Back to Journals » Patient Preference and Adherence » Volume 19
Development and Validation of a New Nomogram for Predicting Medication Nonadherence Risk in a Chinese Hyperlipidemia Population
Authors Guo J, Ning F, Xiao J, Pu P, Zhao Y, Zhang W, Wu M ![]()
Received 10 July 2025
Accepted for publication 20 December 2025
Published 30 December 2025 Volume 2025:19 Pages 4321—4334
DOI https://doi.org/10.2147/PPA.S547265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Jingyue Guo,1,* Feng Ning,2,* Jianbiao Xiao,2,* Peipei Pu,2 Yuesong Zhao,3 Wei Zhang,4 Mingfen Wu5
1Medical Department, Dahongmen Community Health Service Center, Beijing, 100075, People’s Republic of China; 2Executive Office, Dahongmen Community Health Service Center, Beijing, 100075, People’s Republic of China; 3Executive Office, Heyi Community Health Service Center, Beijing, 100076, People’s Republic of China; 4Fengtai District Community Health Service Management Center, Beijing, 100071, People’s Republic of China; 5Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingfen Wu, Email [email protected]
Purpose: This study aimed to explore the factors influencing medication adherence and develop a medication nonadherence risk nomogram in a Chinese population with hyperlipidemia.
Methods: This prospective intervention study was conducted in Beijing from November 2020 to October 2021. Medication adherence was determined according to the 9-question scale and nonadherence patients were intervened by pharmacists and followed up for 3 months. Multivariate logistic regression was used to analyze the risk factors of medication nonadherence, and then a nomogram model was established. The concordance index (C-index), area under the curve (AUC) was used to evaluate the accuracy of the prediction model. The decision curve analysis (DCA) and clinical impact plot analysis were employed to further evaluate the clinical effectiveness of the nomogram.
Results: A total of 685 patients were included for analysis. The rate of medication nonadherence was 238 patients (34.75%). Post-intervention, the average score of medication adherence increased from 20.75± 8.01 to 29.90± 6.93 (p < 0.001). And the number of patients with TC, TG, LDL-C, and HDL-C reaching the standard was 264 (62.86%), 201 (47.43%), 318 (78.52%), and 377 (96.71%), respectively. Five predictors including the course of hyperlipidemia (OR=2.957, 95% CI 1.168– 7.488), following the doctor’s advice to visit (OR=2.757, 95% CI 1.389– 5.472), use of medications empirically (OR=1.189, 95% CI 1.188– 2.786), physical exercise (OR=0.399, 95% CI 0.205– 0.776) and lifestyle compliance (OR=0.910, 95% CI 0.839– 0.988) were identified to build the nomogram model. The AUC was 0.927 and C-index was 0.87.
Conclusion: Patients with hyperlipidemia displayed low medication adherence which pharmaceutical interventions can improve. We developed and validated a nomogram model to facilitate the individual medication nonadherence risk prediction in hyperlipidemia patients.
Limitation: First, using the cut-off value of 27 for adherence assessment in the adherence questionnaire, criterion validity was not enough good to validly screen a patient with nonadherence to medication. Second, our study may have unmeasured confounding variables, which could bias the results. Third, owing to the lack of external validation in this study, it may have some limitations in extrapolation. Fourth, the questionnaire was assessed by self-report measures.
Keywords: hyperlipidemia, medication non adherence, risk factor, intervention, nomogram
Introduction
The high incidence of atherosclerotic cardiovascular and cerebrovascular diseases (ASCVD) endangers people’s health and causes a major economic burden worldwide.1,2 Dyslipidemia is an independent risk factor for developing ASCVD.3,4 Thus, proper management in patients with dyslipidemia can reduce the incidence of cardiovascular and cerebrovascular events. Currently, the primary strategies for managing hyperlipidemia encompass medication therapy and dietary intervention. Medication therapy is still the preferred strategy for improving hyperlipidemia, and statins are the first-line drug for the treatment of dyslipidemia.5 The effectiveness of treatment and prevention of ASCVD can be optimized with adherence to medication treatment. Previous studies have demonstrated that medication adherence has been playing quite an important role in the self-management of patients with hyperlipidemia.6,7 The good statin adherence can decrease the risks of all-cause and cardiovascular mortality.7 Medication nonadherence leads to poor control of blood lipids, which further develops into ASCVD. The annual direct and indirect cost of CVD and stroke in the United States is an estimated $316.6 billion,8 and nonadherence is estimated to account for $290 billion.9 At the same time, studies in China have found that patients with dyslipidemia in the community have poor adherence with statin medication.10 Medication nonadherence is affected by a variety of determinants,7,11 which can be summarized into socioeconomic factors (eg, social support, family income, medical expenses, nationality, and religious belief), patient-related factors (eg, age, sex, working condition, income, and education level), therapy-related factors (eg, drug usage and dosage, type and quantity of medicine, adverse drug reaction, side effects, and medication-related problems), and health system-related factors (eg, health providers, health status, medical insurance, drug supply). Results from previous studies have proved that pharmaceutical interventions could moderate the high risk of nonadherence and improve patients’ long-term clinical outcomes.12 Given so many associated risk factors, the development of accurate tools to predict nonadherence and early intervention may be the most effective strategy to ameliorate poor adherence. However, there are still few researches to explore medication nonadherence and its risk in patients with hyperlipidemia at present. In a US study, researchers evaluated multiple measures of patient previous medication adherence to predict future statin adherence by a large US administrative claims database. However, as the study required a longer retrospective period, this reduced the number of eligible patients, potentially limiting the generalizability of the prediction models. Meanwhile, there is a lack of prediction models of medication nonadherence in China.
As a commonly used clinical disease prediction tool, the nomogram refers to a two-dimensional chart illustrating the relationship between multiple risk factors, which is used to calculate the predictive probability of disease simply and efficiently.13 And the nomogram model has been widely used for clinical prediction of different diseases. The standard procedure for establishing nomogram model comprises: defining research objectives, determining outcome indicators, collecting population data, selecting appropriate models, selecting and finalizing contact real prediction variables and finally evaluating and validating the model.14
Therefore, this study aimed to investigate the current status of medication nonadherence and blood lipid control in patients with hyperlipidemia, identify potential risk factors of medication nonadherence, and develop a nomogram model to predict the risk of non-adherence. We also aimed to assess the effects of pharmaceutical interventions in improving patient adherence and blood lipid control through a pharmacist-led prospective study. The findings may provide evidence for more targeted interventions and further improve the therapeutic effect of medications in patients with hyperlipidemia.
