Back to Journals » Journal of Inflammation Research » Volume 16
Preoperative Systemic Inflammatory Markers as a Significant Prognostic Factor After TURBT in Patients with Non-Muscle-Invasive Bladder Cancer
Authors Ding L ![]() , Deng X, Wang K, Xia W, Zhang Y, Zhang Y, Shao X, Wang J
, Deng X, Wang K, Xia W, Zhang Y, Zhang Y, Shao X, Wang J
Received 20 October 2022
Accepted for publication 24 December 2022
Published 21 January 2023 Volume 2023:16 Pages 283—296
DOI https://doi.org/10.2147/JIR.S393511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Li Ding,1,* Xiaobin Deng,2,* Kun Wang,1,* Wentao Xia,1,* Yang Zhang,1 Yan Zhang,1 Xianfeng Shao,1 Junqi Wang1
1Department of Urology, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221000, People’s Republic of China; 2Department of Urology, the First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 530000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junqi Wang, Email [email protected]
Introduction: Neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and lymphocyte/monocyte ratio (LMR) have been widely proposed to have predictive value for the patient prognosis of many malignancies, including bladder cancer. However, the predictive value of their combination in non-muscle-invasive bladder cancer (NMIBC) is unclear.
Methods: Cases of NMIBC patients who underwent transurethral resection of the bladder tumor were recruited from two tertiary public medical centers. A systemic inflammatory marker (SIM) score was calculated based on comprehensive consideration of NLR, PLR, and LMR. Recurrence-free survival (RFS) and progression-free survival (PFS) were estimated by Kaplan-Meier analysis. The Log rank test was used to compare differences between the groups. Cox regression was used to screen risk factors affecting RFS and PFS. Nomogram models were established and validated, and patients were stratified based on the model scores.
Results: The study dataset was grouped according to a 7:3 randomization, with the training cohort consisting of 292 cases and the validation cohort consisting of 124 cases. Cox regression analysis showed that SIM score is an independent predictor of RFS and PFS in NMIBC patients. The novel models were established based on the SIM score and other statistically significant clinicopathological features. The area under the curve (AUC) for predicting 1-, 2-, and 3-year RFS was 0.667, 0.689, and 0.713, respectively. The AUC for predicting 1-, 2-, and 3-year PFS was 0.807, 0.775, and 0.862, respectively. Based on the risk stratification, patients at high risk of recurrence and progression could be accurately identified. The established models were applied to the patient evaluation of the validation cohort, which proved the great performance of the novel models.
Conclusion: The novel models based on the SIM score and clinicopathological characteristics can accurately predict the survival prognosis of NMIBC patients, and the models can be used by clinicians for individualized patient assessment and to assist in clinical decision-making.
Keywords: systemic inflammatory markers, risk factor, bladder cancer, NMIBC, tumor recurrence, nomogram
Introduction
The proportion of patients initially diagnosed with non-muscle-invasive bladder cancer (NMIBC) accounts for the majority of bladder cancers.1 Patients with NMIBC have a relatively good prognosis compared to those who progress to muscle-invasive bladder cancer (MIBC).2,3 Unfortunately, even after transurethral resection of the bladder tumor (TURBT) and regular postoperative intravesical instillation, tumor recurrence and progression seem to be inevitable.4–6 The risk scoring models established by the European Association of Urology (EAU)2 and the Spanish Urological Organization (Club Urologico Español de Tratamiento Oncologico, CUETO)3 for NMIBC were proposed at the beginning of the 21st century and have proven to be clinically effective.7,8
Numerous studies have shown that different sites of initial invasion have different risks of postoperative progression, and patients with bladder neck invasion (BNI) had the highest risk.9–13 Mediators such as chemokines or cytokines induce an inflammatory state in the body and promote the proliferation and progression of tumor cells. On the other hand, activation of oncogenes can drive the carcinogenesis of an inflammatory state. Thus, inflammation and cancer are mutually reinforcing and closely related.14–17 Neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and lymphocyte/monocyte ratio (LMR), as widely studied systemic inflammatory response indicators, have been widely proven to be valuable predictors of a variety of malignancies.18–20 Some studies focused on NMIBC patients have also shown that these systemic inflammatory response indicators have great potential for application.21–24 In 2018, Cantiello et al first proposed the concept of a “systemic inflammatory marker” (SIM) score, and analyzed it in a cohort of NMIBC patients, which showed that the SIM score can be an independent predictor of recurrence and progression in NMIBC patients.25 This study was innovative, but not modeling it accordingly reduced its usefulness.
There are no studies that have validated the value of the SIM score and integrated the analysis of systemic inflammatory response indicators and BNI. The aim of our study is to comprehensively assess the prognostic role of SMI and BNI in patients with NMIBC who underwent TURBT.
Materials and Methods
Study Population
This study was performed in line with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University and the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University. The medical record databases of two tertiary public medical centers were retrospectively searched to collect data on patients with a pathological diagnosis of “urothelial carcinoma of the bladder” from October 2018 to June 2021. The inclusion criteria were as follows: (1) the surgery was performed in a consistent fashion; (2) postoperative histopathology confirmed urothelial carcinoma of the bladder; (3) specific pathological staging records after surgery. The exclusion criteria were as follows: (1) patients who received adjuvant therapy other than adjuvant intravesical instillation before or after TURBT; (2) clinical, laboratory, and follow-up data were incomplete; (3) tumor recurrence, progression, or death that occurred within one month. The serum biomarkers were collected within one week before surgery. Recurrence-free survival (RFS) was defined as the time from TURBT to the first evidence of either recurrent (or progression), cancer-related death, or last follow-up. Progression-free survival (PFS) was defined as the time from TURBT to the first evidence of progression, cancer-related death, or last follow-up.
Statistical Analysis
Data were collected from a total of 416 patients, and 292 patients were included in the training group through a 7:3 randomization. SIM were transformed from continuous variables to categorical variables using the X-tile program based on the total study cohort. Assign a value of 0 to protective subgroups and 1 to risk subgroups; therefore, the SIM score ranges from 0 to 3. Continuous data are presented as mean (±standard deviation) or median (interquartile range, IQR), categorical data as frequency and percentage. The Chi-square tests were used for categorical variables, and the Mann–Whitney U-tests were used for non-normally distributed continuous variables. Kaplan–Meier analysis was applied with Log rank testing. The univariate and multivariate Cox regression analyses were used to calculate the hazard ratio (HR) with a 95% confidence interval (CI) to identify risk factors. The models validation was performed by the area under the receiver operating characteristics curve (AUC) for discrimination ability and calibration curves for calibration ability. Decision curve analysis (DCA) was performed to determine the clinical net benefit associated with using the predictive models at different threshold probabilities in the patient cohort. After the models were established, patients were stratified by calculating the total points of individual patients. X-tile 3.6.1 (http://tissuearray.org/), SPSS 26.0 (IBM Corp., Chicago, IL), and R 4.1.2 (http://www.R-project.org/) were used to statistically analyze the database. A P-value <0.05 was considered to denote statistical significance.
