Back to Journals » Patient Related Outcome Measures » Volume 14
Incidence and Predictors of Mortality Among Patients with Traumatic Brain Injury at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: A Retrospective Follow-Up Study
Authors Tegegne NG, Fentie DY ![]() , Tegegne BA
, Tegegne BA ![]() , Admassie BM
, Admassie BM ![]()
Received 14 December 2022
Accepted for publication 29 March 2023
Published 5 April 2023 Volume 2023:14 Pages 73—85
DOI https://doi.org/10.2147/PROM.S399603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Nega Getachew Tegegne,1 Demeke Yilkal Fentie,2 Biresaw Ayen Tegegne,2 Belete Muluadam Admassie2
1Department of Anesthesia, School of Medicine, College of Medicine and Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Anesthesia, School of medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Biresaw Ayen Tegegne, Tel +251-9-27-60-14-27, Email [email protected]
Background: Traumatic brain injury is a major list of health and socioeconomic problems especially in low- and middle-income countries which influences productive age groups. Differences in patient characteristics, socioeconomic status, intensive care unit admission thresholds, health-care systems, and the availability of varying numbers of intensive care unit (ICU) beds among hospitals had shown to be the causes for the variation on the incidence in mortality following traumatic brain injury across different continents. The aim of this study was to assess the incidence and predictors of mortality among patients with traumatic brain injury at University of Gondar Comprehensive Specialized Hospital.
Methods: A retrospective follow-up study was conducted based on chart review and selected patient charts admitted from January, 2017 to January, 2022. Participants in the study were chosen using a simple random sample procedure that was computer generated. Data was entered with epi-data version 4.6 and analyzed using SPSS version 26. Both bivariate and multivariate logistic regression analyses were used, and in multivariate logistic regression analysis, P-value < 0.05 with 95% CI was considered statistically significant.
Results: The magnitude of mortality was 28.8%. Most of the injuries were caused by assault followed by road traffic accident (RTA). About 30% of the subjects presented with severe head injuries and epidural hematoma (EDH) followed by skull fracture were the most common diagnoses on admission. The independent predictors of mortality were male sex (AOR: 6.12, CI: 1.82, 20.5), severe class injury with Glasco coma scale (GCS < 9) (AOR: 5.96, CI: 2.07, 17.12), intraoperative hypoxia episode (AOR: 10.5, CI: 2.6– 42.1), hyperthermia (AOR: 25, CI: 5.54, 115.16), lack of pre-hospital care (AOR: 2.64 CI: 1.6– 4.2), abnormal appearance on both eyes (AOR: 13.4, CI: 5.1– 34.6), in-hospital hypoxia episode and having extra-cranial concomitant injury were positively associated with mortality, while on admission, systolic blood pressure (SBP) of 100– 149 (AOR: 0.086, CI: 0.016– 0.46) was negatively associated with mortality.
Conclusion: The overall mortality rate was considerably high. As a result, traumatic brain injury management should be focused on modifiable factors that increase patient mortality, such as on-admission hypotension, a lack of pre-hospital care, post-operative complications, an intraoperative hypoxia episode, and hyperthermia.
Keywords: head injury, mortality, trauma, injury
Introduction
Traumatic brain injury (TBI) is any change in mental or physical functioning as a result of a blow to the head. It can be mild, moderate and severe traumatic brain injury. Falling down accidents (FDA) and road traffic injuries (RTI) are the leading causes of TBI among all age groups, respectively.1,2 It is a major list of health and socioeconomic problems that has been dubbed a silent epidemic.3 The World Health Organization (WHO) estimates that more than 10 million people worldwide suffer TBI each year resulting in death or severe disability.4 Among all trauma-related injuries, brain injuries are considered the greatest contributor to death and disability globally.5 The incidence of estimated TBI in sub-Saharan Africa is 801 per 100,000.6,7 The TBI is particularly frequent in younger people,4 and Ethiopia has more than 70 million citizens younger than 30 years of age.8 The prevalence of TBI in Ethiopia is reported as 29–40%9–11 and a study done at the University of Gondar Specialized Hospital showed that the prevalence of TBI was reported as 40.5%.11 Differences in patient characteristics, socioeconomic status, ICU admission thresholds, health-care systems, and the availability of varying numbers of ICU beds among hospitals had shown to be the causes for the variation across different continents.12
Studies done in Africa have shown that death rates from head injuries range from 4.2% to 35%.13–16 The prevalence of death as a result of TBI was 12.8% and 16.9%.17,18 Besides, the fatality rate of THI relative to total injured patients had found 22.6% and 30.7%.16,19 The mortality rates of THI in Ethiopia (Addis Ababa, Hawassa, and Bahir Dar) were 10.3%, 12.7%, and 25.3%, respectively.20–22
Absence of pre-hospital care, having extra-cranial damage, lack of neurosurgical intervention, increased age, lower GCS on admission, pupil abnormalities were predictive factors for higher mortality in TBI patients.21,23–31 Dysautonomia manifested by vital sign variability tend to have poorer outcomes.18 Hypotension/hypoxia, patients with SBP higher than 149 mmHg or lower than 90 mmHg, on admission arterial oxygen saturation levels lower than 90%, respiratory rate <8 and above 20 breath per minute were recognized as significant variables associated with adverse outcomes following TBI.18,27,32–34,34 Blood loss of >1000 mL, hospital arrival time delays above 24 hours, providing mechanical ventilation for severe TBI and Hypoglycemia were also found to be the predictors of mortality after TBI.21,35–38
Despite the fact of variable magnitude of mortality, there were no studies on the outcome of TBI at the University of Gondar compressive specialized hospital. The aim of this study was to assess the incidence and predictors of mortality among patients with traumatic brain injury at the University of Gondar Comprehensive Specialized Hospital.
Method
Study Design and Period
A retrospective follow-up study was conducted at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, by reviewing charts of brain injury patients who got care from January 30/2017 to January 30/2022.
Study Area
The study was conducted at the University of Gondar Comprehensive Specialized Hospital, North West Ethiopia. University of Gondar Comprehensive Specialized Hospital is located in the Central Gondar administrative zone, Amhara National Regional state, which is about 750 km northwest of Addis Ababa, the capital city of Ethiopia. It serves more than five million people in the Central Gondar zone and the people of the neighboring zones. It has more than 500 beds and delivers both basic and cutting-edge services at its various units. Trauma sufferers are initially assessed and given resuscitation in the emergency room. In one major theater complex and two minor surgery facilities, the hospital offers general surgical services. In terms of emergency response, the hospital offers trauma care for 24 hours.
Source Population
All adult traumatic brain injury patients who got surgical, intensive and/or supportive care at the University of Gondar Comprehensive Specialized Hospital.
Study Population
All adult traumatic brain injury patients who got surgical, intensive and/or supportive care at the University of Gondar Comprehensive Specialized Hospital from January 30/2017 to January 30/2022.
