Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitude, Practice, and Awareness Regarding Disease Management Among Patients with Chronic Lower Limb Ischemia: A Cross-Sectional Study
Authors Wang F, Chen X, Jiang Y, Liu Y, Li Y, Yang X, Zhang H, Gan X
Received 9 September 2025
Accepted for publication 30 December 2025
Published 13 January 2026 Volume 2026:20 566461
DOI https://doi.org/10.2147/PPA.S566461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fei Wang, Xue Chen, Yafei Jiang, Yueqin Liu, Yi Li, Xiaofeng Yang, Hui Zhang, Xiuni Gan
Vascular & Hernia & Abdorminal Wall Surgery Department, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Xiuni Gan, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China, Tel +8613883309318, Email [email protected]
Purpose: This study aims to investigate knowledge, attitude, practice (KAP), and disease awareness among patients with chronic lower limb ischemia.
Patients and Methods: This cross-sectional study was conducted between November 2024 and January 2025 at the Second Affiliated Hospital of Chongqing Medical University. A self-administered questionnaire, with good internal consistency (Cronbach’s α = 0.917), was used to assess knowledge, attitude, and practice, while the Brief Illness Perception Questionnaire measured awareness.
Results: Among 491 participants (73.7% male), most were aged 70– 79 years (38.7%), and 41.5% had a primary school education or below. Nearly half (48.1%) had ischemia for 2– 3 years. The mean knowledge, attitude, practice, and awareness scores were 8.71 ± 5.42, 31.55 ± 2.92, 31.47 ± 4.88, and 31.68 ± 5.03, respectively. Significant correlations were observed between knowledge and attitude (r = 0.513, P < 0.001), practice (r = 0.448, P < 0.001), and awareness (r = 0.175, P < 0.001). Attitude also correlated with practice (r = 0.331, P < 0.001) and awareness (r = 0.227, P < 0.001). Path analysis indicated that knowledge directly affected attitude (β = 0.522, P < 0.001), awareness (β = 0.164, P < 0.001), and practice (β = 0.356, P < 0.001), while attitude directly affected practice (β = 0.159, P < 0.001), knowledge also indirectly affected practice through attitude (β = 0.083, P = 0.001).
Conclusion: Patients with chronic lower limb ischemia showed limited knowledge but generally maintained positive attitudes, proactive practices, and moderate awareness toward disease management. Enhancing awareness alongside knowledge may help improve overall self-management and clinical outcomes.
Keywords: chronic limb-threatening ischemia, disease management, knowledge, attitude, practice, endovascular treatment, patient education, cross-sectional study
Introduction
Peripheral artery disease (PAD) is a chronic atherosclerotic condition affecting the lower extremities, impacting over 200 million individuals worldwide aged 25 and older as of 2015.1 The most severe form of PAD, chronic lower limb ischemia, occurs when reduced blood flow manifests in ischemic symptoms that persist over time.2 Early stages often present as intermittent claudication, numbness, or coldness in the legs, while advanced stages progress to chronic limb-threatening ischemia (CLTI), characterized by persistent rest pain, gangrene, or lower limb ulceration lasting more than two weeks.3 Among patients with lower-extremity PAD, 1% to 2% progress to CLTI. Without timely revascularization, approximately 35% of CLTI patients will require amputations, and 33% will die within five years.4 Epidemiological data indicate that Europe experiences an incidence of 500–1,000 new CLTI cases per million population annually.5 Therefore, increasing awareness and promoting early intervention for chronic lower limb ischemia is essential for improving patient outcomes. In China, recent national estimates based on the Global Burden of Disease 2019 data have shown a substantial and rising burden of peripheral artery disease, with China accounting for nearly one-quarter of global new and prevalent cases and exhibiting increasing disability-adjusted life years (DALYs) and mortality particularly among older adults and diabetic populations.6 This regional trend underscores the urgent need to improve awareness and disease management strategies tailored to local healthcare access and education disparities. Based on the KAP framework, we hypothesized that greater knowledge would be associated with more positive attitudes and improved self-management practices among patients with chronic lower limb ischemia.7–9
Significant advancements in treatment approaches over the past decades include the development of endovascular techniques such as drug-coated balloons and stents, improvements in surgical revascularization procedures, and enhanced wound care protocols.10,11 However, no invasive treatment guarantees limb salvage; up to 25% of patients may still undergo major amputations despite revascularization efforts.11 Effective disease management for patients with chronic lower limb ischemia extends beyond medical interventions to include crucial self-management components. These components encompass regular monitoring of limb symptoms, adherence to medication regimens, lifestyle modifications (such as smoking cessation and exercise), proper foot care, and vigilant attention to wound prevention.12 Additionally, managing comorbid conditions like diabetes and hypertension, maintaining proper nutrition, and attending scheduled follow-up appointments are vital elements of comprehensive care for chronic lower limb ischemia.13
The Knowledge, Attitude, and Practice (KAP) survey is a valuable diagnostic tool for assessing a population’s understanding, beliefs, and behaviors regarding specific health issues. It operates on the principle that knowledge shapes attitudes, which in turn influence practices, making it particularly useful for exploring health literacy.7 This study is conceptually guided by the Health Belief Model, which emphasizes that individuals’ health-related behaviors are influenced by their knowledge, perceived severity and susceptibility, and perceived benefits of action. Within this framework, the KAP approach provides a practical way to evaluate these constructs at the population level. Patients with chronic lower limb ischemia are typically older and often present with multiple comorbidities, resulting in increased risks of mortality and limb loss even after revascularization.14 Consequently, research focused on this high-risk group is crucial for improving clinical outcomes, reducing disability and mortality, and guiding the development of individualized treatment plans. Such efforts could significantly enhance the quality of life and long-term prognosis for these patients. A previous study provided insights into CLTI patients’ perceptions of shared decision-making, treatment, and care,15 but systematic research on the challenges, perceptions, and attitudes of patients with chronic lower limb ischemia is limited in China. Recent findings highlight several clinical practice issues, including insufficient knowledge, a lack of routine nutritional care, and the absence of standardized assessment tools for nutrition, despite the general acknowledgment of its importance in improving outcomes for patients with chronic lower limb ischemia.16 However, little is known about how patients with chronic lower limb ischemia in China perceive their condition and manage it in daily life. In particular, no studies have systematically examined patients’ knowledge, attitudes, practices, and awareness within a unified framework. Specifically, this study combines a KAP survey with the Brief Illness Perception Questionnaire and uses path analysis to examine the relationships among knowledge, attitude, practice, and awareness in a Chinese cohort of patients with chronic lower limb ischemia.
