")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Cost-Effectiveness of Abemaciclib in Early Breast Cancer Patients: One Size Fits All or Tailoring to Patients’ Needs?
Authors Jongbloed EM, Blommestein HM, van Schoubroeck HM, Martens JW, Wilting SM , Uyl-de Groot CA, Jager A
Received 19 September 2022
Accepted for publication 19 January 2023
Published 16 February 2023 Volume 2023:15 Pages 147—161
DOI https://doi.org/10.2147/BCTT.S387375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Elisabeth M Jongbloed,1 Hedwig M Blommestein,2 Hannah M van Schoubroeck,2 John WM Martens,1 Saskia M Wilting,1 Carin A Uyl-de Groot,2 Agnes Jager1
1Department of Medical Oncology; Erasmus MC Cancer Institute, Rotterdam, the Netherlands; 2Erasmus School of Health Policy and Management, Erasmus University, Rotterdam, the Netherlands
Correspondence: Elisabeth M Jongbloed, Department of Medical Oncology; Erasmus MC Cancer Institute, Dr. Molenwaterplein 40, Rotterdam, 3014 GD, the Netherlands, Tel +31 107044375, Email [email protected]
Purpose: The addition of two years of abemaciclib treatment to standard adjuvant endocrine therapy in all patients with high risk ER+, HER2- early breast cancer (EBC) has been approved by the US Food and Drug Administration (FDA). Pre-selection of patients with an immediate risk of recurrence within the group of clinically high risk patients using detection of minimal residual disease (MRD) using patient-informed circulating tumor DNA assays during follow-up could enhance efficacy. Here, we investigate the cost-effectiveness of the addition of two years abemaciclib in all high risk HR+, HER2- patients and in MRD-guided high risk patients only.
Methods: Two semi-Markov models were developed to evaluate the cost-effectiveness of adding two years of abemaciclib compared to “standard treatment”: 1) “abemaciclib all” and 2) “MRD-guided abemaciclib” using MRD-guidance. Data of the MonarchE trial were used to model the invasive disease-free survival (iDFS). Since iDFS and overall survival (OS) data of abemaciclib were currently limited, abemaciclib effects were extrapolated using a favorable, intermediate and unfavorable effect scenario.
Results: The addition of abemaciclib in all high-risk EBC patients prolonged iDFS slightly (0.04 additional quality adjusted life years (QALYs)) and led to higher costs compared to standard ET, leading to a high incremental cost effectiveness ratio (ICER) of € 1,551,876/QALY. Neither the favorable effect scenario (additional 1.09 QALYs) was cost-effective (ICER € 62,935/QALY), using a willingness-to-pay threshold of € 50,000/QALY. The “MRD-guided abemaciclib” strategy resulted in lower costs and an increase in QALYs (1.27) compared to “standard treatment” in the unfavorable effect scenario.
Conclusion: The addition of abemaciclib to adjuvant endocrine therapy in all high-risk ER+, HER2- EBC patients is not cost-effective. However, using MRD detection to justify the addition of abemaciclib treatment dominates standard treatment in this cost-effectiveness analysis. Further evaluation of MRD detection in EBC by means of prospective clinical trials assessing clinical utility is recommended and promising in terms of cost-effectiveness.
Keywords: breast cancer, minimal residual disease, circulating tumor DNA, cost-effectiveness, abemaciclib
Introduction
Hormone receptor positive (HR+) breast cancer represents 70% of all primary breast cancers. Adjuvant endocrine therapy reduces the recurrence rate in these patients,1,2 however a significant proportion still experiences recurrence of disease. This has increased interest in research focusing on additional therapies aiming to prevent recurrences. Currently, several randomized placebo-controlled Phase III trials are investigating the effectiveness of adding 1–3 years of a CDK4/6 inhibitor to standard adjuvant endocrine therapy in early breast cancer (EBC) patients.3–5 One of these trials is the MonarchE study, a phase III trial investigating the efficacy and safety of adding abemaciclib during the first two years of standard endocrine therapy in EBC patients showing a significant improvement in iDFS of 5.4% in the abemaciclib treated arm (88.8% versus 83.4%, respectively) after a median duration of follow-up of 27.0 months.6 Based on these results both the Food and Drug Administration (FDA) and European Medicines Agency (EMA) have approved abemaciclib for the treatment of ER+/HER2-, node-positive EBC patients at high risk of recurrence.
Worldwide implementation of the addition of two years of abemaciclib treatment to standard endocrine therapy for high risk ER+/HER2- EBC patients is expected to have an enormous impact on the health budget. Resources are scarce and can only be spent once. Without a currently proven overall survival benefit, it is questionable whether abemaciclib addition in this patient group provides efficient use of a scarce resource. The expected increase in health care costs, together with the additional burden on patients treated with the combination therapy (extra blood checks, hospital visits and an increase in side effects), emphasize the need for a thorough evaluation of the cost-effectiveness of this treatment strategy.
More adequate patient selection is expected to identify those patients in need of additional treatment in terms of overall survival (OS) and limits the burden on patients without a need for additional treatment. Adequate patient selection could potentially be reached by using minimal residual disease (MRD) detection, since only those EBC patients with detectable MRD over time will develop recurrence of disease.7,8 MRD detection could be performed by monitoring circulating tumor DNA (ctDNA) by serial blood-sampling of patients.8 However, serial detection of ctDNA over time is expensive as well and the overall impact on the cost-effectiveness of such an approach is unknown.
In this study we therefore investigate the cost-effectiveness of adding two years of abemaciclib to standard adjuvant endocrine therapy in all high risk ER+/HER2- EBC patients based on the currently available data. Subsequently, we will calculate the potential influence of adding MRD-guided patient selection as a condition for two years of abemaciclib treatment in this group on the cost-effectiveness.
