Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitudes, and Practices Regarding Postoperative Management Among Patients with Fractures: A Cross-Sectional Study
Authors Wang Y, Chen H, Zhao X, Wang X
Received 23 September 2025
Accepted for publication 21 January 2026
Published 8 February 2026 Volume 2026:20 569742
DOI https://doi.org/10.2147/PPA.S569742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Yiying Wang,1 Hui Chen,1 Xiner Zhao,1 Xianliang Wang2
1Department of Nutrition, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China; 2Department of Orthopaedics, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China
Correspondence: Xiner Zhao, Email [email protected] Xianliang Wang, Email [email protected]
Background: Patients with fractures often face complex postoperative management requirements, and their knowledge, attitude, and practice regarding these aspects remain insufficiently understood.
Purpose: This study aims to assess the knowledge, attitude, and practice (KAP) related to postoperative management among patients with fractures.
Patients and Methods: A cross-sectional study was conducted in the Trauma Orthopedics Department of the Second Affiliated Hospital of Wenzhou Medical University from July 2024 to August 2024. A self-designed questionnaire was administered to collect demographic information and to evaluate KAP scores.
Results: A total of 556 (n = 556) valid responses were analyzed. Of the respondents, 279 (50.18%) were female, and 380 (68.35%) reported fractures resulting from falls. The mean ± SD scores for knowledge, attitude, and practice were 15.24 ± 3.62 (possible range: 0– 22), 31.43 ± 6.40 (possible range: 8– 40), and 83.07 ± 17.24 (possible range: 21– 105), respectively. Based on a 70% cutoff of the total score, 42.73% of participants had adequate knowledge, 82.59% had a positive attitude, and 72.53% reported proactive practice. Correlation analysis revealed significant positive correlations between knowledge scores and attitude scores (r = 0.782, P < 0.001), as well as between knowledge scores and practice scores (r = 0.832, P < 0.001). Additionally, attitude scores were positively correlated with practice scores (r = 0.804, P < 0.001). The structural equation model demonstrated that knowledge had a direct effect on attitude (standardized β = 0.913, P < 0.001) and practice (standardized β = 0.710, P < 0.001), while attitude also directly impacted practice (standardized β = 0.258, P = 0.021).
Conclusion: Patients with fractures exhibited suboptimal knowledge but generally positive attitudes and proactive practices toward postoperative management. Tailored educational interventions to improve patient knowledge could significantly enhance attitude and practice.
Keywords: health knowledge, attitudes, practice, fractures, bone, postoperative care, patient education as topic
Introduction
Fractures are a widespread clinical issue, particularly affecting older adults, and contribute significantly to both morbidity and healthcare costs worldwide.1,2 In China, approximately 5 million fracture cases occur annually.3 Effective postoperative management plays a critical role in ensuring successful recovery and improving patient prognosis. Proper management strategies can mitigate the risk of complications such as infection, nonunion, or refracture, and significantly enhance patients’ quality of life by promoting faster rehabilitation and reducing long-term disability.4–6 Key aspects of postoperative care, including timely rehabilitation, fall prevention, and proper nutrition, are essential for achieving optimal outcomes and reducing the burden of fractures on both patients and healthcare systems.7
Despite the clear importance of effective postoperative management, there are considerable gaps in patients’ understanding and application of recommended care practice. According to the Knowledge-Attitude-Practice (KAP) theory, knowledge forms the foundation for behavior change, while attitude and beliefs act as the driving force behind such changes.8 The process of behavior change, as outlined in KAP theory, involves three stages: first, acquiring knowledge, then forming attitude or beliefs based on that knowledge, and finally, translating these attitudes into practice or behaviors.9 However, simply acquiring knowledge does not guarantee behavior change. A shift in perception or attitude must occur first, which then facilitates the transition to behavior change.10 Patients who possess limited knowledge or hold misconceptions about their postoperative care are more likely to experience delayed rehabilitation, an increased risk of secondary complications, and lower overall recovery outcomes. Non-compliance with postoperative recommendations, such as physical rehabilitation exercises or appropriate dietary modifications, can further exacerbate these challenges. Therefore, understanding patients’ current levels of KAP regarding postoperative fracture management is essential for addressing these issues. In orthopaedic settings, several structured frameworks have been developed to assess and standardize postoperative care, including multidimensional evaluation tools that cover pain control, functional recovery, and patient education. For example, recent work has proposed an integrated postoperative care assessment model for orthopaedic patients, providing a practical reference for monitoring and improving rehabilitation quality in clinical practice.11 In the Chinese context, postoperative fracture care is often embedded within family-centred caregiving, where spouses and adult children commonly act as primary caregivers and participate in health-related decision-making, which may shape patients’ knowledge, attitudes, and everyday management practices.
Currently, there is a lack of KAP studies specifically focused on this topic in the context of fracture management. This study aims to explore the current knowledge, attitude, and practice of fracture patients regarding their postoperative care.
Materials and Methods
Study Design and Patients
This cross-sectional study was conducted on patients who had undergone fracture surgery at the Trauma Orthopaedics Department of the Second Affiliated Hospital of Wenzhou Medical University. The questionnaire distribution and data collection were carried out between July and August 2024. Ethical approval for the study was granted by the Medical Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (Approval No: 2024-K-188-01), and informed consent was obtained from all participants. The inclusion criteria were as follows: (1) postoperative fracture patients; (2) age 18 years or older; (3) ability to understand the purpose of the study and willingness to sign the informed consent form; and (4) clear consciousness with basic cognitive functions to comprehend and respond to the questionnaire. The exclusion criteria were: (1) patients with other severe diseases, such as advanced cancer or serious cardiovascular or pulmonary diseases.
Questionnaire
The design of the questionnaire was based on previous literature12 and relevant national and international guidelines.13–15 After the initial draft was completed, a preliminary survey (n=31) was conducted to test its reliability, yielding an overall Cronbach’s α coefficient of 0.870, which indicates good internal consistency of the questionnaire. To further assess construct validity, we conducted confirmatory factor analysis (CFA) for the knowledge, attitude, and practice domains. A three-factor measurement model with correlated latent variables was specified and estimated using maximum likelihood.