Inclusion and Exclusion Criteria
Inclusion Criteria
All adult traumatic brain injury patients who got surgical, intensive and/or supportive care at the University of Gondar Comprehensive Specialized Hospital during the study period were included.
Exclusion Criteria
Patients who had pre-existing comorbidity (DM, HTN, asthma, and epilepsy), refused care, and referred to other care center were excluded.
Variables
Independent Variable
Socio-demographic data (age, sex, residence)
Cause of injury (assaults, road traffic injury, fall, pedestrian)
Pre-hospital characteristics (pre-hospital management, time from injury to arrival, concomitant injury)
Clinical characteristics at admission to hospital (GCS, heart rate, respiratory rate, systolic blood pressure, oxygen saturation, pupillary response, number of eye abnormality)
Clinical characteristic during hospital treatment (surgical, post-surgical complications, ICU treatment, mechanical ventilation, systemic hypotension, systemic hypoxia, electrolyte disturbance, hyperthermia)
Dependent Variables
Mortality from traumatic brain injury
Operational Definition
Hypoxia episode: two or more record of pulse oximeter oxygen saturation value <90%.21
Hypotension episode: systolic blood pressure value <90 mmHg measured at any time point during hospitalization, including the hospital arrival value.18
Hyperthermia: body temperature ≥38°C during hospitalization.39
Pre-hospital management: any documented intervention from the referral paper and/or documented history by the primary clinician.40
Post-operative complication: Adverse events such as pneumonia, meningitis, wound infection, postoperative wound dehiscence, reoperation occur as a consequence of tissue injury due to surgery or anesthesia, following Surgery and Anesthesia.41
Unfavorable outcome: is the mortality/death following TBI.
Sample Size and Sampling Procedure
Sample Size Determination
The actual sample size for the study was determined by using single population proportion formula, by taking the magnitude of mortality from a study from Addis Ababa, Ethiopia, case-specific mortality for severe associated ASDH reported 54.1%.35
Formula for single population proportion, 
Where n = Initial estimated sample size
Z = Confidence level (alpha, α); α=95%; 
 = proportion;
= proportion;  , from previous study
, from previous study



By adding 10% (39 patient charts) non-response rate; the final sample size was 421.
Sampling Procedures
The participant’s data files having the diagnosis of TBI on the emergency and/or operation room registration books have been listed by their registration ID number. Then after obtaining the list, the medical record numbers of the patients were entered into Microsoft Excel 2010 and the sampling frame was prepared based on random numbers. Study participants were selected using a computer-generated simple random sampling method from the sampling frame of 4803 patients’ chart by medical record numbers to obtain a sample of 464 (43 for pretest and 421 for main study) (Figure 1).
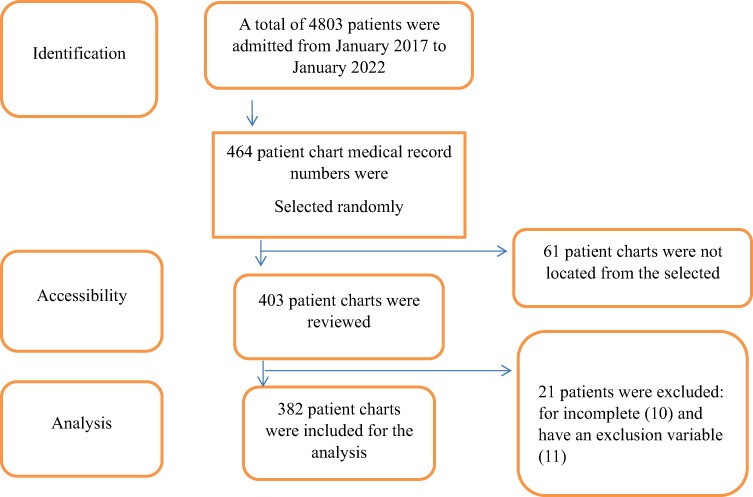 |
Figure 1 Diagram illustrating data collection procedure among traumatic brain injury patients admitted to University of Gondar Comprehensive Specialized Hospital from January 2017 to January 2022. |
Data Collection Procedure and Data Quality Control
Data Collection Procedure
A semi-structured questionnaire was prepared by the principal investigator for all patients who fulfill the inclusion criteria. The data was extracted from the patient’s record (log book), patient history chart, anesthesia record sheet and operation notes using a data extraction tool for the occurrence of the event.
The question list contained demographic characteristics of patients, injury characteristics, clinical findings, vital signs on admission, length of hospital stay, surgical intervention, amount of blood loss and transfusion, perioperative vital sign conditions, and body temperature value (Annex I).
Data Quality Control
A pre-test of the data collection tool has been done on 10% (43 patient charts) of participants and pre-tested respondents who have complete and/or accepted range study variables were also included in the main study. After the pre-test, the questionnaire was modified by excluding those variables that were not feasible to access.
The collected data has been checked for completeness, accuracy, and clarity by the principal investigator. Training was given to a data collector for half a day on how to use the data collection tools and how to collect data from a patient’s record. Finally, prior to analysis, data were cleaned up and cross-checked.
Data Processing and Analysis Procedures
After completion of data collection, the data was coded, entered, and cleaned for errors using Epi-data software (version 4.6). Then, the data was exported into SPSS (version 26) for analysis. The normality of data was tested by using the Shapiro–Wilk normality test. Non-normally distributed data were presented as median ± IQR, and categorical data as count and percentage. Before computing logistic regression, a cross-tabulation was performed to identify whether the variables fulfilled the assumption for bivariate logistic regression. In the bivariate regression, predictor variables with a p-value of <0.2 were fitted for multivariate logistic regression. The model fitness was checked by using Hosmer and Lemeshow’s goodness-of-fit test. In multivariate logistic regression, p-value < 0.05 at 95% CI has been considered as statistically significant.
Result
Socio-Demographic Characteristics
Out of 421 patient charts, a total of 382 having complete data were included in this study, with a response rate of 90.7%. Most of the study participants were males, with a male-to-female ratio of 6.6:1. The most affected age group (79%) was those ranging from 19 to 40 years old, and admission from rural residences accounted for 81.2% of study participants (Table 1).