Therefore, this study aims to investigate knowledge, attitude, and practice regarding disease management among patients with chronic lower limb ischemia. We hypothesized that higher levels of knowledge would be positively associated with more favorable attitudes and better self-management practices, and that attitude would mediate the relationship between knowledge and practice.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted between November 2024 and January 2025 at the Second Affiliated Hospital of Chongqing Medical University, targeting patients diagnosed with chronic lower limb ischemia. Ethical approval for the study was obtained from the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (Approval number: #2024-78). Additionally, informed consent was secured from all participants prior to their inclusion in the study.
The inclusion criteria were as follows: participants had to be over 18 years of age, have a confirmed diagnosis of limb ischemia,12 possess the ability to complete the questionnaire independently or with assistance, and voluntarily agree to participate by signing informed consent. Exclusion criteria included withdrawal from the study or revocation of informed consent, the presence of neuropsychiatric disorders that impaired comprehension of the questionnaire, or being in a state of acute limb ischemia, clinical instability, or lack of effective treatment. Participants were recruited through convenience sampling in both the outpatient clinic and inpatient wards of the vascular surgery department. Eligibility was confirmed using electronic medical records, and patients with documented cognitive impairment were excluded. All participants were required to demonstrate the ability to understand the questionnaire content. Oral consent was obtained from all participants. For online questionnaires, anonymization and encrypted data storage were applied, and no identifiable information was collected. No incentives were provided to avoid influencing participation or introducing selection bias. Data were collected in both the vascular surgery outpatient clinic and inpatient wards of the Second Affiliated Hospital of Chongqing Medical University.
Questionnaire
The questionnaire used in this study was developed de novo based on previous literature and international guidance on chronic limb-threatening ischemia,3,12,17 as no standardized KAP instrument specific to chronic lower limb ischemia was available. Following the completion of an initial draft, a pilot survey was conducted with 30 valid responses to assess the reliability of the questionnaire, which achieved an overall Cronbach’s α coefficient of 0.917, indicating excellent internal consistency. Item–total correlations for the knowledge, attitude, and practice items ranged from approximately −0.41 to 0.67, suggesting acceptable discrimination at the item level. To ensure content validity, the initial draft was reviewed independently by two vascular surgeons and one senior nurse specializing in chronic limb ischemia management. The expert panel assessed each item for clinical relevance, clarity, and redundancy; items that were judged unclear or unnecessary were revised. Because data were collected at a single time point, test–retest reliability was not evaluated and intraclass correlation coefficients were not calculated.
The finalized questionnaire, designed in Chinese, comprised five sections: demographic information, knowledge, attitude, practice, and awareness. The demographic section collected data on participants’ age, gender, residence, education level, job type, monthly income per capita, duration of chronic lower limb ischemia, causes of limb ischemia, comorbid conditions, and treatment history.
The knowledge dimension consisted of 10 items, with responses categorized as “very familiar” (2 points), “somewhat familiar” (1 point), and “not familiar” (0 points), resulting in a total possible score range of 0–20. The attitude dimension included 9 items evaluated using a five-point Likert scale, where positively worded items were scored from “strongly agree” (5 points) to “strongly disagree” (1 point), and negatively worded items were reverse-scored. The total score for the attitude dimension ranged from 9 to 45 points. Additionally, items 10–17 specifically assessed participants’ disease perception (defined as awareness in this study) and were taken from the Brief Illness Perception Questionnaire (Brief IPQ), a widely validated tool that evaluates patients’ cognitive and emotional representations of illness.18 The Brief IPQ includes dimensions such as consequences, timeline, personal control, treatment control, identity, concern, understanding, and emotional response. Each B-IPQ item was scored on a 0–10 scale, with higher scores indicating stronger perceived impact, concern, or understanding depending on the dimension measured. All items were scored in the same direction (no reverse-scored items), and the eight items were summed to generate a total awareness score (range 0–80), with higher scores reflecting greater perceived illness impact and awareness. In our sample, the Brief Illness Perception Questionnaire demonstrated acceptable internal consistency, with a Cronbach’s α of 0.7466, supporting its use as an overall awareness construct in this population. No reverse-scored items were included, and scores were analyzed at the item level rather than as a composite total. Unlike the knowledge dimension, which measures factual understanding of disease-related information, the awareness dimension assessed patients’ cognitive and emotional perceptions of their illness using the Brief IPQ. The practice dimension consisted of 8 items scored on a scale of 1–5, ranging from “never” to “always,” with a total possible score range of 8–40. Participants were classified as having “good” knowledge, attitude, and practice if their respective scores exceeded 70% of the maximum possible score for each dimension.8 This threshold was selected based on commonly used practices in KAP studies, where scores above 70% of the maximum are considered to reflect a high level of understanding or engagement. In our study, “good” knowledge, attitude, and practice refer to participants who reached this level relative to the total possible score of each dimension. In addition, all analyses of associations were conducted using the original continuous KAP scores.
Questionnaire Distribution
The questionnaire was administered through both online and offline methods to ensure comprehensive data collection. The online survey utilized an electronic questionnaire created via Wenjuanxing, which was distributed through a QR code. Participants accessed the questionnaire either by scanning the QR code on-site or via a one-on-one WeChat invitation. To ensure completeness, all questions were set as mandatory.
For the offline paper-based survey, questionnaires were distributed directly in outpatient clinics or hospital wards. Patients who were unable to complete the questionnaire independently received assistance from either nurses or family members. To maintain the integrity of the responses, assistants were instructed to provide only technical support without offering any form of guidance or influence. To reduce potential bias during assisted completion, standardized scripts and unified terminology were used by research nurses. Only a small number of participants required partial assistance, mainly due to dialect, hearing difficulty, or poor literacy. Because this group was small and assistance was limited to technical support, we did not conduct separate statistical comparisons between assisted and self-completed questionnaires. A very small number of illiterate or visually impaired patients unable to complete the questionnaire were excluded. Because all items were mandatory in both paper and electronic formats, there were no missing values in the final analytic dataset, and no imputation was performed. Patient information, including name, diagnosis, and contact details, was obtained through the hospital electronic medical record system after patients visited the hospital. Eligible participants were then approached either face-to-face in the vascular clinic or by telephone. All data were collected by trained research nurses, who explained the study purpose and questionnaire content, obtained informed consent, and, when needed, assisted patients in completing the questionnaire.