The finalized questionnaire was in Chinese and consisted of four sections: demographic data (including age, sex, height, weight, education level, occupation, monthly income, type of fracture, cause of injury, surgical history, and primary caregiver), knowledge dimension (K), attitude dimension (A), and practice dimension (P). The full English versions of the original questionnaire are provided as Supplement Figures 1–7. Body mass index (BMI) was calculated as BMI = weight (kg)/height (m)2. The knowledge dimension included 11 items, with each item scored as 2 points for “very familiar”, 1 point for “somewhat familiar”, and 0 points for “unfamiliar”, resulting in a total possible score of 0–22 points. The attitude dimension consisted of 8 questions, rated on a 5-point Likert scale, with scores ranging from 5 (strongly agree) to 1 (strongly disagree), resulting in a total score range of 8–40 points. The practice dimension included 21 questions, with responses scored from 1 (never) to 5 (always), yielding a total possible score range of 21–105 points. In line with previous KAP studies, we used an empirical threshold of ≥70.0% of the total score to classify “adequate” knowledge, “positive” attitude, and “proactive” practice for descriptive interpretation rather than as a clinically validated diagnostic standard.16–18
Questionnaire Distribution and Quality Control
The questionnaire was distributed using both online and offline methods. Convenience sampling was conducted among surgical patients discharged from the trauma orthopedic ward at our hospital. An online questionnaire was created using the Questionnaire Star platform (https://www.wjx.cn/), generating an electronic survey link. This link was sent via SMS to the mobile phone numbers listed in the patients’ hospitalization records. Additionally, telephone follow-up was conducted by directly calling the patients themselves to ensure that all respondents were indeed fracture patients. In total, 1000 text messages were sent to eligible patients, of whom 503 completed the online questionnaire (SMS response rate: 50.3%). In addition, 70 valid questionnaires were obtained via telephone follow-up among patients who did not complete the online survey, after excluding unanswered or unreachable calls. Throughout the questionnaire completion process, research assistants provided instructions to ensure participants fully understood the content and objectives of the study, without interfering with or influencing their individual responses. Following data collection, quality checks were conducted by members of the research team. Data accuracy of the telephone follow-up questionnaires was ensured through cross-verification by two researchers. Questionnaires were considered invalid and excluded if the completion time was less than 90 seconds, if responses were incomplete, or if logical inconsistencies or repetitive patterns were detected in the answers.
Sample Size
The sample size was calculated using the standard formula for cross-sectional studies:19 n= (Z(1-α/2)/δ)^2×p× (1-p), where Z(1-α/2) = 1.96 for a significance level of α=0.05, p=0.5 (which maximizes the required sample size by assuming maximum variability), and δ=0.05, representing the permissible margin of error. The calculated theoretical sample size was 480, which includes an additional 20% to account for potential subject loss.
Statistical Analysis
Statistical analyses were performed using SPSS 27.0 (IBM, Armonk, NY, USA) and AMOS 26.0 (IBM, Armonk, NY, USA). The normality of the score distribution for each dimension was evaluated. Normally distributed data are presented as means and standard deviations (SD), while non-normally distributed data are reported as medians with interquartile ranges (IQR; 25th and 75th percentiles). For comparisons between two groups, the t-test was applied for normally distributed continuous variables, whereas the Wilcoxon-Mann–Whitney test was used for non-normally distributed variables. For comparisons involving three or more groups, ANOVA was used for normally distributed variables with homogeneity of variance, and the Kruskal–Wallis test was applied to non-normally distributed variables. Spearman correlation coefficient was used to assess correlations between KAP scores. Structural equation modeling (SEM) was conducted to examine the relationships between knowledge, attitude, and practice within the KAP framework, specifically evaluating whether attitude mediates the effect of knowledge on practice behaviors. Both direct and indirect effects were calculated and compared. Model fit of both SEM and CFA was evaluated using the following criteria: Chi-square/degrees of freedom (CMIN/DF) < 3, Root Mean Square Error of Approximation (RMSEA) < 0.08, Standardized Root Mean Square Residual (SRMR) < 0.08, Tucker-Lewis Index (TLI) > 0.8, and Comparative Fit Index (CFI) > 0.8. In addition, univariable and multivariable linear regression models were fitted with knowledge, attitude, and practice scores as dependent variables to explore factors associated with each KAP domain. A two-sided P-value of < 0.05 was considered statistically significant.
Results
Demographic Information on Participants
