Back to Journals » Patient Preference and Adherence » Volume 16
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Authors Siraj EA ![]() , Yayehrad AT
, Yayehrad AT ![]() , Kassaw AT
, Kassaw AT ![]() , Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Received 23 September 2022
Accepted for publication 24 November 2022
Published 5 December 2022 Volume 2022:16 Pages 3157—3172
DOI https://doi.org/10.2147/PPA.S390058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ebrahim Abdela Siraj,1 Ashagrachew Tewabe Yayehrad,1 Abebe Tarekegn Kassaw,2 Dagmawit Kassahun,3 Eyerus Solomon,3 Hadra Abdela,3 Getasew Gizachew,3 Efrem Awoke3
1Department of Pharmacy, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, North-West Ethiopia; 2Department of Pharmacy, College of Medicine and Health Sciences, Woldia University, Woldia, North-East Ethiopia; 3Department of Pharmacy, Medical School, GAMBY Medical and Business College, Bahir Dar, North-West Ethiopia
Correspondence: Ebrahim Abdela Siraj, PO Box: 79, Bahir Dar, North-West Ethiopia, Tel +251 918 02 00 93, Email [email protected]
Background: Reports indicate that health science students are among the frontline of self-medication practitioners. The main objective of this study was to evaluate the self-medication (SM) practice and associated factors with knowledge and attitude of undergraduate health science students at GAMBY Medical and Business College, Bahir Dar, Ethiopia.
Methods: An institutional-based cross-sectional quantitative study was conducted using a self-administered questionnaire from May to July, 2022. A stratified random sampling method was applied to collect the data. The collected data were checked, and exported into SPSS 26. Descriptive statistics and regression analysis were performed to determine the results and the associated factors. Variables with p < 0.05 were regarded as significant.
Results: 301 students (31 medicine, 163 pharmacy, and 107 medical laboratory students) responded (99% response rate). 68.1% of the respondents had practiced SM at least once within the last six months. 58.8% had good knowledge, while 55.5% have a positive attitude towards SM. Headache (33.7%) and cough (29.8%) were the primary disease conditions for SM. Analgesics (37.1%) and antimicrobials (29.8%) are most frequently self-consumed agents. Being a medicine student (AOR = 3.872; 95% CI: (1.263– 11.866); p = 0.018), not having health insurance (AOR = 2.431; 95% CI: (1.383– 4.274); p = 0.002), and not having a known medical illness (AOR = 2.241; 95% CI: (1.226– 4.127); p = 0.010) were independently associated with good knowledge. While, living in an urban area was significantly associated with a positive attitude (AOR = 3.593; 95% CI: (1.404– 9.197); p = 0.004).
Conclusion: The SM rate in GAMBY is significantly higher. Besides, not more than half the students had acceptable knowledge and attitude towards SM. The college and the surrounding regulatory authorities should consider ways of controlling and recapitalizing SM practices by the students.
Keywords: self-medication, health science students, knowledge, attitude, practice, Ethiopia
Introduction
Self-medication (SM) is accessing and using drug products for self-diagnosis, self-treatment, or other purposes without a legal prescription or prescriber order. It is the selection and administration of remedies to manage self-perceived disease conditions.1,2 The International Pharmaceutical Federation (FIP) also defined this similarly as the use of medicines by people without a physician order on their own ingenuity.3 It comprises obtaining drugs without physician order, accessing new drugs with previous prescriptions, using left-over drugs from previous treatments, and the sharing of medicines from others.4 Societal developments in literacy, economy, and access to technological advancements, including social media outlets, are among the promoting factors for SM globally.5 Self-consumption of medicines is an issue with serious global implications even though the WHO encourages proper SM for mild disease conditions.6 Irresponsible SM practice may bring numerous potential health related jeopardies, for instance delay in proper diagnosis and treatment; failure to identify contraindications, exposure to drug interactions, possibility of improper courses of therapy, the risk of tolerance, dependence and abuse, etc.7,8 It may also lead to paradoxical health and economic losses associated with serious consequences such as drug resistance, disease co-existence and, the worst, mortality.9–11
Literacy level, socioeconomic status, access to health information and facilities, exposure to drug promotions,awareness about disease, and health policies are some of the associating factors with SM practice.12–15 Especially for health science students, information access, medicine availability, promotions, previous experiences, self-confidence, and unused or left-over drugs at home all significantly influence the practice.16,17 Level of education, family history, societal background, legislative gaps, and availability of drugs are also reported as determinant factors.18,19 Advanced academic and professional levels have been reported as the foremost factors for SM.20 Prescribers and dispensers are the frontline to be exposed to SM due to their easy access to drugs.21,22 Since today’s health students are the future health practitioners, investigating their SM habits and taking corrective measures plays a significant role in how they will protect themselves and others from improper drug utilization.23,24 Studies showed that health students do not visit health facilities or health care providers for their health information.25 This may be due to the impact of advancements in accessing social media information26,27 which is now ultimately increasing the prevalence of SM.28 Study reports from Saudi Arabia,29 India,30 Uganda,31 Ethiopia.32,33 and Kuwait34 reveal a significant prevalence of SM by health students.
SM practice without proper knowledge on their disease condition and complete information of drugs to be used will bring serious health related consequences. The scenario may be difficult with the case of illiteracy while it may be easier to manage in the case of college and university students if appropriate effort is applied. SM practice is extensive with students and urgent remedial actions are needed.35 SM is also an important health issue for these students as this habit may result in a lack of an appropriate and timely management of their diseases by a specialized health care provider and deferral in the effectiveness of their therapeutic course.36 Therefore, the current study intended to evaluate the knowledge, attitude, practice, and associated factors on SM among the medical school students at GAMBY Medical and Business College.
Methods and Materials
Study Area, Design and Period
The study was conducted in Amhara Regional State, Bahir Dar City. The study setting was GAMBY Medical and Business College among undergraduate health science students. There were a total of 989 health science students in the college (Medicine: 110, Pharmacy: 537, and Medical Laboratory: 342 students). An institutional based cross-sectional study was conducted from May to July, 2022.
Target and Study Populations
All health science school students in GAMBY Medical and Business College were considered as source population. The study subjects were health science students in GAMBY Medical and Business College who were eligible for the study, willing to participate, and available during the study period.
Study Variables
Knowledge, attitude and practice of the students towards SM were considered as dependent variables while demographic characteristics were taken as predictor variables.
Sample Size Determination and Sampling Procedure
The SM practice for undergraduate health science students in the college was not done before. Hence “p” is taken as 50% of the total number of medical school students. The adequate sample size was then determined to be 384 using the following single population proportion formula.

where, n is the required sample size, z is the standard normal deviation at 95% confidence interval (1.96), q = 1-p, and d is the margin of error tolerated (5%).
Since the total number of students in the school is less than 10,000, a population correction formula was used to determine the sample size and the calculated final sample size became 276.65. Then, considering a 10% non-response rate, the corrected total sample size became 304. Hence, 304 health science students were included in this study. Two step stratified random sampling was used to collect the data, ie, sampling from each department, and then sampling from each study year based on the appropriate proportion of the respective field of study.
Data Collection Procedures
A pre-tested questionnaire, adapted from various previous studies, was prepared in English and distributed to collect the relevant data. The questionnaire comprised of 4 main parts; demographic information, knowledge related questions (seven question with yes/no labeling), attitude related questions (seven questions with five levels of agree/disagree), and diverse questions of SM practice. For the SM practice evaluating questions, respondents were asked to answer one most common (prioritized) answer from the given alternatives. The questionnaire was modeled from those used in previous studies37–39 and it was tested on a population of thirty students, and all ambivalent and unclear questions were rephrased or removed. The relevant data were collected by group members of the study after taking the consent from the participants using a printed paper-based questionnaire.
