Back to Journals » ImmunoTargets and Therapy » Volume 15
Emerging Predictive Biomarkers of Immunotherapy Sensitivity in Patients with Non-Small Cell Lung Cancer
Authors Gariazzo E ![]() , Colamartini F, Ubaldi M, Santo V, Brunetti L, Tomarelli C, Ognissanti D
, Colamartini F, Ubaldi M, Santo V, Brunetti L, Tomarelli C, Ognissanti D ![]() , Nassar J, Costabile S, Romano L, De Vita E, Scorpiniti I, Macrì M
, Nassar J, Costabile S, Romano L, De Vita E, Scorpiniti I, Macrì M ![]() , Porreca R, Currà MF, Cortellini A, Ricciuti B, Metro G
, Porreca R, Currà MF, Cortellini A, Ricciuti B, Metro G
Received 16 September 2025
Accepted for publication 24 January 2026
Published 2 February 2026 Volume 2026:15 567238
DOI https://doi.org/10.2147/ITT.S567238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Eleonora Gariazzo,1,2,* Francesca Colamartini,1,* Martina Ubaldi,1 Valentina Santo,2– 4 Leonardo Brunetti,3– 5 Chiara Tomarelli,1 Daniele Ognissanti,1 Jouana Nassar,1 Silvia Costabile,1 Luca Romano,1 Emanuela De Vita,1 Ilenia Scorpiniti,1 Miriam Macrì,1 Roberta Porreca,6 Maria Francesca Currà,6 Alessio Cortellini,3– 5 Biagio Ricciuti,2 Giulio Metro1
1Medical Oncology, Santa Maria Della Misericordia Hospital, University of Perugia, Perugia, Italy; 2Lowe Center for Thoracic Oncology, Dana Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; 3Operative Research Unit of Medical Oncology, Fondazione Policlinico Universitario Campus Bio-Medico, Rome, Italy; 4Department of Medicine and Surgery, Università Campus Bio-Medico, Rome, Italy; 5Department of Surgery and Cancer, Hammersmith Hospital Campus, Imperial College London, London, UK; 6Medical Oncology, Santa Maria della Misericordia Hospital, Perugia, Italy
*These authors contributed equally to this work
Correspondence: Eleonora Gariazzo, Medical Oncology, Santa Maria della Misericordia Hospital, University of Perugia, Perugia, Italy, Email [email protected]
Abstract: In recent years, the therapeutic landscape of non-small cell lung cancer (NSCLC) has been transformed by immune checkpoint inhibitors (ICIs), which have led - in some patients - to unprecedented survival expectancy. Nevertheless, identifying patients most likely to benefit from ICI remains a major challenge. While PD-L1 expression and tumor mutation burden (TMB) represent established predictive biomarkers, their predictive ability still needs to be improved, which underscores the need for identifying additional (bio)markers for treatment selection. Recent research has highlighted multiple emerging biomarkers, including genomic alterations (eg, KEAP1, STK11, SMARCA4), markers of metabolic pathway dysregulation (IDO, adenosine axis), tumor-infiltrating lymphocytes, and blood-based biomarkers (eg soluble markers of inflammation, germline HLA diversity, and circulating tumor DNA). Host-related determinants, such as the history of tobacco exposure and the body mass index, further contribute to immunotherapy outcomes. In addition, artificial intelligence (AI) and machine learning (ML) approaches are enabling integration of multidimensional data, leading to predictive scoring systems which have outperformed conventional biomarkers in certain settings. This review synthesizes current evidence on established and emerging predictive biomarkers in NSCLC, highlighting the potential of combining biological, host, and computational features to inform precision immunotherapy strategies.
Keywords: NSCLC, immunotherapy, predictive biomarkers, tumor microenvironment, host factors, artificial intelligence
Introduction
In recent years, a deeper understanding of the molecular mechanisms driving carcinogenesis and immune escape has led to the development of novel therapeutic agents, resulting in unprecedented survival outcomes for patients with non-small cell lung cancer (NSCLC).1 The current therapeutic landscape relies on two principal strategies: targeted therapies for patients harboring actionable genomic alterations (AGAs) and immune checkpoint inhibitors (ICIs), with or without chemotherapy, for those without AGAs.2 ICIs mediate tumor cells killing by reactivating T cells and restoring the antitumor immune response. In particular, ICIs currently used in clinical practice are monoclonal antibodies that disrupt immune checkpoints (eg, PD-1/PD-L1 and CTLA-4/CD80-86), thereby enhancing the host immune response against cancer. Although many patients derive significant clinical benefit from immunotherapy, virtually all eventually develop resistance, either primary or acquired. While multiple therapeutic strategies are being explored to overcome this challenge, the identification of robust predictive biomarkers to inform treatment selection remains a critical unmet need.
This review introduces established biomarkers used to predict ICI efficacy in NSCLC - namely programmed death-ligand 1 (PD-L1) expression and tumor mutation burden (TMB) – and explores other emerging, promising (bio)markers. To improve clarity, we grouped the emerging predictors of immunotherapy sensitivity discussed in this review into three broad, non-mutually-exclusive categories:
- Tissue-based biomarkers, which rely on adequate tumor sampling and include genomic alterations, tumor microenvironment (TME) characteristics, markers of immunosuppressive metabolic pathways, alternative immune checkpoints, and tumor HLA class I diversity evaluated from tissue;
- Soluble biomarkers, which represent minimally invasive tools and have the potential to overcome the limitations of repeated biopsies. These include inflammatory markers, liquid biopsy—especially circulating tumor DNA (ctDNA)—and germline-derived HLA diversity assessed through peripheral blood;
- Host-related factors, such as tobacco use history, sex, and body mass index (BMI), which have shown associations with ICI outcomes.
Finally, we will discuss how artificial intelligence (AI) may contribute to integrating multiple (bio)markers types and play a role in shaping personalized treatment strategies for NSCLC.
Established Predictors of Immunotherapy Response: PD-L1 and TMB
At present, two biomarkers — PD-L1 and TMB — represent the cornerstone for treatment decision-making in NSCLC without AGAs.3 Both biomarkers have been extensively studied so far, and are widely accepted for informed clinical decision regarding sensitivity to ICI-based therapies.
Importantly, PD-L1 expression early emerged as a key predictive biomarker for ICI-based therapy in NSCLC.4 Assessment of the levels of PD-L1 expression on tumor tissue is performed by immunohistochemistry (IHC) using assays like Dako 22C3 and Ventana SP263 or SP142, with results reported as the percentage of cancer cells with membrane staining of any intensity (tumor proportion score, TPS), or, specifically for SP142, as the percentage of positive PD-L1 expression either on tumor cells or tumor-infiltrating immune cells.4,5
For the selection of patients more likely to benefit from anti–PD-(L)1 monotherapy, a PD-L1 TPS ≥50% has emerged as the most reliable threshold. The pivotal KEYNOTE-024, IMpower110, and EMPOWER-Lung 1 trials demonstrated superior survival of pembrolizumab, atezolizumab, and cemiplimab, respectively, compared with platinum-based chemotherapy in untreated advanced NSCLC with PD-L1 TPS ≥50%,6–8 with 5-year survival reaching approximately 30% with pembrolizumab and cemiplimab versus 15% with chemotherapy.9,10 Furthermore, data from a large real-world cohort indicated that the addition of chemotherapy to anti–PD-(L)1 therapy in this population did not improve progression-free survival (PFS) or overall survival (OS), supporting the preferential use of ICI monotherapy in patients with PD-L1 TPS ≥50%.11 Conversely, the addition of chemotherapy to immunotherapy remains the standard approach for patients with PD-L1 <50%.3
Despite its predictive value, PD-L1 is an imperfect biomarker for several reasons, which are summarized in Table 1. First, PD-L1 expression is quantitative, meaning that it should be interpreted as a continuous variable. Retrospective analyses indicate that, even within the broad PD-L1 categories of ≥50% and <50%, finer thresholds can identify subgroups with different sensitivity to ICI-based therapies.12 Relying solely on the 50% threshold may limit treatment personalization, potentially overlooking patients who derive minimal benefit from immunotherapy (eg, PD-L1<1%) and who might be candidates for treatment escalation, such as the addition of a CTLA-4 inhibitor.13,14
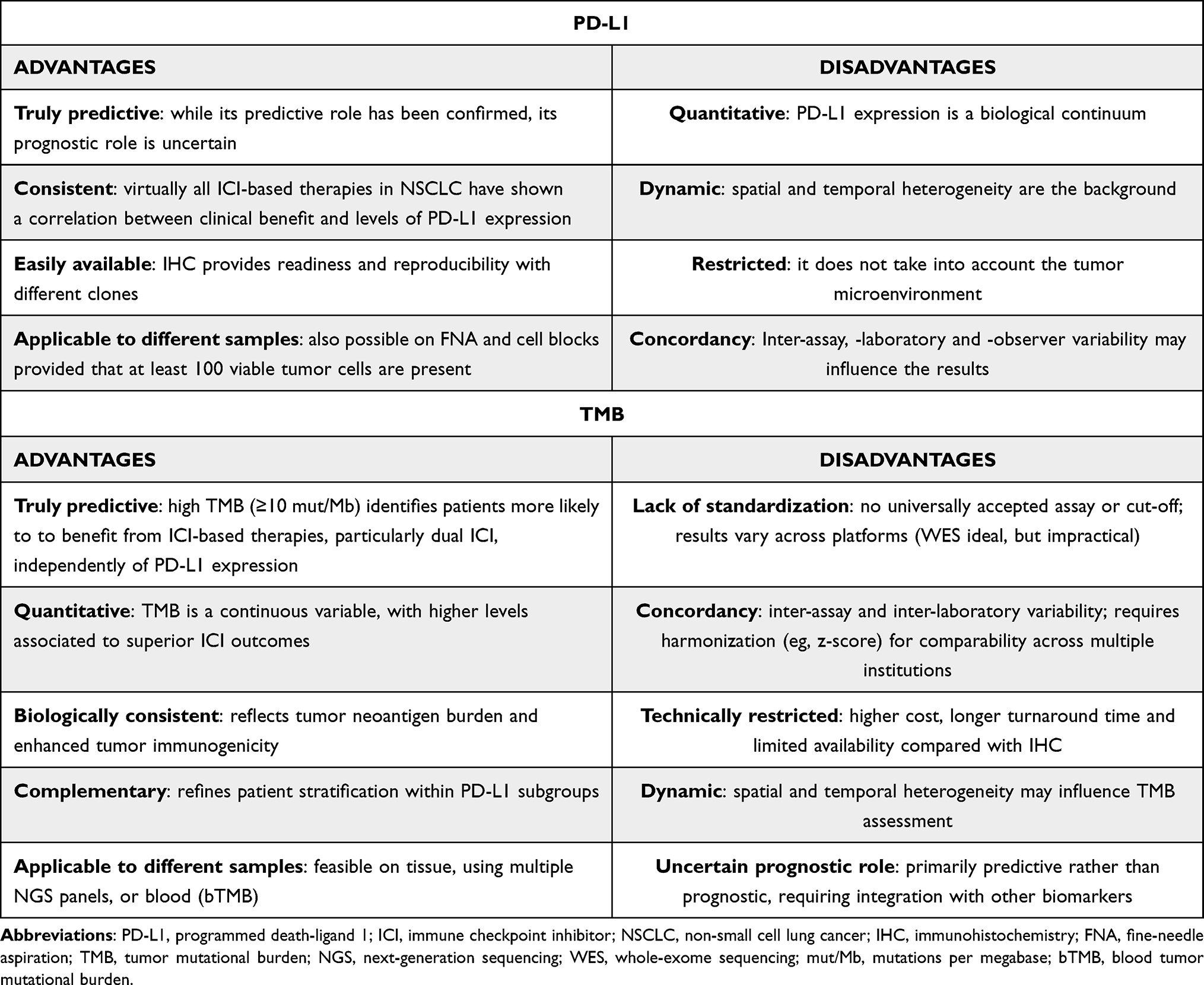 |
Table 1 Advantages and Disadvantages of PD-L1 and TMB Biomarkers |
Second, PD-L1 expression has spatial and temporal heterogeneity, as it may be significantly influenced based on the site that has been biopsied and on the moment of its measurement.15
Finally, inter-assay and inter-observer variability may further complicate its reliability and reproducibility.16,17
The limitations of PD-L1 do not eliminate its central role, rather underscore the urgent need to integrate it with additional biomarkers.
