Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital
Authors ALHazim SS, Al-Otaibi ST, Herzallah NH
Received 19 April 2022
Accepted for publication 10 August 2022
Published 24 August 2022 Volume 2022:15 Pages 1771—1778
DOI https://doi.org/10.2147/JMDH.S371361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Sukainah S ALHazim.
Views: 792
Sukainah S ALHazim,1 Sultan T Al-Otaibi,2 Nawal H Herzallah2
1Occupational Health Department, Dammam Medical Complex, Ministry of Health, Dammam, Saudi Arabia; 2Department of Public Health, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Sultan T Al-Otaibi, Imam Abdulrahman Bin Faisal University, PO Box 1982, Dammam, 31441, Saudi Arabia, Tel +966-13-8948964, Fax +966-13-8645612, Email [email protected]
Background: Musculoskeletal disorders (MSDs) affecting healthcare workers (HCWs) must be considered and addressed as a serious issue. Thus, it is important to incorporate ergonomics into clinical practice to prevent MSDs. The objectives of this study were to investigate HCWs’ knowledge, attitudes, and practices regarding ergonomics in a large governmental healthcare facility.
Methods: A cross-sectional study was conducted in which the participants were interviewed to complete a validated four-section questionnaire (demographic data, knowledge, attitudes, and practice information related to ergonomics). The questionnaire was newly self-developed based on a literature review and was pilot tested after development.
Results: This study included 273 HCWs. Their average knowledge score regarding ergonomics was 2.6, or “fair to good.” Overall, the participants reported good attitude scores, with a total average score of 1 and 2, or “agree to strongly agree.” The findings also indicated that appropriate ergonomics practices were often not implemented, as the average practice score was 1 to 2, or “always to sometimes engaging in bad practice.” The risk factors of being Saudi, being a woman, and having low academic achievement were associated with poor knowledge, attitudes, and practices related to ergonomics among HCWs.
Conclusion: This study showed that the majority of the participants had fair knowledge and good attitudes toward ergonomics at work while practicing. However, the practice of ergonomics at work was not implemented. It is important to apply ergonomics at work to prevent MSDs; therefore, ergonomic principles should be included in the undergraduate health curriculum for all HCWs, with emphasis on practicing ergonomics in their routine clinical work.
Keywords: ergonomic hazards, knowledge, attitude, practice, healthcare worker
Introduction
The International Ergonomics Association defines ergonomics as
the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data, and methods to design to optimize human well-being and overall system performance.1
Ergonomics is also the study of planning the task to fit the laborer (ie, fitting the workstation/task to meet the make-up of the workers) instead of compelling the laborer’s body to fit the work.1,2 Adjusting activities, workstations, apparatuses, and gear to fit the laborer can assist with decreasing the actual impact of the task on the laborer’s body and drive out numerous conceivably genuine and crippling occupational musculoskeletal disorders (MSDs).2–4
MSDs occupy 34% of all lost workday illnesses;5 businesses report almost 600,000 MSD cases requiring time away from work each year. Yearly, this represents $15–18 billion in worker’s compensation direct expenses and up to as much as $50 billion for indirect expenses in the United States.5 For HCWs in the Kingdom of Saudi Arabia (KSA), around 85% of nurses reported encountering no less than one episode of musculoskeletal symptoms.6
The physical redesign of worksites must also be accompanied by appropriate worker practices. Healthcare work is a particularly challenging context to which to apply ergonomic designs because the work is variable and requires behavioral collaboration between the HCWs and their patients. Numerous patients/occupants (particularly in nursing homes) are absolutely reliant upon staff to participate in activities of day-by-day living, such as dressing, washing, general caretaking, and toileting. Every one of these activities includes several postures required to deal with or move patients/occupants that could lead to the development of MSDs. These MSDs lead to exacerbated injury costs, elevated turnover rates, a greater number of sickness absences, and employees shortages.7–9
There are many programs focused on preventing MSDs in HCWs, with most focusing on training (knowledge transmission). Some ergonomics intervention studies emphasizing training have been shown to be beneficial to HCWs by reducing back pain among nurses. However, the persistence of frequent back pain in HCWs suggests the need for an additional approach (eg, back school). Combining physical therapy with ergonomics practices to mitigate occupational back pain among nurses has proven to be effective.10,11
The literature review indicated that specific questions and information related to knowledge, attitudes, and practices toward mitigating ergonomic hazards among HCWs that were published in previous studies can be utilized in future research.7–11
Psychological approaches that have been used to encourage ergonomically safe practices have combined health belief model concepts with the technology acceptance model for personal health management. In addition, an emphasis on using self-efficacy to promote health behaviors can significantly affect workers’ health.12,13
The KSA initiated a program known as Vision 2030 with the ultimate goal of reducing the country’s costs, including work-related injuries from MSDs, and increasing workers’ productivity.14 Therefore, the findings of this study could help policymakers achieve the goals of Vision 2030.