Results
Patient Characteristics
As shown in Table 1, in the training cohort, the median age at diagnosis was 66 years old (IQR 58–74), median tumor size was 20 millimeter (mm) (IQR 15–30), median NLR was 1.863 (IQR 1.429–2.670), median PLR was 113.7 (IQR 90–151.429), and median LMR was 4.348 (IQR 3.265–5.510). The majority of NMIBC patients were male (83.904%) and non-overweight (60.616%). Most tumors status were in Ta stage (59.932%), primary status (86.986%), high pathology grade (57.534%) and multiple lesions (54.110%). Over half of the patients denied a smoking history. The cut-off value for NLR, PLR and LMR was 2.12, 175.71, and 4.58, respectively. Most patients had preoperative NLR and PLR less than the cut-off value (61.643%, 85.616%, respectively), and with LMR greater than or equal to the cut-off value (56.507%) (Table 2). According to the maker cutoffs, we found that patients with NLR≥2.12 or LMR<4.58 have a higher percentage of older patients (p=0.008, p=0.016, respectively); and patients with PLR≥175.71 have a higher percentage of larger tumor size (p=0.02). Table 3 lists the clinical and pathologic variables according to the SIM score. Based on the results in our pre-analysis (Figure 1), elevated NLR, elevated PLR and decreased LMR were identified as risk factors for NMIBC patient prognosis. Therefore, we assigned a value of 0 to the subgroup with NLR and PLR less than the cut-off point and a value of 1 to the subgroup with LMR less than the cut-off point. The majority of patients had a SIM score of 0. The proportion of patients with scores of 0, 1, 2, and 3 was 38.014%, 26.370%, 23.973%, and 11.644%, respectively.
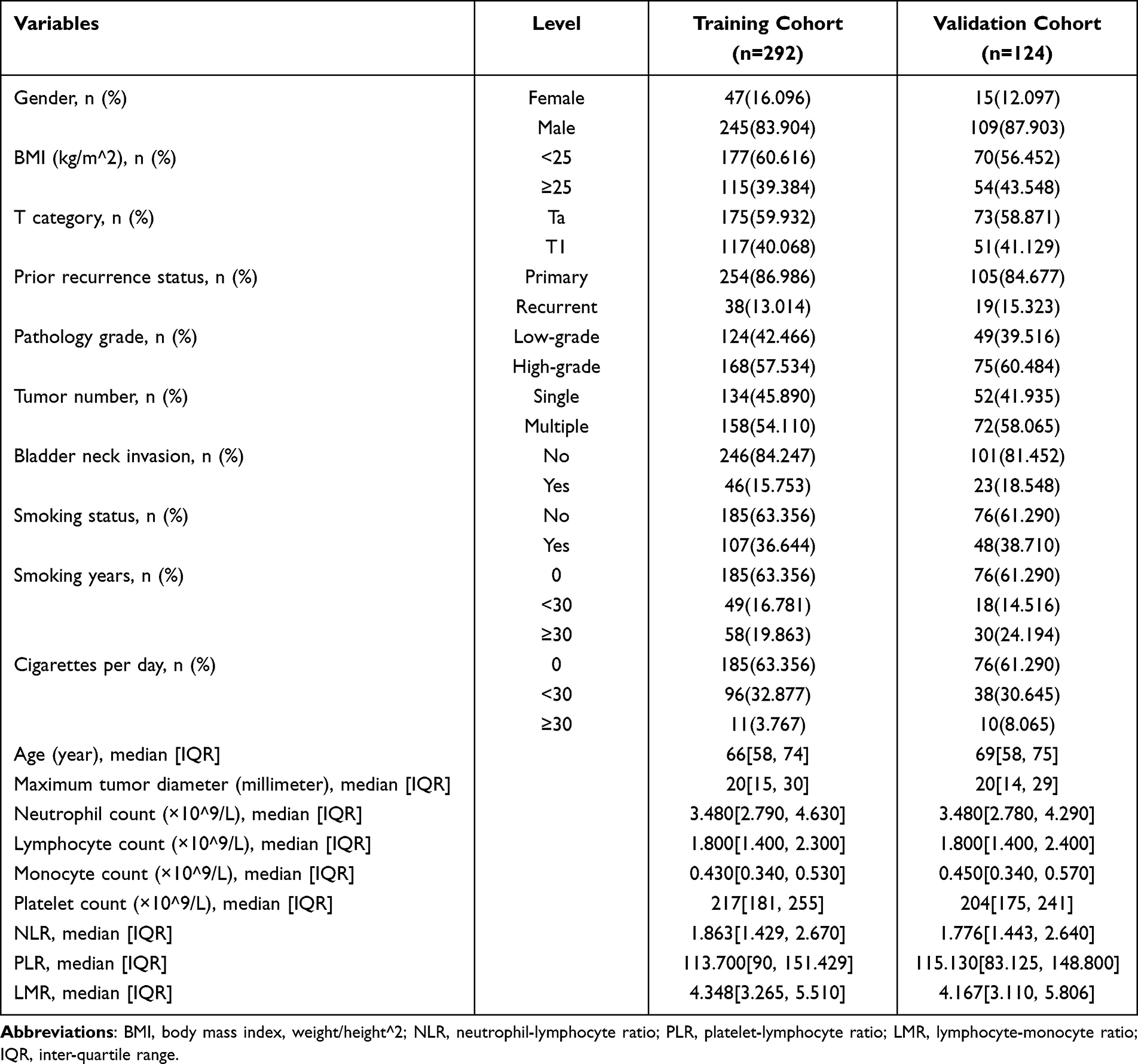 |
Table 1 Baseline Demographics & Clinical Characteristics of Study Population |
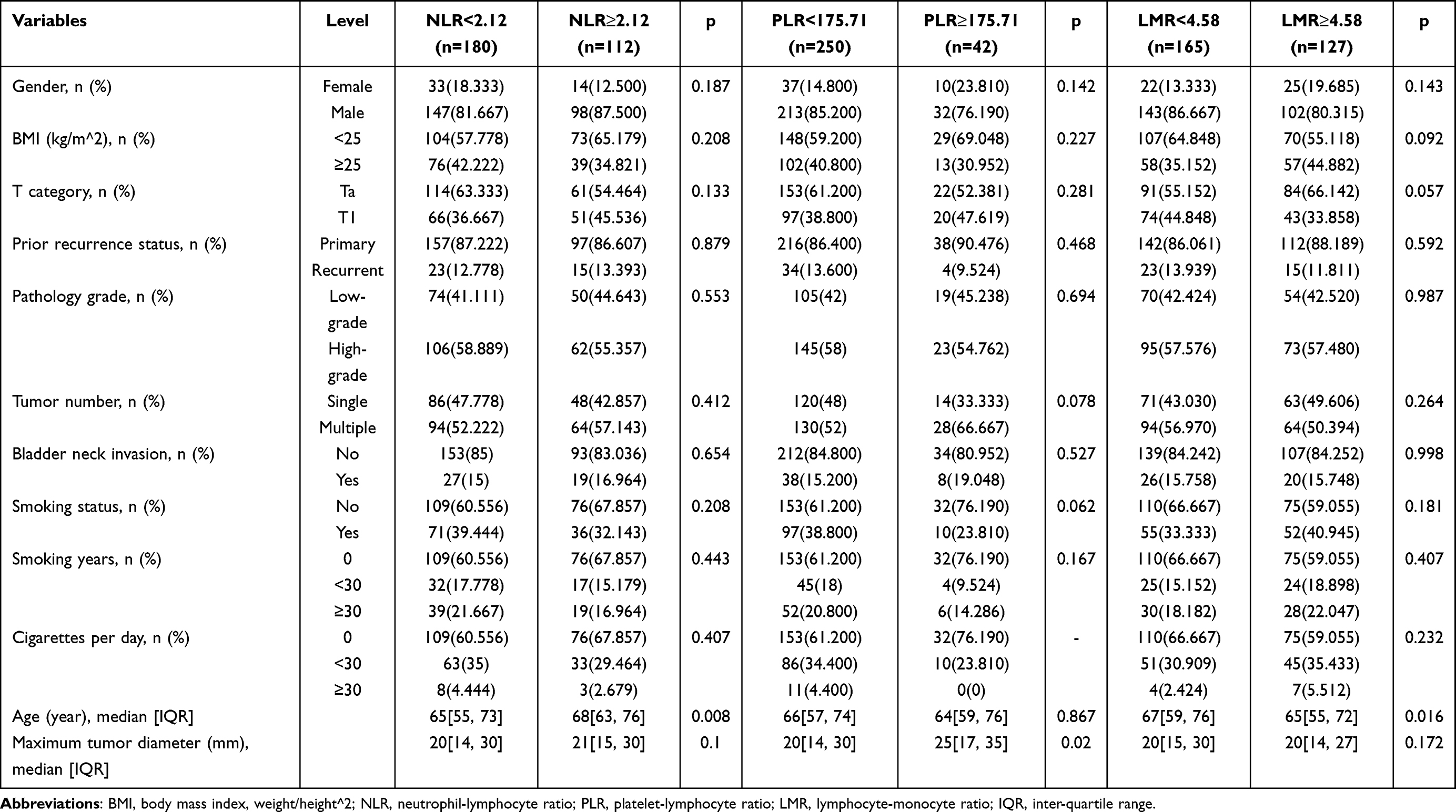 |
Table 2 Demographics & Clinical Characteristics According to NLR, PLR and LMR in the Training Cohort |
 |
