Back to Journals » Lung Cancer: Targets and Therapy » Volume 14
Clinical Utility and Application of Liquid Biopsy Genotyping in Lung Cancer: A Comprehensive Review
Authors Nigro MC, Marchese PV ![]() , Deiana C, Casadio C
, Deiana C, Casadio C ![]() , Galvani L, Di Federico A, De Giglio A
, Galvani L, Di Federico A, De Giglio A
Received 30 August 2022
Accepted for publication 26 January 2023
Published 3 February 2023 Volume 2023:14 Pages 11—25
DOI https://doi.org/10.2147/LCTT.S388047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sai-Hong Ou
Maria Concetta Nigro,1 Paola Valeria Marchese,1 Chiara Deiana,1 Chiara Casadio,1 Linda Galvani,1 Alessandro Di Federico,1 Andrea De Giglio1,2
1Department of Experimental, Diagnostic and Specialty Medicine, S.Orsola-Malpighi University Hospital, University of Bologna, Bologna, 40138, Italy; 2Medical Oncology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, 40138, Italy
Correspondence: Paola Valeria Marchese, Department of Experimental, Diagnostic and Specialty Medicine, S.Orsola-Malpighi University Hospital, University of Bologna, Via Albertoni 15, Bologna, 40138, Italy, Email [email protected]
Abstract: Precision medicine has revolutionized the therapeutic management of cancer patients with a major impact on non-small cell lung cancer (NSCLC), particularly lung adenocarcinoma, where advances have been remarkable. Tissue biopsy, required for tumor molecular testing, has significant limitations due to the difficulty of the biopsy site or the inadequacy of the histological specimen. In this context, liquid biopsy, consisting of the analysis of tumor-released materials circulating in body fluids, such as blood, is increasingly emerging as a valuable and non-invasive biomarker for detecting circulating tumor DNA (ctDNA) carrying molecular tumor signatures. In advanced/metastatic NSCLC, liquid biopsy drives target therapy by monitoring response to treatment and identifying eventual genomic mechanisms of resistance. In addition, recent data have shown a significant ability to detect minimal residual disease in early-stage lung cancer, underlying the potential application of liquid biopsy in the adjuvant setting, in early detection of recurrence, and also in the screening field. In this article, we present a review of the currently available data about the utility and application of liquid biopsy in lung cancer, with a particular focus on the approach to different techniques of analysis for liquid biopsy and a comparison with tissue samples as well as the potential practical uses in early and advanced/metastatic NSCLC.
Keywords: circulating tumor DNA, liquid biopsy, EGFR, minimal residual disease, sequencing technologies, lung cancer, early-stage, non-small cell lung cancer
Introduction/Background
During the last decade, several tumor molecular alterations have been identified as drivers of cancer proliferation and survival, leading to the development of novel specific targeted agents for different tumors, including lung cancer.1,2 Concerning non-small cell lung cancer (NSCLC), the advent of targeted therapy with tyrosine kinase inhibitors (TKIs) improved the overall patient outcomes with a better tolerability and safety profile when compared to platinum-based chemotherapy. Predominant targetable alterations in nonsquamous NSCLC are Epidermal growth factor receptor (EGFR), occurring in about 10–15% of Caucasian patients and up to 40% in Asian population, and Kirsten rat sarcoma virus (KRAS)-mutations, present in 20–30% of patients, followed by Anaplastic lymphoma kinase (ALK) translocations (3–7%), v-raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations (2–4%), c-mesenchymal-epithelial transition factor (MET) amplifications and exon 14 skipping mutations (2–4%), and c-ros oncogene 1 (ROS1) (1–2%), rearranged during transfection (ret proto-oncogene or RET) (1–2%) and Neurotrophic tyrosine receptor kinase (NRTK) fusions (0,5–1%).3–11
However, many patients present a non-oncogene-addicted disease without any of the above-mentioned driver alterations.3 Thus, the proportion of nonsquamous NSCLC patients presenting a non-oncogene addicted disease is progressively decreasing.12 Conversely, the rate of actionable driver mutations among squamous NSCLC is very low, and international guidelines do not recommend comprehensive molecular testing.
The expanding access to various molecular diagnostic strategies, such as next-generation sequencing (NGS) technique, immunohistochemistry and polymerase chain reaction method (PCR), allowed the routine use of molecular tumor assessment to determine the status of the most relevant molecular targets in NSCLC patients.13,14 In fact, since 2018 and with the recent update of 2021, the International Society for the Study of Lung Cancer (IASLC) and the European Society of Medical Oncology (ESMO) recommended the adoption of NGS for the molecular assessment of patients with advanced NSCLC.15
Nowadays, tumor tissue still represents the standard biological sample for molecular analysis. However, this approach has significant limitations due to the potentially difficult technical accessibility of particular sites of disease or the inadequacy of the histological sample for molecular testing, sometimes requiring a new biopsy.16 To overcome these issues, liquid biopsy has gained increasing attention and currently represents an important alternative source to detect tumor genomic alterations.
Liquid biopsy is a minimally invasive procedure that provides the opportunity to detect, analyze and monitor cancer in various body fluids (such as blood, urine, malignant pleural effusion and ascites) and also permits dynamic and real-time monitoring of cancer molecular alterations.16 In fact, metabolic and homeostatic mechanisms, along with micro-environmental factors and drug selection pressures, may all influence and change the molecular features of cancer cells, an important phenomenon that physicians need to detect.14
Although this method has a good specificity in detecting mutations in circulating tumor DNA (ctDNA) (90–100%), the sensitivity levels achieved with the current methodologies are low (60–70%).17,18 The ctDNA is significantly diluted in the circulation by the abundance of background cell-free DNA (cfDNA) released by non-tumoral cells.19 Furthermore, circulating cells, extracellular vesicles, messenger RNA (mRNA), micro RNA (miRNA), proteins, and cell-free DNA (cfDNA) can also be detected in the bloodstream20 (Figure 1).
 |
Figure 1 Comparison between tissue and liquid biopsy: advantages and limitations. Abbreviations: ctDNA, circulating tumor DNA; cfDNA, cell-free DNA; mRNA, messenger RNA; miRNA, micro RNA. |
The term liquid biopsy can be referred to different laboratory techniques that analyze tumor-derived circulating nucleic acids (like ctDNA), tumor-derived fractions of cfDNA in the plasma, mRNA, non-coding RNA such as micro-RNA or long non-coding RNA, tumor-educated platelets (TEP), circulating tumor cells (CTCs), exosomes or proteins, and metabolites.14 Tumor mutations in ctDNA can be detected using NGS techniques. Thus, ctDNA analysis could be employed as a complementary tool that can provide additional information regarding tumor genotyping associated with tumor tissue biopsy for NSCLC.
Given these concepts, liquid biopsy may represent a less invasive and more feasible alternative to tissue biopsy in many cancer settings, from a promising detection method for minimal residual disease (MRD) and recurrence in patients with resected disease, to a dynamic assessment of tumor mutability in advanced disease.20 This review analyzes the clinical utility and application of liquid biopsy genotyping in NSCLC.
Applications of Liquid Biopsy
When dealing with a NSCLC formalin-fixed paraffin-embedded (FFPE) sample, evaluation of PD-L1 expression through immunohistochemistry (IHC) and analysis of molecular alterations in an increasing number of genes are all needed to define appropriate treatment. Tissue genotyping can be performed with FISH or IHC, multiple PCR hot spot single-gene assays, or wide NGS panels, depending on the costs and availability.21
Notwithstanding the cases where biopsy is not feasible due to patient conditions or technical difficulties, even when the tumor tissue is available, sometimes the required analyses are not always successful due to the low quality or scant quantity of available tissue.22
The NILE trial23 showed that, out of 282 patients with treatment-naïve advanced NSCLC, as few as 18% of patients had complete tissue analysis of all the biomarkers of interest at the time of the trial (EGFR mutations, ALK fusions, ROS1 fusions, BRAFV600 mutations, RET fusions, MET amplification, MET exon 14 skipping variants, ERBB2 mutations), while 68.1% had a partial analysis. On the other hand, liquid biopsy with NGS analysis of all recommended genes was successfully performed on 95% of patients, with a sensitivity of 80% for detection of recommended biomarkers and a positive predictive value of 100%. Furthermore, turnaround time (TAT) was shorter with liquid biopsy compared with tissue genotyping (9 vs 15 days). The NILE trial is a prime example of how liquid biopsy can bypass the problem of insufficient FFPE tissue and offers quicker turnaround times.