Patients and Methods
Patients
This research was approved by the Medical Ethics Committee of Beijing Tiantan Hospital, Capital Medical University (ethics number: KY2020-085-02). Written informed consent was obtained from each patient. This multicenter, prospective, interventional study was conducted in Beijing, China from November 2020 to October 2021. All data were collected from 35 hospitals that participated in the study. The inclusion criteria were as follows: (1) patients who were older than 35 years old; (2) patients who were diagnosed with hyperlipidemia by a doctor and received treatment with lipid-lowering drugs for at least 3 months; (3) patients with the ability to record medicine information, monitor blood lipid levels regularly, and follow-up for at least 3 months; and (4) patients that understand the questionnaire or scale after explanation and cooperate with pharmacists to complete the questionnaire. Patients who were suffered from a major mental disorder, illiterate, had severe cognitive impairment or had severe physical constraints were excluded. The collected data of the hyperlipidemia patients included 5 parts: (1) demographic and sociological characteristics of the patients (age, gender, marital status, income, occupational status, type of medical insurance, smoking history, alcohol consumption history); (2) disease information (disease duration, history of the disease, complications, blood lipid monitoring results); (3) list of antihyperlipidemic drugs (types of drugs used, duration of medication, adverse drug reaction); (4) assessment of medication adherence (9-items Medication Adherence Assessment Scale, MAAS15); and (5) lifestyle compliance assessment. It refers to the degree to which individuals adhere to evidence-based health-related behaviors and medical recommendations in daily life, encompassing medication use, dietary management, physical activity, and regular health monitoring. It measured by self-report questionnaire (See Supplementary Figure S1 for more details).15 There was a total of nine items with four options (score of 1–4). Here, the total is the sum of the scores for each question, with the highest score of 36. A higher score meant better compliance. Data such as demographic, blood lipid monitoring indicators such as low-density cholesterol, disease, and treatment characteristics of the patients were collected from medical records.
Medication Adherence Assessment
The Medication Adherence Assessment Scale (MAAS) was used to assess adherence in patients with hyperlipidemia. The MAAS consists of 9 items about taking medicine behavior in the past 3 months, in which patients were asked about the degree of agreement with statements. The nine items contained four forward questions and five reverse questions (see Supplementary Figure S2 for more details). Answers are based on a 4-point Likert scale from 1 to 4 (1: Never; 2: Occasional; 3: Often; and 4: Always; or reverse scoring). The final score allows the identification of nonadherent patients, with 27 as the cut-off point, a higher score represents better adherence, and scores of 36, 27- ˂ 36, and ˂ 27 were defined as good, moderate, and poor adherence. In the multivariate logistic regression analysis, patients with moderate and good adherence were defined as the adherence group, while patients with poor adherence were defined as the non-adherence group. The study was conducted in the form of face-to-face interviews followed by interventions for non-adherence patients by specially trained pharmacists. Pharmacist-led interventions included recommendations on disease management, drug usage, and dosage, adverse effects, periodic monitoring indicators, medication reminders, strategies to improve medicine adherence, advice on lifestyle modifications, and so on. All patients were followed up three times, once a month. The first survey was defined as a baseline study. And the patients were scheduled for follow-up visits at one, two and three months. But the MAAS and serum concentrations of lipids was just surveyed at baseline and the third visit. At the first and second follow-up visits, only any medication related problems or adjustments were recorded. The screening flow chart of enrolled patients was listed in Figure 1. Routine chemical methods were used to measure serum concentrations of lipids.
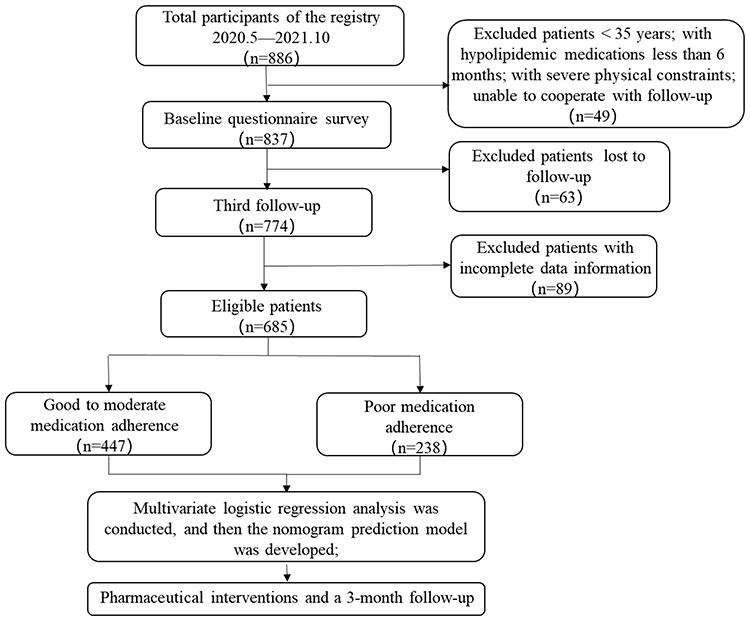 |
Figure 1 Screening flow chart of enrolled patients. |
Statistical Analysis
Statistical analyses were performed using Microsoft Excel 2021 and IBM SPSS Statistics 26.0. The data were plotted using GraphPad Prism v5.0. Enumeration data were statistically described by frequency and rate (%), while the measurement data were expressed as the mean ± SD. Descriptive statistics, chi-square (χ2) test, and t-test were used to evaluate the results. Results were considered statistically significant if the p-value < 0.05. The nomogram model was developed using R software (version 4.2.2, https://www.R-project.org). Multivariate logistic regression analysis was conducted to screen potential risk factors for nonadherence in patients with hyperlipidemia, then a nomogram prediction model was established according to the corresponding risk factors, and the accuracy and clinical effect of the nomogram were verified. C-index and area under the curve (AUC) were selected to evaluate the differentiation ability of the nomogram.16,17 The nonadherence nomogram was verified by bootstrap validation (1,000 bootstrap resamples) to calculate a relatively corrected C-index.16,18 The decision curve analysis (DCA) and clinical impact plot analysis were employed to further evaluate the clinical effectiveness of the nomogram.
Results
Characteristics of Patients with Hyperlipidemia
There was a total of 685 patients included in the study. The average age was 63.95±11.08 years, including 297 males (43.36%) and 388 females (56.64%). The course of hyperlipidemia for more than 10 years was 199 (29.05%), and 526 (76.79%) patients were taking statins for lipid-lowering treatment. According to the MAAS score, the hyperlipidemia patients were divided into 2 groups: the medication adherence (447 patients) and medication nonadherence (238 patients) groups. All characteristics of patients including demographic, disease, clinical characteristics, and treatment in the two groups were displayed in Table 1.
