Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Baseline Sleep Quality and Objective Response in HCC Patients Treated with TACE Combined with Lenvatinib and PD-1 Inhibitors: A Secondary Analysis of a Prospectively Registered Observational Cohort
Authors Tian P ![]() , Zhao H, Sun W, Peng Q, Luo Y
, Zhao H, Sun W, Peng Q, Luo Y ![]() , Sang M, Xi J, Song HY, Yang Z
, Sang M, Xi J, Song HY, Yang Z
Received 12 March 2026
Accepted for publication 30 May 2026
Published 29 June 2026 Volume 2026:13 600627
DOI https://doi.org/10.2147/JHC.S600627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Pengfei Tian,1,* He Zhao,1,* Wei Sun,1 Qing Peng,1 Yingen Luo,1 Mingchen Sang,1 Junqing Xi,1 Ho-Young Song,2 Zhengqiang Yang1
1Department of Interventional Therapy, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Interventional Radiology, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ho-Young Song; Zhengqiang Yang, Email [email protected]; [email protected]
Background: Sleep disturbance is common in patients with cancer and may reflect host immune, inflammatory, and symptom states relevant to treatment response. In hepatocellular carcinoma (HCC), whether baseline sleep quality is associated with objective response among patients receiving transarterial chemoembolization (TACE) combined with lenvatinib and PD-1 inhibitors remains uncertain.
Methods: We conducted a secondary analysis of a prospectively registered observational HCC cohort in the Chinese Clinical Trial Registry. Consecutive patients in the cohort who were treated with TACE plus lenvatinib and PD-1 inhibitors were screened; 129 patients with available baseline Pittsburgh Sleep Quality Index (PSQI), Hospital Anxiety and Depression Scale (HADS), and response data were included. Objective response rate (ORR) was assessed using modified Response Evaluation Criteria in Solid Tumors (mRECIST). Multivariable logistic regression adjusted for age, sex, ECOG performance status, ALBI grade, maximum tumor diameter, tumor number, and portal vein tumor thrombosis. Unstabilized inverse-probability complete-case weighting and multiple imputation were used as sensitivity analyses.
Results: The mean age was 60.9 years, 94 patients (72.9%) were male, and 64 of 129 patients (49.6%) achieved ORR. Responders had better baseline sleep quality than non-responders (mean PSQI 4.14 vs 7.94; p< 0.001). After adjustment, each 1-point increase in PSQI was associated with lower odds of ORR (OR 0.62, 95% CI 0.48– 0.75; p< 0.001). The association was similar after inverse-probability weighting (OR 0.63, 95% CI 0.52– 0.75; p< 0.001) and multiple imputation (OR 0.66, 95% CI 0.55– 0.79; p< 0.001). Baseline HADS-Anxiety and HADS-Depression scores were not independently associated with ORR.
Conclusion: Poorer baseline sleep quality was independently associated with a lower probability of objective response in HCC patients treated with TACE plus lenvatinib and PD-1 inhibitors. PSQI may be a feasible baseline risk-stratification tool in this setting, but causal inference is limited and prospective validation is required before sleep-directed interventions can be expected to improve tumor response.
Keywords: hepatocellular carcinoma, sleep quality, anxiety, depression, immunotherapy, transarterial chemoembolization, objective response
Introduction
Hepatocellular carcinoma (HCC) remains a leading cause of cancer-related mortality worldwide.1,2 For patients who are not candidates for curative therapy, combination strategies integrating TACE, tyrosine kinase inhibitors such as lenvatinib, and PD-1 inhibitors have become increasingly important, with clinical studies reporting meaningful response and survival benefits.3,4 However, objective response remains heterogeneous even among patients with similar tumor burden, liver function, and performance status. Recent studies also continue to identify molecular, clinicopathologic, and immune-related determinants of HCC behavior, underscoring the need to explore additional factors associated with treatment response.5–8
Sleep disturbance is highly prevalent among patients with cancer and has been associated with impaired quality of life and adverse outcomes.9,10 Anxiety and depressive symptoms often co-occur with sleep problems,11 but sleep quality and psychological distress are not interchangeable constructs. Sleep and circadian regulation can affect immune signaling, inflammatory pathways, neuroendocrine function, and immune checkpoint activity, all of which may be relevant to immunotherapy efficacy and cancer-treatment outcomes.12–19
Evidence specific to HCC patients receiving contemporary TACE plus lenvatinib plus PD-1 inhibitor therapy is limited. Most previous work has emphasized survival endpoints or general symptom burden rather than objective tumor response, and few studies have evaluated sleep quality, anxiety, and depression within the same cohort. We therefore examined whether baseline sleep quality, measured using PSQI, was associated with ORR in this treatment setting. We also examined HADS-Anxiety and HADS-Depression scores, tested sleep-distress interaction, and assessed robustness using DCR and sensitivity analyses.
