Back to Journals » International Journal of General Medicine » Volume 19
Immunological and Inflammatory Characteristics of Severe Cutaneous Adverse Drug Reactions: A Retrospective Study
Authors Luo Q, Mou XD, Cao D, Cheng WH
Received 30 October 2025
Accepted for publication 13 March 2026
Published 25 March 2026 Volume 2026:19 572889
DOI https://doi.org/10.2147/IJGM.S572889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Qing Luo,1– 3 Xu-Dong Mou,1– 3 Di Cao,1– 3 Wen-Hao Cheng1– 3
1Department of Dermatology, The First Affiliated Hospital of Kangda College of Nanjing Medical University, Lianyungang, Jiangsu, 222000, People’s Republic of China; 2Department of Dermatology, The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, 222000, People’s Republic of China; 3Department of Dermatology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, Lianyungang, Jiangsu, 222000, People’s Republic of China
Correspondence: Wen-Hao Cheng, Department of Dermatology, The First Affiliated Hospital of Kangda College of Nanjing Medical University, No. 182, Tongguan North Road, Haizhou District, Lianyungang, Jiangsu, 222000, People’s Republic of China, Tel +86 18961322858, Email [email protected]
Background: Severe cutaneous adverse drug reaction (SCADR) is a life-threatening immune-mediated disorder, yet humoral immune markers and inflammatory biomarkers have not been systematically characterized across major SCADR phenotypes. This study aims to identify the immunological and inflammatory characteristics of SCADR.
Methods: We retrospectively enrolled 60 SCADR patients (2015– 2024) and two control cohorts (60 mild drug eruption patients and 60 age- and sex-matched healthy subjects). Baseline serum IgG, IgA, IgM, complement C3/C4, C-reactive protein (CRP), and procalcitonin (PCT) were measured prior to treatment, and between-group comparisons, correlation analyses, and subtype analyses [Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) vs DRESS] were performed.
Results: SCADR patients had lower IgG (8.8± 4.1g/L) and complement levels (C3 1.01± 0.37g/L; C4 0.21± 0.12g/L) than controls (P< 0.05), alongside markedly elevated CRP (median: 31.1mg/L) and PCT (0.68μg/L) (P< 0.001). PCT was higher in SJS/TEN than drug reaction with eosinophilia and systemic symptoms (DRESS) (0.85 vs 0.45μg/L, P=0.04), whereas eosinophil counts were higher in DRESS. C3 correlated positively with CRP (r=0.60, P< 0.001). No significant associations were observed between immunoglobulins and PCT, and PCT and CRP were largely independent.
Conclusion: SCADR is associated with concurrent alterations in humoral immune markers and acute-phase inflammatory biomarkers. Differences in biomarker patterns between SJS/TEN and DRESS may help with early clinical phenotyping. Prospective multicenter studies are needed to validate these findings and clarify their clinical significance subsequently.
Keywords: Stevens–Johnson syndrome, toxic epidermal necrolysis, DRESS, drug-induced hypersensitivity, immunoglobulin, complement, C-reactive protein, procalcitonin, biomarker, severe adverse drug reaction
Introduction
Severe cutaneous adverse drug reactions (SCADR) are rare but life-threatening drug eruptions characterized by extensive skin involvement and systemic inflammation.1 Major entities include Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), DRESS (drug reaction with eosinophilia and systemic symptoms), and acute generalized exanthematous pustulosis (AGEP).2,3 Despite advances in supportive care, SCADR remain associated with substantial morbidity and mortality, and early risk recognition and complication surveillance (including infection and organ dysfunction) are persistent clinical challenges.4
SCADR is classically considered T-cell–mediated delayed hypersensitivity reactions, with cytotoxic injury predominating in SJS/TEN and eosinophilia/viral reactivation features more typical of DRESS.5,6 Beyond cellular immunity, increasing evidence suggests that humoral immune components—immunoglobulins and complement—may also be involved in SCADR immunopathology, and complement activation has been reported in SJS/TEN.7,8 In parallel, systemic inflammation in SCADR is routinely monitored using acute-phase biomarkers such as C-reactive protein (CRP) and procalcitonin (PCT). CRP is broadly sensitive to inflammation but has limited specificity for distinguishing sterile inflammation from superimposed infection, whereas PCT may better reflect bacterial complications in some settings, although elevations have also been reported in severe non-infectious inflammatory states.9,10
However, clinical data characterizing humoral immune markers and their relationship with inflammatory biomarkers across SCADR phenotypes remain limited. Prior work suggested reduced IgG together with elevated CRP/PCT in severe cases, but subtype-specific patterns and biomarker interrelationships were not well defined.11 We therefore conducted this retrospective study to compare immunoglobulins, complement, CRP, and PCT among patients with SCADR, mild drug eruptions, and healthy controls, and to explore whether biomarker patterns differ between major SCADR subtypes, particularly SJS/TEN and DRESS. We hypothesized that SCADR would be associated with concurrent alterations in humoral immune markers and acute-phase inflammatory biomarkers with distinct patterns across major phenotypes.
Methods
Study Design and Setting
A retrospective observational study, designed in the format of an original research investigation, was performed at a tertiary university hospital with a specialized dermatology unit and intensive care capabilities. The study protocol was reviewed and approved by the ethics committee of the First People’s Hospital of Lianyungang (Approval number: KY-20220505003). Due to the retrospective nature of the study and the use of de-identified patient data, the committee granted a waiver of informed consent. The study was conducted in accordance with the ethical principles for medical research involving human subjects outlined in the Declaration of Helsinki. Patient confidentiality was maintained at all stages of the research by assigning anonymous study codes.
All methods were carried out in accordance with relevant guidelines and regulations for retrospective studies. We adhered to the Declaration of Helsinki principles. Patient confidentiality was maintained by assigning anonymous study codes.
Patient Selection
We searched the hospital’s dermatology and allergy service records from January 2015 to December 2024 to identify patients diagnosed with a SCADR. SCADR was defined to include the following categories: Stevens–Johnson Syndrome (SJS)-acute mucocutaneous blistering disease with <10% body surface area (BSA) epidermal detachment. Toxic Epidermal Necrolysis (TEN)-similar process with >30% BSA epidermal detachment. SJS/TEN overlap-cases with 10–30% BSA detachment (these were grouped with SJS/TEN for analysis purposes).12 Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), also known as Drug-Induced Hypersensitivity Syndrome (DIHS), is characterized by rash, fever, eosinophilia, lymphadenopathy, and internal organ involvement. Drug-induced Exfoliative Dermatitis (erythroderma) is characterized by generalized erythema and scaling due to drug, meeting criteria for severe drug-induced dermatitis.
SJS, SJS/TEN overlap, and TEN were considered as a single clinicopathologic spectrum of epidermal necrolysis and are primarily differentiated by the percentage of BSA epidermal detachment (SJS <10%, overlap 10–30%, TEN >30%).13 Therefore, for analysis comparing major SCADR phenotypes, we grouped SJS, overlap, and TEN as the SJS/TEN spectrum, while still reporting the distribution of each subtype.