Initially, 573 questionnaires were collected. Among these, 503 were obtained through SMS-based online responses, following the distribution of 1000 messages to the mobile phone numbers recorded in patients’ hospitalization records. An additional 70 valid questionnaires were obtained through direct telephone follow-up with patients. However, 1 was excluded due to incorrect BMI value and 16 due to incomplete responses, leaving 556 valid cases. Among the respondents, 279 (50.18%) were female, with a mean age of 53.56 ± 15.49 years. A total of 286 participants (51.44%) had a primary school education or lower, 380 (68.35%) reported fractures due to falls, 146 (26.26%) had a history of surgery, 432 (77.70%) were cared for by their spouse, and 216 (38.85%) had other listed conditions. The median [Q1, Q3] scores for knowledge, attitude, and practice were 16.00 [14.00, 18.00], 33.00 [31.00, 35.00], and 92.00 [73.75, 95.00], respectively (Table 1). Also, baseline demographic and clinical characteristics were broadly comparable between online and telephone respondents, although telephone respondents were more likely to live in rural areas, have lower monthly income, and require assistance with activities of daily living (Supplement Table 1).
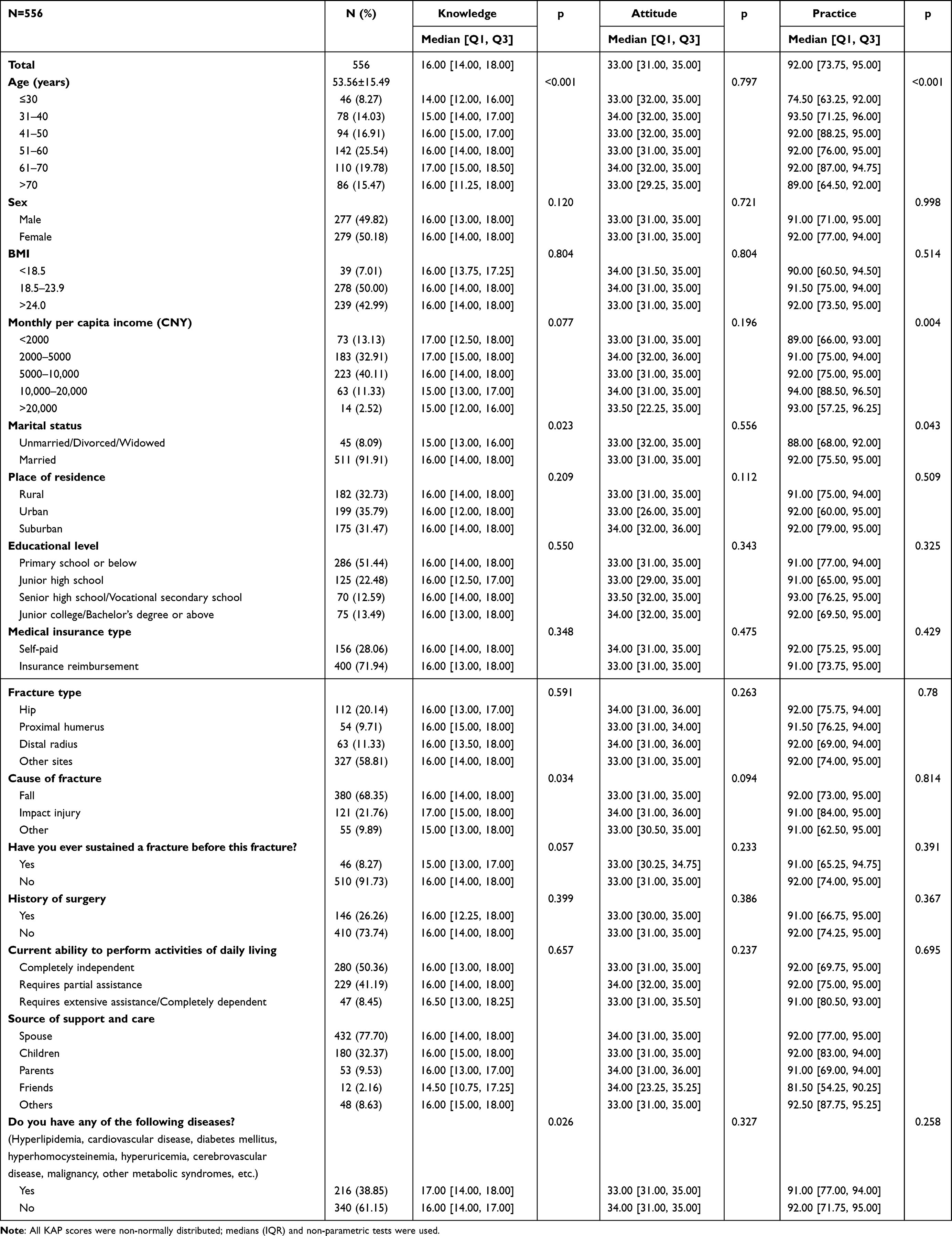 |
Table 1 Sociodemographic and Clinical Characteristics of Fracture Patients and Corresponding KAP Scores (n = 556) |
The mean ± SD scores for knowledge, attitude, and practice were 15.24 ± 3.62 (possible range: 0–22), 31.43 ± 6.40 (possible range: 8–40), and 83.07 ± 17.24 (possible range: 21–105), respectively. These mean scores correspond to 69.3%, 78.6%, and 79.1% of the maximum possible scores, respectively. Thus, the average knowledge score fell just below the prespecified 70% adequacy threshold, whereas attitude and practice scores were above this cutoff, indicating suboptimal knowledge but generally positive attitudes and proactive practices toward postoperative management. Based on a 70% cutoff of the total score, 42.73% of participants had adequate knowledge, 82.59% had a positive attitude, and 72.53% reported proactive practice. Knowledge and practice scores differed significantly across age groups (both P < 0.001). In addition, marital status was associated with knowledge and practice scores (P = 0.023 and P = 0.043, respectively), and monthly per capita income was associated with practice scores (P = 0.004) (Table 1).
Multivariable regression analysis showed that age 41–50 years (β = 1.748, 95% CI: 0.501–2.995, P = 0.006), 51–60 years (β = 1.368, 95% CI: 0.192–2.544, P = 0.023), and 61–70 years (β = 2.186, 95% CI: 0.965–3.408, P < 0.001) were independently associated with higher knowledge scores, whereas a prior history of fracture was independently associated with lower knowledge scores (β = −1.357, 95% CI: −2.439 to −0.275, P = 0.014) (Supplement Table 2). In the multivariable model, knowledge score (β = 1.355, 95% CI: 1.258–1.451, P < 0.001) and unmarried/divorced/widowed marital status (β = 3.578, 95% CI: 2.234–4.922, P < 0.001) were independently associated with higher attitude scores, while junior high school education (β = −0.955, 95% CI: −1.824 to −0.087, P = 0.031) and junior college/bachelor’s degree or above (β = −1.222, 95% CI: −2.384 to −0.059, P = 0.040) were associated with lower attitude scores (Supplement Table 3). Also, higher knowledge score (β = 2.056, 95% CI: 1.747–2.365, P < 0.001), higher attitude score (β = 1.332, 95% CI: 1.161–1.503, P < 0.001), age 31–40 years (β = 5.803, 95% CI: 2.694–8.912, P < 0.001), 41–50 years (β = 7.116, 95% CI: 4.082–10.151, P < 0.001), 51–60 years (β = 7.097, 95% CI: 4.088–10.107, P < 0.001), 61–70 years (β = 6.899, 95% CI: 3.543–10.255, P < 0.001), >70 years (β = 5.210, 95% CI: 1.536–8.884, P = 0.006), and monthly per capita income of 5000–10,000 CNY (β = 3.333, 95% CI: 0.376–6.290, P = 0.028) and 10,000–20,000 CNY (β = 6.531, 95% CI: 2.922–10.141, P < 0.001) were independently associated with higher practice scores (Supplement Table 4).
Distribution of Responses to Knowledge, Attitude, and Practice
In the knowledge dimension, the three questions with the highest percentage of participants selecting “Unclear” were: “Bone mineral density testing is recommended after a fracture” (K2), with 27.34%; “Certain medications, such as loop diuretics, antipsychotics, antidepressants, and opioids, may increase the risk of falls” (K11), also with 27.34%; and “Early functional exercises should primarily involve active contraction and relaxation of the muscles in the affected limb” (K7), with 16.19% (Table 2).
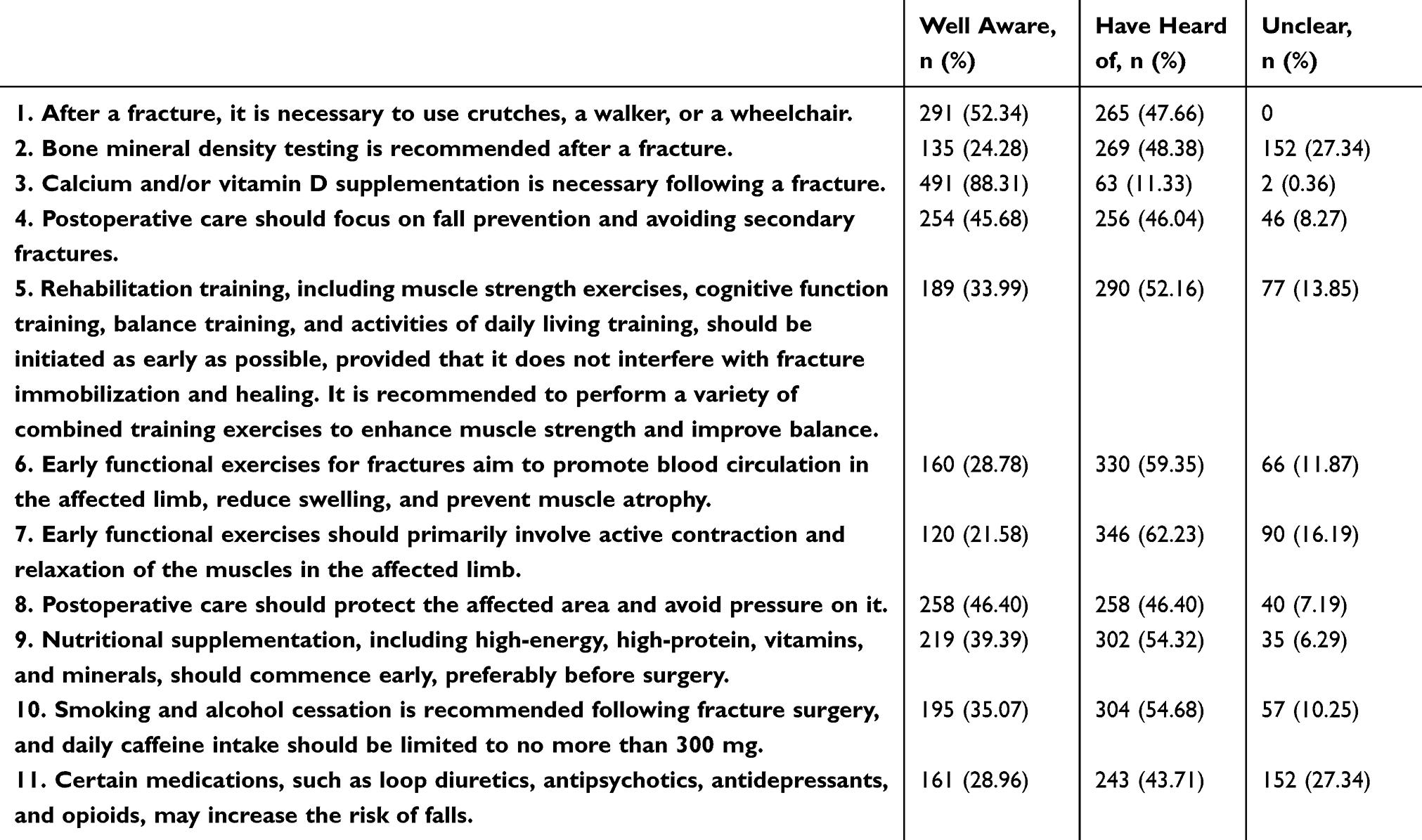 |
Table 2 Item-Level Distribution of Responses in the Knowledge Dimension (n = 556) |
Regarding attitude, 6.29% disagreed and 6.12% strongly disagreed with the statement that “Participating in social activities, as much as their physical condition allows, promotes recovery and physical and mental well-being” (A7). Furthermore, 4.32% disagreed and 5.76% strongly disagreed with the belief that “Calcium supplementation is essential for preventing bone loss and promoting fracture recovery” (A2), and 4.32% disagreed and 5.76% strongly disagreed that “Being attentive to one’s health status is crucial for ensuring successful postoperative fracture recovery” (A4) (Table 3).
