Back to Journals » Journal of Pain Research » Volume 15
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Authors Thapa P ![]() , KC B
, KC B ![]() , Lee SWH
, Lee SWH ![]() , Dujaili JA
, Dujaili JA ![]() , Gyawali S, Mohamed Ibrahim MI
, Gyawali S, Mohamed Ibrahim MI ![]() , Alrasheedy AA
, Alrasheedy AA ![]()
Received 3 February 2022
Accepted for publication 14 May 2022
Published 2 June 2022 Volume 2022:15 Pages 1587—1599
DOI https://doi.org/10.2147/JPR.S360243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Twillman
Parbati Thapa,1 Bhuvan KC,1,2 Shaun Wen Huey Lee,1 Juman Abdulelah Dujaili,1 Sudesh Gyawali,3 Mohamed Izham Mohamed Ibrahim,4 Alian A Alrasheedy5
1School of Pharmacy, Monash University Malaysia, Subang Jaya, Selangor, Malaysia; 2College of Public Health, Medical, and Veterinary Sciences, James Cook University, Townsville, Queensland, Australia; 3Department of Pharmacology, Manipal College of Medical Sciences, Pokhara, Nepal; 4Department of Clinical Pharmacy and Practice, College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 5Department of Pharmacy Practice, College of Pharmacy, Qassim University, Buraidah, Qassim, Saudi Arabia
Correspondence: Bhuvan KC, School of Pharmacy, Monash University Malaysia, Jalan Lagoon Selatan, Subang Jaya, Selangor, 47500, Malaysia, Email [email protected] Alian A Alrasheedy, Department of Pharmacy Practice, College of Pharmacy, Qassim University, Buraidah, Qassim, Saudi Arabia, Email [email protected]
Background: Pain is a public health problem and affects millions of people globally. Effective pain management is possible through comprehensive pain management guidelines, adequate facilities, and trained healthcare professionals. Therefore, this study aims to analyze the healthcare professionals’ knowledge, attitude, and practice regarding pain management in Western Nepal.
Methods: A cross-sectional study was carried out in hospitals of Pokhara, Nepal. Healthcare professionals, including doctors, pharmacists, and nurses, were enrolled. Tools for the study were “The Knowledge and Attitudes Survey Regarding Pain (KASRP)” and a validated practice-based questionnaire. Frequencies and descriptive statistics were used to describe the outcomes. Kruskal–Wallis H-test and Mann-Whitney U-test were used to analyze the association between the mean rank of KASRP score and sample characteristics. A p-value of < 0.05 was considered significant for all statistical tests.
Results: A total of 336 healthcare professionals were enrolled in this study (108 medical doctors, 150 nurses, and 78 pharmacists). The mean KASRP scores (% ± SD) obtained by doctors, pharmacists, and nurses were 58.48± 8.98, 53.01± 7.80, and 52.26± 6.39, respectively. A significant difference was found between the KASRP score and sample characteristics (p< 0.001). The pain assessment tool is used by 96 (29%) healthcare professionals every time they meet the patients. Doctors and nurses used it more frequently as compared to pharmacists. Many of the pharmacists, 40 (51%), reported that they counsel the patients on the prescribed medicine (analgesics, NSAIDs, and opioids) every time. As only few participants had already attended a training on pain management, most healthcare professionals, 110 (33%), agreed and 198 (59%) strongly agreed that training related to pain management is needed in Nepal
Conclusion: Adequate training and support are required to enhance the knowledge, attitude and ultimately better practice for healthcare professionals regarding pain management in Nepal.
Keywords: pain management, knowledge, attitude, practice, healthcare professionals, Nepal
Background
Pain is a common healthcare problem that affects millions of people globally and contributes to seeking medical care for patients.1 Acute pain is initiated by a specific injury or disease coupled with activation of the sympathetic nervous system and self-limited. In contrast, chronic pain is a disease state that outlasts the average healing time and persists or recurs for three months or more.2,3 The International Association for the Study of Pain (IASP) estimates that 1 in 5 patients experience pain and 1 in 10 patients are diagnosed with chronic pain every year.1 The prevalence of chronic pain in low- and middle-income countries (LMICs) varies between 34 and 41%. It causes a high clinical, financial and humanistic burden on people where the public health systems are inadequate and underfunded.4 In Nepal, the prevalence of chronic pain was estimated to be 48–50%, while 24–41% in India.5
Effective pain management requires a comprehensive approach comprising national strategy and guidelines on pain management, adequately trained human resources, and proper healthcare facilities/settings. Pain management in LMICs, especially in developing countries, is inadequate. The infrastructure, human resources, and clinical systems to manage pain are lacking in developing countries.6,7 Access to information and specialist pain service is limited in Nepal.8 Like in other chronic disease management, people often rely on medical care that one can access via out-of-pocket spending at private healthcare facilities.9
Adequate pain management needs a national strategy that recognizes pain as an essential aspect of secondary and long-term care. Institutional guidelines and policies on pain management are formed based on the federal system. In line with this goal, the IASP has recommended various methods to improve pain care including access to pain education for healthcare providers and the general population, coordination of care, quality improvement program, and funding for pain research.10
Proper pain management needs healthcare professionals to be appropriately trained on pain management, which involves appropriately assessing pain and selecting the right medicines and approaches. Therefore, the knowledge and training of healthcare professionals on pain education form the backbone of improved pain care. Studies carried out among healthcare professionals in several countries have revealed varied responses ranging from sufficient to inadequate level of knowledge, attitude, and practice on pain management. Low scores were obtained on key aspects of pain management, including initial assessment, treatment plan, reassessment, and knowledge of the pharmacology of medications, especially narcotics.11,12 Studies have also reported poor knowledge and attitudes regarding pain relief among healthcare professionals, lack of access to medicines and proper pain treatment, financial and socioeconomic factors among patients as the main barriers to effective pain management.13 These studies highlight the need to assess healthcare providers’ knowledge regarding pain management in each country and provide training and support as per the local needs.
