Back to Journals » Nature and Science of Sleep » Volume 15
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Authors Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W ![]()
Received 6 February 2023
Accepted for publication 17 May 2023
Published 26 May 2023 Volume 2023:15 Pages 407—421
DOI https://doi.org/10.2147/NSS.S407388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Rong Yu,1,* Chuan Liu,1,* Jixiang Zhang,1,* Jiao Li,1,* Shan Tian,2 Fugui Ding,1 Zhengru Liu,3 Ting Wang,4 Zhongchun Liu,5 Changqing Jiang,6 Jie Shi,7 Kaichun Wu,8 Weiguo Dong1
1Department of Gastroenterology, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 2Department of Infectious Diseases, Union Hospital of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430000, People’s Republic of China; 3Department of Gastroenterology, First Affiliated Hospital of Kunming Medical University, Kunming, 650032, People’s Republic of China; 4Department of Gastroenterology, First Affiliated Hospital of Hainan Medical College, Haikou, 570102, People’s Republic of China; 5Department of Psychiatry, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 6Department of Clinical Psychology, Beijing Anding Hospital, Capital Medical University, Beijing, 100088, People’s Republic of China; 7Department of Medical Psychology, Chinese People’s Liberation Army Rocket Army Characteristic Medical Center, Beijing, 100088, People’s Republic of China; 8Department of Gastroenterology, Xijing Hospital, Air Force Medical University, Xi’an, 710032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weiguo Dong, Department of Gastroenterology, Renmin Hospital of Wuhan University, No. 99 Zhangzhidong Road, Wuhan, Hubei Province, 430060, People’s Republic of China, Tel +86 027-88041911, Email [email protected] Kaichun Wu, Department of Gastroenterology, Xijing Hospital, Air Force Medical University, No. 127 West Changle Road, Xi’an, Shaanxi Province, 710032, People’s Republic of China, Tel +86 029-84771600, Email [email protected]
Objective: To explore the correlation between disease activity and anxiety, depression, sleep quality, and quality of life in patients with inflammatory bowel disease (IBD).
Methods: The disease activity of IBD patients was evaluated by 66 gastroenterologists from 42 hospitals in 22 provinces in China from September 2021 to May 2022. Anxiety, depression, sleep quality and quality of life of IBD patients were investigated and statistically analyzed by different scales, including Generalized Anxiety Disorder 7-item Scale (GAD-7), Patient Health Questionnaire-9 (PHQ-9), Pittsburgh Sleep Quality Index (PSQI), and Inflammatory Bowel Disease Quality-of-Life Questionnaire (IBD-Q).
Results: A total of 2478 IBD patients were included, of which 1532 (61.8%) were in active stage and 946 (38.2%) were in remission. The proportions of active IBD with anxiety, depression, sleep disturbance, and poor quality of life were 29.5%, 29.7%, 71.1%, and 50.1%, respectively, while the proportions of remission IBD with anxiety, depression, sleep disturbance, and poor quality of life were 19.1%, 24.4%, 69.3%, and 17.4%, respectively. IBD patients who also had anxiety, depression, sleep disturbances and poor quality of life had 80 cases (8.46%) in remission and 114 cases (7.44%) in active stage, with 54 cases (9.18%) in mild activity, 51 cases (6.95%) in moderate activity and 9 cases (4.49%) in severe activity. IBD patients with different disease activity levels differed in GAD-7 scores, PHQ-9 scores, PSQI scores, and IBD-Q scores (all P< 0.001). In IBD patients, anxiety, depression, and sleep disturbance, which interact with each other, can further aggravate their disease activity (all P< 0.001).
Conclusion: Anxiety, depression, sleep disturbances, and quality of life are strongly correlated with disease activity in IBD patients, and IBD patients with psychological disturbances are most often in the active stage and have a poor quality of life.
Keywords: inflammatory bowel disease, disease activity, anxiety, depression, sleep quality, quality of life, survey
Introduction
Inflammatory bowel disease (IBD) is a systemic, autoimmune and recurrent chronic nonspecific inflammatory disease of the intestine that requires lifelong monitoring and treatment, and whose pathophysiological mechanisms are not yet understood, known as the “green cancer”.1 IBD, which mainly includes ulcerative colitis (UC), Crohn’s disease (CD) and Inflammatory Bowel Disease Unclassified (IBD-U), has affected more than 6.8 million people worldwide and its incidence and prevalence are increasing worldwide.2,3 Long-term drug maintenance is the foundation of IBD treatment.