Data Processing and Analysis
Daily follow-ups and appraisals were done during the data collection for data completeness and consistency. SPSS 26 was used to analyze the descriptive statistics. Bivariate and multivariable logistic regression analysis was used in order to identify truly associated factors and control confounding effects. Independent variables with a p-value of <0.25 were selected for multi-variable logistic regression analysis. Odds ratio (OR) with 95% CI was then computed for each variable for the corresponding P-value. The value of P < 0.05 was considered statistically significant.
Data Quality Control
The data collection tool was properly designed and developed. Pre-test was done out of the study area. The data collector group was sufficiently trained by the first author. All the data collection process and the collected data was reviewed and checked by the principal investigator.
Ethical Considerations
Ethical approval was obtained from the Ethical Review Committee of GAMBY Medical and Business College. We got a permission letter from the college administration after the Department of Pharmacy, Medical School, GAMBY Medical and Business College wrote a support letter to the committee. All necessary briefings were done about the study and the participants who were willing to participate and gave consent were included. In accordance with the Declaration of Helsinki, confidentiality was maintained and no personal identifier of the respondents was used during the study.
Operational Definitions
Self-medication practice: use of a drug substance to self-administer for the treatment of physical or psychological ailment perceptions without prescriber consultation.
Good knowledge: knowledge score above the median score (4.0).37
Bad knowledge: knowledge score below the median value.37
Positive attitude: attitude score above 20.37
Negative attitude: attitude score below 20.37
Results
Socio-Demographic Characteristics of the Respondents
301 (31 medicine, 163 pharmacy, and 107 laboratory) of the 304 sample size responded to the study (99% response rate). As shown in Table 1, among the respondents, 50.8% were female, 62.4% were in the age group of 21–23 years, and 90.1% lived in urban areas. Regarding their education, 53.8% were from the pharmacy department and more than s quarter (26.4%) were first year students. 67.7% of the respondents did not have health insurance and 74.9% reported that they do not have a known medical illness.
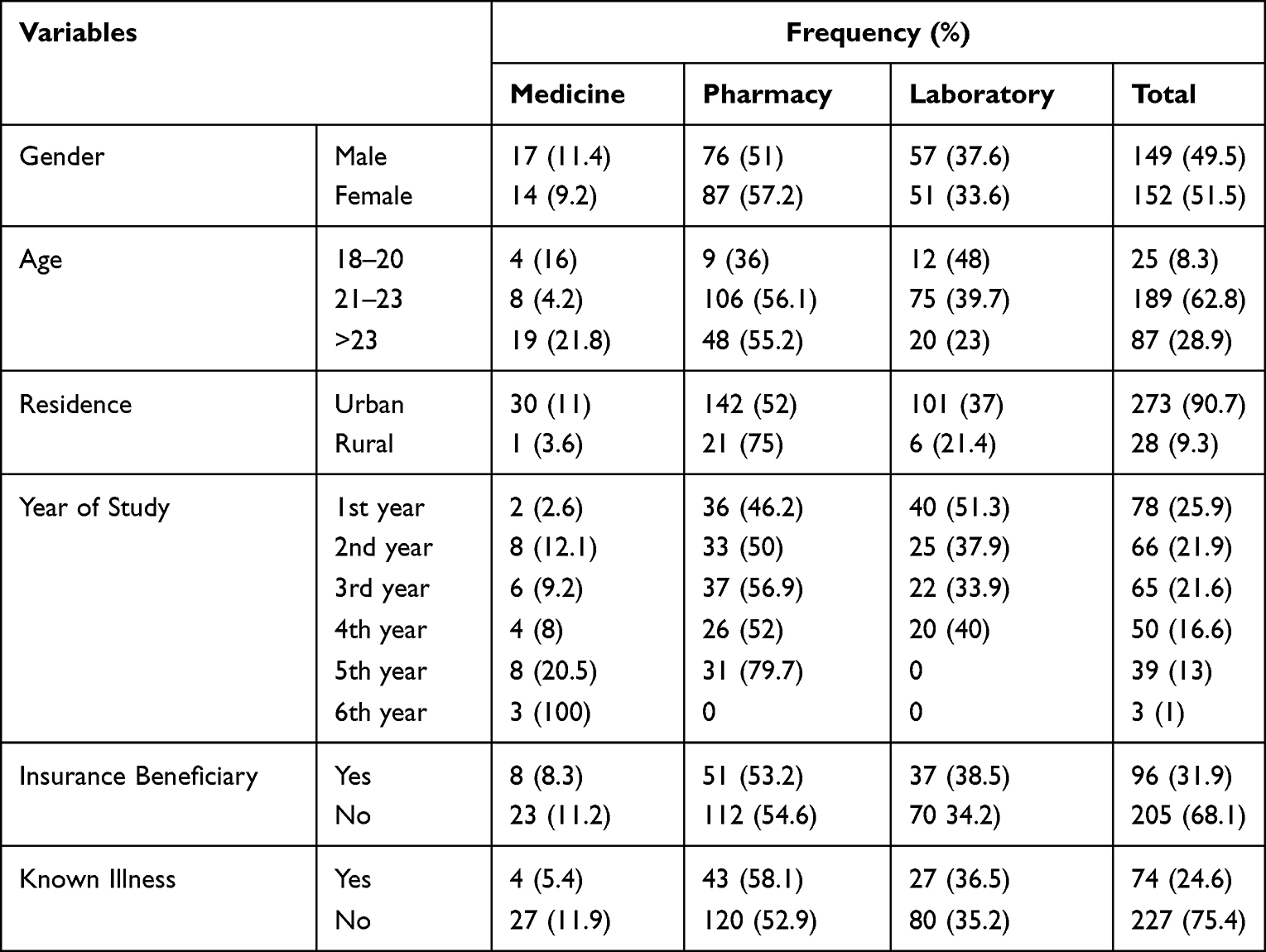 |
Table 1 Socio-Demographic Features of the Respondents (n = 301) |
Students’ Knowledge About Self-Medication
The mean knowledge score in this study was determined to be 4.57 with a standard deviation of 3.27. As summarized in Figure 1, 177 (58.8%) of the students (83.9% of medicine, 61.3% of pharmacy, and 47.7% of laboratory) had good knowledge. About 187 (62.1%) students accepted that SM is self-consuming of drugs without a prescriber order. Only 108 (35.9%) agreed that SM may not always be safe and effective. Nearly half of the students (46.5%) recognized that all drugs can have adverse effects. As shown in Table 2, 198 (65.8%) of the respondents agreed that increasing or decreasing doses by self could be risky and also a similar proportion of the respondents (66.8%) believed that physician help must be sought for adverse events during SM. As can be seen from the chi-square p-values, there are significant associations between knowledge and department of respondents on the definition of SM (p = 0.001), on safety and efficacy of SM (p = 0.007), on the risk of increasing or decreasing by self (p = 0.009), and on the threat of using drugs with unknown ingredients in patients with known medical conditions (p = 0.022).
