Back to Journals » Journal of Pain Research » Volume 19
Intraspinal versus Extraspinal Acupotomy Decompression, or Their Combination, for Lumbar Disc Herniation: Protocol for a Three-Arm, Randomized, Single-Blind Controlled Trial
Authors Yang W ![]() , Liu H, Liu M, Liu L, Liu F
, Liu H, Liu M, Liu L, Liu F ![]() , Dong Z, Li X
, Dong Z, Li X
Received 26 November 2025
Accepted for publication 29 January 2026
Published 13 February 2026 Volume 2026:19 584489
DOI https://doi.org/10.2147/JPR.S584489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Wenlong Yang,1,2 Hailiang Liu,2 Muqing Liu,1 Lei Liu,2 Fangming Liu,2 Zike Dong,1 Xueqi Li1
1School of Acupuncture-Tuina, Shandong University of Traditional Chinese Medicine, Jinan, Shandong Province, People’s Republic of China; 2Department of Pain Medicine, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Institute of Anesthesia and Respiratory Critical Medicine, Jinan, Shandong Province, People’s Republic of China
Correspondence: Wenlong Yang, Department of Pain Medicine, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Institute of Anesthesia and Respiratory Critical Medicine, No. 16766 Jingshi Road, Jinan, Shandong Province, 250014, People’s Republic of China, Email [email protected] Fangming Liu, Department of Pain Medicine, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Institute of Anesthesia and Respiratory Critical Medicine, No. 16766 Jingshi Road, Jinan, Shandong Province, 250014, People’s Republic of China, Email [email protected]
Background: Acupotomy is a minimally invasive procedure integrating traditional Chinese medicine principles with modern anatomy. While effective for low back pain in lumbar disc herniation (LDH), its efficacy for radicular symptoms from nerve root compression remains limited. A novel technique, intraspinal acupotomy decompression, targets the meningovertebral ligaments (MVL) to alleviate neural compression. This study aims to evaluate and compare the clinical efficacy of intraspinal decompression, extraspinal decompression, and their combination for LDH.
Methods: This is a three-arm, randomized, single-center, single-blind (assessor-blinded) controlled trial. Due to the nature of the interventions, participants and practitioners cannot be blinded. The planned sample size is 210 eligible LDH patients aged 20– 85, who will be randomly allocated to one of three groups (n=70 each): the extraspinal acupotomy group, the intraspinal acupotomy group, or the combined group. All groups will receive one treatment session per week for four weeks. The primary outcomes are pain intensity (Visual Analogue Scale, VAS) and lumbar function (Japanese Orthopaedic Association Score, JOA), assessed at baseline, 4 weeks (post-treatment), and 8 weeks (primary endpoint). The secondary outcomes include quality of life (36-Item Short Form Health Survey, SF-36) and adverse events, assessed at 8 weeks.
Conclusion: This study will provide high-quality evidence on the efficacy of a novel intraspinal acupotomy technique. The findings will help determine the optimal acupotomy decompression strategy for LDH, potentially offering a more effective minimally invasive option for patients with radicular symptoms.
Trial Registration: International Traditional Medicine Clinical Trial Registry (ITMCTR2025001872). Registered on 25 September 2025.
Keywords: acupotomy, intraspinal decompression, lumbar disc herniation, randomized controlled trial
Introduction
Lumbar Disc Herniation (LDH) is a prevalent cause of lower back and leg pain, with its incidence steadily increasing in recent years.1,2 Modern lifestyle changes are a contributing factor, and the condition is now appearing at progressively younger ages.3,4 While only a minority of patients require surgery,5,6 non-surgical management often faces limitations. Conventional treatments like pharmacological therapy and physical exercise may alleviate symptoms but frequently fail to address the underlying mechanical compression of the nerve root, and their effects can be gradual or insufficient, particularly in severe cases.7,8
Lumbar disc herniation (LDH) represents a complex disorder shaped by the combined effects of central and peripheral pathophysiological mechanisms. Clinically, herniated disc material often exerts sustained compression or irritation on the nerve root, manifesting as radicular pain accompanied by sensory abnormalities and motor weakness. Importantly, the pathological process is not limited to mechanical compression alone. Biochemical substances released from the degenerated disc, together with immune-mediated reactions in the periradicular microenvironment, can induce neuroinflammatory responses that amplify nociceptive signalling and exacerbate neurological symptoms.9–11 Furthermore, adaptive changes in spinal biomechanics may increase the mechanical burden on adjacent paraspinal tissues, promoting secondary inflammation, hypertrophic changes, and progressive functional impairment.12–15 From this perspective, an ideal therapeutic approach should be capable of accurately alleviating pathological mechanical stimuli both within the spinal canal, by addressing nerve-root pathology, and beyond it, by modulating affected paraspinal soft tissues. However, current conventional interventions often lack the precision required to effectively address both targets simultaneously.16–18
Minimally invasive procedures have emerged as a promising solution. Guided by imaging techniques, they enable targeted decompression with minimal tissue damage, effectively relieving nerve root compression and associated symptoms while offering faster recovery than open surgery.19–21 Acupotomy, a distinctive therapeutic modality from traditional Chinese medicine, represents one such minimally invasive approach. It utilizes a needle-knife (0.8 mm in diameter with a 1-mm blade). The Huatuo Jiaji points (EX-B2), located 0.5 body-cun lateral to the lumbar spinous processes, serve as the primary entry points. Modern anatomy confirms these points correlate with the trajectories for facet joint injections and epidural punctures.22–24 Traditional extraspinal acupotomy at these points decompresses facet joints, muscles, and ligaments, showing notable efficacy for low back pain.25–27
Conventional acupotomy decompression mainly targets peripheral tissues and often provides insufficient relief for radicular symptoms resulting from intraspinal nerve root compression.25–27 Awareness of this limitation has prompted the development of intraspinal acupotomy decompression, a technique that enables access to the spinal canal through penetration of the ligamentum flavum and facilitates the release of restrictive structures, particularly the meningovertebral ligament (MVL). Accumulating evidence suggests that the MVL is closely involved in nerve root entrapment and plays an important role in the pathogenesis of radicular pain in lumbar disc herniation (LDH). Preliminary clinical studies indicate that intraspinal acupotomy decompression can lead to substantial improvement in radicular symptoms.28 Beyond mechanical decompression, MVL release may also exert therapeutic effects by attenuating periradicular neuroinflammation, including reductions in inflammatory mediators and perineural edema, thereby helping to alleviate peripheral sensitization and radicular pain.29,30 Nevertheless, concerns regarding procedural safety—such as dural tears, nerve root injury, and intraspinal haemorrhage—remain.31,32 Although these complications are relatively rare, they emphasize the importance of meticulous technique and rigorous safety protocols. Consistent with previous reports highlighting the value of imaging guidance in risk reduction, the present study incorporates comprehensive safety measures to ensure both efficacy and patient safety.
In current clinical practice, intraspinal and extraspinal acupotomy decompression are both used for the treatment of LDH, yet the comparative effectiveness of these approaches has not been adequately established. Notably, randomized controlled trials (RCTs) directly comparing these techniques, or assessing their potential synergistic effects when combined, are lacking. Despite growing interest in minimally invasive interventions for LDH, direct comparative evidence for different acupotomy decompression strategies remains scarce.17,21,33 Therefore, this study is designed as a three-arm RCT to rigorously evaluate and compare the clinical efficacy of intraspinal acupotomy decompression, extraspinal acupotomy decompression, and their combined application in patients with LDH.