Methods
Study Design and Participants
The parent observational cohort was prospectively registered in the Chinese Clinical Trial Registry (ChiCTR2200056326). The present study was designed as a secondary analysis of available baseline questionnaire, clinical, laboratory, and first post-treatment imaging response data recorded in this cohort. Consecutive patients with HCC who received TACE plus lenvatinib and PD-1 inhibitors were screened. Patients were eligible if they had HCC diagnosed according to accepted clinical or pathological criteria, received the combination regimen, had baseline PSQI and HADS assessments before or at treatment initiation, and had evaluable radiologic response data. Patients were excluded if response data, baseline sleep/psychological assessments, or key analysis variables were unavailable. The selection process is shown in Figure 1.
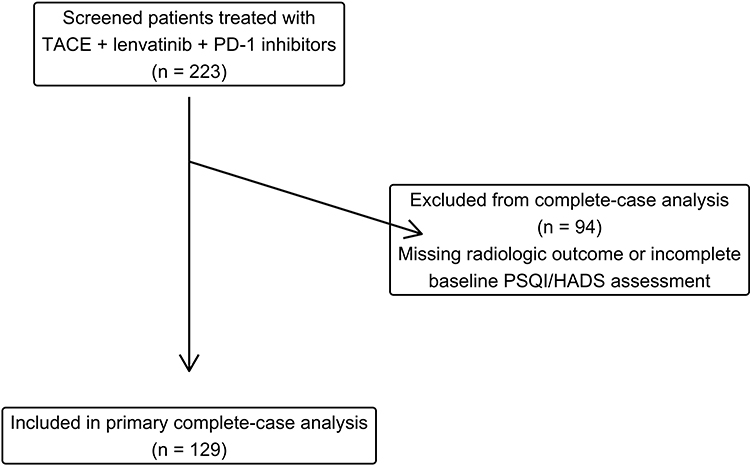 |
Figure 1 Flowchart of patient enrollment and selection. A total of 223 patients treated with TACE plus lenvatinib and PD-1 inhibitors were screened. Ninety-four were excluded because radiologic response data or baseline PSQI/Hads assessment data were unavailable, leaving 129 patients for the primary complete-case analysis. |
Data Collection
Demographic variables, clinical characteristics, liver function indices, tumor burden, portal vein tumor thrombosis (PVTT), laboratory values, baseline PSQI/HADS scores, and treatment response were extracted from institutional clinical records and research datasets. Data were checked for consistency before analysis. Independent pain scores and detailed concomitant analgesic, sedative, or hypnotic medication records were not available in the analytic dataset. The PSQI sleep-medication component was available but was not treated as a substitute for a formal concomitant medication record.
Exposure Assessment
Baseline sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI), a widely used instrument for assessing sleep quality.20 PSQI was analyzed continuously per 1-point increase and categorically using PSQI ≥5 to indicate poor sleep quality, consistent with the conventional cutoff used to identify poor sleepers. Anxiety and depression were assessed using HADS.21 HADS-Anxiety and HADS-Depression were analyzed continuously and using a cutoff of ≥8. Although HADS can also be reported as <8, 8–10, and ≥11, the ≥8 cutoff was selected a priori to capture borderline or clinically relevant symptoms while preserving statistical power in this cohort. We additionally reported three-category HADS distributions descriptively.
Outcome Assessment
The primary endpoint was ORR, defined as complete response or partial response according to mRECIST.22 Response was assessed at the first post-treatment radiologic assessment per institutional practice using contrast-enhanced CT or MRI when available in the clinical record. The source dataset did not contain uniform treatment-initiation and confirmatory imaging dates that would support a reliable X-to-Y-week assessment window; therefore, no unsupported standardized confirmatory time point was added. Patients without adequate measurable disease or evaluable post-treatment response data were excluded from the primary complete-case analysis. DCR, defined as complete response, partial response, or stable disease versus progressive disease, was evaluated as a secondary endpoint.