TMB represents the total number of somatic non-synonimous mutations per megabase (mut/Mb) in the cancer genome. The underlying rationale for using TMB as a predictive biomarker for immunotherapy is that a higher mutational load increases the likelihood of generating neoantigens, which may, in turn, render tumors more immunogenic and susceptible to immune attack.
Initially, a cut-off of 10 mut/Mb as assessed by FoundationOne CDx was set in order to select patients who could benefit from the use of dual anti-PD-1/CTLA-4 blockade with nivolumab plus ipilimumab18 Subsequently the CheckMate 227 trial confirmed that high TMB patients (≥10 mut/Mb) derived greater benefit from dual ICI blockade regardless of PD-L1 expression, thus suggesting that PD-L1 and TMB may act as different, though complementary, biomarkers of benefit from ICI-based therapies.19
Nevertheless, despite these promising findings, the adoption of TMB in routine practice has proven difficult (Table 1). That is mainly due to the lack of universally accepted assays or cut-off values. Although whole-exome sequencing (WES) technique offers the most comprehensive evaluation, it is not feasible for widespread clinical use. Therefore, more practical targeted next-generation sequencing (NGS) panels have become available (eg FoundationOne CDx), but owing to their cost and variable results, comparisons across studies and Institutions are slightly complex.20 To bypass the above-mentioned issue, standardization methods have been proposed. Vokes et al used standardization to z-score for comparing TMB distribution across different platforms. In doing so, they were able to identify a different cut-off of sensitivity to ICI-based therapies in terms of mut/Mb for each of the platform that was taken into account.21 By using the same methodology, they were also able to hypothesize that patients with TMB greater or equal to the 90th percentile were those with the utmost benefit from treatment with ICI-based regimens.22,23
To conclude, the available data underscore the complexity of immune responsiveness in relation to TMB levels, and support the integration of both TMB and PD-L1 into multifactorial or composite (bio)markers. Such models are currently under investigation and may provide a more nuanced prediction of treatment outcomes in the near future.24
Emerging Tissue Biomarkers: From Research to Clinical Application
Beyond PD-L1 and TMB, several techniques are either being employed or under investigation to further characterize NSCLC and predict its sensitivity to different ICI-based regimens, many of which still rely on the availability of tumor tissue obtained through histological sampling. Tissue-based biomarkers are depicted in Figure 1.
 |
Figure 1 Tissue-based biomarkers for immune checkpoint inhibitor response in non–small cell lung cancer. Overview of regulatory-approved and emerging tissue-derived biomarkers, including PD-L1 expression, tumor mutational burden, tumor immune microenvironment features, HLA class I diversity, and tumor genomic alterations. |
Genomic Profiling
Routine comprehensive tumor genomic profiling has paved the way for the inclusion of multiple genomic factors – beyond AGAs - into the therapeutic stratification of NSCLC. Among these, mutations in KEAP1 and STK11, now recognized as robust biomarkers of resistance to PD-(L)1 blockade, are increasingly used to refine prognostic assessment in NSCLC.23,25–27 Interestingly, loss-of-function mutations in these genes appear to adversely affect immunotherapy outcomes especially in the context of a concurrent KRAS mutation. Tumors harboring KRAS/STK11 or KRAS/KEAP1 co-mutations exhibit distinctive immune landscapes, characterized by unique gene expression signatures and altered patterns of immune cell infiltration.26 In particular, transcriptomic analyses revealed a marked downregulation of key immune pathways—including MHC class II complex, T-cell activation, immune response signaling, leukocyte migration and degranulation, and myeloid cell activation—in patients harboring concurrent KRAS and STK11/KEAP1 mutations, even when compared with KRAS-mutant/STK11-KEAP1 wild-type NSCLC. These co-mutant tumors also displayed reduced infiltration of CD8+ T cells and B cells. Notably, Skoulidis et al demonstrated that the addition of CTLA-4 inhibition can overcome KEAP1/STK11-associated resistance to PD-(L)1 blockade, offering a potential strategy to improve outcomes in this challenging patient population.28
Beyond KEAP1 and STK11, other genomic alterations can also shape the immune landscape of KRAS-mutant NSCLC. One notable example is the SWItch/Sucrose Nonfermentable (SWI/SNF) chromatin-remodeling complex, whose disruption has been linked to unfavorable immunotherapy outcomes. Within this family of genes, SMARCA4 has emerged as the most impactful determinant of ICI resistance, with loss-of-function mutations consistently associated with diminished therapeutic benefit.29
The network of genomic determinants influencing ICI response further extends to tumor suppressors involved in signaling regulation. In this regard, PTEN plays a pivotal role: loss-of-function mutations in this gene dysregulate the PI3K/AKT signaling cascade and promote infiltration by regulatory T cells (Tregs), thereby impairing tumor sensitivity to immune checkpoint inhibition.30 In contrast, activating mutations in the MAPK pathway have been associated with increased sensitivity to dual ICI therapy in squamous NSCLC, highlighting the importance of broad genomic profiling even in this histology, where NGS is often underutilized.31
Another gene gaining increasing interest in predicting ICI outcomes is DNMT3A. Somatic loss-of-function mutations in DNMT3A are found across several cancer types, including up to 4–5% of NSCLC, and are associated with a distinct immunophenotype characterized by upregulated PD-1 and IFNγ signatures and an immune-enriched TME.32–35 Ricciuti et al demonstrated that DNMT3A mutations are significantly enriched among responders to immunotherapy, correlating with improved objective response rates as well as longer PFS and OS.35 These findings highlight DNMT3A role not only as a predictive biomarker but also as a potential therapeutic target. Therefore, strategies aimed at modulating the activity or expression of DNMT3A may enhance NSCLC immunogenicity and improve ICI efficacy.
In addition to mutational events, copy number alterations (CNAs), defined as gains or losses of large chromosomal segments, have emerged as significant prognostic biomarkers. Several retrospective studies have demonstrated that high levels of CNAs correlate with poor outcomes to ICI in solid tumors, including NSCLC.36,37 Given that aneuploidy represents an extensive type of CNA, affecting larger regions of the cancer genome, its distinct prognostic significance in NSCLC has been the subject of further investigation. Retrospective analyses have shown that aneuploidy serves as an independent, robust biomarkers and is associated with immunosuppressive TME and reduced ICI efficacy in both locally advanced and metastatic NSCLC.38,39 A genomic region of particular interest is chromosome 9p. Han et al reported that homozygous deletion of 9p21 is associated with poor outcomes under anti–PD-L1 monotherapy, independently of PD-L1 expression and TMB. Notably, approximately half of 9p21.3 deletions also involve the type I interferon (IFN) gene cluster, thus suggesting a role for impaired IFN signaling in resistance to ICIs.40 Consistently, Ebot et al demonstrated that, among non-squamous NSCLC patients treated with single-agent immunotherapy, tumors harboring 9p21.3 deletions - intriguingly encompassing genes currently under active investigation such as CDKN2A, CDKN2B, and MTAP - were associated with worse survival compared with deletion-negative tumors. Interestingly, this negative association was not observed in patients receiving chemo-immunotherapy.41 Alessi et al further confirmed the role of chromosome 9p loss as an independent predictor of immunosuppressive TME and immunotherapy resistance.39
Biomarkers of Immunosuppressive Metabolic Pathways
Beyond genomic profiling, biomarkers of metabolic pathway dysregulation can provide insight into mechanisms sustaining an immunosuppressive TME. Among these, the tryptophan–kynurenine pathway, driven by indoleamine 2,3-dioxygenase 1 and 2 (IDO1/IDO2), represents a key tumor escape mechanism. IDO, expressed by cancer, immune, and stromal cells, catalyzes the degradation of tryptophan into immunosuppressive metabolites such as kynurenine.42,43 This activity—detectable by IHC or quantitative real-time PCR (qPCR)—depletes tryptophan and accumulates kynurenine, thereby promoting T-cell anergy and reducing active immune cell infiltration into the TME. In NSCLC, low tryptophan, high kynurenine and 3-hydroxykynurenine levels, and an elevated kynurenine/tryptophan (Kyn/Trp) ratio, which serves as a functional readout of IDO enzymatic activity and systemic immunosuppression, have been correlated with poor prognosis and primary resistance to ICIs.44–46Although IDO’s role as a prognostic and predictive biomarker is established, its therapeutic targeting remains controversial. Despite encouraging preclinical evidence, clinical trials with IDO1 inhibitors (eg, epacadostat) have failed to improve outcomes,47 though novel agents and combination strategies are under investigation.
Another metabolic pathway under active investigation for its role in shaping an immunosuppressive TME is the adenosine (ADO) axis. ADO is a neurotransmitter and extracellular metabolite with potent immunosuppressive properties. Within the TME, ADO inhibits dendritic cell, NK cell, and T-cell activity, while promoting Tregs recruitment. Its production is enhanced by cellular stress and tissue damage, which induce ATP release into the extracellular space, where it is sequentially converted to ADO via either the CD39–CD73 enzymatic pathway or the CD38–NAD⁺ catabolic pathway.48,49 At low levels, ADO may exert anti-tumor effects by limiting cell proliferation. However, high extracellular ADO levels, documented in several solid tumors including NSCLC, drive immune evasion, metastasis, and angiogenesis through the CD39–CD73–A2A receptor (A2AR) axis.50 Multiple biomarkers along this pathway are being evaluated. IHC studies report elevated CD73 expression in NSCLC as a marker of poor prognosis,51,52 while high A2AR expression has been associated with better outcomes.51 However, CD73 often correlates with PD-L1, and their co-expression may predict improved ICI responsiveness. In summary, CD73 may have a dual role: it reflects tumor aggressiveness as a negative prognostic factor, yet it may also serve as a positive predictive biomarker of immune response.53 Several agents targeting this pathway—via CD39, CD73, or ADO receptor blockade—are under clinical evaluation, both alone and in combination with ICIs.52,53
TME Immune Infiltration as a Predictive Biomarker
An additional research avenue on emerging biomarkers focuses on techniques that allow direct assessment of immune cell infiltration into the TME. The predominant immune cell population in the TME are TILs, which belong to both the adaptive and innate arms of the immune system.54 Previous studies have showed TILs positive impact on the clinical course of multiple cancer types, including NSCLC.55,56 Subsequent analyses have reinforced the prognostic value of this biomarker and highlighted its predictive role in patients treated with ICI-based regimens.54,57
Despite their promising characteristics, the use of TILs in clinical practice remains controversial, primarily due to several limitations that can affect accurate assessment using standard methods, which rely on semiquantitative evaluation of H&E-stained slides and suffer from low reproducibility.58 Consequently, there is growing interest in AI-based computational pathology. Notably, Rakaee et al demonstrated that AI-based assessment of TILs in NSCLC is a reliable tool; in patients with PD-L1–negative NSCLC, digitally assessed TILs were even superior to TMB in predicting response to ICIs.57
However, all available data on TME assessment suggest that single markers are insufficient to capture such a complex entity. Consequently, multiplexed imaging strategies are gaining increasing interest, although their application remains largely confined to the research setting, mainly due to the equipment high costs.59 Multiplex immunohistochemistry (mIHC), which enables the simultaneous detection of multiple markers on a single formalin-fixed paraffin-embedded (FFPE) tissue section while preserving spatial context, has already shown a predictive value in patients treated with ICIs;60,61 however, the impossibility to test more than 3–5 markers per slide is a significant limit. Multiplex immunofluorescence (mIF) builds on this approach by leveraging fluorescent dyes, which offer greater multiplexing capacity and quantitative signal detection. Especially in combination with transcriptomic data, mIF has shown the potential to predict the response to ICI across several cancer types, including NSCLC.22,62,63
Other Immune Checkpoints
There is growing evidence that PD-1 and CTLA4 are not the only immune checkpoints influencing the anti-tumor immune response, although they remain the only ones targeted by clinically approved agents in NSCLC. Other receptors expressed on immune cells can contribute to T-cell exhaustion and predict resistance to ICIs. In this context, LAG-3, TIM-3, and TIGIT have attracted particular interest, both as biomarkers and as potential therapeutic targets.64 Chronic IFN-y signaling – which is often observed in NSCLC patients – may upregulate the expression of these inhibitory receptors on T cells, thereby fostering an immunosuppressive TME. Preclinical models have demonstrated that blockade of these inhibitor receptors can restore T-cell proliferation and enhance their antitumor activity. Following the positive results of the RELATIVITY-047 trial, the anti-LAG3 monoclonal antibody relatlimab has been approved, in combination with nivolumab, for metastatic melanoma.65 However, results with these antibodies in advanced NSCLChave been inconsistent.66–70 Specifically, the RELATIVITY-104 trial, which tested the addition of relatlimab to the first-line standard-of -care in NSCLC, did not demonstrate a statistically significant improvement PFS, while OS data remain immature. Similarly, the addition of the anti-TIGIT antibody tiragolumab to first-line atezolizumab showed encouraging activity in the Phase II CITYSCAPE trial, conducted in untreated patients with PD-L1–positive NSCLC. In contrast, the Phase III SKYSCRAPER-01 trial, which assessed the same combination in patients with PD-L1 ≥50%, failed to meet its endpoints for both PFS and OS. Consequently, none of these agents has yet received regulatory approval for the treatment of of metastatic NSCLC. This underscores the need to validate biomarkers capable of identifying patients most likely to benefit from immune checkpoint blockade, as well as to define which ligand–receptor interactions are most critical for their immunosuppressive effects, particularly given the ongoing development of bispecific antibodies (eg, anti-PD-1/TIGIT, PD-1/LAG-3, PD-1/TIM-3) that will require careful clinical integration. These agents are designed to achieve synchronous, localized, and coordinated inhibition of both receptors on the same T cell, thereby enhancing anti-tumor activity compared with conventional co-administration of separate antibodies. Importantly, they are engineered with reduced Fc functionality, in order to minimize Fc-mediated antibody-dependent cellular cytotoxicity and antibody-dependent cellular phagocytosis that could otherwise lead to unselective depletion of TIGIT-expressing immune cells.71–74
Emerging Soluble Biomarkers
Due to the limitations of tissue-based biomarkers—such as the need for invasive biopsies and the challenge of tumor heterogeneity—there is increasing interest in blood-derived biomarkers. An overview of tissue- and blood-based biomarkers discussed in this review is provided in Table 2. Blood-based biomarkers encompass both circulating tumor-derived components (eg, ctDNA) and soluble biomarkers.