Materials and Methods
Population and Treatment Strategies
The focus of this cost-effectiveness analysis was on pre- and post-menopausal ER+/HER2- EBC patients with positive lymph nodes and at a high risk of recurrence according to the population in which adjuvant abemaciclib is FDA approved. Three different treatment strategies were compared in this analysis (Figure 1). First, “standard treatment” ie patients received current standard of adjuvant endocrine treatment (20 mg tamoxifen or 2.5 mg letrozole/anastrozole daily, including a GnRH agonist in premenopausal patients) during 5 years; second “abemaciclib all” ie patients received abemaciclib (150mg twice daily) for two years added to “standard treatment”; third the explorative “MRD-guided abemaciclib”, ie patients received “standard treatment” and only in patients with detected MRD during five years of follow-up abemaciclib (150mg twice daily) was added for two years. Determining MRD can be performed in multiple ways. In our model we assumed and implemented the method used in the study of Garcia-Murillas et al,8 ie, firstly detecting all mutations present in the primary tumor of a patient using NGS sequencing by a custom Ion AmpliSeq™ Breast Cancer Panel targeting 14 known driver breast cancer genes,9 and secondly measuring the identified tumor specific mutations per patient in the cell free DNA of blood samples using patient-specific digital PCR assays every 6 months starting within 4 weeks postoperatively for 5 years. The presence of MRD was defined as the presence of a tumor specific mutation was detected in cfDNA by dPCR. At the time of MRD detection (ie a positive signal for a tumor-specific mutation in the blood of the patient), abemaciclib was prescribed for two years in these patients. A time frame of five years of MRD detection in our model was chosen to maximize the added value of abemaciclib, ie fewer patients will receive abemaciclib treatment (only those with MRD detection), but ultimately more patients will benefit from therapy by MRD detection because not only during the first two years but up to five years after the surgery MRD detection is performed.
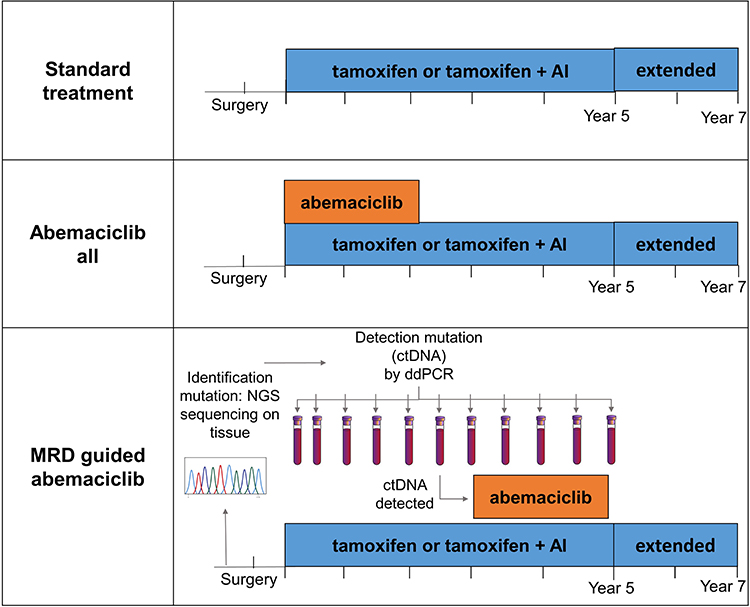 |
Figure 1 Treatment strategies. |
Model
Two semi-Markov model were constructed to compare the costs and effectiveness of endocrine therapy with and without abemaciclib in HR+/HER2- early breast cancer patients. For the treatment strategies “standard treatment” and “abemaciclib all” the model consisted of the following three health states: recurrence free, recurrent disease, and death (Figure 2A). For the treatment strategy “MRD-guided abemaciclib” the model includes one additional health state: minimal residual disease (Figure 2B). A hypothetical population of 1000 EBC patients with a mean age of 57 years, according to the mean age of patients with HR+/HER2- EBC in the Netherlands, starting in the recurrence free state directly at initiation of adjuvant endocrine therapy.10 This hypothetical population was used for all three treatment strategies. For the “standard treatment” and “abemaciclib all” strategies patients could progress from the recurrence free state to the recurrent disease or death state. Patients in the “MRD guided abemaciclib” strategy could also transition from “recurrence free” state to the health state “MRD”, but they could not return to the MRD state after disease recurrence or death. Cycle length was three months, and a half cycle correction was implemented. As the transition from the MRD state to the recurrent disease state is time dependent, additional tunnel states were added each time a blood sample was taken for MRD detection (ie every six months for five years).
 |
Figure 2 Markov models. Abbreviation: EBC, early breast cancer. Notes: Patients enter the model at initiation of adjuvant endocrine therapy for EBC in the health state “Recurrence Free”. (A) Markov model with the three health states and different possible transitions for treatment strategies “standard treatment” and “additional abemaciclib”. (B) Markov model with the four health states and different possible transitions for treatment strategy “MRD based abemaciclib”. |
According to the Dutch pharmaco-economic guidelines a Dutch societal perspective was chosen; a lifetime horizon was used and costs and effects were discounted by 4% and 1.5%, respectively.11
Input
Survival Probabilities and Extrapolation
For the transition between the health states, survival data of several large randomized clinical trials and meta-analyses were used. For the treatment strategy “standard treatment” data on invasive disease-free survival (iDFS) of the first 3 years after initiation of endocrine therapy were derived from the MonarchE trial5 and were extrapolated for one year with a log-normal distribution. Expert opinion (AJ) was used to determine the validity of the type of the curves of the extrapolation. iDFS data until 4 years since the initiation of endocrine therapy were extrapolated using the rate of recurrences of the high risk population (N4-N9) in the study of Pan et al.1 The rate of the recurrences after 20 years was kept equal compared to the rate between 15 and 20 years after initiation of endocrine therapy. OS data were also retrieved from the high risk group (N4-N9) of the study of Pan et al1 and extrapolated with a log-normal distribution, since this distribution had the lowest AIC. Due to the short follow-up of the MonarchE study, assumptions on the nature and duration of the iDFS curve and OS curve of the abemaciclib treatment strategy had to be made. Three different scenarios with different assumptions regarding the recurrence and overall survival after abemaciclib treatment were created: an unfavorable effect scenario, an intermediate effect scenario and a favorable effect scenario (Table 1). The unfavorable scenario assumed that abemaciclib improves iDFS during 3 years, afterwards this effect diminishes and within 1 year the iDFS is comparable for both “standard treatment” and “abemaciclib all” (Supplemental Figure 1A and B). In this most unfavorable scenario, there is no beneficial effect of abemaciclib in terms of OS. In the intermediate effect scenario abemaciclib improves iDFS during 3 years according to the effect in the MonarchE study, after 3 years the recurrence rate for both standard treatment and the addition of abemaciclib is kept equal (Supplemental Figure 1C and D), which is remained over a lifetime. In terms of OS abemaciclib improves OS over a lifetime which is based on the hazard ratio (HR) of abemaciclib compared to endocrine therapy only in the metastatic setting (HR = 0.757).12 The most favorable scenario assumed that the iDFS gain which is reached after 3 years is continued over a lifetime and that abemaciclib improves the OS with an equal HR of abemaciclib compared to endocrine therapy for the iDFS (HR=0.63) (Supplemental Figure 1E and F). Transition probabilities to the MRD health state in the treatment strategy “MRD-based abemaciclib” were retrieved from the study of Garcia Murillas et al.8 Both EBC and non-EBC related deaths were included in the model and OS was adjusted for background mortality using data provided by Statistics Netherlands (CBS).13