Inclusion criteria were as follows: (1) Clinical diagnosis of SCADR subtypes confirmed by established criteria (eg, RegiSCAR for DRESS, BSA-based for SJS/TEN) and dermatological evaluation; histopathological confirmation was required when diagnosis was uncertain. (2) Temporal association with drug exposure, defined as initiation of the suspected drug within 8 weeks for DRESS and 1–3 weeks for SJS/TEN prior to symptom onset. (3) aged ≥18 years. (4) Availability of acute-phase laboratory data including immunoglobulins, complement, CRP, and PCT before initiation of substantial treatment. Exclusion criteria were applied to minimize confounding factors affecting immune markers and included (1) pre-existing immunological or allergic conditions with abnormal immunoglobulin levels (eg, common variable immunodeficiency, IgA deficiency, hyper-IgE syndrome) or chronic atopic diseases (severe atopic dermatitis, asthma). (2) Significant chronic systemic diseases unrelated to SCADR (such as uncontrolled diabetes, chronic kidney disease, liver cirrhosis, autoimmune connective tissue diseases, or malignancies undergoing chemotherapy) that may influence immunoglobulin, complement, or acute phase reactants. (3) Receipt of systemic corticosteroids, intravenous immunoglobulin, plasmapheresis, or other immunomodulatory treatments within 30 days before admission, ensuring baseline immune measurements reflect SCADR rather than therapeutic effects. (4) Active systemic infection or sepsis prior to drug reaction onset, given these conditions independently elevate CRP and PCT. Patients developing infections secondary to SCADR were included, with co-infections noted accordingly. In this study, infection was defined as a clinically suspected or microbiologically documented infection requiring antimicrobial treatment. Sepsis was defined as (1) a documented bloodstream infection (positive blood culture) and/or (2) a clinician-documented sepsis/septic shock syndrome during admission with organ dysfunction requiring escalation of care (eg, vasopressor support), consistent with Sepsis-3 concepts.
Ultimately, as shown in Figure 1, we identified an initial cohort of 72 SCADR patients. After applying exclusions (7 had received corticosteroids before hospital labs, 3 had autoimmune comorbidities, 2 had incomplete lab data), a final SCADR cohort of 60 patients was assembled for analysis.
 |
Figure 1 Flowchart of patient selection in this study. |
Additionally, two control groups were defined: Mild drug eruption controls included 60 patients with common, benign cutaneous drug reactions – maculopapular exanthema (MPE) and fixed drug eruption (FDE) – seen during the same period. These conditions, lacking systemic involvement, serve as a disease control contrasting with SCADR. Cases were frequency-matched by year to avoid temporal bias. Inclusion required clear drug causality and absence of systemic features, while exclusion criteria mirrored those for SCADR controls. The average latency from drug exposure to rash was 7–10 days, and all recovered without hospitalization. Healthy controls comprised 60 age- and sex-matched volunteers or routine health check-up patients with no active illness, normal exams and labs, no recent drug reactions or infections, and no immunosuppressive medication use.
Data Collection
We reviewed medical records using a standardized data extraction form to collect relevant clinical and laboratory data, including demographic and clinical characteristics, SCADR subtype, causative drugs identified by clinical assessment, timing intervals, treatments administered and clinical outcomes. Laboratory measurements at initial hospital evaluation (prior to significant treatment) included immunoglobulins IgG, IgA, and IgM, measured by immunoturbidimetric assay on automated analyzers, normal adult reference ranges were IgG 7–16 g/L, IgA 07–4 g/L, and IgM 0.4–2.3 g/L. Complement components C3 and C4 were measured similarly, with reference ranges of 0.8–1.6 g/L and 0.2–0.4 g/L, respectively. C-reactive protein (CRP) was assessed via high-sensitivity immunonephelometry with normal <8 mg/L. Values >5 mg/L indicate inflammation, and >100 mg/L suggests severe infection or tissue damage. PCT was measured using an electrochemiluminescent immunoassay (ECLIA). The laboratory reference range for PCT was <0.05 µg/L. For clinical interpretation, PCT ≥0.5 µg/L was considered suggestive of significant bacterial infection, and PCT >2.0 µg/L was considered suggestive of severe bacterial infection/sepsis, consistent with published guidance.14
All lab assays underwent internal quality control and were standardized, as the tests were part of routine clinical care. For patients in the mild drug eruption group, blood samples for Ig and complement were drawn during their clinic visit or admission (some MPE patients with extensive rash might have been admitted briefly). For healthy controls, blood samples were part of their health exam (with permission to use leftover serum for research testing).
Statistical Analysis
We used IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA) for data analysis. Prior to hypothesis testing, continuous data were assessed for normality using the Shapiro–Wilk test and by inspecting Q–Q plots. Variables approximately following a normal distribution (eg, IgG, IgA, IgM, C3, C4 in our sample) were presented as mean ± standard deviation (SD). Variables with a skewed distribution (CRP, PCT, which were right-skewed) were presented as median with interquartile range (IQR).
For comparisons between the three groups (SCADR, mild eruption, healthy): One-way analysis of variance (ANOVA) was used for normally distributed variables (Ig and complement levels). If ANOVA showed a significant difference (overall P<0.05), we performed post-hoc pairwise comparisons. We employed the Student–Newman–Keuls (SNK) or Tukey’s honest significant difference test for equal variance, or Games–Howell if variances were unequal, to identify which groups differed. However, for clarity, we primarily reported whether differences between SCADR vs mild and SCADR vs healthy were significant, as those were of greatest interest. Kruskal–Wallis (K–W) H-test was used for non-parametric comparisons of CRP and PCT among the three groups. Because this study was exploratory and included multiple biomarker comparisons, we did not apply a study-wide Bonferroni or false discovery rate (FDR) correction across all analyses. Bonferroni adjustment was used only for post-hoc pairwise comparisons following a significant K–W H-test. We focused on results with large effect sizes and very small P values (eg, P<0001), and we interpreted marginal P values (near 0.05) cautiously in view of multiple testing.
Additionally, we performed a focused comparison between SJS/TEN vs DRESS subgroups within the SCADR cohort. Given the smaller sample sizes, we used non-parametric Mann–Whitney U-tests for continuous variables (since many were not normally distributed in these subgroups, and sample size <30 each) and chi-square or Fisher’s exact test for categorical comparisons (like frequency of infection). This sub-analysis was exploratory.
To assess relationships between variables within the SCADR group, we conducted correlation analyses: Pearson correlation coefficient (r) was calculated for roughly normally distributed pairs (eg, complement vs immunoglobulin levels). Spearman rank correlation (ρ) was used for pairs involving non-normal data (eg, CRP or PCT with other variables, or any ordinal measures). In practice, we ended up using Spearman for most correlations involving CRP/PCT. We particularly examined correlations between humoral markers (IgG, IgA, IgM, C3, C4) and inflammatory markers (CRP, PCT), for example, correlation of each Ig and complement with CRP, and with PCT. We also examined the correlation between CRP and PCT themselves. A two-tailed P<0.05 was considered statistically significant for correlations. We interpreted r values in context: >0.5 as moderate-to-strong correlation, 0.3–0.5 as moderate, and <0.3 as weak. We presented a key subset of results in tabular form (group comparisons) and a scatter plot for one notable correlation. All hypothesis tests used P<0.05 as a significance threshold (after adjustments if applicable). Because this was an exploratory study in part, we did not adjust for multiple comparisons across different markers beyond the mentioned post-hoc tests and Bonferroni for K–W pairwise tests.
The primary outcomes – levels of IgG, IgA, IgM, C3, C4, CRP, and PCT – were tabulated with group means/medians and p-values, as detailed in the Results section. All statistical analyses were two-sided. Given the observational nature, we did not perform a priori sample size calculation. However, our sample of 60 SCADR patients provided >80% power to detect a difference of 2.0 g/L in IgG (assuming SD ~3.5) at alpha 0.05 based on a two-sample comparison with 60 controls. The power for CRP/PCT differences was more than adequate given the large effect sizes observed. Software and graphical tools: In addition to SPSS, we used Python’s matplotlib library (v3.3) for generating the scatter plot of C3 vs CRP for better visualization in publication.