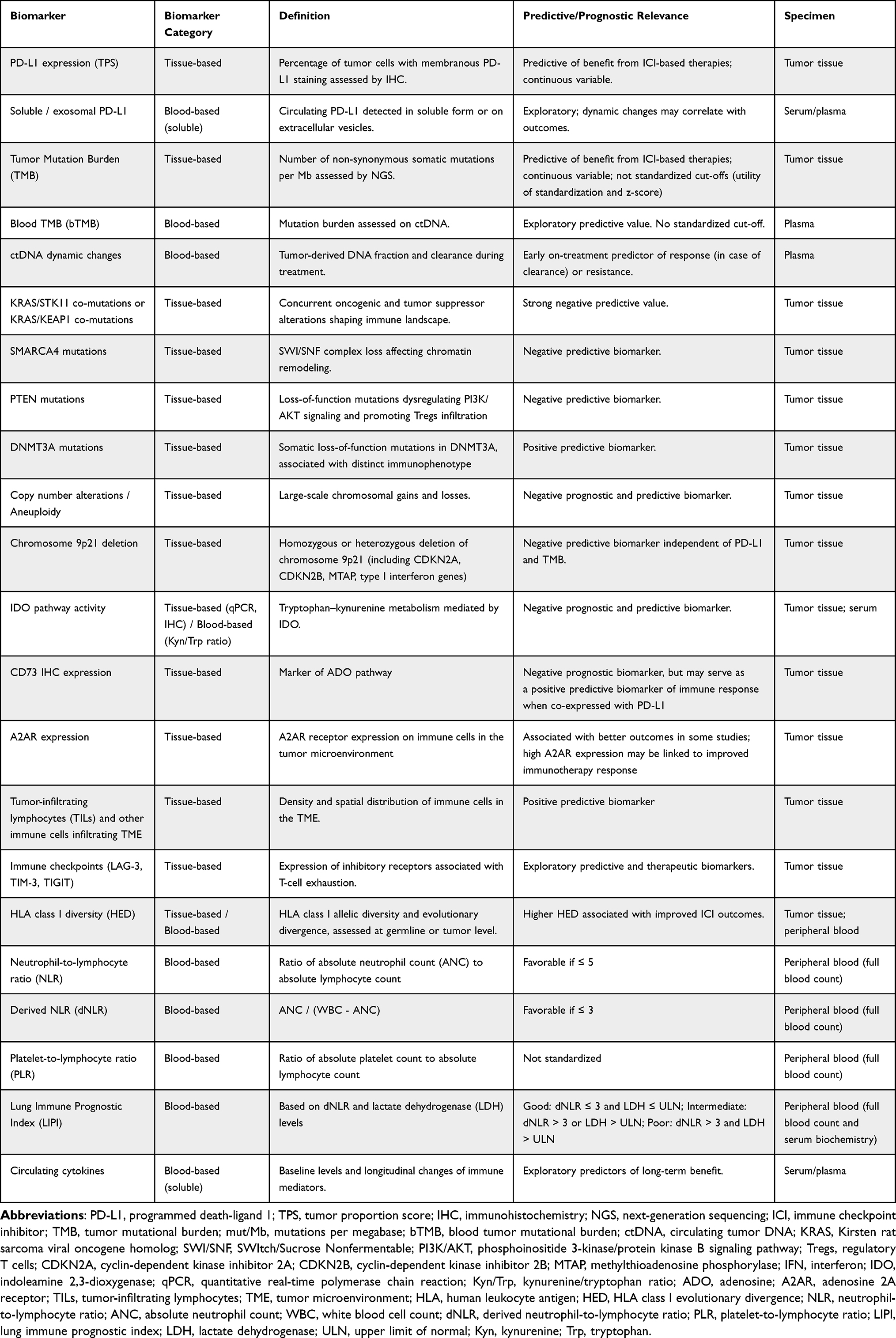 |
Table 2 Overview of Predictive and Prognostic Biomarkers for ICI Response in NSCLC |
Systemic Inflammation Scores as Prognostic Markers
Within this framework, markers of systemic inflammatory response have drawn particular attention, given the key role of inflammation in modulating the efficacy of systemic therapies, including ICIs. In NSCLC, several affordable and reproducible pretreatment blood-based biomarkers—such as the neutrophil-to-lymphocyte ratio (NLR), lactate dehydrogenase (LDH), platelet-lymphocyte ratio (PLR) and the lung immune prognostic index (LIPI) score—are routinely used to predict clinical outcomes, due to their accessibility.75–79
The prognostic relevance of these biomarkers is well established across multiple treatment modalities, including ICI-based regimens.76,80,81 The LIPI prognostic score in NSCLC has been further validated by a meta-analysis of more than 8,000 patients from 8 clinical studies, which consistently showed poorer survival outcomes in patients with higher LIPI scores, regardless of treatment modality.82 In fact, the LIPI score integrates dNLR and LDH, reflecting systemic inflammation, immune activation and tumor burden. An elevated dNLR is associated with neutrophil-driven immunosuppression and relative lymphopenia, whereas LDH reflects tumor metabolism and hypoxia-related aggressiveness. Together, these parameters provide a biologically plausible explanation for the prognostic value of LIPI in immunotherapy-treated patients. Notably, the prognostic value of LIPI is not restricted to NSCLC: intermediate or poor pretreatment scores were also associated with worse outcomes in patients with extensive-stage SCLC treated with chemoimmunotherapy.83 Together, these findings highlight LIPI as a robust prognostic marker across both treatment modalities and lung cancer histologies.
A recent Chinese trial has sought to specifically explore the association between these biomarkers and immunotherapy outcomes.84 Among 202 patients treated with various immunotherapy agents, a «good» LIPI score was significantly associated with prolonged progression-free survival (PFS >24 months). Similarly, lower NLR values were observed in long-responder patients, reflecting a less inflammatory systemic profile. These findings support the hypothesis that reduced systemic inflammation may help preserve circulating lymphocytes and promote TILs, thereby enhancing anti-tumor immune responses. The authors suggested that integrating blood-based biomarkers with clinical characteristics (eg, number and location of metastases) and cytokine profiles could improve patient stratification and help identify those most likely to benefit from long-term immunotherapy.
Interestingly, not only baseline levels but also the evolution of these biomarkers during treatment has shown clinical relevance. An Italian retrospective study demonstrated that improvements in the LIPI score during treatment (eg, from intermediate to good) were associated with a higher likelihood of developing immune-related adverse events (irAEs), potentially reflecting enhanced immune activation79 and a more reactive immune system, with overlapping mechanisms between antitumor immunity and autoimmunity. Similarly, post-treatment deterioration of inflammatory markers—such as increases in NLR or worsening of the LIPI score—has been linked to poorer PFS and OS.85
Liquid Biopsy and ctDNA
Liquid biopsy (LB) is a non-invasive diagnostic tool used to isolate tumor-derived components from biological fluids, such as blood, urine, cerebrospinal fluid, and pleural effusions.86 It is easily reproducible, allowing for longitudinal monitoring and supporting an increasingly personalized approach. The concept of LB encompasses the analysis of circulating tumor cells (CTCs) as well as tumor-derived molecules, including circulating tumor DNA (ctDNA), circulating tumor RNA (ctRNA), microRNAs (miRNAs), and exosomes.
Among these, ctDNA stands out as a promising biomarker for ICIs in NSCLC, because it is highly specific and carries tumor genetic alterations, capturing tumor heterogeneity more effectively than a single tissue biopsy. Detection methods can be either targeted, via panels tailored to known mutations, or untargeted, via tumor-agnostic approaches employing high-throughput NGS to assess broader genomic alterations, including WES or whole-genome sequencing (WGS).87 A key limitation of ctDNA-based monitoring is that not all tumors are “shedders,” meaning that ctDNA may be undetectable in some patients. In this context, assessing the ctDNA tumor fraction—the percentage of ctDNA within the total cell-free DNA (cfDNA)—may help distinguish between truly negative results and non-informative ones. However, tumor fraction is not yet routinely applied in clinical practice, as defining optimal cutoffs, ensuring assay sensitivity, and addressing associated costs remain significant challenges.88 Nevertheless, ctDNA analysis has become an important clinical tool in NSCLC. Since 2016, the FDA has approved ctDNA testing for EGFR mutation detection, thereby establishing liquid biopsy as a standard method for molecular profiling when tissue is unavailable or insufficient. Multiple studies have demonstrated its high mutation-detection rate and its ability to reduce the time to treatment initiation.89,90 Moreover, ctDNA allows real-time monitoring of disease evolution. Decrease or clearance of ctDNA during treatment with ICIs (with or without chemotherapy) has been associated with improved outcomes.91,92 Therefore, ctDNA monitoring may hold a key application in metastatic NSCLCs when selecting which patients should escalate/de-escalate treatment during ICI or continue ICI longer than 2 years.93,94 Notably, a retrospective study by Besse et al suggested that ctDNA tumor fraction may predict early disease progression and help identify patients more likely to benefit from chemotherapy in addition to immunotherapy.95 Finally, ctDNA may serve in the early disease setting to predict who will experience pathological complete response after chemotherapy + ICI as neoadjuvant therapy or who will have improved prognosis on ICI monotherapy in the adjuvant setting, with the ultimate goal to adjust treatment based on whether ctDNA is detected or not after curative-intent therapy, either surgery or definitive chemoradiotherapy.96,97 Overall, ctDNA dynamics reflect tumor burden and disease biology, and early decreases or clearance during treatment are increasingly recognized as markers of effective immune-mediated tumor control. This supports a potential prognostic—and possibly predictive—role for ctDNA beyond static baseline measurements.