The idea of liquid biopsy actually encompasses several techniques with different analyzed bioproducts. It can be used to analyze circulating tumor cells, circulating free RNA or exosomes, but these techniques are yet too unreliable for clinical use24. Most commonly, liquid biopsy refers to the search for cfDNA and in particular one of its components, ctDNA, defined as the DNA released from cancer cells into biofluids.25
Once the cfDNA has been obtained, real-time PCR-based arrays, like allele-specific polymerase chain reaction (ASPCR) for EGFR, digital PCR techniques (such as BEAMing or droplet digital PCR), or multigene NGS-based arrays can be used to analyze the genome.26 The main limitation of PCR-based techniques is that only a finite number of mutations is detectable. For instance, the Cobas® EGFR mutation test v2 can detect only 42 alterations in exons 18–21, despite a sensitivity of 72.1% and specificity of 97.9%.27 This drawback also applies to digital PCR though with relatively higher sensitivity (70–85%).28
Other than qualitative information, liquid biopsy can also give quantitative data in the form of mutant allele fraction (MAF), meaning the percentage of mutant alleles in a specified locus, which helps track the tumor clonal evolution over time.29 ctDNA can be detected in plasma even if present at low levels: the detection limits of modern kits are as low as an allelic fraction of 0.1% or lower, with a median allelic fraction of 0.5%.30,31
Overall, high specificity and high positive-predicted value are core features of ctDNA, meaning that the detection of targetable genomic alterations, even in low allelic fractions, can be clinically relevant.32 This has been proven with single-gene PCR (specificity of PCR-based EGFR tests was close to 98%27,33) and NGS assay (specificity of 97%34) when dealing with targetable variants.
The detection of non-targetable mutations has a more nebulous interpretation, and their origin from tumor DNA is not always certain. Particularly, JAK2 alterations are usually imputable to white blood cells’ DNA, a phenomenon known as clonal hematopoiesis, and this can also apply to TP53 and KRAS mutations.35
On the other hand, false negatives can be more frequent as the sensitivity of ctDNA can be affected by a variable amount of DNA shedding and tumor heterogeneity. Studies report detection rates of around 70–80% for both PCR-based and NGS-based arrays.34,36
A recent study showed that detection rates and concordance percentages between liquid biopsy and tissue samples vary widely, ranging from as low as 14.3% in stage I to as high as 85% in stage IV disease.37 Overall, better results were obtained with more advanced disease stages, higher tumor burden, and in treatment naïve patients or progressing on therapy.37
Overall, several techniques such as real-time PCR, digital PCR or multigene NGS-panel can be applied to liquid biopsy samples, with high specificity results and a wide range of sensitivity rates, depending on the sample, patients’ clinical characteristics, and tumor features.
Early-Stage NSCLC
Patients with early-stage (I, II and resectable III) NSCLC are amenable to radical surgery, followed or not by adjuvant therapy on the basis of primary tumor TNM staging and EGFR mutational status.38–40 Despite the curative intent, 5-years overall survival after radical surgery was about 32%.41 In fact, 30% to 70% of patients show local or distant disease recurrence,38 which might be attributable to the persistence after surgery of MRD. Therefore, the early identification of individuals at high risk of recurrence is crucial to provide them with appropriate treatment. Likewise, detecting viable cancer cells before they spread to distant sites is a primary goal of cancer research. Various studies analyzed the presence of peripheral blood ctDNA in patients affected by early-stage lung cancer before and after surgical treatment, reporting a rapid decrease in ctDNA levels after surgery.42,43 In addition, several analyses showed discrepancies in mutation frequency between tumor-DNA (tDNA), the genetic signature detected on tumor mass analysis, and matched ctDNA detected in patient’s blood, depending on tumor stage, with a more significant mismatch in stage I–IIA.43,44 This discordance may be correlated with the wide intra-tumor heterogeneity, although it would be expected to be more represented in advanced lung cancer than in early lung cancer due to the persistent interaction between tumor cells and the other cells comprised in the tumor microenvironment.45
Detecting ctDNA after surgical resection may guide physicians in identifying patients at higher risk of recurrence and who may benefit from adjuvant therapy. On the contrary, patients with no detection of ctDNA may be initiated to clinical-instrumental monitoring only. A limitation of this approach is that ctDNA is often lacking or present in a meager amount in early-stage disease. To overcome this limitation, more sensitive tests have been developed to detect and quantify extremely low levels of plasma ctDNA.
The CAncer Personalized Profiling by deep Sequencing (CAPP-Seq) is a highly sensitive and specific platform that uses a “selector”, composed of biotinylated DNA oligonucleotides, that is applied first to tDNA to detect specific genetic alterations, then to ctDNA to quantify them.44 From the analysis of Chaudhuri et al,46 this type of test has proven to be highly effective in identifying MRD after treatment of localized tumors, and it has been able to quantify ctDNA also in stage I lung cancer. According to the paper, about 94% of patients enrolled in this trial who subsequently relapsed had detectable ctDNA in their post-treatment blood specimen, making the test a reliable predictor of relapse. In addition, during analysis, the EGFRL858R mutation was identified at the MRD landmark, underlining how ctDNA analysis after radical treatment can help to choose tailored therapies before clinically or radiologically documented disease recurrence.46 For example, an 81-year-old patient, enrolled on trial and underwent stereotactic ablative radiotherapy (SABR) for localized lung disease, died for symptomatic brain metastases and concurrently adrenal metastasis 3 months later. In this case, early treatment with an EGFR TKI should have been considered before the development of symptoms in view of detection of EGFRL858R mutation at the MRD landmark.46
The “Tracking Non-Small-Cell Lung Cancer Evolution Through Therapy (Rx)” (TRACERx) study analyzed the detection of plasma cfDNA of 100 stage IA-IIIA NSCLC patients before and at different time points after surgical treatment to comprehend the clonal evolution of cancer cells from the time of diagnosis to patient’s death.47,48 The investigators devised sequencing assays tailored for each patient, starting with multi-region sequencing of the individual tumor exome, targeting both clonal and sub-clonal single nucleotide variants (SNVs). The study found that necrosis, lymphovascular invasion, Ki67 index, and non-adenocarcinoma pattern predict ctDNA shed, in addition to already recognized factors, such as tumor size, stage of disease, and sites of metastasis. cfDNA was identified only in 48% of early-stage patients, and based on a rough estimate, tumors <10 cm3 of volume have no detectable ctDNA.47,49,50 Strengths of the TRACERx trial are the variety of tumor staging included, such as a large cohort of stage I NSCLC characterized by a minimal tumor burden and the analysis interval of ctDNA (that could have been performed sometimes during adjuvant treatment). In some cases, the evidence of MRD allowed for changing the type of adjuvant therapy based on ctDNA changes. On the contrary, a limitation of the TRACERx study48 and the CAPP-Seq46 was the poor number of certified relapses.
