Back to Journals » Journal of Pain Research » Volume 18
A Retrospective Follow-Up Study of Satisfaction in Patients Undergoing Unicompartmental Knee Arthroplasty: A 3-Month Postoperative Analysis
Authors Wang M, Cao X, Zhang X, Liu H
Received 3 July 2025
Accepted for publication 4 November 2025
Published 9 December 2025 Volume 2025:18 Pages 6617—6625
DOI https://doi.org/10.2147/JPR.S551410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Mengsha Wang, Xuyang Cao, Xiaoling Zhang, Huiqing Liu
Department of Joint Orthopaedics, North China Medical Xingtai General Hospital, Xingtai, Hebei, People’s Republic of China
Correspondence: Mengsha Wang, Department of Joint Orthopaedics, North China Medical Xingtai General Hospital, No. 202 Bayi Street, Xindu District, Xingtai, Hebei, 054000, People’s Republic of China, Tel +86-15833706572, Email [email protected]
Purpose: This study aims to evaluate early postoperative treatment satisfaction among patients with severe knee osteoarthritis (KOA) undergoing unicompartmental knee arthroplasty (UKA) and to identify modifiable factors influencing this outcome, informing strategies to improve patient care pathways.
Methods: A retrospective analysis of 99 severe KOA patients undergoing UKA was conducted, with satisfaction levels assessed three months postoperatively. Patients were stratified into satisfied and dissatisfied groups. Differences in demographic, clinical, and psychological variables were analyzed using appropriate statistical tests. Binary logistic regression was used to identify independent predictors of dissatisfaction. A post-hoc power analysis confirmed the study was adequately powered to detect the observed difference in the primary anthropometric variable (Body Mass Index) between groups.
Results: Twenty-one patients (21.2%) reported dissatisfaction. Significant differences were observed in age, BMI, waist circumference, Self-Rating Anxiety Scale (SAS), and Self-Rating Depression Scale (SDS) scores (all P< 0.05). Notably, the receipt of a preoperative preventive pain psychological intervention was also significantly associated with higher satisfaction in univariate analysis (P=0.008). The dissatisfied group exhibited higher Visual Analog Scale (VAS) pain scores throughout the three-month follow-up. The final multivariate logistic regression model, which identified BMI, waist circumference, and 1-month VAS score as independent predictors, showed excellent predictive accuracy (AUC=0.981).
Conclusion: Higher BMI, larger waist circumference, and greater subacute pain at one month are independent predictors of early dissatisfaction after UKA. Psychological factors, including preoperative anxiety, depression, and the lack of preventive pain psychological interventions, are also strongly associated with this outcome. Reducing postoperative pain, particularly at one month, enhances surgical outcome evaluations at this early time point. Clinicians should consider a multifactorial approach targeting these modifiable risk factors to improve satisfaction.
Keywords: knee, osteoarthritis, unicompartmental arthroplasty, patient satisfaction, postoperative rehabilitation, risk factors
Introduction
Knee osteoarthritis (KOA) is a chronic degenerative joint disease prevalent among older adults, characterized by cartilage loss and osteophyte formation that affects multiple joint structures, including the meniscus and subchondral bone, leading to chronic pain and disability.1–4 Recent epidemiological data estimate that over 140 million individuals in China are affected, with a prevalence exceeding 40% in adults aged ≥60 years.5–7 Unicompartmental knee arthroplasty (UKA) is increasingly preferred for severe medial compartment KOA due to its minimally invasive nature, faster recovery, and preserved knee kinematics compared to total knee arthroplasty.8,9 Biomechanical studies highlight UKA’s advantage in maintaining native joint biomechanics, reducing polyethylene wear, and lowering revision rates.10–12
Despite its benefits, patient satisfaction post-UKA remains variable (reported rates of dissatisfaction range from 14–30%), influenced by preoperative psychological states, pain management, and rehabilitation adherence.13 The three-month time point was chosen for this study as it represents a critical milestone in early recovery, by which time acute surgical pain should have substantially subsided, and patients have begun to form a stable perception of their functional outcomes and overall surgical success, making it a relevant period for assessing initial satisfaction.14 This study includes patients approaching or within early geriatric stages, providing insights applicable to the broader aging population undergoing this procedure. Recent pathophysiological evidence suggests that systemic inflammation and metabolic factors (eg, elevated BMI) may exacerbate postoperative pain, indirectly affecting satisfaction.15 However, there is a relative paucity of studies comprehensively analyzing the dynamics of short-term satisfaction or integrating a broad range of psychological, physiological, and anthropometric predictors in the early postoperative period for UKA patients. Understanding these early factors is crucial as they may establish the trajectory for longer-term outcomes.