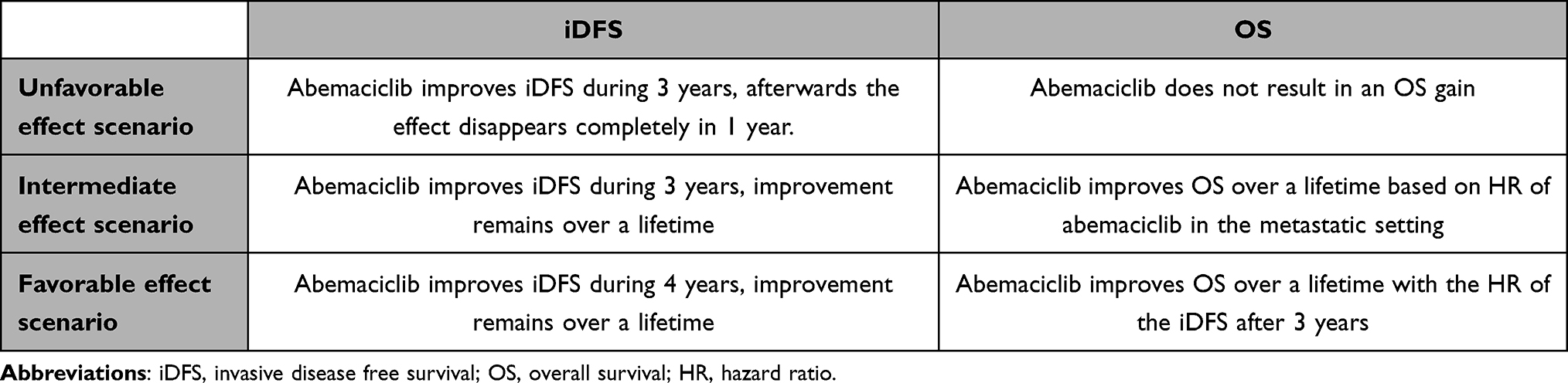 |
Table 1 Abemaciclib Effect Scenarios |
Utility Values
The utility values for the different health states were derived from Rautalin et al.14 By means of the EQ-5D, they calculated utility values of 0.87 and 0.74 for the recurrence free and recurrent disease health states, respectively. As patients have not yet developed full recurrent disease in the MRD state, a utility value of 0.87 was assigned to this state as well. To adjust for discomfort due to treatment, disutility for adverse events were incorporated in the model. Adverse event data were retrieved from the MonarchE study and only grade III and IV events that were present in at least 5% of either treatment arm were included (ie, neutropenia, leukopenia, diarrhea and lymphopenia). Disutility values for these adverse events were retrieved from studies by Uyl-de Groot et al and Bullement et al and can be found in Table 2.15,16 These values were added to the model for 2 days for neutropenia, leukopenia and lymphopenia and for 7 days for diarrhea.
 |
Table 2 Input Parameters |
Cost Inputs
For patients in the disease-free health states, costs within the following categories were included in the model: drug acquisition, hospital visits, imaging, laboratory tests, genetic testing and MRD detection, adverse events and societal costs. In the recurrent disease state, only medical and societal costs were included. Input variables were derived from literature, treatment protocols, the Dutch national health care institute, expert opinion and hospital price lists.17,18 When necessary, costs were indexed to 2021 values. Short term productivity loss was calculated by multiplying the number of work hours (both paid and unpaid) missed by their respective costs per hour. Assuming that patients stop working from the moment of disease recurrence, long-term productivity loss was calculated by means of the friction cost method and implemented as a one-off cost at the moment of disease recurrence. This means that productivity loss is calculated by multiplying the average number of hours a patient would have worked (paid and unpaid work) during the “friction period”, the average period of time in which an employee would be replaced, by their respective costs per hour.19 As productivity loss data was only available for patients receiving standard treatment, estimation on hours lost were made according to differences in the number of hospital visits and the number of days of the occurrence of adverse events.
Outcomes
The average total costs, life years and QALYs generated per patient are the primary outputs of this model. With these outputs the incremental costs and effects between standard treatment and abemaciclib all and between standard treatment and MRD-based abemaciclib were calculated. Based on these costs and effects, ICERs were calculated. The ICERs were compared to the willingness to pay threshold (WTP), ie €50,000/QALY based on the disease burden calculated with the iMTA burden of disease calculator.20
Deterministic Sensitivity Analysis
Deterministic scenario analyses were performed to assess the impact of the uncertainty of the individual input parameters on the ICER. Parameters were varied by their minimum and maximum values (Table 2). Extrapolated survival curves were varied by adding and subtracting 10% on the annually event rate of the applied iDFS and OS curve from the literature.1
Probabilistic Sensitivity Analysis
Probabilistic sensitivity analysis (PSA) was performed to assess the effect of the uncertainty surrounding the input parameters on the ICERs. The PSA consisted of 1000 iterations with random values according to the distribution of all parameters. For the extrapolated survival curves, an upper and lower limit was created by increasing and decreasing the annual event rate with 20%. Assuming a normal distribution, random curves were selected within this range. When standard errors (SE) of input parameters were not provided in literature, an arbitrary percentage of the mean value is applied using 10% for fixed unit costs and 20% for healthcare resource use parameters, since we expect a higher uncertainty around these parameters (Table 2). Beta distributions were used for probabilities, utilities and disutilities, and gamma distributions were used for the costs.
Results
“Abemaciclib All” Compared to “Standard Treatment”
The total average costs per patient of standard adjuvant endocrine therapy were €198,929 per patient (Table 3). When all ER+/HER2- EBC patients were also treated with two years of abemaciclib, total treatment costs increased to €261,995, €264,255 and €267,551 for the unfavorable, intermediate and favorable effect scenarios, as defined in the Materials and Methods section, respectively. The main difference in costs between “standard treatment” and “abemaciclib all” treatment regime is caused by drug acquisition, but also the healthcare resource use costs, adverse event medical costs and societal costs increase when abemaciclib is added (Table 3). The average number of life years was 19.16 in patients treated with “standard treatment” and 19.20, 20.05 and 20.46 life years for patients treated according to the “abemaciclib all” strategy for the unfavorable, intermediate and favorable effect scenario, respectively. Patients who received standard treatment obtained 15.81 QALYs and patients who were treated according to the “abemaciclib all” strategy obtained 15.85 (unfavorable scenario), 16.57 (intermediate scenario) and 16.90 (favorable scenario) QALYs associated with incremental costs of €63,066; €65,326 and €68,622. Together this results in ICERs of €1,551,876/QALY; €86,632/QALY and €62,935/QALY for the unfavorable, intermediate and favorable effect scenarios, respectively. This means that adding abemaciclib for 2 years to standard endocrine treatment in all high risk EBC patients is not cost-effective according to a WTP threshold of €50,000/QALY.
