Back to Journals » Journal of Pain Research » Volume 18
Effectiveness of Acupotomy Combined with Topical Diclofenac for Knee Osteoarthritis: A Randomized Controlled Trial
Authors Du K ![]() , Cheng WZ, Li A, Zhang CY, Yan SY, Han F, Guo R, Chen P, Du WS, Zuo YL, Zuo QH, Li SM
, Cheng WZ, Li A, Zhang CY, Yan SY, Han F, Guo R, Chen P, Du WS, Zuo YL, Zuo QH, Li SM
Received 11 October 2025
Accepted for publication 2 December 2025
Published 17 December 2025 Volume 2025:18 Pages 6779—6790
DOI https://doi.org/10.2147/JPR.S571098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Kai Du,1,2,* Wu-Zhong Cheng,3,* Ao Li,2 Chen-Yu Zhang,2 Shi-Yan Yan,4 Fang Han,5 Ren Guo,1 Ping Chen,1 Wei-Shuai Du,1 Yong-Li Zuo,1 Qi-Heng Zuo,2 Shu-Ming Li1
1Department of Pain Medicine, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, People’s Republic of China; 2Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Department of Tuina, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, People’s Republic of China; 4International Acupuncture and Moxibustion Innovation Institute, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 5Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shu-Ming Li, Department of Pain Medicine, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Purpose: We sought to determine whether acupotomy, when combined with topical diclofenac diethylamine emulgel, could (a) reduce pain, and (b) improve functional outcomes in patients with knee osteoarthritis, compared with topical diclofenac alone.
Methods: This assessor-blinded, single-center randomized clinical trial was conducted at Beijing Hospital of Traditional Chinese Medicine, Capital Medical University. Participants aged 40 to 80 with knee osteoarthritis and a pain score of 4 or higher were randomly assigned, via a computer-generated sequence, to an acupotomy intervention group or a control group. Both groups used diclofenac diethylamine emulgel four times daily for 4 weeks, with acupotomy group receiving four acupotomy sessions. Primary outcome was proportion achieving minimal clinically important pain and function improvements. Analyses followed an intention-to-treat approach, with significance at a two-sided P-value < 0.05. Because of the nature of acupotomy, participants and practitioners could not be blinded.
Results: Response rates at 4 weeks were 92.55% (93 of 100) in acupotomy group and 61.54% (61 of 99) in control group. Rate differences were 31.01% (95% CI, 19.70% to 42.33%; P < 0.001). Benefit persisted at week 24 (90.32% vs 38.46%; rate difference, 51.86%; 95% CI, 40.20% to 63.52%; P < 0.001). Secondary outcomes showed greater improvement in NRS and WOMAC scores in acupotomy group at all time points (P < 0.001).
Conclusion: Acupotomy combined with topical diclofenac effectively reduces pain and improves function in knee osteoarthritis patients. Acupotomy can be considered an adjunctive therapy. This single-center, assessor-blinded trial was limited by the inability to blind participants and practitioners due to the nature of the intervention.
Keywords: acupotomy, knee, osteoarthritis, randomized controlled trial
Introduction
Knee osteoarthritis (OA) is a prevalent joint disorder characterized by chronic pain and functional disability.1,2 Beyond its clinical manifestations, knee OA is now recognized as a complex whole-joint disease, involving coordinated pathological changes across multiple articular structures—including progressive degeneration of hyaline cartilage and the menisci, synovial inflammation and fibrosis, biomechanical and inflammatory alterations of the infrapatellar fat pad, and maladaptive remodeling of the subchondral bone.3–6 Knee OA remains the largest component of the global OA burden, exhibiting a 2020 age-standardized prevalence of 4307.4 cases per 100,000 population.7,8 Driven by population aging and rising comorbidity profiles, its nonfatal disease burden has increased substantially and is projected to grow markedly by 2050. Knee OA is more common among women, the obese, and individuals with a history of knee injuries.9 Key risk factors include advancing age, repetitive joint use, knee misalignment, and muscle weakness.10
No existing treatment can completely prevent the progression of knee OA. Available treatment methods include non-pharmacological approaches like exercise and patient education, pharmacological options such as non-steroidal anti-inflammatory drugs (NSAIDs) and intra-articular corticosteroids, and surgical interventions like knee replacement.11,12 However, exercise therapy faces challenges in implementation and adherence, while patient education alone offers limited benefits.2,13 Long-term use of NSAIDs may bring about gastrointestinal irritation, ulcers and bleeding, and intra-articular steroid injections may have deleterious effects on cartilage.14–16 Knee replacement surgery, though beneficial for severe cases, can result in serious adverse events, lengthy recovery, and minimal effects on quality-adjusted life years.17,18 Due to these limitations, more patients are eagerly seeking complementary therapies that can satisfy the need for pain relief and improved function.
Acupotomy is a minimally invasive technique that integrates principles of acupuncture and micro-invasive soft-tissue release.19,20 It is proposed to act by mechanically releasing periarticular adhesions and contractures, reducing aberrant mechanical stress, and modulating local inflammatory and nociceptive processes.21–23 Given the substantial symptom burden of knee OA and the limitations of existing non-surgical treatments, interest in acupotomy has grown. Although recent reviews and meta-analyses suggest potential benefit, most prior studies are constrained by small samples and methodological weaknesses.24–27 Robust randomized evidence is therefore needed. This trial aims to evaluate whether acupotomy, as an adjunctive therapy to topical diclofenac diethylamine emulgel, can relieve pain and improve function in knee OA patients compared to topical diclofenac diethylamine emulgel alone.
Methods
Study Design
This single-center, parallel-group, assessor-blinded RCT was conducted at the Beijing Hospital of Traditional Chinese Medicine affiliated with Capital Medical University. Ethical approval was obtained from the hospital’s Medical Ethical Review Committee (No. 2020BL02-057-02), and the study was registered with the Chinese Clinical Trial Registry (ChiCTR2100043005). The detailed protocol adhered to the Declaration of Helsinki, and was previously published (Supplement 1).28 All patients provided written informed consent before enrollment. The study follows the Consolidated Standards of Reporting Trials (CONSORT) guidelines.29
Participants
Recruitment involved screening outpatients from the hospital. Additionally, recruitment advertisements were displayed in the outpatient hall and on the We-Media platform.