Results
Patient Characteristics
A total of 60 patients with SCADR were included, alongside 60 patients with mild drug eruptions and 60 healthy controls. The demographic and clinical characteristics of these groups are summarized in Table 1. As shown, the mean age of SCADR patients was 50 years, slightly higher than that of the mild and healthy groups (42–43 years), but this difference was not statistically significant (P=0.08). Ages ranged from 18 to 87 years in SCADR. The gender distribution was virtually equal in all groups (approximately 50% male, 50% female), and there was no significant sex difference between groups (P=0.98). Thus, any differences in immune markers are unlikely to be due to age or sex biases.
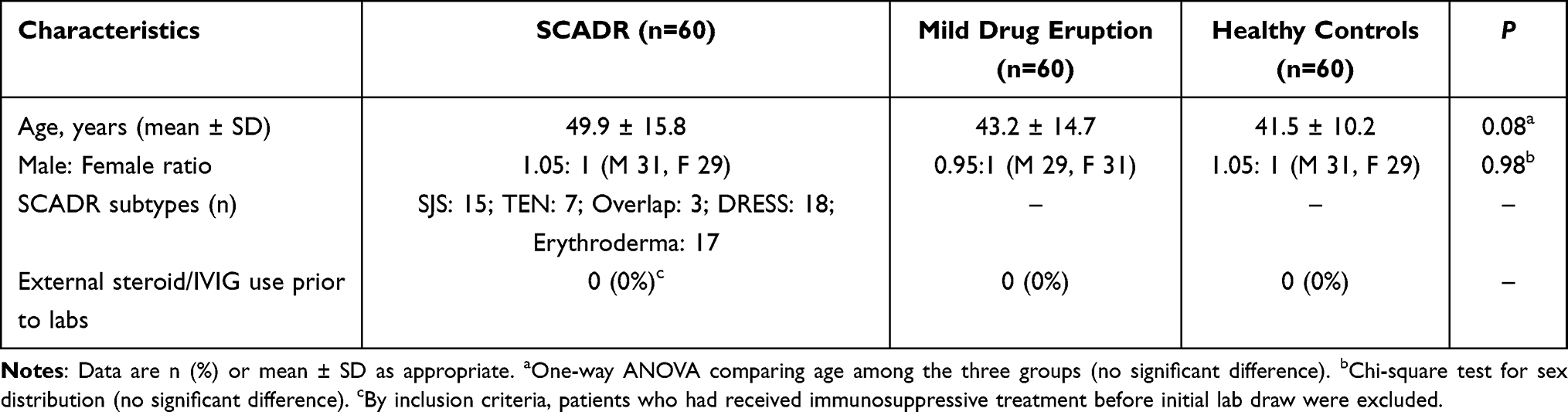 |
Table 1 Baseline Characteristics of SCADR Patients and Control Groups |
Within the SCADR group, the composition was as follows: SJS (n=15), SJS/TEN overlap (n=3), TEN (n=7)-combining these, 25 patients fell into the SJS/TEN spectrum. Eighteen patients had DRESS, and 17 patients had drug-induced erythroderma (exfoliative dermatitis). By inclusion, all SCADR patients met rigorous criteria for their diagnoses. For example, all DRESS cases were definite as per RegiSCAR (score ≥6) and had typical features (mean eosinophil count 1.2×109/L, hepatic involvement in 15/18 cases). SJS/TEN patients had SCORTEN scores ranging from 1 to 4 (mean 2.3). The erythroderma cases were all generalized (>90% BSA erythema) with systemic symptoms. The culprit drugs in SCADR were varied: the most common were allopurinol (8 cases, mostly DRESS or TEN), carbamazepine (6 cases), sulfonamide antibiotics (5 cases), beta-lactam antibiotics (7 cases), nevirapine (3 cases), vancomycin (2, one causing DRESS), among others. In the mild eruption group, culprits included antibiotics (many causing exanthems) and NSAIDs; a few FDE cases were due to antibiotics or analgesics.
Crucially, none of the patients in any group had confounding immunological conditions or pre-treatment with steroids/IVIG due to our exclusion criteria. Hence, the baseline immune marker measurements were attributable to the drug reactions themselves or the patients’ inherent response.
Immunoglobulin and Complement Levels in SCADR vs Controls
Baseline humoral immunity markers were significantly altered in SCADR patients compared to controls. The serum levels of immunoglobulins (IgG, IgA, IgM) and complement components (C3, C4), as well as CRP and PCT across the three groups are presented in Table 2. Immunoglobulin G (IgG): SCADR patients had a markedly lower mean IgG level (8.8 g/L) compared to mild drug eruption patients (10.4 g/L) and healthy individuals (12.0 g/L). This difference was highly significant (P<0.001). In fact, 28 of 60 SCADR patients (46.7%) had IgG levels below the laboratory’s age-adjusted normal range (eg, <7 g/L for older adults), whereas only 10% of mild reaction patients and 5% of healthy controls had mildly low IgG. The lowest IgG values in SCADR were observed in a few TEN and DRESS cases (nadir ~4 g/L). IgA and IgM: Mean IgA and IgM levels in SCADR were somewhat lower than in healthy controls (2.0 vs 2.8 g/L for IgA; 0.79 vs 1.12 g/L for IgM, P<0.01 for both comparisons). However, SCADR vs mild group differences for IgA (2.0 vs 2.1) and IgM (0.79 vs 0.81) were negligible and not significant. The mild group itself had slightly reduced IgA/IgM compared to healthy controls (consistent with a mild acute phase where immunoglobulins could be diluted or slightly consumed). Complement C3 and C4: Complement levels displayed a pattern similar to Ig, SCADR patients had a mean C3 of 1.01 g/L, which was significantly lower than healthy controls (1.19, P=0.01). SCADR C3 was virtually equal to the mild group’s mean (1.00 g/L), thus not significantly different from mild (both mild and SCADR had mildly depressed C3 relative to healthy). For C4, SCADR had a strikingly low mean of 0.21 g/L, whereas mild had 0.29 and healthy 0.36 g/L. The ANOVA for C4 was highly significant (P<0.001), and SCADR vs healthy difference was significant. Interestingly, SCADR vs mild difference in C4 just missed significance (P=0.07 after correction), suggesting SCADR tended to lower C4. Notably, 70% of SCADR patients had a C4 below the normal range (<0.2 g/L), and 50% had low C3 (<0.8 g/L).
 |
Table 2 Serum Immunoglobulin, Complement, and Inflammatory Marker Levels in Patients with SCADR Versus Control Groups |
Inflammatory Markers (CRP, PCT) in SCADR vs Controls
As expected, markers of systemic inflammation were dramatically elevated in SCADR patients and essentially normal in healthy controls with mild drug eruptions showing only slight elevations. C-reactive protein (CRP): Median CRP in SCADR was 31.1 mg/L (IQR 12.2–58.2). By contrast, mild drug reactions had a median CRP of only 3.87 mg/L (IQR 3.03–10.9), and healthy controls median 3.0 mg/L (most <5). The difference was highly significant (P<0.001). In fact, 85% of SCADR patients had CRP above 10 mg/L, and 40% had CRP >50 mg/L. Only 5% of mild reaction patients had CRP >10 (some mild exanthems can cause low-grade fever and CRP in teens), and none exceeded 30 mg/L. Thus, CRP clearly distinguished severe from mild reactions. PCT: Median PCT in SCADR was 0.68 µg/L (IQR 0.34–0.96), which was higher than in mild drug eruption (0.27 µg/L, IQR 0.16–0.41) and healthy controls (0.06 µg/L, IQR 0.03–0.09) (overall P<0.001; Table 2). Within the SCADR cohort, 78% had PCT >0.25 µg/L and 30% had PCT >0.5 µg/L at admission. In a sensitivity analysis stratified by patients meeting the study’s predefined sepsis criteria, admission PCT values were higher in those cases than in the remaining SCADR patients (Results shown in the clinical outcomes/infection summary), while the main between-group findings remained unchanged. Mild vs healthy controls: As a side observation, mild drug eruptions had slightly higher CRP and PCT than healthy controls (CRP medians 3.9 vs 3.0; PCT 0.27 vs 0.06). These small differences reflected that even a mild rash could cause a minimal acute phase reaction (eg, some MPE patients had low-grade fever). However, these differences were not statistically emphasized in pairwise tests (CRP mild vs healthy was P=0.07). Essentially, mild reactions did not trigger significant CRP or PCT responses, staying near normal in most individuals.