The originality of this research is centered on three aspects that differentiate it from prior work. First, it specifically examines the impact of preventive pain psychological interventions on early satisfaction, a factor that has been underexplored in short-term UKA outcome studies. Second, it integrates biochemical markers with established psychosocial metrics and anthropometric data to develop a more holistic predictive framework. Third, by focusing on the early pain trajectory and identifying potentially modifiable preoperative and perioperative factors, this study seeks to provide actionable insights for optimizing care pathways to enhance patient satisfaction in the critical early recovery phase following UKA, an area where existing research has often concentrated on longer-term outcomes or a more restricted set of variables.
The primary aim of this study is to identify demographic, clinical, psychological, anthropometric, and biochemical predictors of 3-month postoperative satisfaction in patients undergoing UKA, while the secondary aim is to evaluate the correlation between early pain reduction and patient-reported satisfaction. We hypothesize that preoperative psychological support, effective pain management (reflected by lower early postoperative VAS scores), and physiological stability (eg, optimized hemoglobin levels, lower BMI) are critical determinants for optimizing short-term satisfaction in UKA patients.
Materials and Methods
Patient Information
All 99 patients undergoing unicompartmental knee arthroplasty (UKA) were retrospectively enrolled from North China Medical Xingtai General Hospital between January 2015 and April 2023. This study employed a retrospective cohort design. During this period, 128 consecutive UKA cases were screened, with 29 excluded due to incomplete data (n=18), loss to follow-up (n=8), or comorbidities significantly affecting recovery (n=3). Follow-up was conducted via a combination of telephone calls and outpatient clinic visits.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Medial compartment knee osteoarthritis confirmed by radiographic Kellgren-Lawrence grade ≥3;16 (2) Primary UKA performed by senior surgeons with >5 years of joint replacement experience; (3) Availability of complete preoperative/postoperative records. Exclusion criteria: (1) Inflammatory arthritis, active infection, or significant lateral/patellofemoral compartment involvement requiring intervention; (2) Clinically documented cognitive impairment limiting the ability to provide self-reported outcomes; (3) Concurrent malignancies or other life-threatening conditions that would confound recovery or satisfaction assessment. These criteria aimed to isolate UKA-specific outcomes by minimizing confounding factors.
Surgical Protocol and Postoperative Care
All UKA surgeries were performed under spinal anesthesia with a pneumatic tourniquet (250–300 mmHg). A standardized medial parapatellar approach and cemented fixed-bearing implants (Zimmer Biomet®) were used. Postoperative care included 24-hour multimodal analgesia (oral celecoxib 200 mg BID + intravenous tramadol 50 mg PRN), cryotherapy, and a structured rehabilitation protocol: ambulation with walker on postoperative day 1, range-of-motion exercises from day 2, and outpatient physiotherapy twice weekly for 6 weeks. The “Preventive Pain Psychological Intervention” consisted of a standardized, single 30-minute preoperative session delivered by a trained clinical nurse specialist. The session included education on the expected postoperative pain trajectory, management of patient expectations, and instruction in basic cognitive-behavioral coping strategies, such as guided relaxation and distraction techniques.
Detection Indicators
Satisfaction Assessment
Patient satisfaction was evaluated 3 months postoperatively using a 5-point Likert scale (1=very dissatisfied, 2=dissatisfied, 3=neutral, 4=satisfied, to 5=very satisfied). Patients scoring ≤3 were classified as “dissatisfied” and those scoring ≥4 as “satisfied”.17 Data validity was ensured as assessments were conducted by two trained nurses blinded to other clinical outcomes.