As a derivative of ctDNA, blood TMB (bTMB) can also be assessed; prior analyses suggest that bTMB may serve as an independent predictive marker of ICI efficacy. However, the role of its longitudinal assessment remains more controversial,98 because bTMB reflects only the fraction of tumor DNA released into the circulation and may be influenced by tumor burden and shedding dynamics.
Other Soluble Biomarkers
Circulating cytokines play diverse roles in immunomodulation, and their concentrations may help clinicians distinguish between good and poor immunotherapy responders. For example, peripheral blood samples from 19 metastatic NSCLC patients were collected before treatment and at 6 weeks after the start of immunotherapy. The study found that increasing CCL11 levels (which inhibit angiogenesis and induce eosinophil migration and activation) and decreasing IL-1Ra (an anti-inflammatory cytokine) and IL-17A (a cytokine which favors cancer cell invasion and resistance to anti-PD-1 therapy) levels were associated with long-term responders (PFS > 24 months). The kinetics of circulating cytokines, when combined with clinical features and other biomarkers, may help identify patients likely to benefit from prolonged treatment responses.84
Researchers are also increasingly interested in soluble PD-L1 (sPD-L1) and exosomal PD-L1 (exoPD-L1), as these can reduce antitumor efficacy. The prognostic role of these biomarkers remains debated: elevated levels generally correlate with worse PFS or OS, although, for example, increases in exoPD-L1 during treatment may indicate favorable outcomes.99,100 Collectively, these biomarkers offer practical advantages for risk stratification, early treatment monitoring, and the potential prediction of toxicity. However, despite growing interest, their routine implementation in clinical practice remains limited, as mechanistic evidence is still incomplete and current findings largely rely on retrospective data that require prospective validation.
HLA-I Heterozygosity and Evolutionary Divergence
CD8⁺ T cell–mediated cytotoxicity against cancer cells depends on efficient tumor antigen presentation by human leukocyte antigen (HLA) molecules. Based on this rationale, HLA class I heterozygosity and diversity have attracted interest as potential predictive biomarkers across multiple cancer types.101,102 Heterozygosity at HLA loci may result in greater allelic polymorphism, enabling the presentation of a broader repertoire of neoantigens compared with homozygosity. However, heterozygosity alone does not necessarily confer functional diversity, which may represent the actual driver of enhanced responsiveness to immune checkpoint inhibition. To address this limitation, Chowell et al proposed the concept of germline HLA-I evolutionary divergence (HED),103 a quantitative metric that captures the functional dissimilarity between the two alleles at each HLA-A, HLA-B, and HLA-C locus. HED is calculated using the Grantham distance104 between the peptide-binding domains of paired alleles, with higher HED values reflecting greater divergence in peptide-binding properties. From a biological standpoint, higher HED may enable the presentation of a more diverse set of tumor-derived antigens, thus broadening the repertoire of T-cells capable of recognizing and killing malignant cells. In their analysis, Chowell et al demonstrated that in patients with melanoma or NSCLC treated with ICIs, higher HED correlated with better outcomes and served as an independent biomarker in Cox multivariable analysis.103
Potentially, HLA diversity and HED can be evaluated through blood-based germline HLA genotyping, thus avoiding the need for biopsies or tumor tissue. However, evidence suggests that tumor cells may acquire (epi)genetic alterations leading to HLA-I downregulation, impaired or reduced antigen presentation, and loss of heterozygosity.105,106 Differences in study design, including the type of biological specimen analyzed and whether only HLA heterozygosity or also HED was assessed, may partly explain why some investigations have reported less consistent results than those of Chowell et al regarding the robustness of HLA as a predictive biomarker.102,107 Overall, while HLA diversity and HED are promising and remain under active investigation, they are not easily integrated into routine clinical practice due to multiple challenges, including cost, test availability, and the choice of the appropriate specimen.
Host Factors and Response to Immunotherapy
There is growing recognition that host-related characteristics substantially influence the efficacy of ICIs. Baseline features such as history of tobacco exposure, sex at birth, and body mass index (BMI) have emerged as clinically relevant variables, with potential implications for treatment outcomes. Taking into account host determinants may therefore support a more individualized approach to immunotherapy in NSCLC.
Tobacco Exposure and Immunotherapy Outcomes
History of tobacco exposure is a key determinant of immunotherapy efficacy in NSCLC. Patients without a history of tobacco use account for 10–25% of cases worldwide, with a higher prevalence among women in Asian and Middle Eastern populations.108,109 These tumors generally have a more favorable prognosis, largely due to the frequent presence of selected AGAs (eg EGFR, ALK, ROS1, RET, NTRK, ERBB2), for which effective targeted therapies are available. In contrast, they typically exhibit molecular and microenvironmental features associated with reduced benefit from ICIs, including lower TMB, a higher transitions/transversions (Ti/Tv) ratio, and a less immunogenic, more suppressive TME.108
Clinical evidence supports this biological observation. Several registrational trials of ICIs have reported lower benefit in this population,110,111 and multiple retrospective analyses have consistently shown a positive association between smoking history and ICI efficacy, even in tumors with PD-L1 expression ≥50%. For example, Li et al conducted a prospective analysis at Princess Margaret Cancer Center showing higher response rates in patients with tobacco exposure, irrespective of PD-L1 status.112 Similarly, Gainor et al reported a favorable trend in both progression-free survival and duration of response among patients with PD-L1 ≥50%.113 Cortellini et al also observed that, within a PD-L1 ≥50% cohort treated with pembrolizumab, tobacco exposure was associated with a lower risk of progression and death. Importantly, this effect was not explained by a more aggressive biology of tumors in patients without tobacco exposure, as the opposite trend was observed in contemporaneous cohorts treated with chemotherapy.114
Given the suboptimal outcomes with PD-(L)1 blockade in NSCLC patients without a history of tobacco exposure, treatment intensification strategies are being explored. Subgroup analyses from multiple prospective trials, as well as a recent meta-analysis by Luo et al, indicate a benefit from chemo-immunotherapy combinations,115–117 while the benefit of the addition of anti-CTLA-4 agents remains controversial.116,118,119 Further research is needed to refine predictive biomarkers and optimize treatment approaches for this understudied subgroup.
The Interplay Between Body Composition and Sex in Shaping Immunotherapy Response
Body composition (BC) and sex modulate the immune system and influence the antitumor response,120,121 potentially affecting immunotherapy efficacy. These parameters reflect patients’ metabolic and hormonal background and can shape both immune function and the TME. Understanding how BC modification and sex-specific factors interact with the tumor and the immune system may provide valuable insight into the variability of ICI outcomes, ultimately helping to optimize patient selection for immunotherapy.
Obesity has long been recognized as a risk factor for solid tumors and is associated with poorer outcomes among cancer patients.122 In fact, obesity exerts multifaceted effects on tumorigenesis across different cancer types: adipose tissue (AT) acts as an endocrine organ through estrogen production,123,124 activation of insulin–IGF-1 signaling,125 and secretion of adipokines that drive chronic inflammation.126,127 Whitin the TME, obesity impairs immunity by promoting macrophage polarization toward the M2 phenotype, expanding myeloid-derived suppressor cells (MDSCs), and inducing CD8+ T cell exhaustion.128–131 Leptin-driven PD-1 overexpression on CD8+ T cells, mediated through STAT3 signaling, further contributes to this dysfunctional state.132
Interestingly, this immunosuppressive environment may enhance tumor susceptibility to checkpoint inhibition: preclinical evidence has shown that in obese mouse models, PD-1 blockade restored T cell effector function and enhanced tumor regression compared to lean controls.132,133 This paradox, known as the “obesity paradox,” suggests that obesity both impairs immunosurveillance and simultaneously primes tumors for ICI efficacy.
Despite its association with chronic inflammation, recent evidence indicates that patients with a BMI ≥ 25 kg/m2 may experience improved survival with ICIs compared with those with normal BMI.134
In NSCLC, several clinical studies have confirmed that overweight and obese patients achieve better outcomes with ICIs. Pooled trial analyses demonstrated longer OS in patients with BMI ≥25 kg/m2 treated with atezolizumab, with the strongest effect in those with BMI ≥30 kg/m2.135 Similarly, in retrospective cohorts of patients with PD-L1 ≥50%, baseline obesity was associated with higher response rates and longer PFS and OS in patients receiving pembrolizumab, but not in those treated with chemotherapy.136 Meta-analyses further supported this survival advantage in obese patients,137 whereas large real-world datasets challenged these findings, showing no independent prognostic role for BMI overall.138–140
Altogether, these findings remain inconclusive, underscoring the need for future studies to incorporate more accurate metrics of BC when evaluating immunotherapy outcomes.
Indeed, the impact of obesity on immunotherapy efficacy cannot be fully understood without considering sex-related dimorphisms. Men and women differ in fat distribution: men predominantly accumulate visceral adipose tissue, while women store more subcutaneous fat before menopause, shifting toward visceral fat in later life. These differences in BC are immunologically relevant, as adiposity distribution influences systemic inflammation and long-term immune memory.141
Several studies suggest that the “obesity paradox” in immunotherapy may be more pronounced in men. In patients with advanced melanoma treated with ICIs, obesity was associated with better survival in male but not in females.142,143 Preclinical data reinforce this sex-specific effect: in murine tumor models of melanoma, obese males responded significantly better to PD-1 blockade, whereas obese females did not experience similar benefit. Interestingly, ovariectomy in female mice led to both weight gain and restored sensitivity to ICIs,144 pointing to sex hormones as critical mediators of the relationship between AT and immunotherapy response.
Beyond adiposity, intrinsic sex-related immune differences also influence ICI outcomes. Meta-analyses have suggested greater ICI benefit in men when ICIs are given as monotherapy, whereas women appear to derive more benefit from chemoimmunotherapy combinations.145,146 Moreover, machine-learning models integrating clinical, genomics and immune features have similarly identified male sex as a positive predictor of ICI response.147
Transcriptomic and molecular analyses of NSCLC tumors have revealed stronger immune infiltration in women, accompanied by higher expression of inhibitory checkpoints and immunosuppressive populations, consistent with adaptive resistance. In contrast, men displayed a more immune-excluded phenotype with frequent HLA loss of heterozygosity.121
In this contest, hormonal signalling plays a central role in modulating response to ICIs. Androgen receptor (AR) activation promotes T cell exhaustion,148 while evidence while evidence from prostate cancer suggests that AR inhibition synergizes with PD-1 blockade to restore T cell cytotoxicity activity.149,150 Estrogen receptor signalling drives M2 macrophage polarization and suppresses CD8+ effector activity, whereas pharmacological blockade with fulvestrant has been shown to enhance ICI efficacy in preclinical models.151
Aging further complicates this interplay: hormonal decline, sarcopenia, and chronic inflammation impair immune surveillance and predict poor immunotherapy outcomes.148,152,153
Taken together, these findings indicate that BMI and sex are not independent, but rather interconnected, host-related factors shaping immunotherapy outcomes. Obesity promotes systemic inflammation and immune dysfunction but, paradoxically, may enhance responses to PD-1/PD-L1 blockade. The magnitude and direction of this effect appear to differ by sex, likely reflecting hormonal regulation and differences in adipose distribution. The distinct metabolic and hormonal environments of men and women influence the quality and extent of ICI benefit. Integrating BC measures, sex-specific immune features, and hormonal status into biomarker development is essential to achieve more precise stratification of patients undergoing immunotherapy.