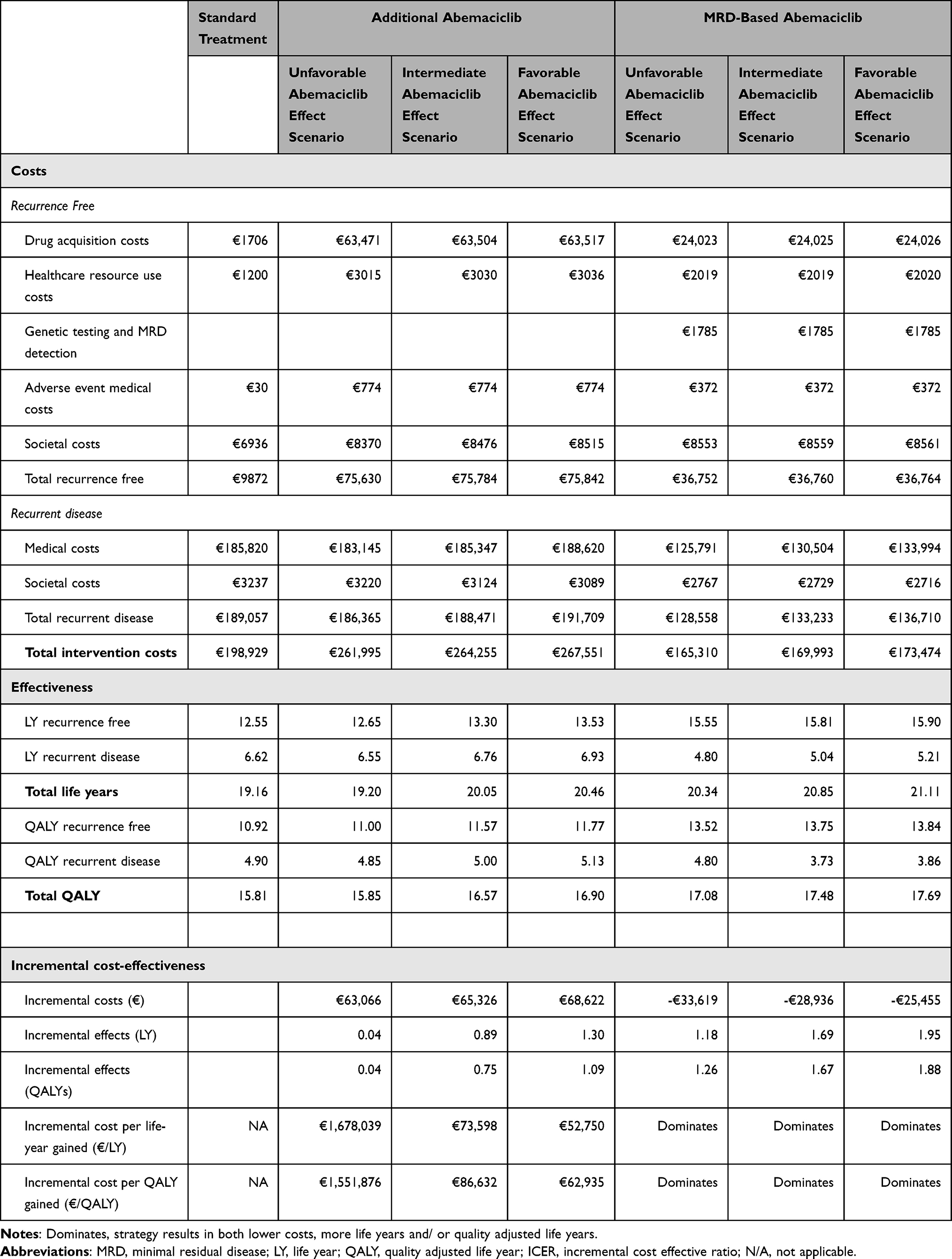 |
Table 3 Costs, Effectiveness and Incremental Cost-Effectiveness per Treatment Strategy and Abemaciclib Effect Scenario |
“MRD-Based Abemaciclib” Compared to “Standard Treatment”
The total treatment costs for the “MRD-based abemaciclib” treatment were €165,310, €169,993 and €173,474 per patient for the unfavorable, intermediate and favorable effect scenarios (Table 3). These costs were substantially lower compared to those of the “standard treatment” regime (€198,929), mainly caused by a decrease in the number of recurrences. These costs were also substantially lower compared to the “abemaciclib all” strategy (€261,995, €264,255 and €267,551, respectively). The diagnostic costs in the MRD-based abemaciclib scenario were much higher (€1785 per patient for genetic testing and MRD detection). However, since in this strategy, only a part of the patients (ie the patients who are or become ctDNA positive) will receive abemaciclib, the lower drug acquisition still results in overall lower costs.
The “MRD based abemaciclib” strategy results in a gain of 1.18, 1.69 and 1.95 life years and 1.26, 1.67 and 1.88 QALYs respectively for the favorable, intermediate and unfavorable effect scenario compared to “standard treatment”. This means that “MRD-based abemaciclib” dominates “standard treatment” for all treatment effect scenarios (ie more effective and less costly).
Deterministic Sensitivity Analyses
The ten most influential input parameters on the ICER, for the comparison between “abemaciclib all” and “standard treatment” for the intermediate scenario are shown in Figure 3. The parameter with the highest impact on the ICER is the iDFS curve of abemaciclib, which is a combination of the observed recurrences in the MonarchE study in combination with recurrences observed in the study of Pan et al.1 None of the lower limits of the parameters resulted in an ICER below the threshold of €50,000/QALY. A decrease in price of abemaciclib of 10% does not make the “abemaciclib all” treatment strategy cost-effective compared to “standard treatment” with an ICER of €78,447. The impact of the individual input parameters on the incremental costs and incremental QALYs for the comparison between “MRD-based abemaciclib” and “standard treatment” in the intermediate abemaciclib effect scenario are shown in Figure 4. The parameter with the highest impact on the costs was recurrent disease, which could be explained by the fact that fewer patients will enter the recurrent disease state in the MRD guided strategy compared to standard treatment because they enter the MRD state. When costs of this state increase or decrease this will have a large effect on total incremental costs of the MRD guided strategy versus standard treatment strategy. The parameter with the highest impact on incremental QALYs was the utility value of recurrent disease-free patients.