Eligible patients were men and women aged 40 to 80 years, diagnosed with knee OA based on the American College of Rheumatology (ACR) criteria.30 They experienced symptoms for more than 6 months and had radiologic evidence of Kellgren-Lawrence grade II to IV within the last 6 months.31 Eligibility required a pain severity score of 4 or higher on a 10-point numerical rating scale (NRS) (range, 0–10, with higher scores indicating greater pain).32 Only those who provided signed written informed consent were enrolled.
The key exclusion criteria included recent or planned knee interventions (including surgery, arthroscopy, intra-articular injection within the past 6 months, or acupotomy/acupuncture within the past 3 months); current use of analgesics, anti-inflammatory drugs, or other medications that may interfere with pain assessment (during the trial, participants were required to avoid all pain-related medications except the prescribed topical diclofenac and rescue medication); knee pain caused by other conditions; severe acute or chronic diseases (such as advanced heart failure, uncontrolled hypertension, recent stroke, severe kidney or liver dysfunction, active malignancy, or poorly controlled diabetes [HbA1c > 9%]); or a pronounced fear of acupotomy. Participants could continue their stable doses of medications for chronic conditions (eg, antihypertensives, hypoglycemics) throughout the trial period. Details are in eTable 1 of Supplement 2.
Randomization and Blinding
Eligible patients were randomly assigned to either acupotomy group or control group in a 1:1 ratio using block randomization, managed by an independent statistician. Each block consisted of 4 slots to ensure even distribution. The randomization sequence was sealed in opaque, sequentially numbered envelopes, accessed only by the researcher responsible for participant enrollment. Due to the nature of acupotomy, blinding of patients and practitioners was not possible. However, outcome assessors and statisticians were blinded to group assignments. Data analysis was independently conducted by the blinded statistician. The study procedure is detailed in Figure 1.
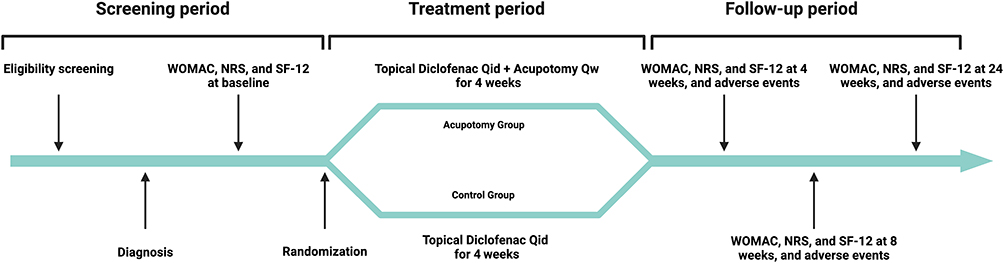 |
Figure 1 Study Procedures. Abbreviations: WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; NRS, Numerical Rating Scale; SF-12, 12-item Short Form Health Survey; Qid, four times a day; Qw, once a week. |
Interventions
Patients in both groups applied topical diclofenac diethylamine emulgel (Voltalin, Beijing Novartis Pharma Ltd) 4 times daily for 4 weeks, with dosage adjusted to the pain area.33 Patients documented their usage of diclofenac diethylamine emulgel daily.
Patients in the acupotomy group received additional weekly acupotomy treatments at five fixed acupoints and two Ah Shi points (tender points identified by a patient’s pain response upon palpation, allowing for targeted pain relief). The fixed acupoints included Dubi (ST35), Neixiyan (EX-LE4), Shiqizhui (EX-B8), Yaoyangguan (GV3), and Xiyangguan (GB33), while Ah Shi points were individually determined based on each patient’s specific pain locations during physical examination. These acupoints represent a standardized clinical regimen at our center and were selected for their relevance to periarticular soft-tissue tension, pain-generating structures, and biomechanical imbalance in knee OA.
The acupotomy procedure included: (a) Localization and Preparation: With the patient in a supine position, the aforementioned acupoints were identified and marked according to the descriptions provided in Supplement 3. The skin at these sites was disinfected, and sterile drapes were applied. (b) Orientation and Pressure Separation: The acupotomy blade was oriented parallel to the skin and key anatomical structures. Slight pressure was applied to separate superficial tissues, nerves, and vessels. (c) Incision and Treatment: The blade was advanced until the tip reached the bone surface. Then, the needle was penetrated into the periosteum and manipulated to release tension and dissolve adhesions. For Ah Shi points, the needle was manipulated in multiple directions to achieve an adequate release. (d) Post-procedure Care: After the treatment, the needle was removed, and pressure was applied to control bleeding. The treated area was covered with a sterile dressing to prevent infection. A photograph of the acupotomy instrument and a schematic of the procedure are provided in Supplement 4.
Loxoprofen sodium tablets (Loxonin, Dachi Sankyo Pharma Ltd) were provided as rescue medication, with usage documented by outcome assessors.34 During the trial, participants were required to avoid all pain-related medications except the prescribed study and rescue medications. They could continue routine medications for chronic conditions, like antihypertensives or hypoglycemics, as long as dosages stayed stable, ensuring consistency in chronic condition management and trial integrity.
Outcomes
The primary outcome was the response rate at week 4, defined as the proportion of patients who achieved minimal clinically important improvement (MCII) on both the NRS and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) function subscale.32,35,36 MCII was operationalized as a reduction of ≥2 points on the 10-point NRS and ≥6 points on the 68-point WOMAC function subscale.
Secondary outcomes, assessed at weeks 4, 8, and 24, included changes in knee pain, physical function, stiffness, quality of life, and rescue medication use. Pain levels were measured using both the NRS (range 0–10) and the WOMAC pain subscale (range 0–20). Physical function and stiffness were evaluated using the WOMAC function (range 0–68) and stiffness (range 0–8) subscales, respectively. Quality of life was assessed with the 12-item Short Form (SF-12) health survey (range 0–100).37 Rescue medication use was documented throughout the study to assess additional pain management needs. Due to the increase in patient volumes and reallocation of medical resources during the COVID-19 pandemic, the planned biomarker analyses, including tumor necrosis factor-α, interleukin-1β, and matrix metalloproteinase-3, were omitted to prioritize essential healthcare services and ensure patient safety.
Adverse events were recorded, including the occurrence time, severity, management, and prognosis, to assess treatment safety and tolerability.