Table 3 Demographics & Clinical Characteristics According to SMI Score in the Training Cohort |
 |
Figure 1 The Kaplan-Meier analysis of RFS stratified by (A) NLR, (B) PLR, (C) LMR; and the Kaplan-Meier analysis of PFS stratified by (D) NLR, (E) PLR, (F) LMR in the training cohort. |
Associations of SIM Score with Recurrence-Free Survival and Progression-Free Survival
We used Kaplan-Meier survival analysis to examine whether the SIM score correlated with patients’ RFS and PFS. Patients were divided into four groups based on the SIM score. As shown in Figure 2, the SIM score can accurately distinguish NMIBC patients with different risks of recurrence and progression (p=0.0013 in RFS, p=0.00015 in PFS). The higher the SIM score, the worse the prognosis of the patients.
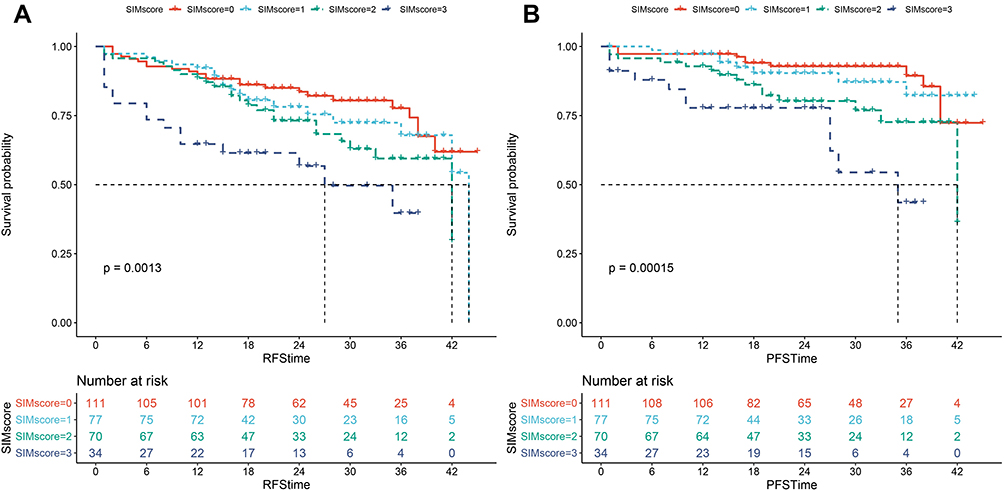 |
Figure 2 The Kaplan-Meier analysis of (A) RFS and (B) PFS stratified by SIM score in the training cohort. |
Screening for Predictive Factors
In univariate regression (Tables 4 and 5), T category (HR=1.729, p=0.013 for RFS, and HR=2.642, p=0.002 for PFS), prior recurrence status (HR=2.461, p=0.001 for RFS, and HR=3.188, p<0.001 for PFS), pathology grade (HR=1.628, p=0.039 for RFS, and HR=3.395, p=0.001 for PFS), tumor number (HR=2.045, p=0.003 for RFS, and HR=3.220, p=0.001 for PFS), BNI (HR=2.133, p=0.003 for RFS, and HR=3.447, p<0.001 for PFS), and SIM score (p=0.003 for RFS, and p=0.001 for PFS) were suggested to be associated with both RFS and PFS. The statistically significant variables in the univariate analysis were then assessed by using the multivariate Cox regression. Ultimately, prior recurrence status (HR=2.564, p=0.001), tumor number (HR=1.968, p=0.008), and SIM score (p=0.002) proved to be independent predictors of RFS, while prior recurrence status (HR=3.172, p=0.003), pathology grade (HR=2.644, p=0.016), tumor number (HR=3.325, p=0.002), and SIM score (p=0.001) were independent predictors of PFS.