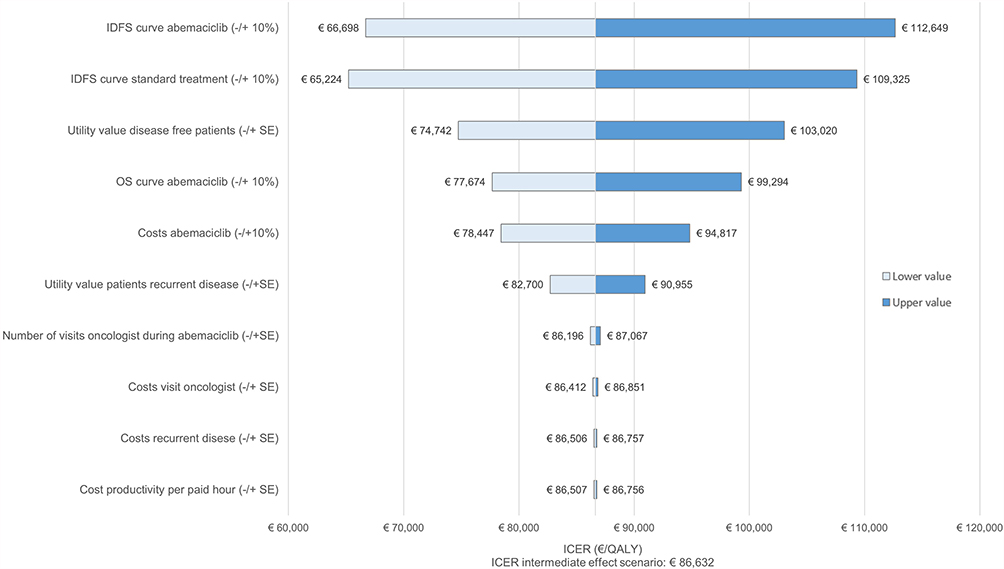 |
Figure 3 Tornado diagrams of one-way sensitivity analysis for “abemaciclib all” versus “standard therapy” for the intermediate effect scenario. Abbreviations: QALY, quality adjusted life year; ICER, incremental cost effective ratio. Notes: Tornado plot shows the impact of changes in the individual parameters on the ICER. ICER for this comparison and effect scenario is: €86.632/QALY. |
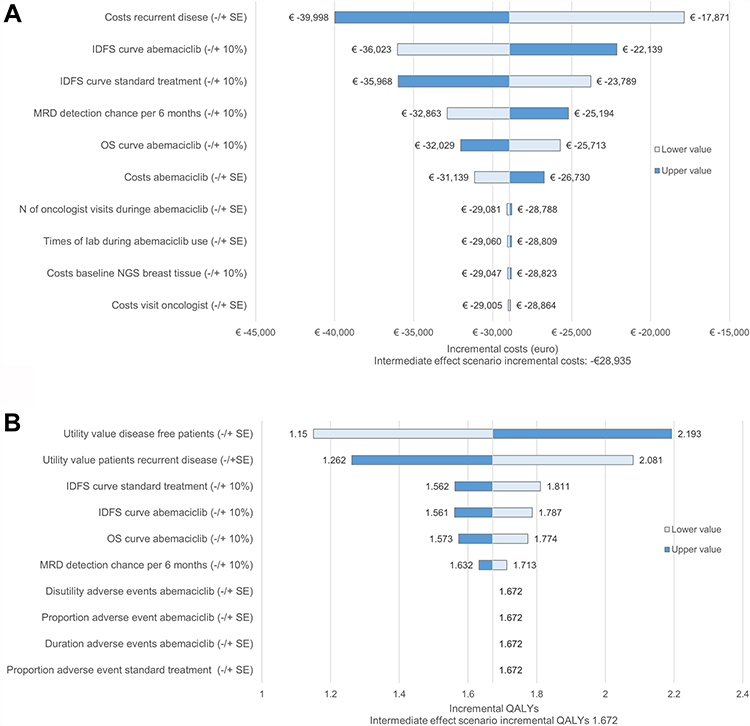 |
Figure 4 Tornado diagrams of one-way sensitivity analyses for “MRD guided abemaciclib” versus “standard therapy” for the intermediate effect scenario. Notes: (A) Tornado diagram showing the impact of changes in the individual parameters on the incremental costs. Incremental costs for this comparison and effect scenario is -€28,935. (B) Tornado diagram showing impact of changes in the individual parameters on the incremental QALYs. Incremental QALYs for this comparison and effect scenario is 1.672. |
Probabilistic Sensitivity Analyses (PSA)
Figure 5 shows the PSA results for “abemaciclib all” compared to “standard treatment” for the unfavorable, intermediate and favorable scenario. The addition of abemaciclib in the abemaciclib all treatment strategy will lead to an increase in costs and QALYs in respectively 62.7%, 99.9% and 100% of the results of the PSA in the unfavorable, intermediate, and favorable abemaciclib effect scenarios (Figure 5A, C and E). This is indicated by the right upper quadrant. The likelihood of the addition of abemaciclib to be cost-effective, given a WTP of €50,000, was 0.1% for the unfavorable effect scenario (Figure 5B), 6.4% for the intermediate and 27.9% for the favorable effect scenario (Figure 5D and F).