Statistical Analysis
The sample size was 80 patients each group calculated by PASS 11.0.7 (NCSS, LLC, USA) software with an aim for a response rate of 60% in the control group and 80% in the acupotomy group, ensuring 80% power at a 5% significance level. Accounting for a 20% dropout rate, 100 patients per group were required (a total of 200 patients).
There were 3 analysis populations: Intention-To-Treat (ITT) set, Per-Protocol (PP) set, and Safety Set (SS) set, with detailed definitions provided in eTable 2 of Supplement 2. Baseline characteristics were summarized using the ITT population. For normally distributed variables, means ± standard deviation (SD) was calculated. For non-normally distributed variables, medians with interquartile ranges (IQR) were used.
The primary analysis was based on the ITT principle. Comparisons of response rates were analyzed using the χ2-test for proportions without imputation for missing data. Sensitivity analyses were conducted for response rates, including additional calculations using the Last Observation Carried Forward (LOCF) method in ITT. Further sensitivity analyses were conducted in the PP set, comparing response rates using the χ2-test. Logistic regression analyses, adjusted for baseline characteristics and rescue medication usage, were performed across both sets, applying three approaches to handle missing data: no imputation, LOCF, and multiple imputation.
Secondary outcomes, including changes from baseline in pain, physical function, stiffness, and quality of life, were compared between groups using independent samples t-tests. Rescue medication usage was assessed using Fisher’s exact test. Safety was analyzed in the SS population, with differences in adverse events assessed using Fisher’s exact test.
All statistical tests were two-sided, with a significance level set at P < 0.05. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA).
Results