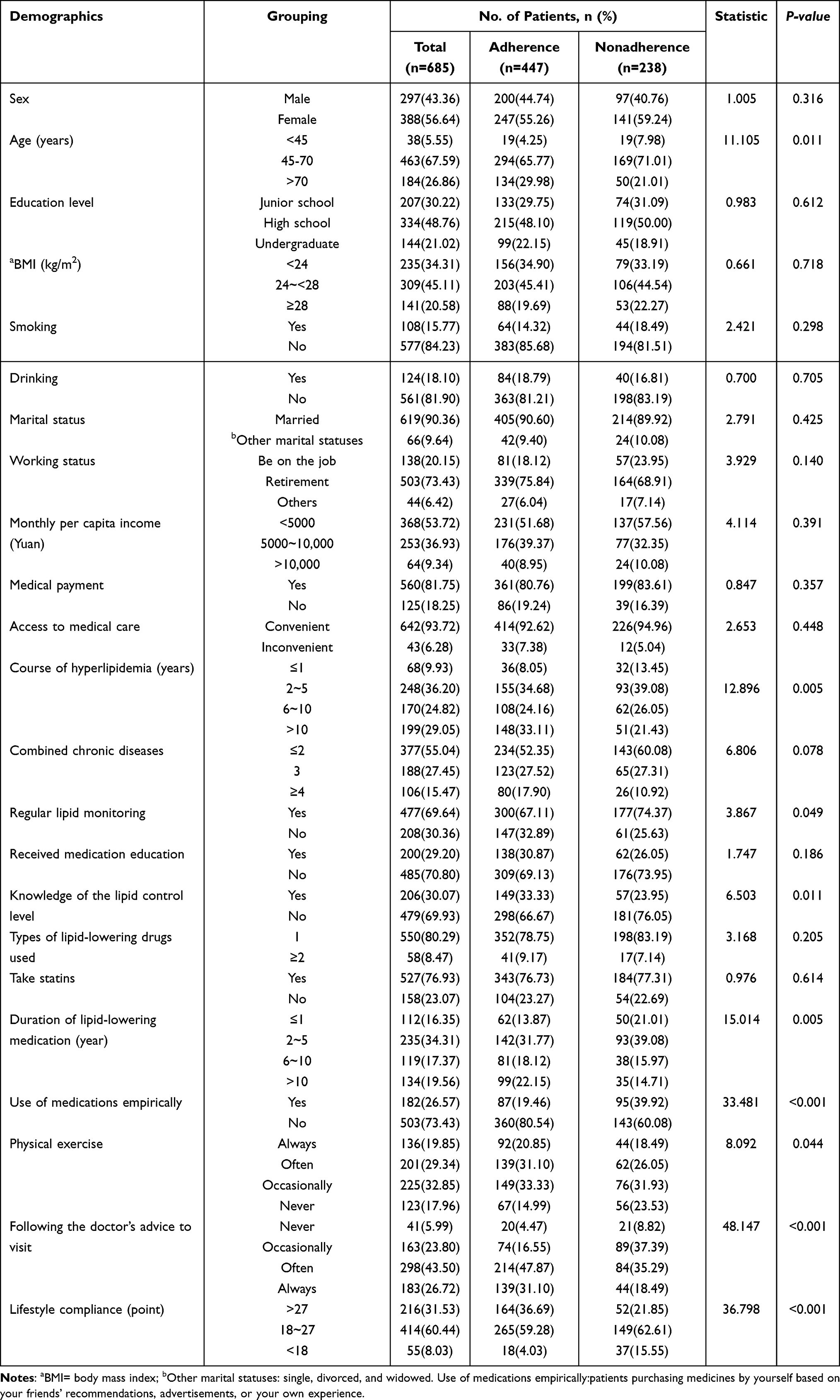 |
Table 1 Differences Between Demographic and Sociological Characteristics of Adherent and Nonadherent Hyperlipidemia Patients |
The Effect of Pharmacist Interventions on Medication Adherence
At the baseline, the patients with good, moderate, and poor compliance were 199 (29.05%), 248 (36.20%), and 238 (34.75%), respectively. Post-intervention, the patients with poor adherence was decreased significantly. And the patients with good, moderate, and poor compliance were 259 (37.81%), 244 (35.62%), and 182 (26.57%), respectively. A paired sample t-test was used to compare the correlation of medication adherence before and after the intervention. Post-intervention, the average score of medication adherence increased significantly (p < 0.001) from 20.75±8.01 to 29.90±6.93 (Figure 2).
 |
Figure 2 Comparison of changes in medication adherence pre- and post-intervention. ***: P < 0.001. |
The Effect of the Pharmaceutical Intervention on Blood Lipid Control
Pre-intervention, there were 213 cases with TC<5.2 mmol/L, 146 cases with TG< 1.7 mmol/L, 290 cases with LDL-C<3.4 mmol/L, and 366 cases with HDL-C≥1.0 mmol/L. The goal attainment rates of TC, TG, LDL-C, and HDL-C were 50.71%, 34.68%, 71.06%, and 93.36%, respectively. Post-intervention, the number of patients with TC, TG, LDL-C, and HDL-C reaching the standard was 264 (62.86%), 201 (47.43%), 318 (78.52%), and 377 (96.71%), respectively. Independent sample t-test was used to compare the changes in the results of blood lipid before and after the pharmaceutical intervention, with statistically significant differences in TC, TG, LDL-C, and HDL-C (p<0.001) (Table 2).
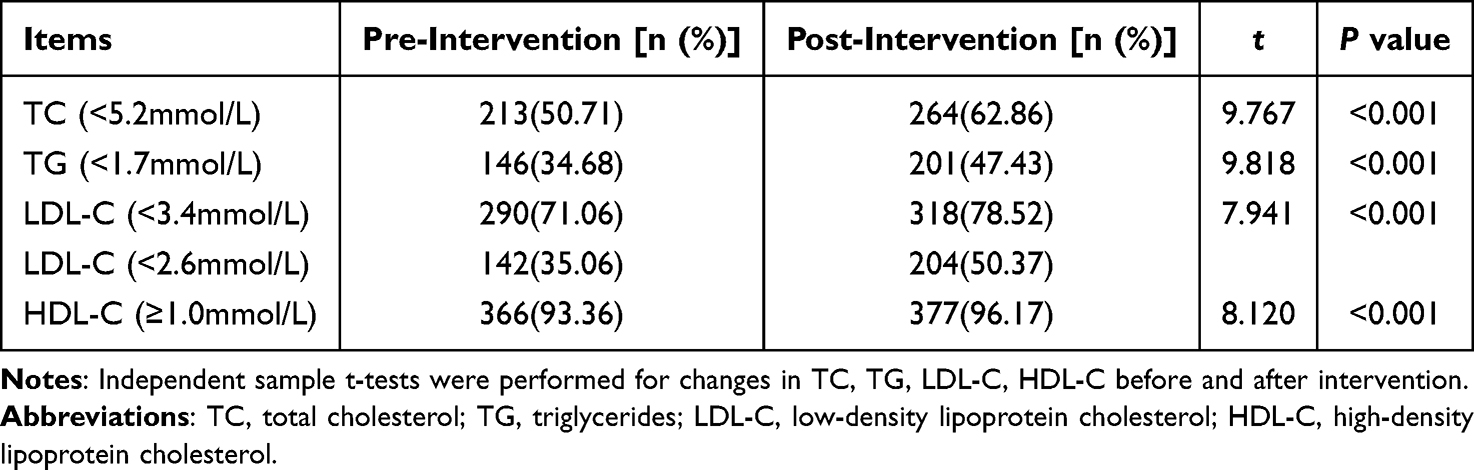 |
Table 2 The Effect of Blood Lipid Control Pre- and Post-Intervention |
Risk Factors Associated with Medication Nonadherence
Patients with good to moderate adherence were divided into one group (adherence), and patients with poor adherence were divided into another group (nonadherence), and one-way ANOVA was conducted to detect risk factors of medication nonadherence between the two groups (Table 1). Age, course of hyperlipidemia, regular lipid monitoring, knowledge of blood lipid control level, duration of lipid-lowering medication, taking drugs empirically, physical exercise, following the doctor’s advice to visit, and lifestyle compliance were the significant risk factors according to univariate analysis (p < 0.05). To reduce the influence of confounding factors, the factors identified above were further analyzed by multivariate logistic regression, and the prediction accuracy of the model was 72.7% (Table 3).