Materials and Methods
This protocol is for a prospective, three-arm, randomized, single-blind, parallel-controlled trial. The study design and reporting will adhere to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines34 and the Consolidated Standards of Reporting Trials (CONSORT) statement,35 respectively. The trial has been approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University (Approval No. [2023] S426) and was prospectively registered with the International Traditional Medicine Clinical Trial Registry (ITMCTR2025001872) on 25 September 2025, prior to participant enrollment. The study will be conducted in accordance with the principles of the Declaration of Helsinki.36 All participants will provide written informed consent prior to any study procedures. Participant enrollment, randomization, allocation, follow-up, and analysis throughout the trial are summarized in Figure 1.
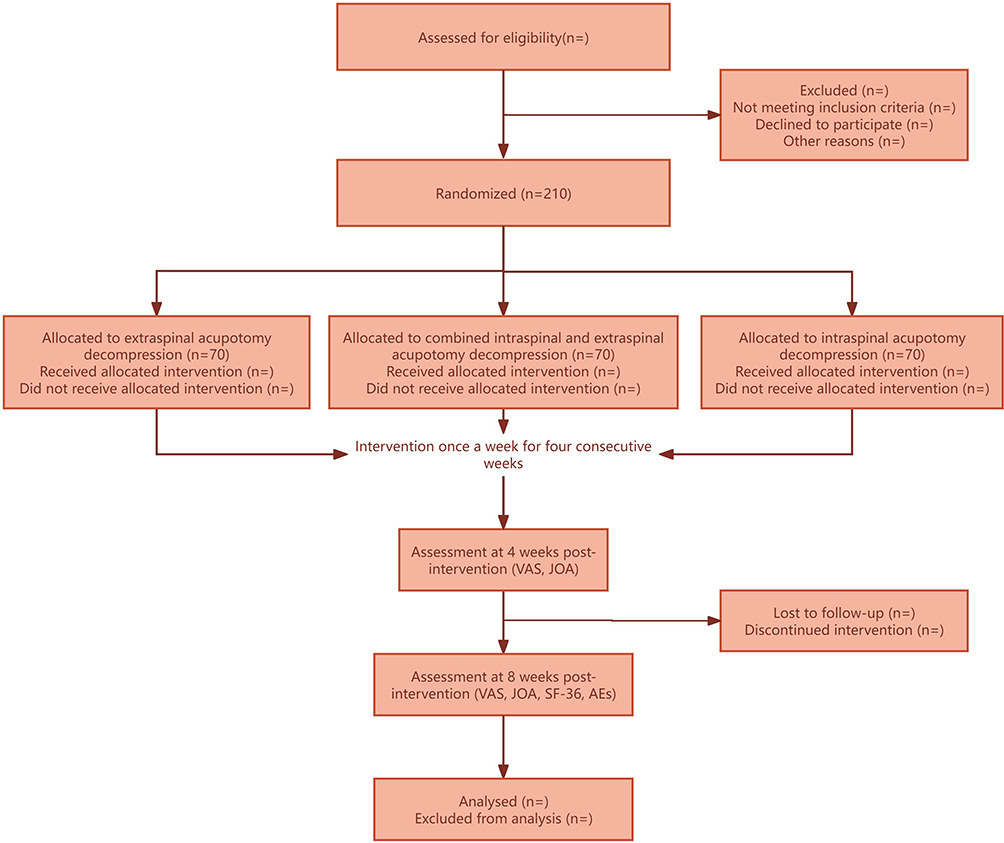 |
Figure 1 Flow diagram of participant enrollment, randomization, allocation, follow-up, and analysis. |
Participants
This study aims to recruit 210 patients diagnosed with lumbar disc herniation who are seeking treatment at the Department of Pain Medicine, The First Affiliated Hospital of Shandong First Medical University, and Shandong Provincial Qianfoshan Hospital, between October 1, 2025, and December 31, 2025. Eligible participants will be included if they provide informed consent and meet the following criteria:
- A confirmed diagnosis of lumbar disc herniation, based on established diagnostic criteria.36–39
- Participants were required to present with lower back pain radiating to the lower limbs, verified by CT or MRI findings demonstrating pathological changes consistent with the corresponding symptomatic spinal segments.
- Age between 20 and 85 years.
- The severity of pain was assessed using the Visual Analog Scale (VAS), and only individuals with a VAS score of ≥ 4 cm on a 10-cm scale were eligible for inclusion.
- Prior to enrollment, all participants were thoroughly informed about the study objectives and procedures, and written informed consent was obtained following approval of the study protocol by the institutional ethics committee.
Participants will be excluded if they meet any of the following conditions:
- Pregnancy, or severe heart, liver, or kidney dysfunction, blood disorders, tumors, respiratory, cardiovascular, or cerebrovascular diseases, autoimmune disorders, extreme frailty, or a history of mental illness.
- Severe neurological dysfunction caused by large disc herniations, cauda equina compression, or other conditions requiring surgical intervention.
- Use of corticosteroids or non-prescription painkillers within the past two weeks.
- Any other condition, as determined by the researcher, that may compromise enrollment or follow-up, such as frequent changes in the work environment, which could result in loss to follow-up.
Participant Grouping
To ensure balanced group allocation, randomization will be performed using a computer-generated random number table Eligible participants who meet the inclusion criteria will be randomly assigned in a 1:1:1 ratio to one of three treatment groups: Group A (intraspinal acupotomy decompression), Group B (extraspinal acupotomy decompression), or Group A+B (combined intraspinal and extraspinal acupotomy decompression). Clinical recruitment staff will strictly follow the inclusion and exclusion criteria when screening participants. Once eligible participants are identified, the recruitment staff will contact the randomization coordinator, who will assign the random number and corresponding group. The randomization details will then be provided to the treatment provider prior to the participant’s treatment. Neither the clinical evaluator nor the participant will be informed of the group allocation until all observations have been completed. The study will conclude at that point.
Intervention Protocol
Extraspinal Acupotomy Decompression (Figure 2a–c)
The Huatuo Jiaji (EX-B2) acupoint corresponding to the affected spinal segment is located 0.5 body-cun lateral to the spinous process of the involved lumbar vertebra. After local anesthesia, and under imaging guidance, a Type I No. 2 acupotomy (Figure 3a) is inserted along an incision line parallel to the spinal axis.