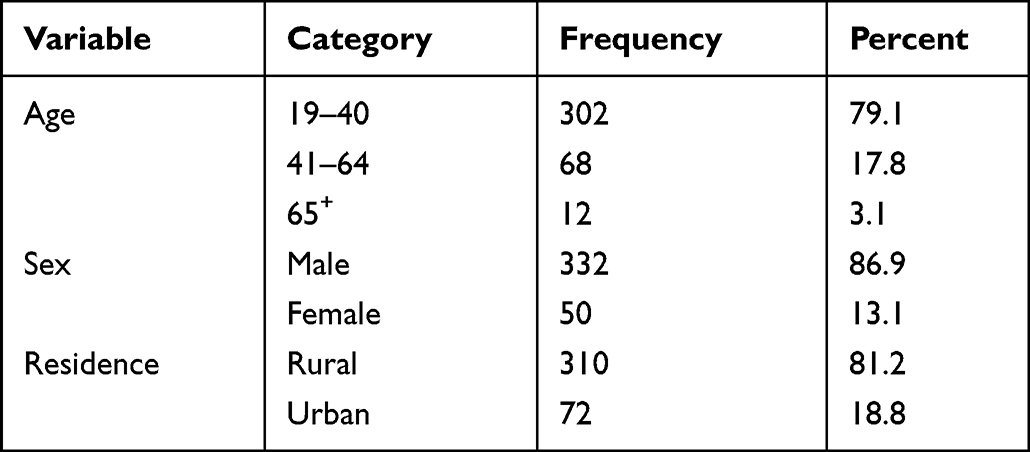 |
Table 1 Socio-Demographic Characteristics of Traumatic Brain Injury Patients Admitted to University of Gondar Comprehensive Specialized Hospital from January 2017 to January 2022, Gondar, Northwest Ethiopia |
Pattern of Admission of TBI Patients
The most common cause of TBI on admission was assault, with 222 (58.1%) cases. The other causes were RTA, FDI and pedestrian, respectively (Table 2).
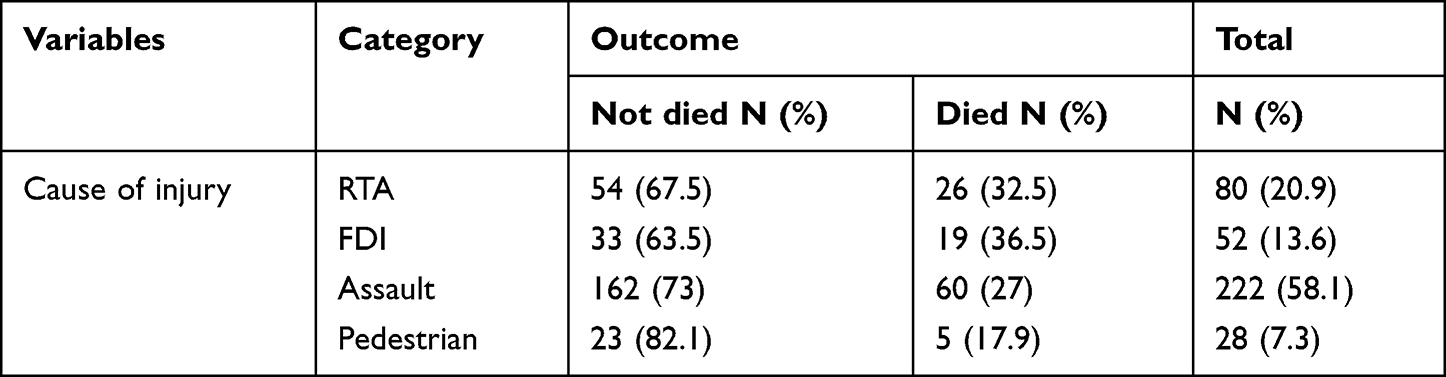 |
Table 2 Cause of Injury with Mortality from Traumatic Brain Injury at UOGCSH from 2017 to 2022 |
Computed tomography scans were obtained for 231 (60.5%) patients. The most common diagnosis seen was epidural hematoma 77 (33.3%), followed by skull fractures 71 (18.6%). Concerning TBI severity, about 30% of the subjects presented with severe TBI (Table 3).
 |
Table 3 The Severity of TBI and Its Diagnosis by Computed Tomography Scans Among Patients Admitted to UOGCSH from January 2017 to January 2022, Gondar, Northwest Ethiopia |
About half 190 (49.7%) of patients had received pre-hospital management. Time from injury to arrival has been ≤24 hour in 229 (59.94%) of the patient. The majority of the study subjects 161 (42.15%) presented with blunt brain injury cases were presented with associated extra-cranial injuries (Table 4).
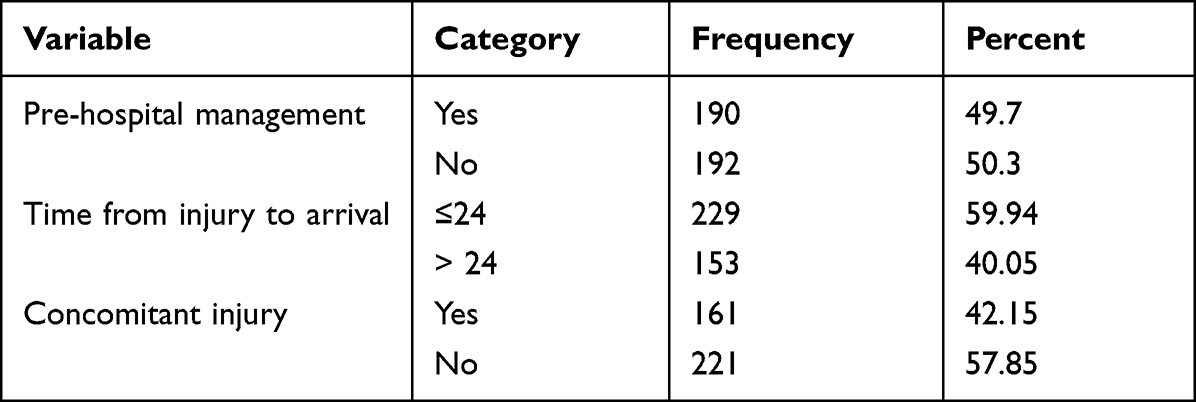 |
Table 4 On Admission Injury Characteristics of Traumatic Brain Injury Patients Admitted to UOGCSH from January 2017 to January 2022, Gondar, Northwest Ethiopia |
About 96 (25.1%) of individuals exposed to hypoxia (SPO2 <90%) (Table 5). About 122 (31.9%) of patients were admitted to ICU and 85 (22.3%) of them had received mechanical ventilation. Around 135 (35.3%) patients were having electrolyte disturbance (Table 6).