Cancer SEEK is another blood test, based on PCR, able to synchronously evaluate several regions of driver genes typically mutated in different types of cancer (lung, breast, ovary, pancreas, liver, esophagus, stomach and colorectal), detecting early-stage tumors and localizing the primary tissue.51 The use of multiplex-PCR allowed each original model molecule to be directly and uniquely labeled with a DNA barcode. This approach minimizes the intrinsic biases of massively parallel sequencing and makes optimal use of the small pool of cfDNA. In addition, the total volume of plasmatic DNA was divided into several portions on which independent assays were performed. By doing so, the number of DNA molecules per sample is reduced, but the fraction of each mutant species is increased, making mutations easier to be detected. In this method, PCR assay is combined with eight specific protein biomarkers that can detect various types of cancer early, with a sensitivity >69% and specificity >99%. The study results showed 90% concordance in mutation detection between plasma and primary tumors, ranging from 100% in ovarian and pancreatic cancers to 82% in gastric cancers.51 However, although this approach detected about 70% of the total cancers tested faithfully, its sensitivity for stage-I tumors was relatively low (43%). In particular, lung cancer and esophageal cancer showed the lowest detection rates. Furthermore, because there is no specific circulating protein marker for lung cancer, site determination was possible in only 39% of cases, compared with 84% for colorectal cancer, 79% for ovarian cancers, and 81% for pancreatic cancers.52 In the screening setting, a next-generation plasma sequencing by using wider panel will be able to help in early tumor diagnosis, considering its good sensitivity, that could be impaired by low tumor spread, and its high specificity, which might be greater in a sample of healthy people such as in a real screening scenario.52
The analysis of ctDNA mediated by the above-mentioned tests may also represent a non-invasive approach for the early diagnosis of NSCLC. Compared with conventional unspecific and insensitive serum tumor markers, occasionally used for early diagnosis of various types of cancer, and similarly unspecific computed tomography (CT) scan,53–55 ctDNA was found to be more sensitive and specific to reveal an early-stage tumor. From the study by Chen et al, no patients with benign lesions had detectable ctDNA in their blood, suggesting that, in the case of positive ctDNA, a suspected lesion should be considered likely malignant, requiring a more intensive diagnostic approach.43 Concerning this concept, the TEC-Seq assay, known as “Targeted Error-Corrected Sequencing”, analyzed, in an ultra-sensitive manner, sequence changes in tumor genes commonly mutated in cfDNA, without first knowing the alterations in the tumor, re-reading each DNA code at least 30,000 times.56,57 By comparing sequence alterations of genes responsible for cell proliferation in healthy individuals with the cancer-specific alterations in the plasma of patients affected by tumors, the authors highlighted both the potential utilities and limits of large-scale testing of ctDNA modifications for the non-invasive detection of early-stage cancers. The main issue is that the detection rate of circulating tumor cells and ctDNA is typically low (<30%). In addition, any inflammatory disorder may release circulating epithelial cells, twisting the findings.58,59
Ilie et al60 selected five chronic obstructive pulmonary disease patients with CTCs identified by an innovative isolation technique by the size of epithelial tumor cells, named ISET, monitoring them with CT scans. All of them subsequently developed lung cancer, diagnosed at an early stage. In contrast, none of the other patients who did not have CTCs at the test developed the tumor. Based on this concept, an earlier analysis of prospective, non-randomized, multicenter AIR study suggested that detection of CTCs in peripheral blood with ISET technique could be used as a screening test for early diagnosis of lung cancer.61 Later, Marquette et al62 revealed that this method is not suitable for cancer screening, showing a CTC detection sensitivity for lung cancer of only 26%.
In summary, although testing ctDNA and CTCs in the blood of high-risk patients can detect lung cancer early, there is no sufficient evidence of its use as a screening method in clinical practice. On the other hand, ctDNA profiling may help identify patients who underwent curative surgery for lung cancer and are less likely to benefit from adjuvant chemotherapy. Vice versa, longitudinal ctDNA analysis may allow the identification of those patients who show increased ctDNA levels during adjuvant chemotherapy and thus may need more careful evaluation. In the future, the use of this new biomarker will depend on novel prospective clinical trials that investigate its clinical benefit as well as its possible integration with diagnostic imaging for earlier detection of disease recurrence.
Advanced/Metastatic Disease – Non-Oncogene Addicted
The liquid biopsy has no well-defined indications in patients with advanced non-oncogene addicted NSCLC. Promising areas of investigation include identifying patients who could benefit the most from immunotherapy, collecting the dynamic genomic heterogeneity and laying a tumor molecular profile during the disease course.63
The advent of immunotherapy has revolutionized the natural history of patients with non-oncogene addicted NSCLC. Identifying predictive biomarkers for anti-PD-1/PD-L1 therapies in NSCLC is crucial for selecting patients who will benefit from immunotherapy while limiting ineffective treatment and their related toxicities.63,64 The only validated biomarker is PD-L1 expression by immunohistochemistry on tumor tissue.65 However, tumor PD-L1 expression is not completely reliable, as improved survival outcomes have also been assessed in negative or low PD-L1 expression, even if the 50% of tumor proportion score represents the best threshold for upfront single-agent PD-(L)1 inhibitor efficacy as demonstrated by several prospective trials.66 Tumor mutational burden (TMB) is defined as the total number of somatic, non-synonymous mutations in the tumor genome. It is garnering a lot of attention, and several studies have reported the evaluation of TMB in blood (bTMB) as this may be estimated from cfDNA NGS.67 It has been suggested that highly mutated tumors tend to produce neoantigens, which can be targeted by activated immune cells. In many tumor types, TMB has been shown to correlate with patient response to both CTLA-4 and PD-(L)1 inhibition.68,69 It seems that TMB and PD-L1 show only a slight overlap in NSCLC, suggesting that these assays measure various aspects of the immune phenotype.70
A meta-analysis performed by Yu et al71 in 14,395 patients demonstrated that the combined use of PD-L1 expression and TMB are promising biomarkers to assess patient survival and response to immunotherapy. Moreover, the matched evaluation of CD8+ tumor-infiltrating lymphocytes, PD-L1, and TMB expression had prognostic relevance, although the predictive value of this assessment needs to be validated in further prospective studies.61 The study by Gandara et al67 optimized a gene panel and an algorithm for bTMB, demonstrating the possibility of using cfDNA to determine TMB and showing its predictive value for NSCLC patients treated with immunotherapy. Likewise, Phase 2 POPLAR and Phase 3 OAK studies revealed that high bTMB was associated with improved response rate and PFS from atezolizumab in single-agent regimen.67,72 In the prospective proof-of-principle B-F1RST (NCT02848651) trial, bTMB (cutoff greater than or equal to 16 mut/Mb), assessed with the FoundationOne Liquid CDx assay, was evaluated as a predictive biomarker of response to first-line atezolizumab in PD-L1-unselected patients with advanced NSCLC.73 A bTMB greater than or equal to 16 mut/Mb was correlated with increased ORR. The Phase 3 Blood-First Assay Screening Trial (NCT03178552) is randomly evaluating bTMB greater than or equal to 16 mut/Mb. Instead, Rizvi et al74 in the phase 3 MYSTIC study compared durvalumab with or without tremelimumab with platinum-based chemotherapy using the Guardant OMNI 500-gene panel to assess bTMB. They demonstrated that a bTMB greater than or equal to 20 mut/Mb in the double checkpoint inhibition arm is associated with improved overall survival, PFS and ORR compared to chemotherapy. In addition, less clinical benefit was shown with durvalumab alone versus chemotherapy.74 In conclusion, the techniques used for the analysis and interpretation of TMB widely vary, and even if high TMB was linked to greater efficacy of immunotherapy, several limitations and conflicting results in different studies have slowed down its translation into clinical practice.63
cfDNA analysis is also emerging as a new plasma biomarker to evaluate disease activity and treatment-related changes, especially as a predictive marker of immunotherapy response.75,76 Composed of double-stranded fragments of 150–200 base pairs, cfDNA derives from normal physiological tissue remodeling events,77 although it may result from necrosis and apoptosis of cancer cells. cfDNA has a short half-life of about 2 hours, allowing a dynamic assessment of tumor-related changes and providing real-time monitoring of response or recurrence.63 In a proof-of-concept study, variations in cfDNA concentration were pointed out as a suitable tool to assess tumor response in patients treated with PD-1 inhibitors.78 The percentage of ctDNA on total cfDNA in cancer patients varies dramatically, ranging from less than 0.1% to more than 90%.77,79,80 ctDNA is isolated uniquely through specific somatic genomic alterations and tends to be more fragmented, with sizes ranging from 90 to 150 base pairs.53 ctDNA changes may appear earlier than radiographic ones, enabling a prompt evaluation of response to treatments.1,81 In addition, several studies have shown that early changes in ctDNA levels during immunotherapy correlated with radiological response and could identify patients who will achieve long-lasting benefits.78–82 Therefore, cfDNA and ctDNA levels may be early markers of efficacy in patients treated with immune checkpoint inhibitors (ICIs).