 |
Table 2 Participant Students’ Knowledge Towards Self-Medication (n = 301) |
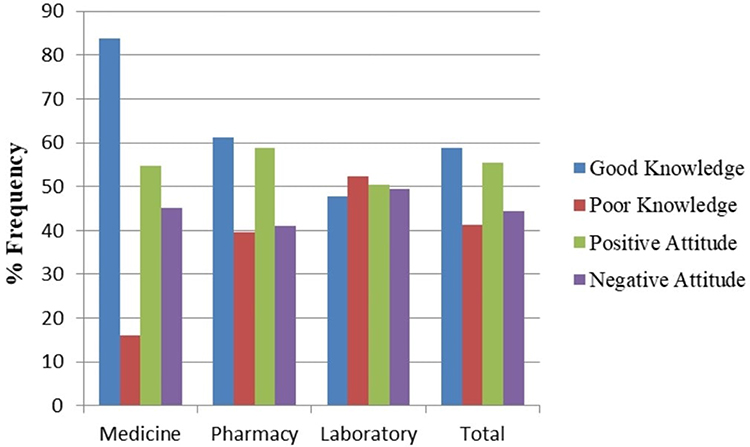 |
Figure 1 Knowledge and Attitude of Students towards Self-Medication (% Frequency). |
Student’s Attitude Towards Self-Medication
The mean attitude score of the respondents was 20.86 with s standard deviation of 5.16. As presented in Figure 1, 167 (55.5%) of the students have positive attitudes. The attitude level between the respondents of the three departments is similar; 54.8%, 58.9%, and 50.5% for medicine, pharmacy, and laboratory students, respectively, for a positive attitude. There was also the absence of a statistically significant association from the chi-square analysis on their attitude (agreement or disagreement) towards all the presented attitude-related questions (p > 0.05). As shown in the results (Table 3), 73 (24.3%) strongly agreed and 33 (11.0%) agreed that SM is part of self-care. 157 (52.2%) of the students responded positively to the need for training on the use of SM. 91 (30.2%) strongly agreed and 33 (11.0%) agreed on the ability of health science students to self-diagnose medical conditions, while only half (50.1%) of the respondents disagreed on the ability of health science students to self-treat different diseases. 139 (46.2%) agreed on recommending SM for others.
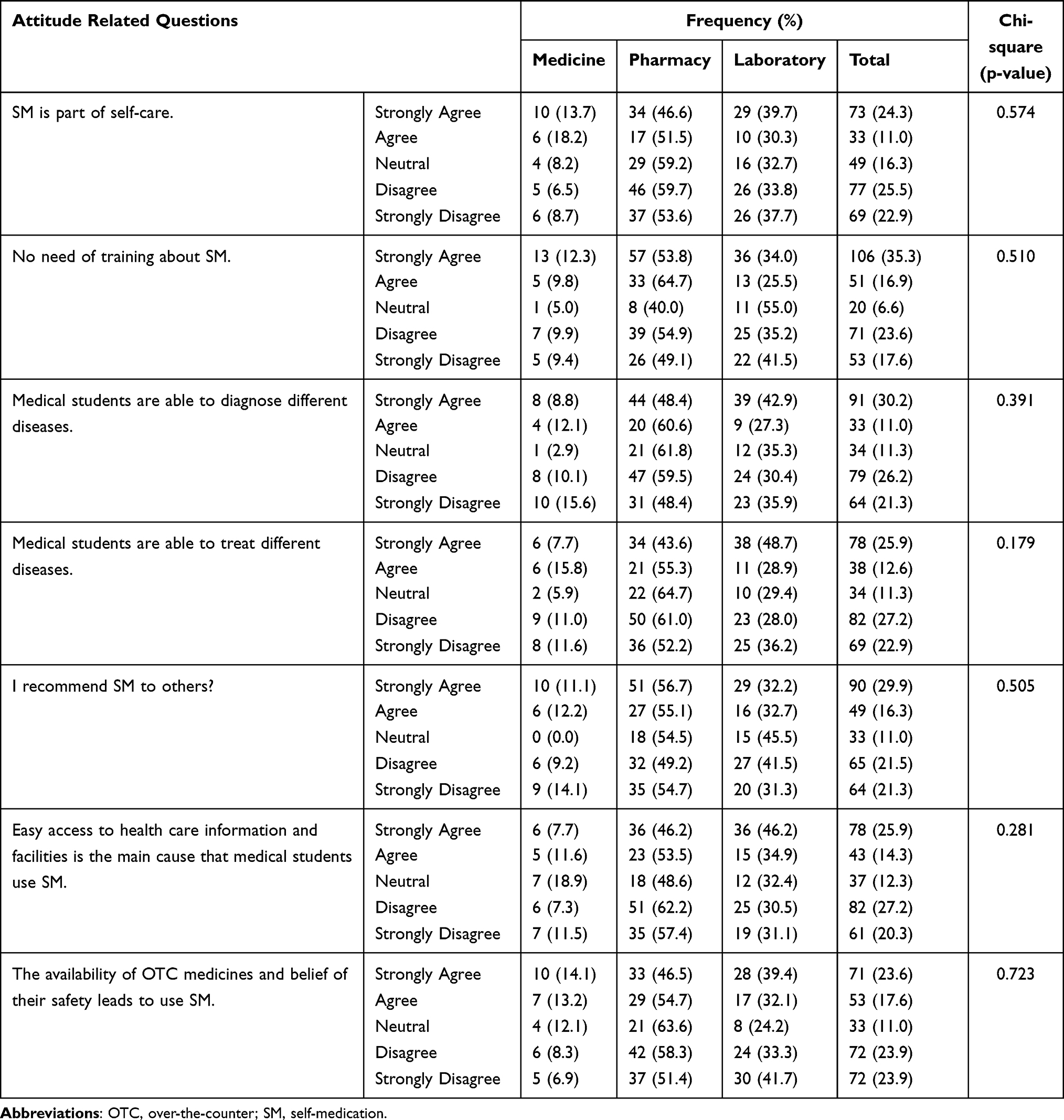 |
Table 3 Attitude of Students to Self-Medication (n = 301) |
Student’s Practice of Self-Medication
The SM pattern of the students is presented in Table 4. 205 (68.1%) of the study participants practiced SM at least once within the last six months. About 84 (41.0%) of them did not know whether their medications need prescription or not. Here, a significant association was observed between department and SM practice (p = 0.004). Anti-pain (37.1%) and antimicrobial (29.8%) drugs were the most commonly self-consumed groups of medications (Figure 2). Whereas, disease perceptions with headache (33.7%) and cough and common cold (29.8%) were the commonly self-treated medical conditions (Figure 3). 83 (40.5%) of them used self-information for their SM practice. A significant association was also observed on their sources of medications (p = 0.008) where 163 (79.5%) of them accessed it in pharmacies while 13 (6.4%) got it from herbalists. The reason for most of the respondents (58.0%) for using SM is need of quick relief. About two-thirds (67.8%) of the respondents with a history of SM did not experience any adverse effect related to their medications. This also resulted in a significant association in SM practices with medicine, pharmacy, and laboratory students (p=0.015). Most of the students (64.4%) felt confident while using SM as part of their health care.