 |
Table 5 On Admission Baseline Clinical Characteristics of Traumatic Brain Injury Patients Admitted to UOGCSH from January 2017 to January 2022, Gondar, Northwest Ethiopia |
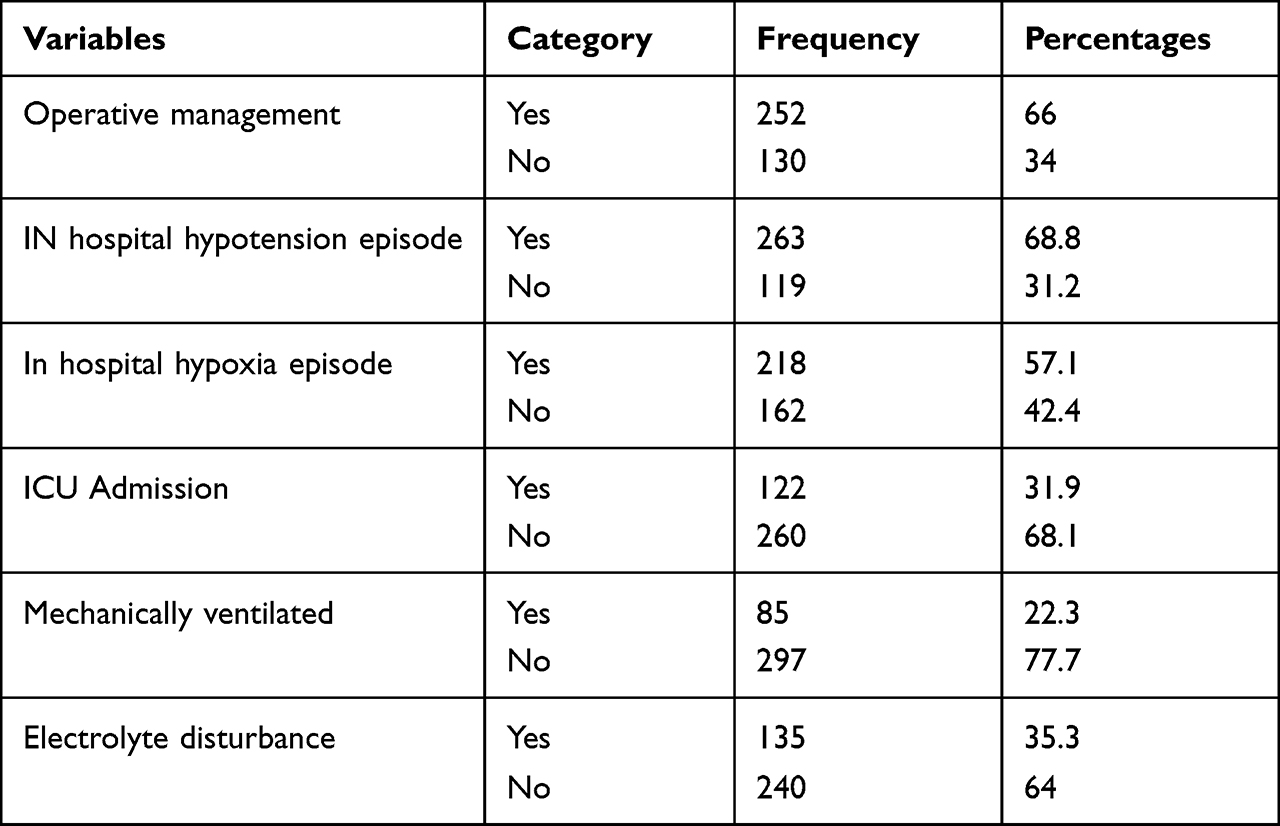 |
Table 6 In Hospital Clinical Management Related Characteristics and Mortality of Traumatic Brain Injury Patients Admitted to UOGCSH from January 2017 to January 2022, Gondar, Northwest Ethiopia |
Magnitude of Mortality from TBI
The incidence of mortality from traumatic brain injury was 28.8% (CI = 27.3–29.7). About 272 (71.2%) of patients were discharged from the hospital with median ± IQR of 5 ± 2–12.
Factors Affecting Patient’s Mortality
Bivariate logistic regression analysis showed that sex, having concomitant extra-cranial injury, lack of pre-hospital management, patients’ condition at presentation (SBP, HR, SpO2, abnormal pupillary reaction), GCS at presentation, having operative management, post-operative complication, hypotension episode during hospitalization, intraoperative hypoxia episode, blood loss above 1000 mL, in-hospital hypoxia episode, in-hospital hypotension episode, and hyperthermia during hospital stay were found to be statistically significant at 95% CI.
When these variables were tested at multivariate logistic regression, being male, having concomitant extra-cranial injury, lack of pre-hospital management, patients’ condition at presentation SBP, low GCS level, number of abnormal pupils, intraoperative hypoxia episode, having post-operative complication, and hyperthermia during hospital stay were found to be statistically significant with p-value < 0.05 at 95% CI.
The odds of mortality had 6.12 times higher in males than females (AOR: 6.12, 95% CI: 1.82–20.5). The odds of death in concomitant injured patients had around two times as compared to those without concomitant injury (AOR: 2.08, 95% CI: 1.28–3.38).
The odds of death for patients who lack pre-hospital management were 2.64 times higher as compared to those who had been managed in the pre-hospital setting (AOR: 2.64; 95% CI: 1.6–4.3).
The odds of death had 5.9 times (AOR: 5.9;95% CI: 2.07–17.12) higher in low GCS3–8 than higher GCS level.13–15 The odds of mortality for a patient with SBP of 100–149 mm Hg had 91.4% (AOR: 0.086, 95% CI: 0.016–0.46) lower compared with patients having SBP of <100 and >149 mmHg.
Patients with pupillary abnormalities in both eyes had 13.34 (AOR: 13.34,95% CI: 5.1–34.6) times the odds of mortality as compared with those with no documented pupil abnormality. The odds of death among patients with hypoxic episodes intra-operatively were 10.5 times higher as compared to no hypoxia episodes (AOR: 10.5; 95% CI: 2.6–42.1). The odds of death had 25.2 (AOR: 25.2,95% CI: 5.54–115.16) time higher in patients with hyperthermia than normothermia. The odds of mortality had 4.98 (AOR: 4.89,95% CI: 1.1–25) times higher in patients with postoperative complication than without postoperative complications (Table 7).