Compared with healthy controls, SCADR patients had lower IgG (mean difference −320 g/L, 95% CI: −4.60 to −1.80) and lower complement levels including C3 (−0.18 g/L, 95% CI: −0.29 to −0.07) and C4 (−0.15 g/L, 95% CI: −0.20 to −0.10). In contrast, inflammatory markers were markedly higher in SCADR, with CRP showing a median difference of 31.40 mg/L (95% CI: 22.57 to 40.23) and PCT a median difference of 0.60 µg/L (95% CI: 0.48 to 0.72) versus healthy controls (all overall P<0.05 in Table 2).
Correlation Between Humoral and Inflammatory Parameters in SCADR
We analyzed correlations within the SCADR group (n=60) between immunoglobulin levels, complement levels, and the inflammatory markers CRP and PCT. Key findings from the correlation analysis include complement C3 and CRP: There was a statistically significant positive correlation between serum C3 levels and CRP levels in SCADR patients (Pearson r=0.60, P<0.001). This correlation for illustration is exhibited in Figure 2 graphically. Importantly, the correlation remained similar after excluding the five patients meeting the predefined sepsis criteria (r remained 0.58, P<0.001). Other Ig/Complement vs CRP: No other humoral markers showed a significant correlation with CRP. As shown in Supplementary Table S1, IgG, IgA, IgM, and C4 each had weak, non-significant correlations with CRP (Pearson r values ranged from −0.18 to +0.17, all P>0.2). For example, IgG vs CRP yielded r =−0.14 (P=0.30), suggesting no clear linear relationship. Patients with low IgG did not consistently show higher or lower CRP in this dataset. Similarly, C4 vs CRP had r=0.17 (P=0.21). Thus, aside from C3, the acute phase CRP elevation appeared largely independent of baseline Ig levels in our sample. Correlations with PCT: We found no significant correlation between PCT and any immunoglobulin or complement level. In detail, the correlation coefficients (Spearman ρ) of PCT with IgG, IgA, IgM, C3, C4 were all between −0.10 and −0.22, with P-values 0.13 to 0.85. Notably, PCT and CRP themselves showed no significant correlation (Spearman ρ=−0.22, P=0.12). Inter-correlations among immunoglobulins and complement: We observed expected positive correlations among certain humoral parameters. For instance, IgG levels correlated moderately with IgA (r=0.45, P<0.001) and IgM (r=0.32, P=0.013) within SCADR patients. C3 and C4 levels were strongly correlated (r=0.68, P<0.001), as these often vary together (both produced by liver as part of complement cascade). However, immunoglobulins did not significantly correlate with complement levels in SCADR (eg, IgG vs C3, r=01, P=0.42), suggesting that the depression of Ig and complement in SCADR might stem from different mechanisms or timing.
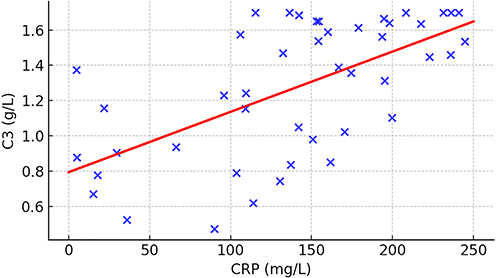 |
Figure 2 Scatter plot illustrating the positive correlation between serum complement C3 and C-reactive protein (CRP) levels in patients with severe cutaneous adverse drug reaction (SCADR). Each point represents an individual SCADR patient (n=45). A trend of increasing C3 concentration with higher CRP levels is observed (Pearson r=0.599, P<0.001), suggesting linkage between the degree of complement activation and the magnitude of systemic inflammation. |
SCADR Subtype Analysis: SJS/TEN vs DRESS
Given the heterogeneity of SCADR, we conducted an exploratory comparison of the two major subgroups in our cohort: (a) SJS/TEN (including overlap) and (b) DRESS. We excluded the erythroderma subgroup from this particular analysis to focus on these well-defined entities. This yielded 25 SJS/TEN patients and 18 DRESS patients for comparison. While the sample sizes were modest, some interesting patterns emerged: IgG levels: Mean IgG was slightly lower in SJS/TEN (8.3±4.5 g/L) compared to DRESS (9.4±3.6 g/L), but this difference was not statistically significant (Mann–Whitney, P=0.40). The proportion of patients with IgG <7 g/L was 50% in SJS/TEN and 33% in DRESS, suggesting more frequent hypogammaglobulinemia in SJS/TEN, though again sample size limited inference. Complement levels: Mean C3 in SJS/TEN was 0.95 ± 0.40 g/L vs 1.08 ± 0.33 in DRESS (P=0.25). C4 was 0.20 ± 0.11 vs 0.24 ± 0.13 (P=0.21). Complements trended lower in SJS/TEN, perhaps reflecting greater consumption in those cases with large areas of tissue injury. But differences did not reach significance. Notably, 5 SJS/TEN patients had undetectably low C4 (<0.10), whereas only 1 DRESS patient did, hinting that complement activation might be more aggressive in SJS/TEN on average. CRP levels: Median CRP was high in both: 35 mg/L in SJS/TEN vs 54 mg/L in DRESS (P=0.33). DRESS showed a wider range (some had CRP >100). If anything, DRESS patients tended to have equal or higher CRP, likely because many had liver inflammation. SJS/TEN CRP levels were also high but could be influenced by fluid losses. Overall, CRP was elevated in both subtypes, not distinguishing them clearly. PCT levels: This marker did show a distinction: SJS/TEN median PCT was 0.85 µg/L (IQR 0.45–1.30), while DRESS median PCT was 0.35 µg/L (IQR 0.20–0.60). This difference was statistically significant (P=0.041 by Mann–Whitney). Moreover, 8 out of 25 SJS/TEN patients (32%) had PCT >1.0 µg/L, compared to only 1 out of 18 DRESS patients (6%). Eosinophils and other markers: Though not the primary focus, we noted that the mean eosinophil count in DRESS was 1.5×109/L (often >20% of WBC differential), compared to 0.2×109/L in SJS/TEN (typically <5%). This significant difference (P<0.001) reiterated that eosinophilia was a hallmark of DRESS and could help differentiate it from SJS/TEN clinically. Ferritin levels were extremely high (>2000 ng/mL) in 4 DRESS patients (all of whom had features of possible HLH), whereas only 1 SJS/TEN patient had ferritin >2000 (who had sepsis).
The median hospital stay for DRESS patients was 12 days versus 18 days for SJS/TEN patients, reflecting that SJS/TEN often required intensive care/burn unit and had a more acute critical phase, whereas DRESS could often be managed on a ward unless complications arise. In our data, this difference in length of stay was significant (P=0.004). There were 2 fatalities in SJS/TEN (8% mortality) and 1 in DRESS (5.5% mortality, due to DRESS-related myocarditis).