 |
Table 4 Univariable and Multivariable Analysis for Predicting Recurrence-Free Survival |
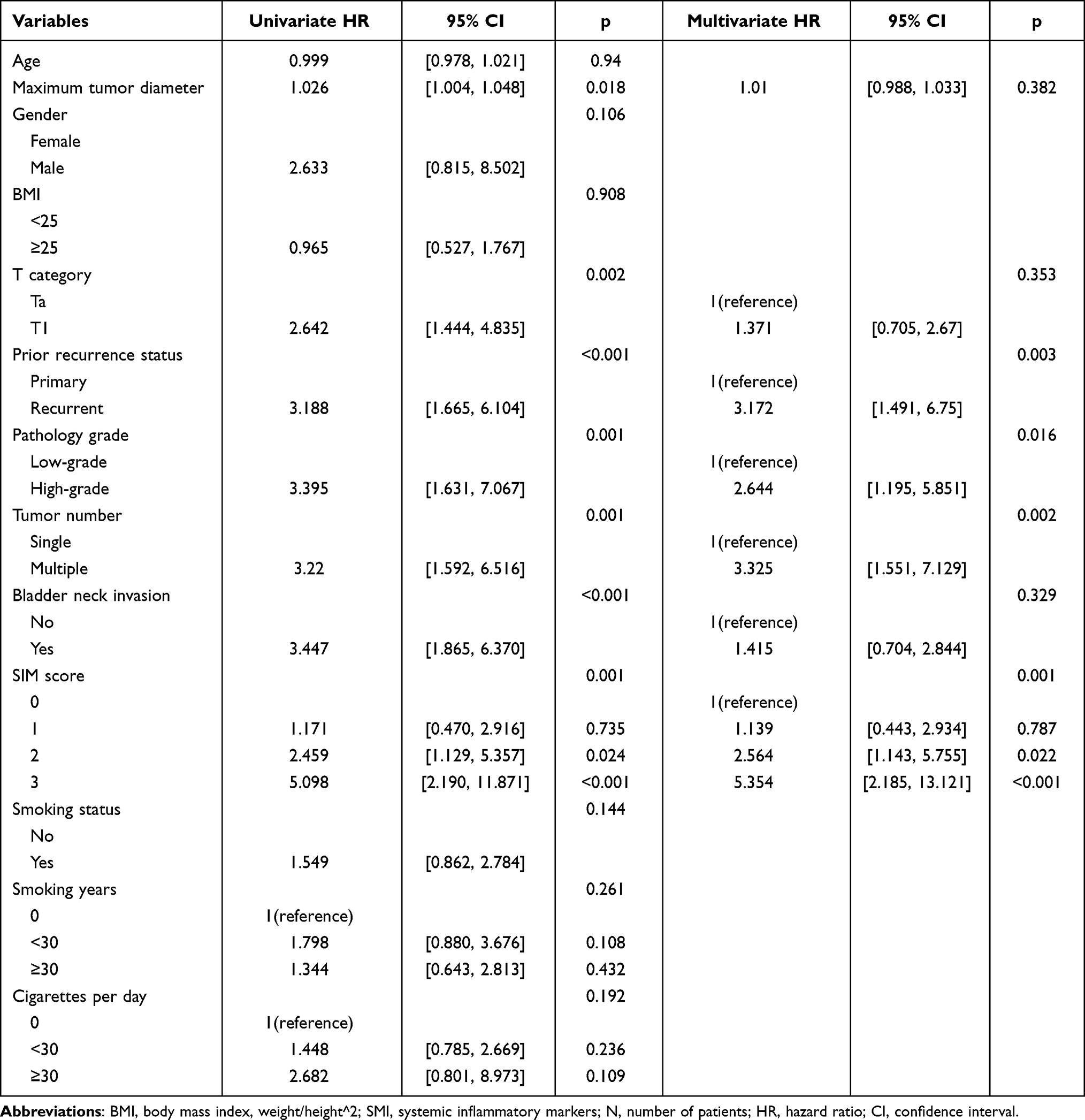 |
Table 5 Univariable and Multivariable Analysis for Predicting Progression-Free Survival |
Development and Validation of the Nomogram Models
The nomogram models were constructed based on the results in the Cox regression (Figures 3A and 4A). The receiver operating characteristic (ROC) curves showed the great predictive accuracy regarding 1-, 2-, and 3-year PFS rates of the models, with the AUC reaching 0.807, 0.775 and 0.862, respectively (Figure 4B). Meanwhile, when predicting patient’s 1-, 2-, and 3-year RFS rates, the AUC was 0.667, 0.689 and 0.713, respectively (Figure 3B). The calibration plots validated by 1000 bootstrap resampling proved the appreciable reliability of new models (Figures 3C and 4C). The DCA curve demonstrated a greater clinical benefit of the new models (Figures 3D and 4D). The AUC and calibration curves of the established models in the validation cohort for predicting RFS and PFS also showed great performance (Figure 5). Patients were then classified into low-risk group or high-risk group based on the models (cutoff-value=149.95 for RFS and 180.84 for PFS). The Kaplan–Meier survival analysis showed the patients in the high-risk group had a clearly worse survival outcomes than patients in the low-risk group (both p < 0.0001) (Figure 6).