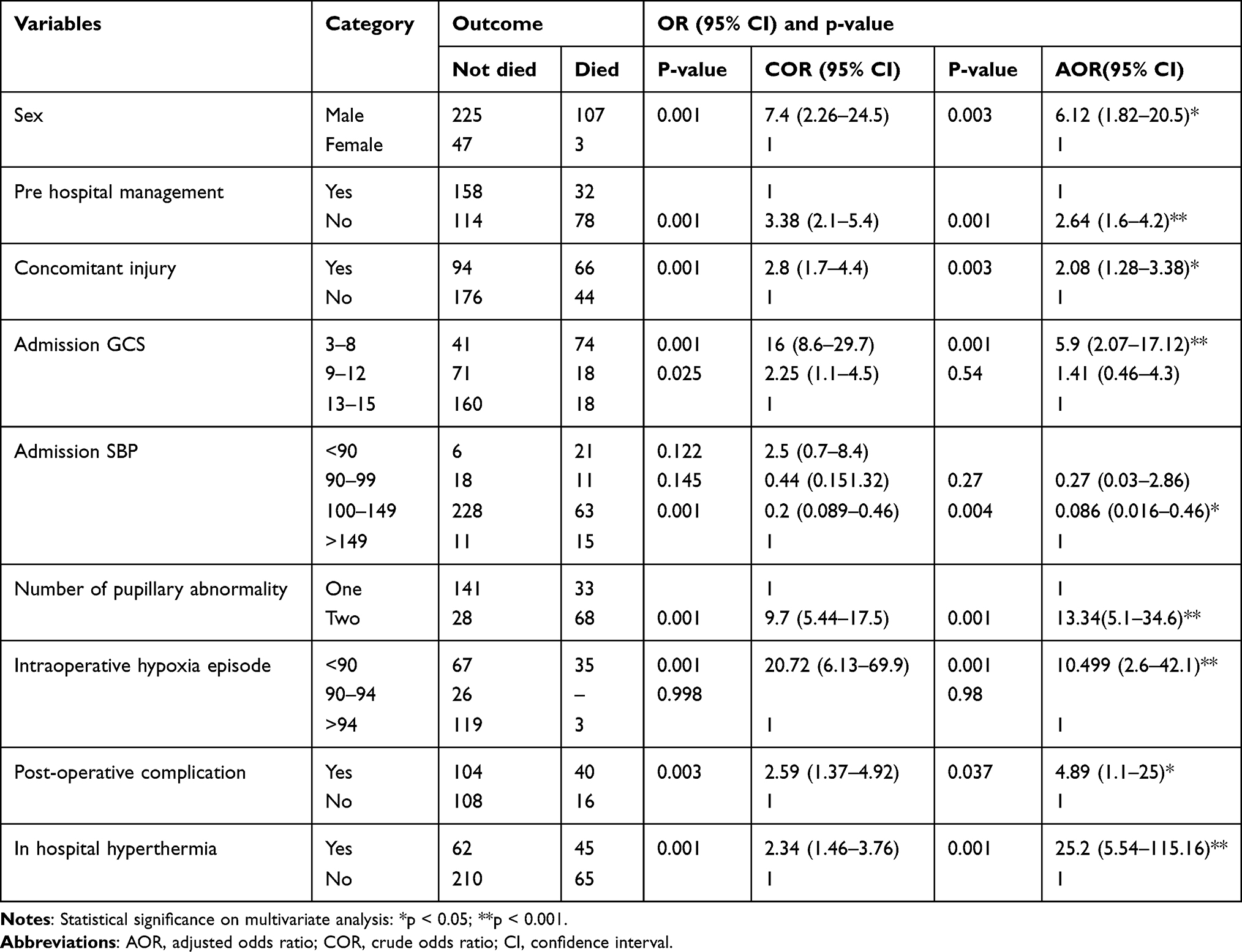 |
Table 7 Bivariate and Multivariate Logistic Regression Showing the Factors Associated with Mortality Among Patients Admitted to UOGCSH from January 2017 to January 2022 |
Discussion
The aim of the current study was to assess the incidence and predictors of mortality among patients with traumatic brain injury at the University of Gondar Comprehensive Specialized Hospital. Determining the clinical outcomes following TBI and identifying the predictors can help as the evidence to allocate the resource and to build trauma system infrastructure. Mobilizing resources and infrastructures had improved the patient’s outcome following TBI.42,43
The overall mortality rate following TBI in this study was 28.8%, which is higher than the overall mortality of 9⋅6% reported in Kampala44 and studies in Addis Ababa, Hawassa, and Bahir Dar, Ethiopia.20–22 In contrast, it is lower than a study done in Tanzania and France which reported as 30.7% and 49% mortality, respectively,16,45 and studies done in Africa as reported that death rates from head injury range from 30% to 35%.13–16 The possible reason for the difference, those as in Mulago, only included patients who were referred to the neurosurgery department, but the current study included all patients who were admitted to the hospital with TBI. Additionally, this might be explained by a lack of cerebral injury diagnostic tools, limited transportation, minimal ICU access, and a significant distance to the closest neurosurgical center, which may all contribute to the study’s apparent variation in mortality. Low mortality rate compared with above studies could be also due to variation in leading causes of TBI. In this study, the most common cause of TBI on admission was assault followed by RTA, FDI and pedestrian, respectively. A study had found that TBI caused by assault was associated with better outcomes than the rest.46–48
Our study demonstrated that there was a statistically significant association between death and male sex, lack of pre-hospital management, extra-cranial concomitant injury, lower admission SBP, lower GCS, pupillary abnormality on presentation, intraoperative hypoxia episode, hyperthermia, and postoperative complications in patients with TBI.
Our finding demonstrated that being male sex is highly associated with in hospital mortality. In contrary to this, studies stated that females had poorer prognosis compared to males.49,50 Other studies have stated that there is no proven relationship between sexual orientation.25,26,28,30 A possible explanation for this discrepancy in our study is that, the number of participants in male gender was much higher than females.
Studies demonstrated that there is no significant association between the pre-hospital care provided and the risk of mortality.51 In contrast, another retrospective study demonstrated less mortality had found when pre-hospital care was offered.52 This study is in line with our finding which stated that patient groups without pre-hospital management resulted in higher mortality.
We identified that having extra-cranial concomitant injury was associated with increased mortality in THI as compared to those without concomitant injury. Consistent with this, having extra-cranial concomitant damage is thought to be a predictive factor for higher mortality in TBI, according to a collaborative investigation of a large number of TBI patients.24 Extra-cranial concurrent damage was found to not only considerably increase mortality but also serve as a standalone predictor of mortality in TBI patients.53 However, a study had demonstrated that having an associated extra-cranial concomitant injury was not associated with an increase in mortality of TBI patients.54 The disparate results would be explained by in our study the extra-cranial injured groups have more severe head injury intensity when compared to those without concurrent injury.
Our study demonstrated that there was a statistically significant association between death and patient clinical conditions like hypotension, hypoxia. Other investigators likewise yielded comparable outcomes as hypotension and hypoxia following TBI was recognized as significant secondary insults associated with adverse outcomes.27,32,33
Studies done on the effect of vital signs on mortality of TBI stated that patients with SBP higher than 149 mmHg or lower than 90 mmHg had poor outcomes.18,34 On admission, arterial oxygen saturation lower than 90% and an intraoperative arterial oxygen hypoxia episode was associated with death.55 Our clinical prediction in this study demonstrates the same result as studies done before on the basis of those variables, though no contradiction ideas in this regard were found to the extent of the investigators’ knowledge. Therefore, patients’ chances of survival are considerably increased by prompt diagnosis and intensive resuscitation during the patient’s first golden hour of arrival.18,34
According to the findings, there is strong evidence for the prognostic value of the GCS on admission and mortality from TBI.18,25,27–29 Studies showed that lower GCS on admission was associated with more unfavorable outcomes.25,28–30 As far as we have found in the literature, all authors agree with a reverse association between GCS and mortality from TBI.56 Our clinical prediction in this study demonstrates the same result as studies done before on the basis of GCS level on admission.