 |
Table 4 Self-Medication Practice of Students (n = 205) |
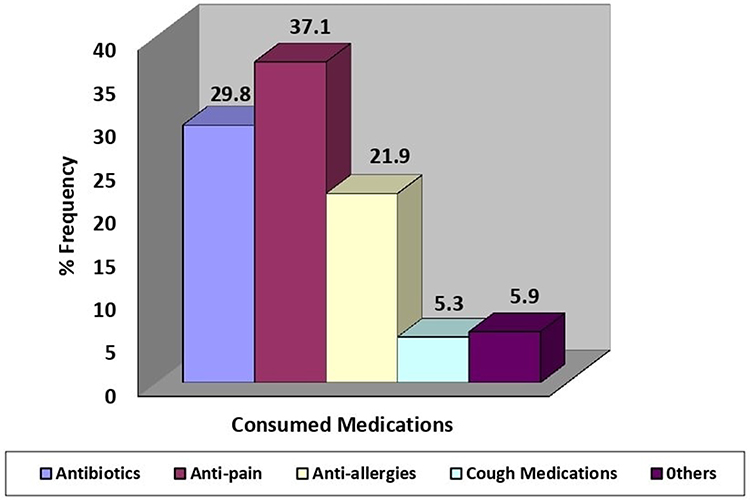 |
Figure 2 Percentage of medications self-consumed by students. |
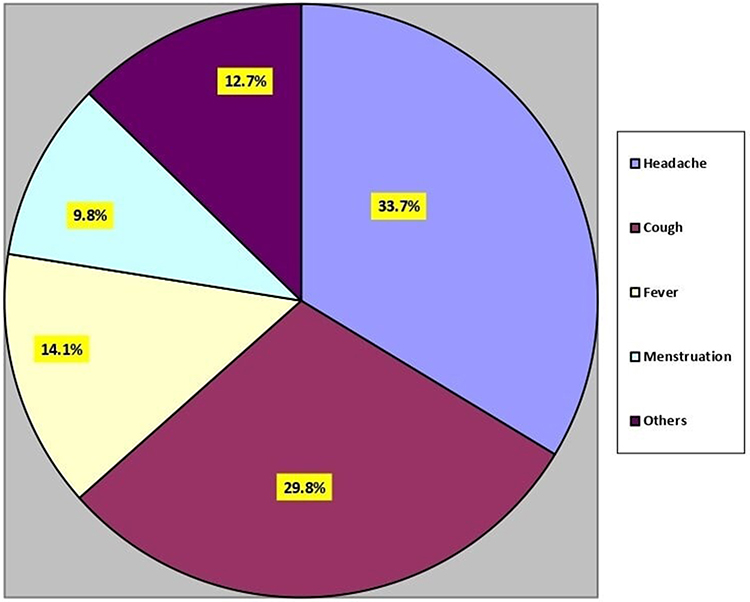 |
Figure 3 Percentage of medical conditions for self-medication. |
Factors Associated with Student’s Knowledge of Self-Medication
Department of the responding students, being an insurance beneficiary, and having a known illness are statistically associated independent variables with s student’s level of knowledge about SM (Table 5). From the regression analysis results it is observed that being a medicine student had a 3.872 times more positive effect on knowledge than being a medical laboratory student (AOR = 3.872, 95% CI: (1.263–11.866); P = 0.018). Pharmacy students also had s 2.491 times better knowledge than laboratory students (AOR = 2.491; 95% CI: (0.853–7.279)), even though the association was not statistically significant (p = 0.095). Students that have health insurance demonstrated 2.431 times worse knowledge that lead them to practice SM than students that do not have health insurance (AOR = 2.431; 95% CI: (1.383–4.274): P = 0.002). Students that have a medical illness had 2.241 times poorer knowledge about SM practice than students that do not have a medical illness (AOR = 2.241; 95% CI: (1.226–4.127); P = 0.010).
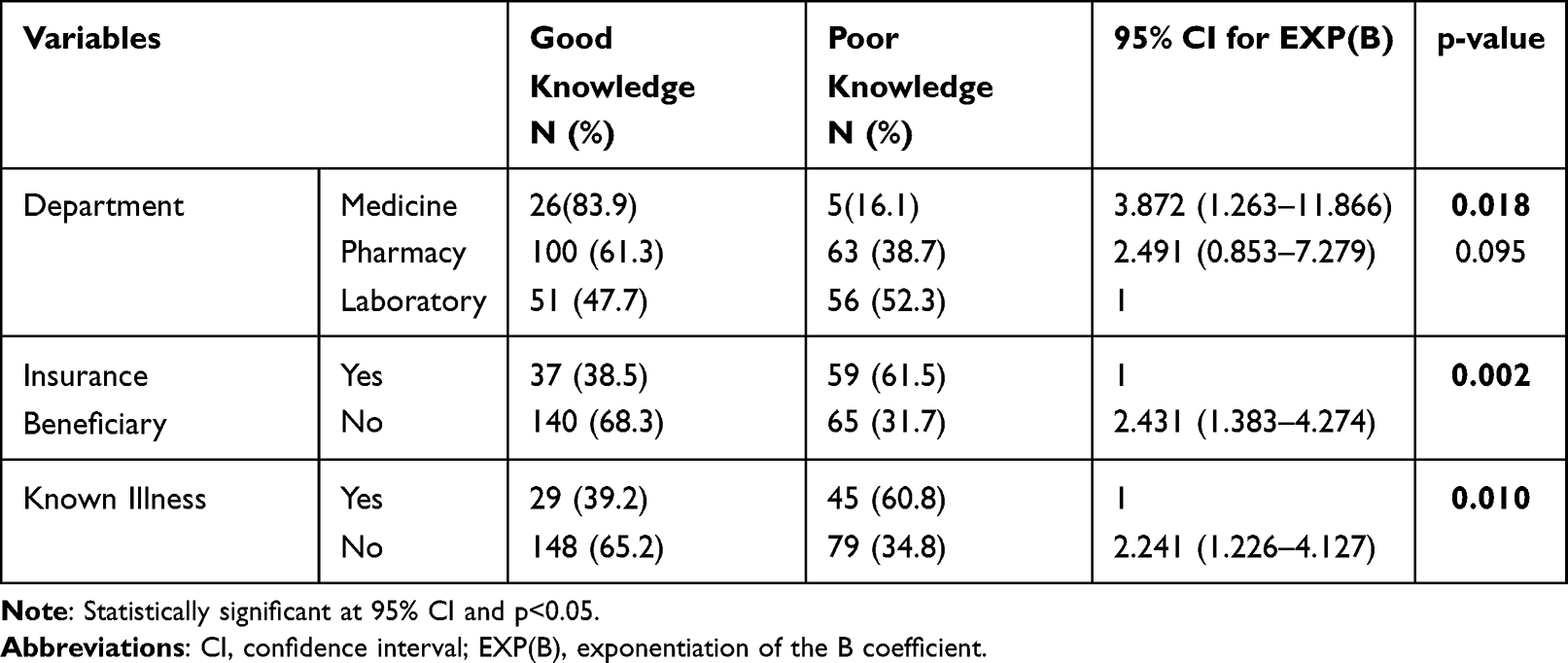 |
Table 5 Associated Independent Variables with Knowledge About Self-Medication |
Factors Associated with Student's Attitude Towards Self-Medication
The only observed significantly associated independent variable with the student's attitude in this study was area of residence of the students (Table 6). Students from urban areas have a 3.593 times better attitude towards SM than students living in rural areas (AOR = 3.593; 95% CI: (1.404–9.197); P = 0.004).
