Back to Journals » Lung Cancer: Targets and Therapy » Volume 16
Genomic Profiling of Extensive Stage Small-Cell Lung Cancer Patients Identifies Molecular Factors Associated with Survival
Authors Canale M ![]() , Urbini M, Petracci E, Angeli D, Tedaldi G
, Urbini M, Petracci E, Angeli D, Tedaldi G ![]() , Priano I, Cravero P, Flospergher M, Andrikou K, Bennati C, Tassinari D, Dubini A, Rossi G, Panzacchi R, Valli M, Bronte G, Crinò L
, Priano I, Cravero P, Flospergher M, Andrikou K, Bennati C, Tassinari D, Dubini A, Rossi G, Panzacchi R, Valli M, Bronte G, Crinò L ![]() , Delmonte A, Ulivi P
, Delmonte A, Ulivi P ![]()
Received 24 August 2024
Accepted for publication 11 January 2025
Published 20 February 2025 Volume 2025:16 Pages 11—23
DOI https://doi.org/10.2147/LCTT.S492825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sai-Hong Ou
Matteo Canale,1 Milena Urbini,1 Elisabetta Petracci,2 Davide Angeli,2 Gianluca Tedaldi,1 Ilaria Priano,3 Paola Cravero,4 Michele Flospergher,4 Kalliopi Andrikou,4 Chiara Bennati,5 Davide Tassinari,6 Alessandra Dubini,7 Giulio Rossi,8 Riccardo Panzacchi,9 Mirca Valli,10 Giuseppe Bronte,11,12 Lucio Crinò,4 Angelo Delmonte,4 Paola Ulivi1
1Biosciences Laboratory, IRCCS Istituto Romagnolo per Lo Studio Dei Tumori (IRST) “dino Amadori”, Meldola, Italy; 2Unit of Biostatistics and Clinical Trials, IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST) “Dino Amadori”, Meldola, Italy; 3Department of Medical Oncology, Vall d´Hebron Institute of Oncology (VHIO), Vall d’Hebron Hospital Universitari, Barcelona, Spain; 4Department of Medical Oncology, IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST) “Dino Amadori”, Meldola, 47014, Italy; 5Department of Onco-Hematology, Santa Maria Delle Croci Hospital, Ravenna, Italy; 6Department of Medical Oncology, Infermi Hospital, Rimini, Italy; 7Department of Pathology, Morgagni-Pierantoni Hospital, Forlì, Italy; 8Fondazione Poliambulanza, Brescia, Italy; 9Department of Pathology, Ospedale S. Maria Della Scaletta, Imola, Italy; 10Department of Pathology, Infermi Hospital, Rimini, Italy; 11Department of Medicina Traslazionale E per la Romagna, University of Ferrara, Ferrara, Italy; 12Department of Medical Oncology, University Hospital of Ferrara, Ferrara, Italy
Correspondence: Angelo Delmonte, Email [email protected]
Objective: Extensive stage Small-Cell Lung Cancer (ES-SCLC) is the most lethal lung cancer, and the addition of immunotherapy conferred a slight survival benefit for patients. Extensive molecular profiling of patients treated with chemotherapy (CT) or chemotherapy plus immunotherapy (CT+IO) would be able to identify molecular factors associated with patients’ survival.
Material and Methods: In this retrospective study, 99 ES-SCLC patients were considered. Of the 79 includible patients, 42 received CT (median age 71 y/o, I–IIIQ: 65– 76), and 37 received CT+IO (median age 71 y/o, I–IIIQ 66– 75). The FoundationOne CDx assay was performed on patients’ tumor tissues.
Results: The most mutated genes were TP53 (99%), RB1 (78%), PTEN (23%) and MLL2 (20%), with no significant differences between the treatment groups. As a continuous variable, Tumor Mutation Burden (TMB) had an effect on patients’ progression-free survival (PFS) by type of treatment (HR 1.81 (95%, CI: 0.99– 3.31) and HR 0.84 (95%, CI: 0.56– 1.26) for patients treated with CT and CT+IO, respectively). TMB was also computed and dichotomized using two different cut-offs: considering cut-offs of 10 mut/Mb and > 16 mut/Mb, 45 patients (57%) and 68 patients (86.1%) had a low TMB, respectively. A high TMB (cut-off 10 mut/Mb) predicted worse PFS in patients treated with CT (p=0.046); even though not statistically significant, a high TMB (cut-off 16 mut/Mb) predicted a better survival in patients treated with CT+IO. Moreover, at univariate analysis, MLL2 mutations were associated with better prognosis in the overall case series (HRPFS = 0.51, 95% CI: 0.28– 0.94), and overall survival (HROS = 0.52, 95% CI: 0.28– 0.97).
Conclusion: In ES-SCLC, TMB is associated with worse survival in patients treated with CT alone, and with better survival in patients treated with CT+IO, whether considered as a continuous or a dichotomized variable, at different cut-offs. Alterations in epigenetic factors are also associated to better patient prognosis.
Keywords: small-cell lung cancer, predictive biomarkers, immunotherapy, patients prognosis, tumor mutation burden
Introduction
Lung cancer accounts for one in 10 diagnosed cancers and one in 5 cancer-related deaths, ranking as the second most common and the most lethal malignancy.1 Small-cell lung cancer (SCLC) accounts for 15% of all lung cancers, representing the most aggressive malignancy of the lung and one of the most lethal cancer histologies, associated with an early metastatic spread and a fast tumor growth rate, resulting in a median 5-year overall survival of 2% and a median survival time of 7 months.2–5 SCLC is a high-grade neuroendocrine tumor frequently associated with paraneoplastic syndromes, eg hypercalcemia or Cushing syndrome, with a strong link with tobacco consumption as the major associated risk factor;6 in fact, SCLC prevalence demonstrated to be similar to smoking prevalence in the last 40 years, and only 2% of SCLC cases are diagnosed in never-smokers (defined as never-smoking or <100 cigarettes in the whole lifetime).7,8
SCLC is defined to be limited stage (LS-SCLC) whether the malignancy can be encompassed within a reasonable radiation field, while extensive stage SCLC (ES-SCLC) is defined for a malignancy greater than a single radiation area,9 and this staging system has an impact both on therapeutic options and patients’ prognosis.
From a genomic point of view, the vast majority of SCLC are associated to functional inactivation of tumor suppressor genes TP53 and RB1, which are crucial checkpoints in response to cell stress in inducing apoptosis and in the inhibition of S phase entry, respectively.6 Frequent genomic alterations found in SCLC patient affect MYC family members (MYC, MYCL and MYCN)10–12 and FGF receptors, as well as alterations in the NOTCH pathway,13,14 PTEN pathway,15,16 and in the cell cycle checkpoints kinases ATR, WEE1 and CHK1.17–20 Another frequent alteration found is the inactivating mutation of KMT2D (also known as MLL2), a histone modifier and chromatin remodeling agent, found mutated in 8% of SCLC patients.21 While genomic profiling did not highlight molecular distinct subtypes, more recently transcriptomic analysis and related epigenetic profiling suggested different SCLC subtypes.