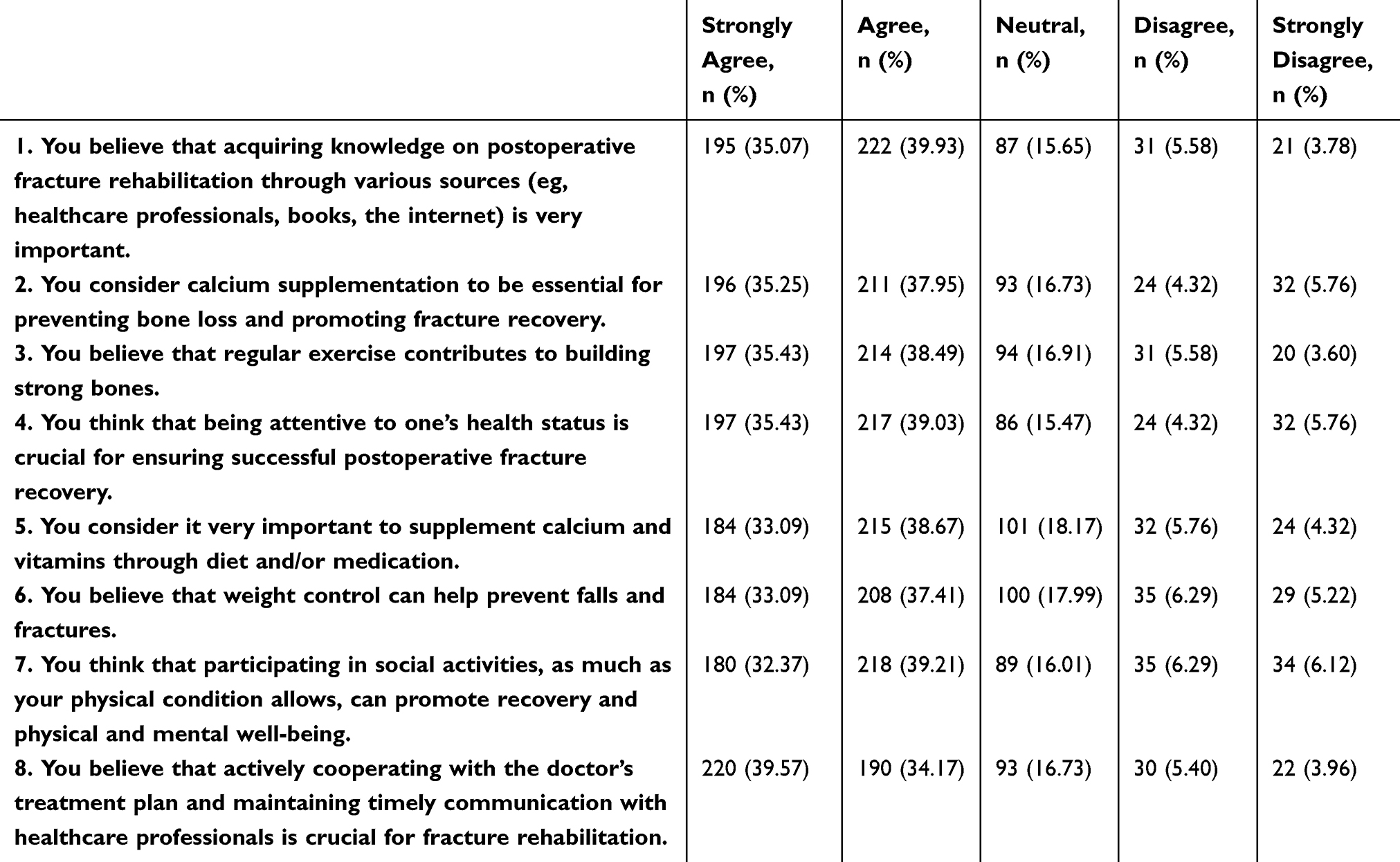 |
Table 3 Item-Level Distribution of Responses in the Attitude Dimension (n = 556) |
In the practice dimension, 16.37% reported never strictly following their doctor’s prescriptions for long-term antihypertensive medication (P16), 12.59% never underwent regular bone-related examinations or paid attention to the results (P2), and 8.99% never limited their intake of foods that inhibit calcium absorption during calcium supplementation (P7) (Table 4).