Psychological and Functional Metrics
Self-Rating Anxiety Scale (SAS)18 and Self-Rating Depression Scale (SDS)19 were administered preoperatively. Both scales demonstrated high internal consistency in our cohort (Cronbach’s α=0.89 for SAS, α=0.85 for SDS), confirming their reliability. The function in Activities of Daily Living (ADL) was assessed using the relevant subscale from the Knee Injury and Osteoarthritis Outcome Score (KOOS-ADL).19 The KOOS is a validated, patient-reported outcome measure specifically designed for knee conditions, including osteoarthritis, and its ADL subscale evaluates difficulty in performing daily physical activities.20
Pain Evaluation
Visual Analog Scale (VAS) scores (0=no pain, 10=worst imaginable pain) were recorded preoperatively and at postoperative day 1, day 7, 1 month, and 3 months postoperatively. The VAS showed excellent test-retest reliability (ICC=0.92) in our population.21
Statistical Methods
Data were analyzed using SPSS 25.0 (IBM Corp). Continuous variables were tested for normality via the Shapiro–Wilk test. Homogeneity of variances for t-tests was assessed using Levene’s test. Normally distributed data (mean ± SD) were compared using independent t-tests; non-parametric data (median [IQR]) used Mann–Whitney U-tests. Categorical variables (n, %) were analyzed with χ2 or Fisher’s exact tests. For repeated measures (eg, VAS trends over time and between satisfaction groups), mixed-effects models with Bonferroni correction for multiple comparisons were applied. Binary logistic regression was used to identify independent predictors of dissatisfaction; variables with P<0.1 in univariate analysis were considered for inclusion in the multivariate model, which was built using a backward stepwise (likelihood ratio) selection method. Model discrimination was assessed via Receiver Operating Characteristic (ROC) curves (Area Under the Curve [AUC] reported with 95% CI). The sample size of 99 patients, with 21 in the dissatisfied group (event rate = 21.2%), was determined retrospectively. For the primary multivariate logistic regression analysis, this sample size allowed for approximately 7 events per predictor variable (EPV) in the final three-variable model, which is within acceptable limits for exploratory studies.22 A post-hoc power analysis was conducted for the key independent t-test comparison of BMI between satisfied (25.6±2.4 kg/m2) and dissatisfied (30.5±2.5 kg/m2) groups. With an alpha of 0.05, the study achieved a power greater than 0.99 to detect the observed difference, indicating the sample was adequate for this specific comparison. Significance threshold: P<0.05.
Results
Baseline Information
This study included 99 patients undergoing UKA, with follow-up satisfaction assessed at 3 months postoperatively. The dissatisfied group comprised 21 patients (21.2%), and the satisfied group comprised 78 patients (78.8%). Demographic and clinical characteristics are detailed in Table 1. Age, BMI, waist circumference, receipt of preoperative preventive pain psychological interventions, Self-Rating Anxiety Scale (SAS), Self-Rating Depression Scale (SDS), hemoglobin (both pre- and post-operatively), and platelet levels (both pre- and post-operatively) differed significantly between the satisfied and dissatisfied groups (P<0.05, Table 1).
 |
Table 1 Baseline Information and Univariate Analysis of Factors Associated with Patient Satisfaction |
Changes in Pain and Function Scores Before and After Surgery
Preoperative to 3-month postoperative VAS scores differed significantly between groups (P<0.001, mixed-effects model). A significant time-satisfaction interaction effect was observed (P<0.001), indicating that the pattern of pain score changes over time differed between the satisfied and dissatisfied groups. The dissatisfied group consistently reported higher pain scores at all postoperative intervals (with particularly high scores on postoperative day 1, consistent with results in Table 1) (Figure 1A). ADL scores improved significantly over time for both groups (P<0.001, mixed-effects model) but differed significantly between groups at all postoperative intervals, with the satisfied group reporting better function. No significant time-satisfaction interaction was observed (P=0.722), indicating that while the absolute ADL scores differed, the trajectories of functional improvement were largely parallel between the two groups (Figure 1B).
