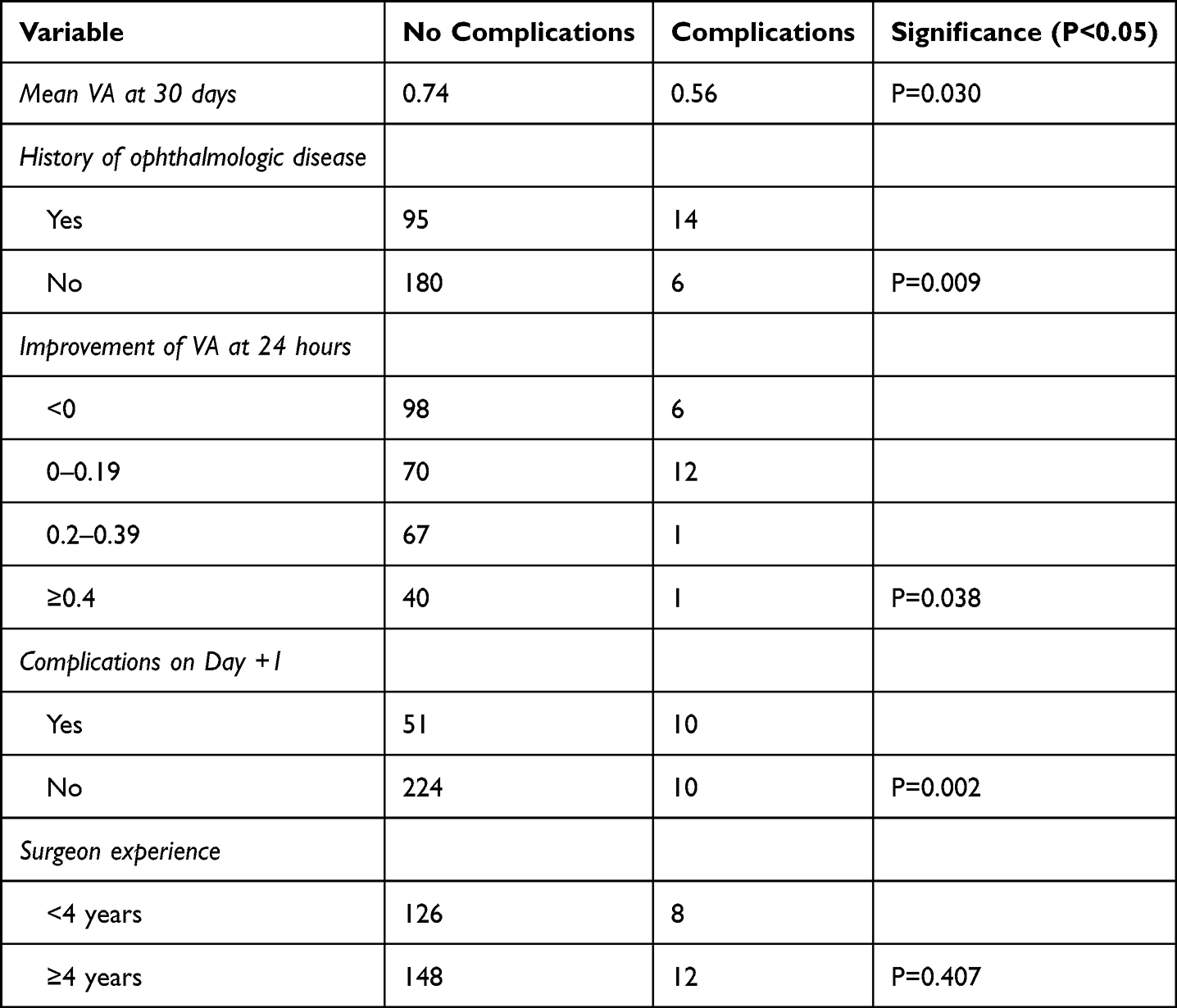 |
Table 3 Univariate Analysis by 30-Day Complication Status |
In the multivariate analysis (Table 4) using binomial logistic regression, the overall model was significant (χ2 = 26.28; p = 0.002). The variables independently associated with the occurrence of complications were the presence of a complication within the first 24 hours (OR = 3.25; p = 0.028) and ophthalmologic comorbidities (OR = 4.30; p = 0.010). Absence of early improvement in visual acuity did not reach statistical significance (OR = 4.53; p = 0.055), although it showed a strong trend toward association.