Our study demonstrated that there was a statistically significant association between death and the number of nonappearance or irregular pupillary responses and mortality in TBI. In line with this, there were conditions between nonappearance or irregular pupillary responses and associated with devastating outcomes following TBI.25,27,29 The possible explanation for this was explained as pupil abnormalities were noted more frequently in patients with severe class injuries such as compressed cisterns, and brain structure shift.31
Studies demonstrated that patients who were exposed to hyperthermia in the perioperative period had a higher risk of mortality compared to normothermic.21,39 In line with this, our study showed that the odds of death among patients who were exposed to hyperthermia were higher as compared with normothermic patients. This finding is in agreement with another study.57 This could be since hyperthermia increases brain metabolic demand, ICP, and cell damage.39 Furthermore, hyperthermia may increase the stress level of the patient, resulting in increased cardiac output and blood pressure, which may increase cerebral blood flow, especially under conditions of impaired pressure autoregulation.58
In our study, we found that the risk of death among patients with intraoperative hypoxia episode was higher as compared with patients without hypoxia episode. This finding was consistent with the previous studies done in Tikur Anbessa Specialized Hospital and University Teaching Hospital of Kigali.20,59
In this study, having postoperative complications along with head injury was associated with mortality. This is in line with studies from other LMICs, which have shown comparable extents of mild and moderate TBI with unfavorable results indeed, with post-operative courses of complications.43 Furthermore, having postoperative complications was highly associated with mortality, as reported by a study done in Addis Ababa, Ethiopia.2 This is more explained by more physiological disturbance and brain nutrient requirement, which may result in bad outcome in case of traumatic head injury with postoperative complication.43
Strength and Limitations of the Study
This study is the first of its type in the study area, with the largest center in Northwest Ethiopia and with the probability of being generalized.
While being the largest center, it was vulnerable to the problems seen in observational study designs with a retrospective data. Some of the prognostic variables were not accessible for analysis in this investigation since the data was not initially documented for the purposes of this study. We did not have data about patients who died before admission, those referred to other centers, and those discharged with morbidity. Besides, we merely used GCS for diagnosing severity of TBI.
Conclusion
There was a high mortality of TBI patients as compared with studies done in the country. Severe brain injury having low admission GCS score, lack of pre-hospital care, having post-operative complication, male sex, having concomitant extra-cranial trauma, systemic factors like admission systolic blood pressure above/below 100–149mmhg, having two pupillary abnormality, intraoperative hypoxia episode and in hospital hyperthermia remain statistically significant association with higher TBI-related mortality.
Recommendation
Strengthening the pre-hospital services system will greatly impact patient outcomes of traumatic brain injured patients. In-hospital, prompt care should be instituted for already established cases, particularly those at risk of unfavorable outcome (death) in cases with low level of consciousness (GCS < 9), extra-cranial concomitant injuries, post-operative complications, and vital sign instability. Furthermore, prioritizing those measured vital parameter instabilities (such as SBP, SpO2, and body temperature) during immediate and ongoing hospital management may aid in prognosis and improve patient outcome.
For future researchers, prospective study designs to incorporate all possible prognostic variables with possible pre-hospital and referred patient outcome studies are recommended.
Abbreviations
ASDH, Acute Subdural Hematoma; BGL, Blood Glucose Level; CT, Computerized Tomography; EDH, Epidural Hematoma; FDI, Fall down injury; GCS, Glasgow Coma Scale/Score; ICU, Intensive Care Unit; LMIC, Low and Middle Income Country; MV, Mechanical Ventilator; PR, Pulse Rate; RR, Respiratory Rate; RTA, Road Traffic Accident; SBP, Systolic Blood Pressure; SDH, Subdural Hematoma; SpO2, Oxygen Saturation; TBI, Traumatic Brain Injury; THI, Traumatic Head Injury; UOGCSH, University of Gondar Comprehensive Specialized Hospital; WHO, World Health Organization.
Data Sharing Statement
Data for this study are available on request.
Ethical Approval
Ethical approval for this study has been received from the institutional review board of School of medicine, College of medicine and health science, University of Gondar with reference number of 1267/2022. The ethics committee approved this study to not need consent from the study participants because of the retrospective nature of data and a support letter has been obtained from the medical director office of the hospital for retrieving retrospective data from the database and records. All the information was kept confidential, and no individual identifiers were collected. We have confirmed that our study complies with the Declaration of Helsinki.
Acknowledgment
The authors thank both Debre Tabor University and University of Gondar for funding and providing necessary resources.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed to be accountable on the journal to which the article has been submitted.
Funding
Debre Tabor University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheng P, Yin P, Ning P, et al. Trends in traumatic brain injury mortality in China, 2006–2013: a population-based longitudinal study. PLoS Med. 2017;14(7):e1002332. doi:10.1371/journal.pmed.1002332
2. Hagos A, Tedla F, Tadele A, Zewdie A. Pattern and outcome of traumatic brain injury, addis ababa, Ethiopia: a cross-sectional hospital-based study. Ethiop J Health Sci. 2022;32:2.
3. Koskinen S, Alaranta H. Traumatic brain injury in Finland 1991–2005: a nationwide register study of hospitalized and fatal TBI. Brain Injury. 2008;22(3):205–214. doi:10.1080/02699050801938975
4. Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341–353. doi:10.3233/NRE-2007-22502
5. Shammassian BH, Wooster L, Wright JM, Kelly ML. Systematic review of trauma system regionalization and implementation on outcomes in traumatic brain injury patients. Neurol Res. 2021;43(2):87–96. doi:10.1080/01616412.2020.1824391
6. Laeke T, Tirsit A, Debebe F, et al. Profile of head injuries: prehospital care, diagnosis, and severity in an Ethiopian tertiary hospital. World Neurosurg. 2019;127:e186–e92. doi:10.1016/j.wneu.2019.03.044
7. Elahi C, Rocha TAH, da Silva NC, et al. An evaluation of outcomes in patients with traumatic brain injury at a referral hospital in Tanzania: evidence from a survival analysis. Neurosurg Focus. 2019;47(5):E6. doi:10.3171/2019.7.FOCUS19316
8. Violence WHODo, Prevention I, Violence WHO, Prevention I, World Health Organization. Global Status Report on Road Safety: Time for Action. World Health Organization; 2009.
9. Eshete A, Taye F. Magnitude of severe head injury and its associated factors among head injury patients in gedeo zone, southern Ethiopia: a two-year retrospective study. Ethiop J Health Sci. 2018;28(3):323–330. doi:10.4314/ejhs.v28i3.10
10. Suga Y, Shimelis W, Yesuf A, Dendena F, Teklewold B. Assessment of magnitude and factors affecting outcomes of head injury at Addis Ababa burn emergency and trauma hospital, Ethiopia. Int J. 2021;7(1):28.
11. Walle TA, Tiruneh BT, Bashah DT. Prevalence of head injury and associated factors among trauma patients visiting surgical emergency department of Gondar University Referral Hospital, Northwest Ethiopia 2016. Int J Africa Nurs Sci. 2018;9:57–61. doi:10.1016/j.ijans.2018.08.002
12. Demyttenaere SV, Nansamba C, Nganwa A, Mutto M, Lett R, Razek T. Injury in Kampala, Uganda: 6 years later. Can J Surg. 2009;52(5):E146.