In Nepal, patients with acute or chronic pain visit hospitals (both public and private), clinics, and other available healthcare facilities that could provide pain management. For minor ailments, including mild to moderate pain, patients prefer self-medication with the available over-the-counter medications.14 Many patients visit tertiary care hospitals or hospitals because of the availability of multiple facilities at low cost and the available insurance policy. Some institutions have pain management clinics that provide outpatient services and interventions. A multidisciplinary approach to pain management is gradually emerging in Nepal, especially in the private sector. There are very few specialized pain management clinics in the country,8 and most of them are localized in the capital city Kathmandu. A study by Shakya et al has reported strict opioid regulation, lack of knowledge among patients about pain management, insufficient staff, and the least priority for pain management services as barriers to pain management in Nepal.15 Furthermore, Nepal lacks a comprehensive pain management strategy at the national level that deals with procedures, policies, systems, and human resources required to manage chronic pain. There is inadequacy in terms of proper training of healthcare professionals on pain management, availability of therapeutic resources, and dedicated pain management programs in hospitals.16 Very few studies have been conducted in Nepal regarding the knowledge, attitude, and practice of healthcare professionals on pain management, and the studies focused only on nurses.15,17
There have not been any attempts to assess and compare the knowledge, attitude, and practice (KAP) of doctors, nurses, and pharmacists in pain management in Nepal. Such studies would contribute to pain management policy and improve pain management practice. Consequently, in this study, we aimed to assess the knowledge, attitude, and practice of pain management among medical doctors, pharmacists, and nurses in hospitals in Western Nepal.
Methods
Study Design and Setting
A cross-sectional study was carried out from June to August 2020 at five hospitals in Pokhara, Western Nepal.
Study Population, Sample Size, and Sampling methods
Registered doctors, pharmacists, and nurses who have been working as full-time employees at the hospitals were included in the study. The sample size for the study was 334, calculated by the Raosoft sample size calculator,18 with a margin of error of 5%, confidence level of 95%, the population of 2500, and response distribution of 50%. Healthcare professionals meeting the inclusion criteria and willing to participate in the study were enrolled. A convenience sampling method was used, and all healthcare professionals available during data collection were enrolled until the required sample size was reached.
The Study Instrument
The questionnaire consisted of 3 main parts: the demographic and participants’ data, knowledge and attitude regarding pain, and participants’ practices for pain management. The items for knowledge and attitude regarding pain were adapted from “The Knowledge and Attitudes Survey Regarding Pain (KASRP),” developed by Ferrel and McCaffery, revised in 2014.19 The tool’s content was based on the standards of pain management such as the American Pain Society and the World Health Organization guidelines etc. Internal consistency reliability for this tool was established (alpha r > 0.7). In our study, we have adopted 31 items from the KASRP based on the study objectives. Out of these, 18 were true or false questions, 11 were multiple-choice questions with four options and 2 items from the case study. We did not include some questions/items, especially those related to cancer pain (n=5), pediatric pain (n=2), culture (n=1), and the 2nd case study (n=2). The response to each item of KASRP was scored as “1” for the correct response and a “0” for the incorrect response. The total score was the sum of all correctly answered questions. The percentage score is calculated by dividing the number of correct responses by the total number of items in the survey. Healthcare professionals were considered to have adequate knowledge and attitude if the score was 80% and above, a level identified by McCaffery and Robinson 2002.20 However, the percentage called “adequate” varies among different studies, as some used 80% or above as representing adequate knowledge and attitudes,21 whereas others used 70% as a minimum score.22 Some studies did not even indicate the pass rate.23 According to Ferrel et al, items should be differentiated with the least correct responses and those with the best scores for better response analysis.19 For the participants’ perspectives on the practice of pain management, eight questions were developed to assess their practices based on the literature review,6,12,24 with six questions on a 4-point Likert scale and two yes/no questions. Consequently, the final questionnaire consisted of 39 items and demographic information. The practice was assessed based on the response provided by the healthcare professionals on the Likert scale.
The final questionnaire was checked by a panel of experts comprising pharmacists, physicians, senior nurses, and academicians to ensure clarity and suitability in the Nepalese healthcare system. In addition, pretesting of the questionnaire was conducted among 17 healthcare professionals: six doctors, six nurses, and five pharmacists. They were requested to fill up the form and provide feedback on the questionnaire. The questionnaire was examined for reliability, and its internal consistency was established (Cronbach alpha of 0.73 was obtained for the practice-based questionnaire, and for the KASRP tool, it was 0.7).
Data Collection
The questionnaire was developed in a google form. Department heads of medical, nursing and pharmacy facilities were contacted and requested coordination among staff to fill out the questionnaire. Healthcare professionals working full time in hospitals, registered in respective professional councils, and consented to participate in the study were enrolled.
Data Analysis
Data from the google forms were checked for completeness and accuracy. Data were retrieved on an excel sheet and were transferred to IBM SPSS Statistics for Windows, version 26.0. Frequencies and descriptive statistics were used to describe the sample characteristics and responses to each item of KASRP and the practice-based question. Mann-Whitney U-test and Kruskal-Wallis H-test were used to analyze the association between the mean rank of KASRP score and sample characteristics as data were non-normally distributed. A p-value of <0.05 was considered significant for all statistical tests.
Ethical Consideration
Ethical approval for the study was obtained from the Nepal Health Research Council (Reg no. 211/2020). Permission to collect the data was obtained from institutional review committees of the respective hospitals.
Results
Participants’ Characteristics
A total of 336 questionnaire were completed, mostly by nurses (n=150, 44.6%), followed by medical doctors (n=108, 32.1%) and pharmacists (n=78, 23.2%) from different hospitals. Most of the respondents were female (n=230, 68.5%), and more than two-thirds of them (n=240, 71.4%) were young adults aged 25–35 years old. The demographic characteristics are shown in Table 1.