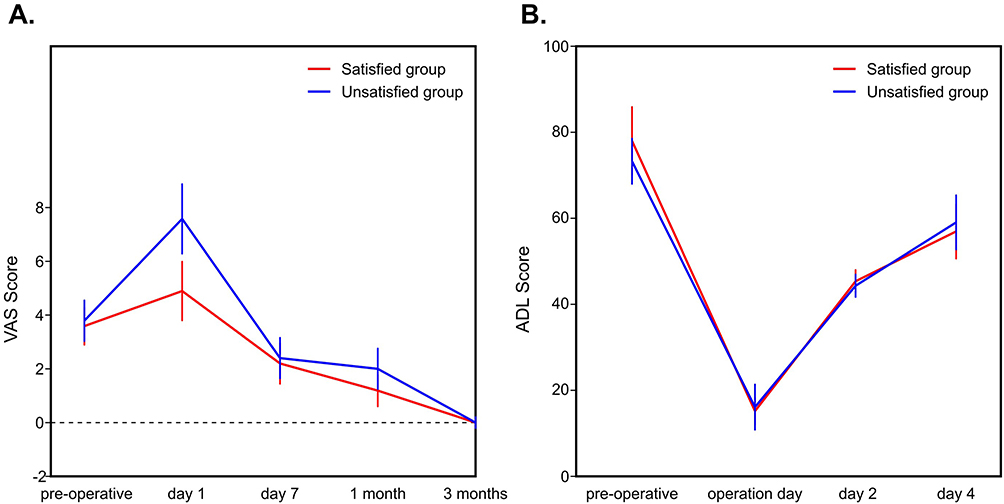 |
Figure 1 Trends in (A) VAS scores and (B) ADL scores from preoperative baseline to 3 months postoperatively, by satisfaction group. VAS: Visual Analog Scale (Higher scores indicate worse pain). ADL: Activities of Daily Living (Higher scores indicate better function). Error bars represent the 95% Confidence Interval. |
Logistic Regression Models
Binary logistic regression (dependent variable: dissatisfaction) identified BMI (OR=1.32, 95% CI: 1.05–1.66; P=0.041), waist circumference (OR=1.18, 95% CI: 1.02–1.37; P=0.028), and 1-month VAS score (OR=2.45, 95% CI: 1.35–4.44; P=0.003) as independent predictors of dissatisfaction. Age was not a significant independent predictor in the multivariate model (P=0.431). Preventive pain psychological intervention, while significant in univariate analysis (OR for “No Intervention” = 3.78, P=0.012), was not retained in the final multivariate model, possibly due to its correlation with other variables like preoperative SAS/SDS or postoperative VAS scores. More details are shown in Table 2.
 |
Table 2 Logistic Regression Results for Predictors of Dissatisfaction (3 Months Post-UKA) |
Diagnostic Value of Included Parameters
ROC analysis (Figure 2) for individual predictors revealed high diagnostic accuracy for predicting dissatisfaction for BMI (AUC=0.928), SAS (AUC=0.945), and SDS (AUC=0.945). The 1-month postoperative VAS score also showed good predictive ability (AUC=0.871). The combined multivariate logistic regression model (including BMI, waist circumference, and 1-month VAS score) achieved an excellent AUC of 0.981 (95% CI: 0.933–0.998), with a sensitivity of 90.5% and a specificity of 96.2% for predicting dissatisfaction at a model-derived probability cutoff of >0.387 (Table 3).