AI-Based Integrative Models for Predicting Immunotherapy Response
AI in oncology refers to the use of computational algorithms to analyze large and complex datasets, with the goal of identifying patterns, classifying outcomes, or generating predictions that can inform clinical decision-making. Within AI, machine learning (ML) refers to algorithms that improve performance by learning from data, while deep learning (DL) represents a subset of ML that uses multilayer neural networks to automatically extract features and recognize complex patterns. In the last years, AI has been successfully employed in diagnostics, therapeutics, and prognostic predictions in several neoplasms.87,154,155
A major challenge in the identification of robust immunotherapy biomarkers is the multifactorial nature of tumor immunogenicity, which is shaped by both tumor-intrinsic and tumor-extrinsic determinants. AI offers the advantage of integrating these diverse variables, while ML approaches further support the development of predictive scoring systems. By employing TCGA data and ML, Charoentong et al described the immunophenoscore, a pan-cancer immune gene signature designed to identify patients more likely to benefit from immunotherapy, thus underscoring the possible contribution of AI in this setting.156 More recently, Christopoulos et al applied a machine learning–based algorithm to classify patients according to their proteomic profile. The test, performed prior to initiation of ICI-based therapy (either alone or in combination with chemotherapy) in metastatic NSCLC, stratified patients into PROphet-negative and PROphet-positive groups. Notably, the PROphet test outperformed PD-L1 in identifying patients more likely to benefit from treatment escalation with the addition of chemotherapy.157 In line with these efforts, SCORPIO (Standard Clinical and labOratory featuRes for Prognostication of Immuno therapy Outcomes), a ML system that utilizes routine blood tests and clinical characteristics, was developed and trained on data from 1628 patients who received ICI at Memorial Sloan Kettering Cancer Center for 17 different cancer types. Internal and external tests validation tests showed that SCORPIO can outperform TMB in predicting ICI outcomes, potentially paving the way for the integration of AI-based predictors of response into clinical practice.158
Conclusion
In recent years, significant efforts have been made to develop novel therapeutic agents, in order to overcome both acquired and primary resistance to ICI: ADCs, bispecific antibodies, vaccines, and adoptive cell therapies have been tested in several trials and are still under active investigation. However, many trials aimed at enhancing ICI efficacy—often through combination strategies with the aforementioned therapeutic approaches—have shown controversial results. A common limitation of these studies has been the lack of appropriate patient selection. It is therefore reasonable to hypothesize that this challenge in approving new therapeutic strategies likely reflects the scarcity of robust predictive biomarkers, which would allow clinicians to identify patients who need treatment escalation and to select the most appropriate strategy. As extensively discussed, PD-L1 and TMB, despite being approved by multiple regulatory authorities and widely used in clinical practice, present important biological and technical limitations. This has fueled increasing interest in the identification of novel and emerging predictors of response to immunotherapy. Overall, the biomarkers discussed in this review can be broadly categorized into tissue-based, soluble and liquid biopsy–derived, host-related, and AI-driven integrative approaches, each capturing distinct and complementary aspects of tumor–immune interactions. While several of these biomarkers have shown predictive potential, none has proven sufficient as a standalone tool, highlighting the need for multidimensional strategies to refine patient stratification.
Given the complexity of both the tumor and the immune system, it is probably necessary to integrate multiple variables that describe tumor genomic profile, TME characteristics, and baseline immune status. For this reason, AI—capable of analyzing multiple variables simultaneously—should be considered a helpful tool, as long as it is guided by the expertise of clinicians. In this context, AI-based models may facilitate the integration of heterogeneous biomarker signals and support the translation of complex biological information into clinically actionable frameworks. Future efforts should focus on integrating predictive biomarkers and using them to design clinical trials capable of effectively pave the way for tailored ICI-based treatments.
Acknowledgments
Dr. Eleonora Gariazzo is supported by Fondazione Avanti Tutta.
Dr. Valentina Santo was supported by an American-Italian Cancer Foundation Post-Doctoral Research Fellowship, year 2025–2026.
Disclosure
Alessio Cortellini reports personal fees from Astrazeneca, personal fees from MSD, personal fees from Roche, personal fees from BMS, personal fees from Yuhan corporation, outside the submitted work. Biagio Ricciuti reports being on the advisory board for AstraZeneca, Regeneron, BMS, AbbVie, Lilly, J & J, and Caris Life, during the conduct of the study. Giulio Metro reports speaker’s fee from Amgen, congress travel fee from Takeda, speaker’s fee from AstraZeneca, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. De Giglio A, Di Federico A, Deiana C, Ricciuti B, Brambilla M, Metro G. Advanced non-small-cell lung cancer: how to manage non-oncogene disease. Drugs in Context. 2022;11:1–20. doi:10.7573/dic.2022-2-4
2. De Giglio A, Ricciuti B, Metro G. The expanding scenario of advanced non-small-cell lung cancer between emerging evidence and clinical tasks. Drugs Context. 2023;12. doi:10.7573/dic.2022-11-4.
3. Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primer. 2024;10(1):71. doi:10.1038/s41572-024-00551-9
4. Dolled-Filhart M, Roach C, Toland G, et al. Development of a companion diagnostic for pembrolizumab in non-small cell lung cancer using immunohistochemistry for programmed death ligand-1. Arch Pathol Lab Med. 2016;140(11):1243–1249. doi:10.5858/arpa.2015-0542-OA
5. Pai T, Aiyer HM, Kulkarni B, et al. Role of PD-L1 SP263 assay in cancer immunotherapy: a comprehensive review. J Cancer Immunol. 2024;6(2):77–91. doi:10.33696/cancerimmunol.6.088
6. Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N Engl J Med. 2020;383(14):1328–1339. doi:10.1056/NEJMoa1917346
7. Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, Phase 3, randomised, controlled trial. Lancet Lond Engl. 2021;397(10274):592–604. doi:10.1016/S0140-6736(21)00228-2
8. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/nejmoa1606774
9. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50. J Clin Oncol off J Am Soc Clin Oncol. 2021;39(21):2339–2349. doi:10.1200/JCO.21.00174
10. Kilickap S, Baramidze A, Sezer A, et al. Cemiplimab monotherapy for first-line treatment of patients with advanced NSCLC With PD-L1 Expression of 50% or Higher: five-Year Outcomes of EMPOWER-Lung 1. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2025;20(7):941–954. doi:10.1016/j.jtho.2025.03.033
11. Pérol M, Felip E, Dafni U, et al. Effectiveness of PD-(L)1 inhibitors alone or in combination with platinum-doublet chemotherapy in first-line (1L) non-squamous non-small-cell lung cancer (Nsq-NSCLC) with PD-L1-high expression using real-world data. Ann Oncol off J Eur Soc Med Oncol. 2022;33(5):511–521. doi:10.1016/j.annonc.2022.02.008
12. Vallejo J, Singh H, Larkins E, et al. Impact of Increasing PD-L1 Levels on Outcomes to PD-1/PD-L1 Inhibition in Patients With NSCLC: a Pooled Analysis of 11 Prospective Clinical Trials. Oncologist. 2024;29(5):422–430. doi:10.1093/oncolo/oyae006
13. Brahmer JR, Lee JS, Ciuleanu TE, et al. Five-year survival outcomes with nivolumab plus ipilimumab versus chemotherapy as first-line treatment for metastatic non-small-cell lung cancer in checkMate 227. J Clin Oncol off J Am Soc Clin Oncol. 2023;41(6):1200–1212. doi:10.1200/JCO.22.01503
14. Reck M, Ciuleanu TE, Schenker M, et al. Five-year outcomes with first-line (1L) nivolumab + ipilimumab + chemotherapy (N + I + C) vs C in patients (pts) with metastatic NSCLC (mNSCLC) in CheckMate 9LA. J Clin Oncol. 2024;42(16_suppl):8560. doi:10.1200/JCO.2024.42.16_suppl.8560
15. Di Federico A, Alden SL, Smithy JW, et al. Intrapatient variation in PD-L1 expression and tumor mutational burden and the impact on outcomes to immune checkpoint inhibitor therapy in patients with non-small-cell lung cancer. Ann Oncol off J Eur Soc Med Oncol. 2024;35(10):902–913. doi:10.1016/j.annonc.2024.06.014
16. Koomen BM, Badrising SK, van den Heuvel MM, Willems SM. Comparability of PD-L1 immunohistochemistry assays for non-small-cell lung cancer: a systematic review. Histopathology. 2020;76(6):793–802. doi:10.1111/his.14040
17. Butter R, Hondelink LM, van Elswijk L, et al. The impact of a pathologist’s personality on the interobserver variability and diagnostic accuracy of predictive PD-L1 immunohistochemistry in lung cancer. Lung Cancer. 2022;166:143–149. doi:10.1016/j.lungcan.2022.03.002
18. Ramalingam SS, Hellmann MD, Awad MM, et al. Abstract CT078: tumor mutational burden (TMB) as a biomarker for clinical benefit from dual immune checkpoint blockade with nivolumab (nivo) + ipilimumab (ipi) in first-line (1L) non-small cell lung cancer (NSCLC): identification of TMB cutoff from CheckMate 568. Cancer Res. 2018;78(13_supplement).
19. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus Ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
20. Bravaccini S, Bronte G, Ulivi P. TMB in NSCLC: a Broken Dream? Int J Mol Sci. 2021;22(12). doi:10.3390/ijms22126536
21. Vokes NI, Liu D, Ricciuti B, et al. Harmonization of tumor mutational burden quantification and association with response to immune checkpoint blockade in non–small-cell lung cancer. JCO Precis Oncol. 2019;3:1–12. doi:10.1200/PO.19.00171
22. Ricciuti B, Wang X, Alessi JV, et al. Association of high tumor mutation burden in non-small cell lung cancers with increased immune infiltration and improved clinical outcomes of PD-L1 blockade across PD-L1 Expression Levels. JAMA Oncol. 2022;8(8):1160–1168. doi:10.1001/jamaoncol.2022.1981
23. Alessi JV, Elkrief A, Ricciuti B, et al. Clinicopathologic and genomic factors impacting efficacy of first-line chemoimmunotherapy in advanced NSCLC. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2023;18(6):731–743. doi:10.1016/j.jtho.2023.01.091
24. Cristescu R, Mogg R, Ayers M, et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science. 2018;362(6411). doi:10.1126/science.aar3593
25. Skoulidis F, Goldberg ME, Greenawalt DM, et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018;8(7):822–835. doi:10.1158/2159-8290.CD-18-0099
26. Ricciuti B, Arbour KC, Lin JJ, et al. Diminished efficacy of programmed death-(Ligand)1 Inhibition in STK11- and KEAP1-mutant lung adenocarcinoma is affected by KRAS mutation status. J Thorac Oncol. 2022;17(3):399–410. doi:10.1016/j.jtho.2021.10.013
27. Ricciuti B, Garassino MC. Precision Immunotherapy for STK11/KEAP1-Mutant NSCLC. J Thorac Oncol. 2024;19(6):877–882. doi:10.1016/j.jtho.2024.03.002
28. Skoulidis F, Araujo HA, Do MT, et al. CTLA4 blockade abrogates KEAP1/STK11-related resistance to PD-(L)1 inhibitors. Nature. 2024;635(8038):462–471. doi:10.1038/s41586-024-07943-7
29. Alessi JV, Ricciuti B, Spurr LF, et al. SMARCA4 and other switch/sucrose nonfermentable family genomic alterations in NSCLC: clinicopathologic characteristics and outcomes to immune checkpoint inhibition. J Thorac Oncol. 2021;16(7):1176–1187. doi:10.1016/j.jtho.2021.03.024
30. Exposito F, Redrado M, Houry M, et al. PTEN loss confers resistance to Anti-PD-1 therapy in non-small cell lung cancer by increasing tumor infiltration of regulatory t cells. Cancer Res. 2023;83(15):2513–2526. doi:10.1158/0008-5472.CAN-22-3023
31. Cappuzzo F, Ricciuti B, Delmonte A, et al. MAPK pathway-activating alteration and immunotherapy efficacy in squamous cell lung carcinoma: results from the randomized, prospective SQUINT Trial. Clin Cancer Res off J Am Assoc Cancer Res. 2025;31(6):1027–1036. doi:10.1158/1078-0432.CCR-24-2077
32. Gao Q, Steine EJ, Barrasa MI, et al. Deletion of the de novo DNA methyltransferase Dnmt3a promotes lung tumor progression. Proc Natl Acad Sci U S A. 2011;108(44):18061–18066. doi:10.1073/pnas.1114946108
33. Yang L, Rau R, Goodell MA. DNMT3A in haematological malignancies. Nat Rev Cancer. 2015;15(3):152–165. doi:10.1038/nrc3895
34. Luo N, Nixon MJ, Gonzalez-Ericsson PI, et al. DNA methyltransferase inhibition upregulates MHC-I to potentiate cytotoxic T lymphocyte responses in breast cancer. Nat Commun. 2018;9(1):248. doi:10.1038/s41467-017-02630-w
35. Ricciuti B, Scalera S, Wang X, et al. DNA methyltransferase 3A (DNMT3A) mutations and PD-(L)1 blockade efficacy in non-small-cell lung cancer. Ann Oncol off J Eur Soc Med Oncol. 2025:S0923–7534(25)00804–X. doi:10.1016/j.annonc.2025.06.003.