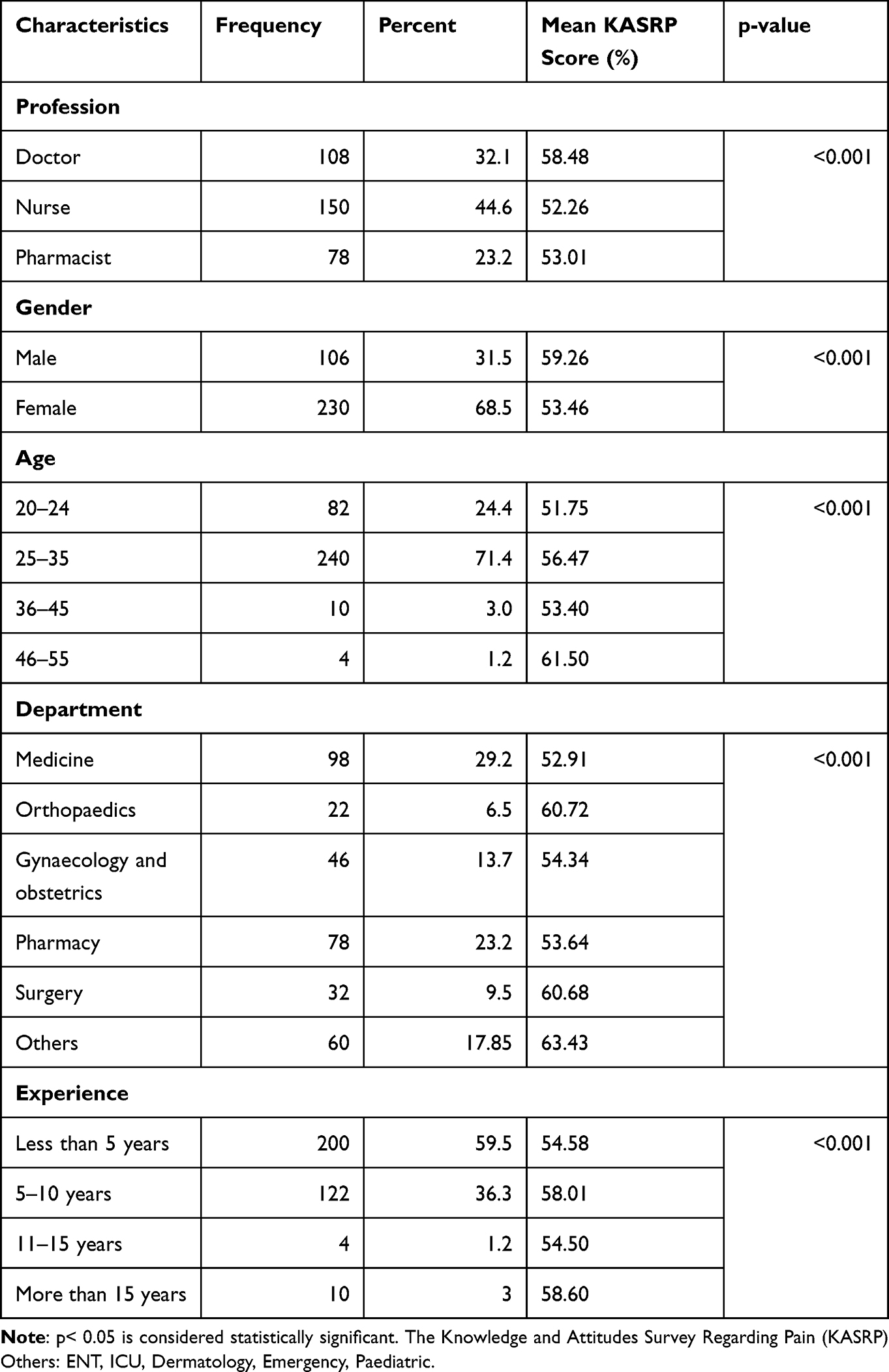 |
Table 1 Demographic Details and the mean Knowledge and Attitudes Survey Regarding Pain (KASRP) Score |
Knowledge and Attitude of Health Care Professionals (HCPs) Regarding Pain
The mean percentage KASRP score obtained was 55.29±8.66 for correct responses. The mean score (% ± SD) obtained by doctors, pharmacists, and nurses were 58.48±8.98, 53.01±7.80, and 52.26±6.39, respectively. The maximum score obtained was 24 (77%), and the minimum was 10 (32%). Most healthcare professionals, 63.1%, have their scores between 40–60%. Details of the score obtained are depicted in Table 2.
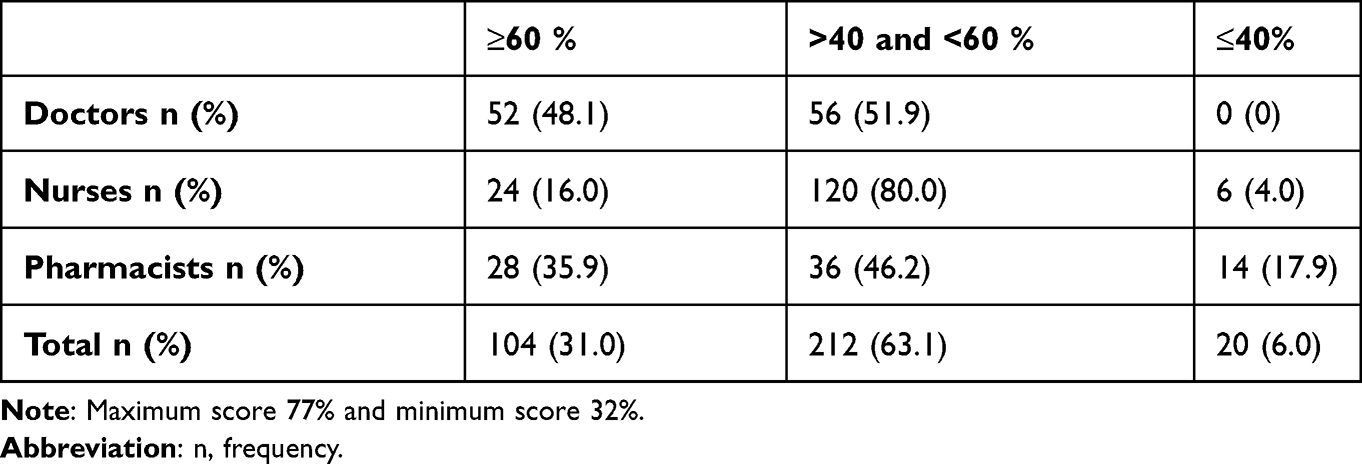 |
Table 2 Distribution of the Knowledge and Attitudes Survey Regarding Pain (KASRP) Score |
Items of the KASRP were classified into assessment, medication, intervention, addiction, and spiritual categories. More than 80% of the healthcare professionals showed a correct response to 5 items of the medication category and 1 item of the addiction category. These items assessed knowledge on respiratory depression due to opioids, the effectiveness of combining analgesics, adjustment of opioid doses, the definition of “equianalgesic,” the peak effect of morphine after intravenous administration, and assessment of sedation during pain management using opioids; however, knowledge and attitude were found poor on using placebo to determine whether the pain is real, initiation of opioid when the source of the pain is not known, use of opioids among patients with substance abuse and symptoms of physical dependency on opioid withdrawal. Details of the correct responses to different items are shown in Table 3.