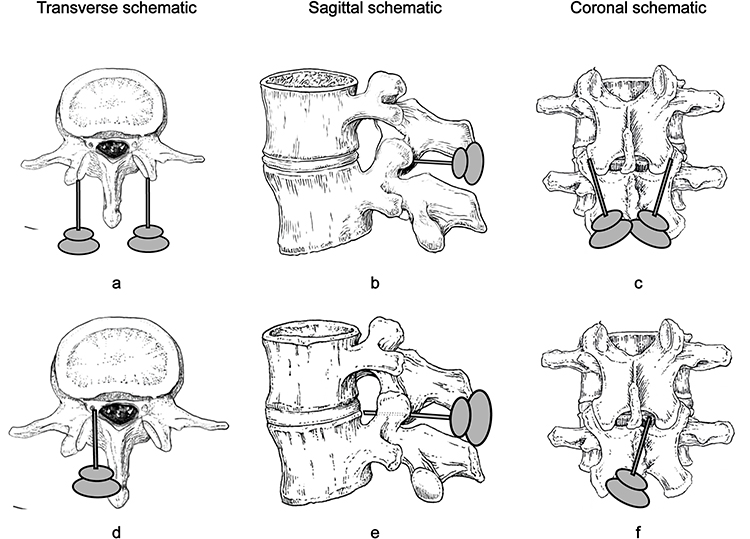 |
Figure 2 Schematic diagram of intraspinal and extraspinal decompression in the lumbar spine. (a–c) illustrate the procedure for extraspinal decompression, in which the needle passes through the deep fascia and paraspinal muscles, ultimately reaching the facet joint capsule for decompression. (d–f) show the target site for intraspinal decompression, where the needle tip is positioned adjacent to the compressed nerve roots and the herniated disc. |
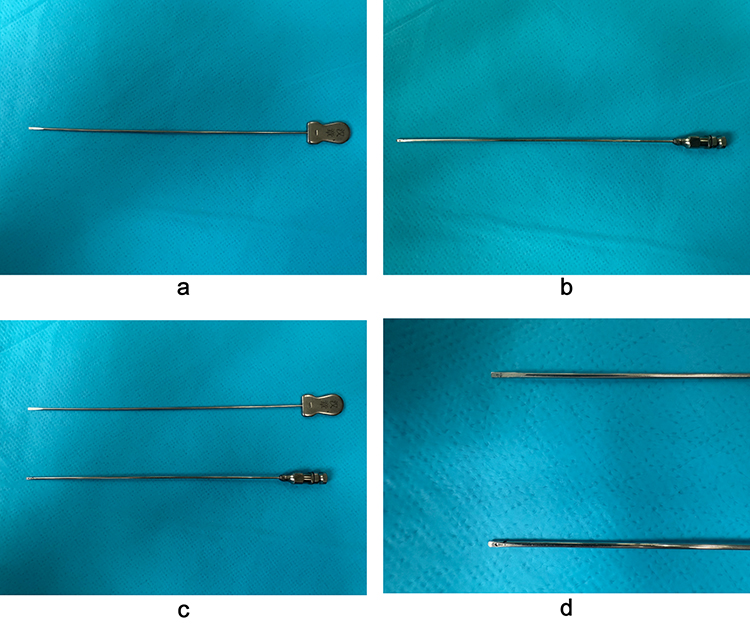 |
Figure 3 Schematic diagram of lumbar Type I No. 2 acupotomy. (a) illustrates the standard lumbar Type I No. 2 acupotomy. (b) presents the specially designed blunt-tip acupotomy specifically intended for intraspinal decompression. In (c), the lengths of both acupotomies are compared, while (d) highlights the morphological differences between their needle tips. |
The procedure is conducted in three sequential stages to ensure progressive tissue release and functional restoration: a. Deep fascia release to alleviate excessive tension. b. Paraspinal muscle release to relieve spasm and restore balanced muscle tone. c. Facet joint capsule release to enhance joint stability and reduce abnormal intra-articular stress. Following completion of these steps, the acupotomy is withdrawn, pressure is applied for 1 minute, and the site was dressed with a sterile covering.
Method of Acupotomy Intraspinal Decompression (Figure 2d–f)
The puncture site is identified 0.5 body-cun lateral to the spinous process of the affected lumbar vertebra. Following local anesthesia, the procedure is performed under X-ray fluoroscopy, CT, and ultrasound guidance to ensure accurate needle placement and procedural safety. A Type I No. 2 acupotomy needle with a blunt tip (Figure 3b–d), specifically designed to minimize the risk of dural or neural injury, is used for guided insertion. The incision line is oriented parallel to the spinal axis, and the needle is advanced toward the inferior posterior margin of the intervertebral disc until it penetrated the ligamentum flavum. During this process, patients occasionally experienced mild soreness, numbness, a sensation of fullness, or an electric shock–like response, which is transient and tolerable.
The primary goal of this intervention is to release the attachment points of the meningovertebral ligament (MVL) within the lateral recess, or to stimulate the affected nerve root to induce contraction, thereby alleviating ligament-induced neural compression and achieving effective decompression of the affected segment. Upon completion, the acupotomy is carefully withdrawn, and manual pressure is applied to the puncture site for 1 to 2 minute to ensure hemostasis, after which the area is covered with a sterile dressing.
Treatment Schedule
All participants will be randomly allocated to one of three treatment groups, each receiving a distinct intervention protocol. The treatment phase will last for 4 weeks, with one session conducted weekly, beginning on the second day of each week. Upon completion of the 4-week treatment, participants entered a rehabilitation phase designed to support recovery and prevent recurrence. The study will conclude after an 8-week postoperative follow-up period, during which clinical outcomes and adverse events will be systematically monitored.
Blinding and Unblinding
Given the nature of the acupotomy interventions, full blinding of both practitioners and participants is not feasible. Therefore, this study will employ a single-blind design. To uphold methodological rigor and minimize bias, a strict separation of roles will be implemented among the acupotomy operators, outcome assessors, and data statisticians. Blinding will be rigorously maintained for the outcome assessors and statisticians throughout the trial.
Blinded Outcome Assessors
All efficacy assessments will be conducted by trained clinical assessors who are independent of the treatment procedures and remain fully blinded to group allocation. These assessors will be prohibited from inquiring about or discussing participants’ treatment assignments and will only record data as specified in the case report forms (CRFs) to ensure the objectivity and reliability of the evaluations.
Blinded Data Analysts
All statistical analyses will be performed by an independent third-party biostatistics team that has no involvement in participant recruitment, intervention, or assessment, and no access to the study protocol or randomization scheme. This ensures that all analyses are conducted with complete blinding to group assignment, safeguarding against analytical bias.
Data Management and Unblinding
All study data will be securely stored and managed by the coordinating center. Formal unblinding of group allocation will not occur until after the database is locked and the final statistical analysis plan is approved. In the event of a serious adverse event requiring knowledge of the treatment to guide clinical management, the Principal Investigator (PI) may request emergency unblinding for that specific participant. Any participant for whom emergency unblinding occurs will be documented, and their data will be included in the safety analysis but may undergo sensitivity analysis in the efficacy evaluation.
Trial Assessment
Prior to enrollment, all potential participants will undergo a comprehensive diagnostic evaluation, conducted by a qualified physician with a minimum of five years of clinical experience. Upon providing written informed consent, eligible participants will complete a baseline assessment. Following this, participants will be randomly assigned to one of the treatment groups using a computer-generated randomization sequence. They will then receive a four-week intervention based on the predefined treatment protocol.
The primary outcome measures, including the Visual Analogue Scale (VAS) and Japanese Orthopaedic Association (JOA) scores, will be assessed at three key time points: baseline, at 4 weeks (end of treatment), and at 8 weeks post-intervention. Secondary outcome measures, including the 36-Item Short Form Health Survey (SF-36) and the total number of adverse events, will be evaluated at 8 weeks post-intervention to provide a more comprehensive assessment of treatment efficacy and patient-reported outcomes.
All evaluations will be carried out in the Outpatient Department of Pain Medicine at the First Affiliated Hospital of Shandong First Medical University. To ensure the reliability, validity, and consistency of the data, all assessments will be performed under standardized clinical conditions. Table 1 illustrates the distribution of measures at each time point throughout the study.