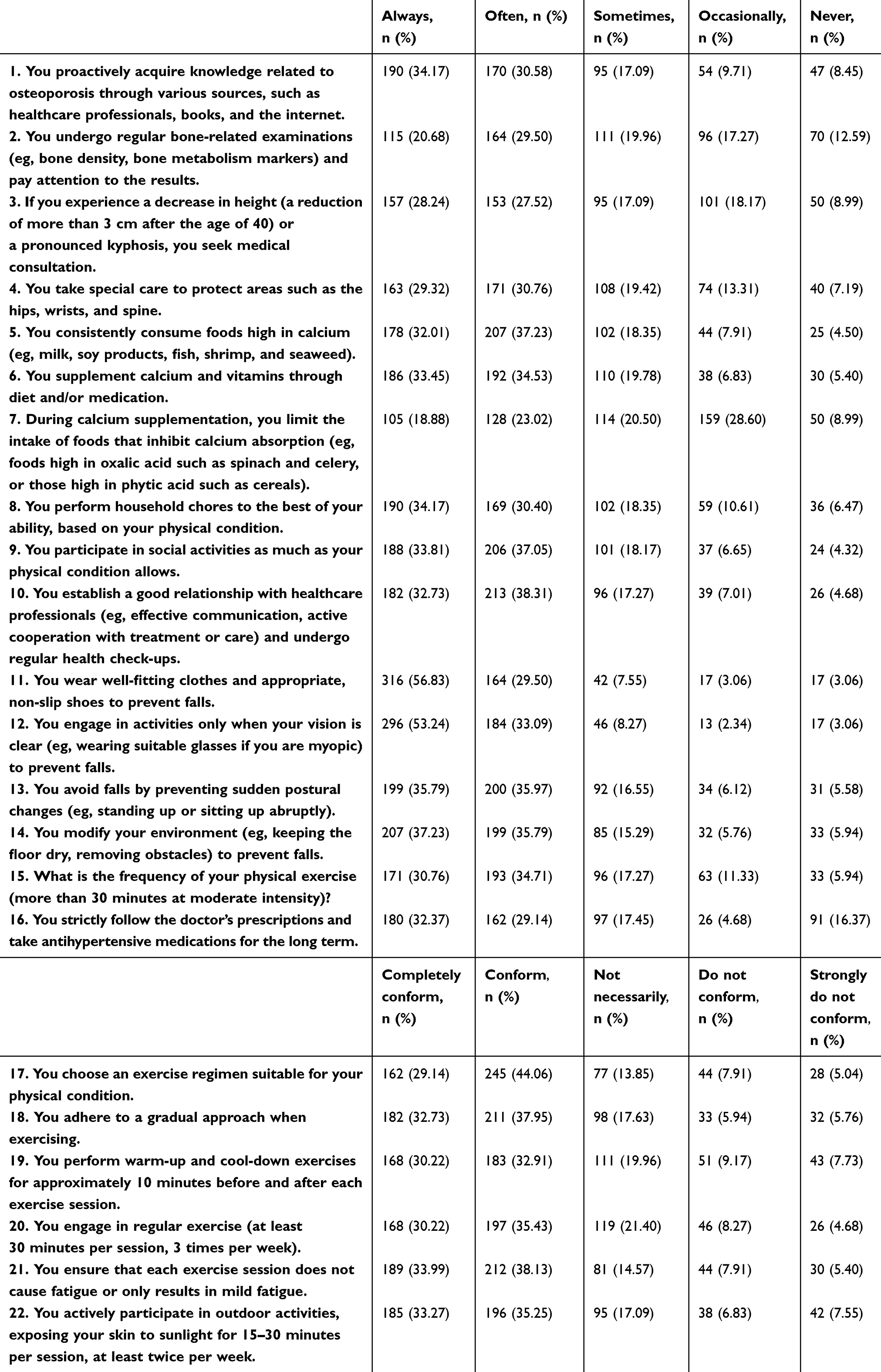 |
Table 4 Item-Level Distribution of Responses in the Practice Dimension (n = 556) |
Regarding health education received, among the 556 valid cases, the majority of patients reported receiving medical education on psychological care (496, 88.89%), fall prevention measures (462, 82.80%), and fracture-related knowledge (455, 81.54%). However, only 185 cases (33.15%) indicated they received education on medication precautions, and just 285 cases (51.08%) reported receiving information on the prevention and management of common complications (Supplement Figure 8 Health Education received).
Correlations Between KAP
Further correlation analysis revealed positive correlations between knowledge scores and attitude scores (r = 0.782, P < 0.001), as well as between knowledge scores and practice scores (r = 0.832, P < 0.001). Additionally, attitude scores were positively correlated with practice scores (r = 0.804, P < 0.001) (Table 5).
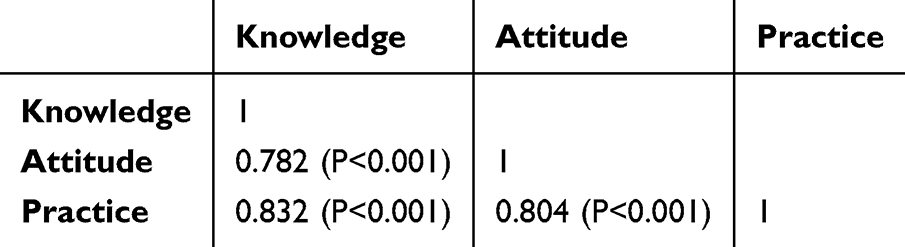 |
Table 5 Spearman Correlation Coefficients Among Knowledge, Attitude, and Practice Scores (n = 556) |
SEM Analysis
Before estimating the structural paths, we first tested a three-factor CFA measurement model for the knowledge, attitude, and practice domains. The CFA demonstrated an acceptable model fit, with RMSEA = 0.056 and SRMR = 0.058, both below the recommended threshold of 0.08, and satisfactory incremental fit indices (TLI = 0.867 and CFI = 0.874), indicating an overall adequate fit of the measurement model (Supplement Table 5). The standardized path coefficients of SEM showed that knowledge had a direct effect on attitude (β = 0.913, 95% CI: 0.877–0.949; P < 0.001) and practice (β = 0.710, 95% CI: 0.495–0.925; P < 0.001), while attitude also directly influenced practice (β = 0.258, 95% CI: 0.040–0.475; P = 0.021). Knowledge also had an indirect effect on practice through attitude (β = 0.235, 95% CI: 0.041–0.430; P = 0.018), indicating that attitude partially mediates the relationship between knowledge and practice (Supplement Table 6 and Figure 1). The SEM demonstrated an acceptable overall fit (Supplement Table 7).
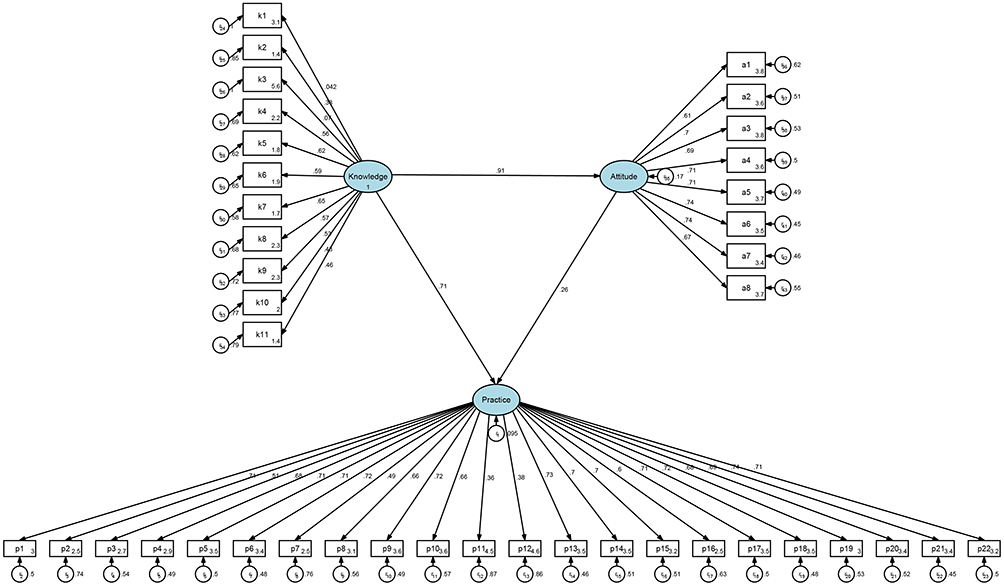 |
Figure 1 Structural equation model of the relationships between knowledge, attitude, and practice. Ellipses represent latent variables (unobserved constructs), including overall knowledge, attitude, and practice. Rectangles represent observed variables (measured questionnaire items) that serve as indicators of the latent variables. Circles represent error terms or residuals associated with the observed variables. Single-headed arrows indicate hypothesized directional relationships (pathways) between latent variables and from latent variables to observed variables, with standardized path coefficients labeled on the arrows. |
Discussion
Patients with fractures demonstrated suboptimal knowledge but exhibited generally positive attitudes and proactive practices toward postoperative management. These findings highlight the need for targeted educational interventions to enhance patient knowledge, which may help promote better attitudes and postoperative management practices.