36. Kim HS, Cha H, Kim J, et al. Genomic scoring to determine clinical benefit of immunotherapy by targeted sequencing. Eur J Cancer. 2019;120:65–74. doi:10.1016/j.ejca.2019.08.001
37. Liu L, Bai X, Wang J, et al. Combination of TMB and CNA stratifies prognostic and predictive responses to immunotherapy across metastatic cancer. Clin Cancer Res. 2019;25(24):7413–7423. doi:10.1158/1078-0432.CCR-19-0558
38. Alessi JV, Price A, Richards AL, et al. Multi-institutional analysis of aneuploidy and outcomes to chemoradiation and durvalumab in stage III non-small cell lung cancer. J Immunother Cancer. 2023;11(11). doi:10.1136/jitc-2023-007618
39. Alessi JV, Wang X, Elkrief A, et al. Impact of aneuploidy and chromosome 9p loss on tumor immune microenvironment and immune checkpoint inhibitor efficacy in NSCLC. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2023;18(11):1524–1537. doi:10.1016/j.jtho.2023.05.019
40. Han G, Yang G, Hao D, et al 9p21 loss confers a cold tumor immune microenvironment and primary resistance to immune checkpoint therapy. Nat Commun. 2021;12(1):5606. doi:10.1038/s41467-021-25894-9
41. Ebot EM, Duncan DL, Tolba K, et al. Deletions on 9p21 are associated with worse outcomes after anti-PD-1/PD-L1 monotherapy but not chemoimmunotherapy. Npj Precis Oncol. 2022;6(1):44. doi:10.1038/s41698-022-00286-4
42. Kocher F, Amann A, Zimmer K, et al. High indoleamine-2,3-dioxygenase 1 (IDO) activity is linked to primary resistance to immunotherapy in non-small cell lung cancer (NSCLC). Transl Lung Cancer Res. 2021;10(1):304–313. doi:10.21037/tlcr-20-380
43. Agustoni F, Yu H, Ellison K, et al. Indoleamine 2,3-dioxygenase-1 expression in non-small-cell lung cancer: analyses of prevalence, clinical correlations and prognostic impact in 2 large patient cohorts. Front Immunol. 2025;16:1586782. doi:10.3389/fimmu.2025.1586782
44. Wang W, Huang L, Jin JY, et al. A validation study on IDO immune biomarkers for survival prediction in non-small cell lung cancer: radiation dose fractionation effect in early-stage disease. Clin Cancer Res off J Am Assoc Cancer Res. 2020;26(1):282–289. doi:10.1158/1078-0432.CCR-19-1202
45. Karayama M, Masuda J, Mori K, et al. Comprehensive assessment of multiple tryptophan metabolites as potential biomarkers for immune checkpoint inhibitors in patients with non-small cell lung cancer. Clin Transl Oncol off Publ Fed Span Oncol Soc Natl Cancer Inst Mex. 2021;23(2):418–423. doi:10.1007/s12094-020-02421-8
46. Ludovini V, Bianconi F, Siggillino A, et al. High PD-L1/IDO-2 and PD-L2/IDO-1 Co-expression levels are associated with worse overall survival in resected non-small cell lung cancer patients. Genes. 2021;12(2). doi:10.3390/genes12020273
47. Boyer M, Hui R, Urban D, et al. Pembrolizumab with platinum-based chemotherapy with or without epacadostat as first-line treatment for metastatic non-small cell lung cancer: a randomized, partially double-blind, placebo-controlled phase II study. BMC Cancer. 2024;23(Suppl 1):1250. doi:10.1186/s12885-022-10427-4
48. Zhang C, Wang K, Wang H. Adenosine in cancer immunotherapy: taking off on a new plane. Biochim Biophys Acta Rev Cancer. 2023;1878(6):189005. doi:10.1016/j.bbcan.2023.189005
49. Kowash RR, Akbay EA. Tumor intrinsic and extrinsic functions of CD73 and the adenosine pathway in lung cancer. Front Immunol. 2023;14:1130358. doi:10.3389/fimmu.2023.1130358
50. Kazemi MH, Raoofi Mohseni S, Hojjat-Farsangi M, et al. Adenosine and adenosine receptors in the immunopathogenesis and treatment of cancer. J Cell Physiol. 2018;233(3):2032–2057. doi:10.1002/jcp.25873
51. Inoue Y, Yoshimura K, Kurabe N, et al. Prognostic impact of CD73 and A2A adenosine receptor expression in non-small-cell lung cancer. Oncotarget. 2017;8(5):8738–8751. doi:10.18632/oncotarget.14434
52. Jin R, Liu L, Xing Y, et al. Dual mechanisms of novel cd73-targeted antibody and antibody-drug conjugate in inhibiting lung tumor growth and promoting antitumor immune-effector function. Mol Cancer Ther. 2020;19(11):2340–2352. doi:10.1158/1535-7163.MCT-20-0076
53. Wang R, Liu Z, Wang T, Zhang J, Liu J, Zhou Q. Landscape of adenosine pathway and immune checkpoint dual blockade in NSCLC: progress in basic research and clinical application. Front Immunol. 2024;15:1320244. doi:10.3389/fimmu.2024.1320244
54. Rakaee M, Kilvaer TK, Dalen SM, et al. Evaluation of tumor-infiltrating lymphocytes using routine H&E slides predicts patient survival in resected non–small cell lung cancer. Hum Pathol. 2018;79:188–198. doi:10.1016/j.humpath.2018.05.017
55. Fridman WH, Pagès F, Sautès-Fridman C, Galon J. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306. doi:10.1038/nrc3245
56. Bremnes RM, Busund LT, Kilvær TL, et al. The role of tumor-infiltrating lymphocytes in development, progression, and prognosis of non–small cell lung cancer. J Thorac Oncol. 2016;11(6):789–800. doi:10.1016/j.jtho.2016.01.015
57. Rakaee M, Adib E, Ricciuti B, et al. Association of machine learning–based assessment of tumor-infiltrating lymphocytes on standard histologic images with outcomes of immunotherapy in patients with NSCLC. JAMA Oncol. 2023;9(1):51. doi:10.1001/jamaoncol.2022.4933
58. Kos Z, Roblin E, Kim RS, et al. Pitfalls in assessing stromal tumor infiltrating lymphocytes (sTILs) in breast cancer. NPJ Breast Cancer. 2020;6:17. doi:10.1038/s41523-020-0156-0
59. Sholl LM. Biomarkers of response to checkpoint inhibitors beyond PD-L1 in lung cancer. Mod Pathol. 2022;35:66–74. doi:10.1038/s41379-021-00932-5
60. Mazzaschi G, Madeddu D, Falco A, et al. Low PD-1 expression in cytotoxic cd8+ tumor-infiltrating lymphocytes confers an immune-privileged tissue microenvironment in nsclc with a prognostic and predictive value. Clin Cancer Res. 2018;24(2):407–419. doi:10.1158/1078-0432.CCR-17-2156
61. Ghiringhelli F, Bibeau F, Greillier L, et al. Immunoscore immune checkpoint using spatial quantitative analysis of CD8 and PD-L1 markers is predictive of the efficacy of anti- PD1/PD-L1 immunotherapy in non-small cell lung cancer. EBioMedicine. 2023;92:104633. doi:10.1016/j.ebiom.2023.104633
62. Parra ER, Zhang J, Duose DY, et al. Multi-omics analysis reveals immune features associated with immunotherapy benefit in patients with squamous cell lung cancer from phase iii lung-MAP S1400I Trial. Clin Cancer Res off J Am Assoc Cancer Res. 2024;30(8):1655–1668. doi:10.1158/1078-0432.CCR-23-0251
63. Zheng Y, Sadée C, Ozawa M, Howitt BE, Gevaert O. Single-cell multimodal analysis reveals tumor microenvironment predictive of treatment response in non-small cell lung cancer. Sci Adv. 2025;11(21):eadu2151. doi:10.1126/sciadv.adu2151
64. Kraehenbuehl L, Weng CH, Eghbali S, Wolchok JD, Merghoub T. Enhancing immunotherapy in cancer by targeting emerging immunomodulatory pathways. Nat Rev Clin Oncol. 2022;19(1):37–50. doi:10.1038/s41571-021-00552-7
65. Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386(1):24–34. doi:10.1056/NEJMoa2109970
66. Cho BC, Abreu DR, Hussein M, et al. Tiragolumab plus atezolizumab versus placebo plus atezolizumab as a first-line treatment for PD-L1-selected non-small-cell lung cancer (CITYSCAPE): primary and follow-up analyses of a randomised, double-blind, Phase 2 study. Lancet Oncol. 2022;23(6):781–792. doi:10.1016/S1470-2045(22)00226-1
67. Davar D, Eroglu Z, Milhem M, et al. 596 AMBER, Part 2B: a Phase 1 study of cobolimab plus dostarlimab in patients with advanced/metastatic non-small cell lung cancer (NSCLC) previously treated with anti-PD(L)-1 therapy. J Immunother Cancer. 2023;11(Suppl 1). doi:10.1136/jitc-2023-SITC2023.0596
68. Girard N, Burotto M, Paz-Ares LG, et al. LBA53 Nivolumab (NIVO) plus relatlimab with platinum-doublet chemotherapy (PDCT) vs NIVO + PDCT as first-line (1L) treatment (tx) for stage IV or recurrent NSCLC: results from the randomized phase II RELATIVITY-104 study. Ann Oncol. 2024;35:S1243–S1244. doi:10.1016/j.annonc.2024.08.2295
69. Socinski MA, Rodriguez Abreu D, Lee DH, et al. LBA2 SKYSCRAPER-06: efficacy and safety of tiragolumab plus atezolizumab plus chemotherapy (tira + atezo + chemo) vs pembrolizumab plus chemotherapy (pembro + chemo) in patients (pts) with advanced non-squamous non-small cell lung cancer (NSq NSCLC). Immuno-Oncol Technol. 2024;24. doi:10.1016/j.iotech.2024.101025
70. Peters S, Herbst R, Horinouchi H, et al. Abstract CT051: SKYSCRAPER-01: a Phase III, randomized trial of tiragolumab (tira) + atezolizumab (atezo) versus placebo (pbo) + atezo in patients (pts) with previously-untreated PD-L1-high, locally advanced unresectable/metastatic NSCLC. Cancer Res. 2025;85(8_Supplement_2):CT051–CT051. doi:10.1158/1538-7445.AM2025-CT051
71. Yang R, Huang S, Huang C, et al. Fc-competent multispecific PDL-1/TIGIT/LAG-3 antibodies potentiate superior anti-tumor T cell response. Sci Rep. 2023;13(1):9865. doi:10.1038/s41598-023-36942-3
72. Luke JJ, Patel MR, Blumenschein GR, et al. The PD-1- and LAG-3-targeting bispecific molecule tebotelimab in solid tumors and hematologic cancers: a phase 1 trial. Nat Med. 2023;29(11):2814–2824. doi:10.1038/s41591-023-02593-0
73. Besse B, Italiano A, Cousin S, et al. 1313MO Safety and preliminary efficacy of AZD7789, a bispecific antibody targeting PD-1 and TIM-3, in patients (pts) with stage IIIB–IV non-small-cell lung cancer (NSCLC) with previous anti-PD-(L)1 therapy. Ann Oncol. 2023;34:S755. doi:10.1016/j.annonc.2023.09.2347
74. Hiltermann TJN, Izumi H, Cho BC, et al. OA11.03 Efficacy and Safety of Rilvegostomig, an Anti-PD-1/TIGIT Bispecific, for CPI-naïve Metastatic NSCLC with PD-L1 1-49% or ≥50%. J Thorac Oncol. 2024;19(10, Supplement):S33. doi:10.1016/j.jtho.2024.09.061
75. Veccia A, Sforza V, Vattemi E, et al. Pretreatment lung immune prognostic index as a biomarker in advanced non-small-cell lung cancer patients receiving first line pembrolizumab. Immunotherapy. 2021;13(13):1093–1103. doi:10.2217/imt-2021-0002
76. Chan SWS, Smith E, Aggarwal R, et al. Systemic inflammatory markers of survival in epidermal growth factor–mutated non–small-cell lung cancer: single-institution analysis, systematic review, and meta-analysis. Clin Lung Cancer. 2021;22(5):390–407. doi:10.1016/j.cllc.2021.01.002