In summary, the subtype analysis indicated that both SJS/TEN and DRESS shared the features of decreased Ig and complement and high CRP. PCT was an outlier, being higher in SJS/TEN, presumably due to infection risk, which was consistent with PCT’s role as an infection marker. In practical terms, a high PCT in a SCADR patient should raise suspicion of SJS/TEN (or overlap) especially if skin detachment was present, whereas a low PCT with very high CRP and eosinophilia fitted DRESS. DRESS and SJS/TEN likely involved somewhat different immunopathological pathways (eg, DRESS with viral reactivation and eosinophils vs SJS/TEN with direct extensive tissue necrosis and secondary infection), but our data showed that humoral immune suppression (low IgG, complement) was common to both.
Discussion
In this study, we systematically analyzed humoral immune parameters and inflammatory markers in SCADR and found distinct abnormalities that shed light on SCADR pathophysiology. To our knowledge, this was one of the first comprehensive investigations to integrate immunoglobulins, complement, CRP, and PCT in a SCADR cohort with subtype analyses, thereby providing a multi-faceted view of the immune response in these conditions. Our findings might be contextualized and interpreted alongside emerging research from 2020 to 2025, leading to several important discussions.
Humoral Immune Suppression in SCADR (Low Immunoglobulins and Complement)
We observed that SCADR patients, at presentation, significantly reduced levels of circulating IgG (and to a lesser extent IgA, IgM) compared to healthy controls. Nearly half of SCADR patients had IgG below the normal range. This aligned with previous clinical observations, especially in DRESS. DRESS/DIHS was known to involve transient hypogammaglobulinemia during its acute phase.15 Indeed, as part of the multi-phase illness in DRESS, investigators had noted a paradoxical decrease in B cells and serum IgG coinciding with the onset of symptoms, which often correlated with herpesvirus reactivations (eg, HHV-6). The postulated mechanism was that the drug-specific immune response triggered widespread lymphocyte activation and then a state of immune suppression-possibly via expansion of regulatory T-cells or activation-induced cell death affecting B-cells, resulting in lower immunoglobulin synthesis and function. The decreased immunoglobulin levels allowed latent viruses to reactivate, which in turn fueled the inflammatory symptoms of DRESS (like fever, organ injury) in a vicious cycle.16 We did not have serial measurements on all patients, but a few DRESS cases showed IgG increasing from ~6 g/L at onset to ~10 g/L at 2-month follow-up, consistent with recovery of humoral immunity17 In SJS/TEN, the notion of immunoglobulin suppression was less documented, but our finding of low IgG in SJS/TEN suggested some overlapping mechanisms or consequences There were a few plausible explanations: JS/TEN patients had extensive skin loss akin to burns. They exuded fluid rich in proteins (including immunoglobulins) from denuded dermis. Also, critical illness caused a catabolic state that might decrease Ig levels. In major burns, total IgG might drop due to fluid shifts and consumption. By analogy, acute TEN could cause a drop in measurable IgG simply by third-spacing of plasma and high metabolic turnover.18 Another possibility was that in SCADR, especially SJS/TEN, drug antigens form complexes with IgG that are deposited in tissues (skin or organs), effectively reducing circulating IgG. Deposition of Ig (including IgM, IgA) along basement membranes in SJS/TEN lesions was reported, and immune complexes might also deposit in internal organs or be cleared by the reticuloendothelial system, thereby lowering blood Ig19 SCADR involved high levels of cytokines (eg, IL-6, IL-10). IL-6 actually would tend to increase Ig production (it drives plasma cell differentiation). However, extremely high interferon-gamma and TNF in SJS/TEN might paradoxically suppress B-cell function or cause loss of immunoglobulins via capillary leak.20 Thus, a deficiency during SCADR might increase susceptibility to infections – compounding the risk already posed by breaches in the skin barrier. This immunoparesis might partly explain why secondary infections were common in SCADR (occurring in up to 30–50% of SJS/TEN patients). Meta-analyses suggested IVIG (especially high-dose ≥2 g/kg) combined with steroids could shorten the disease course and possibly improve ocular outcomes.21 Clinically, reduced IgG might reflect altered humoral status during acute SCADR. However, our study did not assess immunoglobulin kinetics, infection outcomes, or treatment response. Therefore, we do not infer therapeutic benefits from the observed IgG differences, and any treatment implications should be evaluated in prospective studies.
We also found that complement C3 and C4 were significantly reduced in SCADR (vs healthy). Complement consumption was a plausible consequence of SCADR due to immune complex formation and tissue destruction releasing complement-activating substances. The Chinese study we mirrored similarly found lower C3/C4 in SCADR patients than in healthy controls. One interpretation offered was that complement activation during the drug reaction leads to consumption of C3/C4, and if complement levels were insufficient (whether due to genetic factors or prior consumption), immune complexes could not be efficiently cleared, exacerbating inflammation. Complement activation fragments like C3a, C5a promoted inflammation by recruiting cells and increasing vascular permeability, while the membrane attacked complex damages cells.22
In DRESS, the role of complement was less clear. We noted DRESS patients in our study had slightly higher C3/C4 than SJS/TEN on average, which might mean complement was less aggressively consumed than in SJS/TEN where there was massive cell lysis. Our finding that C4 was particularly low in SCADR was notable because C4 was part of the classical pathway (activated by antigen–antibody complexes). Low C4 could indicate a classical complement pathway activation by IgM or IgG drug-antigen complexes. Meanwhile, alternative pathway activation (which affects C3 more) could occur via tissue damage (release of DAMPs that directly activate complement). The differential pattern (C4 more depressed than C3 in some SCADR) might suggest immune-complex driven classical activation is significant.23
Acute-Phase Inflammation and Biomarkers (CRP and PCT)
All SCADR patients in our study had elevated CRP, confirming that severe drug reactions induced a robust acute-phase response. CRP was largely IL-6 driven; indeed, IL-6 was known to be elevated in SJS/TEN and correlated with severity (it is part of the SIRS response). CRP rose quickly and was fairly insensitive to immunosuppression.24 In TEN, CRP could be extremely high acutely, but interestingly, not all prognostic scoring included CRP. A recent review highlighted key knowledge gaps such as how inflammatory markers like CRP are related to outcomes in SJS/TEN.25 While CRP itself might not predict mortality (which depends on multi-factorial SCORTEN elements), it was certainly a gauge of how stormy the immune reaction was.
PCT’s role in SCADR management was emerging. Our data reinforced that PCT was generally low in pure drug hypersensitivity inflammation but spikes in the presence of bacterial infection. In this manuscript, infection refers to patients meeting our predefined sepsis criteria (microbiologically documented bacterial infection and/or clinical sepsis/septic shock with organ dysfunction), as specified in the Methods. The significant difference we found between SJS/TEN and DRESS PCT levels echoed what Thara et al reported: on day 7 of admission, PCT remained higher in SJS/TEN, especially those with infections, whereas DRESS patients had declining PCT and faster recovery.26 They noted that PCT >2.0 ng/mL in SJS/TEN often corresponded to sepsis and correlated with severity (rho ~0.24). Our study captured PCT at baseline. Those who eventually had sepsis already showed higher initial PCT. A high PCT in a SCADR at admission should prompt aggressive sepsis surveillance and possibly empiric antimicrobials, whereas a low PCT was reassuring that no systemic bacterial infection was present, allowing one to focus on immunomodulatory therapy for the drug reaction itself.27 It is worth noting that PCT can be induced by extensive tissue damage in SJS/TEN, so a high PCT is not automatically indicative of infection. Non-bacterial elevation of PCT is thought to occur due to generalized cytokine release. The case we discussed of acetazolamide DRESS with PCT up to 65 µg/L is extreme, patient have multi-organ failure that may have induced a cytokine storm akin to sepsis or even have had microbial translocation.28 PCT may increase not only in bacterial infection but also in severe sterile inflammation and extensive tissue injury. Therefore, elevated PCT in SJS/TEN should be interpreted together with clinical and microbiological evidence of infection. In our cohort, admission PCT was markedly higher in SCADR patients with sepsis than in those without infection, supporting that marked PCT elevations are more consistent with superimposed bacterial sepsis rather than SCADR inflammation alone. PCT may help identify systemic bacterial infection. Because the number of sepsis cases and deaths was limited, we did not perform a robust PCT–mortality analysis, which should be evaluated in larger prospective cohorts.