The findings of this study indicate that while patients with fractures generally display positive attitude and proactive practice towards postoperative management, their knowledge levels remain suboptimal. This gap in knowledge is particularly concerning, as adequate understanding of postoperative care is crucial for preventing complications such as secondary fractures and for ensuring proper rehabilitation. Similar results have been observed in other studies, where patients with orthopedic conditions demonstrated insufficient knowledge about their conditions, leading to poor compliance with rehabilitation protocols and longer recovery periods.20,21 Patient knowledge plays a critical role in shaping adherence to treatment and effective self-management, thereby potentially affecting overall clinical outcomes.22 However, our cross-sectional design did not include objective clinical endpoints, so any link between knowledge deficits and prognosis in this population remains hypothetical. In this context, we cautiously suggest that improving patient knowledge through targeted education may support better self-management and rehabilitation adherence, but the impact on clinical outcomes should be examined in future longitudinal studies.
Regarding the relationships between KAP, the correlation analysis and SEM reveal that knowledge is significantly associated with both attitude and practice. These results are consistent with other studies, which have shown that improving patient knowledge can positively influence health-related behaviors, such as medication adherence and participation in rehabilitation.23,24 The direct effect of knowledge on both attitude and practice emphasizes the importance of patient education in postoperative care. Although the standardized path coefficients indicated moderately strong associations among the three domains, they should be interpreted with caution because the knowledge, attitude, and practice dimensions cover related aspects of postoperative care and may share overlapping content. In particular, items K1 (use of assistive devices) and K3 (calcium and/or vitamin D supplementation) showed relatively lower factor loadings in the measurement model, suggesting that they may capture more general fracture-related awareness rather than postoperative management specifically; these items could be refined in future iterations of the scale. Furthermore, in the CFA, most items showed moderate-to-high standardized factor loadings, whereas a small number of knowledge items (such as K1 and K3) had relatively low or non-significant loadings, indicating potential item ambiguity and measurement error. These items will need to be refined and revalidated in future iterations of the scale, and the KAP relationships observed here should therefore be interpreted with appropriate caution. However, despite this positive relationship, the lower knowledge scores observed in this study suggest that the current educational approaches may not be sufficiently effective. It is possible that the information provided to patients is either too complex, not relevant to their specific needs, or not communicated in a way that promotes long-term retention and understanding.
When exploring the significant differences across demographic variables, several interesting patterns emerge. Age was significantly associated with both knowledge and practice scores, with older participants generally demonstrating better practice. This may be because older adults are more likely to have experienced fractures or other serious health issues in the past,25,26 which may lead to a greater appreciation for postoperative care and the importance of adhering to medical advice. However, despite their better practice, older participants did not necessarily exhibit higher knowledge levels, which may be due to a reliance on healthcare providers rather than self-directed learning.27,28 This trend is consistent with findings from other studies that suggest older adults often trust healthcare providers’ recommendations but may not actively seek additional knowledge.29,30 In contrast, younger patients may not yet fully recognize the long-term consequences of inadequate postoperative care, leading to less proactive behavior despite having better access to information. These age-related patterns in knowledge and practice remained evident after adjustment for other demographic and clinical covariates in multivariable regression models.
Significant differences were also observed between married and unmarried participants, as well as between urban and rural residents, in terms of attitude towards postoperative care. Married participants and those from urban areas generally exhibited lower attitude scores, which might be explained by their access to more comprehensive healthcare systems or greater reliance on external support, such as family or caregivers.31,32 This suggests a passive stance towards self-managed care, as they might perceive less individual responsibility for their recovery outcomes. Previous studies also identified similar patterns, indicating that patients with easier access to healthcare often demonstrate reduced self-efficacy in managing personal health matters.33,34 In contrast, rural and suburban residents may encounter more access barriers and fewer formal support options, which can foster a stronger sense of personal responsibility for self-care and lead to more proactive attitudes despite these structural disadvantages. Consistent with these univariable findings, multivariable models also suggested that unmarried or widowed status was associated with more positive attitudes after accounting for other covariates. This emphasizes the necessity for tailored interventions that promote patient empowerment, regardless of marital status or location.
When analyzing the distribution of responses in the KAP dimensions, several areas of concern become apparent. In the knowledge domain, many participants lacked awareness about key aspects of postoperative care, particularly bone mineral density testing following fractures. Additionally, there was limited understanding of medication risks, such as diuretics and antipsychotics, play in increasing the risk of falls. These knowledge gaps have been similarly documented in previous research, where inadequate patient education has been linked to higher rates of complications, such as refractures or prolonged immobilization.35,36 Furthermore, in the attitude dimension, a considerable proportion of participants underestimated the importance of dietary calcium supplementation and consistent health monitoring after surgery. These misconceptions are likely to lower adherence to rehabilitation protocols and elevate the risk of postoperative complications.
In the practice domain, several concerning trends were observed. Participants often reported irregular bone density tests and inadequate adherence to dietary guidelines, particularly regarding foods that inhibit calcium absorption. Such findings are consistent with other research, where non-compliance with dietary and medical recommendations has been associated with poor long-term recovery outcomes in fracture patients.37,38 This gap between patients’ positive intentions and their actual behaviors may critically impact recovery, indicating that improving practice remains a significant challenge.
To address these gaps, a comprehensive, evidence-based approach to patient education is necessary. Healthcare providers should offer tailored interventions that cater to each patient’s specific condition and circumstances. For instance, visually engaging educational materials could be developed that directly address the weakest items identified in this survey, such as the need for bone mineral density testing after a fracture (K2), the fall risk associated with commonly used medications such as diuretics and psychotropic drugs (K11), and practical examples of calcium-rich diets and foods that inhibit calcium absorption (P7). Personalized materials could be tailored for patients with lower educational attainment and for those who reported irregular bone-related examinations or dietary non-adherence, using plain language, pictorial examples, and step-by-step guidance that match their fracture type and rehabilitation stage. Additionally, structured follow-up consultations should be implemented, focusing on reinforcing key messages and correcting any misconceptions. For example, patients could maintain a health diary to record adherence to rehabilitation exercises, medication schedules, and dietary intake. Regular follow-ups would allow healthcare providers to track progress, provide feedback, and promote positive behavioral changes. Continuous, interactive education—particularly when supported by self-monitoring tools—has been shown to enhance patient engagement and clinical outcomes.39,40
To improve poor practice scores in areas like dietary adherence and regular bone health assessments, follow-up care should be more structured. In line with the low proportions of regular bone-related examinations (P2) and long-term antihypertensive adherence (P16), healthcare providers could use simple SMS- or app-based reminders to prompt patients to schedule bone mineral density tests, attend follow-up appointments, and review short checklists on medication adherence, fall prevention, and exercise intensity.41,42 Integrating these approaches into postoperative fracture care could enhance adherence, contributing to better recovery outcomes.