 |
Table 3 Area Under the ROC Curve for Selected Univariate Predictors and the Final Multivariate Model in Predicting Dissatisfaction |
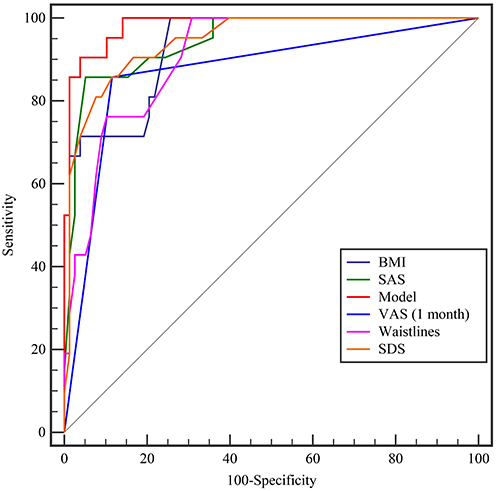 |
Figure 2 Receiver Operating Characteristic (ROC) curves for the independent predictors from the final multivariate model (BMI, Waistline, VAS at 1 month) and the combined regression model in predicting 3-month postoperative dissatisfaction. Abbreviation: AUC, Area Under the Curve. |
Discussion
This study investigated factors associated with patient satisfaction three months after unicompartmental knee arthroplasty, revealing that 21.2% of patients reported dissatisfaction at this early postoperative juncture. Our key findings indicate that higher BMI, larger waist circumference, and higher 1-month postoperative VAS scores were independent predictors of dissatisfaction. Additionally, in univariate analyses, older age, lack of preoperative preventive pain psychological intervention, higher preoperative anxiety (SAS) and depression (SDS) scores, and lower pre- and postoperative hemoglobin and platelet levels were significantly associated with dissatisfaction. These results underscore the multifactorial nature of early patient satisfaction following UKA, encompassing anthropometric, psychological, physiological, and pain-related dimensions.
Our findings regarding the strong predictive role of early postoperative pain align with studies like Singh et al (2019), who identified early postoperative pain trajectories as critical predictors of longer-term satisfaction after total knee arthroplasty.23 This study contributes to the existing literature by demonstrating that a combination of preoperative factors including psychological state (anxiety, depression), receipt of specific psychological interventions, and physiological markers (hemoglobin, platelets), alongside anthropometric measures (BMI, waist circumference), are associated with short-term satisfaction after UKA. The link between psychological distress and poorer outcomes is well-established, potentially mediated through exacerbated inflammatory responses or altered pain perception, which can delay recovery.24,25 Notably, the dissatisfied group exhibited significantly higher preoperative anxiety (mean SAS 59.0) and depression (mean SDS 56.8), supporting the hypothesis that psychosocial factors modulate pain perception pathways and influence overall satisfaction in UKA patients. These results emphasize the potential benefits of integrated biopsychosocial care models,26 which can complement traditional biomechanical-focused approaches to UKA outcome assessment.
Several limitations warrant consideration: First, the short 3-month follow-up precludes assessment of long-term satisfaction dynamics; future studies should aim for longer follow-up periods. Second, the retrospective design introduces risks of selection bias, as the 29 excluded patients may have differed systematically from the study cohort. Third, variations in individual patient adherence to the standardized rehabilitation protocol were not quantified, which could influence outcomes. Future prospective studies could incorporate objective measures (eg, wearable sensors or patient diaries) to track rehabilitation compliance. Fourth, this was a single-center study, which may limit the generalizability of the findings. Lastly, while a post-hoc power analysis for BMI showed adequate power, the exploratory nature of the study and the limited number of events per variable in the regression model mean that the findings, particularly for secondary predictors, should be interpreted with caution until confirmed in larger cohorts.
From a clinical perspective, our findings suggest an actionable framework for improving patient care. Patients presenting with risk factors such as BMI ≥27.5 kg/m2, high preoperative anxiety/depression scores, or who do not receive preventive pain psychological interventions, should be identified as being at higher risk for dissatisfaction. A 1-month VAS score indicating significant ongoing pain should prompt closer attention and potentially intensified multidisciplinary care. This could include targeted weight management advice, enhanced psychological support, and optimized pain management strategies. Such an approach could reduce dissatisfaction rates by targeting modifiable risk factors preemptively or early in the postoperative course.