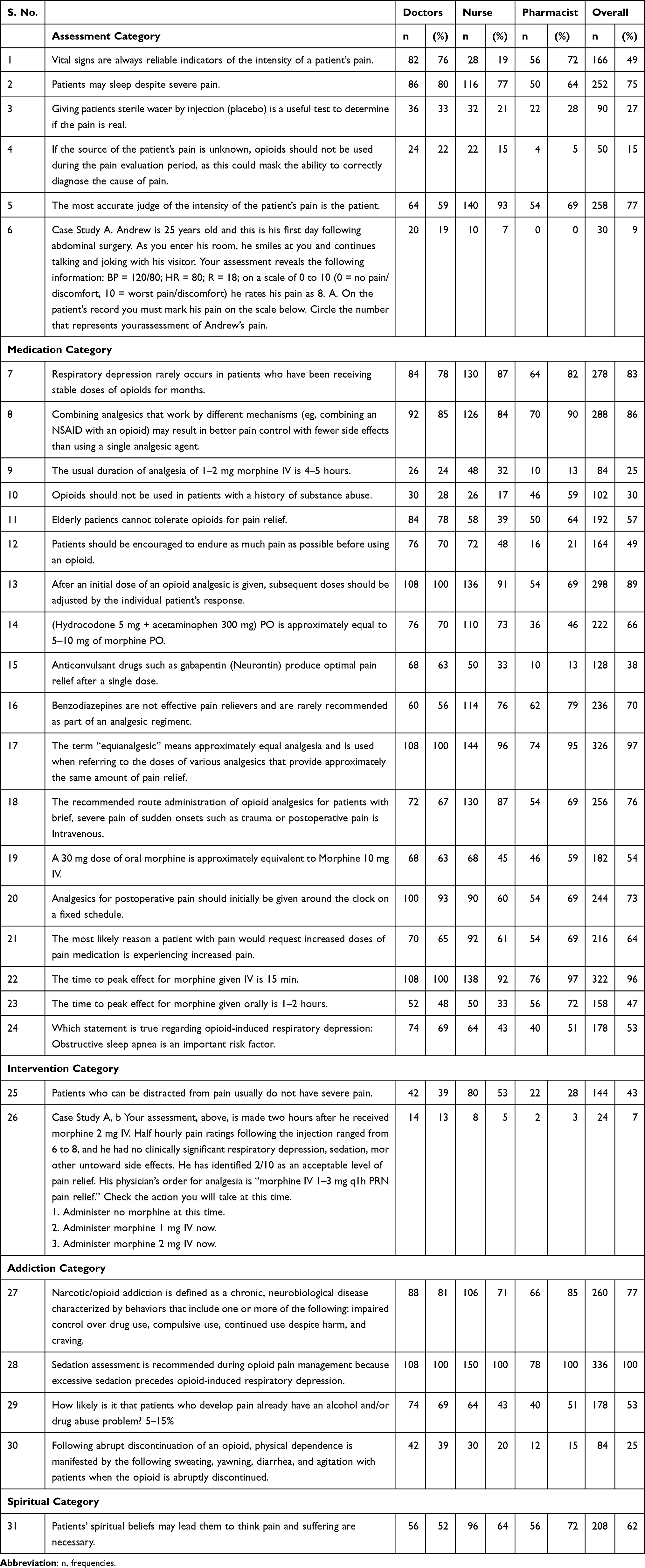 |
Table 3 Frequency of Correctly Answered Questions; the Knowledge and Attitudes Survey Regarding Pain (KASRP) |
Kruskal Wallis tests showed a statistically significant difference in the KASRP score between the professional category (p<0.001), age (p<0.001), department (p<0.001), and their experience (p<0.001). Further pairwise comparison showed a significant difference between doctor and pharmacist, doctor and nurse. For department wise the differences included medicine and surgery, gynaecology/obstetrics and surgery, pharmacy and surgery. A significant difference in score was observed between the gender, as shown by the Mann Whitney U-test (p<0.001). The details are presented in (Table 1).
The Practice of HCPs Regarding Pain Management
Assessment of the practice of healthcare professionals on pain management reveals that only 96 (29%) of them used the pain assessment tool every time during their consultation. Doctors (37%) and nurses (32%) used it more frequently as compared to pharmacists (10%). The verbal/graphic rating scale was reported as the most used tool to assess pain (n=132, 39%). Counselling on the use of analgesics, NSAIDs, opioids, and assessment of allergic response or adverse drug reaction to the prescribed drugs was conducted every time by 128 (38%) healthcare professionals. Similarly, only 100 (31%) of them used opioid risk assessment tools before prescribing, administering, or dispensing. Pharmacist involvement was higher in counselling as 51% reported counselling the patient every time. However, only a few, 10%, assessed the allergic responses and adverse drug reactions. In addition, 30% of the doctors and 41% of the nurses provided the counselling every time, and 44% and 48% assessed allergic responses, respectively.