77. Banna GL, Cortellini A, Cortinovis DL, et al. The lung immuno-oncology prognostic score (LIPS-3): a prognostic classification of patients receiving first-line pembrolizumab for PD-L1 ≥ 50% advanced non-small-cell lung cancer. ESMO Open. 2021;6(2):100078. doi:10.1016/j.esmoop.2021.100078
78. Banna GL, Tiseo M, Cortinovis DL, et al. Host immune-inflammatory markers to unravel the heterogeneous outcome and assessment of patients with PD-L1 ≥50% metastatic non-small cell lung cancer and poor performance status receiving first-line immunotherapy. Thorac Cancer. 2022;13(3):483–488. doi:10.1111/1759-7714.14256
79. Nelli F, Fabbri A, Virtuoso A, et al. Early changes in LIPI score predict immune-related adverse events: a propensity score matched analysis in advanced non-small cell lung cancer patients on immune checkpoint blockade. Cancers. 2024;16(2). doi:10.3390/cancers16020453
80. Mezquita L, Auclin E, Ferrara R, et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non-small cell lung cancer. JAMA Oncol. 2018;4(3):351–357. doi:10.1001/jamaoncol.2017.4771
81. Raphael A, Kamm Feldman A, Lazarev I, et al. Lung immune prognostic index-based predictive score in advanced non-small cell lung cancer with a programmed death ligand-1 tumor proportion score ≥ 50. J Clin Med. 2025;14(10). doi:10.3390/jcm14103543
82. Huang L, Han H, Zhou L, et al. Evaluation of the lung immune prognostic index in non-small cell lung cancer patients treated with systemic therapy: a retrospective study and meta-analysis. Front Oncol. 2021;11:670230. doi:10.3389/fonc.2021.670230
83. Herranz-Bayo E, Chara-Velarde LE, Cassinello-Espinosa J, et al. Lung immune prognostic index (LIPI) as a prognostic factor in patients with extensive-stage small cell lung cancer treated with first-line chemoimmunotherapy. Clin Transl Oncol off Publ Fed Span Oncol Soc Natl Cancer Inst Mex. 2025;27(4):1484–1492. doi:10.1007/s12094-024-03690-3
84. Deng JY, Gao M, Fan X, et al. Clinical and dynamic circulating cytokines profile features of long-term progression-free survival benefit to immune checkpoint inhibitors in advanced non-small cell lung cancer. Cancer Immunol Immunother. 2025;74(6):173. doi:10.1007/s00262-025-03984-7
85. Olgun P, Diker O. Sixth-week immune-nutritional-inflammatory biomarkers: can they predict clinical outcomes in patients with advanced non-small cell lung cancer treated with immune checkpoint inhibitors? Curr Oncol Tor Ont. 2023;30(12):10539–10549. doi:10.3390/curroncol30120769
86. Alix-Panabières C, Pantel K. Liquid biopsy: from discovery to clinical application. Cancer Discov. 2021;11(4):858–873. doi:10.1158/2159-8290.CD-20-1311
87. Guardamagna M, Zamorano E, Albarrán-Artahona V, Mesas A, Benitez JC. Emerging techniques of translational research in immuno-oncology: a focus on non-small cell lung cancer. Cancers. 2025;17(13). doi:10.3390/cancers17132244
88. Rolfo CD, Madison RW, Pasquina LW, et al. Measurement of ctDNA tumor fraction identifies informative negative liquid biopsy results and informs value of tissue confirmation. Clin Cancer Res off J Am Assoc Cancer Res. 2024;30(11):2452–2460. doi:10.1158/1078-0432.CCR-23-3321
89. Madison R, Schrock AB, Castellanos E, et al. Retrospective analysis of real-world data to determine clinical outcomes of patients with advanced non-small cell lung cancer following cell-free circulating tumor DNA genomic profiling. Lung Cancer. 2020;148:69–78. doi:10.1016/j.lungcan.2020.07.033
90. Swalduz A, Schiffler C, Curcio H, et al. LIBELULE: a randomized phase iii study to evaluate the clinical relevance of early liquid biopsy in patients with suspicious metastatic lung cancer. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2025;20(4):437–450. doi:10.1016/j.jtho.2024.12.011
91. Ricciuti B, Jones G, Severgnini M, et al. Early plasma circulating tumor DNA (ctDNA) changes predict response to first-line pembrolizumab-based therapy in non-small cell lung cancer (NSCLC). J Immunother Cancer. 2021;9(3):e001504. doi:10.1136/jitc-2020-001504
92. Assaf ZJF, Zou W, Fine AD, et al. A longitudinal circulating tumor DNA-based model associated with survival in metastatic non-small-cell lung cancer. Nat Med. 2023;29(4):859–868. doi:10.1038/s41591-023-02226-6
93. Hellmann MD, Nabet BY, Rizvi H, et al. Circulating tumor DNA analysis to assess risk of progression after long-term response to PD-(L)1 blockade in NSCLC. Clin Cancer Res. 2020;26(12):2849–2858. doi:10.1158/1078-0432.CCR-19-3418
94. Anagnostou V, Ho C, Nicholas G, et al ctDNA response after pembrolizumab in non-small cell lung cancer: phase 2 adaptive trial results. Nat Med. 2023;29(10):2559–2569. doi:10.1038/s41591-023-02598-9
95. Besse B, Madison R, Cho-Phan CD, et al. CtDNA shed as a tool to select immune checkpoint inhibitors (ICPI) with or without chemotherapy for patients (pts) with advanced non–small cell lung cancer (aNSCLC). J Clin Oncol. 2022;40(16_suppl):9045. doi:10.1200/JCO.2022.40.16_suppl.9045
96. Moding EJ, Liu Y, Nabet BY, et al. Circulating tumor DNA dynamics predict benefit from consolidation immunotherapy in locally advanced non-small cell lung cancer. Nat Cancer. 2020;1(2):176–183. doi:10.1038/s43018-019-0011-0
97. Forde PM, Spicer JD, Provencio M, et al. Overall survival with neoadjuvant nivolumab plus chemotherapy in lung cancer. N Engl J Med. 2025;393(8):741–752. doi:10.1056/NEJMoa2502931
98. Ancel J, Dormoy V, Raby BN, et al. Soluble biomarkers to predict clinical outcomes in non-small cell lung cancer treated by immune checkpoints inhibitors. Front Immunol. 2023;14:1171649. doi:10.3389/fimmu.2023.1171649
99. Liao G, Zhao Z, Qian Y, et al. Prognostic role of soluble programmed death ligand 1 in non-small cell lung cancer: a systematic review and meta-analysis. Front Oncol. 2021;11:774131. doi:10.3389/fonc.2021.774131
100. Oitabén A, Fonseca P, Villanueva MJ, et al. Emerging blood-based biomarkers for predicting immunotherapy response in NSCLC. Cancers. 2022;14(11). doi:10.3390/cancers14112626
101. Chowell D, Morris LGT, Grigg CM, et al. Patient HLA class I genotype influences cancer response to checkpoint blockade immunotherapy. Science. 2018;359(6375):582–587. doi:10.1126/science.aao4572
102. Cuppens K, Baas P, Geerdens E, et al. HLA-I diversity and tumor mutational burden by comprehensive next-generation sequencing as predictive biomarkers for the treatment of non-small cell lung cancer with PD-(L)1 inhibitors. Lung Cancer. 2022;170:1–10. doi:10.1016/j.lungcan.2022.05.019
103. Chowell D, Krishna C, Pierini F, et al. Evolutionary divergence of HLA class I genotype impacts efficacy of cancer immunotherapy. Nat Med. 2019;25(11):1715–1720. doi:10.1038/s41591-019-0639-4
104. Grantham R. Amino acid difference formula to help explain protein evolution. Science. 1974;185(4154):862–864. doi:10.1126/science.185.4154.862
105. McGranahan N, Rosenthal R, Hiley CT, et al. Allele-Specific HLA loss and immune escape in lung cancer evolution. Cell. 2017;171(6):1259–1271.e11. doi:10.1016/j.cell.2017.10.001
106. Shim JH, Kim HS, Cha H, et al. HLA-corrected tumor mutation burden and homologous recombination deficiency for the prediction of response to PD-(L)1 blockade in advanced non-small-cell lung cancer patients. Ann Oncol off J Eur Soc Med Oncol. 2020;31(7):902–911. doi:10.1016/j.annonc.2020.04.004
107. Negrao MV, Lam VK, Reuben A, et al. PD-L1 expression, tumor mutational burden, and cancer gene mutations are stronger predictors of benefit from immune checkpoint blockade than hla class i genotype in non-small cell lung cancer. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2019;14(6):1021–1031. doi:10.1016/j.jtho.2019.02.008
108. De Alencar VTL, Figueiredo AB, Corassa M, Gollob KJ, Cordeiro De Lima VC. Lung cancer in never smokers: tumor immunology and challenges for immunotherapy. Front Immunol. 2022;13:984349. doi:10.3389/fimmu.2022.984349
109. Kim H, Lee W, Kim Y, et al. Proteogenomic characterization identifies clinical subgroups in EGFR and ALK wild-type never-smoker lung adenocarcinoma. Exp Mol Med. 2024;56(9):2082–2095. doi:10.1038/s12276-024-01320-0
110. Reck M, Rodríguez–Abreu D, Robinson AG, et al. Updated Analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer With PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. 2019;37(7):537–546. doi:10.1200/JCO.18.00149
111. Jassem J, De Marinis F, Giaccone G, et al. Updated overall survival analysis from impower110: atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1–selected NSCLC. J Thorac Oncol. 2021;16(11):1872–1882. doi:10.1016/j.jtho.2021.06.019
112. JJN L, Karim K, Sung M, et al. Tobacco exposure and immunotherapy response in PD-L1 positive lung cancer patients. Lung Cancer. 2020;150:159–163. doi:10.1016/j.lungcan.2020.10.023
113. Gainor JF, Rizvi H, Jimenez Aguilar E, et al. Clinical activity of programmed cell death 1 (PD-1) blockade in never, light, and heavy smokers with non-small-cell lung cancer and PD-L1 expression ≥50%. Ann Oncol. 2020;31(3):404–411. doi:10.1016/j.annonc.2019.11.015
114. Cortellini A, De Giglio A, Cannita K, et al. Smoking status during first‐line immunotherapy and chemotherapy in NSCLC</sc> patients: a case–control matched analysis from a large multicenter study. Thorac Cancer. 2021;12(6):880–889. doi:10.1111/1759-7714.13852
115. Rodríguez-Abreu D, Powell SF, Hochmair MJ, et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol. 2021;32(7):881–895. doi:10.1016/j.annonc.2021.04.008
116. Johnson ML, Cho BC, Luft A, et al. Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: the phase iii poseidon study. J Clin Oncol off J Am Soc Clin Oncol. 2023;41(6):1213–1227. doi:10.1200/JCO.22.00975
117. Luo D, Yang D, Cao D, et al. Effect of smoking status on immunotherapy for lung cancer: a systematic review and meta-analysis. Front Oncol. 2024;14. doi:10.3389/fonc.2024.1422160
118. Reck M, Ciuleanu TE, Schenker M, et al. Five-year outcomes with first-line nivolumab plus ipilimumab with 2 cycles of chemotherapy versus 4 cycles of chemotherapy alone in patients with metastatic non-small cell lung cancer in the randomized CheckMate 9LA trial. Eur J Cancer Oxf Engl 1990. 2024;211:114296. doi:10.1016/j.ejca.2024.114296
119. Gariazzo E, Elkrief A, Concannon K, et al. Clinical outcomes and predictors of response to PD-(L)1 blockade in patients with oncogene-driver negative NSCLC who have never smoked.