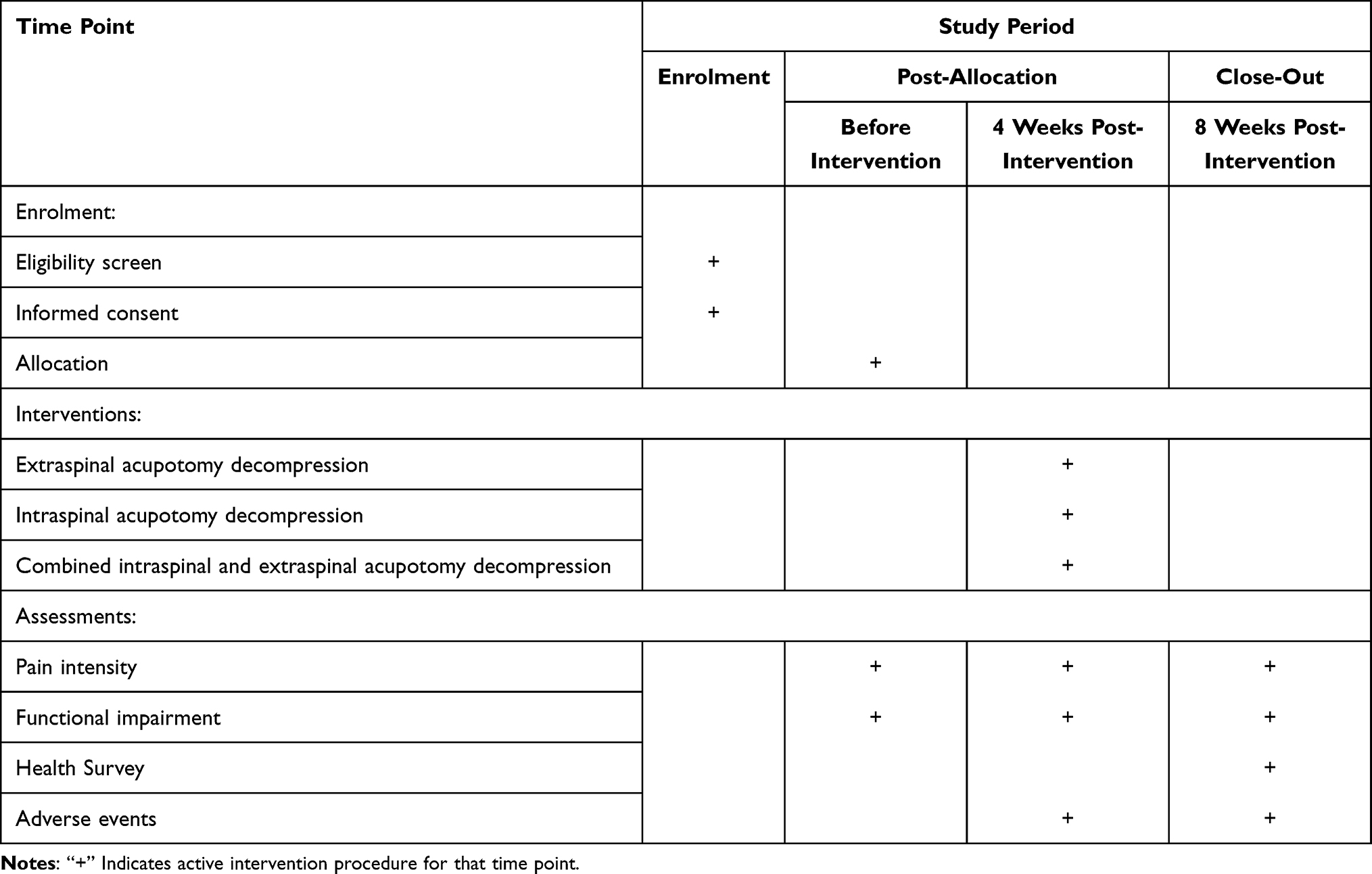 |
Table 1 Schedule of Enrolment, Intervention, and Assessment |
Primary Outcome Measures
The VAS is a widely utilized tool for quantifying pain intensity. It is represented by a 10 cm line, where 0 indicates “no pain” and 10 signifies “the most intense pain.” Participants are instructed to mark a point on the line that corresponds to their perceived pain level. Based on the mark’s position, pain severity is categorized as follows: 0–3 points for mild pain, 4–6 points for moderate pain, and 7–10 points for severe pain. The VAS is commonly used in the assessment of conditions such as lumbar disc herniation, providing a reliable and quantitative measure of pain intensity.
The JOA score is employed to evaluate functional impairment in patients with lumbar spine disorders, including lumbar disc herniation and spinal canal stenosis. This score assesses four key domains: subjective symptoms, clinical signs, daily living abilities, and bladder function, with a maximum possible score of 29 points. Based on the total score, functional status is classified as follows: 0–9 points indicate severe impairment, 10–15 points suggest moderate impairment, 16–24 points reflect good function, and 25–29 points represent normal function. Additionally, the JOA score is valuable for assessing functional improvement by comparing pre- and post-treatment scores, thus serving as a key tool in evaluating treatment efficacy.
Secondary Outcome Measures
The SF-36 is a well-established instrument for evaluating health-related quality of life, treatment efficacy, and overall well-being. The survey consists of 36 items, which assess eight health dimensions: physical functioning, role limitations (due to physical or emotional health), bodily pain, general health perceptions, vitality, social functioning, mental health, and emotional role functioning. By evaluating these dimensions, the SF-36 provides a comprehensive overview of both physical and mental health, as well as their impact on daily functioning.
All researchers are responsible for recording and reporting adverse events (AEs), regardless of their potential association with the clinical intervention. Each AE report will include the time of occurrence, clinical manifestations, severity, management, outcome, trial discontinuation status (if applicable), and follow-up details. All data must be accurately documented in the original case report forms to ensure traceability and data integrity. Investigators will evaluate the causal relationship between each AE and the intervention. Special attention will be paid to treatment-related reactions such as worsening pain, syncope during acupotomy, or subcutaneous bleeding. In emergency situations, immediate medical intervention will be provided to stabilize the participant’s condition. Follow-up will be completed within one month, with the method—hospitalization, outpatient review, home visit, or telephone follow-up—determined according to the severity and nature of the event. All AEs will be systematically documented and categorized. Serious AEs will undergo evaluation using a standardized severity assessment form. The causal relationship between each AE and the treatment will be classified according to the following five-point scale:I. Definitely related; II. Very likely related; III. Possibly related; IV. Possibly unrelated; V. Definitely unrelated. The total number of adverse events will be calculated as the sum of categories I + II + III.
Sample Size Calculation
This study was designed as a randomized controlled trial to evaluate the therapeutic efficacy of acupotomy decompression, with the VAS designated as the primary outcome measure. Based on a comprehensive review of the literature and findings from a preliminary pilot study,40 the mean VAS score in the extraspinal acupotomy decompression group at 8 weeks was 3.49 ± 1.59 (mean ± standard deviation). It was hypothesized that participants receiving combined extraspinal and intraspinal acupotomy decompression would achieve an additional 1.5-point reduction in VAS scores compared with those receiving extraspinal decompression alone. This magnitude of change was selected because a 1.5-point reduction in VAS has been commonly applied in previous clinical studies of lumbar disc herniation and related low back pain conditions and is generally regarded as representing a clinically meaningful improvement in pain intensity.32,41–43
The sample size was determined using a two-tailed significance level (α = 0.05) and statistical power (1–β = 0.90). The required sample size was calculated using the following formula:  . This calculation indicated that a minimum of 60 participants per group was required to detect a statistically significant difference. With a 1:1:1 randomization ratio, 60 participants were assigned to each of the three treatment arms. To compensate for an anticipated 15% dropout rate, the final sample size was increased to 70 participants per group, resulting in a total planned enrollment of 210 participants.
. This calculation indicated that a minimum of 60 participants per group was required to detect a statistically significant difference. With a 1:1:1 randomization ratio, 60 participants were assigned to each of the three treatment arms. To compensate for an anticipated 15% dropout rate, the final sample size was increased to 70 participants per group, resulting in a total planned enrollment of 210 participants.