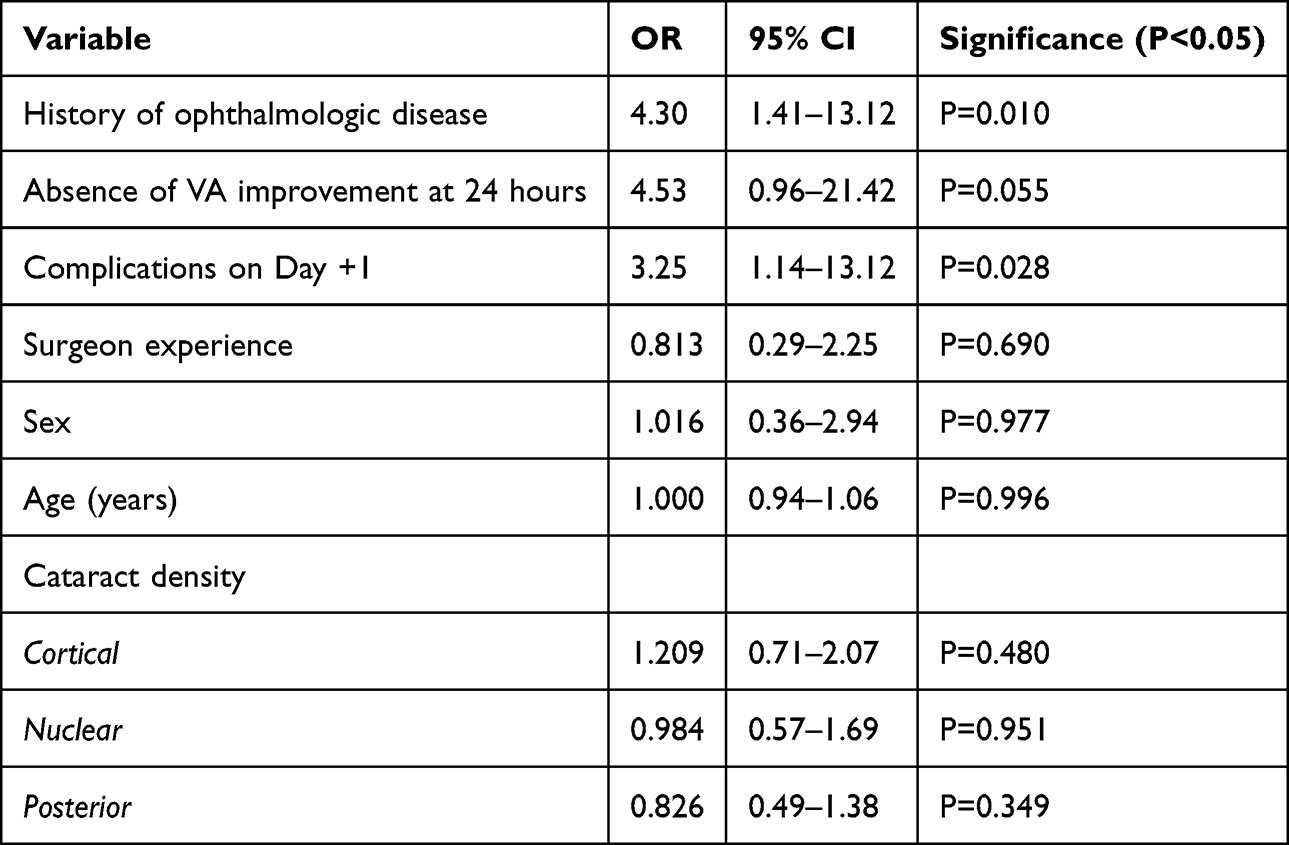 |
Table 4 Multivariate Logistic Regression Predicting 30-Day Postoperative Complications |
Discussion
This study provides an extensive real-world assessment of postoperative outcomes after uncomplicated phacoemulsification in a high-volume tertiary hospital. The results reaffirm the high safety profile of modern cataract surgery and underscore the importance of identifying patient subgroups who could benefit from simplified follow-up strategies without compromising clinical outcomes.10–13
Transient intraocular pressure elevation was the most common early postoperative issue, consistent with the published literature. Although typically benign in eyes without glaucoma, elevated IOP may have implications for patients with pre-existing optic nerve disease. Risk factors for these hypertensive spikes include resident-performed surgeries, a history of corticosteroid use, pseudoexfoliation syndrome (PEX), an axial length greater than 25 mm, and treatment with tamsulosin.9,14,15 In our cohort, the only factor significantly associated with elevated IOP was pseudoexfoliation syndrome, although patients with glaucoma showed a trend toward higher IOP values. Regarding incision leakage, retrospective studies report that only about 1% of patients require incision suturing.16 In our cohort, all cases with this complication were successfully managed conservatively.