The objectives of this study were to investigate HCWs’ knowledge, attitudes, and practices regarding ergonomics in a large governmental hospital. Ultimately, the findings will highlight the importance of ergonomic preventive measures in day-to-day healthcare practices.
Methods
This research was conducted in the Dammam Medical Complex in Dammam City, KSA. A cross-sectional study was carried out with a convenience sample of 273 HCWs. The participants were interviewed to complete a four-section questionnaire (demographic data, knowledge, attitude, and practice information related to ergonomics). The questionnaire was newly self-developed based on a literature review and was pilot tested after its development. A total of 20 subjects participated in the pilot study.
The biodata of the participants included age, gender, nationality, education level, job title, and work experience. Furthermore, we asked the participants whether ergonomics courses were included in their undergraduate health curricula. All workers were invited to complete a questionnaire (Appendix 1). The structured questionnaire had 31 questions subcategorized under three main indices:
- Knowledge Index (KI): The HCWs’ knowledge regarding applying ergonomics to prevent work-related MSDs was investigated (10 questions). The KI score ranged from 1 to 4 (poor, fair, good, and very good), with a higher score indicating better knowledge.
- Attitude Index (AI): This contained information on the perceived importance of preventing MSDs (16 questions). The range for each attitude-related question was 1 to 5 (strongly agree, agree, neutral, disagree, and strongly disagree), with a lower number indicating a better attitude. A composite attitude score (AI) was calculated by summing the values from all 16 attitude questions; the total range for this variable was from 16 to 80.
- Practice Index (PI): This contained information on self-reported practice during work (5 questions). The range for each practice-related question was 1 to 4 (always, sometimes, rarely, and never), with a higher number indicating better practice. A composite practice score (PI) was calculated by summing the values from all 5 practice questions; the total range of this variable was from 5 to 20.
A research supervisor at Imam Abdulrahman Bin Faisal University validated the contents of the questionnaire using Cronbach’s alpha values for knowledge, attitudes, and practice regarding ergonomics, which were 0.67 (95% confidence interval [CI]: 0.66–0.69), 0.78 (95% CI: 0.74–0.79), and 0.81 (95% CI: 0.80–0.86), respectively.
Ethical Considerations
The study protocol was approved by the Ethical Committee of the General Directorate of Health Affairs of the Ministry of Health in the Eastern Province of the KSA (MOH-IRB-2018-4). It was also approved by the Ethical Committee of Imam Abdulrahman Bin Faisal University. Verbal consent was obtained from each participant because no invasive procedures were involved in this study, which was endorsed by the Ethical Committee. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committees and in consideration of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Analysis
All independent variables were cross-tabulated with the three dependent index variables. In the bivariate analysis, the association between variables was tested using t-tests or the Kruskal–Wallis test for continuous covariates and chi-square tests for categorical data. Spearman’s rank correlation was also utilized to investigate the relationships between continuous and interval categorical variables. Tukey’s test was also used in the statistical analysis.
Regression models were explored for each index variable. Gender and age were included for face validity. Other variables were included in the linear and logistic regression models due to tabular significance with the outcomes of interest. The data were entered and analyzed using IBM SPSS Statistics version 22.0 (Chicago, IL, USA). A P-value of < 0.05 was considered statistically significant.