Sample Size Calculation
For this cross-sectional study, the required sample size was estimated using the standard formula n = Z_(1−α/2)^2 × p × (1 − p) / δ^2, where α = 0.05, Z_(1−α/2) = 1.96, p was set at 0.5 to maximize the required sample size, and δ (margin of error) was set at 0.05. The theoretical sample size was 480, including an extra 20% to account for potential dropouts. This estimation was performed as an a priori calculation using the standard formula for cross-sectional studies. Although a formal power analysis based on effect size was not feasible due to the lack of prior data, the final sample size (n = 491) exceeded the planned minimum sample size.
Statistical Methods
Statistical analysis was performed using STATA 18.0 (StataCorp, College Station, TX, USA). Continuous variables were presented as means and standard deviations (SD), while categorical data were expressed as frequencies and percentages (n, %). The normality of continuous data was assessed using Shapiro–Wilk tests prior to the selection of appropriate statistical tests. Shapiro–Wilk tests showed that the total knowledge, attitude, and practice scores were non-normally distributed overall and within baseline subgroups (all P < 0.001); therefore, group comparisons for these scores used non-parametric methods (Mann–Whitney U-tests for two groups and Kruskal–Wallis tests for more than two groups). For variables with more than two categories, significant Kruskal–Wallis tests were followed by post hoc pairwise comparisons using Dunn’s test with Bonferroni correction for multiple testing. For continuous variables with a normal distribution, comparisons between two groups were conducted using independent samples t-tests, while one-way analysis of variance (ANOVA) was applied for comparisons involving three or more groups. For non-normally distributed continuous variables, the Mann–Whitney U-test was used for two-group comparisons, and the Kruskal–Wallis test was employed for comparisons across three or more groups. Spearman correlation analysis was conducted to evaluate the relationships between knowledge, attitude, and practice (KAP) scores. Additionally, path analysis was performed to examine the hypothesized relationships among these variables: (H1) knowledge directly influences attitude, (H2) knowledge directly impacts practice, and (H3) knowledge indirectly affects practice through attitude. In this path model, 10 parameters were estimated (five path coefficients, one variance/covariance term for the exogenous variable, three residual variances, and one residual covariance for the endogenous variables); with 491 participants, the ratio of participants to parameters was approximately 49:1, which is well above commonly recommended minimums (eg, 10–20 participants per parameter) and suggests adequate sample size to detect moderate associations. Path analysis was implemented in Stata 18 using structural equation modelling procedures. Parameter estimation used the robust maximum likelihood estimator (MLR). Missing data in the variables included in the model were handled using full information maximum likelihood (FIML); however, there were no missing values in the observed variables used for the structural equation model, so FIML yielded the same estimates as standard maximum likelihood. Model fit was assessed using the chi-square statistic with degrees of freedom and P-value, the root mean square error of approximation (RMSEA) with its 90% confidence interval, as well as the Tucker–Lewis Index (TLI), the Incremental Fit Index (IFI), the Normed Fit Index (NFI), the Comparative Fit Index (CFI), and the Standardized Root Mean Square Residual (SRMR). We considered CFI, NFI, and IFI values ≥ 0.90 and SRMR values ≤ 0.08 as general benchmarks for acceptable fit, while lower RMSEA values were interpreted as indicating better fit without applying a strict single cut-off because of the small degrees of freedom and simple structure of the model. Indirect (mediation) effects and their 95% confidence intervals were evaluated using nonparametric bootstrap resampling (5,000 samples) with bias-corrected confidence intervals. Subgroup path analysis was adjusted for education level and urban/rural residence.
Additionally, as a sensitivity analysis, we fitted separate univariate and multivariable logistic regression models for dichotomised knowledge, attitude, and practice outcomes (using median splits of the total scores), including age, sex, residence (rural/urban/suburban), education, occupation, household income, duration of chronic lower limb ischemia, and treatment variables (medication, surgery, and endovascular therapy) as covariates. A two-tailed P-value of less than 0.05 was considered statistically significant.
Results
Basic Information
Initially, a total of 498 questionnaires were collected. One questionnaire with missing data in the knowledge dimension and six with logical inconsistencies were excluded, leaving 491 valid questionnaires for analysis. Questionnaires with missing or inconsistent responses were excluded listwise, and no imputation procedures were applied. Among them, 190 (38.7%) were aged 70–79 years, 362 (73.7%) were male, 204 (41.5%) had a primary school education or below, 227 (46.2%) had a monthly income per capita of 2,000–4,999 CNY, 236 (48.1%) had suffered from chronic lower limb ischemia for 2–3 years, 420 (85.5%) were due to arteriosclerosis obliterans, 294 (59.9%) also suffered from hypertension, 418 (85.1%) received medication, and 368 (74.9%) underwent endovascular treatment.
The mean KAP scores were 8.71 ± 5.42 (possible range: 0–20), 31.55 ± 2.92 (possible range: 9–45), and 31.47 ± 4.88 (possible range: 8–40), respectively. Analyses of demographic characteristics showed that participants’ KAP scores varied significantly by gender (P < 0.001, P = 0.003, P < 0.001), residence (P < 0.001 for all), education (P < 0.001 for all), job type (P < 0.001 for all), monthly income per capita (P < 0.001 for all), and endovascular treatment status (P < 0.001, P < 0.001, P = 0.001). Additionally, knowledge scores varied significantly by age (P = 0.042) and treatment status (P < 0.001). Attitude scores varied significantly by medication status (P = 0.001) (Table 1). Moreover, clear subgroup differences were observed: participants living in urban areas and those with higher education levels had notably higher knowledge, attitude, and practice scores compared with those from rural areas or with lower educational attainment (Table 1). Detailed test statistics for the subgroup comparisons, including Dunn’s post hoc tests with Bonferroni-corrected P values, are presented in Supplementary Table 1.