Although clinical guidelines identify refractive assessment as the main objective of the one-month visit, this task is often delegated to community opticians.17–19 Evidence from the United Kingdom shows that community-based optometrists can provide postoperative care safely and with high patient satisfaction, and monthly telephone assessments using validated questionnaires have also demonstrated good accuracy. These approaches may be particularly beneficial for older patients with limited mobility.20,21
In our study, the most frequent complication identified at one month was cystoid macular edema, present in 3.60% of eyes, a rate similar to that reported in the literature.22 These patients also exhibited significantly worse visual acuity. This finding reinforces the value of visual acuity as an indirect clinical marker for detecting complications in a remote follow-up context.
A major contribution of this study is the identification of a clearly defined low-risk subgroup: patients without pre-existing ophthalmologic disease and without early postoperative abnormalities. This aligns with the multivariate findings, where ophthalmologic comorbidities and complications detected within the first 24 hours independently predicted 30-day complications. Although early improvement in visual acuity did not reach statistical significance in the multivariate model, it showed a strong trend toward association and may help identify individuals at lower risk. Overall, patients meeting these criteria demonstrated a very low likelihood of clinically relevant complications at one month and accounted for approximately 50% of the sample. This subgroup could be safely managed through remote or decentralized follow-up pathways, thereby reducing the workload of ophthalmology services.
Cataract surgery is one of the most commonly performed procedures worldwide, generating a considerable postoperative workload in publicly funded healthcare systems.23 In this context, uniform follow-up schedules may not be sustainable in the long term.24 In our cohort, approximately 50% of routine 30-day postoperative visits corresponded to patients meeting low-risk criteria. This proportion translates to nearly 150 potentially avoidable in-person reviews per month, exceeding 1800 visits per year in a high-volume tertiary hospital like ours. Assuming an average review time of 7–10 minutes, a risk-stratified follow-up model could alleviate approximately 300 hours of clinical workload annually. This reduction has the potential to decrease pressure on outpatient services and to enable meaningful reallocation of specialist time toward higher-risk or more complex cases. Although these estimates are based on local practice and cannot be fully generalized to all settings, they serve as illustrative projections and hypothesis-generating data for similar high-volume centers. Remote or decentralized follow-up should therefore be considered a structured component of modern cataract care pathways, provided that patient selection is guided by objective clinical criteria and real-world outcome data.
Nevertheless, reducing postoperative visits entails ethical and logistical considerations. Clinicians must balance their duty to ensure appropriate follow-up with the need to allocate limited healthcare resources efficiently. In teaching hospitals, postoperative evaluations also serve as essential training opportunities for residents. Although no differences in complication rates or visual outcomes were observed between surgeries performed by residents and attendings in our cohort, previous studies have reported higher adverse-event rates among trainees;25 the absence of such differences here likely reflects supervision and case selection, whereby less complex cases are preferentially assigned to residents and performed under the direct guidance of an experienced ophthalmologist.