CTCs are released into the bloodstream from the primary tumor and are characterized by a very short half-life (1–2.4 h).63 The percentage of CTCs in the blood is very low, about 1 CTC for every 106–107 leukocytes.63 Initially, CTCs have an epithelial phenotype that is unlikely to migrate into the bloodstream. Nevertheless, they can undergo epithelial-to-mesenchymal transition (EMT), enhancing plasticity and ability to migrate, invade, and disseminate.63 Some authors found an association between a high number of baseline CTCs and poor overall survival, with an increased risk of death and progression.83 This concept may also be an indicator of the aggressiveness of these CTCs, which may show features of the mesenchymal phenotype (via EMT).84
Moreover, the joint analysis of cfDNA with CTCs helped to discriminate against a low-risk population that might benefit from continuing nivolumab beyond progression. This analysis suggests that the combined evaluation of cfDNA and CTCs could help to select those patients who will benefit most from immunotherapy.63
Advanced/Metastatic Disease – Oncogene Addicted
Nowadays, ctDNA analysis in advanced or metastatic NSCLC has been extensively validated for the assessment of EGFR mutational status when tissue is insufficient for tumor genotyping of treatment-naïve patients, for the detection of T790M resistance mutation, and the monitoring of EGFR sensitive mutations during TKI treatment.85,86
Despite the limitations (non-DNA biomarkers not evaluable, increased costs if used concurrently with tissue testing and false negatives), there is solid evidence to support the use of plasma ctDNA in clinical practice in genotyping multiple other targetable oncogenic drivers through a broad-based platform, such as NGS.23,87,88 Liquid biopsy could be used in newly diagnosed tumors with tumor tissue available for initial genotyping when the tissue sample results are inadequate, or it could be performed simultaneously with tissue analysis to increase the identification rates of relevant targeted oncogenic drivers.23 In fact, the study by Leighl et al23 suggests that initial biomarker evaluation using cfDNA improves biomarker discovery rate and number of newly diagnosed mNSCLC patients receiving guideline-complete biomarker testing. Although this approach represents the more expensive alternative, the simultaneous modality appears to be the most effective option in the case of small tumor biopsies with uncertain adequacy.32 Furthermore, liquid biopsy performed prior to tissue sampling, according to the “plasma first” modality, should represent the standard of care for patients with oncogene-addicted NSCLC progressing after targeted therapy.1
EGFR Mutations
NGS analysis of ctDNA can detect both on-target (secondary mutations or amplification of the target gene) and off-target (“bypass trace”) acquired molecular resistance mechanisms, suggesting tailored treatment at the time of disease progression to targeted agents.
In the FLAURA study,89 ctDNA analysis was performed at the time of disease progression in both study arms (osimertinib vs investigator choice of gefitinib or erlotinib). Several studies have analyzed the agreement between the assessed mutational status in plasma and tumor tissue samples, showing a robust correlation28,90–97 (Table 1). Recently published meta-analyses (Table 2) have a sensitivity for the detection of EGFR mutations ranging from 60% to 70% and a specificity of 80–98%.98–103 However, given the different technologies included, the sensitivity values are very variable. These data suggest the need to standardize procedures through validation of techniques for large-scale implementation. Recent sequencing technologies, such as digital PCR or plasma digital droplet PCR (ddPCR), use probes that allow the detection of del19 and L858R with very high sensitivity rates (greater than 80%) and 100% specificity.96,97 The most common resistance mutation in patients who did not receive osimertinib upfront was the occurrence of EGFR exon 20 p.T790M mutation (47%). Instead, no cases of acquired EGFR exon 20 p.T790M mutation were documented at the time of disease progression among patients who received osimertinib as first-line therapy. The most commonly detected molecular resistance mechanisms in this arm were secondary EGFR mutations, such as exon 20 p.C797X and MET amplification.89 Recent studies suggested that acquired resistance through MET amplification during the treatment with osimertinib could be overcome by combining a MET inhibitor with the third-generation EGFR-TKI.104,105
 |
Table 1 ctDNA plasma detection of EGFR mutation |
 |
Table 2 Meta‐analysis on the diagnostic accuracy of liquid biopsy for detecting EGFR mutations |
The FLAURA trial also evaluated the prognostic impact of detectable EGFR mutations on ctDNA at baseline, and the persistence versus the clearance of mutant EGFR ctDNA levels during the targeted therapy. Progression-free survival (PFS) was significantly longer in patients without detectable EGFR mutations at baseline in both treatment arms than in patients with detectable baseline EGFR mutations on ctDNA.89 Moreover, the reduction of detectable EGFR mutant ctDNA following TKI administration correlated with longer median PFS and OS.105,106
ALK Rearrangements
Detection of an ALK rearrangement can be achieved in a tissue sample by fluorescent in situ hybridization (FISH), immunohistochemistry (IHC), reverse transcription polymerase chain reaction (RT-PCR) or integrated into a multiplex assay using NGS.107 Regarding the use of liquid biopsy for ALK fusion detection, the results are promising, although the sensitivity is not as high as for EGFR. A PCR-based target sequencing showed low sensitivity, 50% with 100% specificity.108 Other several recent investigations suggest a potential use of liquid biopsy in the management of ALK-positive NSCLC.109,110 Two studies demonstrated that the Guardant360 test reliably detects ALK fusions and kinase domain mutations in patients with TKI-resistant ALK disease.110,111 On the other hand, many studies evaluated the evolution of resistance to ALK-directed TKIs during treatments. Dagogo-Jack et al112 demonstrated that ALK resistance mutations increase with each successive generation of ALK-directed TKI and can be effectively detected by liquid biopsy. Considering the increasing number of available ALK-directed therapies and the possibility of sequentially administering them, defining the role of liquid biopsy in the dynamic management of these patients is gaining importance.
ROS1 Rearrangements
ROS1 rearrangements are commonly detected by fluorescent in situ hybridization (FISH) or NGS.113 Due to incomplete ROS1 intron coverage, DNA-based NGS panels are more prone to false negatives than RNA-based ones.114 Detecting rearrangements in plasma via liquid biopsy is more complex than identifying short variants such as point mutations and insertions/deletions.44 Few studies evaluated the feasibility of plasma genotyping in ROS1-positive NSCLC.44,115 In a study of Dagogo-Jack et al,116 a plasma molecular analysis of patients with ROS1-positive NSCLC was performed. The results obtained from the plasma analysis were compared with those obtained from the investigation conducted on the tissue, to evaluate the potential role of fluid biopsies in managing this subgroup of NSCLC. The results showed that NGS-based plasma genotyping is reliable for identifying ROS1 fusions and detecting resistance molecular alterations. However, in those cases where no genetic alteration is detected, it is necessary to integrate the analysis with the histological study of the tissues to identify the possible molecular drivers of resistance.
BRAF Mutation
gSeveral studies showed that detectable BRAF mutations on plasma of patients with BRAF mutated NSCLC correlate with tumor burden and disease dissemination in specific metastatic sites.37,117 A study by Sandra Ortiz-Cuaran et al117 analyzed a prospective cohort of 78 BRAF-positive NSCLC patients. Detectable BRAF mutations were found in 34 of 47 (72%) blood samples of patients naïve to BRAF-targeted therapies and correlated with systemic disease. From the results, it would also seem that the study of ctDNA in the early stages of treatment can be used as a predictor of therapy response.118,119 With regard to this aspect, ctDNA clearance at the first radiological evaluation during targeted therapy was observed in 63% (12/19) of cases and was associated with longer PFS and OS, while ctDNA positivity resulted to be correlated with worse survival outcomes.117 Serial monitoring of BRAF-ctDNA levels during treatment could be a potential marker of tumor response, as well as a surrogate for survival, like what has already been seen in patients with EGFR mutant NSCLC.28 However, further studies are needed to evaluate the reliability of the method, especially in the ability to individuate concomitant oncogenic alterations capable of generating primary resistance to anti-BRAF therapy.105
Other Molecular Targets
Since the first IASLC liquid biopsy statement,106 many studies have been designed to support the extension of ctDNA analysis to other recommended and treatable oncogenic drivers according to international guidelines, including MET amplification and exon 14 skipping mutations,120 RET rearrangements,121 HER2 mutations,122 and, lastly, exon 2 KRAS p.G12C mutation.123 Currently, all these studies are ongoing. Enrollment of patients in clinical trials should be encouraged to further validate the methods.
Conclusion
Considering the wide range of milestones achieved by personalized therapy in many solid tumors, exploiting pioneering molecular-based methods on more accessible tissue such as blood for managing cancer patients represents a practice-changing opportunity in oncology.
As for lung cancer, liquid biopsy has demonstrated to play a key role in both localized and metastatic disease (Figure 2). For early-stage disease, detecting ctDNA and MRD is effective in the early finding of recurrence after loco-regional treatment or as a screening tool. In the metastatic setting, oncogene-addicted NSCLC patients seem to benefit the most. In this subgroup, liquid biopsy is emerging as an integrative analysis of molecular tissue characterization and as a “plasma first” approach for assessing predictive and prognostic biomarkers at the time of diagnosis and during the treatment.