Conclusion
This study identifies higher BMI, larger waist circumference, and greater subacute postoperative pain (1-month VAS score) as significant independent predictors of patient dissatisfaction three months following UKA. Additionally, factors such as preoperative psychological distress (anxiety, depression) and the absence of a preventive pain psychological intervention were associated with dissatisfaction in univariate analyses. These findings highlight the critical need for a multifactorial approach to optimizing early patient satisfaction, integrating preoperative optimization protocols that include psychological support, metabolic risk reduction, and robust perioperative and early postoperative pain control. Reducing early postoperative pain, particularly within the first month, appears to be a key element. Future prospective, multicenter studies with extended follow-up periods are necessary to confirm these findings and evaluate the cost-effectiveness of targeted interventions.
Abbreviations
VAS, Visual Analog Scale; ADL, Activities of Daily Living; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale; KOA, Knee Osteoarthritis; UKA, Unicompartmental Knee Arthroplasty; BMI, Body Mass Index; AUC, Area Under the Curve; ROC, Receiver Operating Characteristic; CI, Confidence Interval; OR, Odds Ratio; ICC, Intraclass Correlation Coefficient; SD, Standard Deviation; IQR, Interquartile Range.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available due to patient personal privacy but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The current study was conducted in accordance with the Helsinki Declaration of the World Medical Association and approved by the Ethics Committee of North China Medical Xingtai General Hospital. Informed consent was waived by the committee due to the retrospective nature of this study, which involved the analysis of anonymized data from existing medical records. Patient data confidentiality was maintained throughout the study by de-identifying all personal information prior to analysis.
Acknowledgments
We are grateful to all staff professionals and participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Xingtai Science and Technology Bureau (No. 2022ZC268).
Disclosure
The authors declare that they have no competing interests.
References
1. Gress K, Charipova K, An D, et al. Treatment recommendations for chronic knee osteoarthritis. Best Pract Res Clin Anaesth. 2020;34(3):369–382. doi:10.1016/j.bpa.2020.06.006
2. Testa G, Giardina SMC, Culmone A, et al. Intra-articular injections in knee osteoarthritis: a review of literature. J Funct Morphol Kinesiol. 2021;6(1):15. doi:10.3390/jfmk6010015
3. Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of Hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. doi:10.1001/jama.2020.22171
4. Atik I, Gul E, Atik S. Evaluation of the relationship between knee osteoarthritis and meniscus pathologies. Malawi Med J. 2024;36(1):48–52. doi:10.4314/mmj.v36i1.8
5. Chen W, Liu W, Jiang T, et al. Tongbi Huoluo Decoction alleviates cartilage degeneration in knee osteoarthritis by inhibiting degradation of extracellular matrix. Chin Med. 2023;18(1):1–21. doi:10.1186/s13020-023-00802-z
6. Summers S, Yakkanti R, Ocksrider J, et al. Effects of venous insufficiency in patients undergoing primary total knee arthroplasty: an analysis of 1.2 million patients. J Knee Surg. 2021;36(03):322–328. doi:10.1055/s-0041-1733901
7. Shao W, Hou H, Han Q, Cai K. Prevalence and risk factors of knee osteoarthritis: a cross-sectional survey in Nanjing, China. Front Public Health. 2024;12:1441408. doi:10.3389/fpubh.2024.1441408
8. Beard DJ, Davies LJ, Cook JA, et al. Total versus partial knee replacement in patients with medial compartment knee osteoarthritis: the TOPKAT RCT. Health Technol Assessment. 2020;24(20):1. doi:10.3310/hta24200
9. Hutyra CA, Gonzalez JM, Yang J-C, et al. Patient preferences for surgical treatment of knee osteoarthritis: a discrete-choice experiment evaluating total and unicompartmental knee arthroplasty. JBJS. 2020;102(23):2022–2031. doi:10.2106/JBJS.20.00132
10. Lp W, Mayr HO, Zhang X, Huang Y, Chen Y, Li Y-M. Knee scores of patients with non‐lateral compartmental knee osteoarthritis undergoing mobile, fixed‐bearing unicompartmental knee and total knee arthroplasties: a randomized controlled trial. Orthopaedic Surg. 2022;14(1):73–87. doi:10.1111/os.13111
11. Plancher KD, Briggs KK, Chinnakkannu K, et al. Isolated lateral tibiofemoral compartment osteoarthritis: survivorship and Patient Acceptable Symptom State after lateral fixed-bearing unicompartmental knee arthroplasty at mean 10-year follow-up. JBJS. 2022;104(18):1621–1628. doi:10.2106/JBJS.21.01523
12. Janssen SJ, van Oost I, Breugem SJM, van Geenen RCI. A structured evaluation of the symptomatic medial Oxford unicompartmental knee arthroplasty (UKA). EFORT Open Rev. 2021;6(10):850–860. doi:10.1302/2058-5241.6.200105
13. Nandal S, Kumar Y. Efficacy of orthotic treatment in knee osteoarthritis: a review from 2000 to 2020. Int J Health Sci Res. 2020;10(9):205–211.