Covariates
Prespecified covariates were selected based on clinical relevance and included age, sex, ECOG performance status, ALBI grade, maximum tumor diameter, tumor number, and PVTT. These variables reflect major determinants of HCC treatment response, including liver function, tumor burden, vascular invasion, and general functional status.
Statistical Analysis
Baseline characteristics are summarized as mean (SD), median (IQR), or n (%) as appropriate and were stratified by ORR status. Standardized mean differences (SMDs) were calculated to quantify between-group differences. Associations of PSQI, HADS-Anxiety, and HADS-Depression with ORR were examined using logistic regression. The primary multivariable model included all three psychosocial measures and the prespecified clinical covariates. A predicted probability curve was generated from the multivariable model to visualize the adjusted association between PSQI and ORR.
Sensitivity Analyses
To evaluate the potential influence of complete-case selection, unstabilized inverse-probability complete-case weights were estimated using logistic regression for the probability of complete-case inclusion among screened records. The weight model included age, sex, ECOG performance status, ALBI grade, Child-Pugh class, maximum tumor diameter, tumor number, PVTT, extrahepatic metastasis, platelet count, albumin, and total bilirubin. Weights were calculated as 1 divided by the predicted probability of complete-case inclusion and truncated at the 1st and 99th percentiles. The complete-case weight model was inspected using the predicted probability distribution, C statistic, Brier score, calibration intercept and slope, Hosmer-Lemeshow decile calibration, and post-weighting covariate balance; it was not used as a causal exposure propensity-score model. The weighted ORR model used robust HC0 standard errors. Balance was assessed using SMDs and effective sample size. Multiple imputation by chained equations with 20 imputed datasets and 20 iterations was also performed as a sensitivity analysis using ORR, PSQI, HADS-A, HADS-D, age, sex, ECOG performance status, ALBI grade, maximum tumor diameter, tumor number, and PVTT. Because 94 screened patients lacked outcome and baseline sleep/psychological assessment data simultaneously, imputation results were interpreted as sensitivity evidence rather than replacing the complete-case primary analysis.
Software and Ethics
All analyses were performed using R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided p values <0.05 were considered statistically significant. The study was approved by the Institutional Review Board of Cancer Hospital, Chinese Academy of Medical Sciences (identifier: 21/402-3073). Informed consent was waived because of the observational design and use of existing clinical data. Patient confidentiality was protected during data extraction and analysis, and the study was conducted in accordance with the Declaration of Helsinki. Data are available from the corresponding author upon reasonable request.
Results
Patient Selection
A total of 223 screened records were identified, and 129 patients with complete baseline PSQI, HADS, and response data were included in the primary analysis (Figure 1). Ninety-four screened records were excluded because radiologic response data or baseline sleep/psychological assessment data were unavailable.
Baseline Characteristics
The mean age of the included patients was 60.90 years (SD 10.27), and 94 patients (72.9%) were male. Baseline characteristics stratified by ORR status are shown in Table 1. Patients who achieved ORR had markedly better baseline sleep quality than those who did not achieve ORR, with mean PSQI scores of 4.14 (SD 2.25) versus 7.94 (SD 4.71), respectively (p<0.001; SMD 1.030). HADS-Anxiety and HADS-Depression scores were numerically lower among responders but did not differ significantly.