This study has limitations. First, the relatively small number of complications observed at 30 days may have limited the robustness of the multivariate analysis, although this was partially mitigated by including only clinically or statistically relevant variables in the model. Second, exclusion of patients without complete follow-up may have introduced selection bias; however, this affected only a minimal number of cases. The retrospective design limits causal inference; nonetheless, the study accurately reflects routine clinical practice in a large tertiary hospital and provides valuable evidence to support the development of prospective trials evaluating remote, risk-stratified postoperative care models. These results represent a cohort in a single Spanish tertiary public hospital with close resident supervision, therefore results may not fully generalize to other healthcare settings.
Conclusions
Postoperative care after uncomplicated cataract surgery may be optimized using a stratified, risk-based approach. Patients without ophthalmologic history, without early complications, and with early visual improvement constitute a low-risk group that could be safely managed through remote or community-based follow-up at 30 days. In high-volume tertiary hospitals like ours, implementation of such follow-up protocols could potentially free up to 50% of postoperative visits while preserving safety and quality of care. These results support the development of multicenter prospective studies to validate remote follow-up models for uncomplicated cataract surgery.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval Statement
The study received approval from the Institutional Review Board/Ethics Committee of Ramón y Cajal University Hospital (approval ID: 388/25).
Informed Consent Statement
Given the retrospective design and full anonymization of data, the requirement for individual informed consent was waived by the Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–9. doi:10.1016/S0140-6736(17)30544-5
2. Brown GC, Brown MM, Menezes A, Busbee BG, Lieske HB, Lieske PA. Cataract surgery cost utility revisited in 2012: a new economic paradigm. Ophthalmology. 2013;120(12):2367–2376. doi:10.1016/j.ophtha.2013.04.030
3. Olson RJ, Braga-Mele R, Chen SH, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2017;124(2):P1–P119. doi:10.1016/j.ophtha.2016.09.027
4. The Royal College of Ophthalmologists. Commissioning guide: cataract surgery. 2015. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2015/03/Commissioning-Guide-Cataract-Surgery-FinalFebruary-2015.pdf.
5. Lundström M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European registry of quality outcomes for cataract and refractive surgery database. J Cataract Refract Surg. 2012;38(6):1086–1093. doi:10.1016/j.jcrs.2012.03.006
6. Jiang B, Wu T, Liu W, et al. Changing trends in the global burden of cataract over the past 30 years: retrospective data analysis of the global burden of disease study 2019. JMIR Public Health Surveill. 2023;9:e47349. doi:10.2196/47349
7. Whitefield L, Crowston J, Little BC. First day follow up for routine phacoemulsification? Br J Ophthalmol. 1996;80(2):148–150. doi:10.1136/bjo.80.2.148
8. Tufail A, Foss AJ, Hamilton AM. Is the first day postoperative review necessary after cataract extraction? Br J Ophthalmol. 1995;79(7):646–648. doi:10.1136/bjo.79.7.646
9. Kass MA, Heuer DK, Higginbotham EJ, et al. The ocular hypertension treatment study. Arch Ophthalmol. 2002;120(6):701–713. doi:10.1001/archopht.120.6.701
10. Grzybowski A, Kanclerz P. Do we need day-1 postoperative follow-up after cataract surgery? Graefes Arch Clin Exp Ophthalmol. 2019;257(5):855–861. doi:10.1007/s00417-018-04210-0