Results
A total of 273 HCWs from the Dammam Medical Complex participated in this study. Table 1 shows the participants’ characteristics. It was noted that 8.1% of the participants were less than 25 years old, 59.3% were between 25 and 49 years old, and 32.6% were 50 years old or older. Of the participants, 71.4% were male, and 28.6% were female. Additionally, 74.7% of the participants were Saudis, whereas 25.3% were non-Saudis. The majority of the HCWs in this study had degrees: 31.2% had a bachelor’s degree as their highest qualification, and 21.2% had a master’s degree and/or PhD. With regard to job titles, 60.4% of the participants were nurses, 4.4% were residents, 8.8% were technicians, and 26.4% were physicians. As for the amount of work experience, 28.6% of the participants had less than 5 years of experience, 27.1% had between 5 and 10 years, and 44.3% had more than 10 years.
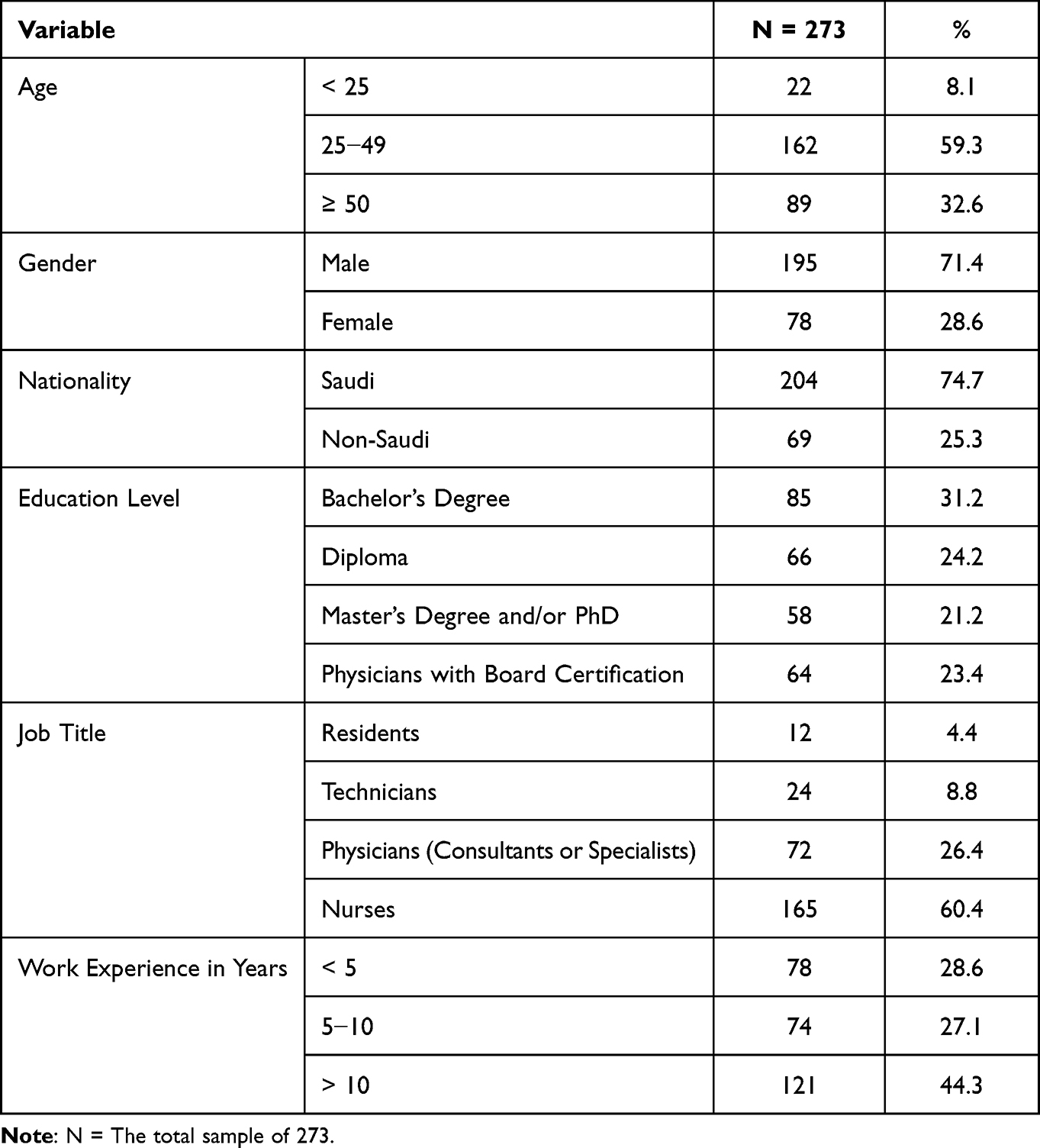 |
Table 1 Demographic Characteristics of the Participants |
As shown in Table 2, the average knowledge score, KI, was 2.6, or “fair to good.” Overall, the participants reported good attitude scores, with a total average AI score of 30/80. The average for each of the 16 attitude questions was between 1 and 2, or “agree to strongly agree.” Results indicated that appropriate practices were often not implemented, as shown by a total average PI score of 10/20 from the 5 questions. The average of the answers for each of the 5 practice questions was 1 to 2, or “always to sometimes engaging in bad practice.”