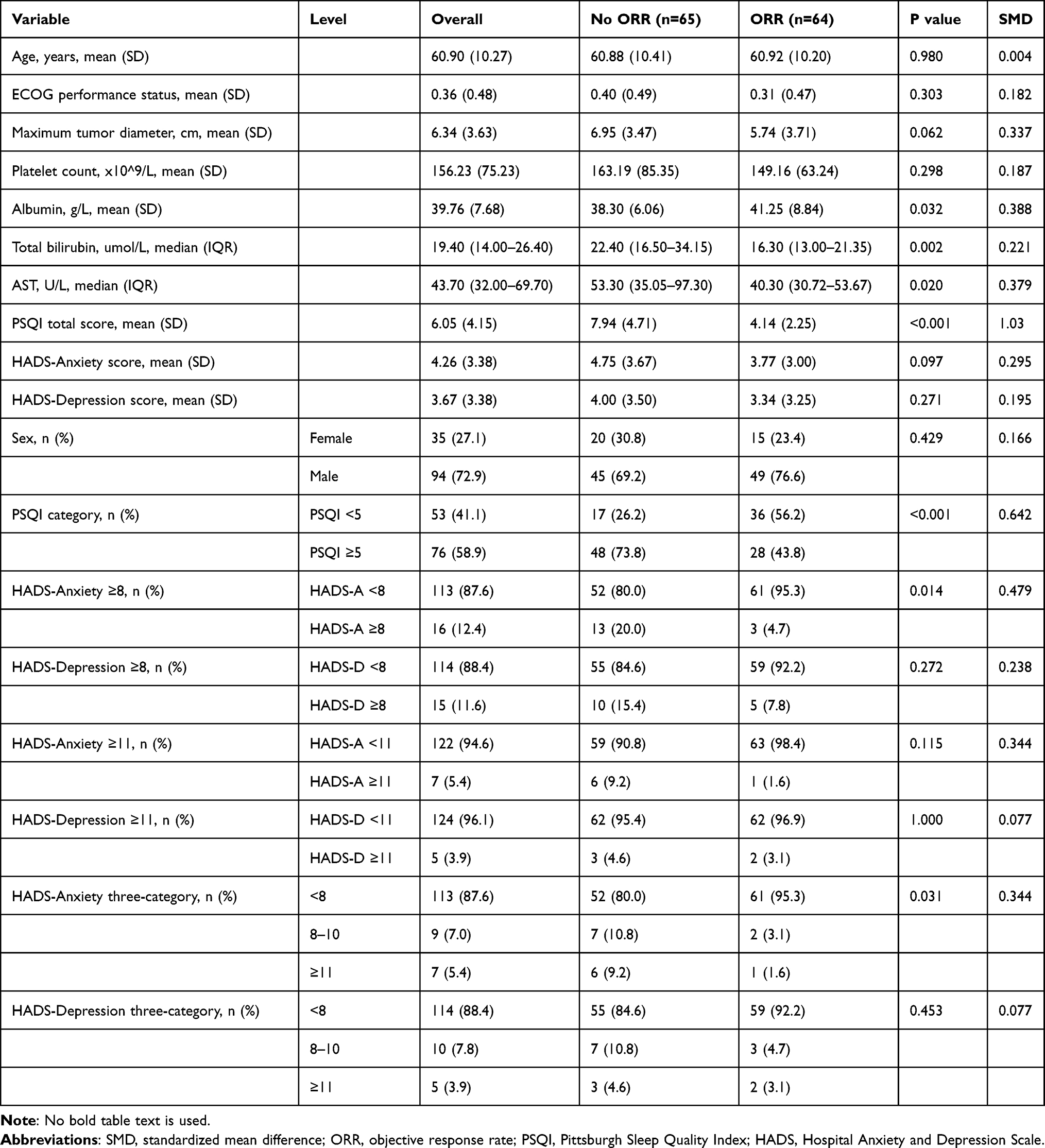 |
Table 1 Baseline Characteristics of the Study Population Overall and Stratified by ORR |
Using established thresholds, 76 patients (58.9%) had PSQI ≥5. Clinically relevant anxiety (HADS-Anxiety ≥8) was present in 16 patients (12.4%), and clinically relevant depression (HADS-Depression ≥8) in 15 patients (11.6%). When HADS was described using three categories, only 7 patients (5.4%) had HADS-Anxiety ≥11 and 5 patients (3.9%) had HADS-Depression ≥11, supporting the use of the ≥8 cutoff for the primary categorical analyses.
Primary ORR Analysis
Associations between PSQI, HADS-Anxiety, HADS-Depression and ORR are shown in Table 2. In unadjusted analysis, each 1-point increase in PSQI was associated with lower odds of ORR (OR 0.73, 95% CI 0.62–0.83). After adjustment for clinical covariates, PSQI remained independently associated with ORR (OR 0.62, 95% CI 0.48–0.75; p<0.001). HADS-Anxiety (OR 1.06, 95% CI 0.87–1.30; p=0.536) and HADS-Depression (OR 1.06, 95% CI 0.89–1.27; p=0.537) were not independently associated with ORR. A forest plot and PSQI probability curve are shown in Figure 2, and the full complete-case multivariable model is provided in Supplementary Table S1.