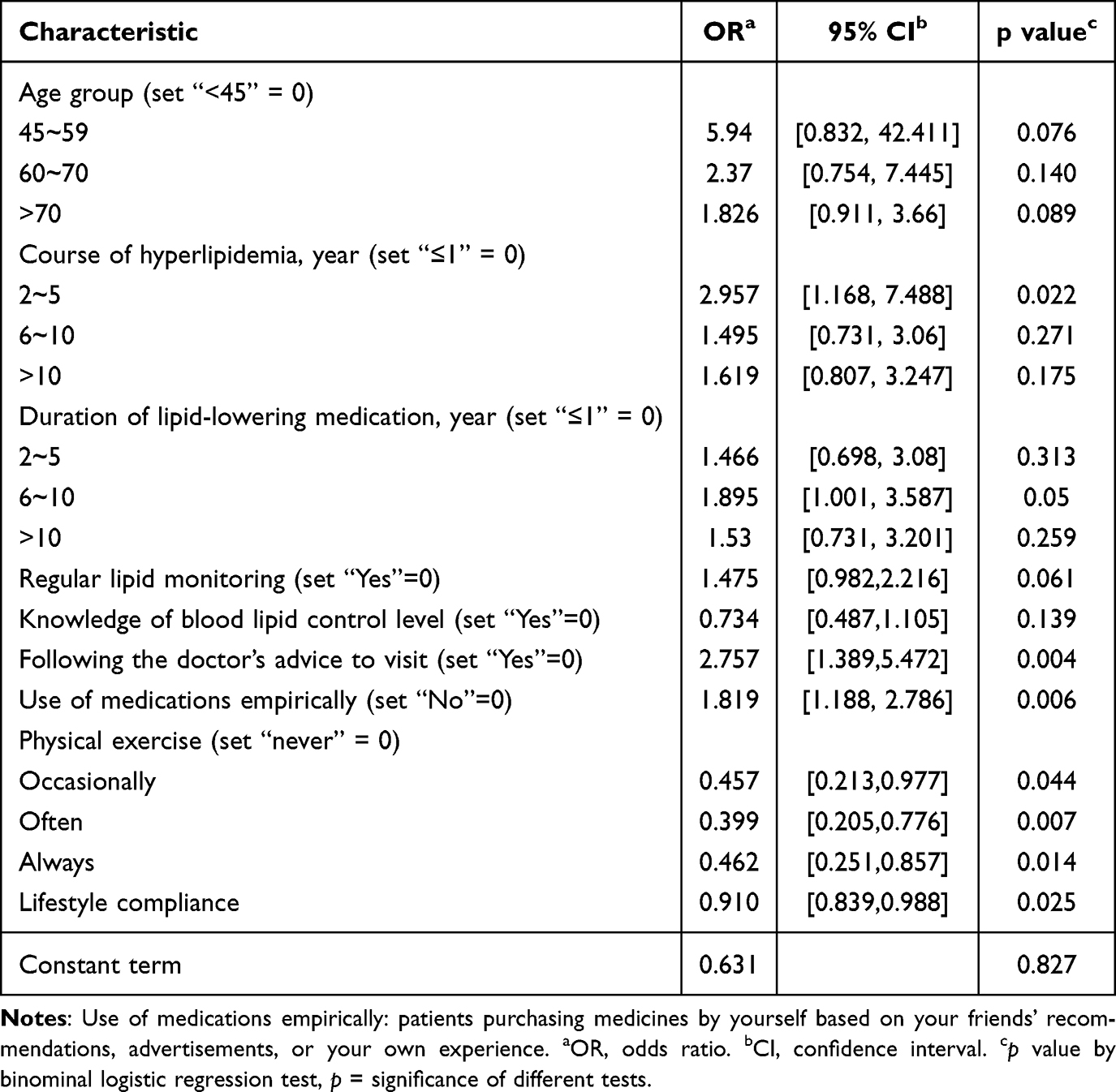 |
Table 3 Multivariate Logistic Regression Analysis of Risk Factors of Medication Nonadherence |
As the results are shown in Table 3, the factors that have a significant influence on medication nonadherence mainly include the course of hyperlipidemia (OR 2.957; 95% CI 1.168–7.488; P=0.022), use of medications empirically (OR 1.819; 95% CI 1.188–2.786; P=0.006), physical exercise (occasionally exercise (OR 0.457; 95% CI 0.213–0.977; P=0.044); often exercise (OR 0.399; 95% CI 0.205–0.776; P=0.007); always exercise (OR 0.462; 95% CI 0.251–0.857; P=0.014)), following the doctor’s advice to visit (OR 2.757; 95% CI 1.389–5.472; P=0.004), and lifestyle compliance (OR 0.910; 95% CI, 0.839–0.988; P=0.025). The course of hyperlipidemia, following the doctor’s advice to visit, and use of medications empirically were positively correlated with nonadherence. Physical exercise and lifestyle compliance were negatively correlated with nonmedication adherence.
Risk Prediction of Nonadherence in Patients with Hyperlipidemia
We established a nomogram model for predicting nonadherence in patients with hyperlipidemia according to the above 5 risk factors (Figure 3). The AUC was 0.927, indicating favorable discrimination and accuracy by the medication nonadherence risk nomogram (Figure 4). The internal bootstrap resampling approach suggested the nomogram has sufficient discriminatory power with a C-index of 0.87. The calibration slopes of this study also exhibited good nomogram consistency, and the prediction ability was good (Figure 5). DCA (Figure 6) and clinical impact plot analysis (Figure 7) also demonstrated that the nomogram model performs well in clinical practice.