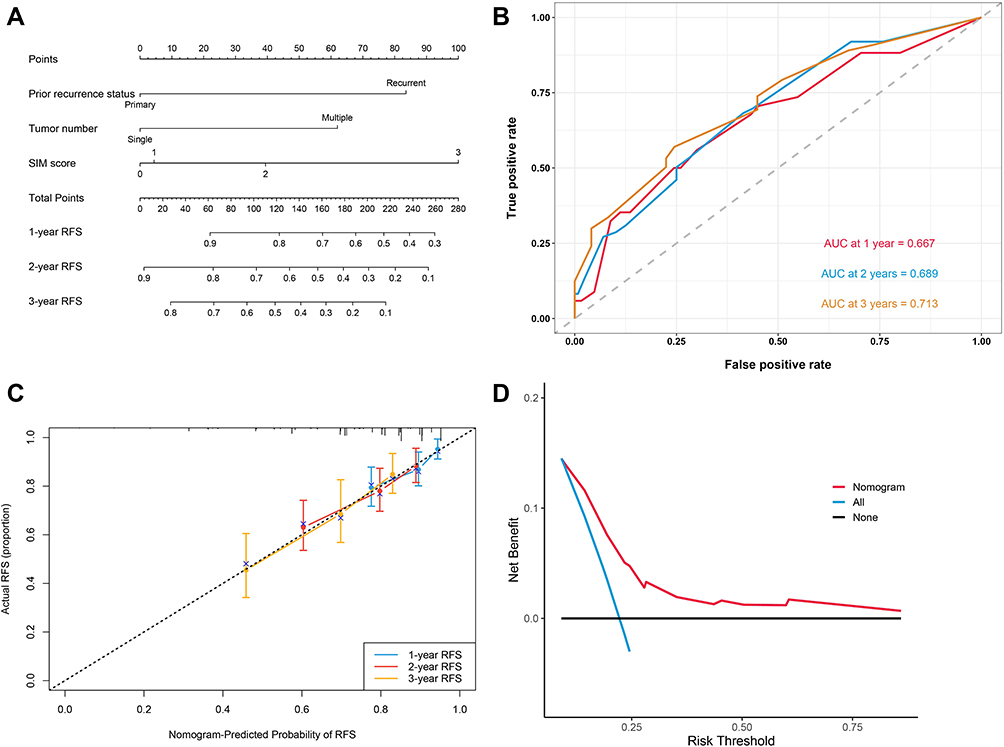 |
Figure 3 (A) The nomogram for predicting RFS after TURBT for NMIBC. (B) Time-dependent ROC curves of the nomogram for predicting RFS in the training cohort. (C) Calibration plot of the nomogram by bootstrapping with 1000 resamples for predicting RFS in the training cohort. (D) Decision-curve analyses demonstrating the net benefit associated with the use of the model for predicting RFS. |
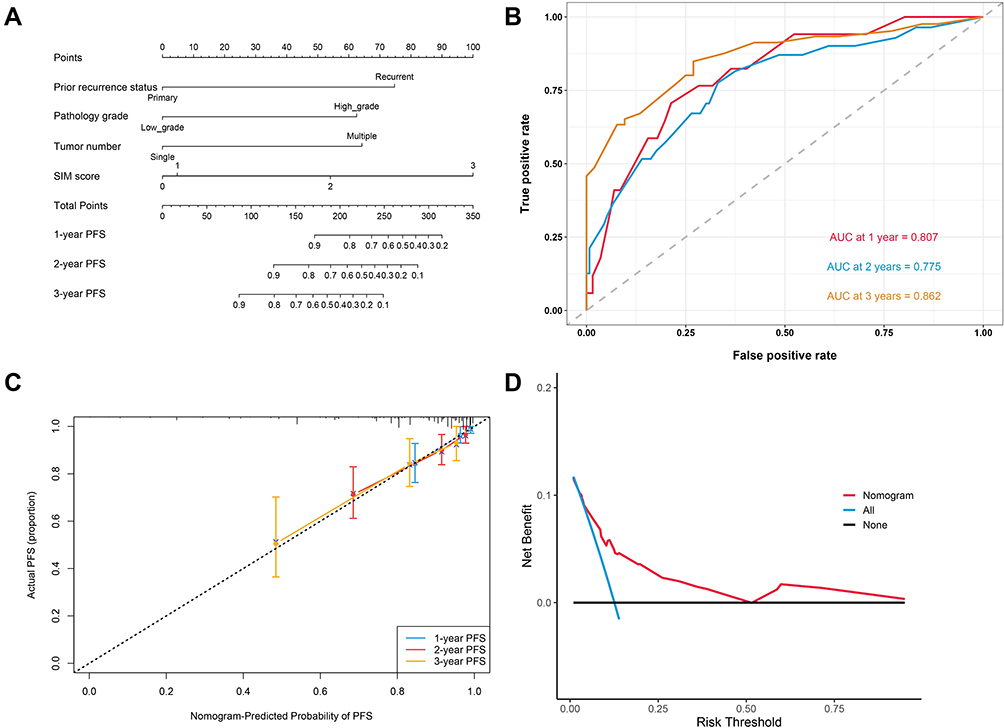 |
Figure 4 (A) The nomogram for predicting PFS after TURBT for NMIBC. (B) Time-dependent ROC curves of the nomogram for predicting PFS. (C) Calibration plot of the nomogram by bootstrapping with 1000 resamples for predicting PFS. (D) Decision-curve analyses demonstrating the net benefit associated with the use of the model for predicting PFS. |
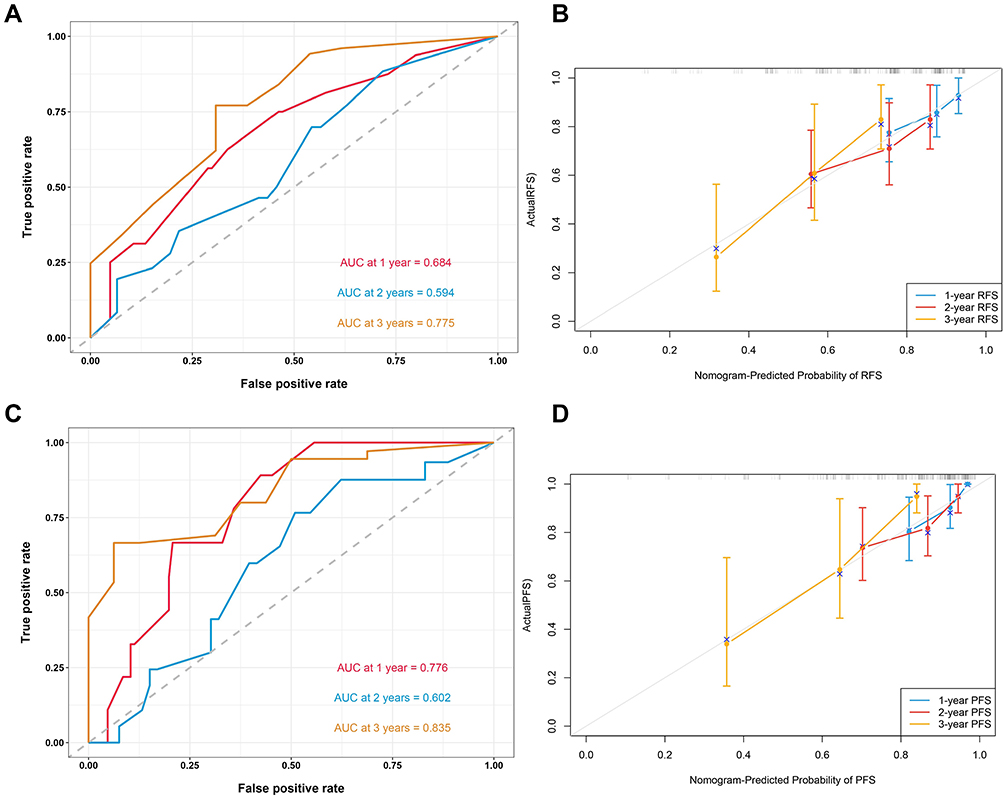 |
Figure 5 (A) Time-dependent ROC curves of the nomogram for predicting RFS in the validation cohort in the validation cohort. (B) Calibration plot of the nomogram by bootstrapping with 1000 resamples for predicting RFS in the validation cohort in the validation cohort. (C) Time-dependent ROC curves of the nomogram for predicting PFS in the validation cohort in the validation cohort. (D) Calibration plot of the nomogram by bootstrapping with 1000 resamples for predicting PFS in the validation cohort in the validation cohort. |
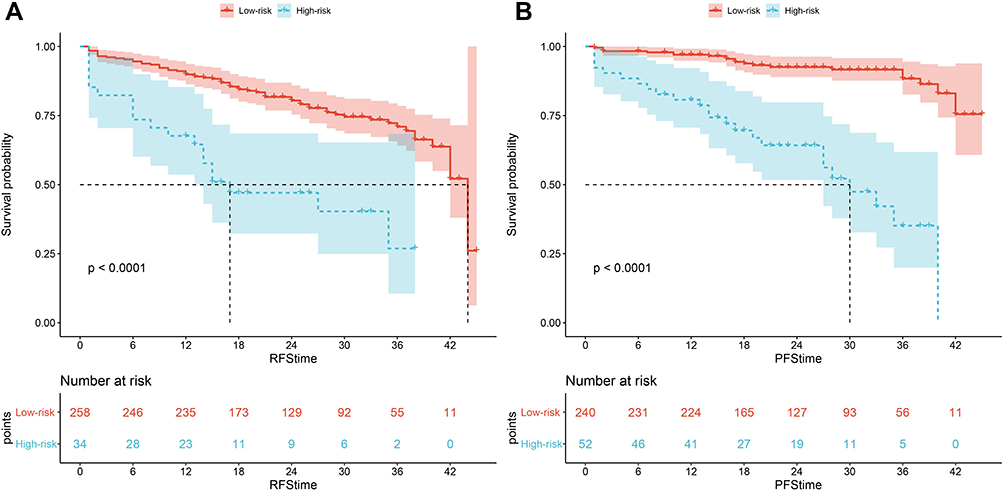 |
Figure 6 The Kaplan-Meier curves of low-risk and high-risk groups based on the prediction of the nomogram models for (A) RFS and (B) PFS. |
Discussion
Our study explored the value of the SIM score in predicting RFS and PFS in NMIBC patients who underwent TURBT. The results showed that the SIM score remained a statistically significant independent predictor even after adjusting for common clinicopathological variables and tumor status data such as BNI. The models based on variables, including the SIM score, had great accuracy and stability. To our knowledge, this is the first predictive models constructed for bladder cancer that includes the SIM score.
Systemic inflammatory response markers have been widely demonstrated to play an important role in assessing the prognosis of patients with a variety of malignancies.18,26–29 NLR, PLR, and LMR are the most well-studied of these factors. In 2018, a review of previous literature by Vartolomei et al In six studies that used multivariate analysis to assess the value of NLR in tumor recurrence and progression in patients with