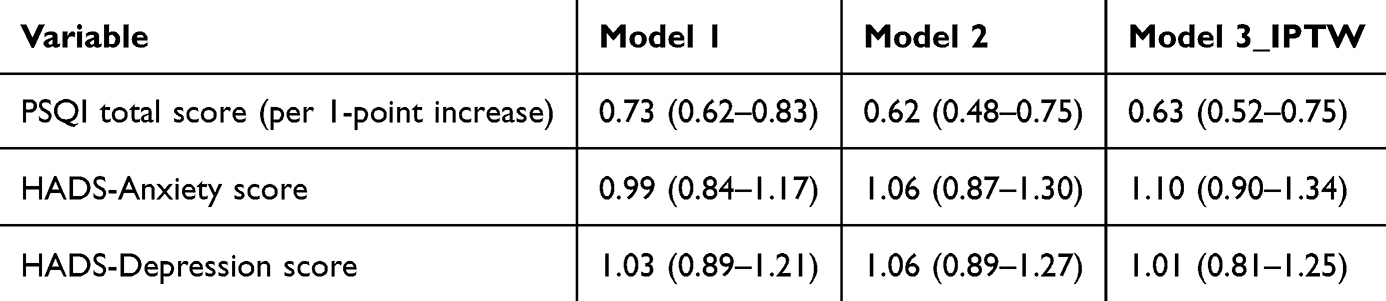 |
Table 2 Associations of PSQI and HADS Scores with Objective Response Rate |
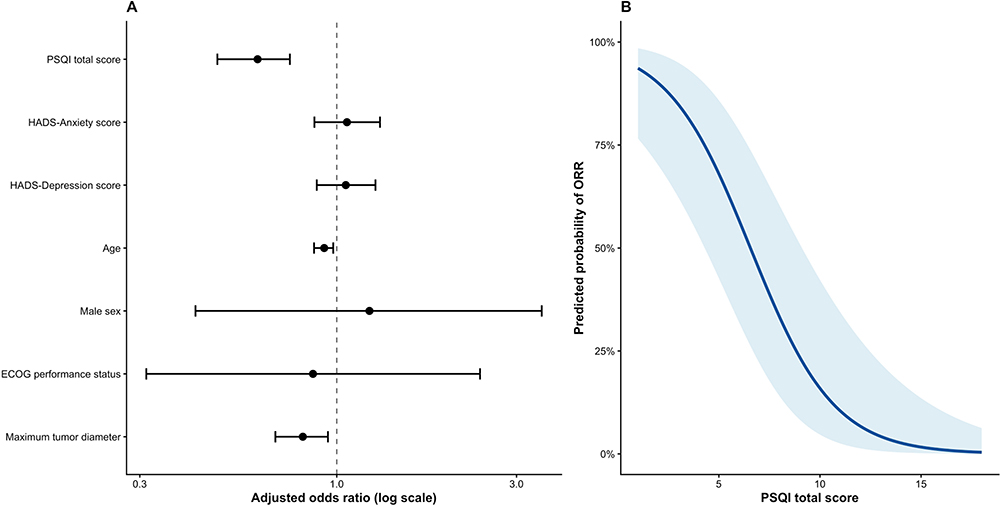 |
Figure 2 Multivariable-adjusted associations between psychosocial measures and ORR. (A) shows adjusted odds ratios and 95% confidence intervals for selected variables in the multivariable logistic regression model. (B) shows the modeled relationship between PSQI total score and predicted probability of ORR, with other covariates fixed at representative values. |
Sensitivity Analyses
The inverse-probability complete-case weighted analysis yielded similar results. PSQI remained significantly associated with ORR (OR 0.63, 95% CI 0.52–0.75; p<0.001), whereas HADS-Anxiety and HADS-Depression remained non-significant. Full weighted model estimates are shown in Supplementary Table S2. The complete-case probability model used 206 screened records, and 124 complete-case records had estimated weights. Model inspection showed a C statistic of 0.794, Brier score of 0.179, calibration intercept of −0.000, calibration slope of 1.000, and Hosmer-Lemeshow p value of 0.101. After 1st/99th percentile truncation, the effective sample size was 100.8. Most weighted SMDs improved compared with unweighted SMDs, although some residual imbalance remained for sex and tumor number (Supplementary Table S3).