In fact, basing on both human and murine models, different dominant transcriptional regulators of SCLC, which could uncover novel tumor susceptibilities based on cancer heterogeneity have been identified.22–24 In particular, four cancer subtypes have been identified, based on the expression of ASCL-1 (subtypes SCLC-A and SCLC-A2, depending on the high co-expression of HES1), NEUROD1 (subtype SCLC-N), both characterizing neuroendocrine tumors from an histological point of view, and POU2F3 (subtype SCLC-P) and YAP1 (subtype SCLC-Y) as less neuroendocrine subtypes.25,26 Moreover, it has been demonstrated that the different subtypes show heterogeneity and plasticity in relation to time and the treatment received, with a certain hierarchy of SCLC-A evolving to SCLC-N and then to SCLC-Y,26 representing the possible main evasion mechanism to treatment.27
Despite the identification of these subtypes, the treatment for SCLC remains the same for all patients. In the last three decades, the standard of care for ES-SCLC has consisted in the use of platinum-based agents (cisplatin or carboplatin) together with etoposide.6 While radiotherapy has been usually administered with a palliative intent in ES-SCLC patients, in the last years two different Phase III trials demonstrated that the addition of an anti PD-L1 agent (either atezolizumab or durvalumab) to the first-line chemotherapy prolong both progression-free survival (PFS) and overall survival (OS) of patients.28,29 The approximate doubling of 2-year survival (from 11% to 22%) suggests that a portion of SCLC patients have a durable benefit from immunotherapy treatment, while a consistent subset of patients show no substantial clinical benefit. These emerging points create the need for the identification of molecular biomarkers of response to treatment, usable by clinicians to perform a patient’s selection.
Several biomarkers have been hypothesized to be predictive of survival and response to immunotherapeutic treatment, but to date no clinical or biological parameters have been validated to be useful in clinical practice in guiding patient stratification.
The aim of this study was to identify factors associated with patient survival through an extensive molecular characterization performed by the FoundationOne next-generation sequencing panel on the tumor tissue before the start of a chemo-immunotherapy or a treatment with chemotherapy alone.
Materials and Methods
Patients
This is an observational study on patients with ES-SCLC treated between 2011 and 2020 at the Oncology Departments of the Area Vasta Romagna catchment area, Italy. The main inclusion criteria were the diagnosis of ES-SCLC, >18 years old and the receiving of a cisplatin or carboplatin-etoposide based therapy, or a chemotherapy regimen with the addition of PD-L1 inhibitor atezolizumab as the first-line therapy. For each patient, clinical information was retrospectively collected through medical charts review. The most tumor representative histologic formalin-fixed paraffin-embedded block was selected, and an expert pathologist was required to select a tumor area containing at least 70% of malignant cells by hematoxylin-eosin staining. Ten tissue slides of 10 µM each were cut and sent for molecular analysis.
A total of 99 patients satisfied the inclusion criteria. However, 18 patients had inadequate FFPE material. Of the remaining 81 patients, 2 patients were excluded due to missing follow-up information. Thus, 79 patients were finally analysed (Figure 1). Among the 79 eligible patients, 42 (53.2%) received chemotherapy alone and 37 (46.8%) chemo-immunotherapy as a first-line therapy; most of the patients included in our study (67 patients, 84.8%) had an ECOG ≤1 (Table 1).
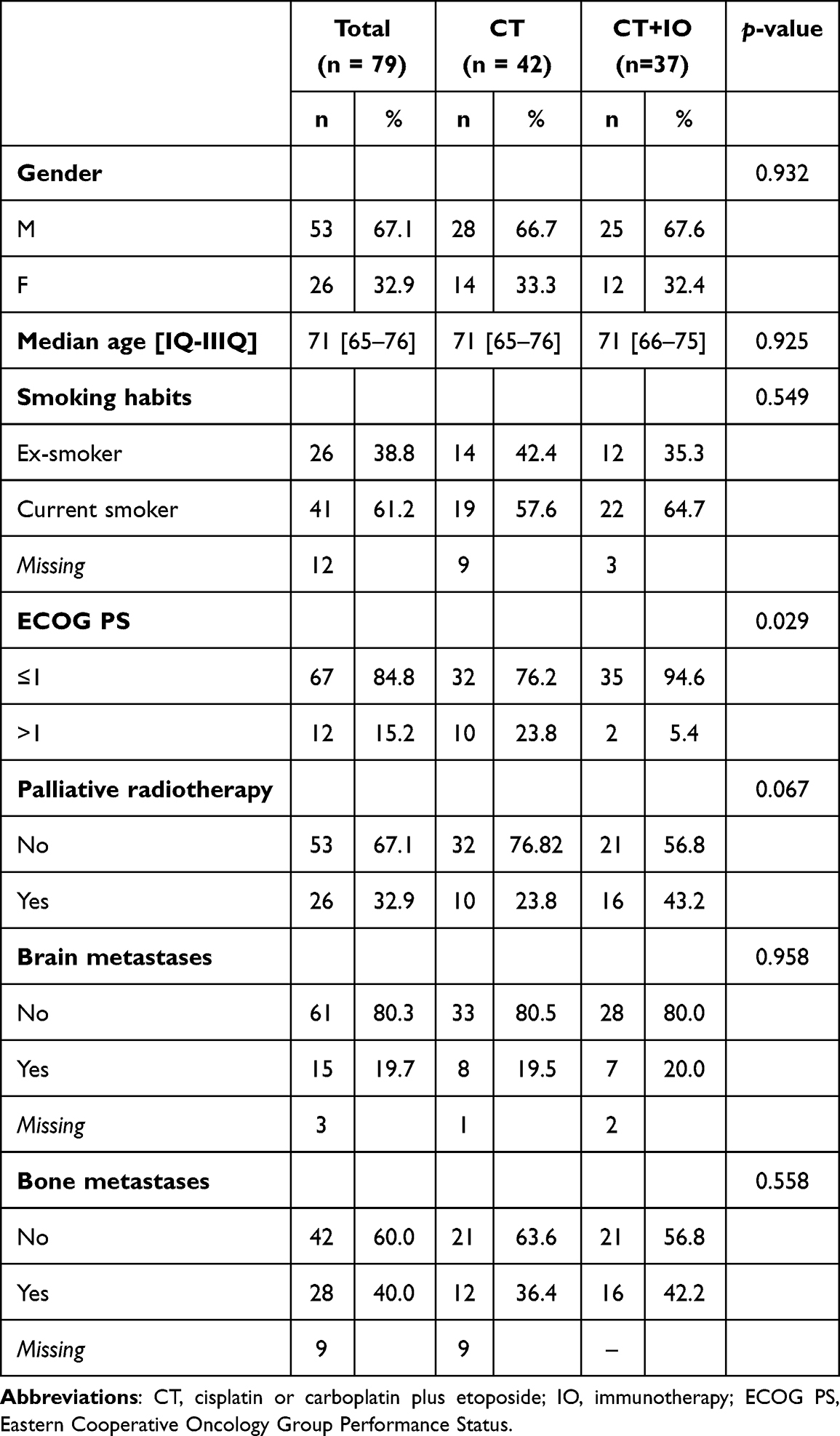 |
Table 1 Baseline Clinical and Pathological Features of Patients (n = 79) |
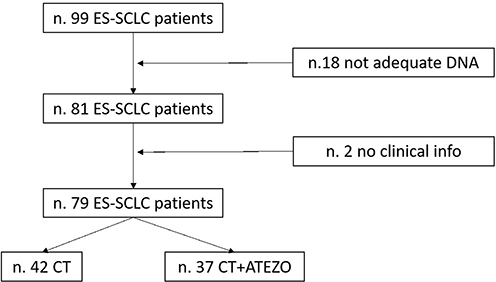 |
Figure 1 Flow-chart of patients included in the study. Abbreviations: ES-SCLC, Extensive Stage Small-Cell Lung Cancer; CT, cisplatin or carboplatin plus etoposide; Atezo, atezolizumab. |
The study was approved by the Romagna Ethics Committee (CEROM), No. IRSTB128, Prot. 516/2021, I.5/150. It was also conducted in accordance with the Declaration of Helsinki 1964 and later versions, and all patients signed the informed consent.