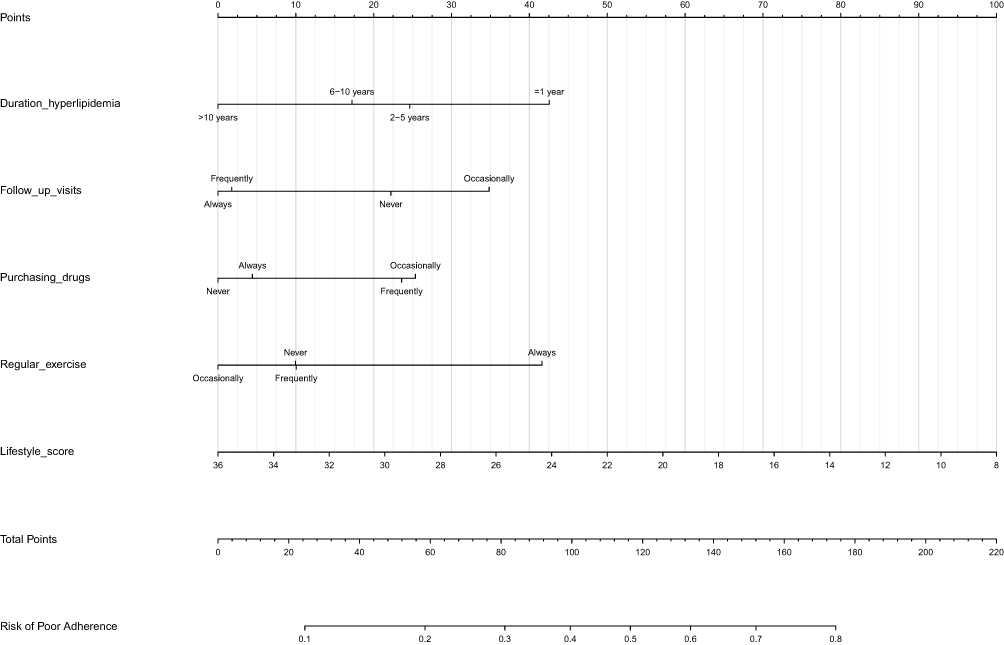 |
Figure 3 Nomogram prediction of medication nonadherence in patients with hyperlipidemia. |
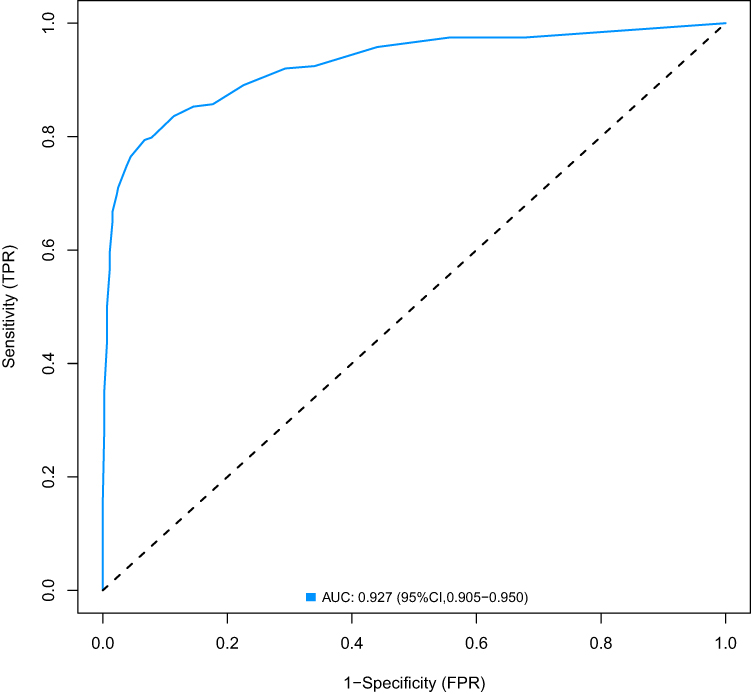 |
Figure 4 ROC curve based on the predictive nomogram for medication nonadherence in patients with hyperlipidemia. The dashed black line represents random performance (AUC=0.5), and solid blue line represents real performance (AUC=0.927). |
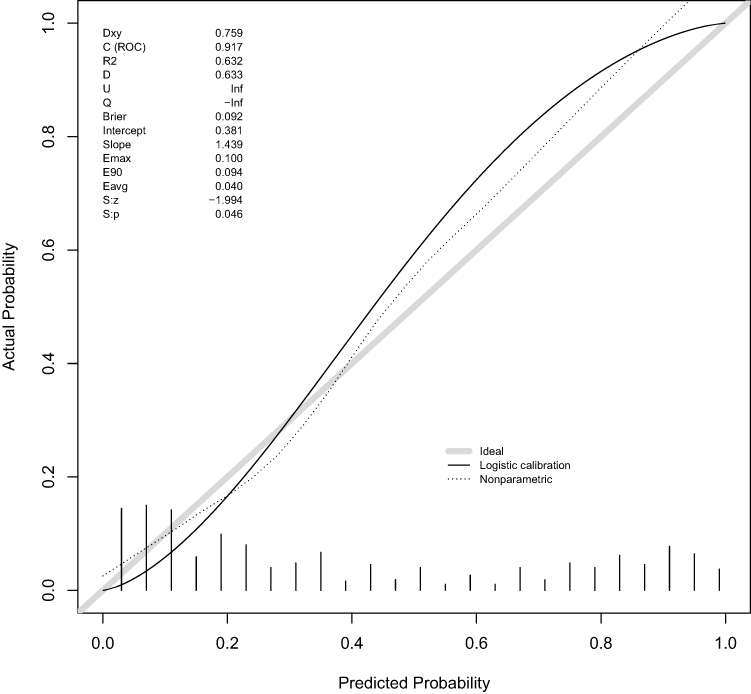 |
Figure 5 Calibration slopes of the nonadherence nomogram prediction. |
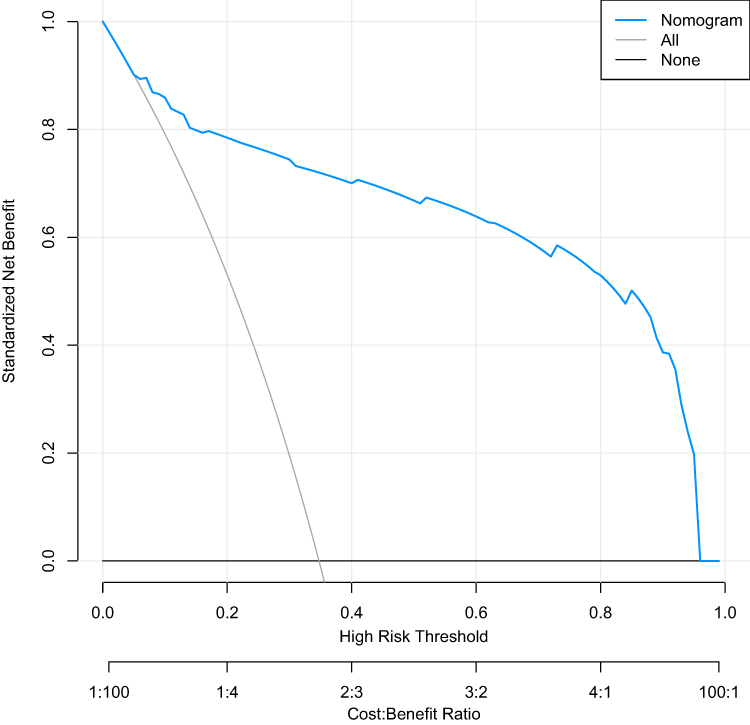 |
Figure 6 DCA of the nonadherence nomogram prediction. |
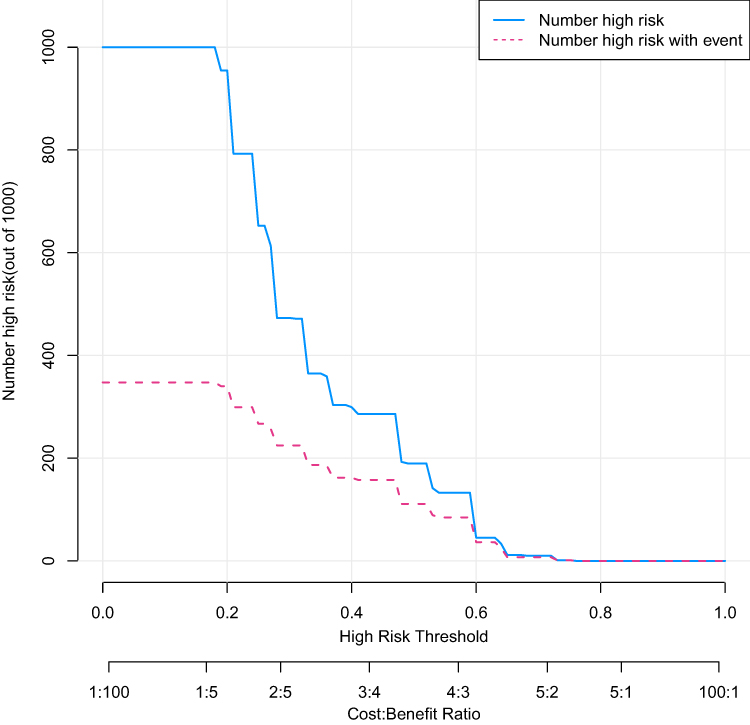 |
Figure 7 Clinical impact plot analysis of the nonadherence nomogram prediction. |
Discussion
The reported medication adherence of hyperlipidemia patients in our study was suboptimal but high compared to the global range.19,20 It was also higher than 57.9% from a previous study carried out in China.21 The findings indicated that the adherence of patients with hyperlipidemia had improved somewhat in recent years, although it was still not ideal. Previous studies have similarly found that medication nonadherence was higher for lipid-lowering medications among the four chronic disease medications assessed (including hypoglycemics, antihypertensives, lipid-lowering and antidepressants).22 Moreover, our study found that LDL-C control was better than 60.1% reported in a previous study in China23 and 53.8% reported in a study in Spanish.24 These results once again proved that improving adherence could ameliorate the control of hyperlipidemia. It was estimated that optimally controlled blood cholesterol would prevent 62% of coronary heart disease events.25 The hyperlipidemia patients with ASCVD had higher LDL-C levels than patients without ASCVD,26 indicating that more attention should be paid to medication adherence in hyperlipidemia patients with ASCVD.
Our results showed that 34.75% of patients with hyperlipidemia displayed medication nonadherence. Nonadherence negatively affects the efficacy, safety, and costs of therapies.27 A variety of factors can contribute to nonadherence,19 which can be grouped into social and economic-related factors, therapy-related factors, patient-related factors, and health provider and health system-related factors.7,28 In the analysis of risk factors for medication nonadherence, we found that duration of hyperlipidemia, taking drugs empirically, physical exercise, following the doctor’s advice to visit regularly, and lifestyle compliance were closely related to medication adherence. Patients with the duration of hyperlipidemia between 2 and 5 years were almost 3 times more nonadherent than patients with duration less than or equal to 1 year. The risk of nonadherence in patients who did not follow the doctor’s advice to visit were nearly 3 times that of patients who followed up periodically. Patients who take drugs empirically, who never exercise, or who were lifestyle noncompliant were more prone to nonadherence. Per a 1-point increase in lifestyle compliance score, the risk of nonadherence decreased by 9%.