Correlation of Complement C3 with CRP – a Link Between Complement and Inflammation
One intriguing result was the positive correlation between C3 and CRP levels in SCADR patients. At face value, one might have expected an inverse relationship if more inflammation meant more complement consumption (hence lower C3). However, our data (and the Chinese study’s data) showed the opposite-those with higher CRP had higher C3 levels remaining. Several possible interpretations: Acute phase production: C3, like CRP, is an acute phase protein (though a moderate one). During acute inflammation, the liver can increase synthesis of complement components. It is possible that in patients with extremely high IL-6 (hence very high CRP), the liver produces more C3 as well.29 Therefore, their measured C3 might be relatively preserved or even elevated, despite usage. Conversely, patients with lower CRP (less IL-6 drive) might not upregulate C3 and thus their C3 appears lower, perhaps due to consumption not being offset. This would create a positive correlation, as observed.30 Pre-existing nutritional or immunological status: Patients with low baseline complement (eg, due to genetic or nutritional factors) might mount a weaker inflammatory response (hence lower CRP). Conversely, individuals with robust complement levels (perhaps due to genetics or functional asplenia causing high baseline complement) might react vigorously with high CRP too. In our context, none had known genetic complement deficiencies, but there might be individual variance.31 Timing of sample: It could be that those who presented earlier in the course (when complement had been consumed heavily at the reaction site but before acute phase rise) might show low C3 with relatively lower CRP, whereas those who presented slightly later had both CRP and C3 trending up from acute phase response. Without serial measurements, timing could confound a snapshot correlation.32
From a mechanistic insight perspective, this correlation invites further study. It suggests that complement and CRP – both parts of innate immunity – are co-regulated in SCADR. Perhaps, therapies targeting one will influence the other. On the flip side, if complement is deliberately inhibited (say eculizumab, an anti-C5 drug, in a trial setting for TEN), CRP may not be directly affected by that, but overall inflammation may drop, which will lower CRP secondarily.33 Our correlation result essentially underscores that complement C3 level is not simply depleted in proportion to inflammation. Rather, it tends to remain higher when inflammation is high, hinting at an acute phase compensation. We observed a moderate positive association between C3 and CRP within the SCADR cohort. This finding should be interpreted as exploratory and does not establish a mechanistic link or directionality. Because we did not measure upstream cytokines (eg, IL-6), complement activation fragments, or longitudinal trajectories, we could not determine whether this association reflects acute-phase regulation, consumption/replenishment dynamics, timing of sampling, or other unmeasured factors Future prospective studies with serial measurements are needed to clarify the biological basis and clinical relevance of this association.
Differences Between SCADR Subtypes (SJS/TEN vs DRESS) and Biomarker Utility
Both SJS/TEN and DRESS manifest humoral immune suppression (low Ig, low complement) and high CRP. This suggests that these markers (Ig, complement, CRP) can signal a severe reaction in general, but are not specific to which type of eosinophil count remains a key differentiator-high in DRESS, low in SJS/TEN. PCT differences we already elaborated-higher in SJS/TEN, often normal in DRESS (unless DRESS patient has an infection-like pneumonia, which can happen but is less frequent early on). Also, our data and literature indicate that ferritin can be extremely high in DRESS (due to HLH-like immunopathology) as well as in severe SJS/TEN (due to extensive inflammation), but perhaps more consistently elevate in DRESS given the frequent HLH overlap.34 The prognostic implications are noteworthy. In SJS/TEN, mortality is mostly driven by acute epithelial loss and sepsis in the first 1–2 weeks. Therefore, markers that indicate infection risk (like PCT) or systemic inflammation (CRP) are relevant. A study pointed out knowledge gaps in SJS/TEN severity assessment, suggesting research needed to include biomarkers for disease progression. PCT may be one such biomarker for early detection of sepsis, and perhaps even as a severity marker (since a very high PCT may mean the patient’s systemic inflammation is out of control, or they have developed bacterial translocation through gut or skin).25 In DRESS, mortality can occur later (weeks into illness) often from organ failures (like liver failure or myocarditis) or HLH. Biomarkers that predict those complications early may be valuable.35 For instance, a rising ferritin and falling fibrinogen may hint at HLH development. Complement levels can be of interest: in DRESS-associated myocarditis, complement deposition in heart tissue has been observed in some case reports (with low circulating complement).
Combining markers can enhance early differentiation: If a patient has high CRP, high eosinophils, low PCT, this strongly suggests DRESS (especially with rash and liver involvement), whereas high CRP, normal eosinophils, and high PCT suggest SJS/TEN with likely infection or sepsis. Very low IgG levels or a rapid early decline in IgG can be a clue to DRESS, since the early IgG drop is reported to corroborate suspicion of DRESS Conversely, in an SJS case, Ig levels may not drop until maybe later (or might drop primarily due to loss).
It is also worth noting that some SCADR cases defy easy classification (overlap or atypical). In those, a biomarker panel may help—eg, an overlap patient who has both features may show a mixed picture (moderate eos, moderate PCT, etc.). The field is moving toward precision medicine even in adverse reactions; HLA genotyping is used to predict risks (like HLA-B*58:01 for allopurinol causing both DRESS and SJS).36 Perhaps immunophenotyping with markers may eventually stratify patients by predominant immune pathway.
Therapeutic Considerations and Future Directions
Our findings open a discussion about potential targeted therapies. As suggested in the Chinese study conclusion, complement factors can be new targets. If complement activation is contributing to tissue damage in SCADR, drugs like eculizumab (C5 inhibitor) may theoretically reduce the formation of membrane attack complex and C5a-mediated inflammation.37 There is precedent in other severe immune reactions. Eculizumab has been used in severe Steven-Johnson syndrome-like reactions in acute GVHD (graft-vs-host disease) with some success in case reports, and in other hyperinflammatory states (eg, transplant-associated thrombotic microangiopathy). No trials have yet been conducted in SCADR, but given the parallels between TEN and burns/SIRS, and the known role of complement in other acute inflammatory conditions, exploring complement blockade can be worthwhile. IVIG therapy: We have touched on this, but to elaborate, IVIG at high dose (2g/kg) in SJS/TEN is controversial – some studies show reduced mortality, others show no effect. There is speculation that IVIG’s benefit may be more pronounced in pediatric SJS/TEN and in certain ethnic groups. A recent network meta-analysis suggested that combination therapy of IVIG plus corticosteroids might reduce mortality in TEN and SJS/TEN overlap, whereas cyclosporine alone was also effective.21 Our study underscores a simple point: SCADR patients are in an Ig-deficient and immune-complex-rich state; giving IVIG can both raise Ig levels and help scavenge immune complexes (through the reticuloendothelial system uptake of IgG-coated complexes). Corticosteroids and immunosuppressants: Systemic corticosteroids remain first-line for DRESS and are commonly used in SJS/TEN in many centers (though some debate optimal dosing).38 Steroids will suppress IL-6 (lower CRP), but as noted, CRP may remain high in the presence of ongoing tissue necrosis. Steroids also raise neutrophil counts and can decrease lymphocyte counts-interestingly in DRESS, after starting steroids, some immunoglobulin recovery may happen as inflammation subsides.39 Cyclosporine (CsA) has gained traction for SJS/TEN in recent years. CsA targets T-cells (inhibiting IL-2). It may indirectly reduce some inflammatory markers (IL-6, etc). There is evidence from small studies that cyclosporine improves outcomes in SJS/TEN, possibly by halting cytotoxic T-cell activity quicker.40 Monitoring and personalized therapy: One can envision that in the future, SCADR management may involve periodic measurement of immunological biomarkers to guide therapy duration.