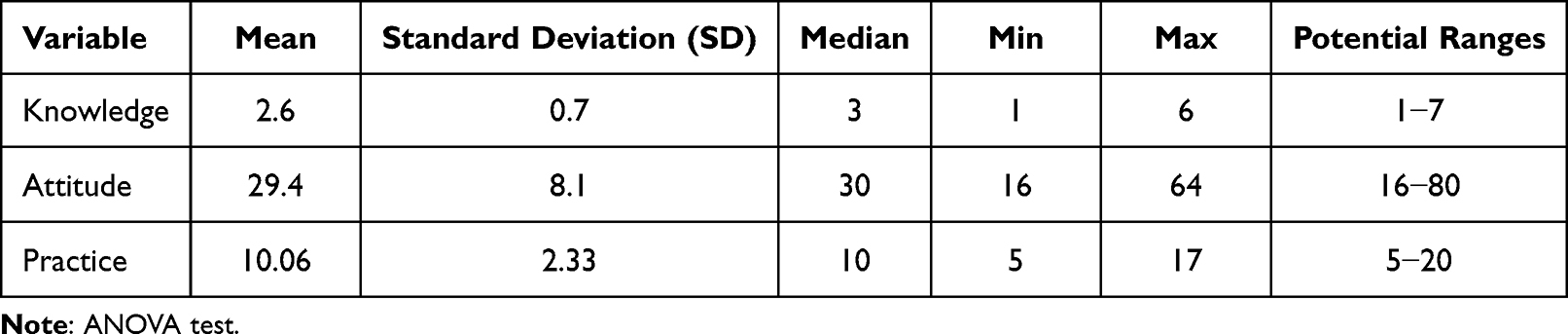 |
Table 2 Knowledge, Attitudes, and Practice Toward Ergonomics Among the Participants |
The three indices all differed according to education level. Workers (physicians) who were board certified had better knowledge (mean = 3.04, p = 0.01), attitudes (mean = 25.3, p = 0.002), and practices (mean = 10.8, p = 0.002) than other workers. The workers with a diploma had the worst knowledge (mean = 2.5, p = 0.01), attitudes (mean = 30.4, p = 0.002), and practices (mean = 9.3, p = 0.002). These results are shown in Table 3.