Having effective, economical, and applicable techniques is essential for hyperlipidemia patients to change their adherence and improve their health. Pharmaceutical interventions constitute the primary strategies used to improve patient adherence.29 The findings of our study provided scientific evidence of the effectiveness of pharmaceutical interventions to improve the blood lipid control in patients with hyperlipidemia and reduce the number of patients with medication non-adherence, consistent with the previous study in which among participants taking lipid-lowering medication, low adherence was associated with higher mean LDL-C.30 Pharmaceutical interventions in our study involved comprehensive interventions and frequent contact with patients, which prompted that multi-faceted interventions were more likely to be effective in improving the overall outcome measures. Our results underscore the need for multidimensional interventions aimed at improving medication adherence and the overall health of patients with hyperlipidemia according to adherence risk factors. With the development of the Internet and the popularization of telemedicine, Telematics interventions can be used to improve patients’ medication adherence and clinical outcomes. A systematic review confirmed that telehealth modalities including eHealth and telehealth medication adherence interventions were associated with improved adherence.31 Future research could incorporate telehealth modalities interventions into multi-faceted measures to improve effectiveness.
However, nonadherence is a multifactorial problem, factors influencing medication adherence vary across studies.32,33 An overview of systematic reviews suggested that there was a social gradient in adherence. Whereas, for most factors, the evidence was not conclusive due to the risk of bias, inconsistency, or imprecision.27 In clinical practice, interventions could focus on the risk factors to improve antihyperlipidemic medication adherence. The nomogram model is a simple and effective tool to identify patients with high risk of nonadherence and can provide evidence for more targeted interventions. Nomograms have been widely used in the field of diagnosis and prognosis of diseases, such as oncology,34,35 hypertension,36 and in recent years have been successfully used in the prediction of medication nonadherence.17,18,37 To the best of our knowledge, this is the first study to use a nomogram to predict medication nonadherence in hyperlipidemia patients. The nomogram was established based on the five risk factors of a multivariate Logistic regression analysis of medication adherence. The internal bootstrap resampling approach suggested the nomogram has sufficient discriminatory power with a C-index of 0.87. The calibration slops also showed good consistency between the prediction and the observation. In recent years, many models for predicting disease risk factors have been mentioned in a few studies,38–40 but few for non-adherence.41 Compared to individual risk factors, the predictive model based on several risk factors is further capable of assisting the clinician in noticing the patients who are prone to non-adherence. Therefore, we presented and validated a nomogram, which is constructed by non-adherence influencing variables. Clinicians can utilize this model to estimate the risk of nonadherence and make preventions accordingly.