The majority of them either agreed or strongly agreed that standard pain management guidelines should be followed, and training related to pain management is needed for healthcare professionals in Nepal. However, more than three-quarters of the healthcare professionals (n=254, 76%) reported that they do not follow any specific pain management guidelines. Likewise, the majority (n=284, 85%) of them had never attended any training regarding pain management. Details of the response of healthcare professionals on the practice-based questions are shown in Table 4.
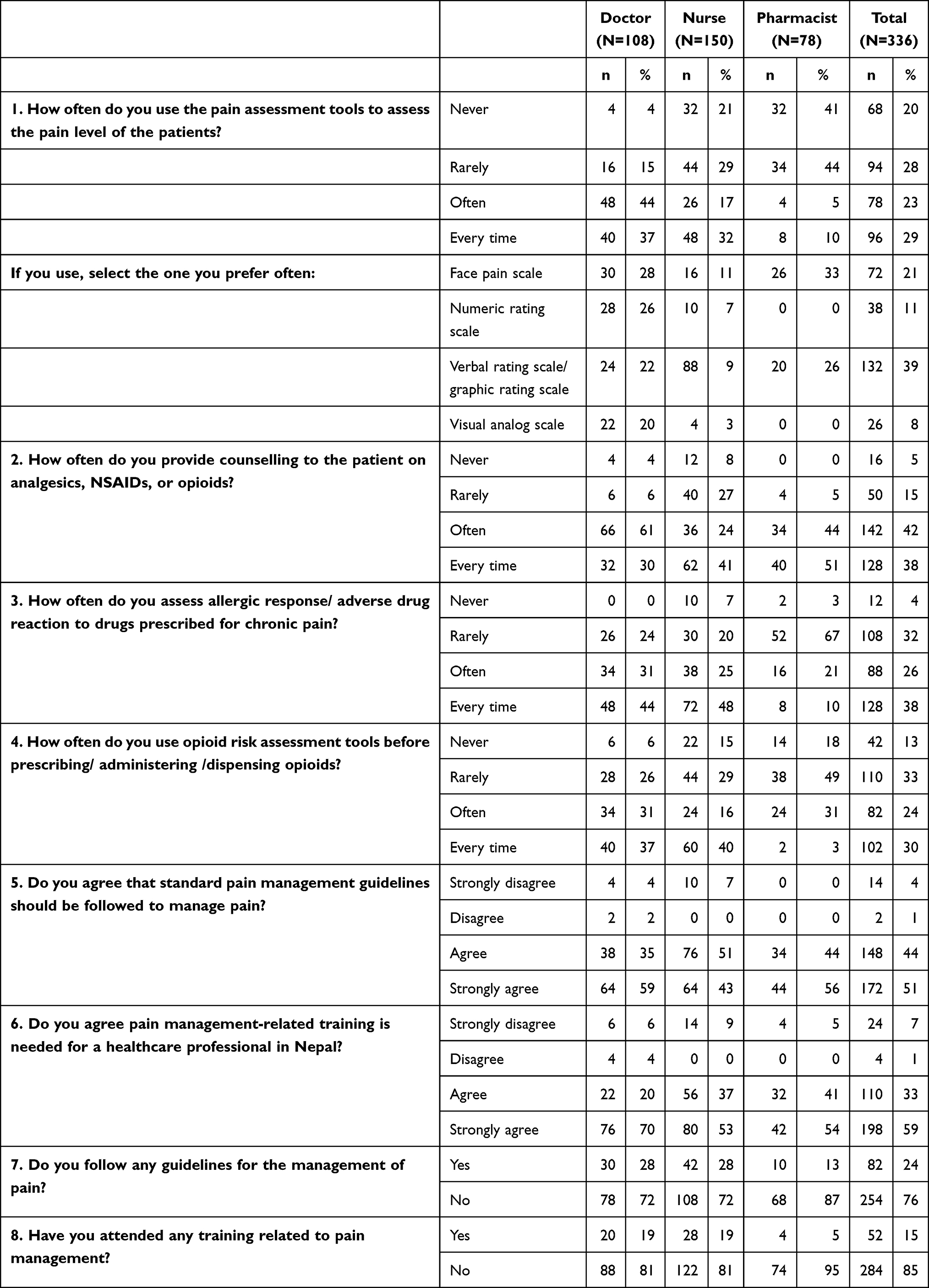 |
Table 4 Response to Practice-Based Question |
Discussion
The current study assessed doctors, pharmacists, and nurses’ knowledge, attitude, and practice regarding pain management in hospitals of Western Nepal. In general, our study indicated that the performance of healthcare professionals on the selected aspect of knowledge and attitude was low to moderate. Healthcare professionals were considered to have adequate knowledge and attitude if the score was 80% and above.20 However, in comparison, doctors’ scored higher than pharmacists and nurses. These results align with several other studies’ outcomes where doctors scored higher than pharmacists or nurses on these aspects.11,12,25 Furthermore, a pairwise comparison shows a significant difference in scores between doctors and nurses, consistent with the results of the studies by Nuseir et al, 2016, Fallatah et al, 2017 and Alkhatib et al, 2020.12,25,26 Doctors’ better knowledge and attitude scores in our study may be due to their experience and prior education on pain management. Doctors lead the current pain management paradigm with only a supportive role for nurses and a minor role/involvement for pharmacists. However, these discrepancies could be resolved through continuing education and the development of multidisciplinary pain management team in an organization.11,27 The low percentage and variation of correct response among the healthcare professionals might be due to inadequate pain management content in the educational curriculum and insufficient training regarding pain management, especially in low resources settings like Nepal.6 Similarly, a lack of institutional policy and guidelines regarding pain management, limited inter-professional education, and knowledge sharing between healthcare professionals could also contribute to the variability in the pain management knowledge and attitude score.