Sequencing Analysis
The samples were analysed using the next-generation sequencing Foundation One CDx panel, a clinically validated platform to detect substitutions, insertion and deletion alterations (indels), and copy number alterations (CNAs) in 324 genes. Moreover, selected gene fusions, as well as genomic signatures such as microsatellite instability (MSI) and tumor mutational burden (TMB) are also included.
Gene variants emerged by sequencing analyses were classified according to Foundation One annotation, and categorized in known pathogenic, likely pathogenic and variants of unknown significance, by predicted somatic status and functional impact. Then, unknown variants by Foundation One annotation were annotated with Varsome (v. 11.7.6), to perform a further selection of non-pathogenic alterations. Then, variants classified as known and likely pathogenic, or of unknown significance by the two consequent annotation systems, were considered for analyses.
TMB was classified (I) as a continuous variable, and using two different cut-offs, (II) at 10 mut/mB, and (III) at 16 mut/mB, as the most commonly referred to stratify patients who would likely benefit from immunotherapy.30–32
Statistical Analysis
Data were summarized by using median, first (IQ) and third (IIIQ) quartiles for continuous variables and natural frequencies and percentages for categorical ones.
Progression-free survival (PFS) was computed as the time in months from the start of first-line treatment to the date of disease progression or death from any cause, whichever occurred first, whereas the overall survival (OS) was computed as the time in months from the start of first-line treatment to the date of death from any cause. Patients alive without progression were censored at the date of the last follow-up contact. The median follow-up time was computed using the reverse Kaplan–Meier method whereas the survival curves were estimated using the Kaplan–Meier method, and comparisons were made using the Log rank test. Univariable and multivariable Cox regression models were employed to estimate hazard ratios (HR) and their corresponding 95% confidence intervals (CIs). For multivariate analyses, the decision about which factors to include into the models was not based exclusively on the results from univariate analyses but also on literature data and on the correlation among the available variables.
Results were considered statistically significant if the two-sided p-values were <0.05. Statistical analyses were conducted using STATA 15.0 (College Station, TX, USA).
Results
Association Between Clinical Information and Survival
The median PFS was 5.2 months (95% CI: 3.26–5.72) whereas the median OS was 7.5 months (95% CI 5.20–8.29) with a median follow-up time of 28.8 months (95% CI: 22.3 - Not reached - NR).
In our sample, there was no evidence of an association, at univariate level, between survival (both PFS or OS) and gender, age, smoking status, and presence of brain metastases whereas patients with a higher performance status showed a shorter survival as compared with patients with lower values (HRPFS = 2.98, 95% CI: 1.58–5.65, p = 0.001; HROS = 3.20, 95% CI: 1.68–6.10, p <0.001) as well as those reporting bone metastases at diagnosis (HRPFS = 1.77, 95% CI: 1.06–2.97, p = 0.029; HROS = 1.75, 95% CI: 1.05–2.93, p = 0.032), Supplementary Table 1. Patients treated with the addition of atezolizumab to carboplatin-etoposide had a significantly longer PFS and OS as compared with patients receiving chemotherapy alone. In particular, patients treated with chemo-immunotherapy reported a median PFS of 6.9 months (95% CI: 4.77–8.52) as compared with 2.8 months (95% CI: 2.37–5.23) observed for patients treated with chemotherapy alone (HRPFS of CT+IO vs CT alone = 0.52, 95% CI: 0.33–0.83, p = 0.007). The median OS for patients treated with CT alone was 9.4 months (95% CI: 6.38–17.50), while median OS for patients treated with CT+IO was 5.2 months (95% CI: 3.29–7.53), with a HROS of CT+IO vs CT alone = 0.50, 95% CI: 0.31–0.80, p = 0.004), Figure 2. When combined in multivariate analyses, ECOG PS, type of treatment received, and the presence of bone metastases resulted to be the main factors associated with both PFS and OS, Supplementary Table 1.
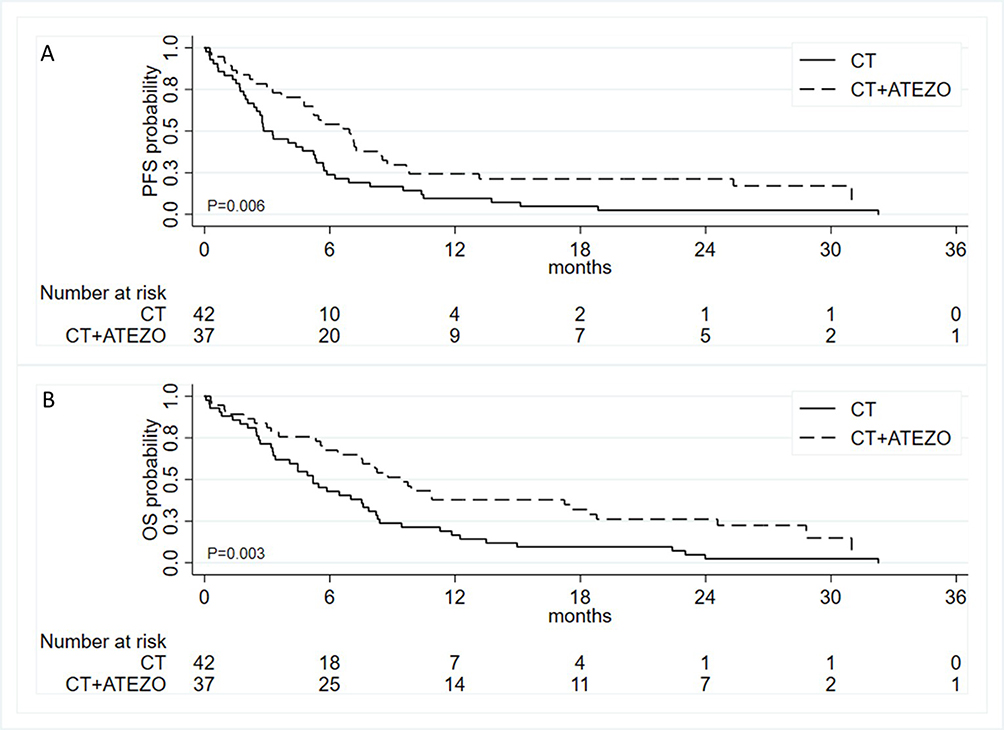 |
Figure 2 Kaplan–Meier curves for progression-free survival (A) and overall survival (B) by type of treatment. Abbreviations: CT, cisplatin or carboplatin plus etoposide; Atezo, atezolizumab. |
Sequencing results
Overall, the most frequently mutated genes were TP53 (78/79 patients, 99%) and RB1 (62/79 patients, 78%), with missense mutations as the most represented alterations. PTEN showed an alteration in 18/79 patients (23%) and, in particular, it was deleted in 7/79 (8.9%) patients. KMTD2, also known as MLL2, was found altered in 16 patients (20%). Other common mutations were those affecting SOX2 (11/79, 14% of patients), NKX2-1 (12/79, 15% of patients), CDKN2A (8/79, 10% of patients) and RICTOR (8/79, 10% of patients). Genes frequently altered in SCLC, such as CDKN2A, RICTOR, ARID1A and FGFR1 were found to be altered in 10%, 10%, 8% and 8%, respectively. The most frequently altered genes (mutation frequency higher than 5%) are displayed in Figure 3.