In recent years, the social pressure on patients has gradually increased and the problem of mental health disorders has become more serious due to various factors, and the disease activity of patients with IBD would be influenced.4,5 Anxiety/depression is at least twice as prevalent in IBD as in the general population, and depression accounts for approximately 34.7% of IBD active patients and 19.9% of IBD remission patients.6,7 The brain-gut axis is the link between the physiological connection between the human central nervous system and the gastrointestinal tract, and psychological disorders may affect gastrointestinal function by generating a stress response, which leads to activation of the hypothalamic–pituitary–adrenal axis exacerbating the intestinal inflammatory response. In addition, reduced bacterial diversity and pro-inflammatory bacterial microbiota are associated with IBD disease activity,8 and may modulate brain development, function, and behavior through immune, endocrine, and neural pathways of the brain-gut-microbiota axis.9
This study is the first large-sample study in China to collect basic information from IBD patients through a multicenter and to assess the correlation between mental health status and quality of life of IBD patients through relevant scales. It mainly analyzes the clinical data of patients with active and remitting IBD, further analyzes the correlation between anxiety, depression, sleep disorders and quality of life and disease activity, and aids patients and clinicians in monitoring and treating IBD activity, and also strengthens the correct understanding of mental health status and the importance of psychological treatment for IBD patients, so as to achieve early screening and treatment of psychological disorders at the early stage of the disease.
Methods
Study Design and Patient Population
This is a national multicenter cross-sectional survey on the correlation between disease activity and the mental psychological state, and quality of life in IBD patients in China, conducted by the Psychology Club of IBD Group of Gastroenterology Society of Chinese Medical Association and the Chinese Association for Mental Hygiene from September 2021 to May 2022. Uniformly trained investigators explained to eligible patients the purpose, methods, voluntary participation, and harmlessness of the results of the survey, and obtained informed consent, during which standardized speech techniques were used. In this study, IBD patients were investigated by an online survey platform system. Sixty-six gastroenterologists from 42 hospitals in 22 provinces (autonomous regions and municipalities) in China participated in this study, and a total of 2478 valid questionnaires were included, including 1532 patients in active stage (967 with UC and 565 with CD) and 946 patients in remission (404 with UC and 542 with CD).
Inclusion criteria: patients diagnosed with IBD according to the consensus opinion on the diagnosis and treatment of IBD formulated by the Chinese Society of Gastroenterology in 2018;9 age ≥18 years; patients who could understand and agree to be surveyed (willingness to accept physician management and psychological aspects of the survey, submission to management of medication adherence, etc.).
Study Assessments and Data Collection
General Information Collection
The general clinical data of IBD patients were collected, and 66 attending physicians with extensive work experience from 42 hospitals nationwide were trained to refine the scores of the patients, and the modified Mayo score and CDAI score were used to assess the disease activity of UC and CD, respectively. Modified Mayo score and CDAI score are currently the most commonly used clinical indicators to evaluate disease activity and efficacy. The modified Mayo score: <2 is considered in remission, 3–5 is mild activity, 6–10 is moderate activity, and 11–12 is severe activity;10 the CDAI score: <150 is clinical remission, 150–220 is mild activity, 219–450 is moderate activity, and >450 is severe activity.11
Generalized Anxiety Disorder 7-Item Scale (GAD-7) and Patient Health Questionnaire-9 (PHQ-9)
GAD-7 is a widely used anxiety screening scale and has been validated in several studies with a sensitivity of 89% and specificity of 82%.12 It includes 7 entries, each with a score of 0 to 3 and a total score between 0 and 21. PHQ-9 is a widely used international universal depression screening scale with 88% sensitivity and 88% specificity.13 It consists of nine main entries, each with a score of 0 to 3 and a total score between 0 and 27. Ten points were taken as the cut-off point in this study. The score ranges for anxiety and depressive symptom severity in the results of both GAD-7 and PHQ-9 are as follows: minimal symptoms (0–4), mild,5–9 moderate,10–15 and severe (15+) symptoms. In addition, the GAD-7, PHQ-9 and PSQI are simple to operate and have been validated by domestic and international studies to have reliable diagnostic sensitivity and specificity for anxiety disorders, depression and sleep disorders and are also widely used in various studies in China.14–17
Pittsburgh Sleep Quality Index (PSQI)
PSQI is used to evaluate the sleep quality of the subjects in the last 1 month. There are 7 dimensions and 9 entries with a total score between 0 and 21, where a score higher than 5 indicates a sleep quality problem, 0 to 5 indicates good sleep quality, 6 to 10 indicates moderate sleep quality, 11 to 15 indicates poor sleep quality, and 16 to 21 indicates very poor sleep quality.