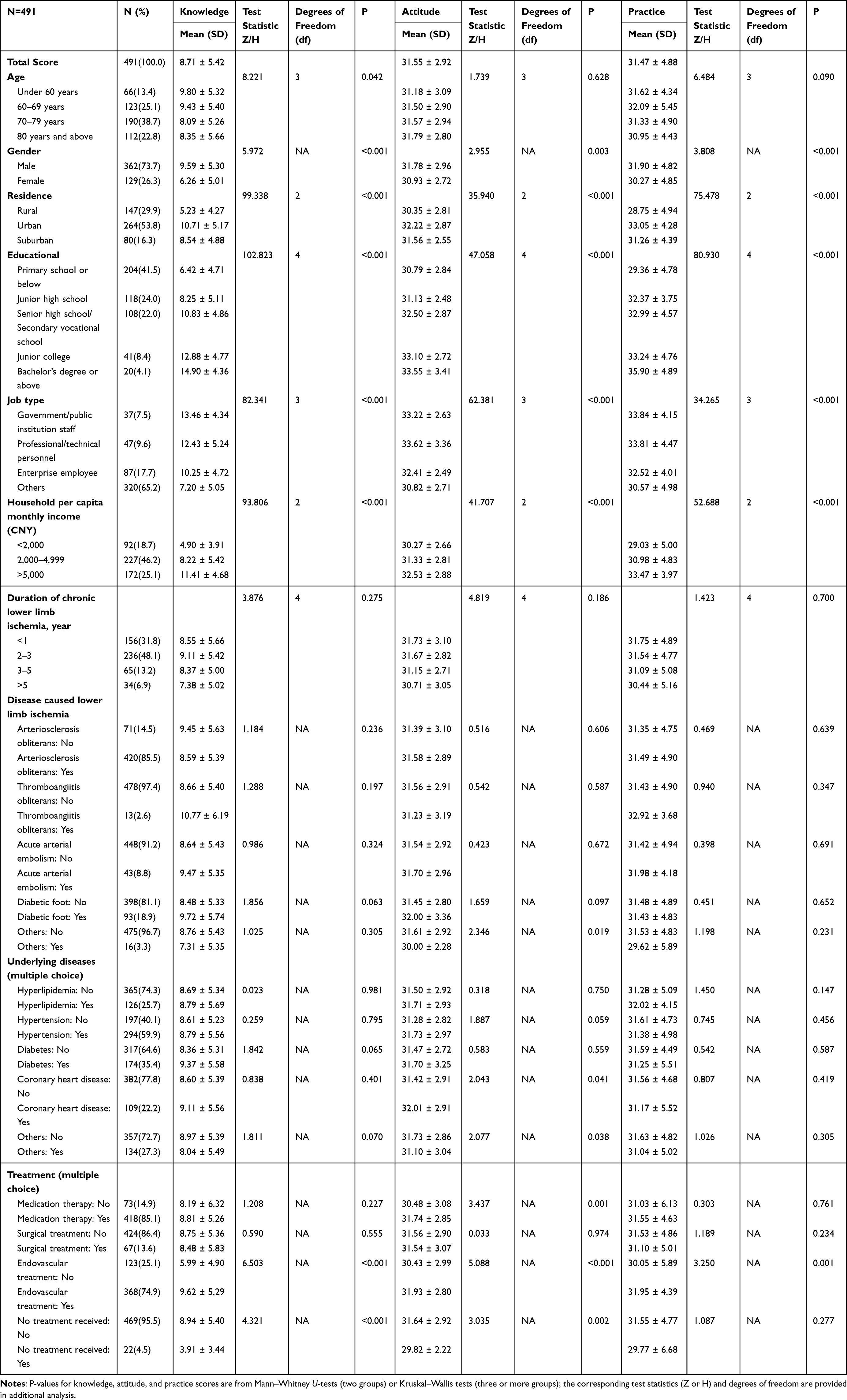 |
Table 1 Basic Characteristics |
Kap
The distribution of knowledge dimensions showed that the three questions with the highest number of participants choosing the “Not clear” option were “Patients with severe lower limb ischemia can consider revascularization treatment.” (K9) with 59.3%, “Patients with chronic lower limb ischemia should undergo antithrombotic therapy.” (K4) with 54.6%, and
Revascularization is an important treatment for CLTI patients to relieve symptoms and promote wound healing, including surgical treatment and endovascular therapy.
(K8) with 54.4% (Supplementary Table 2).
Responses to the attitude dimension showed that 19.8% strongly agreed and 65.4% agreed that chronic lower limb ischemia has a significant impact on their work (A2), 17.9% were very concerned and 66.8% were concerned that chronic lower limb ischemia will relapse after treatment (A7), and 5.5% strongly agreed and 23.6% agreed that chronic lower limb ischemia is unrelated to lifestyle factors such as prolonged sitting and smoking (A3) (Supplementary Table 3).
Responses to the Disease Perception Scale showed that 9% believed that the disease had severely impacted their lives (D1), 13.8% believed that the disease would last forever (D2), 7.3% reported experiencing many severe symptoms after being diagnosed with the disease (D5), and 2% stated that the disease had greatly impacted their emotions (D8) (Supplementary Table 4).
Responses to the practice dimension revealed relatively low engagement in active learning and consultation behaviors. Specifically, when asked about actively learning about chronic lower limb ischemia management through various media (P6), 33% reported doing so rarely and 15.7% never did. Similarly, regarding actively consulting healthcare professionals about disease management (P7), 18.5% rarely sought consultation, and 5.5% never did (Supplementary Table 5).
Correlations Between KAP
In the correlation analysis, significant positive correlations were found between knowledge and attitude (r = 0.513, 95% CI 0.445–0.576, P < 0.001), knowledge and practice (r = 0.448, 95% CI 0.375–0.516, P < 0.001), and knowledge and awareness (r = 0.230, 95% CI 0.144–0.312, P < 0.001). Significant positive correlations were also observed between attitude and practice (r = 0.331, 95% CI 0.250–0.407, P < 0.001) and between attitude and awareness (r = 0.273, 95% CI 0.189–0.353, P < 0.001) (Supplementary Table 6). These correlation coefficients were interpreted as effect sizes, and 95% confidence intervals for the corresponding standardized path coefficients are reported in Supplementary Table 6.