Adherence Management in the Trial
In this trial, adherence refers not only to participants’ timely engagement in acupotomy therapy but also to their confidence in treatment efficacy, understanding of the recovery process, and psychological preparedness. For participants exhibiting poor adherence, the underlying causes will be thoroughly documented, and potential confounding factors will be minimized to the extent possible. Inadequate symptom improvement is one of the most common reasons for non-adherence, often leading to doubts regarding the effectiveness of the treatment. To improve participant adherence, the following strategies will be implemented:
Development of a Treatment Manual
A comprehensive treatment manual will be prepared and distributed to all participants. The manual will provide detailed information on acupotomy procedures, treatment goals, and expected therapeutic benefits. Trained clinical staff will explain the content either in person or by telephone to ensure that participants fully understand the treatment rationale, process, and anticipated outcomes. This measure aims to strengthen participants’ confidence and promote active engagement in the intervention.
Regular Follow-Ups
During the recovery period, participants will receive regular follow-ups via telephone or online communication platforms. These follow-ups will assess changes in key symptoms, monitor treatment efficacy, and evaluate adherence levels. Continuous communication will enable the timely identification and resolution of concerns, provide reassurance, and reinforce participants’ trust in the treatment process, thereby sustaining adherence throughout the intervention period.
Building Trust
To foster long-term trust and engagement, continuous communication channels will be established between the research team and participants. Comprehensive treatment information will be provided to enhance participants’ understanding of the therapy and its potential benefits. When necessary, personalized consultations will be arranged to address specific concerns, clarify treatment expectations, and encourage ongoing adherence to the therapeutic regimen.
Risk Control and Management Procedures
Given the specific characteristics of acupotomy therapy for LDH, this study will incorporate comprehensive risk control measures throughout the trial process—including study design, participant selection, procedural standardization, and outcome assessment—to minimize potential biases and systematic errors.
Control of Study-Related Risk Factors
To minimize selection and performance bias, this study will adopt a randomized controlled design and adhere to the principle of procedural separation, ensuring that researchers, clinical evaluators, and statisticians perform their roles independently. Outcome assessments will be conducted by evaluators blinded to treatment allocation, and subjective measures will be assessed using blinded observation methods to maintain objectivity in statistical analyses.
Participants will be rigorously screened according to the inclusion and exclusion criteria. To avoid confounding influences, all participants will be instructed to refrain from using medications specifically targeting lumbar disc herniation during the study period.
Control of Participant Inclusion Risks
All participants will be diagnosed by pain specialists from the Department of Pain Medicine at the First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital. Screening will be conducted in strict accordance with the eligibility criteria. During the baseline assessment, participants will be evaluated for prior lumbar trauma, ankylosing spondylitis, and other relevant comorbidities, as well as for anxiety and depression levels.
Individuals with significant medical histories or severe anxiety or depression will be excluded to minimize baseline variability and prevent confounding effects on clinical outcomes.
Control of Acupotomy Procedural Risks
The research team has established standardized clinical operating procedures (SOPs) to ensure consistent implementation of acupotomy techniques across all treatment sites. Each acupotomy operator will undergo professional training and will strictly adhere to the established protocols. All procedures will be performed by physicians with an attending or higher professional title from the Department of Pain Medicine at the First Affiliated Hospital of Shandong First Medical University.
These measures are designed to ensure procedural uniformity, optimize patient comfort, and minimize adverse procedural variations, thereby enhancing the reliability and reproducibility of clinical outcomes.
Statistical Analysis
All statistical analyses will be performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Data visualization will be conducted using GraphPad Prism version 8.0.1 (GraphPad Software, San Diego, CA, USA). Continuous variables will be expressed as mean ± standard deviation (SD). The primary analyses for comparing outcomes across the three intervention groups will be conducted using one-way analysis of variance (ANOVA) for data obtained at a single time point, or two-way repeated-measures ANOVA for assessments across multiple time points (baseline, 4 weeks, 8 weeks). If a significant overall difference is found, Tukey’s post hoc test will be used for pairwise comparisons between groups. For data that do not meet the assumptions of normality, the non-parametric Kruskal–Wallis test will be employed, followed by appropriate post-hoc tests. A p-value of less than 0.05 will be considered statistically significant.
Discussion
This study examined the therapeutic efficacy of intraspinal and extraspinal acupotomy decompression in alleviating pain and improving lumbar function among patients with LDH. The growing prevalence of sedentary lifestyles and prolonged sitting associated with modern occupations has contributed significantly to the increasing global incidence of LDH.44 Acupotomy, a minimally invasive intervention rooted in Traditional Chinese Medicine meridian theory, integrates mechanical incision, soft-tissue stimulation, and targeted release of pathological adhesions to relieve pain and restore spinal mobility.45–47 Because of its rapid onset, limited tissue trauma, and low complication rate, acupotomy has become a widely adopted clinical treatment for LDH. However, its effectiveness in relieving radicular pain and improving neurological deficits remains limited.25–27 To optimize outcomes, some clinicians have proposed combining nerve root decompression at the external intervertebral foramen with peripheral pain-point release to enhance nerve root mobility and reduce intraspinal compression.48 Nonetheless, this combined approach lacks consistent clinical validation. Intraoperative endoscopic findings during foraminal decompression frequently reveal persistent nerve root compression and adhesions, even after adequate enlargement of the foraminal openings, suggesting that isolated foraminal expansion may not fully resolve neural entrapment.49,50
In recent years, intraspinal acupotomy decompression through the Huatuo Jiaji (EX-B2) acupoint has been introduced as a promising alternative. In this approach, the acupotomy is inserted between the laminae along the medial margin of the facet joint until a characteristic “breakthrough sensation”is perceived, followed by controlled cutting and sweeping maneuvers. This method aims to release the ligamentum flavum and adjacent posterior spinal canal structures, thereby achieving dorsal decompression and creating an “escape space” for the affected nerve root.51,52 Theoretically, this technique mitigates mechanical irritation and compression of neural tissues. Despite its solid biomechanical rationale, clinical outcomes remain variable—some patients experience substantial symptom improvement, while others achieve only partial or transient relief. Such inconsistency may stem from the multifactorial nature of nerve root compression, as the ligamentum flavum is not always the primary compressive element. For example, in posterior lumbar endoscopic surgery, even after complete resection of the ligamentum flavum, ventrally herniated disc material may continue to exert pressure on the nerve root, indicating that decompression confined to posterior structures may be inadequate for achieving full neural release.53,54
Parallel to these clinical advances, recent anatomical research has significantly enhanced the understanding of LDH pathogenesis. Through detailed anatomical dissections and comprehensive literature analyses, researchers specializing in acupotomy have identified the MVL as a critical structure involved in LDH development.55 The MVL, first described in 1817 as a connective tissue linking the dura mater to the inner wall of the vertebral canal, is an intrinsic ligament within the spinal canal. Following over a century of anatomical investigation, Gray’s Anatomy formally recognized and defined this structure as the meningovertebral ligament.56–58 Anatomically, the anterior portion of the MVL connects the dura mater to the posterior longitudinal ligament or vertebral body, whereas the posterior portion attaches to the lamina or ligamentum flavum. Functionally, the MVL stabilizes the spinal nerve roots within the canal, preventing excessive traction or displacement during spinal motion, thereby minimizing mechanical compression that can contribute to low back and leg pain. However, under pathological conditions such as disc herniation or chronic abnormal mechanical loading, the MVL—similar to the ligamentum flavum and facet joint capsules—may undergo fibrotic thickening, hyperplasia, or degenerative remodeling. These changes can lead to adhesion or entrapment between the nerve root and adjacent structures, restricting nerve root mobility and exacerbating radicular pain and neurological dysfunction.59–61 Building upon these anatomical and pathological insights, acupotomy practitioners have developed an innovative intraspinal needle-knife release technique. This procedure precisely targets and releases the MVL and associated adhesive tissues through an interlaminar approach, thereby relieving nerve root restriction and improving lumbar and leg symptoms. By addressing both the mechanical compression and biological mechanisms underlying neural entrapment, this technique provides a novel, evidence-based, and minimally invasive therapeutic strategy for the management of LDH.