From March 1st, 2021, and June 30th, 2023, 285 patients with knee OA were screened, of whom 200 patients were randomized (Figure 2). A single participant was mistakenly registered in the randomization system twice. The duplicate record, which contained no clinical data, was eliminated prior to analysis in accordance with CONSORT recommendations. In the acupotomy group, 93 patients completed all scheduled treatments and final follow-up assessments. Five patients dropped out due to adverse events and 2 due to loss to follow-up. In the control group, 91 patients completed the study, with 8 patients dropping out: 1 during week 2 and 7 during week 4, all due to loss to follow-up. The detailed baseline demographics are presented in Table 1.
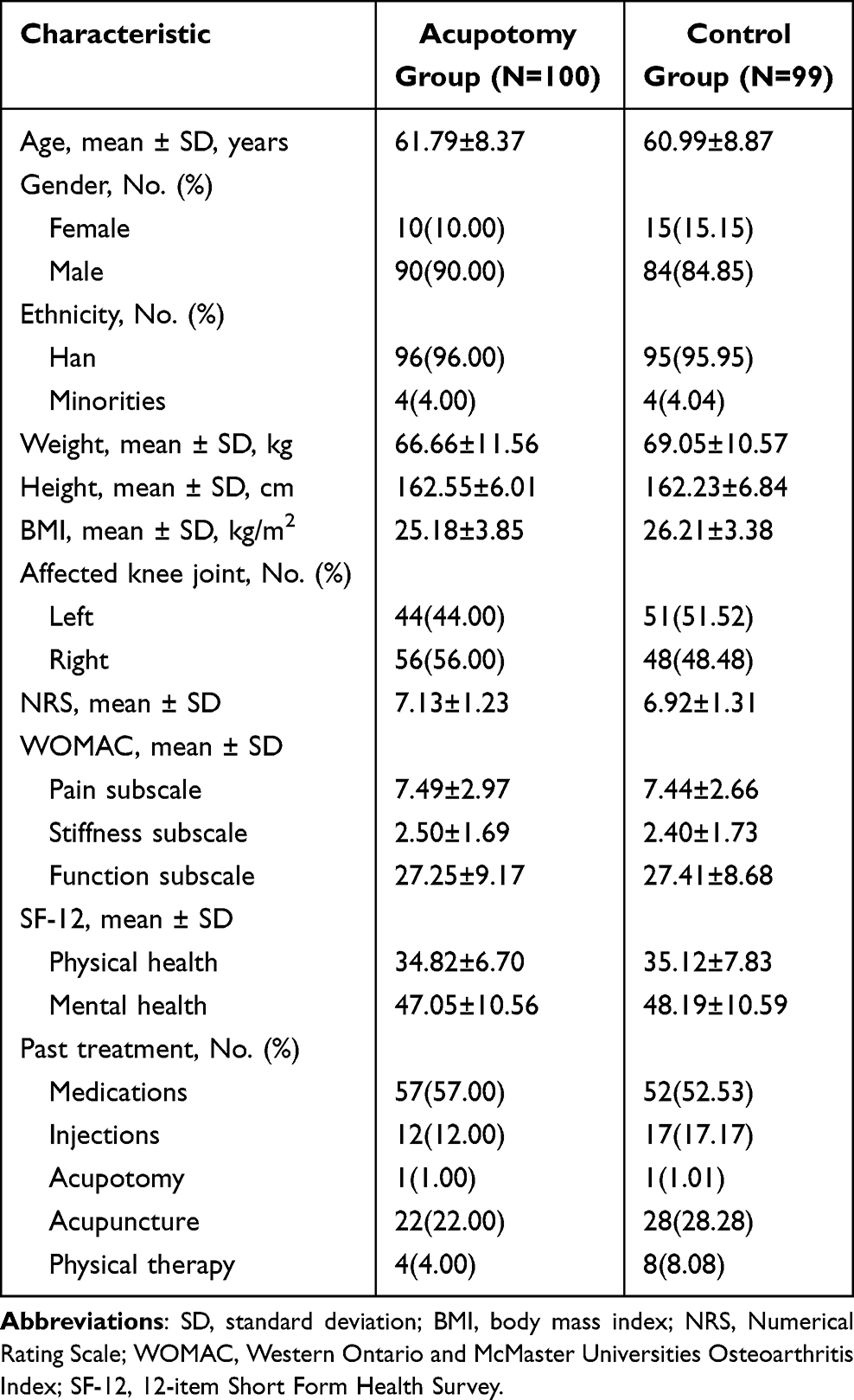 |
Table 1 Participant Demographic and Baseline Characteristics |
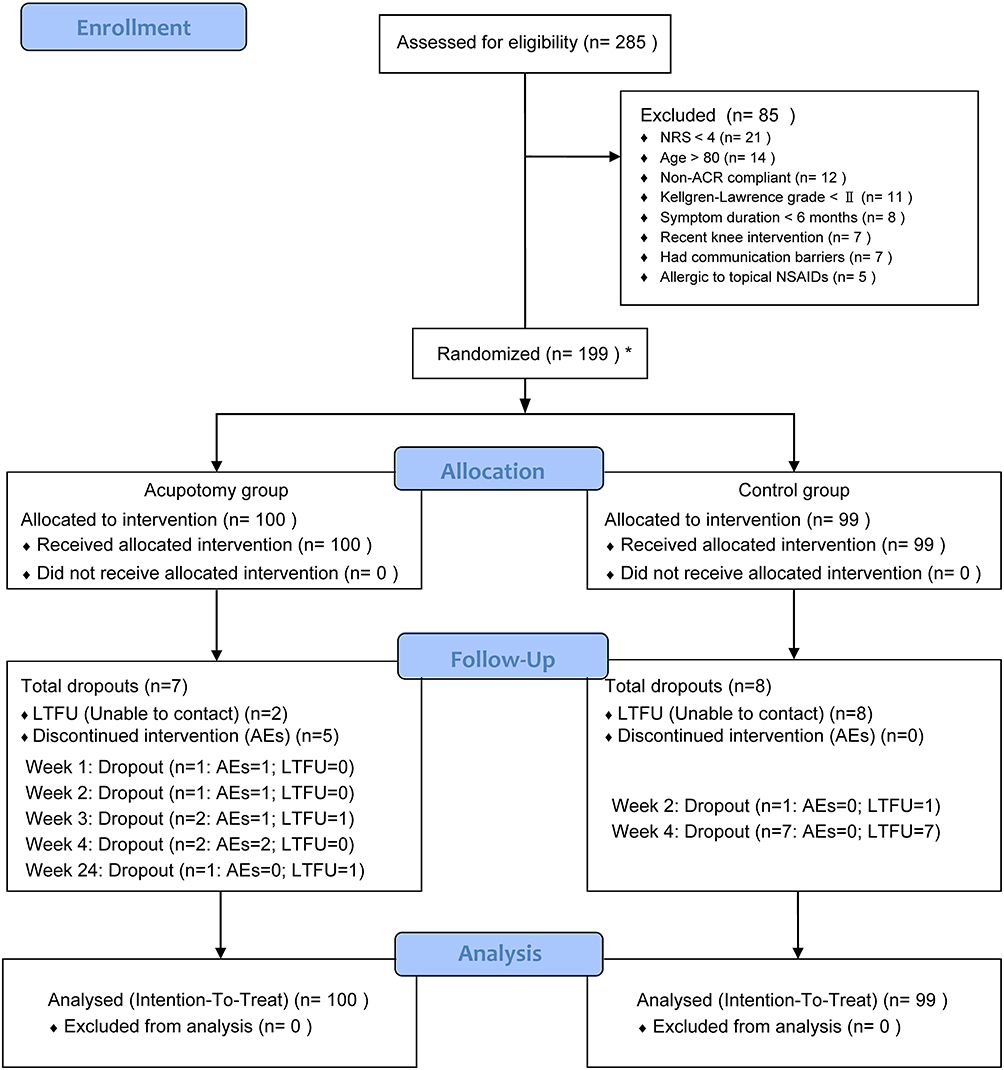 |
Figure 2 The Patient Enrollment Flowchart. * One duplicate participant was removed, resulting in 199 patients being. Abbreviations: NRS, Numerical Rating Scale; ACR, American College of Rheumatology; NSAIDs, Nonsteroidal Anti-Inflammatory Drugs; AEs, Adverse Events; LTFU, Loss to Follow-Up. |
For the primary outcome in the ITT population without imputation, the response rate at week 4 in the acupotomy group was higher than that in the control group (92.55% vs 61.54%; difference, 31.01%; 95% CI, 19.70%-42.33%; P < 0.001). The benefit persisted at subsequent time points, with rates at week 8 (91.49% vs 59.34%; difference, 32.15%; 95% CI, 20.59%-43.71%; P < 0.001) and week 24 (90.32% vs 38.46%; difference, 51.86%; 95% CI, 40.20%-63.52%; P < 0.001) (Table 2 and Figure 3). The robustness of our findings was supported by sensitivity analyses using different imputation methods, adjusted logistic regression, and per-protocol analysis (eTables 3 and 4 of Supplement 2). Subgroup analyses by age, BMI, and sex showed consistent treatment effects across subgroups, with no significant interactions (eTables 5 and 6 of Supplement 2).