This study exhibits several notable strengths. First, it adopts a multicenter, prospective interventional design conducted across 35 hospitals in Beijing, ensuring a large and representative sample of 685 hyperlipidemia patients, which enhances the generalizability of findings within the population of Beijing districts. Second, the study integrates pharmacist-led comprehensive interventions, demonstrating significant improvements in both medication adherence and blood lipid control, providing direct evidence for clinical practice. Third, it identifies five key predictors of medication nonadherence through multivariate logistic regression, constructing a nomogram model with acceptable discriminative ability and good calibration. It is an individualized assessment tool for predicting risks of medication non-adherence, rarely reported in hyperlipidemia research.
This study has some limitations. First, using the cut-off value of 27 for adherence assessment in the adherence questionnaire, criterion validity was not enough good to validly screen a patient with nonadherence to medication. This may bias the determination of nonadherence. Second, our study may have unmeasured confounding variables, which could bias the results. For example, we did not investigate information about socioeconomic factors42 and health literacy,43 which were found to be important barriers to medication adherence. Third, although the robustness of our nomogram has been validated internally, we did not verify the nomogram externally. Therefore, it cannot be applied to hyperlipidemia populations in other regions and countries. It needs to be externally evaluated in a wider population with hyperlipidemia. Fourth, the questionnaire was assessed by self-report measures, which may be subjected to self-report biases.
Conclusion
(1) This study revealed a high rate of nonadherence to medication treatment for hyperlipidemia but it may possible to improve it by pharmacist-led interventions. Therefore, pharmacist-led interventions should be encouraged in the management of hyperlipidemia patients. (2) Medication nonadherence was significantly associated with long duration of hyperlipidemia, taking drugs empirically, never physical exercise, not following the doctor’s advice to visit regularly, and poor lifestyle compliance. And we developed a nomogram model with a relatively accurate predictive ability by internal validation. In future, we hope to integrate this model with community health records, thereby helping doctors identify high-risk hyperlipidemia patients with poor medication adherence.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The research was following the Declaration of Helsinki. The study was approved by the Ethics Committee of Beijing Tiantan Hospital, the reference number KY2020-085-02. Informed written consent has been obtained from each patient after a full explanation of the purpose and nature of all procedures used.
Acknowledgments
We thank all the pharmacists who participated in the study. The authors would like to appreciate all the hyperlipidemia patients who voluntarily participated in this study for their contribution to the success of this work.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 72404196) and clinical Pharmacy Research fund of the Beijing Pharmaceutical Society. (Funded project: Study on medication adherence and control rate of chronic disease). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448–457. doi:10.1056/NEJMra1201534
2. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
3. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
4. Luijten J, van Greevenbroek M, Schaper NC, et al. Incidence of cardiovascular disease in familial combined hyperlipidemia: a 15-year follow-up study. Atherosclerosis. 2019;280:1–6. doi:10.1016/j.atherosclerosis.2018.11.013
5. Masoura C, Pitsavos C, Aznaouridis K, et al. Arterial endothelial function and wall thickness in familial hypercholesterolemia and familial combined hyperlipidemia and the effect of statins. A systematic review and meta-analysis. Atherosclerosis. 2011;214(1):129–138. doi:10.1016/j.atherosclerosis.2010.10.008
6. Lee YR, Oh SS, Jang S-I, Park E-C. Statin adherence and risk of all-cause, cancer, and cardiovascular mortality among dyslipidemia patients: a time-dependent analysis. Nutr Metab Cardiovasc Dis. 2020;30(12):2207–2214. doi:10.1016/j.numecd.2020.07.024
7. Marzec LN, Maddox TM. Medication adherence in patients with diabetes and dyslipidemia: associated factors and strategies for improvement. Curr Cardiol Rep. 2013;15(11):418. doi:10.1007/s11886-013-0418-7
8. Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke Statistics—2016 update. Circulation. 2016;133(4):447–454. doi:10.1161/CIR.0000000000000366
9. Castellano JM, Bueno H, Fuster V. The cardiovascular polypill: clinical data and ongoing studies. Int J Cardiol. 2015;201:S8–S14. doi:10.1016/S0167-5273(15)31027-5
10. Liu H, Xin D, Wenhua W, et al. Statin adherence and influencing factors in hyperlipidemia patients treated in community health centers in Beijing. Chinese J Health Manage. 2018;12(4):300–306.
11. Rolnick SJ, Pawloski PA, Hedblom BD, Asche SE, Bruzek RJ. Patient characteristics associated with medication adherence. Clin Med Res. 2013;11(2):54–65. doi:10.3121/cmr.2013.1113
12. Taitel M, Jiang J, Rudkin R, Ewing D, Duncan D. The impact of pharmacist face-to-face counseling to improve medication adherence among patients initiating statin therapy. Patient Prefer Adherence. 2012;6:323–329. doi:10.2147/PPA.S29353
13. Byeon H. Predicting South Korean adolescents vulnerable to obesity after the COVID-19 pandemic using categorical boosting and shapley additive explanation values: a population-based cross-sectional survey. Front Pediatr. 2022;10:955339. doi:10.3389/fped.2022.955339
14. Wang X, Lu J, Song Z, Zhou Y, Liu T, Zhang D. From past to future: bibliometric analysis of global research productivity on nomogram (2000–2021). Front Public Health. 2022;10:997713. doi:10.3389/fpubh.2022.997713
15. Wu M, Xu X, Zhao R, Bai X, Zhu B, Zhao Z. Effect of pharmacist-led interventions on medication adherence and glycemic control in type 2 diabetic patients: a study from the chinese population. patient prefer adherence. Patient Preference and Adherence. 2023;17:119–129. doi:10.2147/PPA.S394201
16. Pencina MJ, D’Agostino RB. Overall C as a measure of discrimination in survival analysis: model specific population value and confidence interval estimation. Stat Med. 2004;23(13):2109–2123. doi:10.1002/sim.1802
17. Wang Y, Yao Y, Hu J, et al. Development of a predictive nomogram for estimating medication nonadherence in hemodialysis patients. Med Sci Monit. 2022;28:e934482. doi:10.12659/MSM.934482
18. Wang H, Zhang L, Liu Z, et al. Predicting medication nonadherence risk in a Chinese inflammatory rheumatic disease population: development and assessment of a new predictive nomogram. Patient Prefer Adherence. 2018;12:1757–1765. doi:10.2147/PPA.S159293
19. Wiegand P, McCombs JS, Wang JJ. Factors of hyperlipidemia medication adherence in a nationwide health plan. Am J Manag Care. 2012;18(4):193–199.