NMIBC, all confirmed that elevated NLR was associated with reduced RFS and PFS.21 A study by Wu et al demonstrated that, for NMIBC patients receiving BCG immunotherapy, the PLR levels before and during induction treatment may serve as indicators of disease progression and recurrence.30 Yıldız et al showed that reduced LMR was an independent risk factor for predicting tumor recurrence in NMIBC patients.22 By inducing cytotoxic cell death and preventing tumor cell growth and metastasis, lymphocytes play a critical role in the host’s ability to fight tumors. A reduction in lymphocytes affects the body’s ability to fight tumors, which raises the chance of cancer development and recurrence.31 While neutrophils emit huge amounts of vascular endothelial growth factor, which speeds up tumor angiogenesis and encourages tumor carcinogenesis and metastasis,16 platelets boost the production of angiogenic factors, which stimulate tumor angiogenesis and protect tumor cells from cytolysis.14 In the tumor microenvironment, monocytes can differentiate into tumor-associated macrophages, which promote tumor infiltration and metastasis. An increase in serum monocyte count can reflect the activity of tumor-associated macrophages.28 Previous studies have shown that the anatomical location of the tumor at the time of the first electrosurgery is closely related to tumor recurrence and progression. This may be related to factors such as the pathological and histological characteristics of the different sites and intraoperative visualization. Intraoperatively, patients with BNI have a greater risk of tumor residuals.32,33 In recent years, the emergence of the field of molecular biomarkers34–36 may have been of further help in predicting treatment response in patients with bladder cancer. Also, liquid biopsy37 has potential as a new technique in the therapeutic evaluation of patients with bladder cancer, factors that have not been fully demonstrated clinically have great value for future research. Despite the attractiveness of these metrics, prospective large studies of these metrics in the clinical setting are difficult due to the high cost of the tests required, especially in countries and regions where genetic testing is not yet widely available. Hematologic markers such as the SIM score, for example, have better utility as essential tests in the perioperative period with the advantages of low price, easy access, and stable values, even if the disadvantage of their lower specificity cannot be ignored.