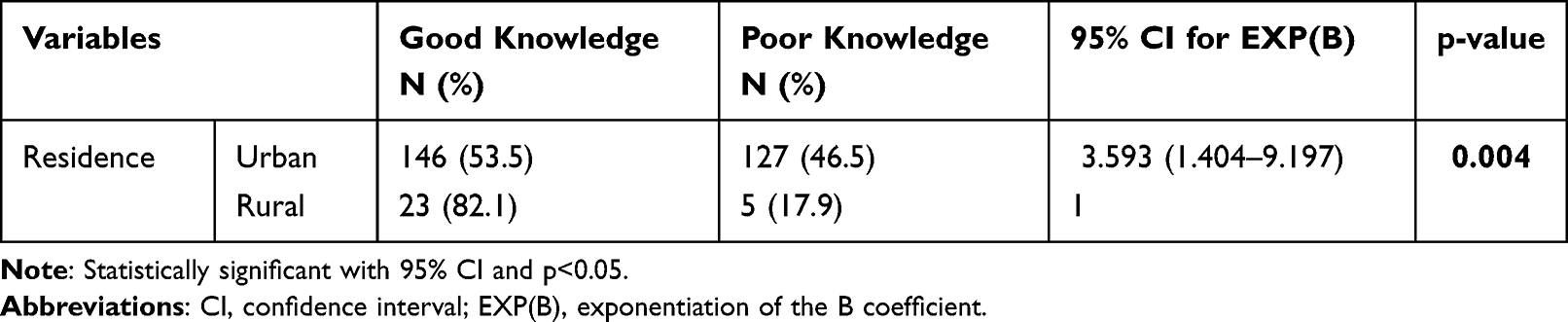 |
Table 6 Associated Independent Variables with Attitude Towards Self-Medication |
Discussion
Self-Medication Prevalence
The present study revealed that the prevalence of SM at GAMBY Medical School students was 68.1%. This is a very significant number which is almost consistent with similar study reports from Rift Valley University (72.7%),7 Qassim University (63.9%),29 Wollo University, Ethiopia (64.98%),32 and Indian Colleges (57.1–92.0%).40 But, the prevalence is considerably higher than similar study reports of the Arabian Gulf University, Bahrain (44.8),22 universities in Kuwait (35.9%),34 Zabol University, Iran (57.1%),41 and among students and other population groups in the developed western regions such as German (8%),42 France (17%),43 USA (22%),44 United Kingdom (39.2%),45 Spain (45%),46 Italy (53.4%),47 and Norway (54%).48 Still, there are some studies indicating a higher prevalence of SM among health science students in those European and other developed countries such as Serbia (79.9% and 81.3%),3,49 Slovenia (92.3%),50 and Australia (91.7%).51 From these reports, it can be posed that SM is a commonly practiced part of health care all over the world, in varying degrees. Generally, SM prevalence is reported to be higher in developing than developed countries. The welfare status, income per capita, better quality health care, and more efficient drug supply management system can be listed as the main factors. In addition, educational level and specialty, socio-economical differences, acquired knowledge about specific disease perceptions, and other related sociodemographic variations could be reasons for the similarity and differences among those reports.41 By any means, the results of this study generally show an urgency of vigilant monitoring and regulation of the drug use pattern, drug delivery systems, distribution and dispensing practices, especially in developing countries like Ethiopia, to avert SM and related adverse events in a timely manner.
Knowledge About Self-Medication and Associated Factors
SM has nowadays turned out to be a global habit, where individuals are apt to bargain for over-the-counter (OTC) drugs just based on symptom perceptions. The fortune and infortunate effects consequently after SM have shown SM is a global public health concern.52 Health science students, especially those in medicine and pharmacy professions are expected to have well equipped knowledge regarding appropriate drug use. They are expected to be medication experts as they take numerous drug-related courses that may well upsurge students’ knowledge and understanding about drug utilization principles.33 Unfortunately, not more than 58.8% of the respondents in this survey had good levels of knowledge regarding SM. The overall knowledge score result is consistently lower like those investigations in India,53 Riyadh54 and Taiwan.55 This is even less than similar studies in other academic institutions of Ethiopia such as Debre Markos University (64.6%)56 and University of Gondar (67.6%).33 Similarly, it is significantly at a lower level compared with other global reports like Oman (75%)57 and Osun State (91%).58 However, it is better than a study report from public and private universities in Kuwait where 53.5% of the students in the study failed to score the median value34 and the case of Iran where only 16% and 35% of medicine and pharmacy students achieved good scores regarding drug information.41 These differences may be due to the level of education and field of study of respondents, the level and experience of the academic institutions, or other socio-demographic variables of the respondents. Unsatisfactory knowledge level of health science students results in unsuitable medication consumption. Accordingly, promoting knowledge of students and the general public regarding medication use can aid the aptitude of using medication cautiously. Hence, knowledge enrichment mediations using campus-based seminars, evidence-based brochures, and self-instructional modules can be applied.53
SM has not only pros, but also cons. Should it have been practiced with great responsibility, it can be a suitable substitute to manage minor illnesses as part of self-care. However, its unfortunate application can lead to unexpected destructive outcomes. Its use inappropriately due to insufficient knowledge about drug side-effects may be one major reason for such misadventures.59 Based on the results of this study, only 35.9% agreed that SM may not always be safe and effective. Additionally, less than half of the students (46.5%) knew that all medications, whether prescription, OTC, or herbal drugs can have adverse effects. The proportion of respondents who knew the danger of increasing or decreasing medication dose without a prescriber consultation, the need of physician help in case of adverse events, and the dangerousness of using medications with unknown substances were also not adequate. This finding was similar with research done in Sudan where 54.7% of the participants have no information about the effects of medicines they used.60 In another similar study, only 14.43% of students knew the side-effects of drugs they had taken as SM.59 Such results are indicative of animated shortcomings in the knowledge of health science students about drugs which are commonly being self-medicated. Thus, hard work is needed to maximize students’ awareness on the side-effects, precautions, and necessary measurements of scenarios for reducing incidences, early detection, and treatment of side effects as they occur. Creating sufficient awareness about the different adverse effects, risk of drug interactions, and antibiotic resistance among health science students will not only ensure nonviolent SM practices but also will benefit the society.30
Various associated factors may affect the knowledge level of students about SM. In one study, there was a significant association between knowledge and the age of the participants.53 On another similar investigation, it was significantly associated with the field of study (department), year of entrance (level of education or class year), and the history of SM or previous ailments.41 Gender is also reported as a possible associating factor.34,50 Similarly, in this study, being a medicine student, not being an insurance beneficiary, and not having a known illness are positively associated with a good level of knowledge about SM.
Attitude Towards Self-Medication and Associated Factors
In this study, only 55.5% of the students have positive attitudes. This is in-line with survey reports in Gondar21 and Eritrea.39 However, it is considerably lower than study reports of similar surveys in Asella of Ethiopia,33 South Tamilnadu,30 Riyadh54 and Bahrain22,61 as most of the respondents in these studies demonstrated a positive attitude towards practicing SM. According to the result of this research, more than one-third of the respondents agreed that SM is part of self-care while almost half of them responded positively for the need of training about SM. Consistently, 40% of respondents from a study in India agreed with this statement.59 A similar study in Iran also reported that 41.2% of health science students believed that SM is part of self-care and 67.7% students agreed with the need of training about SM.41
91 (30.2%) respondents strongly agreed and 33 (11.0%) agreed on the ability of health science students to self-diagnose medical conditions, while only half (50.1%) of the respondents disagreed on the ability of health science students to self-treat different diseases. This is nearly similar with the investigation in India, where 52.9% of undergraduate health science students in a tertiary care hospital confidently prescribed medicines on their own to themselves, their friends, and family members.62 The belief of self-diagnosis and self-treatment is not limited only to the developing countries, but it is also prevalent in developed western regions with various degrees of prevalence. Earlier study reports revealed that 39.2% of the health science students in the United Kingdom45 and about 22% of health students in the USA44 agreed on the appropriateness of self-prescribing. 46.2% of the respondents under this study recommend SM for others. This is higher than the case in Eritrea (35.9%)39 but importantly lower than the reports in southern India (64%)63 and northern Uganda (68.2%).64
The only observed significantly associated independent variable with the attitude of students towards SM in this study was the area of residence of the students. Students are similar in their attitude towards SM in all other parameters except being significantly higher for students from urban residency. Similar studies in Eritrea39 and Egypt65 also revealed that being from urban areas was an independent predictor for SM. The fact that residence may be associated with SM remains in that lots of the rural communities have little or no access to modern healthcare due to the irregular or insufficient facility distributions. Numerous reasons related with the social, economic, and cultural perception towards diseases and their perceived responses to indigenous medications around where they live can also affect SM patterns of the rural society.65–67 Another similar study in Bangladesh also revealed the impact of the cultural, socio-economical, geographical, and traditional distinction over the plain land population towards their SM practices. This study also suggested that such associations bring important policy implications. Hence, the government bodies, notably the Ministry of Health, should implement awareness raising initiatives among the rural people about the dangers of SM.38
The Pattern of Self-Medication Practice
Common Illness and Medications for Self-Medication
Medications for pain management were the most frequently used among others followed by antimicrobial drugs. Whereas, disease perceptions related with headache and coughing were the commonly self-treated medical conditions. This result is consistent with other similar studies of health science students in Ethiopian higher educational institutions such as Arsi University,33 University of Gondar,37,68 Private Health Science Colleges in Gondar,69 and Mekelle University.70 There are also confirming reports from Bahrain,22 Eritrea,39 Saudi Arabia,71 and India30,53,62 on the frequently used SM groups and perceived disease conditions. Similarly, analgesics and antibiotics were the two foremost self-medicated drugs in Nigerian students,72 whereas non-steroidal analgesic, anti-inflammatory, and antipyretic drugs were the most frequently used OTC drugs for self-treating fever and headaches in Nepal.73 In a study among students in Kuwait, similar findings were found on the causative medical conditions for SM and higher rates of consumption of pain killer medicines but antibiotics were self-consumed by only 2.9% of the students.34 Conversely, SM using oral antibacterial agents outweighs those with oral anti-inflammatory agents and antipyretics among medical and paramedical students in India40,59 and Iran.41
The most common medical conditions perceived as initiatives for SM in this study were typically self-limiting “minor illnesses” which are listed primarily in most study reports as the most frequent indications for self-treatment.22 Moreover, stress-induced headache and other associated health perceptions are common among college students due to educational loads, especially in medicine and health science students. They may also be victims of the common cold and other cough inducing illnesses due to their living environmental conditions, especially in institutions of less-developed countries where facilities are not well-furnished. The antimicrobial SM report for this study is not a negligible figure. The unlimited and excessive antimicrobial self-consumption in this study and other similar reports may be due to the inadequate regulation of the dispensing practice.