14. Carr AJ, Robertsson O, Graves S, et al. Knee replacement. Lancet. 2012;379(9823):1331–1340. doi:10.1016/S0140-6736(11)60752-6
15. Christoforakis Z, Dermitzaki E, Paflioti E, et al. Correlation of systemic metabolic inflammation with knee osteoarthritis. Hormones. 2022;21(3):457–466. doi:10.1007/s42000-022-00381-y
16. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheumatic Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
17. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthopaedics Related Res. 2010;468(1):57–63. doi:10.1007/s11999-009-1119-9
18. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
19. Zung WW. A SELF-RATING DEPRESSION SCALE. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
20. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J Orthopaedic Sports Phys Ther. 1998;28(2):88–96. doi:10.2519/jospt.1998.28.2.88
21. Ahmed M, Bux M, Kumar M, Ahmed N, Hussain G, Ishtiyaque M. Proximal fibular osteotomy in the management of osteoarthritis of medial compartment of knee joint. Cureus. 2020;12(6).
22. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
23. Singh JA, Lemay CA, Nobel L, et al. Association of early postoperative pain trajectories with longer-term pain outcome after primary total knee arthroplasty. JAMA Network Open. 2019;2(11):e1915105. doi:10.1001/jamanetworkopen.2019.15105
24. Rohleder N. Stimulation of systemic low-grade inflammation by psychosocial stress. Psychosomatic Med. 2014;76(3):181–189. doi:10.1097/PSY.0000000000000049
25. Riddle DL, Reza Jafarzadeh S. Effects of psychological distress on the general health to self-reported pain and function outcome relationship in knee arthroplasty: a causal mediation study. Osteoarthritis Cartilage Open. 2022;4(4):100315. doi:10.1016/j.ocarto.2022.100315
26. Rahman MH, Nam Y, Kim JH, Lee WH, Suk K. Optogenetics of the spinal cord: use of channelrhodopsin proteins for interrogation of spinal cord circuits. Curr Protein Pept Sci. 2018;19(7):714–724. doi:10.2174/1389203719666171229230012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a New Patient-Reported Outcome Measure in the Arabic Language for Patients with Knee Osteoarthritis in Saudi Arabia
Alotaibi AD, Vennu V, BinNasser AS, Idres M, Mohammed A, Aldawai H, Bindawas SM
Patient Preference and Adherence 2023, 17:187-198
Published Date: 19 January 2023
An Evaluation of Different Strategies for Sampling Controls in an Online Case-Crossover Study of Acute Flares in Knee Osteoarthritis
Rathod-Mistry T, Peat G, Neogi T, Thomas MJ
Clinical Epidemiology 2023, 15:635-644
Published Date: 16 May 2023
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024
Effectiveness of Acupotomy Combined with Topical Diclofenac for Knee Osteoarthritis: A Randomized Controlled Trial
Du K, Cheng WZ, Li A, Zhang CY, Yan SY, Han F, Guo R, Chen P, Du WS, Zuo YL, Zuo QH, Li SM
Journal of Pain Research 2025, 18:6779-6790
Published Date: 17 December 2025