Although intraspinal acupotomy demonstrates notable advantages — including minimal invasiveness, procedural simplicity, and cost-effectiveness — it is not without potential risks. Deviations in the puncture trajectory can lead to complications such as dural tears, nerve root injury, or intraspinal hemorrhage. To mitigate these risks, all procedures in this study were conducted under X-ray fluoroscopy, CT, or ultrasound guidance guidance using a specially designed blunt-tipped acupotomy. This design allows tactile precision during decompression, thereby minimizing the likelihood of iatrogenic injury and improving procedural safety. Collectively, these characteristics make intraspinal acupotomy a potentially valuable and safe interventional approach for the treatment of LDH.
However, this study has certain limitations that warrant consideration. The follow-up duration was restricted to eight weeks, which may not adequately reflect long-term outcomes, recurrence rates, or delayed complications. Incorporating longer follow-up periods, such as 6 months, in future studies would help assess the durability of the results and provide more comprehensive insights into recurrence rates and potential long-term complications. Additionally, the relatively small sample size and single-center design may limit the external validity and generalizability of the findings. Future research should consider multicenter randomized controlled trials with larger cohorts and extended follow-up periods to further validate the long-term efficacy, safety, and reproducibility of intraspinal acupotomy decompression. Furthermore, cost-effectiveness analyses should be conducted to compare the clinical benefits of intraspinal acupotomy with traditional surgical approaches, as well as its integration with global treatment guidelines for LDH management. Lastly, subgroup analyses, such as by herniation type or baseline severity, could provide more granular insights into the efficacy of intraspinal acupotomy across different patient populations.
Nonetheless, this study has certain limitations that warrant consideration. The follow-up duration was restricted to eight weeks, which may not adequately reflect long-term outcomes, recurrence rates, or delayed complications. Incorporating longer follow-up periods, such as 6 months, in future studies would help assess the durability of the results and provide more comprehensive insights into recurrence rates and potential long-term complications. Additionally, the relatively small sample size and single-center design may limit the external validity and generalizability of the findings. Future research should consider multicenter randomized controlled trials with larger cohorts and extended follow-up periods to further validate the long-term efficacy, safety, and reproducibility of intraspinal acupotomy decompression. Furthermore, cost-effectiveness analyses should be conducted to compare the clinical benefits of intraspinal acupotomy with traditional surgical approaches, as well as its integration with global treatment guidelines for LDH management. Lastly, subgroup analyses, such as by herniation type or baseline severity, could provide more granular insights into the efficacy of intraspinal acupotomy across different patient populations.
Conclusion
This study provides the first systematic evaluation of the feasibility and clinical efficacy of intraspinal acupotomy decompression in the management of LDH. By clarifying the role of the MVL in nerve root entrapment from both anatomical and pathophysiological perspectives, the present research establishes a comprehensive theoretical and procedural framework for the intracanalar application of acupotomy in spinal decompression therapy. This framework not only deepens the mechanistic understanding of LDH pathology but also offers a new minimally invasive treatment paradigm. The findings of this study have significant implications for clinical guidelines, particularly in incorporating intraspinal acupotomy decompression as a valuable, minimally invasive treatment option for managing lumbar disc herniation (LDH).
This trial will evaluate whether intraspinal acupotomy decompression can meaningfully reduce pain and improve lumbar function in patients with lumbar disc herniation (LDH), and in doing so, clarify its potential position among contemporary minimally invasive spinal interventions. By targeting intracanalar restrictive structures, the study addresses a practical clinical question—whether a more precisely directed decompression strategy can help close the gap between conservative care and conventional surgery for patients whose symptoms are driven by nerve-root involvement. Beyond clinical outcomes, the protocol is structured to support subsequent mechanistic work on MVL release, including imaging assessments before and after the procedure and investigations into MVL-related physiological and pathological alterations in LDH. Together, these components are expected to strengthen the biological rationale for the intervention and to inform future studies on durability and longer-term outcomes. Ultimately, this work may broaden the therapeutic landscape for LDH and provide a clearer basis for further evaluation of intraspinal acupotomy decompression as a targeted, minimally invasive option.
Trial Status
This clinical trial is currently ongoing and actively recruiting participants. The finalized study protocol (version 1.0) received ethical approval from the institutional review board on 28 August 2023. Participant enrollment began on 1 October 2025, and full recruitment is anticipated by January 2026. As of 1 November 2025, a total of 30 participants have been enrolled, with 24 having completed their first or second treatment session.
Abbreviations
LDH, Lumbar Disc Herniation; CT, computed tomography; VAS, Visual Analog Scale; MVL, meningovertebral ligament; CRFs, case report forms; JOA, Japanese Orthopaedic Association; SF-36, 36-Item Short Form Health Survey; AEss, adverse events; RCT, randomized controlled trial; SOPs, standardized clinical operating procedures.
Data Sharing Statement
The datasets generated and/or analyzed during the current study will not be publicly available due to patient privacy and ethical considerations but are available from the corresponding author, Liufangming, upon reasonable request.
Ethics Approval and Consent to Participate
The trial protocol follows the latest The SPIRIT, and the results are reported according to The CONSORT. The study was conducted in the Department of Pain Medicine, The First Affiliated Hospital of Shandong First Medical University and Shandong Provincial Qianfoshan Hospital. The protocol was approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University ([2023] No. S426), and the trial is registered in the International Traditional Medicine Clinical Trial Registry (ITMCTR2025001872). The study complies with the most recent version of the Declaration of Helsinki. All participants with lumbar disc herniation provided written informed consent.
Acknowledgments
The authors would like to express their sincere gratitude to all study participants.