120. Exley MA, Hand L, O’Shea D, Lynch L. Interplay between the immune system and adipose tissue in obesity. J Endocrinol. 2014;223(2):R41–48. doi:10.1530/JOE-13-0516
121. Conforti F, Pala L, Pagan E, et al. Sex-based dimorphism of anticancer immune response and molecular mechanisms of immune evasion. Clin Cancer Res off J Am Assoc Cancer Res. 2021;27(15):4311–4324. doi:10.1158/1078-0432.CCR-21-0136
122. Petrelli F, Cortellini A, Indini A, et al. Association of obesity with survival outcomes in patients with cancer: a systematic review and meta-analysis. JAMA Network Open. 2021;4(3):e213520. doi:10.1001/jamanetworkopen.2021.3520
123. Renehan AG, Zwahlen M, Egger M. Adiposity and cancer risk: new mechanistic insights from epidemiology. Nat Rev Cancer. 2015;15(8):484–498. doi:10.1038/nrc3967
124. Friedenreich CM, Ryder-Burbidge C, McNeil J. Physical activity, obesity and sedentary behavior in cancer etiology: epidemiologic evidence and biologic mechanisms. Mol Oncol. 2021;15(3):790–800. doi:10.1002/1878-0261.12772
125. Shahid RK, Ahmed S, Le D, Yadav S. Diabetes and Cancer: risk, Challenges, Management and Outcomes. Cancers. 2021;13(22). doi:10.3390/cancers13225735
126. Iyengar NM, Gucalp A, Dannenberg AJ, Hudis CA. Obesity and cancer mechanisms: tumor microenvironment and inflammation. J Clin Oncol off J Am Soc Clin Oncol. 2016;34(35):4270–4276. doi:10.1200/JCO.2016.67.4283
127. Afify SM, Hassan G, Seno A, Seno M. Cancer-inducing niche: the force of chronic inflammation. Br J Cancer. 2022;127(2):193–201. doi:10.1038/s41416-022-01775-w
128. Xia S, Sha H, Yang L, Ji Y, Ostrand-Rosenberg S, Qi L. Gr-1+ CD11b+ myeloid-derived suppressor cells suppress inflammation and promote insulin sensitivity in obesity. J Biol Chem. 2011;286(26):23591–23599. doi:10.1074/jbc.M111.237123
129. Maimela NR, Liu S, Zhang Y. Fates of CD8+ T cells in Tumor Microenvironment. Comput Struct Biotechnol J. 2019;17:1–13. doi:10.1016/j.csbj.2018.11.004
130. Núñez-Ruiz A, Sánchez-Brena F, López-Pacheco C, Acevedo-Domínguez NA, Soldevila G. Obesity modulates the immune macroenvironment associated with breast cancer development. PLoS One. 2022;17(4):e0266827. doi:10.1371/journal.pone.0266827
131. Vick LV, Rosario S, Riess JW, et al. Potential roles of sex-linked differences in obesity and cancer immunotherapy: revisiting the obesity paradox. Npj Metab Health Dis. 2024;2(1):5. doi:10.1038/s44324-024-00007-4
132. Wang Z, Aguilar EG, Luna JI, et al. Paradoxical effects of obesity on T cell function during tumor progression and PD-1 checkpoint blockade. Nat Med. 2019;25(1):141–151. doi:10.1038/s41591-018-0221-5
133. Dudzinski SO, Bader JE, Beckermann KE, et al. Leptin augments antitumor immunity in obesity by repolarizing tumor-associated macrophages. J Immunol Baltim Md 1950. 2021;207(12):3122–3130. doi:10.4049/jimmunol.2001152
134. Cortellini A, Bersanelli M, Buti S, et al. A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: when overweight becomes favorable. J Immunother Cancer. 2019;7(1):57. doi:10.1186/s40425-019-0527-y
135. Kichenadasse G, Miners JO, Mangoni AA, Rowland A, Hopkins AM, Sorich MJ. Association between body mass index and overall survival with immune checkpoint inhibitor therapy for advanced non-small cell lung cancer. JAMA Oncol. 2020;6(4):512–518. doi:10.1001/jamaoncol.2019.5241
136. Cortellini A, Ricciuti B, Tiseo M, et al. Baseline BMI and BMI variation during first line pembrolizumab in NSCLC patients with a PD-L1 expression ≥ 50%: a multicenter study with external validation. J Immunother Cancer. 2020;8(2). doi:10.1136/jitc-2020-001403
137. Zhang T, Li S, Chang J, Qin Y, Li C. Impact of BMI on the survival outcomes of non-small cell lung cancer patients treated with immune checkpoint inhibitors: a meta-analysis. BMC Cancer. 2023;23(1):1023. doi:10.1186/s12885-023-11512-y
138. Cortellini A, Ricciuti B, Vaz VR, et al. Prognostic effect of body mass index in patients with advanced NSCLC treated with chemoimmunotherapy combinations. J Immunother Cancer. 2022;10(2). doi:10.1136/jitc-2021-004374
139. Ihara Y, Sawa K, Imai T, et al. Immunotherapy and overall survival among patients with advanced non-small cell lung cancer and obesity. JAMA Network Open. 2024;7(8):e2425363. doi:10.1001/jamanetworkopen.2024.25363
140. Nie W, Lu J, Qian J, et al. Obesity and survival in advanced non-small cell lung cancer patients treated with chemotherapy, immunotherapy, or chemoimmunotherapy: a multicenter cohort study. BMC Med. 2024;22(1):463. doi:10.1186/s12916-024-03688-2
141. Han SJ, Glatman Zaretsky A, Andrade-Oliveira V, et al. White adipose tissue is a reservoir for memory t cells and promotes protective memory responses to infection. Immunity. 2017;47(6):1154–1168.e6. doi:10.1016/j.immuni.2017.11.009
142. McQuade JL, Daniel CR, Hess KR, et al. Association of body-mass index and outcomes in patients with metastatic melanoma treated with targeted therapy, immunotherapy, or chemotherapy: a retrospective, multicohort analysis. Lancet Oncol. 2018;19(3):310–322. doi:10.1016/S1470-2045(18)30078-0
143. Naik GS, Waikar SS, Johnson AEW, et al. Complex inter-relationship of body mass index, gender and serum creatinine on survival: exploring the obesity paradox in melanoma patients treated with checkpoint inhibition. J Immunother Cancer. 2019;7(1):89. doi:10.1186/s40425-019-0512-5
144. Vick L, Wang Z, Collins C, et al. 534 Sex-linked differences in obesity markedly impact the anti-tumor efficacy of PD-1 blockade. J Immunother Cancer. 2022;10(Suppl 2). doi:10.1136/jitc-2022-SITC2022.0534
145. Conforti F, Pala L, Bagnardi V, et al. Cancer immunotherapy efficacy and patients’ sex: a systematic review and meta-analysis. Lancet Oncol. 2018;19(6):737–746. doi:10.1016/S1470-2045(18)30261-4
146. Conforti F, Pala L, Bagnardi V, et al. Sex-based heterogeneity in response to lung cancer immunotherapy: a systematic review and meta-analysis. J Natl Cancer Inst. 2019;111(8):772–781. doi:10.1093/jnci/djz094
147. Litchfield K, Reading JL, Puttick C, et al. Meta-analysis of tumor- and T cell-intrinsic mechanisms of sensitization to checkpoint inhibition. Cell. 2021;184(3):596–614.e14. doi:10.1016/j.cell.2021.01.002
148. Pala L, De Pas T, Catania C, et al. Sex and cancer immunotherapy: current understanding and challenges. Cancer Cell. 2022;40(7):695–700. doi:10.1016/j.ccell.2022.06.005
149. Graff JN, Alumkal JJ, Drake CG, et al. Early evidence of anti-PD-1 activity in enzalutamide-resistant prostate cancer. Oncotarget. 2016;7(33):52810–52817. doi:10.18632/oncotarget.10547
150. Graff JN, Beer TM, Alumkal JJ, et al. A phase II single-arm study of pembrolizumab with enzalutamide in men with metastatic castration-resistant prostate cancer progressing on enzalutamide alone. J Immunother Cancer. 2020;8(2). doi:10.1136/jitc-2020-000642
151. Chakraborty B, Byemerwa J, Shepherd J, et al. Inhibition of estrogen signaling in myeloid cells increases tumor immunity in melanoma. J Clin Invest. 2021;131(23). doi:10.1172/JCI151347
152. Gubbels Bupp MR, Potluri T, Fink AL, Klein SL. The confluence of sex hormones and aging on immunity. Front Immunol. 2018;9:1269. doi:10.3389/fimmu.2018.01269
153. Deng HY, Chen ZJ, Qiu XM, Zhu DX, Tang XJ, Zhou Q. Sarcopenia and prognosis of advanced cancer patients receiving immune checkpoint inhibitors: a comprehensive systematic review and meta-analysis. Nutr Burbank Los Angel Cty Calif. 2021;90:111345. doi:10.1016/j.nut.2021.111345
154. Zhang H, Meng D, Cai S, et al. The application of artificial intelligence in lung cancer: a narrative review. Transl Cancer Res. 2021;10(5):2478–2487. doi:10.21037/tcr-20-3398
155. Fang Y, Chen X, Cao C. Cancer immunotherapy efficacy and machine learning. Expert Rev Anticancer Ther. 2024;24(1–2):21–28. doi:10.1080/14737140.2024.2311684
156. Charoentong P, Finotello F, Angelova M, et al. Pan-cancer Immunogenomic analyses reveal genotype-immunophenotype relationships and predictors of response to checkpoint blockade. Cell Rep. 2017;18(1):248–262. doi:10.1016/j.celrep.2016.12.019
157. Christopoulos P, Harel M, McGregor K, et al. Plasma proteome-based test for first-line treatment selection in metastatic non-small cell lung cancer. JCO Precis Oncol. 2024;8:e2300555. doi:10.1200/PO.23.00555
158. Yoo SK, Fitzgerald CW, Cho BA, et al. Prediction of checkpoint inhibitor immunotherapy efficacy for cancer using routine blood tests and clinical data. Nat Med. 2025;31(3):869–880. doi:10.1038/s41591-024-03398-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Molecular Characteristics and the Effect of KRAS Mutation on the Prognosis of Immunotherapy in Non-Small Cell Lung Cancer in Xinjiang, China
Gu G, Yu B, Wan H, Lu S, Zhu X, Zhao Y, Fuxi Y, Liu C
OncoTargets and Therapy 2022, 15:1021-1032
Published Date: 21 September 2022
Overexpression of TREM1 is Associated with the Immune-Suppressive Microenvironment and Unfavorable Prognosis in Pan-Cancer
Zhou X, Lin K, Fu L, Liu F, Lin H, Chen Y, Zhuang B, Liang H, Deng Q, Wang Z, Chen W, Luo J, Cao J, Li P
Journal of Inflammation Research 2023, 16:1375-1391
Published Date: 27 March 2023
Exploring the Correlation Between GPR176, a Potential Target Gene of Gastric Cancer, and Immune Cell Infiltration
Gu X, Shen H, Xiang Z, Li X, Zhang Y, Zhang R, Su F, Wang Z
Pharmacogenomics and Personalized Medicine 2023, 16:519-535
Published Date: 1 June 2023
Integrating Bulk and Single-Cell RNA Sequencing Reveals Heterogeneity, Tumor Microenvironment, and Immunotherapeutic Efficacy Based on Sialylation-Related Genes in Bladder Cancer
Tan Z, Chen X, Zuo J, Fu S, Wang J, Wang H
Journal of Inflammation Research 2023, 16:3399-3417
Published Date: 14 August 2023
NOTCH1 Mutations Predict Superior Outcomes of Immune Checkpoint Blockade in Non-Small Cell Lung Cancer
Huang Q, Cao H, Yao Q, Zhou X, Li H, Bai Q, Hu H
ImmunoTargets and Therapy 2023, 12:165-173
Published Date: 5 December 2023