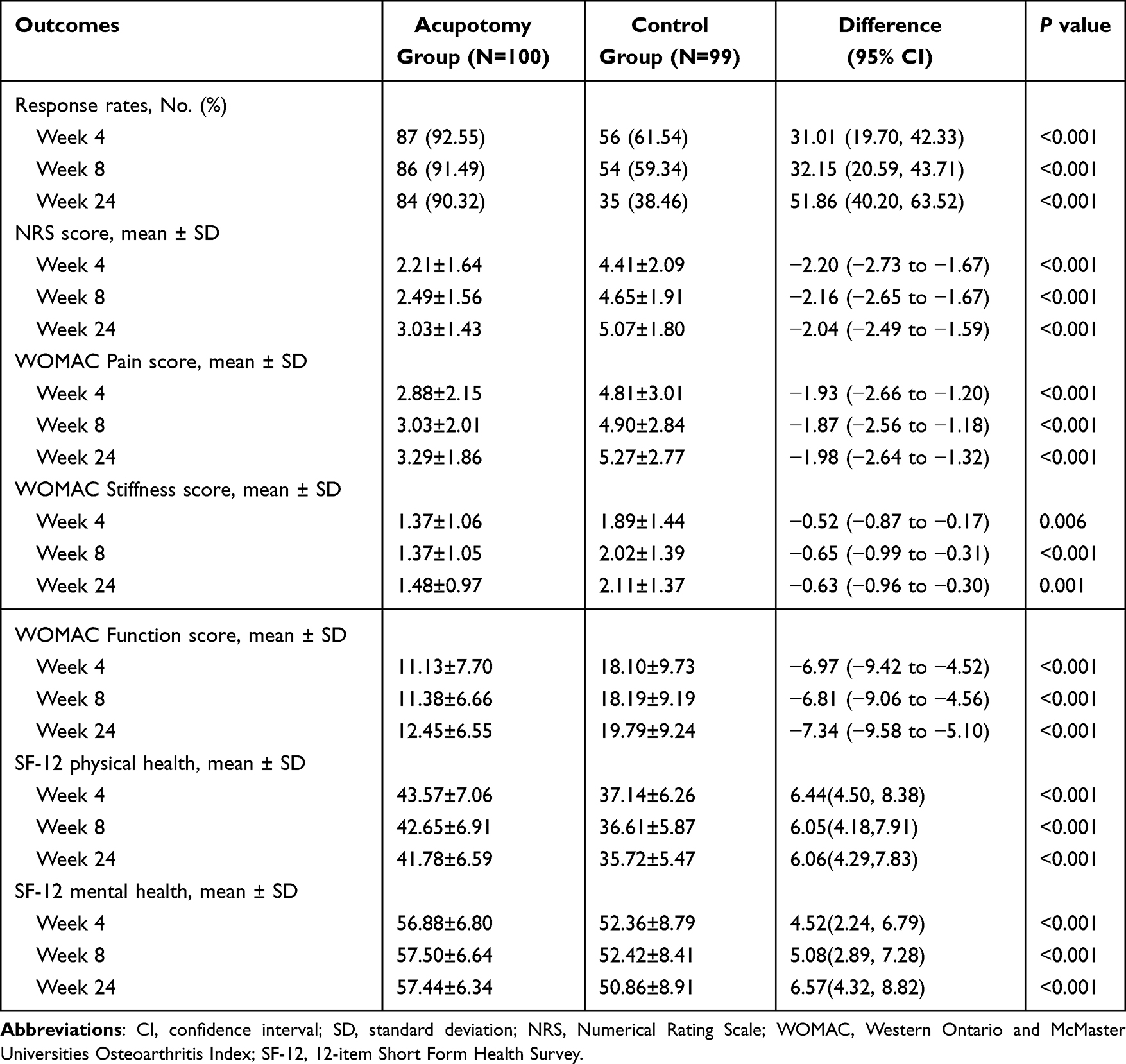 |
Table 2 Primary and Secondary Outcomes of This Study Without Imputation |
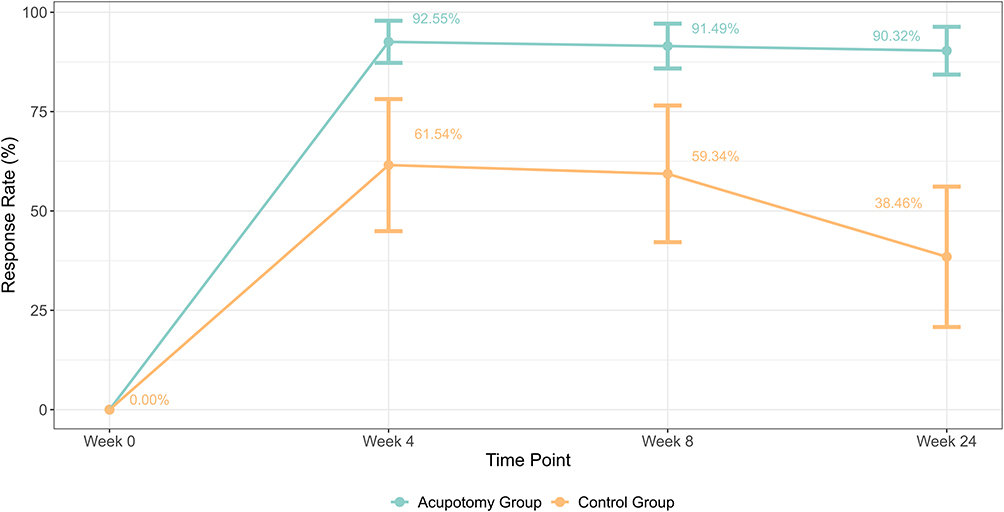 |
Figure 3 Trajectory of Response Rates Over Time Between Groups. Bars show the 95% CI. |
Consistent improvements were observed in the acupotomy group across secondary outcomes. At week 4, the NRS scores indicated a substantial reduction in the acupotomy group compared to the control group (2.21±1.64 vs 4.41±2.09; difference, −2.20; 95% CI, −2.73 to −1.67; P < 0.001). These improvements persisted at weeks 8 (2.49±1.56 vs 4.65±1.91; difference, −2.16; 95% CI, −2.65 to −1.67; P < 0.001) and 24 (3.03±1.43 vs 5.07±1.80; difference, −2.04; 95% CI, −2.49 to −1.59; P < 0.001). Similarly, the WOMAC function scores demonstrated significant enhancements in the acupotomy group at week 4 (11.13±7.70 vs 18.10±9.73; difference, −6.97; 95% CI, −9.42 to −4.52; P < 0.001), with sustained improvements noted at weeks 8 (11.38±6.66 vs 18.19±9.19; difference, −6.81; 95% CI, −9.06 to −4.56; P < 0.001) and 24 (12.45±6.55 vs 19.79±9.24; difference, −7.34; 95% CI, −9.58 to −5.10; P < 0.001). Further details on outcomes are provided in Table 2.
No patients required rescue medication in both groups during the first 8 weeks. By week 24, 6 (6.00%) patients used rescue medication in the acupotomy group and 8 (8.08%) in the control group (P = 0.59).
Five (5.10%) patients in the acupotomy group experienced adverse events (one occurred in week 1, one in week 2, one in week 3, and two in week 4). The most common were persistent post-treatment pain, defined as pain lasting over 24 hours and exceeding 4 on the NRS, affecting 4 (4.08%) patients. One patient (1.02%) experienced needle intolerance—manifested as severe anxiety or autonomic symptoms during manipulation—and subsequently discontinued treatment and follow-up.
Discussion
Our RCT showed that compared with diclofenac diethylamine emulgel alone, acupotomy combined with diclofenac diethylamine emulgel effectively alleviates pain, reduces stiffness, enhances functional capacity, and improves quality of life through week 24.