Author Contributions
Wenlong Yang and Hailiang Liu contributed equally to this work and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted Journal of Pain Research; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Administration of Traditional Chinese Medicine Science and Technology Project, China (grant no. GZY-KJS-2023-019); the Shandong Provincial Natural Science Foundation, China (grant no. ZR2023MH118); the National Natural Science Cultivation Foundation of China (grant no. QYPY2022NSFC0609); and the Mount Taishan Scholar Distinguished Expert Project, China (grant no. tstp20231253).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jin H, Lopez AM, Romero FG, Hoang R, Ramesh A, Bow HC. A systematic review of treatment guidelines for lumbar disc herniation. Neurospine. 2025;22(2):389–14. doi:10.14245/ns.2550398.199
2. Hincapié CA, Kroismayr D, Hofstetter L, et al. Incidence of and risk factors for lumbar disc herniation with radiculopathy in adults: a systematic review. Eur Spine J. 2024;34(1):263–294. doi:10.1007/s00586-024-08528-8
3. Zhang A, Xu A, Ansari K, et al. Lumbar disc herniation: diagnosis and management. Am J Med. 2023;136:645–651. doi:10.1016/j.amjmed.2023.03.024
4. Qi L, Luo L, Meng X, et al. Risk factors for lumbar disc herniation in adolescents and young adults: a case–control study. Front Surg. 2023;9. doi:10.3389/fsurg.2022.1009568
5. Hammed A, Al-Qiami A, Alsalhi H, et al. Surgical vs. Conservative management of chronic sciatica (>3 months) due to lumbar disc herniation: systematic review and meta-analysis. Cureus. 2024;16. doi:10.7759/cureus.59617
6. Song K, Liang J, Zhang M, Cai S, Wang Y, Wu W. Comparison of different treatments for lumbar disc herniation: a network meta-analysis and systematic review. BMC Surgery. 2025;25(1). doi:10.1186/s12893-025-02992-9
7. Liu C, Ferreira GE, Abdel Shaheed C, et al. Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials. BMJ. 2023;381:e070730. doi:10.1136/bmj-2022-070730
8. Kögl N, Petr O, Löscher W, Liljenqvist U, Thomé C. Lumbar disc herniation. Dtsch Arztebl Int. 2024. doi:10.3238/arztebl.m2024.0074
9. Yang W, Li K, Pan Q, et al. An engineered bionic nanoparticle sponge as a cytokine trap and reactive oxygen species scavenger to relieve disc degeneration and discogenic pain. ACS Nano. 2024;18(4):3053–3072. doi:10.1021/acsnano.3c08097
10. Li Y, Dai C, Wu B, et al. Intervertebral disc injury triggers neurogenic inflammation of adjacent healthy discs. Spine J. 2024;24(8):1527–1537. doi:10.1016/j.spinee.2024.04.002
11. Ye F, Lyu F-J, Wang H, Zheng Z. The involvement of immune system in intervertebral disc herniation and degeneration. JOR Spine. 2022;5(1):e1196. doi:10.1002/jsp2.1196
12. Kim KD, Ahadian F, Hassanzadeh H, et al. A Phase 3, randomized, double-blind, sham-controlled trial of SI-6603 (condoliase) in patients with radicular leg pain associated with lumbar disc herniation. Spine J. 2024;24(12):2285–2296. doi:10.1016/j.spinee.2024.08.006
13. Samuelly‐Leichtag G, Eisenberg E, Zohar Y, et al. Mechanism underlying painful radiculopathy in patients with lumbar disc herniation. Eur J Pain. 2022;26(6):1269–1281. doi:10.1002/ejp.1947
14. Ozevren H, Cetin A, Baloglu M, Deveci E. Comparison of histopathologic findings of initial and recurrent lumbar disc herniation. Int J Neurosci. 2024;135(10):1156–1162. doi:10.1080/00207454.2024.2348123
15. Chen X, Cui P, Li Y, Wang Y, Lu S. Links among MRI features in paraspinal muscles, inflammatory processes, and related back pain in patients with lumbar disc herniation. JOR Spine. 2023;7(1). doi:10.1002/jsp2.1310
16. Zhang H, Gao J. Clinical comparison of percutaneous endoscopic lumbar discectomy and posterior lumbar interbody fusion for L4/5 and L5/S1 dual-level disc herniation. Sci Rep. 2025;15(1). doi:10.1038/s41598-025-92128-z
17. Liu S, Zhang X, Xiong Y, He H. Minimally invasive surgery for lumbar disc herniation: a meta-analysis of efficacy and safety. Int J Surg. 2025;111(8):5623–5636. doi:10.1097/js9.0000000000002434
18. Tan H, Zhou J, Pu Y, He L, Wang L. Efficacy of selective nerve root block for different types of lumbar disc herniation: study protocol for a single-blind, prospective cohort study. J Pain Res. 2025;18:1035–1043. doi:10.2147/jpr.S494496
19. Karasin B, Kleban M, Rizzo G, Hardinge T, Eskuchen L, Watkinson J. Minimally invasive spine surgery for lumbar decompression or disc herniation. AORN J. 2024;120(5):281–289. doi:10.1002/aorn.14233
20. Lan W, Cui H, Zhou D, Xiao X, Xiong H. Advances in minimally invasive surgical techniques for lumbar disc herniation: a comprehensive review. Front Surg. 2025;12. doi:10.3389/fsurg.2025.1593195
21. Liu S, Zhou J. Comparative efficacy and safety of three surgical procedures for the treatment of lumbar disc herniation: a Bayesian-based network analysis. BMC Surg. 2025;25(1). doi:10.1186/s12893-025-02856-2
22. Brotis AG, Spiliotopoulos T, Kalogeras A, Fountas KN, Demetriades AK. Epidural steroid injections in lumbar disc herniation- Evidence synthesis from 72 randomised controlled trials (RCTs) and a total of 7701 patients. Brain Spine. 2025;5:104216. doi:10.1016/j.bas.2025.104216
23. Muralidhar S, Jain H, Kumar M, Jindal RC. Epidural steroid injections for lumbar disc herniation and lumbar degenerative disc disease. J Orthop Case Rep. 2025;15(10):288–294. doi:10.13107/jocr.2025.v15.i10.6238
24. Ünal HA, Başarı A, Özgencil BK, Özgencil GE, Erkoç SK. Comparison of unilateral and bilateral transforaminal epidural steroid injections in unilateral lumbar disc herniation: a randomized controlled trial. J Clin Med. 2024;14(1):147. doi:10.3390/jcm14010147
25. Y-h W, Zhou Y, Y-z X, et al. The effect of ultrasound-guided acupotomy and Juanbi decoction on lumbar disc herniation: a randomized controlled trial. Medicine. 2023;102(1). doi:10.1097/md.0000000000032622
26. Hong K, Gao J, Hu L, Long X, Wu X, Wen B. Acupotomy for military training-induced lumbar radiculopathy with sciatica: protocol of a randomized controlled trial. J Pain Res. 2025;18:4123–4138. doi:10.2147/jpr.S535852
27. Zhong Y, Ding Y, Fu B, et al. Effect of acupotomy on the fat infiltration degree of lumbar multifidus muscle in patients with lumbar disc herniation after percutaneous transforaminal endoscopic discectomy. Zhongguo Zhen Jiu. 2023;43:153–157. doi:10.13703/j.0255-2930.20220628-k0002
28. Zhu X, Qiu Z, Liu Z, et al. CT-guided percutaneous lumbar ligamentum flavum release by needle knife for treatment of lumbar spinal stenosis: a case report and literature review. J Pain Res. 2020;13:2073–2081. doi:10.2147/jpr.S25524925
29. Shi B, Zheng X, Min S, et al. The morphology and clinical significance of the dorsal meningovertebra ligaments in the cervical epidural space. Spine J. 2014;14(11):2733–2739. doi:10.1016/j.spinee.2014.04.014
30. Shi B, Li X, Li H. Ding Z.The morphology and clinical significance of the dorsal meningovertebra ligaments in the lumbosacral epidural space. Spine. 2012;37(18):E1093–8. doi:10.1097/BRS.0b013e31825c05ea
31. Jiang C, Li Y, Guo M, et al. Acupotomy therapy for lumbar disc herniation: protocol for a systematic review and meta-analysis. Medicine. 2018;97(40):e12624. doi:10.1097/MD.0000000000012624