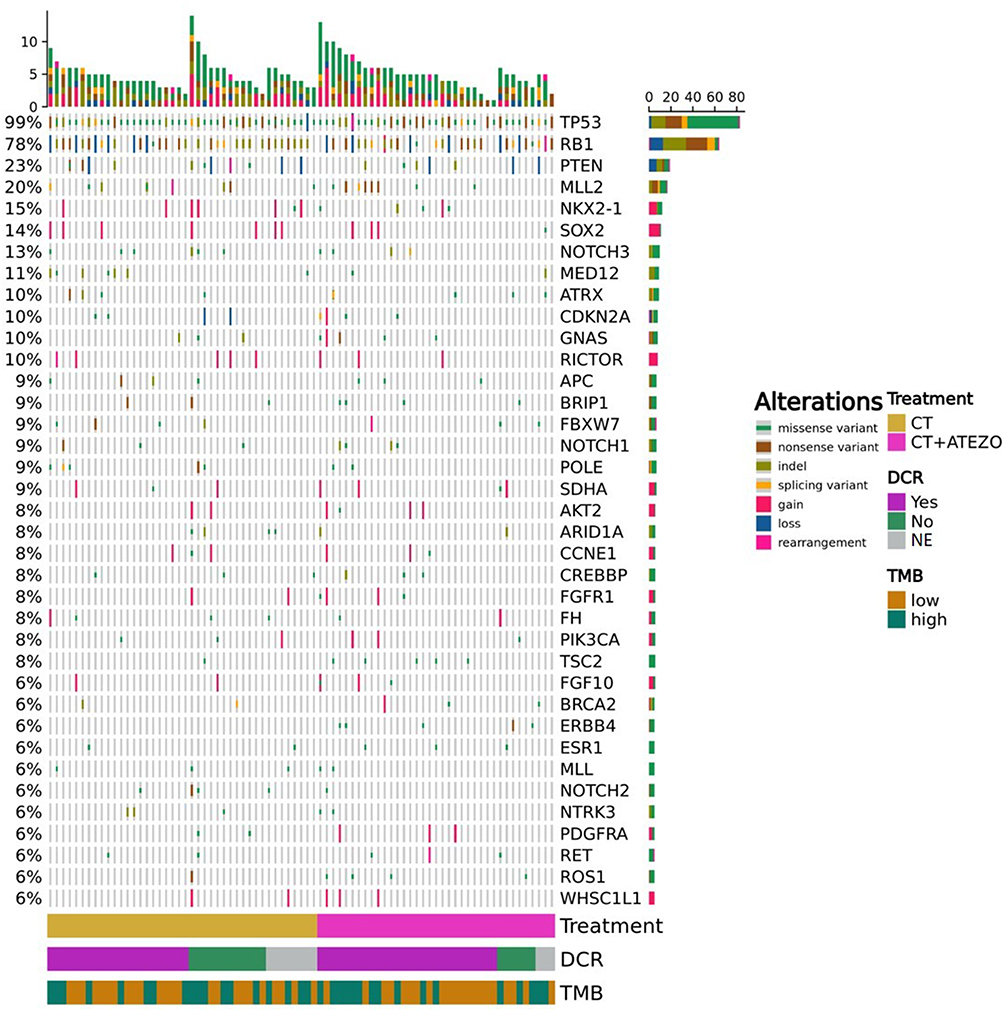 |
Figure 3 Oncoprint of the most frequently altered genes in the overall samples, with the indication of type of mutation, first-line treatment and response, and tumor mutation burden using the 10 mut/Mb. Abbreviations: CT, cisplatin or carboplatin plus etoposide; Atezo, atezolizumab; DCR, Disease Control Rate; NE, Not Evaluable. |
Overall, the median TMB was 8.8 mut/Mb [IQ-IIIQ 6.0–12.6]. Considering the TMB cut-off of 10 mut/Mb 34 patients (43.0%) had a high TMB while considering the cut-off of 16 mut/Mb only 11 patients (13.9%) were defined to have a high TMB (Table 2).
 |
Table 2 Tumor Mutation Burden (TMB) Distribution |
Molecular Determinants of Patient Survival
Association Between Gene Alterations and Survival
Overall, only MLL2 alterations were associated with both longer PFS (HRPFS = 0.51, 95% CI: 0.28–0.94, p = 0.032), and OS (HROS = 0.52, 95% CI: 0.28–0.97, p = 0.041), Figure 4. MLL2 alterations were not associated with other clinical characteristics, results not shown.
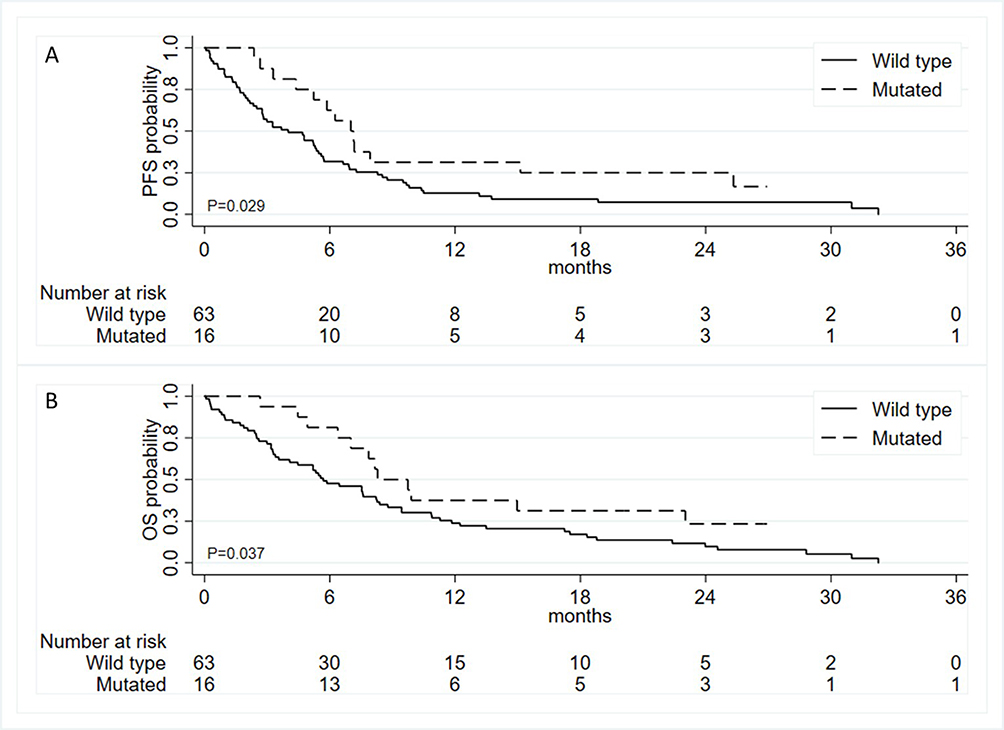 |
Figure 4 Kaplan–Meier curves for progression-free survival (A) and overall survival (B) by MLL2 mutational status. |
Association Between Molecular Signatures and Survival
In the overall case series, microsatellite instability (MSI) status was available for 70 patients (88.6%); it resulted in undetermined by Foundation One analyses for 9 patients (11.4%). All patients except one (98.7%) were classified as MSI stable patients, while the only patient classified as MSI unstable also has a really high TMB (35.3 mut/Mb).