Based on our study, the SIM score was a strong predictor of survival prognosis in NMIBC patients, with higher scores associated with a poorer prognosis. Although BNI was a significant variable in predicting RFS and PFS in the univariate regression analysis, unfortunately, it was not significant in any of the multivariate analyses. We believe this may be due to the small sample size. Although smoking has been shown to be the most important causal factor in the development of bladder cancer, the relationship between smoking intensity and tumor recurrence and progression remains unclear.38,39 Our study could not confirm that smoking status was associated with recurrence or progression of NMIBC, which may be explained by several reasons: due to social factors, some patients may conceal their smoking history at the time of initial diagnosis or follow-up, while our sample size was still not large enough to influence the results of the study.
There are inevitable limitations to our study. First, there may be some heterogeneity in the samples from the two medical centers. Second, conclusions might have been more reliable if preoperative serological indicators could have been collected the exact day before surgery. Also, although the vast majority of subjects included in the study received adjuvant intravesical instillation and subsequent further intravesical chemotherapy or BCG treatment, we have not included this variable in our analysis. Whereas, as the first study to build predictive models based on the SIM score, our study has some positive implications for the prognostic analysis of NMIBC patients.
Conclusion
We constructed novel models for predicting the survival prognosis of NMIBC patients based on the SIM score and clinicopathological features. Due to the inherent drawbacks of a retrospective design, more prospective studies are needed to confirm this result in the future.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (XYFT2022-KL340-01) and the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (2022-E318-01). The requirement for written informed consent has been accordingly waived due to the retrospective study design. Patient data involved in the study are confidential. Due to ethical restrictions, the raw data underlying this paper are available upon request to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether it was in the conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the second round of Xuzhou Medical Leading Talents Training Project (XWRCHT20210027).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. Ca Cancer J Clin. 2022;72:7–33. doi:10.3322/caac.21708
2. Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage ta t1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49:466–477. doi:10.1016/j.eururo.2005.12.031
3. Fernandez-Gomez J, Madero R, Solsona E, et al. Predicting nonmuscle invasive bladder cancer recurrence and progression in patients treated with bacillus calmette-guerin: the cueto scoring model. J Urol. 2009;182:2195–2203. doi:10.1016/j.juro.2009.07.016
4. Fujii Y. Prediction models for progression of non-muscle-invasive bladder cancer: a review. Int J Urol. 2018;25:212–218. doi:10.1111/iju.13509
5. Bree KK, Shan Y, Hensley PJ, et al. Management, surveillance patterns, and costs associated with low-grade papillary stage ta non–muscle-invasive bladder cancer among older adults, 2004–2013. JAMA Netw Open. 2022;5:e223050. doi:10.1001/jamanetworkopen.2022.3050
6. Koie T, Ohyama C, Hosogoe S, et al. Oncological outcomes of a single but extensive transurethral resection followed by appropriate intra-vesical instillation therapy for newly diagnosed non-muscle-invasive bladder cancer. Int Urol Nephrol. 2015;47:1509–1514. doi:10.1007/s11255-015-1048-3
7. Brausi M, Witjes JA, Lamm D, et al. A review of current guidelines and best practice recommendations for the management of nonmuscle invasive bladder cancer by the international bladder cancer group. J Urol. 2011;186:2158–2167. doi:10.1016/j.juro.2011.07.076
8. Konety B, Isharwal S. Non-muscle invasive bladder cancer risk stratification. Indian J Urol. 2015;31:289. doi:10.4103/0970-1591.166445
9. Kobayashi S, Fujii Y, Koga F, et al. Impact of bladder neck involvement on progression in patients with primary non–muscle invasive bladder cancer: a prospective validation study. Urol Oncol. 2014;32:29–38. doi:10.1016/j.urolonc.2013.04.001
10. Zhan X, Guo J, Chen L, et al. Prognostic significance of bladder neck involvement in non‐muscle‐invasive bladder cancer: a seer database analysis with 19,919 patients. Cancer Med. 2021;10:6868–6880. doi:10.1002/cam4.4219
11. Fukushima H, Moriyama S, Waseda Y, et al. Significance of bladder neck involvement in risk substratification of intermediate-risk non–muscle-invasive bladder cancer. Eur Urol Focus. 2021;7:366–372. doi:10.1016/j.euf.2020.01.006
12. Ye F, Liang Y, Hu J, et al. DNA methylation modification map to predict tumor molecular subtypes and efficacy of immunotherapy in bladder cancer. Front Cell Dev Biol. 2021;9:760369. doi:10.3389/fcell.2021.760369
13. Ye F, Liang Y, Cheng Z, et al. Immunological characteristics of alternative splicing profiles related to prognosis in bladder cancer. Front Immunol. 2022;13:911902. doi:10.3389/fimmu.2022.911902
14. Sierko E, Wojtukiewicz MZ. Platelets and angiogenesis in malignancy. Semin Thromb Hemost. 2004;30:95–108. doi:10.1055/s-2004-822974
15. Sierko E, Wojtukiewicz MZ. Inhibition of platelet function: does it offer a chance of better cancer progression control? Semin Thromb Hemost. 2007;33:712–721. doi:10.1055/s-2007-991540
16. Mollinedo F. Neutrophil degranulation, plasticity, and cancer metastasis. Trends Immunol. 2019;40:228–242. doi:10.1016/j.it.2019.01.006
17. Xiong S, Dong L, Cheng L. Neutrophils in cancer carcinogenesis and metastasis. J Hematol Oncol. 2021;14:173. doi:10.1186/s13045-021-01187-y
18. Ohno Y. Role of systemic inflammatory response markers in urological malignancy. Int J Urol. 2019;26:31–47. doi:10.1111/iju.13801