Our results corroborated the prior study in several aspects: they also found SCADR patients had lower IgG and higher CRP/PCT than a fixed drug eruption group. However, they did not find significant differences in IgA, IgM, C3, C4 between SCADR and FDE, which was similar to our finding of those being mainly different vs healthy but not mild.41 They reported no correlation of Ig levels with CRP, except a positive correlation of C3 with CRP-exactly as we did. This consistency strengthened confidence in those findings. Our expansion by adding healthy controls and more patients, plus separating SJS/TEN vs DRESS, extended that prior work. Other literature included studies on immune checkpoint inhibitor-related SJS/DRESS (which we did not specifically address)-those suggested similar immune patterns but often concomitant autoimmunity.42 As SCADR research moved forward, integrating these biomarkers in larger multi-center studies (for example, the RegiSCADR registry might consider collecting such data) could be useful.
We acknowledge the limitations of our study. The sample size, while moderate for an uncommon disease, is still relatively small for subgroup analyses. Our study is retrospective and single-center, which may limit generalizability. There may be referral bias (a tertiary center sees more severe cases). We measure markers at a single time-point (on admission); dynamic changes over time are not captured in a standardized way. A prospective study with serial measurements will be ideal to understand the trajectory of these markers (eg, how quickly does IgG recover? Does complement remain low or rebound? What happens to CRP/PCT over the course and with treatment?).
Another limitation is that we do not measure other relevant cytokines or mediators (like IL-6, IL-5, TNF, granulysin levels, etc.) which may have provided a more direct mechanistic correlation with CRP/PCT changes. We rely on CRP and PCT as surrogates for the cytokine environment. In addition, total IgE is not routinely measured in this study. Given that elevated IgE has been reported in some patients with DRESS, the lack of IgE data may have limited a more comprehensive assessment of humoral immune alterations, particularly in the DRESS subgroup, which should be addressed in future prospective studies. Additionally, while we exclude patients with confounders as much as possible, it is challenging to ensure that some SCADR patients do not have subclinical infections at presentation (eg, maybe a TEN patient has a bit of bacterial translocation, raising PCT slightly without overt infection). Besides, baseline complete blood count (CBC) data are not consistently available in this retrospective cohort. Thus, we fail to evaluate neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) or their associations with CRP, PCT and complement levels, future prospective studies should collect standardized CBC data to evaluate the prognostic value of these markers in SCADR. Finally, we perform multiple comparisons (many markers between groups) which can inflate Type I error, although the differences are large and mostly consistent with prior knowledge.
Conclusion
SCADR is associated with concurrent alterations in humoral immune markers and acute-phase inflammatory biomarkers, including lower IgG/complement levels and higher CRP/PCT compared with mild drug eruptions and healthy controls. Biomarker patterns differ across major phenotypes with higher PCT in SJS/TEN and more prominent eosinophilia in DRESS, which may assist early phenotyping and risk stratification. Prospective, multicenter studies with standardized sampling and outcome assessment are needed to validate these observations and clarify their clinical utility.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Zhang J, Lei Z, Xu C, Zhao J, Kang X. Current perspectives on severe drug eruption. Clin Rev Allergy Immunol. 2021;61(3):282–14. doi:10.1007/s12016-021-08859-0
2. Chang HC, Wang TJ, Lin MH, Chen TJ. A review of the systemic treatment of stevens-johnson syndrome and toxic epidermal necrolysis. Biomedicines. 2022;10(9). doi:10.3390/biomedicines10092105
3. Kliniec K, Snopkowska A, Łyko M, Jankowska-Konsur A. Erythroderma: a retrospective study of 212 patients hospitalized in a tertiary center in Lower Silesia, Poland. J Clin Med. 2024;13(3). doi:10.3390/jcm13030645
4. Moshayedi MA, Asilian A, Mokhtari F. Evaluation of severe adverse cutaneous drug reactions in patients admitted to tertiary care center: a cross-sectional study. Health Sci Rep. 2024;7(3):e1969. doi:10.1002/hsr2.1969
5. Chen CB, Hung WK, Wang CW, Lee CC, Hung SI, Chung WH. Advances in understanding of the pathogenesis and therapeutic implications of drug reaction with eosinophilia and systemic symptoms: an updated review. Front Med. 2023;10:1187937. doi:10.3389/fmed.2023.1187937
6. Cadot R, Gery P, Lenief V, Nicolas JF, Vocanson M, Tauber M. Exploring recent advances in drugs severe cutaneous adverse reactions immunopathology. Allergy. 2025;80(1):47–62. doi:10.1111/all.16316
7. Marks ME, Botta RK, Abe R, et al. Updates in SJS/TEN: collaboration, innovation, and community. Front Med. 2023;10:1213889. doi:10.3389/fmed.2023.1213889
8. Gibson A, Ram R, Gangula R, et al. Multiomic single-cell sequencing defines tissue-specific responses in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Commun. 2024;15(1):8722. doi:10.1038/s41467-024-52990-3
9. Castelli GP, Pognani C, Meisner M, Stuani A, Bellomi D, Sgarbi L. Procalcitonin and C-reactive protein during systemic inflammatory response syndrome, sepsis and organ dysfunction. Crit Care. 2004;8(4):R234–42. doi:10.1186/cc2877
10. Bhatt KP, Alsoud F, Prashad A, et al. Drug reaction with eosinophilia and systemic symptoms (DRESS): an unusual manifestation of multi-visceral abnormalities and long-term outcome. Discoveries. 2023;11(1):e170. doi:10.15190/d.2023.9
11. Mizukawa Y, Kimishima M, Aoyama Y, Shiohara T. Predictive biomarkers for cytomegalovirus reactivation before and after immunosuppressive therapy: a single-institution retrospective long-term analysis of patients with drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic syndrome (DRESS). Int J Infect Dis. 2020;100:239–246. doi:10.1016/j.ijid.2020.08.078
12. Frantz R, Huang S, Are A, Motaparthi K. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of diagnosis and management. Medicina. 2021;57(9). doi:10.3390/medicina57090895
13. Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1):92–96.