32. Jeong K-J, Eunseok K, Kwang S-Y, et al. Acupotomy versus manual acupuncture for the treatment of back and/or leg pain in patients with lumbar disc herniation: a multicenter, randomized, controlled, assessor-blinded clinical trial. J Pain Res. 2020;13:677–687. doi:10.2147/JPR.S234761
33. Tommy A, Farhad B, Donny W, Christin P. A comparative study of transforaminal and interlaminar approaches in percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation: systematic review. J Clin Neurosci. 2025;133:111022. doi:10.1016/j.jocn.2024.111022
34. Chan A-W, Boutron I, Hopewell S, et al. SPIRIT 2025 statement. JAMA. 2025;334(5):435. doi:10.1001/jama.2025.4486
35. Hopewell S, Chan A-W, Collins GS, et al. CONSORT 2025 statement. JAMA. 2025;333(22):1998. doi:10.1001/jama.2025.4347
36. Magdalena K, Cyprian M, Agnieszka U, et al. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Crit Care. 2025;29:78. doi:10.1186/s13054-025-05295-w
37. Qin X, Sun K, Xu W, et al. An evidence‐based guideline on treating lumbar disc herniation with traditional Chinese medicine. J Evidence-Based Med. 2024;17(1):187–206. doi:10.1111/jebm.12598
38. Haro H, Ebata S, Inoue G, et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lumbar disc herniation, third edition - secondary publication. J Orthop Sci. 2022;27(1):31–78. doi:10.1016/j.jos.2021.07.028
39. Kreiner DS, Hwang SW, Easa JE, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014;14(1):180–191. doi:10.1016/j.spinee.2013.08.003
40. Lee JH, Lee H-J, Woo SH, et al. Effectiveness and safety of acupotomy on lumbar spinal stenosis: a pragmatic, pilot, randomized controlled trial. J Pain Res. 2023;16:659–668. doi:10.2147/jpr.S399132
41. Tu J-F, Shi G-X, Yan S-Y, et al. Acupuncture vs Sham acupuncture for chronic sciatica from herniated disk: a randomized clinical trial. JAMA Intern Med. 2024;184(12):1417–1424. doi:10.1001/jamainternmed.2024.5463
42. Mathieson S, Maher CG, McLachlan AJ, et al. Trial of pregabalin for acute and chronic sciatica. N Engl J Med. 2017;376(12):1111–1120. doi:10.1056/NEJMoa1614292
43. Robertson K, Marshman LAG, Plummer D, Downs E. Effect of gabapentin vs pregabalin on pain intensity in adults with chronic sciatica: a randomized clinical trial. JAMA Neurol. 2019;76(1):28–34. doi:10.1001/jamaneurol.2018.3077
44. Palluppetta P, Lambroussis CG, Dhillon A, et al. Management of lumbar disc herniation with nerve compression in a 21-year-old male: a case report exploring multifactorial causes of disc herniation. Cureus. 2025. doi:10.7759/cureus.77916
45. Ma S. Clinical advantages of ultrasound-guided acupotomy targeting the suboccipital muscles versus the posterior occipital tendinous arch for cervicogenic dizziness: a controlled trial. Am J Transl Res. 2025;17(9):7136–7145. doi:10.62347/zggx5031
46. Liu Y, Shang J, Zhang Y, et al. A clinical study of ultrasound-guided acupotomy combined with mindfulness meditation to improve lumbar myofascial pain syndrome. Front Neurol. 2025:16. doi:10.3389/fneur.2025.1627376
47. Li Y, Li Q. Ultrasound-guided acupotomy in stroke limb rehabilitation: efficacy insights and unaddressed methodological concerns. Neurol Sci. 2025. doi:10.1007/s10072-025-08555-3
48. Song X, Zhang C, Zuo X, et al. Different entry points of needle knife for lumbar disc herniation: a randomized controlled trial. Zhongguo Zhen Jiu. 2022;42:35–40. doi:10.13703/j.0255-2930.20201204-k0004
49. Masatoshi M, Sudharshan T, Niloufar S, G VK, Koichi S. Biomechanical effects of cage position in full-endoscopic trans-Kambin’s triangle lumbar interbody fusion: 510 a finite element analysis. Neurol Med Chir. 2025. doi:10.2176/jns-nmc.2025-0083
50. Chen H, Chen L, Zhang Y. Endoscopic discectomy for L4–L5 disc herniation: percutaneous endoscopic transforaminal discectomy vs. unilateral biportal endoscopic discectomy. Front Surg. 2025;12. doi:10.3389/fsurg.2025.1565165
51. Fang N, Wang Z, Jiang J, et al. Nonsurgical therapy for lumbar spinal stenosis caused by ligamentum flavum hypertrophy: a review. Medicine. 2024;103(27):e38782. doi:10.1097/md.0000000000038782
52. Zhu X, Shen Y, Liu Z, Gu P, Li S, Zhang W. Ultrasound-guided percutaneous release procedures in the lumbar ligamentum flavum by acupotomy: a cadaveric study. Evid Based Complement Alternat Med. 2019;2019:1–9. doi:10.1155/2019/2807901
53. Chang H, Xu J, Yang D, Sun J, Gao X, Ding W. Comparison of full-endoscopic foraminoplasty and lumbar discectomy (FEFLD), unilateral biportal endoscopic (UBE) discectomy, and microdiscectomy (MD) for symptomatic lumbar disc herniation. Eur Spine J. 2022;32(2):542–554. doi:10.1007/s00586-022-07510-6
54. Li L, An J, Guo L, et al. Comparison of percutaneous endoscopic lumbar discectomy (PELD) and unilateral biportal endoscopic (UBE) discectomy in the treatment of far lateral lumbar disc herniation (FLLDH): a retrospective study. J Orthopaedic Surg Res. 2025. doi:10.1186/s13018-025-05906-w
55. Krystkiewicz K, Maślanka M, Skadorwa T, Ciszek B, Tosik M, Furtak J. Meningovertebral ligaments could be a barrier for migration of a herniated intervertebral disc: an anatomical study. Front Surg. 2022;9. doi:10.3389/fsurg.2022.969244
56. Chen R, Shi B, Zheng X, et al. Anatomic study and clinical significance of the dorsal meningovertebral ligaments of the thoracic dura mater. Spine. 2015;40(10):692–698. doi:10.1097/brs.0000000000000860
57. Santos JLM, Kalhorn SP. Anatomy of the posterolateral spinal epidural ligaments. Surg Neurol Int. 2021;12:12. doi:10.25259/sni_894_2020
58. Zhong E, Zhao Q, Shi B, et al. The morphology and possible clinical significance of the intraforaminal ligaments in the entrance zones of the L1-L5 levels. Pain Physician. 2018;21:E157–E165.
59. Zhou Y, Chai X, Zheng H, Song R, Qin X. Spinal cord compression syndrome caused by intraspinal epidural fibrous cord. Medicine. 2017;96(33). doi:10.1097/md.0000000000007592
60. Marc K, Eric N, Rache B, Joshua D, Alexander L. Anatomic description and clinical relevance of the meningovertebral ligament in dogs. J Am Vet Med Assoc. 2019;255:687–694. doi:10.2460/javma.255.6.687
61. Strauss SB, Gordon SR, Burns J, Bello JA, Slasky SE. Differentiation between tuberculous and pyogenic spondylodiscitis: the role of the anterior meningovertebral ligament in patients with anterior epidural abscess. Am J Neuroradiol. 2020;41(2):364–368. doi:10.3174/ajnr.A6370
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Randomized, Sham-Controlled Trial on the Efficacy and Safety of Electroacupuncture for Lumbar Disc Herniation with Radiculopathy: Rationale and Study Protocol
Yang Y, Liu L, Yuan L, Liu X, Ding H, Zhou X, Cao Q
Journal of Pain Research 2025, 18:2307-2319
Published Date: 5 May 2025
Effectiveness of Acupotomy Combined with Topical Diclofenac for Knee Osteoarthritis: A Randomized Controlled Trial
Du K, Cheng WZ, Li A, Zhang CY, Yan SY, Han F, Guo R, Chen P, Du WS, Zuo YL, Zuo QH, Li SM
Journal of Pain Research 2025, 18:6779-6790
Published Date: 17 December 2025
Acupotomy Combined with Celecoxib and Zhenggu Shenjin Capsules for Lumbar Disc Herniation: A Propensity Score-Matched Retrospective Cohort Study
Sun X, Zhang S, Liu S
Journal of Pain Research 2026, 19:594368
Published Date: 21 April 2026