Interactions Between KAP
The path model showed acceptable fit on the incremental indices, with IFI = 0.956, NFI = 0.953, CFI = 0.956, and an SRMR of 0.046. The full set of model fit indices, including the Tucker–Lewis Index (TLI), RMSEA with its 90% confidence interval, and the chi-square statistic with degrees of freedom and P-value (TLI = 0.734; RMSEA = 0.166, 90% CI 0.098–0.246; χ2(6) = 309.841, P < 0.001), is summarized in Supplementary Table 7. Mediation analysis showed that knowledge directly affected attitude (β = 0.522, P < 0.001), awareness (β = 0.164, P < 0.001), and practice (β = 0.356, P < 0.001). Meanwhile, attitude directly affected practice (β = 0.159, P < 0.001). Further, knowledge indirectly affected practice (β = 0.083, P = 0.001) (Table 2 and Figure 1). All coefficients shown in Figure 1 are standardized estimates. Overall, patients with better knowledge tended to show stronger motivation, more active behaviors, and clearer understanding of their illness. The model results indicated that knowledge was associated with both attitude and practice, partly through the influence of attitude itself.
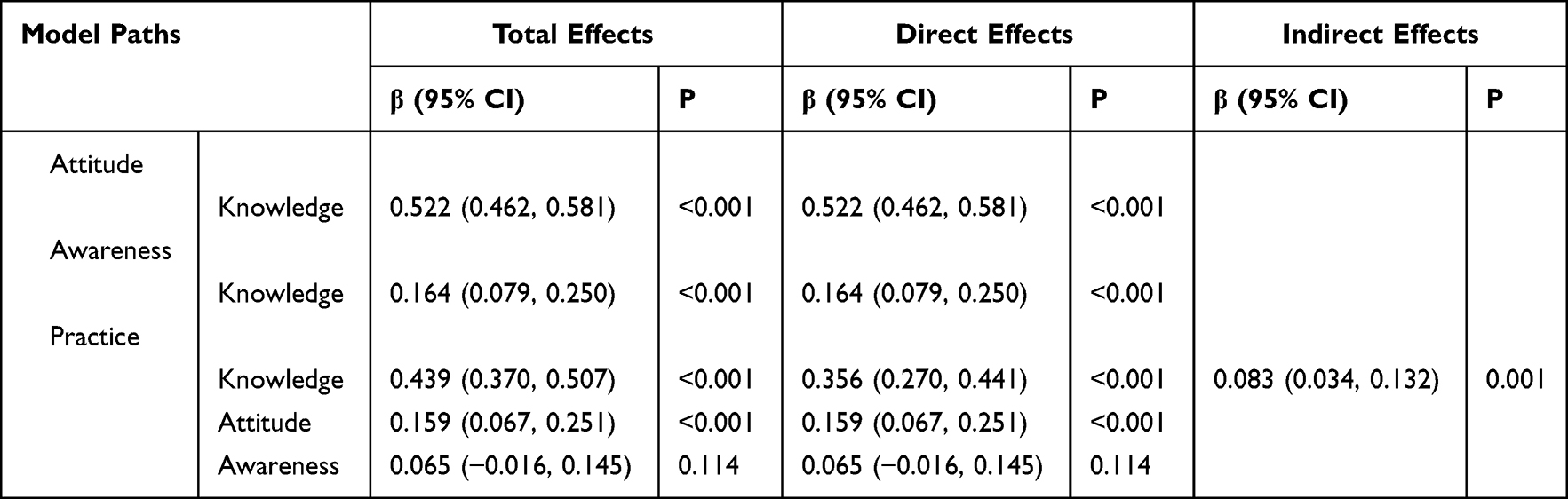 |
Table 2 Direct and Indirect Effects in Path Analysis |
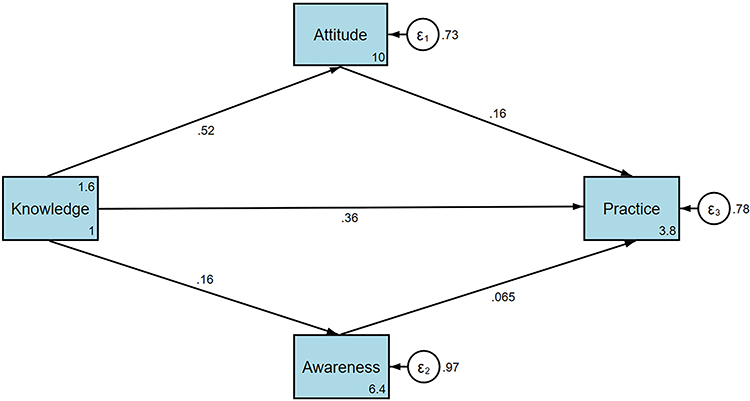 |
Figure 1 Path diagram with standardized path coefficients for the relationships among knowledge, attitude, awareness, and practice. Solid arrows indicate statistically significant paths (P < 0.001); the dashed arrow indicates the non-significant path from awareness to practice. All coefficients are standardized estimates. |
A subgroup path analysis adjusted for education level and urban/rural residence showed that the pattern of associations remained similar after this adjustment (Supplementary Figure 1 and Supplementary Table 8).
Multivariable Logistic Regression
In multivariable logistic regression analyses adjusting for age, sex, residence, education, occupation, household income, duration of chronic lower limb ischemia, and treatment variables, higher knowledge scores remained independently associated with higher odds of better attitude and practice, whereas the association between attitude and practice was attenuated and became non-significant after adjustment. Specifically, each one-point increase in the knowledge score was associated with higher odds of having an attitude score at or above the median (adjusted OR = 1.178, 95% CI 1.120–1.240) and a practice score at or above the median (adjusted OR = 1.110, 95% CI 1.052–1.170), while the adjusted association between attitude and practice was weaker and did not reach statistical significance (adjusted OR = 1.072, 95% CI 0.982–1.171). These findings were consistent with the pattern observed in the correlation and path analyses, and detailed results are presented in Supplementary Tables 9–11.