The concept of pain management in Nepal dates to 1970. However, it could not progress much due to a resource crunch, an inadequate public health system, and a lack of comprehensive pain management policy and training system in healthcare institutions. Over the recent years, pain management as a specialized discipline has been increasing as more and more training, fellowship, and practice environments are being provided to healthcare professionals in Nepal.8 However, our study shows that there is still a need for institutional policy and environmental support for pain management, especially in public hospitals outside the Kathmandu valley and other healthcare settings.
A significant difference in KASRP score was observed between different professions (p<0.001), genders (p<0.001), age (p<0.001), department (p<0.001), and experience (p<0.001). Differences in gender might be because almost all nurses were female, and their score was relatively lower than doctors and pharmacists. More than half of the doctors were male and obtained higher scores. This finding is similar to Al-Quliti and Alamri, where there was a statistical difference in scores obtained by physicians compared to nurses.28 In the study findings of Alkhatib et al, there was no significant difference observed based on gender.26 A gender skewed scenario can be observed among healthcare professionals in Nepal as more females work as nurses and more males as doctors. However, the impact of gender differences in KASRP scores between departments and professionals needs further study to see the effect of gender on collaborative practice and knowledge sharing among professionals regarding pain management.
Our study showed that the healthcare professionals scored low (ie, 30% and below) on three items of the assessment category and these items were about the use of sterile water (placebo) to determine whether the pain is real using placebo, use of opioids during the pain evaluation period and pain assessment based on patient medical history and facial expression. Items from the medication category which were less scored were the duration of action of 1–2 mg morphine and the use of opioids among substance abusers. Likewise, one item from the intervention category that dealt with a selection of morphine dose based on pain rating and clinical condition, and one item from the addiction category about symptoms of physical dependency on abrupt cessation of morphine, were also scored low. Most of these items were related to opioids. This result was consistent with the study’s findings by Kheshti et al, where the narcotic questions get the lowest percentage of correct responses.29 Another survey by Nuseir et al, also reported a deficit in knowledge of the pharmacology of narcotics among healthcare professionals.12 The poor knowledge regarding opioids (narcotic analgesics) could probably be due to low use of narcotics, policy constraints, and training regarding its use among healthcare professionals. In hospitals, all healthcare professionals do not have the same privilege /opportunities to prescribe and dispense narcotics which could also be a reason for inadequate knowledge. Narcotics are considered controlled drugs due to their abuse potential.30 Morriss et al reported the poor knowledge and attitude about pain relief and access to opioids as a barrier to pain management in LMICs.13 Nepal has ranked in the bottom three countries in the WHO Regional Office for Southeast Asia (SEARO) between 1996 and 2005 for the consumption of morphine.31 Physicians were reluctant to prescribe opioids due to a lack of education and training in pain management, which led to the expiration of 49% of the sustained release morphine products in 2011. Likewise, though Nepal’s national drug policy promotes the rational use of medicines, there is no specific mention or details, or guidance for opioids for pain management.30 Consequently, adequate training and proper guidelines regarding opioids in pain management are crucial for Nepalese healthcare professionals.
Participants had inadequate knowledge of pain assessment and drug dosing, as reflected by their response to the case study-based question. A small number of healthcare professionals provided the correct response (< 10%). These are similar to the finding of Kahsay et al, where the nurses from resource-limited settings scored least for pain assessment and drug dosing.32 The deficit in pain assessment and management knowledge was also identified among healthcare providers in Saudi Arabia, and the study suggested the requirement of pain education among the providers.25 The lack of comprehensive pain management guidelines that outline a routine assessment of pain in clinical settings and its appropriate might have resulted in low scores on pain assessment and drug dosing.28 Likewise, the selection of minimum doses shows a reluctance from healthcare professionals to prescribe higher doses of analgesics. It also shows that the patients, mostly with moderate to severe pain, might not be receiving adequate analgesics. Healthcare professionals were quite aware of the possible adverse effects of opioids, as depicted by the response to item “22,” where all of them correctly answered the questions about the sedation assessment during opioid management to prevent respiratory depression. So, a fear of side effects from a higher dose of opioids and other factors might have contributed to using a low dose of analgesics (narcotic analgesics). Inadequate pain treatment is a grave issue, and we need studies to identify possible reasons for the use of analgesics with low doses.