Source of Information and Medication Access
40.5% of the respondents in this study relied on self-information for their SM practice. Other studies also comply with this result.39,70 This is obvious since they are health science students and the familiarity with diseases and therapeutics persuades them to attain self-confidence to treat themselves without consulting prescriber professionals. Family or friends with a health professional background can also impact students’ SM practice as they could advise purchasing medications related to their symptoms without being diagnosed. A study on SM practice of adults in Wolaita Soddo town, southern Ethiopia confirmed this assertion as more than 75% of the respondents were advised by pharmacists and other health professionals for SM.74
In the current study, 79.5% of the students collected their medications from pharmacies. This is common that most self-medicated drugs are purchased from drug retail outlets. Survey reports from other study areas in Ethiopia,33,68–70 Australia,51 Eritrea,39 and Bangladesh38 also indicated that drug retailers are the primary sources of SM access. This is also an indication of the gaps in regulatory performances in those study areas. Unless revitalized in a timely manner, such dispensing malpractices by drug retailers could be among the leading predictors to irrational drug use, drug resistance, and consequent health hazards in general. 6.4% of the respondents got their drugs from traditional herbal producers. Almost s similar proportion of respondents also accessed medications from herbalists in one other study in Ethiopia.70 This should also not be undermined as unknown drug content, unevaluated concentrationd, and unjustified dosage may lead to serious adverse effects. Concomitant use of the traditional and the conventional medicines during SM may also bring in unexpected adverse events.
Reasons for Self-Medications and Experience of Adverse Effect
The need for quick relief and saving time were the most frequently mentioned reasons for SM by the students. Health science students in Bahrain also reported the need for time saving as a primary reason for SM.22 Perception in the mildness of the illness, similarity of disease conditions with previous symptoms and incapability to afford health care costs were also reported as the major reasons for SM practice in other similar studies.75,76 Conversely, saving time and money are the least common reasons for health science students in Eritrea where previous experience and perceived sufficient knowledge towards SM were the prior reasons.39 However, self-treating perceived illnesses based on past experiences or with perceived knowledge without accurate diagnosis could lead to misdiagnosis, missed therapeutics, and subsequent unwanted health problems. Practicing SM to save time and money may also result in costing the irreplaceable health and life. One-third of the respondents with a history of SM experienced some adverse effect related to their medications. This is a significant number as at least a few and less-serious cases could happen with higher prevalence of SM practice. The report in the current study is significantly higher than that of Eritrea39 and south India.63 This difference may be from misinterpretation of symptoms and side effects as an adverse effect. Whatever the case, the report should not be neglected and appropriate measures should be outlined to prevent further losses.
Relaxed availability and accessibility of medications, including those prescription-only drugs from drug retail outlets, might be allied to the lack of strict legislation concerning medicine utilization in developing countries. This regulation gap could subsidize to an increased prevalence of SM practice, thus resulting in irrational drug use, possibility of resistance development, and harmful life conspiracy at large.39 Students in the health departments are the future health practitioners, health leaders, health policymakers, and decision makers. Hence, investing in them about appropriate use of medicines and OTCs is reimbursing in the generation for a better health management system that will come tomorrow. Studies should be promoted to attract government attention in order to diminish the factors promoting SM in low income and developing countries.
Conclusion
From this study a significantly higher prevalence of SM practice was seen among health science students in GAMBY. The proportion of students with good knowledge and a positive attitude level is low. This result implies that students need more awareness regarding SM. Giving induction training about the consequences of SM to decrease the practice, to improve students’ knowledge, and to upgrade their attitude level should be one target of intervention in higher educational institutions. Appropriately regulated dispensing practice of medications with adequate counseling and with prescriptions only when needed should be applied. Suitable supportive supervision and gap filling from responsible bodies related to SM are recommended to overcome SM associated problems. Further investigations are needed on the prevalence, impact, risks, and associated factors regarding the practice of SM and consumption pattern of OTC medications.
Abbreviations
FIP, International Pharmaceutical Federation; KAP, Knowledge, Attitude and Practice; OTC, over-the-counter.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Montast NC, Bagher H, Geraud T, Lapeyre-Mestre M. Pharmacovigilance of self-medication. Therapie. 1997;52(2):105–110.
2. Sharif SOL, Bugaighism MSR, Sharif RS. Self-medication practices among pharmacist sin UAE. Pharmacol Pharm. 2015;6(09):4a. doi:10.4236/pp.2015.69044
3. Lukovic JA, Miletic V, Pekmedzovic T, Trajakovic C, Ratkovic N, Aleksic DGA. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One. 2014;9:1–14. doi:10.1371/journal.pone.0114644
4. Zafar SN, Syed R, Waqars ZAJ, et al. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58(4):214.
5. Gyawali S, Shankar PR, Poudel P. Knowledge, attitude and practice of self-medication among basic science undergraduate medical students in a medical school in western Nepal. J Clin Diagnost Res. 2015;9(12):Fc117.
6. Ocan M, Obuku EA, Bwanra F, Akana D, Ricnard SO. Household antimicrobial self-medication: a systematic review and meta-analysis of the burden, risk factors & outcomes in developing countries. BMC Public Health. 2015;15(1):11. doi:10.1186/s12889-014-1340-7
7. Beyene A, Getachew E, Dobecni A, Poulos E, Abdurahman KAM. Knowledge attitude and practice of self-medication among pharmacy students of rift wallet university, Abichw campus, Addis Ababa, Ethiopia. J Heal Medinformat. 2017;2(269):2.
8. Alsows M, Elayeh E, Jalil MA. Evaluations of self-medication practice among pharmacy students in Jordan. Jordan J Pharm Sci. 2018;11(1):1–10.
9. Hughes CM, Elnay MC, Fleming GF. Benefits and risks of self medication. Drug Saf. 2001;24(14):1027–1037. doi:10.2165/00002018-200124140-00002
10. Chalker J. Improving antibiotic prescribing in HaiPhong province Viet Nam: the “antibiotic dose” indicator. Bull World Health Organ. 2001;79:313–320.
11. Sharif SI, Ibrahim OH, Mouslli LWR. Evaluation of self-medication among pharmacy students. Am J PharmacolToxicol. 2012;7(4):135–140.