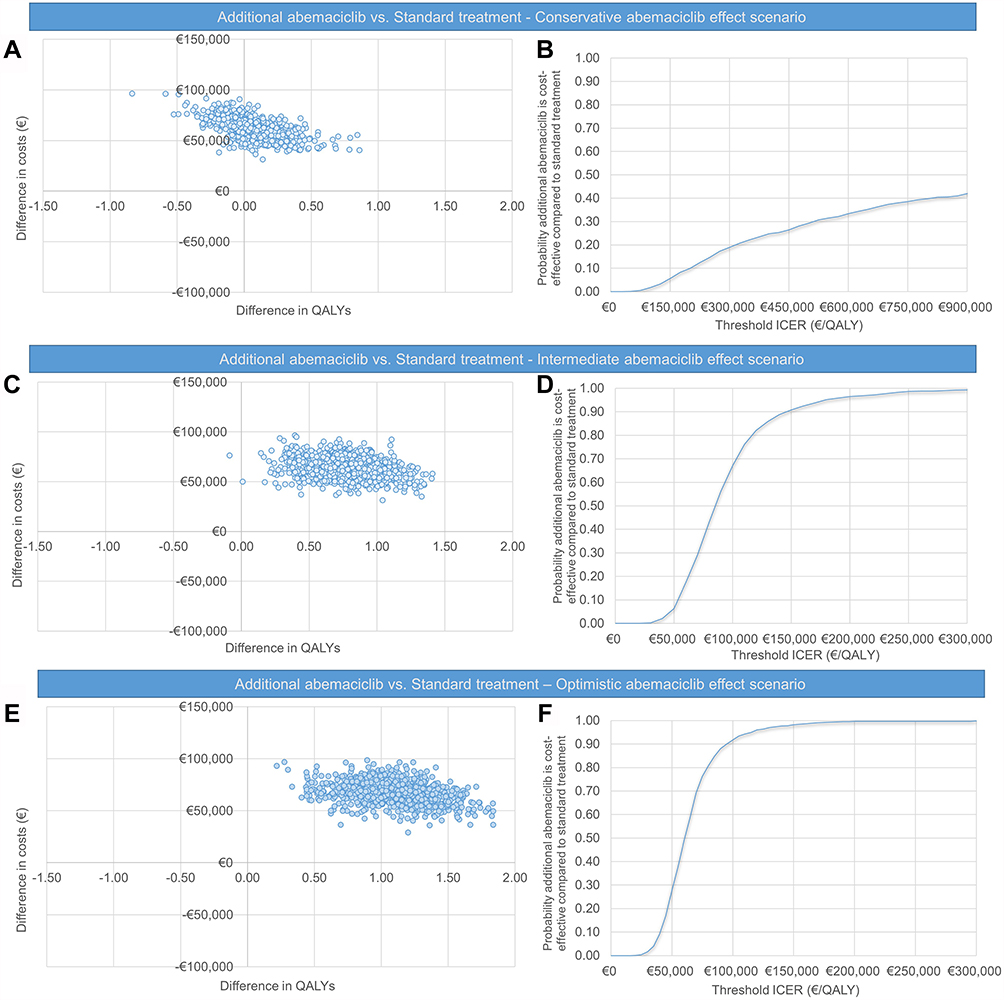 |
Figure 5 Sensitivity analyses of “abemaciclib all” versus “standard therapy”. Abbreviations: ICER, incremental cost effectiveness ratio; QALY, quality adjusted life year. Notes: (A) Incremental cost-effectiveness plane of the QALYs per cost for “abemaciclib all” in high risk ER+/HER2- EBC patients versus “standard treatment”. The scatter plot shows the results in mean differences in costs and QALYs of 1000 times running the model. For the unfavorable abemaciclib effect scenario. (B) Cost-effectiveness acceptability curve (CEAC) for abemaciclib all versus standard adjuvant endocrine treatment, for the unfavorable abemaciclib effect scenario. (C) CE-plane for the intermediate abemaciclib effect scenario. (D) CEAC for the intermediate abemaciclib effect scenario (E) CE-plane for the favorable abemaciclib effect scenario (F) CEAC for the favorable abemaciclib scenario. |
 |
Figure 6 Sensitivity analyses of MRD guided abemaciclib versus standard therapy. Abbreviation: QALY, quality adjusted life year. Notes: (A) CE-plane for the unfavorable effect scenario. (B) CE-plane for the intermediate effect scenario. (C) CE-plane for the favorable effect scenario. |
Figure 6 shows the PSA results for the comparison between “MRD-based abemaciclib” versus “standard treatment” for the different abemaciclib effect scenarios. MRD-based addition of abemaciclib will lead to an increase in QALYs in approximately 98% and savings of costs in 99% of the results of the PSA of most unfavorable scenario. This is indicated by results which are in the right lower quadrant.
Scenario Analyses Abemaciclib All versus Standard Treatment
Since the addition of abemaciclib was not cost effective according to the WTP of €50,000 for all abemaciclib effect scenarios, the necessary reduction in the price for abemaciclib to be cost-effective was calculated. Cost effectiveness according to a WTP of €50,000 was reached when the price of abemaciclib was reduced with at least 98.9%, 44.8% and 22.9%, respectively for the unfavorable, intermediate and favorable effect scenarios.
Scenario Analyses MRD Guided Abemaciclib versus Standard Treatment
A risk of MRD-guided abemaciclib is the fact that patients could develop recurrence of disease without preceding MRD detection. This chance was maximally 11% based on 2 trials which explored the clinical validity of MRD detection in patients with high risk EBC.7,8 When this risk of 11% was included in the model the MRD-guided abemaciclib treatment strategy still dominates standard treatment in the intermediate effect scenario, with a decrease in costs of €18,745 and a gain of 1.45 QALYs (Supplemental Table 1).
Discussion
To the best of our knowledge, this is the first study investigating the cost-effectiveness of adding two years of abemaciclib to adjuvant endocrine therapy in high risk ER+/HER2- EBC patients, expected to become the new treatment standard after the recent FDA and EMA approval. We find that the addition of abemaciclib in this group of patients (“abemaciclib all” strategy) is associated with a small gain in QALYs and results in substantial incremental costs compared to “standard treatment”. This resulted in an ICER of €86,632/QALY for the intermediate effect scenario, which is above the WTP threshold for high risk adjuvant EBC patients (€ 50,000/QALY). Even when assuming an extremely favorable abemaciclib effect, this did not result in “abemaciclib all” being cost-effective (ICER €62,935/QALY). To reach cost effectiveness in this favorable scenario still a 23% reduction in abemaciclib price is needed. Interestingly, using MRD detection to select patients in need of additional treatment to standard treatment and thereby reducing overtreatment in those patients without MRD improves the gain in QALYs (gain of 1.67 QALYs for the intermediate effect scenario compared to standard treatment). This gain in QALYs in combination with a reduction in costs (€28,936 in the intermediate effect scenario) results in the fact that the “MRD based abemaciclib” strategy dominates “standard treatment” in all three abemaciclib effect scenarios.
Currently, there seems to be a trend that expensive drugs, despite limited follow-up, are increasingly being approved by the FDA and EMA. While this may seem desirable from a patient’s perspective, early drug approval also carries risks.21,22 The addition of abemaciclib to endocrine treatment in high risk ER+/HER2- EBC patients might be an example of this phenomenon. The MonarchE study showed a significant improvement in iDFS of 5.4% after a median follow-up of 27 months in the group of patients treated with abemaciclib for two years compared to the group of patients which were treated with endocrine therapy alone. At the same time, in the Penelope-B study one year palbociclib was added to endocrine treatment, which resulted in a comparable improvement in iDFS of 4.3% after a median follow-up of 24 months in the palbociclib group.3 However, this improvement disappeared after a longer follow-up of 43 months, suggesting that the effect of adding a CDK4/6 inhibitor to adjuvant endocrine therapy postpones rather than prevents recurrences. On the one hand, this highlights the importance of a longer follow-up of studies in ER+ EBC patients, but it also emphasizes the importance of performing early health technology assessments for making approval decisions because of the potentially high impact of these new drugs on the budget for health care.23 Insight in the long term outcome of a treatment is, however, also important for cost-effectiveness analyses. Performing a cost-effectiveness analysis at this early stage therefore means that more assumptions have to be made, resulting in including multiple outcome scenarios in the analyses before conclusions can be drawn. In the current cost-effective analysis we incorporated three different abemaciclib effect scenarios, from an unfavorable to a highly favorable effect of abemaciclib on the long term, as a solution for the lack of long term outcome data. None of the scenarios however appeared to be cost-effective for the “abemaciclib all” treatment strategy. Even after performing probabilistic sensitivity analyses, in which the uncertainty of all individual parameters was taken into account, we found a low probability for all three effect scenarios that the “abemaciclib all” strategy was cost-effective at a WTP of €50,000 (probability of 0.1 for unfavorable effect scenario till 27.9% for favorable effect scenario).