Practice related to pain management among healthcare professionals revealed that still few doctors, pharmacists, and nurses do not use any assessment tool to assess the patient’s pain level, which is consistent with the findings of Shakya et al, 2020 and Nuseir et al, 2016.6,12 Limited consultation time of the physician’s 5.26±2.31 minutes33 due to several contributing factors; higher patient flow, workload and lack of clear protocol on patient assessment could also have impacted the pain assessment. Likewise, inadequate training and inappropriate nurse-to-patient ratios were considered barriers to implementing the nursing process, which could relate to pain assessment as well.34
The verbal or graphical rating scale is the most widely used tool to assess pain in the current study, in contrast to the study by Shakya et al, 2020 where the visual analog scale was primarily used almost by 84% of healthcare professionals.6 However, there is still variation in the choice of pain assessment tool between healthcare professionals. A common practice for pain assessment of outpatients in Nepal is to verbally ask the patient the intensity and types of pain and note the patient’s response. This could be due to the lack of implementation of pain management guidelines and knowledge of the available pain assessment tools. However, nurses use different pain assessment tools in the in-patient hospital settings, including the numeric pain rating scale35 and The Wong-Baker Faces Pain Rating Scale.10 These pain assessment tools are available in Nepalese languages, and they can be used in hospital and clinical settings for better practice. Likewise, pain characterization with an appropriate tool like McGill pain questionnaire could help in better pain assessment and management.36
Most pharmacists reported that they never or rarely used the pain assessment tool. Clinical pharmacy practice is a recent establishment in Nepalese hospital settings as per the government’s directive (2015 hospital pharmacy guidelines).37 Nepalese hospital pharmacists are primarily involved in dispensing medications and counselling. Their involvement in pain management activities such as pain assessment, pain medication education, and pharmacotherapy review of pain medications are still lacking in Nepalese hospitals. Therefore, pharmacists have less opportunity to deal with the patient’s symptoms as they meet the patient only after the assessment is complete. This trend might change if more clinical pharmacists are well trained and involved in multidisciplinary pain management teams involving nurses, physicians, and pharmacists are set up at Nepalese hospitals in the near future. These pharmacists can help with pain management via medication review, pain assessment, discharge counselling, medication reconciliation, and medication education.38
Most healthcare professionals provide counselling on the use of NSAIDs and opioids, assess allergic responses, and use the opioid risk assessment tool. Patients managing their pain via self-medication practice with paracetamol and NSAIDs is high in Western Nepal, where this study was carried out.39 These NSAIDs are over-the-counter drugs and may benefit mild to moderate pain or manage chronic pain. However, OTC analgesics, without proper consideration, could result in adverse effects and serious complications such as gastrointestinal bleeding and kidney diseases.14 Pharmacists need to promote the safe use of OTC analgesics in Nepal via appropriate dispensing and medication safety education.40
More than three-quarters of the healthcare professionals (76%) reported that currently, they do not follow any standard pain management guidelines, and very few follow the WHO pain management guidelines. Likewise, 85% of the healthcare professionals have not attended any training regarding pain management. However, they agreed that standard protocol should be followed, and pain-related training should be provided to the healthcare professionals in Nepal. Comprehensive pain management guidelines are essential as they promote evidence-based practice. Many international and national pain management guidelines are available. However, there are no specific pain management guidelines formulated or made mandatory to follow in Nepal. Pain management has not been given priority in secondary and tertiary care settings.6 This could be the barrier to optimal practice. The treatment gap in pain management is prevalent in Nepal and many developing countries. Inadequate education and training of health professionals coupled with limited resources and facilities for pain management and limited access to medicines for pain relief are the significant reasons for this gap. In addition to the government policies, fear of opioid addiction, patient noncompliance, and the high cost of medication are the barriers to effective pain management in developing countries, as per the International Association for the Study of pain study.16 So, it is necessary for the hospital management and healthcare professional’s organization to be aware of the status of pain management and provide the essential training and support to enhance the knowledge, attitude, and improve practice.
Overall, the study findings emphasize the need for developing a national pain management strategy and comprehensive institutional guidelines for hospitals, primary care centers, and community pharmacies. A systematic assessment and management of pain can be carried out at Nepal’s different healthcare facilities. Revision of the healthcare professionals teaching curriculum with the addition of modules on pain management could have positive impact on the practice. Continuing Professional Development training modules for doctors, nurses, and pharmacists will help them enhance their knowledge and equip them with the right tools and approaches for pain management.32
Strength and Limitations of the Research
This study depicts healthcare professionals’ current knowledge, attitude, and practice in pain management in Western Nepal. It opens the opportunity for the development and implementation of intervention programs to strengthen the ability of healthcare professionals and healthcare institutions in pain management. Limitations include the study site, only one part of Nepal, so studies with multiple healthcare facilities and a larger sample could provide a better representation of the situations. Data were collected using a self-reported questionnaire which could limit the identification of the problem, so further studies with quantitative and qualitative component could better portray the scenario.
Conclusions
This study highlights the need of improvement in knowledge and attitude toward pain management among healthcare professionals in Western Nepal. Variation of practice exists among healthcare professionals in the implementation of pain assessment tools, opioid risk assessment tools, counselling, and assessing allergic reactions. Only a few participants reported having and following pain management guidelines, and the majority agreed that pain management training is crucial.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11(1):1–5. doi:10.1186/1471-2458-11-770
2. Grichnik KP, Ferrante FM. The difference between acute and chronic pain. Mt Sinai J Med. 1991;58(3):217–220.
3. Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
4. Enright A, Goucke R. The global burden of pain: the tip of the iceberg? Anesth Analg. 2016;123:529–530. doi:10.1213/ANE.0000000000001519
5. Walters LJ, Baxter K, Chapman H, et al. Chronic pain and associated factors in India and Nepal: a pilot study of the Vanderbilt global pain survey. Anesth Analg. 2017;125(5):1616–1626. doi:10.1213/ANE.0000000000002360
6. Shakya BM, Ninadini Shrestha SS. Pain management practices and perceived barriers among the health professionals in different hospitals of Nepal. J Clin Diagn Res. 2020;14(1):UC01–UC05.
7. Goucke R, Morriss W. Pain management in Low and Middle Income Countries (LMIC) just put up with it? Egypt J Anaesth. 2012;28(1):1–2. doi:10.1016/j.egja.2011.11.005
8. Anil Shrestha RA, Shrestha N. Evolution of pain management services in Nepal. Anaesth Intensive Care Med. 2020;24(4):
9. Sapkota T, Houkes I, Bosma H. Vicious cycle of chronic disease and poverty: a qualitative study in present day Nepal. Int Health. 2020;13:30–38.
10. IASP. International association for the study of pain. Available from: https://www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=8340.
11. Lalonde L, Leroux-Lapointe V, Choinière M, et al. Knowledge, attitudes and beliefs about chronic noncancer pain in primary care: a Canadian survey of physicians and pharmacists. Pain Res Manag. 2014;19(5):241–250. doi:10.1155/2014/760145
12. Nuseir K, Kassab M, Almomani B. Healthcare providers’ knowledge and current practice of pain assessment and management: how much progress have we made? Pain Res Manag. 2016;2016:1–7. doi:10.1155/2016/8432973
13. Morriss W, Roques C. Pain management in low-and middle-income countries. BJA Educ. 2018;18(9):265–270. doi:10.1016/j.bjae.2018.05.006
14. Thapa S, Shankar P, Palaian S, et al. Promoting rational self. medication of nonsteroidal anti. inflammatory drugs in Nepal. Arch Pharm Pract. 2016;7(2):61–66. doi:10.4103/2045-080X.181035
15. Shakya BM, Shakya S. Knowledge and attitude of nurses on pain management in a tertiary hospital of Nepal. Age. 2016;20(24):21.