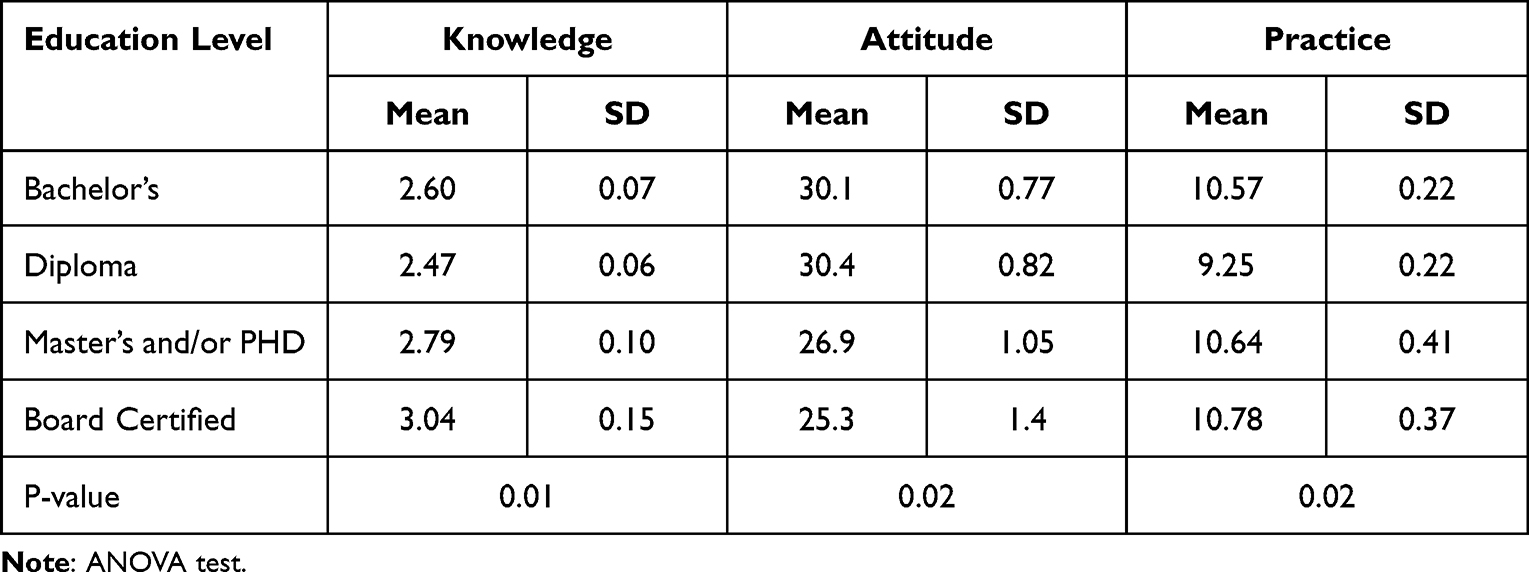 |
Table 3 Differences in the Three Indices According to Level of Education |
There were statistically significant differences in the three indices according to job category, as physicians had the best attitudes (mean = 28.6, p = 0.02) and practices (mean = 10.7, p = 0.02) compared to the other job categories. The post hoc test (Tukey’s test) results showed that there was a significant difference in the mean scores for attitudes and practices among physicians (p = 0.014 and p = 0.012, respectively).
Technicians and pharmacists showed the worst attitudes toward ergonomics (mean = 31.7 and 30.8, respectively, p = 0.02), whereas they had good ergonomics practices (mean = 9.4 and 10, respectively, p = 0.02). Knowledge of ergonomics was statistically insignificant for all job categories. These results are shown in Table 4. All Saudi participants indicated that ergonomics courses were not included in their undergraduate health curricula.
 |
Table 4 Differences in the Three Indices According to Job Title |
The non-Saudis also had higher knowledge, with an average of 2.8 (“good”) compared to 2.5 for the Saudis (p = 0.006). The Saudis’ attitudes toward ergonomics were not as positive as non-Saudis’ (mean = 30.1 compared to 25.3, respectively, p = 0.041). Non-Saudis had better ergonomic practices (mean = 10.7 compared to 9.9 on average, p = 0.005). These results are shown in Table 5.