12. Ramadan M, Eltaweel A, El Nakhal T, Hemead H, Maraqa A, Abish DE. Self-medication among undergraduate medical students of Alexandria faculty of medicine: were do we stand. Int J Med Students. 2018;6(2):52–55. doi:10.5195/ijms.2018.41
13. Sandhu S, Suryani Y, Dwiprahasto IA. A survey of antibiotic self-medication and over the counter drug use among undergraduate medical students in Yogyakarta, Indonesia, South-East. Asian J Trop Med Public Heal. 2017;48(6):1290–1298.
14. Zhu X, Pan H, Yang Z, Cui B, Zhang D, Ba-Thein W. Self-medication practices with antibiotics among Chinese university students’. Public Health. 2016;1(130):78–83. doi:10.1016/j.puhe.2015.04.005
15. Gelayee DA. Self-medication pattern among social science university students in Northwest Ethiopia. J Pharm. 2017;2017:8680714.
16. Hussian S, Malik F, Hamed A, Ahmads RH. Exploring health seeking behaviour, medicine use and self-medication in urban and rural Pakistan southern. Med Rev. 2010;3(2):32–35.
17. Klemanc-ketis z Kersnik J, Kersnik J. Sources and predictors of home kept prescription drugs. Int J Clin Pharmacol Ther. 2010;48(11):705–707. doi:10.5414/CPP48705
18. Habeeb GE. Common Patient symptoms: patterns of self-treatment and prevention. J Missippi State Med Assoc. 1993;34(5):179–181.
19. Seam M, Reza O, Bhatta R, et al. Assessing the perceptions and practice of self-medication among Bangladesh; undergraduate pharmacy students. Pharmacol. 2018;6(1):6.
20. Martins AP, da Costa Miranda A, Mendes Z, Soares MA, Ferreira PNA. A self-medication in a Portuguese urban Population: a Prevalence study. Pharm Epidemiol Drug Safty. 2002;11(5):409–414. doi:10.1002/pds.711
21. Abay SM, Amelo W. Assessment of self-medication practices among medical, pharmacy, health science students in Gondar University, Ethiopia. J Young Pharm. 2010;293:306–310. doi:10.4103/0975-1483.66798
22. James H, Handu SS, Al KKA, Ottom S, Sequeira RP. Evaluations of the knowledge, attitude and practice of self-medication among first year medical students. Med Princ Pract. 2006;15(4):270–275. doi:10.1159/000092989
23. Awad AZ, Eltayeb IB, Capps PA. Self-medication practices in Khartoum state, Sudan. Eur J Clin Pharmacol. 2006;62940:317–324. doi:10.1007/s00228-006-0107-1
24. Michelle P. An examination of awareness of over the counter no steroidal anti-inflammatory drugs and adverse events. UMI. 2011;9:121–125.
25. Brener ND, Gowda VR. Us college students reports of receiving health information on college campuses. J Am Coll Health. 2001;49(5):223–228. doi:10.1080/07448480109596307
26. Hanauer D, Dibbl E, Fortin JCN, Col NF. Internet user among community college students: implication is designing health care interventions. J Am Coll Heal. 2004;52(5):197–202. doi:10.3200/JACH.52.5.197-202
27. Escoffery C, Miner KR, Adame DD, Butler S, Cormick MC, Mendell E. Internet use for health information among college students. J Am Collage Health. 2005;53(4):183–188. doi:10.3200/JACH.53.4.183-188
28. Ryan AWS, Wilson S. Internet health care: do self-diagnosis sites do more harm than good? Expert Opin Drug Safety. 2008;7(3):227–229. doi:10.1517/14740338.7.3.227
29. Alduraibi R, Altowayan WM. A cross sectional survey: knowledge, attitudes, and practices. BMC Health Serv Res. 2022;22(1):1–10. doi:10.1186/s12913-022-07704-0
30. Sundararajan A, Thangappan AK. Knowledge, attitude and practice of self medication among undergraduate medical students in a teaching institution. Int J Basic Clin Pharmacol. 2018;7(12):2414–2419. doi:10.18203/2319-2003.ijbcp20184857
31. Niwandinda F, Lukyamuzi EJ, Ainebyona C, Ssebunya VN, Murungi GAE. Patterns and practices of self-medication among students enrolled at Mbarara University of Science and Technology in Uganda. Integr Pharm Res Pract. 2020;9:41.
32. Zewdie S, Andargie AKH, Kassahun H. Self-medication practices among undergraduate University Students in Northeast Ethiopia. Risk Manag Healthc Policy. 2020;13:1375. doi:10.2147/RMHP.S266329
33. Bekele SA, Argaw MD, Yalew AW. Magnitude and factors associated with self-medication practices among university students: the case of Arsi University, College of Health Science, Asella, Ethiopia: cross-sectional survey based study. Open Access Libr J. 2016;3(6):1–5.
34. Mitra AK, Imtiaz A, Al-ibrahim YA, Bulbanat MB, Mutairi MFA, Musaileem SFA. Factors influencing knowledge and practice of self-medication among college students of health and non-health professions. IMC J Med Sci. 2018;12(2):57–68. doi:10.3329/imcjms.v12i2.39662
35. Khandelwal S, Deb DGJ. Practice of self-medication among medical students in Manipal. Int Res J Pharm Appl Sci. 2013;3(5):175–179.
36. Kalyan VS, Sudhakar K, Srinivas P, Sudhakar GV, Pretab KV. Evaluation of self-medication practices among undergraduate dental students of tertiary care teaching dental hospital in south India. J Educ Ethics Dent. 2018;12(2):57–68.
37. Bekele KM, Abay AM, Mengistu KA, et al. Knowledge, attitude, and practice on over-the-counter drugs among pharmacy and medical students: a facility-based cross-sectional study. Integr Pharm Res Pract. 2020;9:135–146. doi:10.2147/IPRP.S266786
38. Saha A, Marma SKK, Rashid A, et al. Risk factors associated with self-medication among the indigenous communities of Chittagong Hill Tracts, Bangladesh. PLoS One. 2022;17:1–16.
39. Araia ZZ, Gebregziabher NK, Mesfun AB. Self medication practice and associated factors among students of Asmara College of Health Sciences, Eritrea: a cross sectional study. J Pharm Policy Pract. 2019;2:1–9.
40. Kumar R, Goyal A, Padhy BM, Gupta Y. Self-medication practice and factors influencing it among medical and paramedical students in India: a two-period comparative cross-sectional study. J Nat Sc Biol Med. 2016;7:143–148. doi:10.4103/0976-9668.184700
41. Hashemzaei M, Afshari M, Koohkan Z, Bazi A, Rezaee R, Tabrizian K. Knowledge, attitude, and practice of pharmacy and medical students regarding self-medication, a study in Zabol University of Medical Sciences; Sistan and Baluchestan province in south-east of Iran. BMC Med Educ. 2021;21:1–10.
42. Du Y, Knopf H. Self-medication among children and adolescents in Germany: results of the National Health Survey for Children and Adolescents (KiGGS). Br J Clin Pharmacol. 2009;68(4):599–608. doi:10.1111/j.1365-2125.2009.03477.x
43. Bretagne J, Richard-Molard B, Honnorat C, Caekaert ABP, Barthélemy P. Gastroesophageal reflux in the French general population: national survey of 8000 adults. Press Med. 2006;35:23–31. doi:10.1016/S0755-4982(06)74515-8
44. Roberts LW, Hardee JT, Franchini G, Stidley CASM, Siegler M. Medical students as patients: a pilot study of their health care needs, practices, and concerns. Acad Med. 1996;71:1225–1231. doi:10.1097/00001888-199611000-00019
45. Hooper C, Meakin RJM, Jones M. Where students go when they are ill: how medical students access health care. Med Educ. 2005;39(6):588–593. doi:10.1111/j.1365-2929.2005.02175.x
46. Carrasco-garrido P, De AAL, Barrera VH, et al. Predictive factors of self-medicated analgesic use in Spanish adults: a cross-sectional national study. BMC Pharmacol Toxicol. 2014;15:1–9.