Our study demonstrated substantial response rates of 92.55% for acupotomy combining with diclofenac diethylamine emulgel at week 4. Another RCT that evaluated intensive acupuncture for knee OA used the identical outcome measures. That acupuncture study reported response rates of 45.0% for the electroacupuncture (EA) group and 41.4% for the manual acupuncture (MA) group at week 4. The superior response rate observed is likely attributable to the combined effects of diclofenac reducing inflammation and pain and acupotomy addressing structural issues.38
A previous study evaluated the combination of acupotomy with intra-articular sodium hyaluronate for treating knee OA.39 After 4 weeks of treatment, that study reported WOMAC pain scores of 2.7±1.9, stiffness scores of 1.0±0.7, and function scores of 12.2±7.1, while our study showed similar result (pain scores of 2.88±2.15, stiffness scores of 1.37±1.06, and function scores of 11.13±7.70). This comparison highlights the versatility of acupotomy as a treatment option, supporting its potential as a complementary therapy alongside other treatments for knee OA.25
The effectiveness of acupotomy in treating knee OA may be attributed to a combination of anti-inflammatory, neuromodulatory, and biomechanical effects. Experimental and preclinical studies suggest that acupotomy may attenuate joint inflammatory responses and cartilage catabolism, help preserve extracellular matrix integrity, and may modulate pain-related neurotransmitter systems in the central nervous system, thereby raising the pain threshold and reducing symptom intensity.21,40 In addition, acupotomy has been reported to release periarticular adhesions and contractures, reduce abnormal mechanical stress, and may improve joint mobility, with animal models suggesting favorable changes in the biomechanical properties of periarticular muscles and tendons.41–44
Consistent with these mechanistic considerations, we adopted a fixed combination of local and proximal acupoints that reflects a standardized acupotomy regimen at our center. Dubi (ST35) and Neixiyan (EX-LE4) are among the most frequently used local points for knee OA and lie adjacent to the patellofemoral joint capsule and peripatellar soft tissues, making them suitable targets for releasing periarticular adhesions and reducing anterior knee pain and stiffness.45,46 Xiyangguan (GB33), located lateral to the knee joint, is conventionally used for lateral knee pain and tendon tightness and has been reported to influence deep periarticular tissue perfusion, supporting its use to address lateral soft-tissue tension and joint mechanics.47 Shiqizhui (EX-B8) and Yaoyangguan (GV3) are lumbosacral points commonly indicated for low back pain and lower-limb dysfunction; their inclusion was intended to modulate the lumbosacral–lower-limb kinetic chain and neuromuscular control, thereby complementing the local periarticular effects at the knee.48
We chose topical NSAIDs as the co-intervention for several compelling reasons. First topical NSAIDs have been proven effective for pain relief in knee OA, with a more favorable safety profile compared to oral NSAIDs. This aligns perfectly with our study’s focus on providing effective and low-risk treatment options.49 Second, the localized nature of acupotomy’s therapeutic effects warrants a topical rather than systemic comparator, to allow for a more precise assessment of acupotomy’s incremental benefits. Finally, diclofenac diethylamine emulgel, a widely accessible topical NSAID recommended in many authoritative OA guidelines, serves as a highly clinically relevant and appropriate control.
Acupotomy produced only mild, self-limited adverse events and no serious treatment-related complications. Although these findings indicate a favorable short-term safety profile, the sample size and single-center design limit conclusions regarding rare events, and further safety assessment in larger cohorts remains warranted.
Limitations
This trial has several limitations. Because acupotomy is an invasive procedure with characteristic tactile sensations, blinding of patients and practitioners was not feasible. This limitation may introduce expectation or performance bias. To reduce detection bias, outcome assessment and statistical analysis were conducted by blinded personnel using standardized instruments. The single-center setting and the use of one highly experienced practitioner for all acupotomy procedures may limit the extent to which these findings can be generalized to practitioners with varying levels of expertise or to different clinical environments. Moreover, the trial population was predominantly male, which may limit the generalizability of these findings, particularly to women with knee OA. Although both groups were permitted to use loxoprofen sodium tablets as rescue medication under an identical protocol, and no significant between-group differences in usage were observed, the possibility of a modest nondifferential analgesic effect cannot be completely excluded. The high response rate in the acupotomy group should be interpreted cautiously, as it may partly reflect practitioner expertise and the characteristics of a single-center cohort. Lastly, although subjective outcomes like the NRS and WOMAC scores are validated, incorporating objective metrics in future studies could enhance the robustness of the findings.
A prior observational analysis from our group used only the baseline demographic and clinical data from this cohort to compare large-language-model–generated versus clinician-written patient education materials. No randomization procedures, treatment allocations, follow-up assessments, or clinical or safety outcomes related to acupotomy from the present RCT were included in that publication. We cite this work for transparency regarding data reuse and to clarify that the current manuscript is the first to report the randomized interventional outcomes and safety profile of acupotomy in this cohort.50
Conclusions
Acupotomy combined with topical diclofenac, compared with topical diclofenac alone, resulted in reduced pain and improved function among patients with knee OA. Acupotomy combined with topical NSAIDs shows promise as an adjunctive, non-surgical option for knee OA management, but confirmation in multicenter, blinded trials is warranted.
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Abbreviations
NSAIDs, non-steroidal anti-inflammatory drugs; RCTs, randomized controlled trials; ACR, American College of Rheumatology; NRS, numerical rating scale; MCII, minimal clinically important improvement; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; ITT, Intention-To-Treat; PP, Per-Protocol; SD, standard deviation; IQR, interquartile ranges; LOCF, Last Observation Carried Forward; EA, electroacupuncture; MA, manual acupuncture.
Data Sharing Statement
Deidentified data supporting the findings of this study are available for non-commercial research purposes by academic or public health researchers who submit a sound methodological proposal. Requests can be made within one-year post-publication to the corresponding author at [email protected]. The sharing of data will be subject to approval, and only data relevant to the proposed research will be provided.
Ethic Approval Statement
This study was conducted at the Beijing Hospital of Traditional Chinese Medicine affiliated with Capital Medical University. The study protocol was reviewed and approved by the Medical Ethical Review Committee of the Beijing Hospital of Traditional Chinese Medicine (No. 2020BL02-057-02). All procedures were performed in accordance with the ethical standards laid down in the Declaration of Helsinki. The trial was registered with the Chinese Clinical Trial Registry (ChiCTR) under the registration number ChiCTR2100043005 (https://www.chictr.org.cn/showproj.html?proj=121348).