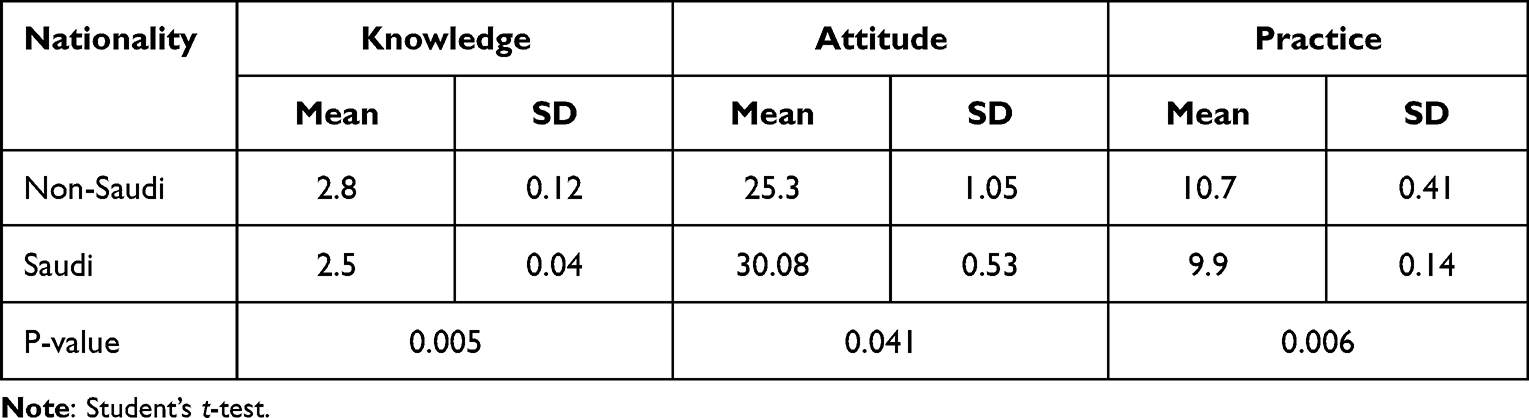 |
Table 5 Differences in the Three Indices According to Nationality |
Univariate regression analyses showed that AI was significantly associated with nationality (p = 0.01); Saudis had worse AI scores on average than non-Saudis. Physicians had better AI scores than nurses (p = 0.02). From the regression model for PI, those with a diploma engaged in significantly worse practices than those with a bachelor’s degree or board certification (p = 0.01 and p = 0.04, respectively). Men engaged in significantly better practices than women (p = 0.03).
A multiple logistic regression model was used to explore the relationship between the aforementioned covariates and KI (comparing the odds of good or very good knowledge to very poor or poor knowledge). Workers with board certification had significantly higher odds of having good knowledge than those with a bachelor’s degree, with an odds ratio of 3.6 (95% CI: 2.8, 6.1; p = 0.02).
Discussion
MSDs have been reported as common and costly problems among HCWs, and they have been attributed to the poor design of workplace ergonomics. However, this study and previous studies have also found that ergonomics was neglected from both the knowledge and practice perspectives by HCWs during clinical work.15–18
This study revealed that the participants had fair knowledge of ergonomics in preventing MSDs, and the same finding was also previously reported among dental care teams.19 The HCWs in this study had positive attitudes toward ergonomics, but they did not implement ergonomic practices during their work, as PI scores in the current study were low. A similar finding was reported in other studies where HCWs also accepted the importance of applying ergonomics while working but neglected to implement relevant practices.20,21
In this study, there was a statistically significant association between the highest academic level of HCWs (physicians with board certification) and knowledge, attitudes, and practices regarding ergonomics. Furthermore, physicians, compared to all other job categories, had the best attitudes. These findings were in agreement with other studies that reported good knowledge and attitudes among participants who had more progressive academic levels and job titles, leading to a low prevalence of musculoskeletal complaints related to ergonomic hazards among physicians.19,22
The non-Saudis in this study had better knowledge, attitudes, and practices regarding ergonomics compared to the Saudi HCWs; this might be explained by ergonomics being a part of non-Saudis’ undergraduate health curriculum. This finding was previously reported among expatriate HCWs working in the KSA.23
In this study, we found that the participants had fair knowledge and poor practices regarding ergonomics during their daily work activities. Risk factors for this outcome included being Saudi, being a woman, job title, and low academic achievements.
HCWs are prone to MSDs due to their lack of awareness of ergonomic principles when practicing clinical work. If ergonomic principles were applied in healthcare facilities, occupational ergonomic health hazards could be prevented, enhancing HCWs’ safety.24–26 These occupational ergonomic hazards at hospitals include the design of the workplace and workstation, working in awkward positions, and repetitive procedures.9,27 Program administrators should consider a job’s characteristics and required physical tasks to provide important intervention opportunities for preventing work-related MSDs among the staff. A behavioral preventive model should be applied. Our results are consistent with the widely used Health Belief Model.28 This is a mental well-being conduct model to clarify and anticipate well-being-related practices, especially the adoption of healthcare services. Unless workers understand and believe that the health consequences of ergonomic hazards are both serious and preventable, prevention efforts may remain inadequate. Additionally, a clear and concise protocol policy statement, along with health and safety committees, is needed for the management and prevention of MSDs to contribute through occupational health programs.29,30 The results that demonstrated that HCWs had fair to good knowledge of ergonomics showed that the respondents clearly endorsed this idea.