47. Garofalo L, Di GG, Angelillo IF. Self-medication practices among parents in Italy. BioMed Res Int. 2015;2015. doi:10.1155/2015/580650
48. Hem E, Stokke G, Tyssen R, Grønvold NT, Vaglum PEØ, Ekeberg Ø. Self-prescribing among young Norwegian doctors: a nine-year follow-up study of a nationwide sample. BMC Med. 2005;3(1):16. doi:10.1186/1741-7015-3-16
49. Petrovi AT, Stilinovi N, Kusturica MP. Self-medication perceptions and practice of medical and pharmacy students in Serbia. Int J Environ Res Public Health. 2022;19(3):1193.
50. Klemenc-keti Z, Kersnik J, Cross Sectional A. Study of sex differences in self-medication practices among university students in Slovenia. Coll Antropol. 2011;35:329–334.
51. Williams AA, Crawford K. Self-medication practices among undergraduate nursing and midwifery students in Australia: a cross sectional study. Contemp Nurse. 2016;6178.
52. Behzadifar M, Behzadifar M, Aryankhesal A, et al. Prevalence of self-medication in university students: systematic review and meta-analysis. East Mediterr Heal J. 2020;26:846–857. doi:10.26719/emhj.20.052
53. Gabriel DC, Balakrishna BB, Coll M, Brugada R, Parisi P, Striano P. Knowledge and practices of self-medication among adolescents. Ann Clin Translat Neurol. 2021;8(9):1557–1565. doi:10.1002/acn3.51382
54. Mannasaheb BA, Al-Yamani MJ, Alajlan SA, et al. Knowledge, attitude, practices and viewpoints of undergraduate university students towards self-medication: an institution-based study in Riyadh. Int J Environ Res Public Health. 2021;18(16):16. doi:10.3390/ijerph18168545
55. Hsiao FY, Lee J-A, Huang W-F, Chen S-M, Chen H-Y. Survey of medication knowledge and behaviors among college students in Taiwan. Am J Pharm Educ. 2006;70(2):30. doi:10.5688/aj700230
56. Abebe D, Tenaw G, Dessalegn HFA, Franelee AZ. Knowledge, attitude and practice of self-medication among health science students at DebreMarkos university, Northwest Ethiopia. J public Heal Epidemiol. 2017;9(5):106–113. doi:10.5897/JPHE2017.0926
57. Al FM, Al BK, Hakami WO, Khan SA. Evaluation of self-medication practices in acute diseases among university students in Oman. J Acute Dis. 2014;3(3):249–252. doi:10.1016/S2221-6189(14)60056-1
58. Adebisi AA. Knowledge and Practice of self-medication among students of school of nursing in selected schools in Osun State. Knowl Pract. 2016;4(4):1–10.
59. Patil SB, Vardhamane SH, Patil BV, Santoshkumar J, Binjawadgi AS, Kanaki AR. Self-medication practice and perceptions among undergraduate medical students: a cross-sectional study. J Clin Diagnostic Res. 2014;8(12):10–13.
60. Isameldin E, Saeed AA, Mousnad MA. Self-medication Practice among patients living in Soba. Dspace Reposit. 2020;4:1–5.
61. Gaikwad NR, Patil ABKT. Comparative evaluation of knowledge, attitude and practice of self-medication among first and second year medical students. J Datta Meghe Inst Med Sci Univ. 2010;5:157–162.
62. Rachamanti R, Bano Z. The pattern of self-medication practice among undergraduate medical students of tertiary care hospital, Andhra Pradesh, India. Int J Basic Clin Pharmacol. 2017;6(12):2848–2852. doi:10.18203/2319-2003.ijbcp20175206
63. Badiger S, Kundapur R, Jain A, Kumar A, Patanashetty S, Thakolkaran NB. Self-medication patterns among medical students in South India. AMJ. 2012;5(4):217–220. doi:10.4066/AMJ.2012.1007
64. Ocan M, Bwanga F, Bbosa GS, et al. Patterns and predictors of self-medication in northern Uganda. PLoS One. 2014;9(3):e92323. doi:10.1371/journal.pone.0092323
65. Helal RM, Abou-Elwafa HS. Self-medication in University students from the city of Mansoura, Egypt. J Env Public Heal. 2017;2017:1–7. doi:10.1155/2017/9145193
66. Arikpo G, Eja M. Self-Medication in Rural Africa. Internet J Heal. 2009;11(1):1–7.
67. Shah AP, Parmar SA, Kumkishan A, Knowledge, Attitude and Practice (KAP) Survey Regarding the safe use of Medicines in rural area of Gujarat. Adv Trop Med Pub Heal. 2011;1(2):66–70.
68. Tesfaye ZT, Ergena AE, Yimer BT. Self-medication among medical and nonmedical students at the University of Gondar, Northwest Ethiopia: a cross-sectional study. Scientifica. 2020;2020:1–5. doi:10.1155/2020/4021586
69. Kifle ZD, Mekuria AB, Anteneh DA, Enyew EF. Self-medication Practice and Associated Factors among Private Health Sciences Students in Gondar Town, North West. INQUIRY. 2021;58:1–10.
70. Gutema GB, Gadisa DA, Abebe Z, et al. Self-medication practices among health sciences students: the case of Mekelle University. J Appl Pharm Sci. 2011;1(10):183–189.
71. Al-Qahtani AM, Shaikh IA, Shaikh MAK, Mannasaheb BA, Al-Qahtani FS. Prevalence, perception, and practice, and attitudes towards self-medication among undergraduate medical students of Najran University, Saudi Arabia: a Cross-Sectional Study. Risk Manag Healthc Policy. 2022;15:257–276. doi:10.2147/RMHP.S346998
72. Esan DT, Fasoro AA, Odesanya OE, Esan TO, Ojo EF, Faeji CO. Assessment of self-medication practices and its associated factors among undergraduates of a Private University in Nigeria. J Environ Public Health. 2018;2018:1–7. doi:10.1155/2018/5439079
73. Bhattarai N, Basyal D, Bhattarai N. Self medication practice among undergraduate pharmacy students in Kathmandu Valley, Nepal. Int J Pharma Sci Res. 2014;5(11):737–746.
74. Mathewos T, Daka K, Bitew S, Daka D. Self-medication practice and associated factors among adults in Wolaita Soddo town, Southern Ethiopia. Int J Infect Control. 2021;1:1–8.
75. Kassie AD, Bifftu BB, Mekonnen HS. Self-medication practice and associated factors among adult household members in Meket district, Northeast Ethiopia, 2017. BMC Pharmacol Toxicol. 2018;19(5):4–11. doi:10.1186/s40360-018-0205-6
76. Mekonnen M, Zelalem D, Tezera N. Self-medication practice and associated factors among non-health professional students of university. Hos Pal Med Int Jnl. 2018;2(6):347–353.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude and Practice of Antimicrobial Usage Among Undergraduate Medical Students in Universities and Institutes, Thamar, Yemen
Al-Haifi AY, Al-Shami AS, Al-Akhali KM, Al-Mehdar AA
Infection and Drug Resistance 2025, 18:1675-1686
Published Date: 1 April 2025
Knowledge, Attitude, and Practice of Medical Students Toward Prehospital Emergency Care: A Cross-Sectional Study
Liu X, Wang B, Xing J, Zhang H, Ye S
Advances in Medical Education and Practice 2025, 16:1559-1568
Published Date: 27 August 2025