13. Tran TM, Fuller AT, Kiryabwire J, et al. Distribution and characteristics of severe traumatic brain injury at Mulago national referral hospital in Uganda. World Neurosurg. 2015;83(3):269–277. doi:10.1016/j.wneu.2014.12.028
14. Smart LR, Mangat HS, Issarow B, et al. Severe traumatic brain injury at a tertiary referral Center in Tanzania: epidemiology and adherence to brain Trauma Foundation guidelines. World Neurosurg. 2017;105:238–248. doi:10.1016/j.wneu.2017.05.101
15. Jerome E, Laing GL, Bruce JL, Sartorius B, Brysiewicz P, Clarke DL. An audit of traumatic brain injury (TBI) in a busy developing-world trauma service exposes a significant deficit in resources available to manage severe TBI. S Afr Med J. 2017;107(7):621–625. doi:10.7196/SAMJ.2017.v107i7.10562
16. Boniface R, Lugazia ER, Ntungi AM, Kiloloma O. Management and outcome of traumatic brain injury patients at Muhimbili Orthopaedic Institute Dar es Salaam, Tanzania. Pan Afr Med J. 2017;2017:26.
17. Abdelgadir J, Smith ER, Punchak M, et al. Epidemiology and characteristics of neurosurgical conditions at Mbarara Regional Referral Hospital. World Neurosurg. 2017;102:526–532. doi:10.1016/j.wneu.2017.03.019
18. Saadat S, Akbari H, Khorramirouz R, Mofid R, Rahimi-Movaghar V. Determinants of mortality in patients with traumatic brain injury. Ulus Travma Acil Cerrahi Derg. 2012;18(3):219–224. doi:10.5505/tjtes.2012.03453
19. Onwuchekwa RC, Echem RC. An epidemiologic study of traumatic head injuries in the emergency department of a tertiary health institution. J Med Trop. 2018;20(1):24. doi:10.4103/jomt.jomt_28_17
20. Landes M, Venugopal R, Berman S, Heffernan S, Maskalyk J, Azazh A. Epidemiology, clinical characteristics and outcomes of head injured patients in an Ethiopian emergency centre. Afr J Emerg Med. 2017;7(3):130–134. doi:10.1016/j.afjem.2017.04.001
21. Assele DD, Lendado TA, Awato MA, Workie SB, Faltamo WF. Incidence and predictors of mortality among patients with head injury admitted to Hawassa University Comprehensive Specialized Hospital, Southern Ethiopia: a retrospective follow-up study. PLoS One. 2021;16(8):e0254245. doi:10.1371/journal.pone.0254245
22. Amare AT, Tesfaye TD, Ali AS, et al. Survival status and predictors of mortality among traumatic brain injury patients in an Ethiopian hospital: a retrospective cohort study. Afr J Emerg Med. 2021;11(4):396–403. doi:10.1016/j.afjem.2021.06.003
23. Owattanapanich N, Chittawatanarat K, Benyakorn T, Sirikun JJ. Risks and benefits of hypotensive resuscitation in patients with traumatic hemorrhagic shock: a meta-analysis. Scand J Trauma Resusc Emerg Med. 2018;26(1):1–10. doi:10.1186/s13049-018-0572-4
24. van Leeuwen N, Lingsma HF, Perel P, et al. Prognostic value of major extracranial injury in traumatic brain injury: an individual patient data meta-analysis in 39,274 patients. Neurosurgery. 2012;70(4):811–818. doi:10.1227/NEU.0b013e318235d640
25. Murray GD, Butcher I, McHugh GS, et al. Multivariable prognostic analysis in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):329–337. doi:10.1089/neu.2006.0035
26. Mushkudiani NA, Engel DC, Steyerberg EW, et al. Prognostic value of demographic characteristics in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):259–269. doi:10.1089/neu.2006.0028
27. Hebb MO, McArthur DL, Alger J, et al. Impaired percent alpha variability on continuous electroencephalography is associated with thalamic injury and predicts poor long-term outcome after human traumatic brain injury. J Neurotrauma. 2007;24(4):579–590. doi:10.1089/neu.2006.0146
28. Husson EC, Ribbers GM, Willemse-van Son AH, Verhagen AP, Stam HJ. Prognosis of six-month functioning after moderate to severe traumatic brain injury: a systematic review of prospective cohort studies. J Rehabil Med. 2010;42(5):425–436. doi:10.2340/16501977-0566
29. Marmarou A, Lu J, Butcher I, et al. Prognostic value of the Glasgow Coma Scale and pupil reactivity in traumatic brain injury assessed pre-hospital and on enrollment: an IMPACT analysis. J Neurotrauma. 2007;24(2):270–280. doi:10.1089/neu.2006.0029
30. Fabbri A, Servadei F, Marchesini G, Stein S, Vandelli A. Early predictors of unfavourable outcome in subjects with moderate head injury in the emergency department. J Neurol Neurosurg Psychiatry. 2008;79(5):567–573. doi:10.1136/jnnp.2007.120162
31. Maas AI, Steyerberg EW, Butcher I, et al. Prognostic value of computerized tomography scan characteristics in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):303–314. doi:10.1089/neu.2006.0033
32. McHugh GS, Engel DC, Butcher I, et al. Prognostic value of secondary insults in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):287–293. doi:10.1089/neu.2006.0031
33. Imen RB, Olfa C, Kamilia C, et al. Factors predicting early outcome in patients admitted at emergency department with severe head trauma. J Acute Dis. 2015;4(1):68–72. doi:10.1016/S2221-6189(14)60087-1
34. Butcher I, Maas AI, Lu J, et al. Prognostic value of admission blood pressure in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):294–302. doi:10.1089/neu.2006.0032
35. Laeke T, Tirsit A, Kassahun A, et al. Prospective Study of Surgery for Traumatic Brain Injury in Addis Ababa, Ethiopia: surgical procedures, complications, and postoperative outcomes. World Neurosurg. 2021;150:e316–e23. doi:10.1016/j.wneu.2021.03.004
36. Vaca SD, Kuo BJ, Nickenig Vissoci JR, et al. Temporal delays along the neurosurgical care continuum for traumatic brain injury patients at a tertiary care hospital in Kampala, Uganda. Neurosurgery. 2019;84(1):95–103.