Conclusion
This study showed that the majority of participants had fair knowledge and a good attitude regarding ergonomics at work. However, ergonomic practices were not generally implemented at work. Risk factors identified in this study included being Saudi, being a woman, and holding a low academic degree. It is important to apply ergonomics at work to prevent MSDs; therefore, ergonomic principles should be included in the undergraduate health curriculum for all HCWs to emphasize the practice of ergonomics in their routine clinical work.
Limitations of This Study
- This cross-sectional study was susceptible to survivor bias because it assessed prevalence rather than incidence and did not consider workers who had retired or resigned.
- This study was subject to reporting bias, as personal data were collected via a questionnaire.
- The researchers were unable to find many national statistics with which to compare our findings directly.
Author Contributions
All authors made significant contributions to the work reported, whether in its conception, study design, execution, data acquisition, analysis, interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was not supported or funded by any drug company.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Anonymous. International ergonomics association (IEA) [Internet]; [cited June 27, 2021]. Available from: https://iea.cc/what-is-ergonomics/.
2. Bridger RS. Introduction to Human Factors and Ergonomics.
3. Wilson JR. Fundamentals of systems ergonomics/human factors. Appl Ergon. 2014;45(1):5–13. doi:10.1016/j.apergo.2013.03.021
4. Poole Wilson T, Davis KG. Health care ergonomics: contributions of Thomas Waters. Hum Factors. 2016;58(5):726–747. doi:10.1177/0018720816648553
5. Anonymous. OSHA. Ergonomics programs: preventing musculoskeletal disorders; [Cited June 27, 2021]. Available from: https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=4167&p_table=UNIFIED_AGENDA.
6. Attar SM. Frequency and risk factors of musculoskeletal pain in nurses at a tertiary center in Jeddah, Saudi Arabia: a cross sectional study. BMC Res Notes. 2014;7(1):61. doi:10.1186/1756-0500-7-61
7. Choi SD, Brings K. Work-related musculoskeletal risks associated with nurses and nursing assistants handling overweight and obese patients: a literature review. Work. 2015;53(2):439–448. doi:10.3233/WOR-152222
8. Schlussel AT, Maykel JA. Ergonomics and musculoskeletal health of the surgeon. Clin Colon Rectal Surg. 2019;32(6):424–434. doi:10.1055/s-0039-1693026
9. Che Huei L, Ya-Wen L, Chiu Ming Y, Li Chen H, Jong YW, Ming Hung L. Occupational health, and safety hazards faced by healthcare professionals in Taiwan: a systematic review of risk factors and control strategies. SAGE Open Med. 2020;
10. Karahan A, Bayraktar N. Effectiveness of an education program to prevent nurses’ low back pain: an interventional study in Turkey. Workplace Health Saf. 2013;61:73–78.
11. Jaromi M, Nemeth A, Kranicz J, Laczko T, Betlehem J. Treatment and ergonomics training of work-related lower back pain and body posture problems for nurses. J Clin Nurs. 2012;21(11–12):1776–1784. doi:10.1111/j.1365-2702.2012.04089.x
12. Ahadzadeh AS, Pahlevan Sharif S, Ong FS, Khong KW. Integrating health belief model and technology acceptance model: an investigation of health-related internet use. J Med Internet Res. 2015;17(2):e45. doi:10.2196/jmir.3564
13. Schopp LH, Bike DH, Clark MJ, Minor MA. Act Healthy: promoting health behaviors and self-efficacy in the workplace. Health Educ Res. 2015;30:542–553. doi:10.1093/her/cyv024
14. Anonymous. 2030 Vision of Saudi Arabia; [Cited May 26, 2021]. http://vision2030.gov.sa/en.
15. Gomaa AE, Tapp LC, Luckhaupt SE, et al. Occupational traumatic injuries among workers in health care facilities - United States, 2012–2014. MMWR Morb Mortal Wkly Rep. 2015;64(15):405–410.