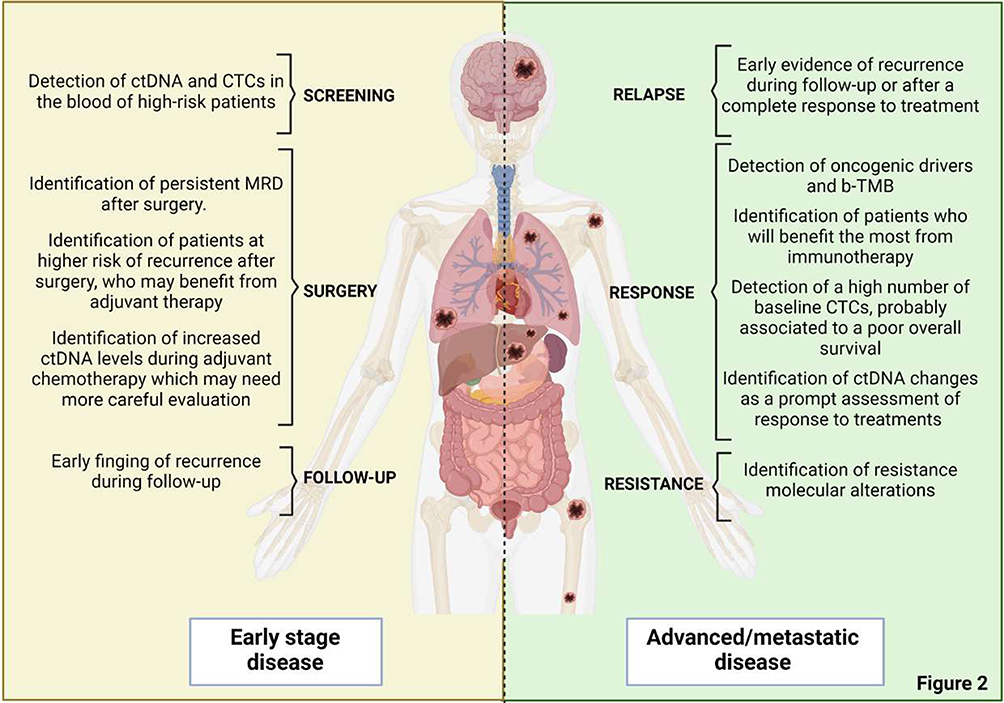 |
Figure 2 Potential applications of liquid biopsy in both localized and metastatic non-small cell lung cancer. Abbreviations: b-TMB, blood tumor mutational burden; ctDNA, circulating tumor DNA; MRD, minimal residual disease. |
In conclusion, liquid biopsy is an up-and-coming tool in NSCLC management, but further studies are needed before it enters routine evaluation practices.
Author Contributions
All authors made significant contributions to the reported work, whether in conception, study design, execution, data acquisition, analysis and interpretation, or all of these areas; participated in the drafting, review or critical review of the article; gave final approval of the version to be published; agreed on which journal the article was submitted to; and agrees to be responsible for all aspects of the job.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Rolfo C, Mack P, Scagliotti GV, et al. Liquid biopsy for advanced NSCLC: a consensus statement from the international association for the study of lung cancer. J Thorac Oncol. 2021;16(10):1647–1662. doi:10.1016/j.jtho.2021.06.017
2. Gambardella V, Tarazona N, Cejalvo JM, et al. Personalized medicine: recent progress in cancer therapy. Cancers. 2020;12(4):1009. doi:10.3390/cancers12041009
3. Ferrara MG, Di Noia V, D’Argento E, et al. Oncogene-addicted non-small-cell lung cancer: treatment opportunities and future perspectives. Cancers. 2020;12(5):1196. doi:10.3390/cancers12051196
4. Paez JG, Jänne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–1500. doi:10.1126/science.1099314
5. Kwak EL, Bang Y-J, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363:1693–1703. doi:10.1056/NEJMoa1006448
6. Shaw AT, Solomon BJ. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2015;372:683–684.
7. Wang R, Hu H, Pan Y, et al. RET fusions define a unique molecular and clinicopathologic subtype of non-small-cell lung cancer. J Clin Oncol. 2012;30(35):4352–4359. doi:10.1200/JCO.2012.44.1477
8. Farago AF, Taylor MS, Doebele RC, et al. Clinicopathologic features of non-small-cell lung cancer harboring an NTRK gene fusion. JCO Precis Oncol. 2018;2018:253.
9. Planchard D, Besse B, Groen HJ, et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Lancet Oncol. 2016;17:984–993.
10. Ou SH, Kwak EL, Siwak-Tapp C, et al. Activity of crizotinib (PF02341066), a dual mesenchymal-epithelial transition (MET) and anaplastic lymphoma kinase (ALK) inhibitor, in a non-small cell lung cancer patient with de novo MET amplification. J Thorac Oncol. 2011;6:942–946. doi:10.1097/JTO.0b013e31821528d3
11. Awad MM, Oxnard GR, Jackman DM, et al. MET exon 14 mutations in non-small-cell lung cancer are associated with advanced age and stage-dependent MET genomic amplification and c-Met overexpression. J Clin Oncol. 2016;34:721–773. doi:10.1200/JCO.2015.63.4600
12. Rossi A. New options for combination therapy for advanced non-squamous NSCLC. Expert Rev Respir Med. 2019;13(11):1095–1107. doi:10.1080/17476348.2019.1667233
13. Joyner MJ, Paneth N. Promises, promises, and precision medicine. J Clin Invest. 2019;129(3):946–948. doi:10.1172/JCI126119
14. Imyanitov EN, Iyevleva AG, Levchenko EV. Molecular testing and targeted therapy for non-small cell lung cancer: current status and perspectives. Crit Rev Oncol Hematol. 2021;157:103194. doi:10.1016/j.critrevonc.2020.103194
15. Mosele F, Remon J, Mateo J, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol. 2020;31:1491–1505. doi:10.1016/j.annonc.2020.07.014
16. Ignatiadis M, Sledge GW, Jeffrey SS. Liquid biopsy enters the clinic - implementation issues and future challenges. Nat Rev Clin Oncol. 2021;18(5):297–312. doi:10.1038/s41571-020-00457-x
17. Douillard JY, Ostoros G, Cobo M, et al. Gefitinib treatment in EGFR mutated caucasian NSCLC: circulating-free tumor DNA as a surrogate for determination of EGFR status. J Thorac Oncol. 2014;9(9):1345–1353. doi:10.1097/JTO.0000000000000263
18. Mok T, Wu YL, Lee JS, et al. Detection and dynamic changes of EGFR mutations from circulating tumor DNA as a predictor of survival outcomes in NSCLC patients treated with first-line intercalated erlotinib and chemotherapy. Clin Cancer Res. 2015;21(14):3196–3203. doi:10.1158/1078-0432.CCR-14-2594
19. Diaz LA, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014;32(6):579–586. doi:10.1200/JCO.2012.45.2011
20. Chen M, Zhao H. Next-generation sequencing in liquid biopsy: cancer screening and early detection. Hum Genomics. 2019;13(1):34. doi:10.1186/s40246-019-0220-8
21. ESMO. Clinical practice living guidelines – metastatic non-small-cell lung cancer. Available from: https://www.esmo.org/guidelines/guidelines-by-topic/lung-and-chest-tumours/clinical-practice-living-guidelines-metastatic-non-small-cell-lung-cancer.