Potential Selection Biases and Generalizability
Several features of our study design may have introduced selection bias and affected the generalizability of the findings. First, all participants were recruited from a single tertiary trauma orthopaedics department, where clinical pathways, discharge planning, and patient education practices may differ from those in other hospitals and regions of China. Second, we used convenience sampling and a mixed recruitment strategy, inviting patients via SMS and supplementing with telephone follow-up. Only 50.3% of patients invited by SMS completed the online questionnaire, and telephone follow-up mainly included patients who could be reached at the recorded phone numbers. As a result, our sample may over-represent patients who are more reachable, more motivated, or have better access to mobile devices, and under-represent those with lower health literacy or poorer access to digital tools. These potential selection biases should be taken into account when extrapolating our KAP estimates to the broader population of fracture patients.
This study has several limitations. First, as an inherent limitation of cross-sectional studies, the design precludes the ability to establish causal relationships between knowledge, attitude, and practice variables. Second, the study was conducted in a single tertiary hospital, where clinical pathways, discharge planning, and patient education practices may differ from those in other regions of China, which may limit the generalizability of the findings. Third, the use of convenience sampling from a single trauma orthopaedics department and the mixed recruitment strategy (SMS invitations and telephone follow-up) may limit the representativeness of the sample and introduce selection bias. Fourth, self-reported data from questionnaires are subject to recall bias and social desirability bias, particularly for practice items; because the survey was conducted under the auspices of the treating hospital and the telephone follow-up was performed by study personnel, some participants may have over-reported desirable self-management behaviors, which could lead to an overestimation of practice levels. Finally, among the 1000 individuals invited to participate via SMS, 503 provided online responses, yielding an initial response rate of 50.3%. This relatively low response rate raises the possibility of non-response bias in addition to selection bias, as those who chose to participate might have had a greater interest in postoperative management than non-respondents, potentially skewing the findings. Moreover, the 70% cutoff used to define adequate knowledge, positive attitude, and proactive practice was an empirical threshold adopted from previous KAP studies and has not been specifically validated in fracture populations; alternative classification approaches such as quartiles or standardized scores may yield complementary insights. Some questionnaire items (eg, antihypertensive adherence, vision correction, dietary choices) may not apply to all patients. Future studies with longitudinal designs, multi-center settings, and improved response rates are warranted to validate and expand upon these findings.
Conclusion
In conclusion, using a ≥70% adequacy threshold adopted in previous KAP studies,16,17 patients with fractures showed suboptimal knowledge yet generally positive attitudes and proactive practices toward postoperative management. Implementing targeted educational strategies that enhance patient knowledge may also positively influence attitudes and practices.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Informed Consent
The study was approved by Medical Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (2024-K-188-01). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Einhorn TA, Gerstenfeld LC. Fracture healing: mechanisms and interventions. Nat Rev Rheumatol. 2015;11(1):45–14. doi:10.1038/nrrheum.2014.164
2. Groff H, Kheir MM, George J, Azboy I, Higuera CA, Parvizi J. Causes of in-hospital mortality after hip fractures in the elderly. Hip Int. 2020;30(2):204–209. doi:10.1177/1120700019835160
3. Chen W, Lv H, Liu S, et al. National incidence of traumatic fractures in China: a retrospective survey of 512 187 individuals. Lancet Glob Health. 2017;5(8):e807–e817. doi:10.1016/S2214-109X(17)30222-X
4. Chang CJ, Jou IM, Wu TT, Su FC, Tai TW. Cigarette smoke inhalation impairs angiogenesis in early bone healing processes and delays fracture union. Bone Joint Res. 2020;9(3):99–107. doi:10.1302/2046-3758.93.BJR-2019-0089.R1
5. Cheng C, Shoback D. Mechanisms underlying normal fracture healing and risk factors for delayed healing. Curr Osteoporos Rep. 2019;17(1):36–47. doi:10.1007/s11914-019-00501-5
6. Zura R, Xiong Z, Einhorn T, et al. Epidemiology of fracture nonunion in 18 human bones. JAMA Surg. 2016;151(11):e162775. doi:10.1001/jamasurg.2016.2775
7. Takahashi K, Momosaki R, Yasufuku Y, Nakamura N, Maeda K. Nutritional therapy in older patients with hip fractures undergoing rehabilitation: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21(9):1364–1364.e1366. doi:10.1016/j.jamda.2020.07.005
8. Gao L, Su S, Du N, et al. Medical and non-medical students’ knowledge, attitude and willingness towards the COVID-19 vaccine in China: a cross-sectional online survey. Hum Vaccin Immunother. 2022;18(5):2073757. doi:10.1080/21645515.2022.2073757
9. Twinamasiko N, Olum R, Gwokyalya AM, Nakityo I, Wasswa E, Sserunjogi E. Assessing knowledge, attitudes and practices towards COVID-19 public health preventive measures among patients at Mulago national referral hospital. Risk Manag Healthc Policy. 2021;14:221–230. doi:10.2147/RMHP.S287379
10. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
11. Moldovan F, Moldovan L. Assessment of patient matters in healthcare facilities. Healthcare. 2024;12(3):325. doi:10.3390/healthcare12030325
12. Wang A, Mu W, Wang Y, Xu Z, Wang X. Summary of the best evidence for the prevention and management of secondary hip fracture in elderly patients. Evidence-Based Nursing. 2023;9(17):3067–3071.
13. National Clinical Guideline C. National Institute for Health and Care Excellence: Clinical Guidelines. Fractures (Complex): Assessment and Management. London: National Institute for Health and Care Excellence (UK)Copyright © National Clinical Guideline Centre; 2016.
14. National Institute for Health and Care Excellence. Guidelines. Fractures (Complex): Assessment and Management. London: National Institute for Health and Care Excellence (NICE) Copyright © NICE; 2022.
15. Chinese Society of Surgery CMA. Chinese Society of Anesthesiology CMA, Yu-pei Z, Yu-guang H. Clinical practice guidelines for enhanced recovery after surgery in China(2021 edition). Chinese J Pract Sur. 2021;41(09):961–992.