16. Oranye NO, Wallis B, Roer K, Archer-Heese G, Aguilar Z. Do personal factors or types of physical tasks predict workplace injury? Workplace Health Saf. 2016;64(4):141–151. doi:10.1177/2165079916630552
17. Bin Homaid M, Abdelmoety D, Alshareef W, et al. Prevalence and risk factors of low back pain among operation room staff at a Tertiary Care Center, Makkah, Saudi Arabia: a cross-sectional study. Ann Occup Environ Med. 2016;28:1. doi:10.1186/s40557-016-0089-0
18. Ephraim-Emmanuel B, Ogbomade R, Idumesaro B, Ugwoke I. Knowledge, attitude and practice of preventing the occurrence of work-related musculoskeletal disorders among doctors in University of Port-Harcourt Teaching Hospital. J Med Res Innov. 2019;3(2):e000161. doi:10.32892/jmri.161
19. Bârlean L, Dănilă I, Săveanu I. Dentists ergonomic knowledge and attitude in north-east region, Romania. Romanian J Oral Rehabil. 2012;4(1):40–43.
20. Kalghatgi S, Prasad KV, Chhabra KG, Deolia S, Chhabra C. Insights into ergonomics among dental professionals of a dental institute and private practitioners in Hubli-Dharwad twin cities, India. Saf Health Work. 2014;5(4):181–185. doi:10.1016/j.shaw.2014.09.001
21. Bushra R, Ayesha A, Afsheen A, Anum T. Ergonomic hazards to dental surgeons: a cross-sectional study. Pak Oral Dent J. 2016;36:168–177.
22. Mehrdad R, Dennerlein JT, Morshedizadeh M. Musculoskeletal disorders and ergonomic hazards among Iranian physicians. Arch Iran Med. 2012;15(6):370–374.
23. Haleem A. Evaluation of ergonomic aspects of meal trolleys in Jazan region hospitals to ameliorate musculoskeletal disorder. J King Saud Univ Eng Sci. 2016;27(2):51–66.
24. Siddiqui TM, Wali A, Khan OH, Khan M, Zafar F. Assessment of knowledge, practice, and work environment related to ergonomics among dental students and dental practitioners. Int J Contemp Dent Med Rev. 2016;2016:40316. https://core.ac.uk/download/pdf/228420611.pdf.
25. Seyed AZ, Mohammad RM, Somayeh FD, Majid HM, Hossein S, Mehdi A. Relationship between knowledge of ergonomics and workplace conditions with musculoskeletal disorders among nurses: a questionnaire survey. World Appl Sci J. 2013;24:227–233.
26. Ashu MA, Kamo H. Work-related musculoskeletal disorders amongst oral health workers in Cameroon. Oral Health Dent Manag. 2016;15:1–6.
27. Ketkar GN, Malaiappan S. Knowledge attitude and practice of ergonomics and musculoskeletal disorders as an occupational hazard among periodontists in India – a questionnaire based survey. Int J Pharm Res. 2020;32(20):162–183. doi:10.9734/jpri/2020/v32i2030739
28. Green EC, Murphy EM, Gryboski K. The health belief model. In: The Wiley Encyclopedia of Health Psychology. 2020. doi:10.1002/9781119057840.ch68
29. Sakzewski L, Naser-ud-Din S. Work-related musculoskeletal disorders in Australian dentists and orthodontists: risk assessment and prevention. Work. 2015;52(3):559–579. doi:10.3233/WOR-152122
30. Feiler JL, Stichler JF. Ergonomics in healthcare facility design, part 2: support areas. J Nurs Adm. 2011;41(3):97–99. doi:10.1097/NNA.0b013e31820c72a1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Knowledge, Attitude and Associated Factors of Monkeypox Infection Among Healthcare Workers in Injibara General Hospital, Northwest Ethiopia
Aynalem ZB, Abate MD, Meseret F, Muhamed AN, Abebe GK, Adal AB, Wondmieneh A, Andualem A, Ademe S, Workye H, Bewket B, Beyene GA, Alene T, Tsega TD
Journal of Multidisciplinary Healthcare 2024, 17:1159-1173
Published Date: 15 March 2024
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024