22. Goswami RS, Luthra R, Singh RR, et al. Identification of factors affecting the success of next-generation sequencing testing in solid tumors. Am J Clin Pathol. 2016;145(2):222–237. doi:10.1093/ajcp/aqv023
23. Leighl NB, Page RD, Raymond VM, et al. Clinical utility of comprehensive cell-free DNA analysis to identify genomic biomarkers in patients with newly diagnosed metastatic non–small cell lung cancer. Clin Cancer Res. 2019;25(15):4691–4700. doi:10.1158/1078-0432.CCR-19-0624
24. Kapeleris J, Kulasinghe A, Warkiani ME, et al. The prognostic role of circulating tumor cells (CTCs) in lung cancer. Front Oncol. 2018;8:311. doi:10.3389/fonc.2018.00311
25. Crowley E, Di Nicolantonio F, Loupakis F, Bardelli A. Liquid biopsy: monitoring cancer-genetics in the blood. Nat Rev Clin Oncol. 2013;10(8):472–484. doi:10.1038/nrclinonc.2013.110
26. Russo A, De Miguel Perez D, Gunasekaran M, et al. Liquid biopsy tracking of lung tumor evolutions over time. Expert Rev Mol Diagn. 2019;19(12):1099–1108. doi:10.1080/14737159.2020.1680287
27. Wu YL, Lee V, Liam CK, et al. Clinical utility of a blood-based EGFR mutation test in patients receiving first-line erlotinib therapy in the ENSURE, FASTACT-2, and ASPIRATION studies. Lung Cancer. 2018;126:1–8. doi:10.1016/j.lungcan.2018.10.004
28. Oxnard GR, Thress KS, Alden RS, et al. Association between plasma genotyping and outcomes of treatment with osimertinib (AZD9291) in advanced non–small-cell lung cancer. JCO. 2016;34(28):3375–3382. doi:10.1200/JCO.2016.66.7162
29. Malapelle U, Buono M, Pisapia P, et al. Circulating tumor DNA in cancer: predictive molecular pathology meets mathematics. Crit Rev Oncol Hematol. 2021;163:103394. doi:10.1016/j.critrevonc.2021.103394
30. Zill OA, Banks KC, Fairclough SR, et al. The landscape of actionable genomic alterations in cell-free circulating tumor DNA from 21,807 advanced cancer patients. Clin Cancer Res. 2018;24(15):3528–3538. doi:10.1158/1078-0432.CCR-17-3837
31. Darbeheshti F, Yu F, Makrigiorgos GM. Pre-PCR mutation-enrichment methods for liquid biopsy applications. Cancers. 2022;14(13):3143. doi:10.3390/cancers14133143
32. Aggarwal C, Rolfo CD, Oxnard GR, Gray JE, Sholl LM, Gandara DR. Strategies for the successful implementation of plasma-based NSCLC genotyping in clinical practice. Nat Rev Clin Oncol. 2021;18(1):56–62. doi:10.1038/s41571-020-0423-x
33. Keppens C, Palma JF, Das PM, et al. Detection of EGFR variants in plasma: a multilaboratory comparison of a real-time PCR EGFR mutation test in Europe. J Mol Diagn. 2018;20(4):483–494. doi:10.1016/j.jmoldx.2018.03.006
34. Remon J, Lacroix L, Jovelet C, et al. Real-world utility of an amplicon-based next-generation sequencing liquid biopsy for broad molecular profiling in patients with advanced non–small-cell lung cancer. JCO Precis Oncol. 2019;3:1–14.
35. Hu Y, Ulrich BC, Supplee J, et al. False-positive plasma genotyping due to clonal hematopoiesis. Clin Cancer Res. 2018;24(18):4437–4443. doi:10.1158/1078-0432.CCR-18-0143
36. Gray JE, Okamoto I, Sriuranpong V, et al. Tissue and plasma EGFR mutation analysis in the FLAURA trial: osimertinib versus comparator egfr tyrosine kinase inhibitor as first-line treatment in patients with EGFR-mutated advanced non–small cell lung cancer. Clin Cancer Res. 2019;25(22):6644–6652. doi:10.1158/1078-0432.CCR-19-1126
37. Zhang M, Feng Y, Qu C, et al. Comparison of the somatic mutations between circulating tumor DNA and tissue DNA in Chinese patients with non-small cell lung cancer. Int J Biol Markers. 2022;37(4):386–394.
38. Goldstraw P, Chansky K, Crowley J, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (Eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):39–51. doi:10.1016/j.jtho.2015.09.009
39. Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552–3559. doi:10.1200/JCO.2007.13.9030
40. Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711–1723. doi:10.1056/NEJMoa2027071
41. Downey RJ, Martini N, Rusch VW, Bains MS, Korst RJ, Ginsberg RJ. Extent of chest wall invasion and survival in patients with lung cancer. Ann Thorac Surg. 1999;68(1):188–193. doi:10.1016/S0003-4975(99)00456-7
42. Guo N, Lou F, Ma Y, et al. Circulating tumor DNA detection in lung cancer patients before and after surgery. Sci Rep. 2016;6:33519. doi:10.1038/srep33519
43. Chen K, Zhang J, Guan T, et al. Comparison of plasma to tissue DNA mutations in surgical patients with non-small cell lung cancer. J Thorac Cardiovasc Surg. 2017;154(3):1123–1131. doi:10.1016/j.jtcvs.2017.04.073
44. Newman AM, Bratman SV, To J, et al. An ultrasensitive method for quantitating circulating tumor DNA with broad patient coverage. Nat Med. 2014;20:548–554. doi:10.1038/nm.3519
45. Wu F, Fan J, He Y, et al. Single-cell profiling of tumor heterogeneity and the microenvironment in advanced non-small cell lung cancer. Nat Commun. 2021;12(1):2540. doi:10.1038/s41467-021-22801-0
46. Chaudhuri AA, Chabon JJ, Lovejoy AF, et al. Early detection of molecular residual disease in localized lung cancer by circulating tumor DNA profiling. Cancer Discov. 2017;7(12):1394–1403. doi:10.1158/2159-8290.CD-17-0716
47. Abbosh C, Birkbak NJ, Wilson GA, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545(7655):446–451. doi:10.1038/nature22364
48. Ulrich B, Pradines A, Mazières J, Guibert N. Detection of tumor recurrence via circulating tumor DNA profiling in patients with localized lung cancer: clinical considerations and challenges. Cancers. 2021;13(15):3759. doi:10.3390/cancers13153759
49. Jamal-Hanjani M, Wilson GA, Horswell S, et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann Oncol. 2016;27(5):862–867. doi:10.1093/annonc/mdw037
50. Ulrich BC, Guibert N. Towards a comprehensive framework for cell-free DNA analysis: lessons from TRACERx. Ann Transl Med. 2017;5:428. doi:10.21037/atm.2017.08.12
51. Cohen JD, Li L, Wang Y, et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science. 2018;359(6378):926–930. doi:10.1126/science.aar3247
52. Guibert N, Pradines A, Favre G, Mazieres J. Current and future applications of liquid biopsy in nonsmall cell lung cancer from early to advanced stages. Eur Respir Rev. 2020;29(155):190052. doi:10.1183/16000617.0052-2019
53. Aberle DR, Adams AM; National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395–409.
54. de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503–513. doi:10.1056/NEJMoa1911793
55. Pastorino U, Sverzellati N, Sestini S, et al. Ten-year results of the Multicentric Italian Lung Detection trial demonstrate the safety and efficacy of biennial lung cancer screening. Eur J Cancer. 2019;118:142–148. doi:10.1016/j.ejca.2019.06.009
56. Phallen J, Sausen M, Adleff V, et al. Direct detection of early-stage cancers using circulating tumor DNA. Sci Transl Med. 2017;9(403):eaan2415. doi:10.1126/scitranslmed.aan2415
57. Bohers E, Viailly PJ, Jardin F. cfDNA sequencing: technological approaches and bioinformatic issues. Pharmaceuticals. 2021;14(6):596. doi:10.3390/ph14060596
58. Pierga JY, Bidard FC, Mathiot C, et al. Circulating tumor cell detection predicts early metastatic relapse after neoadjuvant chemotherapy in large operable and locally advanced breast cancer in a Phase II randomized trial. Clin Cancer Res. 2008;14(21):7004–7010. doi:10.1158/1078-0432.CCR-08-0030
59. van Dalum G, Stam G-J, Scholten LFA, et al. Importance of circulating tumor cells in newly diagnosed colorectal cancer. Int J Oncol. 2015;46:1361–1368. doi:10.3892/ijo.2015.2824