Discussion
Patients with chronic lower limb ischemia demonstrated insufficient knowledge yet exhibited generally positive attitude and proactive practice toward disease management. These findings underscore the need for targeted educational interventions Patients with chronic lower limb ischemia demonstrated insufficient knowledge but generally positive attitudes and proactive practices, suggesting the need for targeted educational interventions to enhance disease understanding and management.
This study highlights the critical gap between knowledge and practice among patients with chronic lower limb ischemia. While patients exhibited positive attitude and proactive practice, their knowledge about the condition remained insufficient. This pattern mirrors findings in chronic disease research, where knowledge gaps persist despite patients’ recognition of disease severity and their intent to adhere to management strategies.19 Similar findings have been reported in recent studies. In a cross-sectional survey among high-risk individuals for chronic obstructive pulmonary disease in China, Zhao et al (2023)20 found that participants had limited understanding of preventive measures but maintained active attitudes toward health and self-care. This supports the observation that positive attitudes can coexist with insufficient knowledge across chronic disease populations. The observed knowledge deficits in this study—particularly in areas such as the importance of revascularization, lifestyle modifications, and postoperative care—are consistent with the literature, which has frequently highlighted the challenges of effectively conveying complex medical concepts to diverse patient populations.21 These findings underscore the intricate relationship between knowledge, attitude, and practice, revealing that while attitude can drive initial engagement with care, adequate knowledge is essential to sustain meaningful, long-term management behaviors. One possible explanation for this pattern is that patients often follow physicians’ instructions even without a full understanding of the disease itself. In China, long-term doctor–patient relationships and repeated outpatient visits may help reinforce treatment routines and self-care behaviors. Many patients also learn practical management habits through direct experience—such as pain control, limb care, and medication adherence—rather than from formal knowledge. In addition, family members frequently assist elderly patients in daily management, which may further support good practice despite limited health literacy.
The positive correlations between knowledge, attitude, and practice observed in this study align with existing evidence that knowledge serves as a cornerstone for fostering positive attitude and encouraging proactive practice.22 However, the moderate strength of these relationships, as shown by statistical analyses, suggests that other factors, such as socio-cultural influences, access to healthcare, and individual health literacy levels, also play a significant role. Similar patterns have been observed in populations managing other chronic conditions, where educational interventions have shown limited success without addressing broader systemic and psychological barriers.23 Additionally, the role of awareness, as measured through the Disease Perception Scale, reveals an important but complex dynamic. While knowledge positively influenced awareness, the lack of a significant direct effect of awareness on practice highlights the difficulty in translating awareness into actionable behaviors without concurrent improvements in knowledge and attitudinal support.9 These findings are consistent with the broader literature suggesting that heightened disease awareness alone often leads to anxiety rather than constructive action unless accompanied by targeted educational and psychosocial interventions.9
The findings regarding the distribution of knowledge, attitude, and practice further reflect systemic challenges in healthcare delivery and patient education. The disparities observed in knowledge scores across demographic groups, particularly by residence and education level, are consistent with studies showing that rural and less-educated populations often face significant barriers to accessing and comprehending health information.24 In our subgroup analysis, the disparities observed in knowledge scores across demographic groups, particularly by residence and education level, are consistent with previous studies and were also evident in our findings, as participants from urban regions and those with higher education achieved better KAP scores. These disparities may result from limited access to healthcare resources, inadequate patient–physician communication, or cultural attitudes that deprioritize proactive health management, and they are consistent with qualitative findings in PAD populations showing that social determinants such as education, income, and access to vascular services shape patients’ understanding and disease management.25,26 For example, similar studies in chronic disease management have found that patients in urban settings tend to have better knowledge and adherence outcomes due to greater availability of educational programs and healthcare infrastructure.27 These patterns emphasize the need for culturally tailored educational initiatives that account for varying levels of health literacy and access to care.
The findings reveal significant knowledge gaps among patients with chronic lower limb ischemia, particularly regarding treatment outcomes and management requirements. Notable misconceptions, such as the belief that revascularization eliminates the risk of recurrence, could potentially undermine long-term outcomes. This trend reflects a well-documented challenge in chronic disease care, where patients often rely on incomplete or overly optimistic assumptions about treatment efficacy.28 Addressing these misconceptions requires clear, consistent, and reinforced messaging from healthcare providers, particularly during critical junctures such as treatment planning and follow-up consultations.29 Regarding patient attitudes, our findings demonstrate generally positive perceptions about the importance of managing chronic lower limb ischemia and adhering to treatment plans. This is consistent with broader literature indicating that chronic disease patients often recognize the severity of their conditions.30 The positive attitudes observed suggest a strong foundation for implementing educational interventions to address the aforementioned knowledge gaps.
The patterns observed in practice, such as high adherence to medical advice but limited engagement with educational resources, echo findings in studies of other chronic conditions, where structural and systemic barriers often impede patient engagement beyond immediate clinical settings.31 For example, limited time during consultations, insufficient follow-up mechanisms, and a lack of easily accessible educational materials have been cited as reasons for poor patient engagement with self-directed learning.32 These systemic issues are compounded by socio-cultural factors, such as mistrust of healthcare providers or reliance on non-professional sources of health information, which can further hinder effective disease management.33
To address these gaps, healthcare systems must implement multifaceted interventions that go beyond traditional patient education. First, healthcare providers should adopt a more proactive approach to patient education, incorporating tailored, multi-platform strategies to ensure that information is accessible, understandable, and actionable for patients with diverse backgrounds. For instance, community-based programs leveraging local health workers or patient support groups could help bridge gaps in rural or underserved areas by fostering trust and providing culturally relevant education.14 Additionally, integrating health literacy training into routine care, such as through visual aids, digital tools, or brief educational videos, can enhance patient comprehension and retention of key information.34
In this context, education programmes for patients with chronic lower limb ischemia should at least include core modules on basic disease concepts and warning signs, the purpose and limitations of revascularization, lifestyle modification (such as smoking cessation, limb protection and appropriate physical activity), and clear instructions on medication use and follow-up schedules after endovascular or surgical treatment. For patients with lower educational attainment, these modules may be delivered using plain-language brochures with simple images, short nurse-led teaching sessions before discharge, and brief telephone or WeChat reminders that are built into routine discharge planning. Future intervention studies could use changes in knowledge scores and the proportion of patients reaching the predefined “good” knowledge threshold, as well as adherence to recommended revascularization follow-up visits, as measurable outcomes.