Multiple imputation also supported the primary finding. In the pooled imputed analysis, PSQI remained associated with lower odds of ORR (OR 0.66, 95% CI 0.55–0.79; p<0.001), while HADS-Anxiety (OR 1.05, 95% CI 0.88–1.25; p=0.590) and HADS-Depression (OR 1.04, 95% CI 0.87–1.25; p=0.631) were not significant (Supplementary Table S4).
Interaction Analysis
The interaction model evaluating poor sleep and psychological distress is shown in Table 3. Poor sleep was associated with lower odds of ORR (OR 0.31, 95% CI 0.14–0.68; p=0.004). Psychological distress alone was not significantly associated with ORR (OR 0.44, 95% CI 0.05–3.96; p=0.434), and the interaction term was not significant (p=0.944). Figure 3 displays the joint exposure estimates.
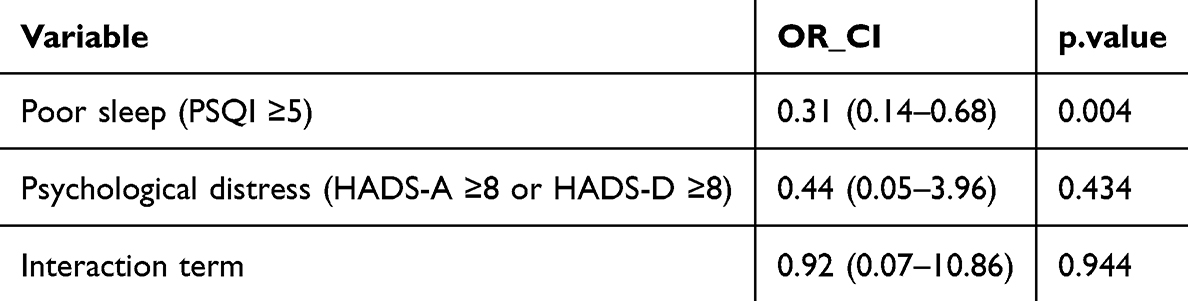 |
Table 3 Interaction Analysis of Poor Sleep Quality and Psychological Distress in Relation to ORR |
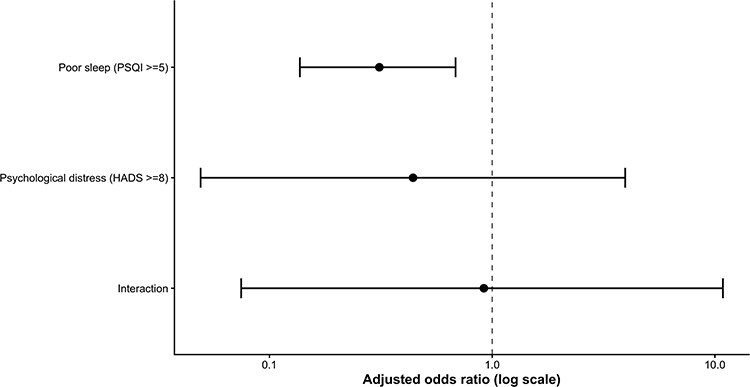 |
Figure 3 Joint exposure analysis evaluating poor sleep quality (PSQI ≥5), psychological distress (Hads-Anxiety ≥8 or HADS-Depression ≥8), and their interaction in relation to ORR. |
DCR Analysis
For DCR, PSQI showed the same general direction of association. In the multivariable DCR model using continuous psychosocial scores, higher PSQI was associated with lower odds of DCR (OR 0.60, 95% CI 0.47–0.77; p<0.001). In the separate threshold-based DCR model, PSQI ≥5 was also associated with lower odds of DCR (OR 0.13, 95% CI 0.02–0.73; p=0.020), whereas HADS threshold estimates remained non-significant (Supplementary Tables S5 and S6). These secondary analyses should be interpreted as supportive but exploratory.
Exploratory biomarker comparisons by sleep quality and psychological distress categories are shown in Supplementary Figure S1. These exploratory comparisons are presented for hypothesis generation and were not used for primary inference.
Discussion
In this cohort of HCC patients treated with TACE plus lenvatinib and PD-1 inhibitors, poorer baseline sleep quality was consistently associated with a lower probability of objective response. The association persisted after adjustment for major HCC prognostic factors, after inverse-probability complete-case weighting, and in multiple-imputation sensitivity analysis. In contrast, baseline anxiety and depression were not independently associated with ORR after adjustment.