20. Yim -H-H, Hwang H-S, Park H-K, Park K-Y, Park M. Association between patient experience and medication compliance of dyslipidemia: using korea national health and nutrition examination survey (2015). Korean J Fam Med. 2021;42(2):116–122. doi:10.4082/kjfm.19.0128
21. Zheng F, Ding S, Lai L, et al. Relationship between medication literacy and medication adherence in inpatients with coronary heart disease in Changsha, China. Front Pharmacol. 2019;10:1537. doi:10.3389/fphar.2019.01537
22. Lemstra M, Nwankwo C, Bird Y, Moraros J. Primary nonadherence to chronic disease medications: a meta-analysis. Patient Prefer Adherence. 2018;12:721–731. doi:10.2147/PPA.S161151
23. Yan X, Li Y, Dong Y, et al. Blood pressure and low-density lipoprotein cholesterol control status in Chinese hypertensive dyslipidemia patients during lipid-lowering therapy. Lipids Health Dis. 2019;18(1):32. doi:10.1186/s12944-019-0974-y
24. Lahoz C, Mostaza JM, Pinto X, et al. LDL-cholesterol control in patients with genetic dyslipidemia followed up by lipid and vascular risk units of the spanish society of arteriosclerosis. Clin Investig Arterioscler. 2015;27(1):1–8. doi:10.1016/j.arteri.2014.04.001
25. Thomas F, Bean K, Guize L, et al. Combined effects of systolic blood pressure and serum cholesterol on cardiovascular mortality in young (<55 years) men and women. Eur Heart J. 2002;23(7):528–535. doi:10.1053/euhj.2001.2888
26. Liu G, Shepherd J, Rane P, et al. Characteristics of patients with dyslipidemia treated in routine care setting in China. Journal of Drug Assessment. 2019;8(1):192–198. doi:10.1080/21556660.2019.1684926
27. Gast A, Mathes T. Medication adherence influencing factors—an (updated) overview of systematic reviews. Syst Rev. 2019;8(1):112. doi:10.1186/s13643-019-1014-8
28. Mondesir FL, Levitan EB, Malla G, et al. Patient perspectives on factors influencing medication adherence among people with coronary heart disease (CHD) and CHD risk factors. Patient Prefer Adherence. 2019;13:2017–2027. doi:10.2147/PPA.S222176
29. Milosavljevic A, Aspden T, Harrison J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: a systematic review. Int J Pharm Pract. 2018;26(5):387–397. doi:10.1111/ijpp.12462
30. Hennein R, Hwang S-J, Au R, et al. Barriers to medication adherence and links to cardiovascular disease risk factor control: the Framingham heart study. Intern Med J. 2018;48(4):414–421. doi:10.1111/imj.13687
31. Bingham JM, Black M, Anderson EJ, et al. Impact of telehealth interventions on medication adherence for patients with type 2 diabetes, hypertension, and/or dyslipidemia: a systematic review. Ann Pharmacother. 2021;55(5):637–649. doi:10.1177/1060028020950726
32. Caliskan UA, Yurdakul FG, Bodur H. What are the risk factors of poor medication adherence in the target-to-treat era? Turk J Phys Med Rehabil. 2019;65(4):343–351. doi:10.5606/tftrd.2019.3071
33. Yue Z, Bin W, Weilin Q, Aifang Y. Effect of medication adherence on blood pressure control and risk factors for antihypertensive medication adherence. Journal of Evaluation in Clinical Practice. 2015;21(1):166–172. doi:10.1111/jep.12268
34. Balasubramanian D, Subramaniam N, Missale F, et al. Predictive nomograms for oral tongue squamous cell carcinoma applying the American Joint Committee on Cancer/Union Internationale Contre le Cancer 8th edition staging system. Head Neck. 2021;43(4):1043–1055. doi:10.1002/hed.26554
35. Wang X, Mao M, He Z, et al. Development and validation of a prognostic nomogram in AFP-negative hepatocellular carcinoma. Int J Biol Sci. 2019;15(1):221–228. doi:10.7150/ijbs.28720
36. Deng X, Hou H, Wang X, et al. Development and validation of a nomogram to better predict hypertension based on a 10-year retrospective cohort study in China. Elife. 2021;10. doi:10.7554/eLife.66419
37. QiMuge N, Fang X, Chang B, Li DM, Li Y. Predicting population: development and validation of a new predictive nomogram for evaluating medication nonadherence risk in a type 2 diabetes. Peerj. 2022;10:e13102. doi:10.7717/peerj.13102
38. Chen D, Li Y, Li Q, et al. Risk factors and a nomogram model establishment for postoperative delirium in elderly patients undergoing arthroplasty surgery: a single-center retrospective study. Biomed Res Int. 2021;2021(1):6607386. doi:10.1155/2021/6607386
39. Zhou Z, Yin X, Niu Q, et al. Risk factors and a nomogram for predicting intracranial hemorrhage in stroke patients undergoing thrombolysis. Neuropsychiatr Dis Treat. 2020;16:1189–1197. doi:10.2147/NDT.S250648
40. Mosk CA, van Vugt J, de Jonge H, et al. Low skeletal muscle mass as a risk factor for postoperative delirium in elderly patients undergoing colorectal cancer surgery. Clin Interv Aging. 2018;13:2097–2106. doi:10.2147/CIA.S175945
41. Chu H-Y, Huang H-C, Huang C-Y, et al. A predictive model for identifying low medication adherence among older adults with hypertension: a classification and regression tree model. Geriatric Nursing. 2021;42(6):1309–1315. doi:10.1016/j.gerinurse.2021.08.011
42. Kvarnstrom K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
43. Schonfeld MS, Pfisterer-Heise S, Bergelt C. Self-reported health literacy and medication adherence in older adults: a systematic review. BMJ Open. 2021;11(12):e056307. doi:10.1136/bmjopen-2021-056307
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preoperative Systemic Inflammatory Markers as a Significant Prognostic Factor After TURBT in Patients with Non-Muscle-Invasive Bladder Cancer
Ding L, Deng X, Wang K, Xia W, Zhang Y, Zhang Y, Shao X, Wang J
Journal of Inflammation Research 2023, 16:283-296
Published Date: 21 January 2023
Predicting the Risk of Incorrect Inhalation Technique in Patients with Chronic Airway Diseases by a New Predictive Nomogram
Chen S, Peng Y, Shen B, Zhong L, Wu Z, Zheng J, Gao Y
Journal of Asthma and Allergy 2023, 16:159-172
Published Date: 24 January 2023
Development and External Validation of Nomogram to Identify Risk Factors for CHD in T2DM in the Population of Northwestern China
Meng Q, Yang J, Wang F, Li C, Sang G, Liu H, Shen D, Zhang J, Jiang S, Yusufu A, Du G
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1271-1282
Published Date: 4 May 2023
Establishment and Validation of a Nomogram Prediction Model for the Severe Acute Pancreatitis
Li B, Wu W, Liu A, Feng L, Li B, Mei Y, Tan L, Zhang C, Tian Y
Journal of Inflammation Research 2023, 16:2831-2843
Published Date: 8 July 2023
A Retrospective Study of Biological Risk Factors Associated with Primary Knee Osteoarthritis and the Development of a Nomogram Model
Zhang Q, Yao Y, Chen Y, Ren D, Wang P
International Journal of General Medicine 2024, 17:1405-1417
Published Date: 9 April 2024