60. Ilie M, Hofman V, Long-Mira E, et al. ”Sentinel” circulating tumor cells allow early diagnosis of lung cancer in patients with chronic obstructive pulmonary disease. PLoS One. 2014;9:e111597. doi:10.1371/journal.pone.0111597
61. Leroy S, Benzaquen J, Mazzetta A, et al. Circulating tumour cells as a potential screening tool for lung cancer (the AIR study): protocol of a prospective multicentre cohort study in France. BMJ Open. 2017;7:e018884. doi:10.1136/bmjopen-2017-018884
62. Marquette CH, Boutros J, Benzaquen J, et al. Circulating tumour cells as a potential biomarker for lung cancer screening: a prospective cohort study. Lancet Respir Med. 2020;8(7):709–716. doi:10.1016/S2213-2600(20)30081-3
63. Brozos-Vázquez EM, Díaz-Peña R, García-González J, et al. Immunotherapy in nonsmall-cell lung cancer: current status and future prospects for liquid biopsy. Cancer Immunol Immunother. 2021;70(5):1177–1188. doi:10.1007/s00262-020-02752-z
64. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–2454. doi:10.1056/NEJMoa1200690
65. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
66. De Giglio A, Di Federico A, Deiana C, et al. Advanced non-small-cell lung cancer: how to manage non-oncogene disease. Drugs Context. 2022;11:2–4. doi:10.7573/dic.2022-2-4
67. Gandara DR, Paul SM, Kowanetz M, et al. Blood-based tumor mutational burden as a predictor of clinical benefit in non-small-cell lung cancer patients treated with atezolizumab. Nat Med. 2018;24(9):1441–1448. doi:10.1038/s41591-018-0134-3
68. Le DT, Uram JN, Wang H, et al. Blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372(26):2509–2520. doi:10.1056/NEJMoa1500596
69. Rizvi NA, Hellmann MD, Snyder A, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348(6230):124–128. doi:10.1126/science.aaa1348
70. Vanderwalde A, Spetzler D, Xiao N, et al. Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients. Cancer Med. 2018;7(3):746–756. doi:10.1002/cam4.1372
71. Yu Y, Zeng D, Ou Q, et al. Association of survival and immune-related biomarkers with immunotherapy in patients with non-small cell lung cancer: a meta-analysis and individual patient-level analysis. JAMA Netw Open. 2019;2(7):e196879. doi:10.1001/jamanetworkopen.2019.6879
72. Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med. 2020;383(14):1328–1339. doi:10.1056/NEJMoa1917346
73. Kim ES, Velcheti V, Mekhail T, et al. Blood-based tumor mutational burden as a biomarker for atezolizumab in non-small cell lung cancer: the phase 2 B-F1RST trial. Nat Med. 2022;28(5):939–945. doi:10.1038/s41591-022-01754-x
74. Rizvi NA, Cho BC, Reinmuth N, et al. Durvalumab with or without tremelimumab vs standard chemotherapy in first-line treatment of metastatic non-small cell lung cancer: the MYSTIC Phase 3 randomized clinical trial. JAMA Oncol. 2020;6(5):661–674. doi:10.1001/jamaoncol.2020.0237
75. Zhang Q, Luo J, Wu S, et al. Prognostic and predictive impact of circulating tumor DNA in patients with advanced cancers treated with immune checkpoint blockade. Cancer Discov. 2020;10(12):1842–1853. doi:10.1158/2159-8290.CD-20-0047
76. Gobbini E, Swalduz A, Levra MG, et al. Implementing ctDNA analysis in the clinic: challenges and opportunities in non-small cell lung cancer. Cancers. 2020;12(11):3112. doi:10.3390/cancers12113112
77. Corcoran RB, Chabner BA. Application of cell-free DNA analysis to cancer treatment. N Engl J Med. 2018;379(18):1754–1765. doi:10.1056/NEJMra1706174
78. Giroux Leprieur E, Herbretau G, Dumenil C, et al. Circulating tumor DNA evaluated by Next-Generation Sequencing is predictive of tumor response and prolonged clinical benefit with nivolumab in advanced non-small cell lung cancer. Oncoimmunology. 2018;7(5):e1424675. doi:10.1080/2162402X.2018.1424675
79. Diehl F, Schmidt K, Choti MA, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008;14:985–990. doi:10.1038/nm.1789
80. Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014;6:224ra24. doi:10.1126/scitranslmed.3007094
81. Goldberg SB, Narayan A, Kole AJ, et al. Early assessment of lung cancer immunotherapy response via circulating tumor DNA. Clin Cancer Res. 2018;24(8):1872–1880. doi:10.1158/1078-0432.CCR-17-1341
82. Anagnostou V, Forde PM, White JR, et al. Dynamics of tumor and immune responses during immune checkpoint blockade in non-small cell lung cancer. Cancer Res. 2019;79(6):1214–1225. doi:10.1158/0008-5472.CAN-18-1127
83. Guibert N, Delaunay M, Lusque A, et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer. 2018;120:108–112. doi:10.1016/j.lungcan.2018.04.001
84. Nicolazzo C, Raimondi C, Mancini M, et al. Monitoring PD-L1 positive circulating tumor cells in non-small cell lung cancer patients treated with the PD-1 inhibitor Nivolumab. Sci Rep. 2016;6:31726. doi:10.1038/srep31726
85. Ulivi P. Non-invasive methods to monitor mechanisms of resistance to tyrosine kinase inhibitors in non-small-cell lung cancer: where do we stand? Int J Mol Sci. 2016;17(7):1186. doi:10.3390/ijms17071186
86. Lim M, Kim CJ, Sunkara V, Kim MH, Cho YK. Liquid biopsy in lung cancer: clinical applications of circulating biomarkers (CTCs and ctDNA). Micromachines. 2018;9(3):100. doi:10.3390/mi9030100
87. Aggarwal C, Thompson JC, Black TA, et al. Clinical Implications of plasma-based genotyping with the delivery of personalized therapy in metastatic non-small cell lung cancer. JAMA Oncol. 2019;5(2):173–180. doi:10.1001/jamaoncol.2018.4305
88. Mack PC, Banks KC, Espenschied CR, et al. Spectrum of driver mutations and clinical impact of circulating tumor DNA analysis in non-small cell lung cancer: analysis of over 8000 cases. Cancer. 2020;126(14):3219–3228. doi:10.1002/cncr.32876
89. Ramalingam SS, Gray JE, Ohe Y, et al. Osimertinib vs comparator EGFR-TKI as first-line treatment for EGFRm advanced NSCLC (FLAURA): final overall survival analysis. Ann Oncol. 2019;30(suppl 5):v914–v915. doi:10.1093/annonc/mdz394.076
90. Douillard JY, Ostoros G, Cobo M, et al. First‐line gefitinib in Caucasian EGFR mutation‐positive NSCLC patients: a phase‐IV, open‐label, single‐arm study. Br J Cancer. 2014;110(1):55–62. doi:10.1038/bjc.2013.721
91. Reck M, Hagiwara K, Han B, et al. ctDNA determination of EGFR mutation status in European and Japanese patients with advanced NSCLC: the ASSESS study. J Thorac Oncol. 2016;11(10):1682–1689. doi:10.1016/j.jtho.2016.05.036
92. Wu YL, Sequist LV, Hu CP, et al. EGFR mutation detection in circulating cell‐free DNA of lung adenocarcinoma patients: analysis of LUX‐Lung 3 and 6. Br J Cancer. 2017;116(2):175–185. doi:10.1038/bjc.2016.420
93. Han B, Tjulandin S, Hagiwara K, et al. EGFR mutation prevalence in Asia‐Pacific and Russian patients with advanced NSCLC of adenocarcinoma and non‐adenocarcinoma histology: the IGNITE study. Lung Cancer. 2017;113:37–44. doi:10.1016/j.lungcan.2017.08.021
94. Papadimitrakopoulou VA, Wu YL, Han JY, et al. Analysis of resistance mechanisms to osimertinib in patients with EGFR T790M advanced NSCLC from the AURA3 study. Ann Oncol. 2018;29:Viii741. doi:10.1093/annonc/mdy424.064
95. Karlovich C, Goldman JW, Sun JM, et al. Assessment of EGFR mutation status in matched plasma and tumor tissue of NSCLC patients from a Phase I study of rociletinib (CO‐1686). Clin Cancer Res. 2016;22(10):2386–2395. doi:10.1158/1078-0432.CCR-15-1260
96. Sacher AG, Paweletz C, Dahlberg SE, et al. Prospective validation of rapid plasma genotyping for the detection of EGFR and KRAS mutations in advanced lung cancer. JAMA Oncol. 2016;2(8):1014–1022. doi:10.1001/jamaoncol.2016.0173
97. Zheng D, Ye X, Zhang MZ, et al. Plasma EGFR T790M ctDNA status is associated with clinical outcome in advanced NSCLC patients with acquired EGFR‐TKI resistance. Sci Rep. 2016;6(1):20913. doi:10.1038/srep20913