The stability of the PSQI association suggests that baseline sleep quality may capture a clinically relevant host state not fully represented by tumor burden, liver function, or performance status. Sleep disturbance may reflect symptom burden, inflammatory activation, circadian disruption, or immune-metabolic vulnerability. These pathways are biologically plausible in the setting of PD-1 blockade, where antitumor efficacy depends on immune activation and sustained effector function.
The lack of independent HADS associations requires careful interpretation. Clinically relevant anxiety and depression were uncommon in this cohort, and high HADS scores were particularly rare: HADS-Anxiety ≥11 occurred in 7 patients and HADS-Depression ≥11 in 5 patients. This limited statistical power for categorical HADS analyses and may explain why crude subgroup differences did not persist after clinical adjustment. Sleep quality and psychological distress are related but distinct; PSQI may be more proximal to physiologic processes involved in treatment response than baseline anxiety or depression scores alone.
Our findings should also be interpreted in the context of mixed and still-developing evidence across cancer types. Circadian and sleep disruption have been linked to immune function and immunotherapy outcomes in some studies, but available evidence is heterogeneous and often indirect. Therefore, the present results should be viewed as hypothesis-generating rather than proof that modifying sleep will improve tumor response.
Clinically, PSQI is brief, low-cost, and feasible to administer before combination therapy. If validated, it could help identify patients who may require closer monitoring or supportive care. However, sleep improvement has established value for quality of life and symptom control; it remains unproven that sleep-directed interventions improve ORR. We have revised the interpretation accordingly to avoid causal overstatement.
This study has limitations. First, the single-center design and secondary-analysis approach may limit generalizability. Second, 94 screened records lacked response and baseline sleep/psychological assessment data, and complete-case selection may introduce bias. We addressed this with inverse-probability complete-case weighting and multiple imputation, but residual bias cannot be excluded. Third, independent pain scores and detailed concomitant analgesic, sedative, or hypnotic medication records were unavailable, leaving potential unmeasured confounding. Fourth, ORR was assessed at the first post-treatment radiologic assessment per institutional practice, and the available dataset did not include uniform confirmatory assessment time points or sufficient date fields to calculate a consistent X-to-Y-week imaging window. Fifth, PSQI and HADS were self-reported baseline measures, and longitudinal changes were not assessed. Finally, DCR and biomarker analyses were exploratory and should not be overinterpreted.
Future multicenter prospective studies should validate whether PSQI adds predictive value beyond standard HCC clinical factors, collect serial sleep and psychological assessments, standardize radiologic assessment timing, and include pain, medication, and adherence data. Interventional trials would be needed to determine whether sleep optimization can improve tumor response or other oncologic outcomes.
Conclusions
Poorer baseline sleep quality was independently associated with reduced odds of objective response in HCC patients treated with TACE plus lenvatinib and PD-1 inhibitors, whereas baseline anxiety and depression were not independently associated with ORR. PSQI may be a feasible baseline risk-stratification tool in this population, but causality cannot be inferred from these observational data. Prospective studies are needed to validate these findings and determine whether sleep-targeted supportive care can influence treatment outcomes.
Funding
This research was funded by the Foreign Expert Project of the Ministry of Science and Technology of China (Grant NO. G2023026016L) and the National High Level Hospital Clinical Research Funding (2025-LYZX-Z-B04).