Healthcare organizations should also focus on enhancing follow-up care through systematic changes. Structured follow-up programs, including regular check-ins via telemedicine or community health visits, can reinforce knowledge and encourage adherence to recommended practice. Moreover, providing incentives for patients to participate in educational workshops or support groups, such as subsidized transportation or small financial rewards, could increase engagement.35 At the provider level, training programs should emphasize communication skills, equipping clinicians with tools to simplify complex medical information and address patient misconceptions effectively. These efforts must be supported by organizational policies that allocate adequate time and resources for patient education during consultations.
In the longer term, healthcare systems should prioritize the development of sustainable educational infrastructure, including partnerships with schools, workplaces, and community organizations, to promote health literacy as a societal norm. Policymakers should also address systemic inequities, such as the availability of healthcare resources in rural areas, by increasing funding for mobile clinics, telehealth initiatives, and public health campaigns.36 Ensuring sustainability will require continuous evaluation of these interventions to adapt to changing healthcare contexts and patient needs. In practical terms, the findings suggest that patient education should be integrated into routine vascular care to help patients recognize early warning signs, manage risk factors, and follow medical advice more effectively. Strengthening follow-up communication between patients and healthcare teams may also support long-term adherence and reduce avoidable complications.
This study has several limitations. First, as this was a cross-sectional study, all reported relationships, including those suggested by the path (mediation) analysis, should be interpreted as associations rather than causal effects, and no temporal ordering between knowledge, attitude, awareness, and practice can be established. Second, the reliance on self-administered questionnaires delivered through an online survey platform and paper forms, with some assisted completion by nurses or family members, may have introduced information and social desirability bias, as participants might have over- or under-reported their actual practice and perceptions and helpers could have unintentionally influenced responses. In addition, although mandatory fields in the electronic questionnaire helped avoid missing data, they may have encouraged some participants to provide hurried or satisficing responses. Third, data were collected over a relatively short period (November 2024–January 2025), and participation was voluntary and based on convenience sampling within a single hospital, so patients who were more health-conscious or cooperative may have been overrepresented, leading to potential selection bias. However, chronic lower limb ischemia is a long-standing condition, and patient knowledge, attitudes, and practices are not expected to vary markedly by season, so substantial seasonality bias is unlikely. Fourth, being a single-center study conducted in a tertiary vascular surgery department, the findings may not fully represent patients from other hospitals or regions with different healthcare access, socioeconomic conditions, or educational backgrounds, and referral patterns to our center may limit generalizability. Moreover, the sample was drawn from a tertiary vascular surgery center with a predominance of male patients (73.7%) and a high proportion of individuals who had undergone endovascular treatment (74.9%), which likely reflects referral of more complex or treatment-seeking cases and may limit generalizability to community or primary-care PAD populations. In addition, we conducted a large number of subgroup comparisons; although Dunn’s tests with Bonferroni correction were applied to control for multiple testing in the post hoc analyses, these analyses were exploratory and the risk of both type I and type II errors cannot be completely ruled out. Fifth, we did not perform additional multivariable or stratified regression or path models by education level or urban/rural residence, so residual confounding by these factors cannot be excluded and should be explored in future studies.
Conclusion
In conclusion, patients with chronic lower limb ischemia demonstrated inadequate knowledge but exhibited generally positive attitude and proactive practice regarding disease management. These findings highlight the need to develop targeted educational strategies that focus on patient knowledge while taking attitudes and current practices into account, and to examine whether such strategies are associated with better self-management and follow-up in future studies. As a next step, a structured education module integrated into discharge counseling and routine vascular follow-up could be designed and tested, for example in a randomized or pragmatic trial, using changes in knowledge scores and adherence to revascularization follow-up as key outcomes. Future studies should include multiple centers and larger, more diverse samples to confirm these findings and to evaluate such interventions. The main limitations of this study include its cross-sectional design, reliance on self-reported questionnaire data (including online administration and some assisted completion), and single-center sampling with a predominantly male, highly treated population, which may limit the generalizability of the findings.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its Supplementary Information files.
Ethics Approval and Informed Consent
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This work was approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (Approval number: #2024-78). Informed consent was secured from all participants prior to their inclusion in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Song P, Rudan D, Zhu Y, et al. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019;7(8):e1020–15. doi:10.1016/S2214-109X(19)30255-4
2. Sobolevskaya EV, Shumkov OA, Smagin MA, et al. Markers of restenosis after percutaneous transluminal balloon angioplasty in patients with critical limb ischemia. Int J Mol Sci. 2023;24(10):9096. doi:10.3390/ijms24109096
3. Conte MS, Bradbury AW, Kolh P, et al. global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1s):S1–S109.e133. doi:10.1016/j.ejvs.2019.05.006
4. Verwer MC, Wijnand JGJ, Teraa M, Verhaar MC, de Borst GJ. Long term survival and limb salvage in patients with non-revascularisable chronic limb threatening ischaemia. Eur J Vasc Endovasc Surg. 2021;62(2):225–232.