98. Qian X, Liu J, Sun Y, et al. Circulating cell‐free DNA has a high degree of specificity to detect exon 19 deletions and the single‐point substitution mutation L858R in non‐small cell lung cancer. Oncotarget. 2016;7(20):29154–29165. doi:10.18632/oncotarget.8684
99. Luo J, Shen L, Zheng D. Diagnostic value of circulating free DNA for the detection of EGFR mutation status in NSCLC: a systematic review and meta‐analysis. Sci Rep. 2014;4:6269. doi:10.1038/srep06269
100. Qiu M, Wang J, Xu Y. Circulating tumor DNA is effective for the detection of EGFR mutation in non‐small cell lung cancer: a meta‐analysis. Cancer Epidemiol Biomarkers Prev. 2015;24(1):206–212. doi:10.1158/1055-9965.EPI-14-0895
101. Mao C, Yuan JQ, Yang ZY, Fu XH, Wu XY, Tang JL. Blood as a substitute for tumor tissue in detecting EGFR mutations for guiding EGFR TKIs treatment of nonsmall cell lung cancer: a systematic review and meta‐ analysis. Medicine. 2015;94(21):e775. doi:10.1097/MD.0000000000000775
102. Zhou S, Huang R, Cao Y. Detection of epidermal growth factor receptor mutations in peripheral blood circulating tumor DNA in patients with advanced non‐small cell lung cancer: a PRISMA‐compliant meta‐analy‐ sis and systematic review. Medicine. 2020;99(40):e21965. doi:10.1097/MD.0000000000021965
103. Passiglia F, Rizzo S, Di Maio M, et al. The diagnostic accuracy of circulating tumor DNA for the detection of EGFR‐T790M mutation in NSCLC: a systematic review and meta‐analysis. Sci Rep. 2018;8(1):13379. doi:10.1038/s41598-018-30780-4
104. Piper-Vallillo AJ, Sequist LV, Piotrowska Z. Emerging treatment paradigms for EGFR-mutant lung cancers progressing on osimertinib: a review. J Clin Oncol. 2020;38:2926–2936. doi:10.1200/JCO.19.03123
105. Zhou C, Imamura F, Cheng Y, et al. Early clearance of plasma EGFR mutations as a predictor of response to osimertinib and comparator EGFR-TKIs in the FLAURA trial. J Clin Oncol. 2019;37(suppl 15):9020. doi:10.1200/JCO.2019.37.15_suppl.9020
106. Mack PC, Redman MW, Moon J, et al. Residual circulating tumor DNA (ctDNA) after two months of therapy to predict progression-free and overall survival in patients treated on S1403 with Afatinib ± cetuximab. J Clin Oncol. 2020;38(suppl 15):9532. doi:10.1200/JCO.2020.38.15_suppl.9532
107. Hofman P. Detecting resistance to therapeutic ALK inhibitors in tumor tissue and liquid biopsy markers: an update to a clinical routine practice. Cells. 2021;10(1):168. doi:10.3390/cells10010168
108. Kunimasa K, Kato K, Imamura F, et al. Quantitative detection of ALK fusion breakpoints in plasma cell‐free DNA from patients with non‐small cell lung cancer using PCR‐based target sequencing with a tiling primer set and two‐step mapping/alignment. PLoS One. 2019;14(9):e0222233. doi:10.1371/journal.pone.0222233
109. Dagogo-Jack I, Brannon AR, Ferris LA, et al. Tracking the Evolution of Resistance to ALK Tyrosine Kinase Inhibitors through Longitudinal Analysis of Circulating Tumor DNA. JCO Precis Oncol. 2018;2018:
110. McCoach CE, Blakely CM, Banks KC, et al. Clinical utility of cell-free DNA for the detection of ALK fusions and genomic mechanisms of ALK inhibitor resistance in non-small cell lung cancer. Clin Cancer Res. 2018;24(12):2758–2770. doi:10.1158/1078-0432.CCR-17-2588
111. Shaw AT, Solomon BJ, Besse B, et al. ALK resistance mutations and efficacy of lorlatinib in advanced anaplastic lymphoma kinase-positive non-small-cell lung cancer. J Clin Oncol. 2019;37(16):1370–1379. doi:10.1200/JCO.18.02236
112. Dagogo-Jack I, Rooney M, Lin JJ, et al. Treatment with next-generation ALK inhibitors fuels plasma ALK mutation diversity. Clin Cancer Res. 2019;25(22):6662–6670. doi:10.1158/1078-0432.CCR-19-1436
113. Lin JJ, Shaw AT. Recent advances in targeting ROS1 in lung cancer. J Thorac Oncol. 2017;12(11):1611–1625. doi:10.1016/j.jtho.2017.08.002
114. Davies KD, Le AT, Sheren J, et al. Comparison of molecular testing modalities for detection of ros1 rearrangements in a cohort of positive patient samples. J Thorac Oncol. 2018;13(10):1474–1482. doi:10.1016/j.jtho.2018.05.041
115. Paweletz CP, Sacher AG, Raymond CK, et al. Bias-corrected targeted next-generation sequencing for rapid, multiplexed detection of actionable alterations in cell-free DNA from advanced lung cancer patients. Clin Cancer Res. 2016;22(4):915–922. doi:10.1158/1078-0432.CCR-15-1627-T
116. Dagogo-Jack I, Rooney M, Nagy RJ, et al. Molecular analysis of plasma from patients with ROS1-positive NSCLC. J Thorac Oncol. 2019;14(5):816–824. doi:10.1016/j.jtho.2019.01.009
117. Ortiz-Cuaran S, Mezquita L, Swalduz A, et al. Circulating tumor DNA genomics reveal potential mechanisms of resistance to BRAF-targeted therapies in patients with braf-mutant metastatic non-small cell lung cancer. Clin Cancer Res. 2020;26(23):6242–6253. doi:10.1158/1078-0432.CCR-20-1037
118. Garlan F, Laurent-Puig P, Sefrioui D, et al. Early evaluation of circulating tumor DNA as marker of therapeutic efficacy in metastatic colorectal cancer patients (PLACOL Study). Clin Cancer Res. 2017;23:5416–25.17. doi:10.1158/1078-0432.CCR-16-3155
119. Guibert N, Jones G, Beeler JF, et al. Targeted sequencing of plasma cell-free DNA to predict response to PD1 inhibitors in advanced non-small cell lung cancer. Lung Cancer. 2019;137:1–6. doi:10.1016/j.lungcan.2019.09.005
120. Guo R, Offin M, Brannon AR, et al. MET exon 14-altered lung cancers and MET inhibitor resistance. Clin Cancer Res. 2021;27:799–806. doi:10.1158/1078-0432.CCR-20-2861
121. Lin JJ, Liu SV, McCoach CE, et al. Mechanisms of resistance to selective RET tyrosine kinase inhibitors in RET fusion-positive non-small-cell lung cancer. Ann Oncol. 2020;31:1725–1733. doi:10.1016/j.annonc.2020.09.015
122. Schwartzberg LS, Horinouchi H, Chan D, et al. Liquid biopsy mutation panel for non-small cell lung cancer: analytical validation and clinical concordance. NPJ Precis Oncol. 2020;4:15. doi:10.1038/s41698-020-0118-x
123. Nacchio M, Sgariglia R, Gristina V, et al. KRAS mutations testing in non-small cell lung cancer: the role of liquid biopsy in the basal setting. J Thorac Dis. 2020;12:3836–3843. doi:10.21037/jtd.2020.01.19
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outcomes of Patients with EGFR-Mutant Advanced NSCLC in a Developing Country in Southeast Asia
How SH, Liam CK, Zainal Abidin MA, Hasbullah HH, Tho LM, Ho GF, Muhamad Nor I, Pang YK, Ho KF, Thiagarajan M, Ariffin R, Samsudin A, Omar A, Tan SN, Ong CK, Soon SY, Poh ME
Cancer Management and Research 2022, 14:1995-2005
Published Date: 16 June 2022
Overcoming Obstacles in Liquid Biopsy Developments for Prostate Cancer
Jang A, Rauterkus GP, Vaishampayan UN, Barata PC
OncoTargets and Therapy 2022, 15:897-912
Published Date: 26 August 2022
AC099850.3/NCAPG Axis Predicts Poor Prognosis and is Associated with Resistance to EGFR Tyrosine-Kinase Inhibitors in Lung Adenocarcinoma
Bao J, Wu Y, Zhang K, Qi H
International Journal of General Medicine 2022, 15:6917-6930
Published Date: 29 August 2022
Cost-Effectiveness of Abemaciclib in Early Breast Cancer Patients: One Size Fits All or Tailoring to Patients’ Needs?
Jongbloed EM, Blommestein HM, van Schoubroeck HM, Martens JW, Wilting SM, Uyl-de Groot CA, Jager A
Breast Cancer: Targets and Therapy 2023, 15:147-161
Published Date: 16 February 2023
Post-IMvigor011 Era: CtDNA-Guided Postoperative Adjuvant Treatment Stratification in Muscle-Invasive Bladder Cancer
Sui J, Chen Y, Jiang Y, He Q, Guo X
Cancer Management and Research 2026, 18:609903
Published Date: 10 July 2026