Acknowledgments
We would like to express our sincere gratitude to all the patients who participated in this study. Their cooperation and commitment were invaluable to the successful completion of this research. Figure 1 and eFigure in Supplement 3 were created using BioRender.com.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Dr. Shu-Ming Li was supported by Capital’s Funds for Health Improvement and Research (No. 2020-2-2231).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Duong V, Oo WM, Ding C, Culvenor AG, Hunter DJ. Evaluation and Treatment of Knee Pain: a Review. JAMA. 2023;330(16):1568–1580. doi:10.1001/jama.2023.19675
2. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
3. Battistelli M, Favero M, Burini D, et al. Morphological and ultrastructural analysis of normal, injured and osteoarthritic human knee menisci. Eur J Histochem. 2019;63(1):2998. doi:10.4081/ejh.2019.2998
4. Sanchez-Lopez E, Coras R, Torres A, Lane NE, Guma M. Synovial inflammation in osteoarthritis progression. Nat Rev Rheumatol. 2022;18(5):258–275. doi:10.1038/s41584-022-00749-9
5. Pettenuzzo S, Berardo A, Belluzzi E, et al. Mechanical insights into fat pads: a comparative study of infrapatellar and suprapatellar fat pads in osteoarthritis. Connect Tissue Res. 2025;66(4):272–283. doi:10.1080/03008207.2025.2502591
6. Zhu X, Chan YT, Yung PSH, Tuan RS, Jiang Y. Subchondral Bone Remodeling: a Therapeutic Target for Osteoarthritis. Front Cell Dev Biol. 2020;8:607764. doi:10.3389/fcell.2020.607764
7. Steinmetz JD, Culbreth GT, Haile LM, et al. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
8. Courties A, Kouki I, Soliman N, Mathieu S, Sellam J. Osteoarthritis year in review 2024: epidemiology and therapy. Osteoarthritis Cartilage. 2024;32(11):1397–1404. doi:10.1016/j.joca.2024.07.014
9. Garstang SV, Stitik TP. Osteoarthritis: epidemiology, Risk Factors, and Pathophysiology. Am J Phys Med Rehabil. 2006;85(11):S2. doi:10.1097/01.phm.0000245568.69434.1a
10. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022;30(2):184–195. doi:10.1016/j.joca.2021.04.020
11. Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of Hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. doi:10.1001/jama.2020.22171
12. Gregori D, Giacovelli G, Minto C, et al. Association of Pharmacological Treatments With Long-term Pain Control in Patients With Knee Osteoarthritis: a Systematic Review and Meta-analysis. JAMA. 2018;320(24):2564–2579. doi:10.1001/jama.2018.19319
13. Goff AJ, De Oliveira Silva D, Merolli M, Bell EC, Crossley KM, Barton CJ. Patient education improves pain and function in people with knee osteoarthritis with better effects when combined with exercise therapy: a systematic review. J Physiother. 2021;67(3):177–189. doi:10.1016/j.jphys.2021.06.011
14. McAlindon TE, LaValley MP, Harvey WF, et al. Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis. JAMA. 2017;317(19):1967–1975. doi:10.1001/jama.2017.5283
15. Zeng C, Lane NE, Hunter DJ, et al. Intra-articular corticosteroids and the risk of knee osteoarthritis progression: results from the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2019;27(6):855–862. doi:10.1016/j.joca.2019.01.007
16. da Costa BR, Reichenbach S, Keller N, et al. Effectiveness of non-steroidal anti-inflammatory drugs for the treatment of pain in knee and Hip osteoarthritis: a network meta-analysis. Lancet. 2017;390(10090):e21–e33. doi:10.1016/S0140-6736(17)31744-0
17. Ferket BS, Feldman Z, Zhou J, Oei EH, Bierma-Zeinstra SMA, Mazumdar M. Impact of total knee replacement practice: cost effectiveness analysis of data from the Osteoarthritis Initiative. BMJ. 2017;356:j1131. doi:10.1136/bmj.j1131
18. Skou Søren T, Roos Ewa M, Laursen Mogens B, et al. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med. 2015;373(17):1597–1606. doi:10.1056/NEJMoa1505467
19. Kwon CY, Yoon SH, Lee B. Clinical effectiveness and safety of acupotomy: an overview of systematic reviews. Complement Ther Clin Pract. 2019;36:142–152. doi:10.1016/j.ctcp.2019.07.002
20. Yoon SH, Kim YS, Jo HG, Kwon CY. Current Usage of Terminologies Related to Acupotomy: a Literature Research and Standardization Suggestion. Chin J Integr Med. 2019;25(2):147–150. doi:10.1007/s11655-018-3015-1
21. Ma SN, guo XZ, Guo Y, et al. Effect of Acupotomy on FAK-PI3K Signaling Pathways in KOA Rabbit Articular Cartilages. Evid Based Complement Alternat Med. 2017;2017:4535326. doi:10.1155/2017/4535326
22. Xie K, Pan X, Huang F, et al. Needle knife therapy plus sodium hyaluronate injection for knee osteoarthritis: a protocol for a systematic review and meta-analysis. Medicine. 2020;99(46):e23242. doi:10.1097/MD.0000000000023242
23. Xu D, Lee M, Huang C, et al. Effect of acupotomy in knee osteoarthritis patients: study protocol for a randomized controlled trial. Trials. 2021;22(1):295. doi:10.1186/s13063-021-05247-z
24. Sun J, Zhao Y, Zhu R, et al. Acupotomy Therapy for Knee Osteoarthritis Pain: systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2020;2020(1):2168283. doi:10.1155/2020/2168283
25. Peng CY, Qiang HX, Zhi CJ. Acupotomy combined with intra-articular injection of sodium hyaluronate in the treatment of knee osteoarthritis. Medicine. 2022;101(35):e30225. doi:10.1097/MD.0000000000030225
26. Di A, Xu D, Zhang A, et al. Acupotomy for knee osteoarthritis: literature review and meta-analysis. J Back Musculoskelet Rehabil. 2025;2025:10538127251349150. doi:10.1177/10538127251349150
27. Zhang J, Pang T, Yao J, et al. Acupotomy therapy for knee osteoarthritis: an overview of systematic reviews. Medicine. 2024;103(47):e39700. doi:10.1097/MD.0000000000039700