5. Roijers JP, Rakké YS, Hopmans CJ, et al. Incidence and risk factors for delirium in elderly patients with critical limb ischaemia. Eur J Vasc Endovasc Surg. 2020;59(4):598–605. doi:10.1016/j.ejvs.2019.11.029
6. Hu Y, Gao J, Zhuo Q, et al. The burden of peripheral artery disease in china from 1990 to 2019 and forecasts for 2030: findings from the global burden of disease study 2019. Int J Public Health. 2024;69:1607352. doi:10.3389/ijph.2024.1607352
7. Shubayr MA, Kruger E, Tennant M. Oral health providers’ views of oral health promotion in Jazan, Saudi Arabia: a qualitative study. BMC Health Serv Res. 2023;23(1):214. doi:10.1186/s12913-023-09170-8
8. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
9. Hu W, Li T, Cao S, Gu Y, Chen L. Influence of nurse-led health education on self-management ability, satisfaction, and compliance of elderly patients with chronic obstructive pulmonary disease based on knowledge, belief, and practice model. Comput Math Methods Med. 2022;2022:1782955. doi:10.1155/2022/1782955
10. Duff S, Mafilios MS, Bhounsule P, Hasegawa JT. The burden of critical limb ischemia: a review of recent literature. Vasc Health Risk Manag. 2019;15:187–208. doi:10.2147/VHRM.S209241
11. Steunenberg SL, de Vries J, Raats JW, et al. Quality of life and traditional outcome results at 1 year in elderly patients having critical limb ischemia and the role of conservative treatment. Vasc Endovascular Surg. 2020;54(2):126–134. doi:10.1177/1538574419885478
12. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6s):3S–125S.e140. doi:10.1016/j.jvs.2019.02.016
13. Farber A, Eberhardt RT. The current state of critical limb ischemia: a systematic review. JAMA Surg. 2016;151(11):1070–1077. doi:10.1001/jamasurg.2016.2018
14. Castro-Dominguez Y, Shishehbor MH. Team-based care in patients with chronic limb-threatening ischemia. Curr Cardiol Rep. 2022;24(3):217–223. doi:10.1007/s11886-022-01643-2
15. Soendergaard SF, Simony A, Christiansen JL, Laursen HS, Dahl M. Patients with chronic limb-threatening ischemia: experiences of their disease, treatment, and care in a cross-sectoral setting. A scoping review. J Vasc Nurs. 2024;42(4):240–250. doi:10.1016/j.jvn.2024.08.002
16. Kolen AM, Jager-Wittenaar H, Geertzen JHB, et al. Perceptions, barriers and facilitators regarding nutritional care for patients with chronic limb threatening ischemia: a focus group study among healthcare professionals. Ann Vasc Surg. 2025;110(Pt B):84–94. doi:10.1016/j.avsg.2024.09.052
17. Troisi N, D’Oria M, Fernandes EFJ, et al. International union of angiology position statement on no-option chronic limb threatening ischemia. Int Angiol. 2022;41(5):382–404. doi:10.23736/S0392-9590.22.04933-1
18. Weinman J, Petrie KJ, Moss-morris R, Horne R. The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychol Health. 1996;11(3):431–445. doi:10.1080/08870449608400270
19. Mechanick JI, Farkouh ME, Newman JD, Garvey WT. Cardiometabolic-based chronic disease, addressing knowledge and clinical practice gaps: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(5):539–555. doi:10.1016/j.jacc.2019.11.046
20. Zhao L, Zhao Q. Knowledge, attitude, and practice toward disease prevention among a high-risk population for chronic obstructive pulmonary disease: a cross-sectional study. Int J Nurs Sci. 2023;10(2):238–244. doi:10.1016/j.ijnss.2023.03.012
21. Larsen CB, Gilstad H. Trust and distrust toward online health information in nurse-patient communication and implications for eHealth literacy. J Commun Healthc. 2023;16(4):412–420. doi:10.1080/17538068.2023.2279397
22. Sadanandan SA, Shreedevi AU, Padmanabha H. Parental KAP and its relation with the quality of life in children with epilepsy. Ann Indian Acad Neurol. 2023;26(4):419–423. doi:10.4103/aian.aian_199_23
23. Shi Y, Wu W. Multimodal non-invasive non-pharmacological therapies for chronic pain: mechanisms and progress. BMC Med. 2023;21(1):372. doi:10.1186/s12916-023-03076-2
24. Hallit S, Zeidan RK, Saade S, et al. Knowledge, attitude and practice of lebanese community pharmacists toward chronic obstructive pulmonary disease. J Epidemiol Glob Health. 2020;10(1):86–95. doi:10.2991/jegh.k.191215.004
25. Rice T, Rosenau P, Unruh LY, Barnes AJ. United states: health system review. Health Syst Transit. 2020;22(4):1–441.
26. Costa D, Ielapi N, Marino P, et al. A qualitative study on the role of social determinants of health in patients with peripheral artery disease. Societies. 2025;15(4):87. doi:10.3390/soc15040087
27. Chan SW. Chronic disease management, self-efficacy and quality of life. J Nurs Res. 2021;29(1):e129. doi:10.1097/JNR.0000000000000422
28. Amdani S, Conway J, George K, et al. Evaluation and management of chronic heart failure in children and adolescents with congenital heart disease: a scientific statement from the American heart association. Circulation. 2024;150(2):e33–e50. doi:10.1161/CIR.0000000000001245
29. Lurie F, Branisteanu DE. Improving chronic venous disease management with micronised purified flavonoid fraction: new evidence from clinical trials to real life. Clin Drug Investig. 2023;43(Suppl 1):9–13. doi:10.1007/s40261-023-01261-y
30. Nash DB. The future of chronic disease management. Popul Health Manag. 2023;26(S1):S2–s3. doi:10.1089/pop.2023.0128
31. Maurer M, Kolkhir P, Pereira MP, et al. Disease modification in chronic spontaneous urticaria. Allergy. 2024;79(9):2396–2413. doi:10.1111/all.16243
32. Abdi Z, Ravaghi H, Sarkhosh S, Nafar H, Khani S, Letaief M. Patient and family engagement in patient safety in the Eastern Mediterranean Region: a scoping review. BMC Health Serv Res. 2024;24(1):765. doi:10.1186/s12913-024-11198-3
33. Sasie SD, Van Zuylen P, Ayano G, Aragaw FM, Spigt M. Information sharing across institutions: practices and barriers during public health emergencies in Ethiopia. Int J Med Inform. 2024;186:105439. doi:10.1016/j.ijmedinf.2024.105439
34. Cheng TW, Farber A. Surgery or endovascular therapy for chronic limb-threatening ischemia. Adv Surg. 2024;58(1):121–133. doi:10.1016/j.yasu.2024.04.008
35. Kim Y, Decarlo CS, Thangappan K, Zacharias N, Mohapatra A, Dua A. Distal bypass versus infrageniculate endovascular intervention for chronic limb-threatening ischemia. Vasc Endovascular Surg. 2022;56(5):539–544. doi:10.1177/15385744221086347
36. Shishehbor MH, Powell RJ, Montero-Baker MF, et al. transcatheter arterialization of deep veins in chronic limb-threatening ischemia. n engl j med. 2023;388(13):1171–1180. doi:10.1056/NEJMoa2212754
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025