16. Bond M. Pain education issues in developing countries and responses to them by the International Association for the Study of Pain. Pain Res Manag. 2011;16(6):404–406. doi:10.1155/2011/654746
17. Thapa RD, Gurung G. Nurses’knowledge, attitude and practice regarding postoperative pain management at selected hospitals, Bharatpur, Nepal. J Chitwan Med Coll. 2020;10(1):64–68. doi:10.3126/jcmc.v10i1.28074
18. Raosoft I. Sample size calculator by Raosoft, Inc; 2020.
19. Ferrell BM. “Knowledge and attitudes survey regarding pain” developed by Betty Ferrell, RN, PhD, FAAN and Margo McCaffery, RN, MS, FAAN; 2012. Available from: http://prc.coh.org.
20. McCaffery M, Robinson ES. Your patient is in pain—here’s how you respond. Nursing 2019. 2002;32(10):36–45.
21. Latina R, Mauro L, Mitello L, et al. Attitude and knowledge of pain management among Italian nurses in hospital settings. Pain Manag Nurs. 2015;16(6):959–967. doi:10.1016/j.pmn.2015.10.002
22. Yava A, Çicek H, Tosun N, Özcan C, Yildiz D, Dizer B. Knowledge and attitudes of nurses about pain management in Turkey. Int J Caring Sci. 2013;6(3):494.
23. Keen A, McCrate B, McLennon S, et al. Influencing nursing knowledge and attitudes to positively affect care of patients with persistent pain in the hospital setting. Pain Manag Nurs. 2017;18(3):137–143. doi:10.1016/j.pmn.2017.04.002
24. Louriz M, Belayachi J, Madani N, et al. Practices and perceived barriers regarding pain management among emergency department physicians: a nationwide multicenter survey in Moroccan hospitals. Acute Med Surg. 2016;3(4):360–363. doi:10.1002/ams2.201
25. Fallatah SMA. Pain knowledge and attitude survey among health-care professionals at a university hospital in Saudi Arabia. Saudi J Med Med Sci. 2017;5(2):155–159.
26. Alkhatib GS, Al Qadire M, Alshraideh JA. Pain management knowledge and attitudes of healthcare professionals in primary medical centers. Pain Manag Nurs. 2020;21(3):265–270. doi:10.1016/j.pmn.2019.08.008
27. Hammick M, Freeth D, Koppel I, et al. A best evidence systematic review of interprofessional education: BEME guide no. 9. Med Teach. 2007;29(8):735–751. doi:10.1080/01421590701682576
28. Al-Quliti KW, Alamri MS. Assessment of pain. Knowledge, attitudes, and practices of health care providers in Almadinah Almunawwarah, Saudi Arabia. Neurosciences. 2015;20(2):131–136. doi:10.17712/nsj.2015.2.20140546
29. Kheshti R, Namazi S, Mehrabi M, et al. Health care workers’ knowledge, attitude, and practice about chronic pain management, Shiraz, Iran. Anesthesiol Pain Med. 2016;6(4):e37270–e37270. doi:10.5812/aapm.37270
30. Paudel BD, Ryan KM, Brown MS, et al. Opioid availability and palliative care in Nepal: influence of an international pain policy fellowship. J Pain Symptom Manage. 2015;49(1):110–116. doi:10.1016/j.jpainsymman.2014.02.011
31. Foley KM, et al. Pain control for people with cancer and AIDS. Disease Control Priorities in Developing. World Bank; 2006.
32. Kahsay DT, Pitkäjärvi M. Emergency nurses knowledge, attitude and perceived barriers regarding pain management in resource-limited settings: cross-sectional study. BMC Nurs. 2019;18(1):1–13. doi:10.1186/s12912-019-0380-9
33. Paudel S, Krishna Bahadur GC, Subedi M, Arjyal A, Daha SK, Lamichhane B, Sharma PK.Communication skills of physicians during consultation in out-patient settings at a tertiary hospital in Nepal. Middle East J Fam Med. 2017;7(10):28.
34. Katel K. Nursing process application in Nepal teaching hospital. RUDN J Med. 2022;26(1):79–87. doi:10.22363/2313-0245-2022-26-1-79-87
35. Sharma S, Palanchoke J, Reed D, et al. Translation, cross-cultural adaptation and psychometric properties of the Nepali versions of numerical pain rating scale and global rating of change. Health Qual Life Outcomes. 2017;15(1):236. doi:10.1186/s12955-017-0812-8
36. Melzack R. The short-form McGill Pain Questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
37. Hospital pharmacy guideline 2072. Kathmandu (Nepal): Government of Nepal, Ministry of Health and Population. Available from: http://www.dda.gov.np/content/hospital-pharmacy-guideline-2072
38. Thapa P, Lee SWH, KC B, et al. Pharmacist‐led intervention on chronic pain management: a systematic review and meta‐analysis. Br J Clin Pharmacolog. 2021;87:3028–3042. doi:10.1111/bcp.14745
39. Shankar P, Partha P, Shenoy N. Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: a questionnaire-based study. BMC Fam Pract. 2002;3(1):1–7. doi:10.1186/1471-2296-3-17
40. Phueanpinit P, Pongwecharak J, Krska J, et al. Evaluation of community pharmacists’ roles in screening and communication of risks about non-steroidal anti-inflammatory drugs in Thailand. Prim Health Care Res Dev. 2018;19(6):598–604. doi:10.1017/S1463423618000142
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Role of Community Pharmacist in Asthma Management: Knowledge, Attitudes and Practice
Jarab AS, Al-Qerem W, Alzoubi KH, Almomani N, Abu Heshmeh SR, Mukattash TL, Al Hamarneh YN, Al Momany EM
Journal of Multidisciplinary Healthcare 2024, 17:11-19
Published Date: 3 January 2024
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024