An important phenomenon in the adjuvant treatment of ER+/HER- EBC in general is the high degree of overtreatment because a substantial part of the patients has already been cured by the breast surgery alone and does not need any form of adjuvant systemic treatment.24 An important step in reducing this overtreatment is a better identification of patients who will experience a recurrence, so that only those patients can be selected to receive adjuvant treatment. This selection could be performed by using MRD detection over time with ctDNA after surgery has taken place. Previous studies have shown that EBC patients in which MRD is detected by the presence of ctDNA in plasma have a very high risk to develop recurrence of disease.7,8 For example the study of Garcia Murillas et al8 which included 51 ER+/HER2- EBC patients in which plasma was analyzed for the presence of ctDNA every 6 months. In total 7 of the 12 patients in which ctDNA was detected relapsed, with a median lead time of 13.3 months. For the remaining 5 patients follow up was probably too short to detect a recurrence. At the same time none of the ctDNA negative patients relapsed. The median follow-up in this study was 35.5 months (IQR, 27.9–43.0 months). On the other hand in the study of Coombes et al7 two of the eighteen patients who experienced a recurrence had no detectable ctDNA on forehand. These patients will consequently not receive additional abemaciclib in the “MRD guided abemaciclib” strategy, while they would have received abemaciclib in the “abemaciclib all” strategy. We took the effect of this lack of treatment in these patients into account for the cost-effectiveness and found that, the “MRD based abemaciclib” strategy still results in a gain of QALYs and lower costs compared to the standard treatment strategy.
However, the clinical utility of using MRD detection over time as a preselection method in ER+ EBC patients needs to be proven in prospective studies. Interestingly, the first proof of clinical utility of using ctDNA detection in colorectal cancer patients to select patients for adjuvant treatment was recently published.25 This Phase 2 trial compared a ctDNA-guided approach with an approach based on standard clinico-pathological features for the selection of patients with stage 2 colorectal carcinoma for treatment with adjuvant chemotherapy. The ctDNA guided approach was non-inferior in terms of recurrence free survival compared to the standard treatment strategy and resulted in a lower rate of chemotherapy prescriptions. Performing these types of studies in EBC populations could have important implications for future adjuvant treatment strategies. Ideally, these future studies should gather the necessary data for cost effectiveness analysis (eg, extensive quality of life evaluations (EQ-5D) and resource use of patients). These studies should focus on the optimal interval of blood sampling and the optimal method of detecting ctDNA as well. Currently several methods are available to detect ctDNA with a high sensitivity.7,9 These methods will improve in terms of reliability and costs and new techniques will be developed in the coming years. In the model we presented here, we incorporate one of the currently available methods with the actual prices.8 The sensitivity, specificity and costs of the incorporated method will influence the outcomes of the analysis, resulting in more favorable ICERs when these ctDNA detection methods improve.
This study has some limitations. First, no data was available about the effect of CDK4/6 inhibitors specifically in patients with detected MRD. In this study the assumption was made that these effects were comparable with the effect in all high risk patients in the MonarchE trial. Potentially this is a underestimation of the real effect of the addition of abemaciclib in EBC patients with MRD detected since the studies of Coombes et al7 and Garcia-Murillas et al8 have shown that patients without detectable MRD have a highly favorable recurrence free survival curve. This makes it plausible that the improvement in iDFS for the addition of abemaciclib to endocrine treatment in the MonarchE trial originates for a large part from the EBC patients with MRD. Second, we used a duration of adjuvant endocrine treatment of five years, instead of prolonged endocrine treatment of 7 till 10 years which is indicated in this patient group, since only long term survival data of the treatment duration of 5 years is available for the high risk group, ER+/HER2- EBC in which we were interested. Consequently the costs in the recurrence free state will be underestimated however it will not have any effect on the comparison between the treatment strategies since we used this duration for all treatment strategies. Another potential limitation is the fact that we did not correct for the fact that the effect of abemaciclib in de recurrent disease state could be decreased when patients have already received abemaciclib in the adjuvant setting. In our model, life years were gained in the recurrent disease state of the abemaciclib all treatment strategy when an intermediate or favorable treatment effect was applied. No data is available yet about the impact of adjuvant abemaciclib on the length of recurrent disease when patients experience a recurrence. It is not expected that this will prolong the duration of recurrent disease, so this gain in years of recurrent disease is probably an overestimation of the effect on OS of abemaciclib and results in a lower ICER than the actual ICER in both the “abemaciclib all” and “MRD based abemaciclib” scenario.
This study also has several strengths. First, conducting this economic evaluation in an early phase could give important insight in the consequences of implementing abemaciclib in the adjuvant setting of ER+/HER2- EBC in terms of costs and QALYs for EBC patients. Second, the incorporation of three effect scenarios of abemaciclib, from unfavorable to a highly favorable abemaciclib effect in terms of iDFS and OS, in which different assumptions were made about the long-term treatment effect made the results more reliable. Of course, uncertainty remains but even when extreme assumptions were implemented, most conclusions were not altered.
Conclusion
The addition of abemaciclib in all high-risk ER+HER2- early breast cancer patients is not cost-effective based on abemaciclib effectiveness data from the MonarchE study. Even highly favorable abemaciclib effect scenarios did not led to cost-effectiveness whereby even in the most favorable abemaciclib effect scenario an unlikely price reduction of abemaciclib of 23% is needed to reach cost-effectiveness. Adequate patient selection by using MRD detection over time may lead to cost-effectiveness of abemaciclib in the adjuvant setting. This cost-effectiveness analysis, conducted in an early phase, showed that further evaluation of MRD detection in EBC by using prospective clinical trials assessing the clinical utility is highly recommended and promising in terms of cost-effectivity.