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–9. doi:10.3322/caac.21834
2. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
3. Llovet JM, Kelley RK, Villanueva A, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, Phase 3 study. Lancet. 2025;405(10474):203–215. doi:10.1016/S0140-6736(24)02575-3
4. Qu S, Zhang X, Wu Y, et al. Efficacy and safety of TACE combined with lenvatinib plus PD-1 inhibitors compared with TACE alone for unresectable hepatocellular carcinoma patients: a prospective cohort study. Front Oncol. 2022;12:874473. doi:10.3389/fonc.2022.874473
5. Xu W, Liao S, Hu Y, Huang Y, Zhou J. Upregulation of miR-3130-5p enhances hepatocellular carcinoma growth by suppressing ferredoxin 1: miR-3130-5p enhances HCC growth via inhibiting FDX1. Curr Mol Pharmacol. 2024;17:e18761429358008. doi:10.2174/0118761429358008250305070518
6. Gudivada IP, Amajala KC. Integrative bioinformatics analysis for targeting hub genes in hepatocellular carcinoma treatment. Curr Genom. 2025;26(1):48–80. doi:10.2174/0113892029308243240709073945
7. Ye W, Wang J, Zheng J, Jiang M, Zhou Y, Wu Z. Association between higher expression of Vav1 in hepatocellular carcinoma and unfavourable clinicopathological features and prognosis. Protein Pept Lett. 2024;31(9):706–713. doi:10.2174/0109298665330781240830042601
8. Sensi B, Angelico R, Toti L, et al. Mechanism, potential, and concerns of immunotherapy for hepatocellular carcinoma and liver transplantation. Curr Mol Pharmacol. 2024;17:e18761429310703. doi:10.2174/0118761429310703240823045808
9. Al Maqbali M, Al Sinani M, Alsayed A, Gleason AM. Prevalence of sleep disturbance in patients with cancer: a systematic review and meta-analysis. Clin Nurs Res. 2022;31(6):1107–1123. doi:10.1177/10547738221092146
10. Chen MY, Zheng WY, Liu YF, et al. Global prevalence of poor sleep quality in cancer patients: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2024;87:92–102. doi:10.1016/j.genhosppsych.2023.12.004
11. Irwin MR. Depression and insomnia in cancer: prevalence, risk factors, and effects on cancer outcomes. Curr Psychiatry Rep. 2013;15(11):404. doi:10.1007/s11920-013-0404-1
12. Karaboue A, Innominato PF, Wreglesworth NI, Duchemann B, Adam R, Levi FA. Why does circadian timing of administration matter for immune checkpoint inhibitors’ efficacy? Br J Cancer. 2024;131(5):783–796. doi:10.1038/s41416-024-02704-9
13. Fortin BM, Pfeiffer SM, Insua-Rodriguez J, et al. Circadian control of tumor immunosuppression affects efficacy of immune checkpoint blockade. Nat Immunol. 2024;25(7):1257–1269. doi:10.1038/s41590-024-01859-0
14. Qian DC, Kleber T, Brammer B, et al. Effect of immunotherapy time-of-day infusion on overall survival among patients with advanced melanoma in the USA (MEMOIR): a propensity score-matched analysis of a single-centre, longitudinal study. Lancet Oncol. 2021;22(12):1777–1786. doi:10.1016/S1470-2045(21)00546-5
15. Karaboue A, Collon T, Pavese I, et al. Time-dependent efficacy of checkpoint inhibitor nivolumab: results from a pilot study in patients with metastatic non-small-cell lung cancer. Cancers. 2022;14(4):896. doi:10.3390/cancers14040896
16. Li X, Huang D, Liu F, et al. Sleep characteristics and cancer-related outcomes: an umbrella review of systematic reviews and meta-analyses of observational studies. J Clin Med. 2022;11(24):7289. doi:10.3390/jcm11247289
17. Balachandran DD, Bashoura L, Sheshadri A, Manzullo E, Faiz SA. The impact of immunotherapy on sleep and circadian rhythms in patients with cancer. Front Oncol. 2023;13:1295267. doi:10.3389/fonc.2023.1295267
18. Coleman M, Mascialino SJ, Panjwani A, et al. Readily available drugs and other interventions to potentially improve the efficacy of immune checkpoint blockade in cancer. Front Immunol. 2024;14:1281744. doi:10.3389/fimmu.2023.1281744
19. Strom L, Danielsen JT, Amidi A, Cardenas Egusquiza AL, Wu LM, Zachariae R. Sleep during oncological treatment: a systematic review and meta-analysis of associations with treatment response, time to progression and survival. Front Neurosci. 2022;16:817837. doi:10.3389/fnins.2022.817837
20. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
21. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
22. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
The Influence of Drug-Eluting Beads Transarterial Chemoembolization on Serum Levels of Soluble Programmed Cell Death Protein-1 in Advanced Hepatocellular Carcinoma Patients
Ma X, Sun X, Xie F, Jian W, Wang Q, Xie Y, Li C, Zhang K
Journal of Hepatocellular Carcinoma 2024, 11:619-628
Published Date: 25 March 2024
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
Association Between Depression, Anxiety, and Stress and Sleep Quality Among University Students from Saudi Arabia: A Cross-Sectional Study
Gosadi IM, Shnaimer JA
Psychology Research and Behavior Management 2025, 18:2287-2298
Published Date: 14 November 2025