At univariate analyses, TMB was not associated with both PFS and OS, Table 3 – column “Univariate analyses”. When the type of treatment was considered, including also an interaction term between TMB and treatment, we found some evidence for a differential effect of TMB on PFS by type of treatment received. In particular, appropriately combining and exponentiating the coefficients from Model 3 in the top of Table 3, it results that the effect of TMB, as a continuous variable, among patients treated with chemotherapy alone was equal to an HRPFS of 1.81 (95% CI: 0.99–3.31) whereas that for those treated with chemo-immunotherapy was equal to an HRPFS of 0.84 (95% CI: 0.56–1.26), with a p-value for the interaction of 0.039. Similar results were obtained when using TMB as a dichotomous variable based on the two different cut-offs of 10 mut/Mb and of 16 mut/Mb (see Model 1 and 2 in the top of Table 3). With regard to OS, we obtain to some extent similar results as for PFS but without reaching the statistical significance. Indeed, in this case, the HRs for TMB are, respectively, 1.55 (95% CI: 0.87–2.78) and 0.89 (95% CI: 0.57–1.40), with a p-value for the interaction term of 0.139 (Model 3 in the bottom of Table 3). Supplementary Table 2 shows the results of additional analyses adjusting for gender, age, ECOG PS, and presence of bone metastases. Overall, most of the results were consistent with those reported in Table 3, especially for the PFS. Indeed, as from model 6 of Table S2, the effect of TMB on PFS among patients treated with chemotherapy alone resulted in a HR 1.88 (95% CI: 0.97–3.67) whereas HR for those treated with chemo-immunotherapy was 0.82 (95% CI: 0.53–1.30), with a p-value for the interaction of 0.048. With regard to the OS, after the adjustment, we did not observe an association with the TMB and the clinical endpoint.
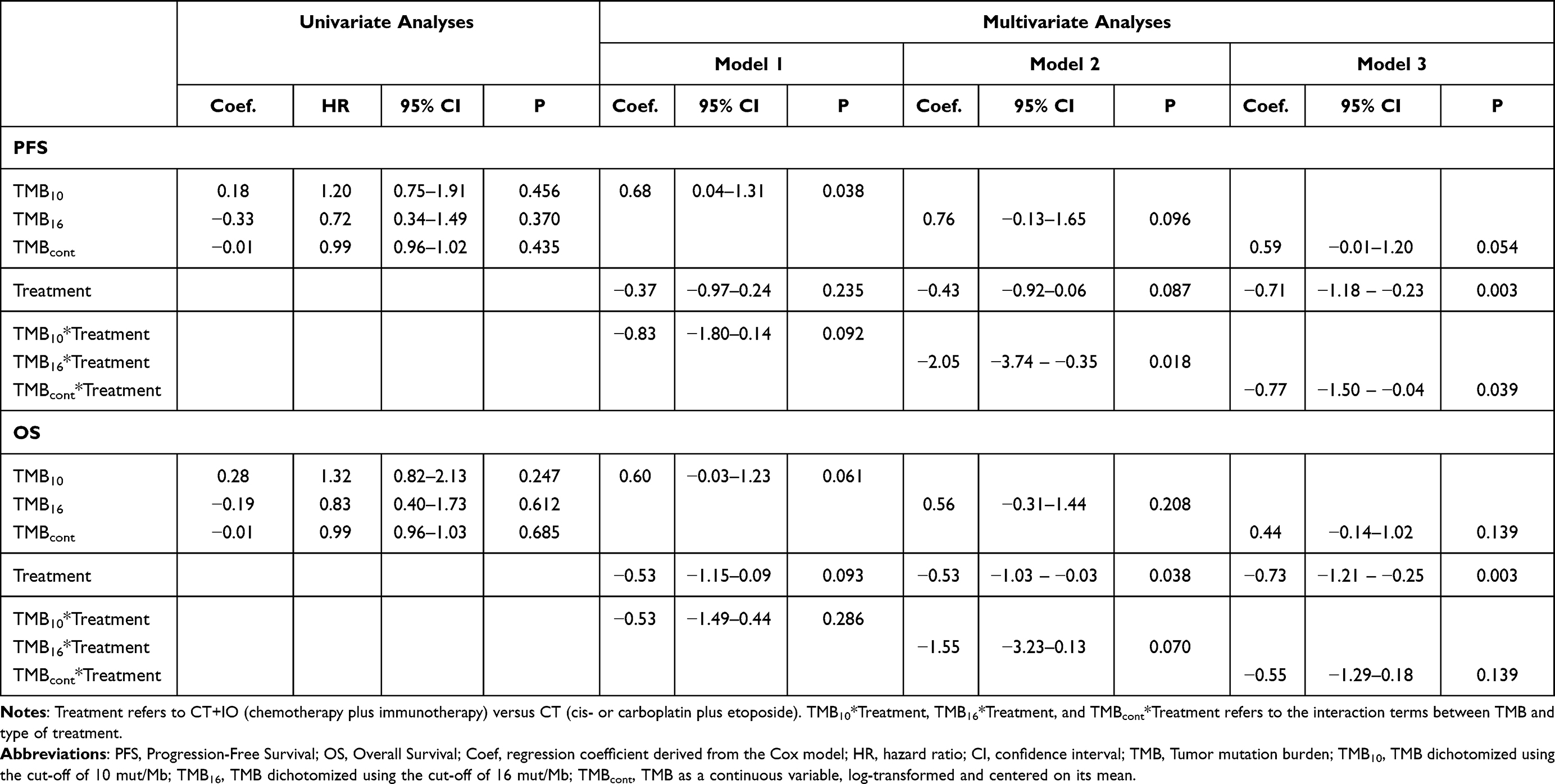 |
Table 3 Results from Univariable and Multivariable Cox Regression Models |
Considering TMB with the two different cut-offs in PFS and OS analyses, we found that a cut-off of 10 mut/Mb was associated with worse PFS in patients treated with chemotherapy alone (p = 0.046), with a trend in OS (p = 0.057). Considering the cut-off of 16 mut/Mb, patients treated with chemotherapy plus immunotherapy had a slight better PFS with respect to patients treated with chemotherapy alone (p = 0.064), Supplementary Figure 1.
Discussion
ES-SCLC accounts for the 65% of new SCLC diagnoses, and a 5-years OS less than 5% establishes ES-SCLC as one of the most lethal malignancies worldwide.33 The addition of immunotherapy to standard platinum-based plus etoposide regimens demonstrated a survival benefit for ES-SCLC patients in the IMPOWER133 and CASPIAN trials,28,34 finally shedding a light on a long-lasting clinical management algorithm. On the other hand, median OS in the IMPOWER133 and CASPIAN updates were 12.3 months and 13.0 months for intention-to-treat populations, respectively, with respect to 10.3 months in both studies for the control group,29,35,36 confirming ES-SCLC as a highly lethal malignancy, and creating the need to new biomarkers for better patient stratification.