Acknowledgments
The authors thank the registration team of the Netherlands Comprehensive Cancer Organisation (IKNL) for the collection of data for the Netherlands Cancer Registry’. This paper was presented at the “13th European Breast Cancer Conference” as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in European Journal of Cancer: https://www.ejcancer.com/article/S0959-8049(22)01511-8/fulltext.
Disclosure
Dr Hedwig M Blommestein reports fees from Pfizer BV paid to institute for participation in advisory board, outside the submitted work. Prof. Dr. John WM Martens reports grants from Dutch Cancer Society, during the conduct of the study; research grants from Eurostar, KWF, Roche, ZonMW, Pfizer, GSK, Oncode, NWO, MLDS, and Daniel den Hood Foundation; personal fees from Novartis for ctDNA assay recommendation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Eng J Med. 2017;377(19):1836–1846. doi:10.1056/NEJMoa1701830
2. Early Breast Cancer Trialists’ Collaborative G. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. doi:10.1016/S0140-6736(05)66544-0
3. Loibl S, Marmé F, Martin M, et al. Palbociclib for Residual High-Risk Invasive HR-Positive and HER2-Negative Early Breast Cancer-The Penelope-B Trial. J Clin Oncol. 2021;39(14):1518–1530. doi:10.1200/JCO.20.03639
4. Mayer EL, Dueck AC, Martin M, et al. Palbociclib with adjuvant endocrine therapy in early breast cancer (PALLAS): interim analysis of a multicentre, open-label, randomised, Phase 3 study. Lancet Oncol. 2021;22(2):212–222. doi:10.1016/S1470-2045(20)30642-2
5. Johnston SRD, Harbeck N, Hegg R, et al. Abemaciclib Combined With Endocrine Therapy for the Adjuvant Treatment of HR+, HER2-, Node-Positive, High-Risk, Early Breast Cancer (monarchE). J Clin Oncol. 2020;38(34):3987–3998. doi:10.1200/JCO.20.02514
6. Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32(12):1571–1581. doi:10.1016/j.annonc.2021.09.015
7. Coombes RC, Page K, Salari R, et al. Personalized Detection of Circulating Tumor DNA Antedates Breast Cancer Metastatic Recurrence. Clin Cancer Res. 2019;25(14):4255–4263. doi:10.1158/1078-0432.CCR-18-3663
8. Garcia-Murillas I, Chopra N, Comino-Mendez I, et al. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. JAMA Oncol. 2019;5(10):1473–1478. doi:10.1001/jamaoncol.2019.1838
9. Garcia-Murillas I, Schiavon G, Weigelt B, et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci Transl Med. 2015;7(302):302ra133. doi:10.1126/scitranslmed.aab0021
10. Netherlands Cancer Registry (NCR) NCCOI. Available from: www.iknl.nl/en/ncr/ncr-data-figures.
11. Versteegh M, Knies S, Brouwer W. From Good to Better: new Dutch Guidelines for Economic Evaluations in Healthcare. Pharmacoeconomics. 2016;34(11):1071–1074. doi:10.1007/s40273-016-0431-y
12. Sledge GW, Toi M, Neven P, et al. The Effect of Abemaciclib Plus Fulvestrant on Overall Survival in Hormone Receptor–Positive, ERBB2-Negative Breast Cancer That Progressed on Endocrine Therapy—MONARCH 2: a Randomized Clinical Trial. JAMA Oncol. 2020;6(1):116–124. doi:10.1001/jamaoncol.2019.4782
13. Central Bureau for Statistics. 2021.
14. Rautalin M, Färkkilä N, Sintonen H, et al. Health-related quality of life in different states of breast cancer - comparing different instruments. Acta Oncol. 2018;57(5):622–628. doi:10.1080/0284186X.2017.1400683
15. Uyl-de Groot C, Zaim R. Nivolumab (Opdivo) bij Gevorderd Plaveiselcelcarcinoom van de Long. Instituut Beleid Manage Gezondheidszorg. 2015;1:548.
16. Bullement A, Nathan P, Willis A, et al. Cost effectiveness of avelumab for metastatic Merkel cell carcinoma. Pharmacoeconomics-Open. 2019;3(3):377–390. doi:10.1007/s41669-018-0115-y
17. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(8):1194–1220. doi:10.1093/annonc/mdz173
18. Hakkaart-van Roijen L, Van der Linden N, Bouwmans C, Kanters T, Tan SS Kostenhandleiding. Methodologie van kostenonderzoek en referentieprijzen voor economische evaluaties in de gezondheidszorg In opdracht van Zorginstituut Nederland Geactualiseerde versie. 2015.
19. Koopmanschap MA, Rutten FFH, van Ineveld BM, Van Roijen L. The friction cost method for measuring indirect costs of disease. J Health Econ. 1995;14(2):171–189. doi:10.1016/0167-6296(94)00044-5
20. Versteegh MM, Ramos IC, Buyukkaramikli NC, Ansaripour A, Reckers-Droog VT, Brouwer WBF. Severity-adjusted probability of being cost effective. Pharmacoeconomics. 2019;37(9):1155–1163. doi:10.1007/s40273-019-00810-8
21. Prasad V, Kim C, Burotto M, Vandross A. The Strength of Association Between Surrogate End Points and Survival in Oncology: a Systematic Review of Trial-Level Meta-analyses. JAMA Intern Med. 2015;175(8):1389–1398. doi:10.1001/jamainternmed.2015.2829
22. Frakt AB, Risks T. Benefits of Expedited Drug Reviews. JAMA. 2018;320(3):225–226. doi:10.1001/jama.2018.8262
23. Ling DI, Lynd LD, Harrison M, Anis AH, Bansback N. Early cost-effectiveness modeling for better decisions in public research investment of personalized medicine technologies. J Comp Eff Res. 2019;8(1):7–19. doi:10.2217/cer-2018-0033
24. Ragusi MAA, van der Velden BHM, van Maaren MC, et al. Population-based estimates of overtreatment with adjuvant systemic therapy in early breast cancer patients with data from the Netherlands and the USA. Breast Cancer Res Treat. 2022;193(1):161–173. doi:10.1007/s10549-022-06550-2
25. Tie J, Cohen JD, Lahouel K, et al. Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. N Eng J Med. 2022;386(24):2261–2272. doi:10.1056/NEJMoa2200075
26. Specialisten FM Richtenlijnendatabase. Borstkanker - Endocriene therapie; 2021.
27. Braal CL, Kleiburg A, Jager A, et al. Therapeutic Drug Monitoring-guided adjuvant tamoxifen dosing in early breast cancer patients: a cost-effectiveness analysis from the prospective TOTAM trial. Clin Drug Investigation. 2021;42(2):163.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.