11. Deshpande R, Vora U, Mangiraj V, et al. Can the postoperative follow-up visit be deferred up to four weeks after an uneventful cataract surgery? A randomized controlled trial. Indian J Ophthalmol. 2021;69(6):1409–1413. doi:10.4103/ijo.IJO_2390_20
12. Kessel L, Andresen J, Erngaard D, et al. Safety of deferring review after uneventful cataract surgery until 2 weeks postoperatively. J Cataract Refract Surg. 2015;41(12):2755–2764. doi:10.1016/j.jcrs.2015.11.010
13. Yao LY, Fleshner PR, Zaghiyan KN. Impact of postoperative telemedicine visit versus in-person visit on patient satisfaction: a randomized clinical trial. Surgery. 2023;173(2):322–327. doi:10.1016/j.surg.2022.09.036
14. McKellar MJ, Elder MJ. The early complications of cataract surgery: is routine review of patients 1 week after cataract extraction necessary? Ophthalmology. 2001;108(5):930–935. doi:10.1016/S0161-6420(00)00431-0
15. Rainer G, Menapace R, Findl O, et al. Effect of topical brimonidine on intraocular pressure after small-incision cataract surgery. J Cataract Refract Surg. 2001;27(8):1227–1231. doi:10.1016/S0886-3350(01)00790-8
16. Zaidi FH, Corbett MC, Burton BJ, Bloom PA. The 1000 cataract operations audit and survey. Br J Ophthalmol. 2007;91(6):731–736. doi:10.1136/bjo.2006.104216
17. Al-Ani HH, Li S, Niederer RL. Telephone follow-up one day post-cataract surgery. Clin Exp Optom. 2023;106(7):741–745. doi:10.1080/08164622.2022.2146482
18. Tan P, Foo FY, Teoh SC, Wong HT. Nurse-administered telephone questionnaire for postoperative cataract surgery review. Int J Health Care Qual Assur. 2014;27(4):347–354. doi:10.1108/IJHCQA-11-2012-0120
19. Claessens JLJ, Wanten JC, Bauer NJC, et al. Web-based telemonitoring in cataract care: randomized controlled trial. J Cataract Refract Surg. 2024;50(9):947–955. doi:10.1097/j.jcrs.0000000000001492
20. O’Regan A, McGlacken-Byrne A, Chetty S, et al. Community optometrist-led postoperative cataract care. Ir J Med Sci. 2021;190(4):1613–1617. doi:10.1007/s11845-021-02514-5
21. Moustafa GA, Borkar DS, Borboli-Gerogiannis S, et al. Optimization of cataract surgery follow-up. PLoS One. 2019;14(9):e0221243. doi:10.1371/journal.pone.0221243
22. Giansanti F, Bitossi A, Giacomelli G, et al. Evaluation of macular thickness after uncomplicated cataract surgery using OCT. Eur J Ophthalmol. 2013;23(5):751–756. doi:10.5301/ejo.5000280
23. Ginel J, Burguera N, Piñero D, et al. Economic evaluations in cataract surgery: a narrative review. Eye. 2024;38(8):1418–1424. doi:10.1038/s41433-024-02965-x
24. Meltzer ME, Congdon N, Kymes SM, et al. Cost and expected visual effect of interventions to improve follow-up after cataract surgery. JAMA Ophthalmol. 2017;135(2):85–94. doi:10.1001/jamaophthalmol.2016.4735
25. Kang C, Lee MJ, Chomsky A, et al. Risk factors for complications in resident-performed cataract surgery: a systematic review. Surv Ophthalmol. 2024;69(4):638–645. doi:10.1016/j.survophthal.2024.04.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
Comparison of Phacoemulsification Grooving Efficiency in Longitudinal vs Transversal Handpieces
Wilkinson SW, Ungricht EL, West WB, Harris JT, Zaugg B, Olson RJ, Pettey JH
Clinical Ophthalmology 2023, 17:191-195
Published Date: 11 January 2023
Prospective Randomized Single-Masked Study of Bilateral Isofocal Optic-Design or Monofocal Intraocular Lenses
Ang RET, Stodulka P, Poyales F
Clinical Ophthalmology 2023, 17:2231-2242
Published Date: 4 August 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023
Clinical Outcomes of a Bi-Aspheric Trifocal Diffractive Intraocular Lens
Tañá-Sanz S, Tañá-Sanz P, Rodríguez-Carrillo MD, Ruiz-Santos M, Álvarez de Toledo C, Tañá-Rivero P
Clinical Ophthalmology 2024, 18:27-40
Published Date: 4 January 2024