19. Hu H, Yao X, Xie X, et al. Prognostic value of preoperative nlr, dnlr, plr and crp in surgical renal cell carcinoma patients. World J Urol. 2017;35:261–270. doi:10.1007/s00345-016-1864-9
20. Barua SK, Singh Y, Baruah SJ, et al. Predictors of progression-free survival and overall survival in metastatic non-clear cell renal cell carcinoma: a single-center experience. World J Oncol. 2019;10:101–111. doi:10.14740/wjon1188
21. Vartolomei MD, Porav-Hodade D, Ferro M, et al. Prognostic role of pretreatment neutrophil-to-lymphocyte ratio (nlr) in patients with non–muscle-invasive bladder cancer (nmibc): a systematic review and meta-analysis. Urol Oncol. 2018;36:389–399. doi:10.1016/j.urolonc.2018.05.014
22. Yıldız HA, Değer MD, Aslan G. Prognostic value of preoperative inflammation markers in non‐muscle invasive bladder cancer. Int J Clin Pract. 2021;75:e14118. doi:10.1111/ijcp.14118
23. Mano R, Baniel J, Shoshany O, et al. Neutrophil-to-lymphocyte ratio predicts progression and recurrence of non–muscle-invasive bladder cancer. Urol Oncol. 2015;33:61–67. doi:10.1016/j.urolonc.2014.06.010
24. Mbeutcha A, Shariat SF, Rieken M, et al. Prognostic significance of markers of systemic inflammatory response in patients with non–muscle-invasive bladder cancer. Urol Oncol. 2016;34:417–483. doi:10.1016/j.urolonc.2016.05.013
25. Cantiello F, Russo GI, Vartolomei MD, et al. Systemic inflammatory markers and oncologic outcomes in patients with high-risk non–muscle-invasive urothelial bladder cancer. Eur Urol Oncol. 2018;1:403–410. doi:10.1016/j.euo.2018.06.006
26. Pikuła A, Skórzewska M, Pelc Z, et al. Prognostic value of systemic inflammatory response markers in patients undergoing neoadjuvant chemotherapy and gastrectomy for advanced gastric cancer in the Eastern European population. Cancers. 2022;14:1997. doi:10.3390/cancers14081997
27. Savioli F, Morrow ES, Dolan RD, et al. Prognostic role of preoperative circulating systemic inflammatory response markers in primary breast cancer: meta-analysis. Br J Surg. 2022;109:1206–1215. doi:10.1093/bjs/znac319
28. Yamamoto T, Kawada K, Obama K. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int J Mol Sci. 2021;22:8002. doi:10.3390/ijms22158002
29. Zou Y, Xie J, Zheng S, et al. Leveraging diverse cell-death patterns to predict the prognosis and drug sensitivity of triple-negative breast cancer patients after surgery. Int J Surg. 2022;107:106936. doi:10.1016/j.ijsu.2022.106936
30. Wu R, Li D, Zhang F, Bai Y, Wang X, Han P. Prognostic value of platelet-to-lymphocyte ratio in non-muscle invasive bladder cancer patients: intravesical bacillus calmette-guerin treatment after transurethral resection of bladder tumor. Front Surg. 2022;9:907485. doi:10.3389/fsurg.2022.907485
31. Pfeffer C, Singh A. Apoptosis: a target for anticancer therapy. Int J Mol Sci. 2018;19:448. doi:10.3390/ijms19020448
32. Waseda Y, Inoue M, Ito M, et al. Mp15-04 new predictive scoring model for recurrence incorporating bladder neck involvement in patients with non-muscle-invasive bladder cancer. J Urol. 2017;197:e172. doi:10.1016/j.juro.2017.02.489
33. Fujii Y, Fukui I, Kihara K, et al. Significance of bladder neck involvement on progression in superficial bladder cancer. Eur Urol. 1998;33:464–468. doi:10.1159/000019636
34. van Rhijn BWG, Zuiverloon TCM, Vis AN, et al. Molecular grade (fgfr3/mib-1) and EORTC risk scores are predictive in primary non–muscle-invasive bladder cancer. Eur Urol. 2010;58:433–441. doi:10.1016/j.eururo.2010.05.043
35. Claps F, Mir MC, Zargar H. Molecular markers of systemic therapy response in urothelial carcinoma. Asian J Urol. 2021;8:376–390. doi:10.1016/j.ajur.2021.05.001
36. Mertens LS, Claps F, Mayr R, et al. Prognostic markers in invasive bladder cancer: fgfr3 mutation status versus p53 and ki-67 expression: a multi-center, multi-laboratory analysis in 1058 radical cystectomy patients. Urol Oncol. 2022;40:110–111. doi:10.1016/j.urolonc.2021.10.010
37. de Kruijff IE, Beije N, Martens J, de Wit R, Boormans JL, Sleijfer S. Liquid biopsies to select patients for perioperative chemotherapy in muscle-invasive bladder cancer: a systematic review. Eur Urol Oncol. 2021;4:204–214. doi:10.1016/j.euo.2020.01.003
38. van Osch FH, Jochems SH, van Schooten F, Bryan RT, Zeegers MP. Quantified relations between exposure to tobacco smoking and bladder cancer risk: a meta-analysis of 89 observational studies. Int J Epidemiol. 2016;45:857–870. doi:10.1093/ije/dyw044
39. Freedman ND. Association between smoking and risk of bladder cancer among men and women. JAMA. 2011;306:737. doi:10.1001/jama.2011.1142
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Instillation Strategies for Non-Muscle-Invasive Bladder Cancer in the Bacillus Calmette-Guerin Shortage Era: A Simple Solution for BCG Discontinuation
Lin PT, Hsieh ML, Su SH, Chang YH, Huang LK, Chu YC, Kan HC, Lin PH, Yu KJ, Chuang CK, Wu CT, Pang ST, Shao IH
Cancer Management and Research 2022, 14:3121-3130
Published Date: 4 November 2022
Development and External Validation of Nomogram to Identify Risk Factors for CHD in T2DM in the Population of Northwestern China
Meng Q, Yang J, Wang F, Li C, Sang G, Liu H, Shen D, Zhang J, Jiang S, Yusufu A, Du G
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1271-1282
Published Date: 4 May 2023
Establishment and Validation of a Nomogram Prediction Model for the Severe Acute Pancreatitis
Li B, Wu W, Liu A, Feng L, Li B, Mei Y, Tan L, Zhang C, Tian Y
Journal of Inflammation Research 2023, 16:2831-2843
Published Date: 8 July 2023
An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction
Chen Y, Xie K, Han Y, Xu Q, Zhao X
Journal of Inflammation Research 2023, 16:4061-4071
Published Date: 13 September 2023
Prognostic Value of Body Composition and Systemic Inflammatory Markers in Patients with Locally Advanced Cervical Cancer Following Chemoradiotherapy
Guo H, Feng S, Li Z, Yin Y, Lin X, Yuan L, Sheng X, Li D
Journal of Inflammation Research 2023, 16:5145-5156
Published Date: 10 November 2023