In this study, we evaluated genetic features of an ES-SCLC patient cohort, half treated with standard chemotherapy, and half treated with the addition of anti-PD-L1 atezolizumab to standard schedule, to assess whether a mutational profile or genetic pattern could be a predictor of survival to an immunotherapy-based treatment. In our patients, the addition of atezolizumab to standard chemotherapy was associated to both longer PFS and OS, as observed in IMPOWER133 and CASPIAN prospective studies.28,34
The results obtained in our retrospective case series reflect those from the work by Sivakumar et al, who performed an integrative molecular analysis of the real-world repository of SCLC by Foundation Medicine Inc,37 even though we recorded slightly higher mutation rates in our case series, possibly for the inclusion of only ES-SCLC in our study. In fact, sequencing analyses of patients’ tumor tissue reflected the known molecular profile of SCLC, confirming TP53 and RB1 as the most frequently altered genes, found mutated in 99% and 78% of patients, respectively. These tumor suppressor genes are commonly inactivated in SCLC, and they are also involved in lung cancer cell plasticity, as the loss of TP53 and RB1 could guide the transition to SCLC as an acquired resistance mechanism to EGFR-tyrosine kinase inhibitors in EGFR-mutated NSCLC patients.38–42 PTEN was also found inactivated at high frequency in our case series. The loss of this tumor suppressor is another common event in SCLC carcinogenesis, concurring in loss of heterozygosity in lung cancer.43 Moreover, a recent study by Zhang et al identified PTEN loss as a driver of lineage plasticity, and transcriptional heterogeneity of SCLC in TP53 and RB1 in vivo models, underlining the evidence that PTEN loss occurs spontaneously and it is kept selected during SCLC evolution.15,44 Interestingly, in all except one patient, a PI3KCA alteration was found co-occurring with a SOX2 mutation, underlining the cross-interaction between these two oncogenes in SCLC.45 Moreover, considering together the mutations affecting PTEN, PI3KCA, AKT2 and RICTOR, we identified that almost half of patients carried at least one gene alteration in the PI3K pathway, in a general mutually exclusive fashion.
In our case series, we also evaluated DNA mutational signatures, ie microsatellite instability status and TMB. As expected, almost all patients were classified as microsatellite stable, as already highlighted by several reports; notably, the only patient with MSI had the highest TMB in the whole case series.37,46,47 In recent years, the hypothesis that a higher TMB could predict better response to immunotherapy has been tested in different malignancies, based on the rationale that neo-antigens generated by cancer-specific mutations could be recognized by the immune system.48,49 Actually, a higher TMB has been associated with prolonged OS in patients with different cancer histologies treated with immune checkpoint inhibitors, and on the basis of the results from the KEYNOTE-158, the Food and Drug Administration (FDA) approved the anti-PD 1 pembrolizumab for solid tumors with high TMB (>10 mut/Mb) by the Foundation One CDx assay.50,51 On the other hand, TMB predictive value was demonstrated only for a portion of patients in other studies, also depending on cancer histology, making it difficult to establish a single TMB cut-off for different cancers; moreover, stochastic errors and harmonization still need to be addressed.52,53 For this, TMB value as a predictive marker for cancer immunotherapy has been questioned. Same observations emerged in SCLC, in which the role of TMB in predicting response to immunotherapy remains controversial, as the blood-based test in the IMPOWER133 did not find an association between TMB and response, while the Checkmate-032 did.28,54 In this study, we considered TMB (I) as a continuous variable, and (II) using two different cut-offs at 10 mut/mB and 16 mut/mB. In our case series, median TMB was relatively low (8 mut/Mb), and we found a non-significant higher probability of prolonged PFS and OS for patients treated with chemo-immunotherapy, but not for those treated with only chemotherapy. A similar trend in OS was observed using a cut-off of 13 mut/mB in Checkmate-451, which tested the clinical efficacy of nivolumab plus ipilimumab as a maintenance therapy.55 In Checkmate-032, Hellman et al performed cut-off analysis as used in Checkmate-026, defining patients with low TMB (0 to less than 100 mutations), medium TMB (100–242 mutations), and high TMB (243 or more mutations);56 the authors found a predictive value for the higher tertile in predicting response to nivolumab plus ipilimumab as a first-line therapy.57 Taken together, these data suggest that TMB has a role in predicting response to immunotherapy and survival, but harmonization and data from prospective cohorts are needed to assess the real potential use of this biomarker in clinical practice.
In the last years, great interest in SCLC has been focused on transcriptomic profiles and methylation patterns for the identification of clinically relevant SCLC subtypes.24,58 Alterations in chromatin modifiers is a common event in SCLC, and it has also been related to drug sensitivity.59,60 In our case series, we found high mutation frequency in the MLL2 gene, a key regulator of transcriptional enhancer function by lysine 4 (K4) of histone H3 mono-methylation,61 and gene alterations affecting MLL2 were associated with better PFS and OS. Interestingly, worse prognosis was reported for MLL2-mutated NSCLC patients, but not for SCLC patients.62 By the sequencing of 29 SCLC exomes, 2 genomes and 15 transcriptomes, Peifer et al found a high frequency of alterations in epigenetic machinery, especially in CREBBP, EP300 and MLL genes, all encoding for histones modifiers.63 While Augert et al found a high frequency of nonsense/truncating mutations in MLL2, to our knowledge, this is the first study highlighting different responses to therapy and survivals for patients with mutations in genes involved in the epigenetic machinery. Due to the small number of patients in the two treatment groups, we were not able to highlight a different response to chemotherapy or chemo-immunotherapy of patients carrying MLL2 mutations, but further investigations in this direction are warranted. In fact, the role of therapeutic inhibition of epigenetic agents is still unclear,64 but our data suggest that peculiar chromatin dynamic states could play a role in response to therapy.
This study had some limitations. First, due to the retrospective nature of the study, only a limited number of clinical information with some missing data. Second, it was a single-area experience with a limited sample size, especially critical in the identification of the associations between rare genomic factors and the survival endpoints. Thus, all results should be verified by future prospective studies including also centers outside the Area Vasta Romagna and with a larger sample size and longer follow-up, especially for the overall survival endpoint.
Conclusions
Our results show that molecular features of patients with ES-SCLC are able to predict patients’ survival. We confirmed the role of TMB in relation to treatment, as a higher TMB was associated with better survival in patients treated with CT+IO, with respect to patients treated with CT alone. In relation to this, we found a role for TMB also whether used as a continuous variable, confirming that a clinically useful cut-off is a demanding challenge. Moreover, we demonstrated the role of altered epigenetic machinery genes in association with patients’ survival. As these results have been achieved in a small cohort of patients, once confirmed in larger case series, our results could be useful in identifying which molecular determinants could help in guiding clinicians in ES-SCLC patients’ treatment stratification.
Acknowledgments
This work was partly supported thanks to the contribution of Ricerca Corrente by the Italian Ministry of Health within the research line ”Appropriateness, outcomes, drug value and organizational models for the continuity of diagnostic-therapeutic pathways in oncology”.
This work was partly supported thanks to the contribution of Roche Italy, which had no role in study design, data collection, data analysis, data interpretation, or writing the report.
The authors acknowledge Dr. Fabrizio Citarella for significant contribution to the present study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funding has been received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Ortega-Franco A, Ackermann C, Paz-Ares L, Califano R. First-line immune checkpoint inhibitors for extensive stage small-cell lung cancer: clinical developments and future directions. ESMO open. 2021;6(1):100003. doi:10.1016/j.esmoop.2020.100003
3. Früh M, De Ruysscher D, Popat S, et al. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol off J Eur Soc Med Oncol. 2013;24(Suppl 6):vi99–105. doi:10.1093/annonc/mdt178
4. Wang S, Tang J, Sun T, et al. Survival changes in patients with small cell lung cancer and disparities between different sexes, socioeconomic statuses and ages. Sci Rep. 2017;7(1):1339. doi:10.1038/s41598-017-01571-0
5. Zheng Z, Zhu D, Liu L, et al. Survival of small-cell lung cancer patients after surgery: a single-center retrospective cohort study. J Investig Med off Publ Am Fed Clin Res. 2023;71(8):917–928.
6. Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3. doi:10.1038/s41572-020-00235-0
7. Varghese AM, Zakowski MF, Yu HA, et al. Small-cell lung cancers in patients who never smoked cigarettes. J Thorac Oncol. 2014;9(6):892–896. doi:10.1097/JTO.0000000000000142
8. Huang R, Wei Y, Hung RJ, et al. Associated links among smoking, chronic obstructive pulmonary disease, and small cell lung cancer: a pooled analysis in the international lung cancer consortium. EBioMedicine. 2015;2(11):1677–1685. doi:10.1016/j.ebiom.2015.09.031
9. Stinchcombe TE, Gore EM. Limited-stage small cell lung cancer: current chemoradiotherapy treatment paradigms. Oncologist. 2010;15(2):187–195. doi:10.1634/theoncologist.2009-0298
10. Little CD, Nau MM, Carney DN, Gazdar AF, Minna JD. Amplification and expression of the c-myc oncogene in human lung cancer cell lines. Nature. 1983;306(5939):194–196. doi:10.1038/306194a0
11. Nau MM, Carney DN, Battey J, et al. Amplification, expression and rearrangement of c-myc and N-myc oncogenes in human lung cancer. Curr Top Microbiol Immunol. 1984;113:172–177. doi:10.1007/978-3-642-69860-6_29
12. Nau MM, Brooks BJ, Battey J, et al. L-myc, a new myc-related gene amplified and expressed in human small cell lung cancer. Nature. 1985;318(6041):69–73. doi:10.1038/318069a0
13. Lim JS, Ibaseta A, Fischer MM, et al. Intratumoural heterogeneity generated by Notch signalling promotes small-cell lung cancer. Nature. 2017;545(7654):360–364. doi:10.1038/nature22323
14. Augert A, Eastwood E, Ibrahim AH, et al. Targeting NOTCH activation in small cell lung cancer through LSD1 inhibition. Sci Signal. 2019;12(567). doi:10.1126/scisignal.aau2922
15. McFadden DG, Papagiannakopoulos T, Taylor-Weiner A, et al. Genetic and clonal dissection of murine small cell lung carcinoma progression by genome sequencing. Cell. 2014;156(6):1298–1311. doi:10.1016/j.cell.2014.02.031
16. Cui M, Augert A, Rongione M, et al. PTEN is a potent suppressor of small cell lung cancer. mol Cancer Res. 2014;12(5):654–659. doi:10.1158/1541-7786.MCR-13-0554
17. Mollaoglu G, Guthrie MR, Böhm S, et al. MYC drives progression of small cell lung cancer to a variant neuroendocrine subtype with vulnerability to aurora kinase inhibition. Cancer Cell. 2017;31(2):270–285. doi:10.1016/j.ccell.2016.12.005
18. Doerr F, George J, Schmitt A, et al. Targeting a non-oncogene addiction to the ATR/CHK1 axis for the treatment of small cell lung cancer. Sci Rep. 2017;7(1):15511. doi:10.1038/s41598-017-15840-5
19. Sen T, Tong P, Stewart CA, et al. CHK1 inhibition in small-cell lung cancer produces single-agent activity in biomarker-defined disease subsets and combination activity with cisplatin or olaparib. Cancer Res. 2017;77(14):3870–3884. doi:10.1158/0008-5472.CAN-16-3409
20. Sen T, Tong P, Diao L, et al. Targeting AXL and mTOR pathway overcomes primary and acquired resistance to WEE1 inhibition in small-cell lung cancer. Clin Cancer Res. 2017;23(20):6239–6253. doi:10.1158/1078-0432.CCR-17-1284
21. Augert A, Zhang Q, Bates B, et al. Small cell lung cancer exhibits frequent inactivating mutations in the histone methyltransferase KMT2D/MLL2: CALGB 151111 (Alliance). J Thorac Oncol. 2017;12(4):704–713. doi:10.1016/j.jtho.2016.12.011
22. Meuwissen R, Linn SC, Linnoila RI, Zevenhoven J, Mooi WJ, Berns A. Induction of small cell lung cancer by somatic inactivation of both Trp53 and Rb1 in a conditional mouse model. Cancer Cell. 2003;4(3):181–189. doi:10.1016/S1535-6108(03)00220-4
23. Gazdar AF, Savage TK, Johnson JE, et al. The comparative pathology of genetically engineered mouse models for neuroendocrine carcinomas of the lung. J Thorac Oncol. 2015;10(4):553–564. doi:10.1097/JTO.0000000000000459
24. Gay CM, Stewart CA, Park EM, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell. 2021;39(3):346–360.e7. doi:10.1016/j.ccell.2020.12.014
25. Wooten DJ, Groves SM, Tyson DR, et al. Systems-level network modeling of Small Cell Lung Cancer subtypes identifies master regulators and destabilizers. PLoS Comput Biol. 2019;15(10):e1007343. doi:10.1371/journal.pcbi.1007343
26. Rudin CM, Poirier JT, Byers LA, et al. Molecular subtypes of small cell lung cancer: a synthesis of human and mouse model data. Nat Rev Cancer. 2019;19(5):289–297. doi:10.1038/s41568-019-0133-9
27. Stewart CA, Gay CM, Xi Y, et al. Single-cell analyses reveal increased intratumoral heterogeneity after the onset of therapy resistance in small-cell lung cancer. Nat Cancer. 2020;1(4):423–436. doi:10.1038/s43018-019-0020-z
28. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
29. Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, Phase 3 trial. Lancet. 2019;394(10212):1929–1939. doi:10.1016/S0140-6736(19)32222-6
30. Hellmann MD, Ciuleanu T-E, Pluzanski A, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med. 2018;378(22):2093–2104. doi:10.1056/NEJMoa1801946
31. Klempner SJ, Fabrizio D, Bane S, et al. Tumor mutational burden as a predictive biomarker for response to immune checkpoint inhibitors: a review of current evidence. Oncologist. 2020;25(1):e147–59. doi:10.1634/theoncologist.2019-0244
32. Friedman CF, Hainsworth JD, Kurzrock R, et al. Atezolizumab treatment of tumors with high tumor mutational burden from mypathway, a multicenter, open-label, phase IIa multiple basket study. Cancer Discov. 2022;12(3):654–669. doi:10.1158/2159-8290.CD-21-0450
33. Yang S, Zhang Z, Wang Q. Emerging therapies for small cell lung cancer. J Hematol Oncol. 2019;12(1):47. doi:10.1186/s13045-019-0736-3
34. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
35. Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619–630. doi:10.1200/JCO.20.01055
36. Zugazagoitia J, Paz-Ares L. Extensive-stage small-cell lung cancer: first-line and second-line treatment options. J Clin Oncol off J Am Soc Clin Oncol. 2022;40(6):671–680. doi:10.1200/JCO.21.01881
37. Sivakumar S, Moore JA, Montesion M, et al. Integrative analysis of a large real-world cohort of small cell lung cancer identifies distinct genetic subtypes and insights into histologic transformation. Cancer Discov. 2023;13(7):1572–1591. doi:10.1158/2159-8290.CD-22-0620
38. George J, Lim JS, Jang SJ, et al. Comprehensive genomic profiles of small cell lung cancer. Nature. 2015;524(7563):47–53. doi:10.1038/nature14664
39. Niederst MJ, Sequist LV, Poirier JT, et al. RB loss in resistant EGFR mutant lung adenocarcinomas that transform to small-cell lung cancer. Nat Commun. 2015;6(1):6377. doi:10.1038/ncomms7377
40. Popat S. Histologically Transformed SCLC from EGFR-Mutant NSCLC: understanding the Wolf in Sheep’s Clothing. J Thorac Oncol. 2019;14(10):1689–1691. doi:10.1016/j.jtho.2019.07.010
41. Offin M, Chan JM, Tenet M, et al. Concurrent RB1 and TP53 alterations define a subset of EGFR-mutant lung cancers at risk for histologic transformation and inferior clinical outcomes. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2019;14(10):1784–1793.