14. Meisner M. Update on procalcitonin measurements. Ann Lab Med. 2014;34(4):263–273. doi:10.3343/alm.2014.34.4.263
15. Kano Y, Inaoka M, Shiohara T. Association between anticonvulsant hypersensitivity syndrome and human herpesvirus 6 reactivation and hypogammaglobulinemia. Arch Dermatol. 2004;140(2):183–188. doi:10.1001/archderm.140.2.183
16. Manieri E, Dondi A, Neri I, Lanari M. Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome in childhood: a narrative review. Front Med. 2023;10:1108345. doi:10.3389/fmed.2023.1108345
17. Primisawitri PP, Mawardi P. The correlation of neutrophil-lymphocyte ratio and eosinophil count with SCORTEN in SJS/TEN. Clin Cosmet Invest Dermatol. 2022;15:547–556. doi:10.2147/ccid.s356450
18. Shah H, Parisi R, Mukherjee E, Phillips EJ, Dodiuk-Gad RP. Update on Stevens-Johnson syndrome and toxic epidermal necrolysis: diagnosis and management. Am J Clin Dermatol. 2024;25(6):891–908. doi:10.1007/s40257-024-00889-6
19. Justice J, Mukherjee E, Martin-Pozo M, Phillips E. Updates in the pathogenesis of SJS/TEN. Allergol Int. 2025;74(3):361–371. doi:10.1016/j.alit.2025.05.002
20. Koduri MA, Prasad D, Upadhyaya S, et al. Differential expression of tear film cytokines in Stevens-Johnson syndrome patients and comparative review of literature. Sci Rep. 2021;11(1):18433. doi:10.1038/s41598-021-97575-y
21. Tsai TY, Huang IH, Chao YC, et al. Treating toxic epidermal necrolysis with systemic immunomodulating therapies: a systematic review and network meta-analysis. J Am Acad Dermatol. 2021;84(2):390–397. doi:10.1016/j.jaad.2020.08.122
22. Kinoshita M, Ogawa Y, Hama N, et al. Neutrophils initiate and exacerbate Stevens-Johnson syndrome and toxic epidermal necrolysis. Sci Transl Med. 2021;13(600). doi:10.1126/scitranslmed.aax2398
23. Coss SL, Zhou D, Chua GT, et al. The complement system and human autoimmune diseases. J Autoimmun. 2023;137:102979. doi:10.1016/j.jaut.2022.102979
24. Horcajada-Reales C, Pulido-Pérez A, Suárez-Fernández R. Severe cutaneous drug reactions: do overlapping forms exist? Actas Dermosifiliogr. 2016;107(1):23–33. doi:10.1016/j.ad.2015.08.006
25. Lehloenya RJ. Disease severity and status in Stevens-Johnson syndrome and toxic epidermal necrolysis: key knowledge gaps and research needs. Front Med. 2022;9:901401. doi:10.3389/fmed.2022.901401
26. Thara GN, Pai VV, Kadkol A, Fernandes E, Shulka P. A cross-sectional analysis of inflammatory markers as a severity and prognostic indicator in severe cutaneous adverse drug reactions. Indian J Dermatol Venereol Leprol. 2026;92(1):22–30. doi:10.25259/ijdvl_1284_2024
27. Tempark T, John S, Rerknimitr P, Satapornpong P, Sukasem C. Drug-Induced Severe Cutaneous Adverse Reactions: insights Into Clinical Presentation, Immunopathogenesis, Diagnostic Methods, Treatment, and Pharmacogenomics. Front Pharmacol. 2022;13:832048. doi:10.3389/fphar.2022.832048
28. Sfia M, Boeckler P, Lipsker D. High procalcitonin levels in patients with severe drug reactions. Arch Dermatol. 2007;143(12):1591. doi:10.1001/archderm.143.12.1591-a
29. Thorgersen EB, Barratt-Due A, Haugaa H, et al. The Role of Complement in Liver Injury, Regeneration, and Transplantation. Hepatology. 2019;70(2):725–736. doi:10.1002/hep.30508
30. Bhaskar S, Sinha A, Banach M, et al. Cytokine storm in COVID-19-immunopathological mechanisms, clinical considerations, and therapeutic approaches: the REPROGRAM Consortium position paper. Front Immunol. 2020;11:1648. doi:10.3389/fimmu.2020.01648
31. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.00754
32. Triggianese P, Conigliaro P, De Martino E, Monosi B, Chimenti MS. Overview on the link between the complement system and auto-immune articular and pulmonary disease. Open Access Rheumatol. 2023;15:65–79. doi:10.2147/oarrr.s318826
33. Noone DP, Isendoorn MME, Hamers S, et al. Structural basis for surface activation of the classical complement cascade by the short pentraxin C-reactive protein. Proc Natl Acad Sci U S A. 2024;121(37):e2404542121. doi:10.1073/pnas.2404542121
34. Pan Y, Tang S, Zheng S, et al. Association between serum ferritin and the severity of drug eruptions. J Clin Lab Anal. 2020;34(2):e23043. doi:10.1002/jcla.23043
35. Fadhel NB, Ammar H, Ben Romdhane H, et al. Hemophagocytic lymphohistiocytosis overlapping drug reaction with eosinophilia and systemic symptoms syndrome: a retrospective study and a brief review of the literature. Dermatitis. 2023;34(3):262–264. doi:10.1097/der.0000000000000890
36. Wang Q, Sun S, Xie M, Zhao K, Li X, Zhao Z. Association between the HLA-B alleles and carbamazepine-induced SJS/TEN: a meta-analysis. Epilepsy Res. 2017;135:19–28. doi:10.1016/j.eplepsyres.2017.05.015
37. Wang F, Huang L, Yu J, Zang D, Ye L, Zhu Q. Altered levels of complement components associated with non-immediate drug hypersensitivity reactions. J Immunotoxicol. 2020;17(1):1–9. doi:10.1080/1547691x.2019.1695985
38. Brüggen MC, Walsh S, Ameri MM, et al. Management of adult patients with drug reaction with eosinophilia and systemic symptoms: a delphi-based international consensus. JAMA Dermatol. 2024;160(1):37–44. doi:10.1001/jamadermatol.2023.4450
39. Fay ME, Myers DR, Kumar A, et al. Cellular softening mediates leukocyte demargination and trafficking, thereby increasing clinical blood counts. Proc Natl Acad Sci U S A. 2016;113(8):1987–1992. doi:10.1073/pnas.1508920113
40. Ng QX, De Deyn M, Venkatanarayanan N, Ho CYX, Yeo WS. A meta-analysis of cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res. 2018;11:135–142. doi:10.2147/jir.s160964
41. Yoon SY, Baek SH, Kim S, et al. Serum procalcitonin as a biomarker differentiating delayed-type drug hypersensitivity from systemic bacterial infection. J Allergy Clin Immunol. 2013;132(4):981–983. doi:10.1016/j.jaci.2013.04.038
42. Zhou J, Wang CP, Li J, Zhang HL, He CX. Stevens-Johnson syndrome and toxic epidermal necrolysis associated with immune checkpoint inhibitors: a systematic review. Front Immunol. 2024;15:1414136. doi:10.3389/fimmu.2024.1414136
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of Neutrophil to Lymphocyte Ratio for Predicting 90-Day Poor Outcomes in Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Feng X, Xiao H, Duan Y, Li Q, Ou X
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1219-1230
Published Date: 14 June 2023
The Role of Albumin in the Diagnosis of Neonatal Sepsis Over the Last 11 Years: A Retrospective Study
Shi J, Lu ZQ, Lin QM, Zeng W, Gu PJ, Yu Q, Long J, Huang DG, Dai YH
Journal of Inflammation Research 2023, 16:2855-2863
Published Date: 19 July 2023
High Level of Serum Complement C3 Expression is Associated with Postoperative Vasculopathy Progression in Moyamoya Disease
Wang MJ, Wang J, Zhang H, Hao FB, Gao G, Liu SM, Wang XP, Li JJ, Zou ZX, Guo QB, Fu HG, Han YQ, Han C, Duan L
Journal of Inflammation Research 2024, 17:1721-1733
Published Date: 18 March 2024
Diagnostic Utility of Pleural C-Reactive Protein and Procalcitonin for Parapneumonic Pleural Effusion: A Head-to-Head Comparison Study
Yang Q, Cha SN, Niu Y, Wen JX, Yan L, Hai L, Wang YJ, Gao WH, Zhou F, Zhou Q, Hu ZD, Zheng WQ
Infection and Drug Resistance 2025, 18:919-927
Published Date: 17 February 2025
Integrated Early CRP Kinetics and Plasma EBV DNA Clearance as Prognostic Biomarkers in De Novo Metastatic Nasopharyngeal Carcinoma Treated with First-Line Chemoimmunotherapy
Fang M, Hu Y, Wang T, Su Y, Lu T, Zhang H, Li J, Xie C, Gong X
Journal of Inflammation Research 2025, 18:6783-6794
Published Date: 26 May 2025