28. Li SM, Li TL, Guo R, et al. Effectiveness and safety of acupotomy for knee osteoarthritis: study protocol for a randomized controlled trial. Trials. 2021;22(1):824. doi:10.1186/s13063-021-05786-5
29. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
30. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part I. Osteoarthritis of the Hip. American College of Rheumatology. Arthritis Rheum. 1995;38(11):1535–1540. doi:10.1002/art.1780381103
31. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
32. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(11):S240–S252. doi:10.1002/acr.20543
33. Derry S, Conaghan P, Da Silva JAP, Wiffen PJ, Moore RA. Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2016;2016(4):CD007400. doi:10.1002/14651858.CD007400.pub3
34. Greig SL, Garnock-Jones KP. Loxoprofen: a Review in Pain and Inflammation. Clin Drug Investig. 2016;36(9):771–781. doi:10.1007/s40261-016-0440-9
35. Tubach F, Ravaud P, Baron G, et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and Hip osteoarthritis: the minimal clinically important improvement. Ann Rheum Dis. 2005;64(1):29–33. doi:10.1136/ard.2004.022905
36. Xie F, Li SC, Goeree R, et al. Validation of Chinese Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) in patients scheduled for total knee replacement. Qual Life Res. 2008;17(4):595–601. doi:10.1007/s11136-008-9340-7
37. Fong DYT, Chan BKY, Li S, Wan CH, Kazis LE. Average and individual differences between the 12-item MOS Short-form Health Survey version 2 (SF-12 V.2) and the veterans RAND 12-item Health Survey (VR-12) in the Chinese population. Health Qual Life Outcomes. 2022;20:102. doi:10.1186/s12955-022-02010-z
38. Tu JF, Yang JW, Shi GX, et al. Efficacy of Intensive Acupuncture Versus Sham Acupuncture in Knee Osteoarthritis: a Randomized Controlled Trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
39. Zhang X, Sun X, Chen G. Effect of the combinative use of acupotomy therapy and ultrasonic drug penetration in treating knee joint osteoarthritis. QJM: Int J Med. 2022;115(1):12–16. doi:10.1093/qjmed/hcaa278
40. Ji B, Guo C, Jin Y, Zhong D, Chen Y, Guo M. Effects of acupotome and electro-acupuncture on pain threshold and monoamine-neurotransmitters of central nerves in rats with knee osteoarthritis. Chinese J Pathophysiol. 2010;26(6):1091–1095.
41. LongFei X, Yan G, XiLin C, et al. Application of Acupotomy in a Knee Osteoarthritis Model in Rabbit. J Vis Exp. 2023;2023(200):1. doi:10.3791/65584
42. Zhang W, Gao Y, Guo C, Ibrahim Zeyad Ali K, Farid M. Effect of acupotomy versus electroacupuncture on ethology and morphology in a rabbit model of knee osteoarthritis. J Tradit Chin Med. 2019;39(2):229–236.
43. Lin M, Li X, Liang W, et al. Needle-knife therapy improves the clinical symptoms of knee osteoarthritis by inhibiting the expression of inflammatory cytokines. Exp Ther Med. 2014;7(4):835–842. doi:10.3892/etm.2014.1516
44. Guo Y, Xu Y, He M, et al. Acupotomy Improves Synovial Hypoxia, Synovitis and Angiogenesis in KOA Rabbits. JPR. 2023;16:749–760. doi:10.2147/JPR.S396955
45. Yao K, Shamim MF, Xia J, Liu TT, Guo Y, Lin X. Therapeutic Potential of Acupuncture in Knee Osteoarthritis: clinical Efficacy and Mechanistic Insights. JIR. 2025;18:12169–12190. doi:10.2147/JIR.S526890
46. Jia P, Liu J, Li L, et al. Acupuncture for knee osteoarthritis with sensitized acupoints: results from a pilot, feasibility randomized controlled trial. Pilot Feasibility Stud. 2020;6(1):144. doi:10.1186/s40814-020-00687-x
47. Litscher G, Ofner M, He W, Wang L, Gaischek I. Acupressure at the Meridian Acupoint Xiyangguan (GB33) Influences Near-Infrared Spectroscopic Parameters (Regional Oxygen Saturation) in Deeper Tissue of the Knee in Healthy Volunteers. Evid Based Complement Alternat Med. 2013;2013:370341. doi:10.1155/2013/370341
48. Chen H, Yeung WF, Yang M, et al. Acupuncture for low back pain: a clinical practice guideline from the Hong Kong taskforce of standardized acupuncture practice. J Tradit Chin Med. 2022;42(1):140–147. doi:10.19852/j.cnki.jtcm.2022.01.009
49. da Costa BR, Pereira TV, Saadat P, et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and Hip osteoarthritis: network meta-analysis. BMJ. 2021;375:n2321. doi:10.1136/bmj.n2321
50. Du K, Li A, Zuo QH, et al. Comparing Artificial Intelligence-Generated and Clinician-Created Personalized Self-Management Guidance for Patients With Knee Osteoarthritis: blinded Observational Study. J Med Internet Res. 2025;27:e67830. doi:10.2196/67830
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a New Patient-Reported Outcome Measure in the Arabic Language for Patients with Knee Osteoarthritis in Saudi Arabia
Alotaibi AD, Vennu V, BinNasser AS, Idres M, Mohammed A, Aldawai H, Bindawas SM
Patient Preference and Adherence 2023, 17:187-198
Published Date: 19 January 2023
An Evaluation of Different Strategies for Sampling Controls in an Online Case-Crossover Study of Acute Flares in Knee Osteoarthritis
Rathod-Mistry T, Peat G, Neogi T, Thomas MJ
Clinical Epidemiology 2023, 15:635-644
Published Date: 16 May 2023
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024
A Retrospective Follow-Up Study of Satisfaction in Patients Undergoing Unicompartmental Knee Arthroplasty: A 3-Month Postoperative Analysis
Wang M, Cao X, Zhang X, Liu H
Journal of Pain Research 2025, 18:6617-6625
Published Date: 9 December 2025
Intraspinal versus Extraspinal Acupotomy Decompression, or Their Combination, for Lumbar Disc Herniation: Protocol for a Three-Arm, Randomized, Single-Blind Controlled Trial
Yang W, Liu H, Liu M, Liu L, Liu F, Dong Z, Li X
Journal of Pain Research 2026, 19:584489
Published Date: 13 February 2026