42. Liu Y, Li Z, Meng Q, et al. Identification of the consistently differential expressed hub mRNAs and proteins in lung adenocarcinoma and construction of the prognostic signature: a multidimensional analysis. Int J Surg. 2024;110(2):1052–1067. doi:10.1097/JS9.0000000000000943
43. Specker BL, Valanis B, Hertzberg V, Edwards N, Tsang RC. Sunshine exposure and serum 25-hydroxyvitamin D concentrations in exclusively breast-fed infants. J Pediatr. 1985;107(3):372–376. doi:10.1016/S0022-3476(85)80509-6
44. Zhang L, Liu C, Zhang B, et al. PTEN loss expands the histopathologic diversity and lineage plasticity of lung cancers initiated by Rb1/Trp53 Deletion. J Thorac Oncol. 2023;18(3):324–338. doi:10.1016/j.jtho.2022.11.019
45. Schaefer T, Lengerke C. SOX2 protein biochemistry in stemness, reprogramming, and cancer: the PI3K/AKT/SOX2 axis and beyond. Oncogene. 2020;39(2):278–292. doi:10.1038/s41388-019-0997-x
46. Ouyang W, Yu J, Zeng Z, Gong J, Zhang J, Xie C. Genomic profiling of relapsed small cell lung cancer reveals potential pathways of therapeutic targets. J Thorac Dis. 2023;15(12):6796–6805. doi:10.21037/jtd-23-1657
47. Yang S-R, Gedvilaite E, Ptashkin R, et al. Microsatellite instability and mismatch repair deficiency define a distinct subset of lung cancers characterized by smoking exposure, high tumor mutational burden, and recurrent somatic MLH1 inactivation. J Thorac Oncol. 2024;19(3):409–424. doi:10.1016/j.jtho.2023.10.004
48. McGranahan N, Furness AJS, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science. 2016;351(6280):1463–1469. doi:10.1126/science.aaf1490
49. Jardim DL, Goodman A, de Melo Gagliato D, Kurzrock R. The challenges of tumor mutational burden as an immunotherapy biomarker. Cancer Cell. 2021;39(2):154–173. doi:10.1016/j.ccell.2020.10.001
50. Strickler JH, Hanks BA, Khasraw M. Tumor mutational burden as a predictor of immunotherapy response: is more always better? Clin Cancer Res. 2021;27(5):1236–1241. doi:10.1158/1078-0432.CCR-20-3054
51. Samstein RM, Lee C-H, Shoushtari AN, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet. 2019;51(2):202–206. doi:10.1038/s41588-018-0312-8
52. Chan TA, Yarchoan M, Jaffee E, et al. Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann Oncol off J Eur Soc Med Oncol. 2019;30(1):44–56. doi:10.1093/annonc/mdy495
53. Yarchoan M, Hopkins A, Jaffee EM. Tumor mutational burden and response rate to PD-1 Inhibition. N Engl J Med. 2017;377(25):2500–2501. doi:10.1056/NEJMc1713444
54. Hellmann MD, Callahan MK, Awad MM, et al. Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell. 2019;35(2):329. doi:10.1016/j.ccell.2019.01.011
55. Owonikoko TK, Park K, Govindan R, et al. Nivolumab and ipilimumab as maintenance therapy in extensive-disease small-cell lung cancer: checkMate 451. J Clin Oncol. 2021;39(12):1349–1359. doi:10.1200/JCO.20.02212
56. Carbone DP, Reck M, Paz-Ares L, et al. First-line nivolumab in stage IV or recurrent non-small-cell lung cancer. N Engl J Med. 2017;376(25):2415–2426. doi:10.1056/NEJMoa1613493
57. Hellmann MD, Callahan MK, Awad MM, et al. Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell. 2018;33(5):853–861.e4. doi:10.1016/j.ccell.2018.04.001
58. Heeke S, Gay CM, Estecio MR, et al. Tumor- and circulating-free DNA methylation identifies clinically relevant small cell lung cancer subtypes. Cancer Cell. 2024;42(2):225–237.e5. doi:10.1016/j.ccell.2024.01.001
59. Mohammad HP, Smitheman KN, Kamat CD, et al. A DNA hypomethylation signature predicts antitumor activity of LSD1 inhibitors in SCLC. Cancer Cell. 2015;28(1):57–69. doi:10.1016/j.ccell.2015.06.002
60. Gardner EE, Lok BH, Schneeberger VE, et al. Chemosensitive relapse in small cell lung cancer proceeds through an EZH2-SLFN11 Axis. Cancer Cell. 2017;31(2):286–299. doi:10.1016/j.ccell.2017.01.006
61. Shechter D, Dormann HL, Allis CD, Hake SB. Extraction, purification and analysis of histones. Nat Protoc. 2007;2(6):1445–1457. doi:10.1038/nprot.2007.202
62. Ardeshir-Larijani F, Bhateja P, Lipka MB, Sharma N, Fu P, Dowlati A. KMT2D mutation is associated with poor prognosis in non-small-cell lung cancer. Clin Lung Cancer. 2018;19(4):e489–501. doi:10.1016/j.cllc.2018.03.005
63. Peifer M, Fernández-Cuesta L, Sos ML, et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat Genet. 2012;44(10):1104–1110. doi:10.1038/ng.2396
64. Denninghoff V, Russo A, de Miguel-Pérez D, et al. Small cell lung cancer: state of the art of the molecular and genetic landscape and novel perspective. Cancers. 2021;13(7):1723. doi:10.3390/cancers13071723
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
EPAS1/HIF-2α Acts as an Unanticipated Tumor-Suppressive Role in Papillary Thyroid Carcinoma
Zhang R, Zhao J, Zhao L
International Journal of General Medicine 2023, 16:2165-2174
Published Date: 31 May 2023
Extensive-Stage Small-Cell Lung Cancer: Current Landscape and Future Prospects
Saida Y, Watanabe S, Kikuchi T
OncoTargets and Therapy 2023, 16:657-671
Published Date: 2 August 2023
The Synergistic Mechanisms and Prospects of Transarterial Chemoembolization Combined with Immunotherapy for Hepatocellular Carcinoma
Chen QF, Chen S, Zhao M
Journal of Hepatocellular Carcinoma 2025, 12:841-854
Published Date: 30 April 2025
Emerging Predictive Biomarkers of Immunotherapy Sensitivity in Patients with Non-Small Cell Lung Cancer
Gariazzo E, Colamartini F, Ubaldi M, Santo V, Brunetti L, Tomarelli C, Ognissanti D, Nassar J, Costabile S, Romano L, De Vita E, Scorpiniti I, Macrì M, Porreca R, Currà MF, Cortellini A, Ricciuti B, Metro G
ImmunoTargets and Therapy 2026, 15:567238
Published Date: 2 February 2026
Increased Expression of HLA-DR and CD69 on Peripheral CD4+ T Cells Predicts Better Clinical Outcomes in Cutaneous Melanoma
Tomás A, Maximino J, Nunes H, Salvador R, Luís R, Brito C, Saraiva DP, Gouveia E, Pereira C, Gonçalves F, Farricha V, Lopez Carvalho E, Moura C, Passos MJ, Cristóvão-Ferreira S, Pereira PM, Cabral MG, Pojo M
ImmunoTargets and Therapy 2026, 15:606640
Published Date: 22 July 2026