16. Hebo HJ, Gemeda DH, Abdusemed KA. Hepatitis B and C viral infection: prevalence, knowledge, attitude, practice, and occupational exposure among healthcare workers of jimma university medical center, Southwest Ethiopia. Sci World J. 2019;2019:9482607. doi:10.1155/2019/9482607
17. Salman M, Mustafa ZU, Rao AZ, et al. Serious inadequacies in high alert medication-related knowledge among Pakistani nurses: findings of a large, multicenter, cross-sectional survey. Front Pharmacol. 2020;11:1026. doi:10.3389/fphar.2020.01026
18. Deng X, Li Q, Weng M, et al. Knowledge, attitudes, and practices of patients with lower limb fractures post-surgery regarding deep vein thrombosis. Sci Rep. 2025;15(1):9520. doi:10.1038/s41598-025-92632-2
19. Zhi X, Chen J, Yang L, et al. Knowledge, attitudes, and practices toward nutritional management among patients with gastrointestinal cancer: a cross-sectional study. Asia Pac J Oncol Nurs. 2025;12:100688. doi:10.1016/j.apjon.2025.100688
20. Childs BR, Breslin MA, Andres BA, et al. Enhancing trauma patient experience through education and engagement: development of a mobile application. J Am Acad Orthop Surg Glob Res Rev. 2020;4(3). doi:10.5435/JAAOSGlobal-D-20-00025
21. Pang Z, Hu B, Chai D, et al. Effect of WeChat-based health preaching combined with an enhanced recovery after surgery model on perioperative limb motor function and complications in orthopaedic patients. J Healthc Eng. 2022;2022:9538138. doi:10.1155/2022/9538138
22. Luc M, Corriveau H, Boire G, Filiatrault J, Beaulieu M-C, Gaboury I. Patient-related factors associated with adherence to recommendations made by a fracture liaison service: a mixed-method prospective study. Int J Environ Res Public Health. 2018;15(5):944. doi:10.3390/ijerph15050944
23. Muhammad Haskani NH, Ming LC, Dhaliwal JS, et al. Diabetes mellitus and its therapy in Brunei Darussalam - a critical revisit. Patient Prefer Adherence. 2023;17:1131–1136. doi:10.2147/PPA.S366152
24. Wakui N, Ozawa M, Yanagiya T, et al. Factors associated with medication compliance in elderly patients with type 2 diabetes mellitus: a cross-sectional study. Front Public Health. 2021;9:771593. doi:10.3389/fpubh.2021.771593
25. Belmin J, Khellaf L, Pariel S, et al. Validation of the French version of the vulnerable elders survey-13 (VES-13). BMC Med Res Methodol. 2020;20(1):21. doi:10.1186/s12874-020-0910-x
26. Hasani-Ranjbar S, Jafari-Adli S, Payab M, et al. Association of osteoporosis with anthropometric measures in a representative sample of Iranian adults: the Iranian multicenter osteoporosis study. Int J Prev Med. 2019;10:157. doi:10.4103/ijpvm.IJPVM_326_17
27. Pan L, Wang C, Cao X, Zhu H, Luo L. Unmet healthcare needs and their determining factors among unwell migrants: a comparative study in Shanghai. Int J Environ Res Public Health. 2022;19(9):5499.
28. Wang L, Di X, Yang L, Dai X. Differences in the potential accessibility of home-based healthcare services among different groups of older adults: a case from Shaanxi Province, China. Healthcare. 2020;8(4):452.
29. AlMulla A, Mamtani R, Cheema S, et al. Epidemiology of tobacco use in Qatar: prevalence and its associated factors. PLoS One. 2021;16(4):e0250065. doi:10.1371/journal.pone.0250065
30. Nikodem K, Ćurković M, Borovečki A. Trust in the healthcare system and physicians in croatia: a survey of the general population. Int J Environ Res Public Health. 2022;19(2):993. doi:10.3390/ijerph19020993
31. Hao H, Nicholas S, Xu L, Leng A, Sun J, Han Z. Productivity losses due to diabetes in Urban Rural China. Int J Environ Res Public Health. 2022;19(10):5873. doi:10.3390/ijerph19105873
32. Hu X, Liu Z, Zhou H, Fang J, Lu H. Deep HT: a deep neural network for diagnose on MR images of tumors of the hand. PLoS One. 2020;15(8):e0237606. doi:10.1371/journal.pone.0237606
33. Andreou A, Dhand A, Vassilev I, Griffiths C, Panzarasa P, De Simoni A. Understanding online and offline social networks in illness management of older patients with asthma and chronic obstructive pulmonary disease: mixed methods study using quantitative social network assessment and qualitative analysis. JMIR Form Res. 2022;6(5):e35244. doi:10.2196/35244
34. Tebelu DT, Tadesse TA, Getahun MS, Negussie YM, Gurara AM. Hypertension self-care practice and its associated factors in Bale Zone, Southeast Ethiopia: a multi-center cross-sectional study. J Pharm Policy Pract. 2023;16(1):20. doi:10.1186/s40545-022-00508-x
35. Chevalley T, Brandi ML, Cavalier E, et al. How can the orthopedic surgeon ensure optimal vitamin D status in patients operated for an osteoporotic fracture? Osteoporos Int. 2021;32(10):1921–1935. doi:10.1007/s00198-021-05957-9
36. Pei F, Zhao R, Li F, Chen X, Guo K, Zhu L. Osteonecrosis of femoral head in young patients with femoral neck fracture: a retrospective study of 250 patients followed for average of 7.5 years. J Orthop Surg Res. 2020;15(1):238. doi:10.1186/s13018-020-01724-4
37. Cheng P, Ying F, Li Y. Effects of different concentrations of ropivacaine lumbar plexus-sciatic nerve block on recovery from anesthesia, postoperative pain and cognitive function in elderly patients with femoral neck fracture. Evid Based Complement Alternat Med. 2022;2022:4096005. doi:10.1155/2022/4096005
38. Hu Y, Shi H, Wang F, Ren G, Cheng R, Zhang Z. Functional outcomes of extra-articular scapula fracture fixation with distal humeral Y-type locking plate: a retrospective study. J Orthop Surg Res. 2019;14(1):176. doi:10.1186/s13018-019-1205-y
39. LeBoff MS, Greenspan SL, Insogna KL, et al. The clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2022;33(10):2049–2102.
40. Sabri SA, Chavarria JC, Ackert-Bicknell C, Swanson C, Burger E. Osteoporosis: an update on screening, diagnosis, evaluation, and treatment. Orthopedics. 2023;46(1):e20–e26. doi:10.3928/01477447-20220719-03
41. Cheng KC, Lau KMK, Cheng ASK, et al. Use of mobile app to enhance functional outcomes and adherence of home-based rehabilitation program for elderly with Hip fracture: a randomized controlled trial. Hong Kong Physiother J. 2022;42(2):99–110. doi:10.1142/S101370252250010X
42. Tran-Nguyen K, Berger C, Bennett R, Wall M, Morin SN, Rajabiyazdi F. Mobile app prototype in older adults for postfracture acute pain management: user-centered design approach. JMIR Aging. 2022;5(4):e37772. doi:10.2196/37772
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude, Practice, and Awareness Regarding Disease Management Among Patients with Chronic Lower Limb Ischemia: A Cross-Sectional Study
Wang F, Chen X, Jiang Y, Liu Y, Li Y, Yang X, Zhang H, Gan X
Patient Preference and Adherence 2026, 20:566461
Published Date: 13 January 2026