37. Krishnamoorthy V, Vavilala MS, Mills B, Rowhani-Rahbar A. Demographic and clinical risk factors associated with hospital mortality after isolated severe traumatic brain injury: a cohort study. J Intensive Care. 2015;3(1):46. doi:10.1186/s40560-015-0113-4
38. Liu-DeRyke X, Collingridge DS, Orme J, Roller D, Zurasky J, Rhoney DH. clinical impact of early hyperglycemia during acute phase of traumatic brain injury. Neurocrit Care. 2009;11(2):151. doi:10.1007/s12028-009-9228-6
39. Nyholm L, Howells T, Lewén A, Hillered L, Enblad P. The influence of hyperthermia on intracranial pressure, cerebral oximetry and cerebral metabolism in traumatic brain injury. Ups J Med Sci. 2017;122(3):177–184. doi:10.1080/03009734.2017.1319440
40. Pélieu I, Kull C, Walder B. Prehospital and emergency care in adult patients with acute traumatic brain injury. Med Sci. 2019;7(1):12. doi:10.3390/medsci7010012
41. Bayissa BB, Mummud M, Miressa F, Fekadu GJOAS. Postoperative complications and associated factors among surgical patients treated at a tertiary hospital, Eastern Ethiopia: a prospective cohort study. Open Access Surg. 2021;14:37. doi:10.2147/OAS.S320506
42. Perel P, Edwards P, Wentz R, Roberts I. Systematic review of prognostic models in traumatic brain injury. BMC Med Inform Decis Mak. 2006;6(1):38. doi:10.1186/1472-6947-6-38
43. De Silva MJ, Roberts I, Perel P, et al. Patient outcome after traumatic brain injury in high-, middle-and low-income countries: analysis of data on 8927 patients in 46 countries. Int J Epidemiol. 2009;38(2):452–458. doi:10.1093/ije/dyn189
44. Kuo BJ, Vaca SD, Vissoci JRN. A prospective neurosurgical registry evaluating the clinical care of traumatic brain injury patients presenting to Mulago National Referral Hospital in Uganda. PLoS One. 2017;12(10):e0182285. doi:10.1371/journal.pone.0182285
45. Baucher G, Troude L, Pauly V, Bernard F, Zieleskiewicz L, Roche P. Predictive factors of poor prognosis after surgical management of traumatic acute subdural hematomas: a single-center series. World Neurosurg. 2019;126:e944–e52. doi:10.1016/j.wneu.2019.02.194
46. Butcher I, McHugh GS, Lu J. Prognostic value of cause of injury in traumatic brain injury: results from the IMPACT Study. J Neurotrauma. 2007;24(2):281–286. doi:10.1089/neu.2006.0030
47. Zia N, Mehmood A, Namaganda RH, Ssenyonjo H, Kobusingye O, Hyder AA. Causes and outcomes of traumatic brain injuries in Uganda: analysis from a pilot hospital registry. Trauma Surg Acute Care Open. 2019;4(1):e000259. doi:10.1136/tsaco-2018-000259
48. Younis R, Younis M, Hamidi S, Musmar M, Mawson AR. Causes of traumatic brain injury in patients admitted to Rafidia, Al-Ittihad and the specialized Arab hospitals, Palestine, 2006–2007. Brain Injury. 2011;25(3):282–291. doi:10.3109/02699052.2010.546823
49. Moppett I. Traumatic brain injury: assessment, resuscitation and early management. Br J Anaesth. 2007;99(1):18–31. doi:10.1093/bja/aem128
50. Ponsford JL, Myles PS, Cooper DJ, et al. Gender differences in outcome in patients with hypotension and severe traumatic brain injury. Injury. 2008;39(1):67–76. doi:10.1016/j.injury.2007.08.028
51. Lee A, Garner A, Fearnside M, Harrison K. Level of prehospital care and risk of mortality in patients with and without severe blunt head injury. Injury. 2003;34(11):815–819. doi:10.1016/S0020-1383(02)00395-9
52. Garner A, Crooks J, Lee A, Bishop R. Efficacy of prehospital critical care teams for severe blunt head injury in the Australian setting. Injury. 2001;32(6):455–460. doi:10.1016/S0020-1383(01)00013-4
53. Shibahashi K, Sugiyama K, Okura Y, Hoda H, Hamabe Y. Serious concomitant injuries in pediatric patients with severe traumatic brain Injury. World Neurosurg. 2018;110:e1078–e84. doi:10.1016/j.wneu.2017.12.002
54. Stewart TC, Alharfi IM, Fraser DD. The role of serious concomitant injuries in the treatment and outcome of pediatric severe traumatic brain injury. J Trauma Acute Care Surg. 2013;75(5):836–842. doi:10.1097/TA.0b013e3182a685b0
55. Hukkelhoven CW, Steyerberg EW, Farace E, Habbema JDF, Marshall LF, Maas AI. Regional differences in patient characteristics, case management, and outcomes in traumatic brain injury: experience from the tirilazad trials. J Neurosurg. 2002;97(3):549–557. doi:10.3171/jns.2002.97.3.0549
56. Foreman BP, Caesar RR, Parks J, et al. Usefulness of the abbreviated injury score and the injury severity score in comparison to the Glasgow Coma Scale in predicting outcome after traumatic brain injury. J Trauma. 2007;62(4):946–950. doi:10.1097/01.ta.0000229796.14717.3a
57. Li J, Jiang JY. Chinese Head Trauma Data Bank: effect of hyperthermia on the outcome of acute head trauma patients. J Neurotrauma. 2012;29(1):96–100. doi:10.1089/neu.2011.1753
58. Elf K, Nilsson P, Ronne-Engström E, Howells T, Enblad PJ. Temperature disturbances in traumatic brain injury: relationship to secondary insults, barbiturate treatment and outcome. Neurol Res. 2008;30(10):1097–1105. doi:10.1179/174313208X319125
59. Krebs E, Gerardo CJ, Park LP, et al. Mortality-associated characteristics of patients with traumatic brain injury at the University Teaching Hospital of Kigali, Rwanda. World Neurosurg. 2017;102(571–82):571–582. doi:10.1016/j.wneu.2017.03.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Protective Role of Obesity on Trauma Impact: A Retrospective Analysis of Patients with Surgical Blunt Bowel Mesenteric Injury Due to Road Traffic Accidents
Hsieh TM, Chuang PC, Liu CT, Wu BY, Liu YW, Hsieh CH
Risk Management and Healthcare Policy 2022, 15:1533-1543
Published Date: 18 August 2022
Fat Embolism Syndrome and in-Hospital Mortality Rates According to Patient Age: A Large Nationwide Retrospective Study
Tsai SHL, Chen CH, Tischler EH, Kurian SJ, Lin TY, Su CY, Osgood GM, Mehmood A, Fu TS
Clinical Epidemiology 2022, 14:985-996
Published Date: 19 August 2022
The Association of Albumin-Bilirubin (ALBI) Grade with Mortality Risk in Trauma Patients with Liver Injuries
Chou SE, Rau CS, Su WT, Tsai CH, Hsu SY, Hsieh CH
Risk Management and Healthcare Policy 2023, 16:279-286
Published Date: 24 February 2023
A High De Ritis Ratio is Associated with Mortality in Adult Trauma Patients
Tsai CH, Hsieh TM, Hsu SY, Hsieh CH
Risk Management and Healthcare Policy 2023, 16:879-887
Published Date: 12 May 2023
Treatment Outcome, Pattern of Injuries and Associated Factors Among Traumatic Patients Attending Emergency Department of Dessie City Government Hospitals, Northeast Ethiopia: A Cross-Sectional Study
Birhan S, Gedamu S, Belay MZ, Mera Mihiretu M, Tadesse Abegaz N, Fissha Adem Y, Tilahun Yemane T, Abdu Yesuf K
Open Access Emergency Medicine 2023, 15:303-312
Published Date: 8 September 2023