Inflammatory Bowel Disease Quality-of-Life Questionnaire (IBD-Q)
IBD-Q has been widely used to evaluate the quality of life of IBD patients, including 4 dimensions of bowel symptoms, systemic symptoms, emotional ability, and social ability, with a total of 32 items.18 Each item is divided into 7 levels, counting from 1 to 7, with 1 indicating the most severe degree and 7 indicating the least severe degree. The total score ranged from 32 to 224, and the higher the total score, the better the patient’s quality of survival.
Study Size
The sample size needed for the questionnaire survey was calculated according to the principles of international psychometrics and questionnaire design. If the number of items in the questionnaire increases, the recommended sample size will increase, that is, 5–20 times the number of items in the questionnaire. If N is the number of questionnaire items in this study, the sample size is at least 5N. In addition, about 10% of the questionnaires may be withdrawn or invalid, so the sample size needs to be 5.5N. Therefore, the sample size should be greater than 451. Considering the large population and other confounding factors in our country, we try to expand the sample size when conducting the study. Therefore, 2478 questionnaires were finally included in the study.
Statistical Analysis
SPSS 27.0, GraphPad prism, and Excel 2021 software were used for data entry, statistical analysis, and visualization in this study. Count data were expressed as frequencies and percentages using the cross-tabulated χ2 test or Fisher’s exact test. The measurement data that conformed to normal distribution were expressed as  , and t-test or non-parametric test was used. The test level for this study was α = 0.05, and P<0.05 was considered a statistically significant difference.
, and t-test or non-parametric test was used. The test level for this study was α = 0.05, and P<0.05 was considered a statistically significant difference.
Results
Clinical Characteristics of IBD Patients of Different Disease Activity
A total of 2478 patients with IBD were included, including 1371 (55.33%) with UC and 1107 (44.67%) with CD. A total of 1532 (61.8%) and 946 (38.2%) patients with IBD were in the active and remission stages, respectively, and 967 (70.5%) and 565 (51.4%) patients with UC and CD, respectively, were in the active stage. Age and gender were associated with disease activity in IBD patients (both P<0.05). The mean age of patients with IBD in the active stage was 38.57 ± 12.48 years, and the proportion of women in the active stage was higher than in the remission stage (39.8% vs 33.9%) (Table 1).
 |
Table 1 General Clinical Features with Remission and Activity in Patients of Inflammatory Bowel Disease |
Anxiety, Depression, Sleep Quality and Quality of Life in IBD Patients of Different Disease Activity
As shown in Table 2 and Table 3 and Figures 1 and 2, the proportion of anxiety in active stage was significantly higher than that in remission (IBD: 29.4% vs 19.1%, P<0.001; UC: 31.4% vs 21.0%, P<0.001; CD: 25.8% vs 17.7%, P=0.001), and there were differences in the severity of anxiety in different disease activity (IBD: P=0.011; UC: P=0.051; CD: P=0.243). The proportion of depression in active stage was higher than that in remission (IBD: 33.0% vs 24.4%, P<0.001; UC: 34.4% vs 24.0%, P<0.001; CD: 30.6% vs 24.7%, P=0.032), and there were differences in the severity of depression in different disease activity (IBD: P=0.017; UC: P=0.02; CD: P=0.588). There was no statistical difference in the proportion of sleep disturbances between active IBD patients and those in remission (IBD: 72.1% vs 69.3%, P=0.145; UC: 70.4% vs 73.0%, P=0.842; CD: 71.7% vs 66.6%, P=0.069), and the proportion of poor quality of life in active stage was higher than that in remission (IBD: 50.1% vs 17.4%, P<0.001; UC: 52.4% vs 17.6%, P<0.001; CD: 46.2% vs 17.3%, P<0.001).
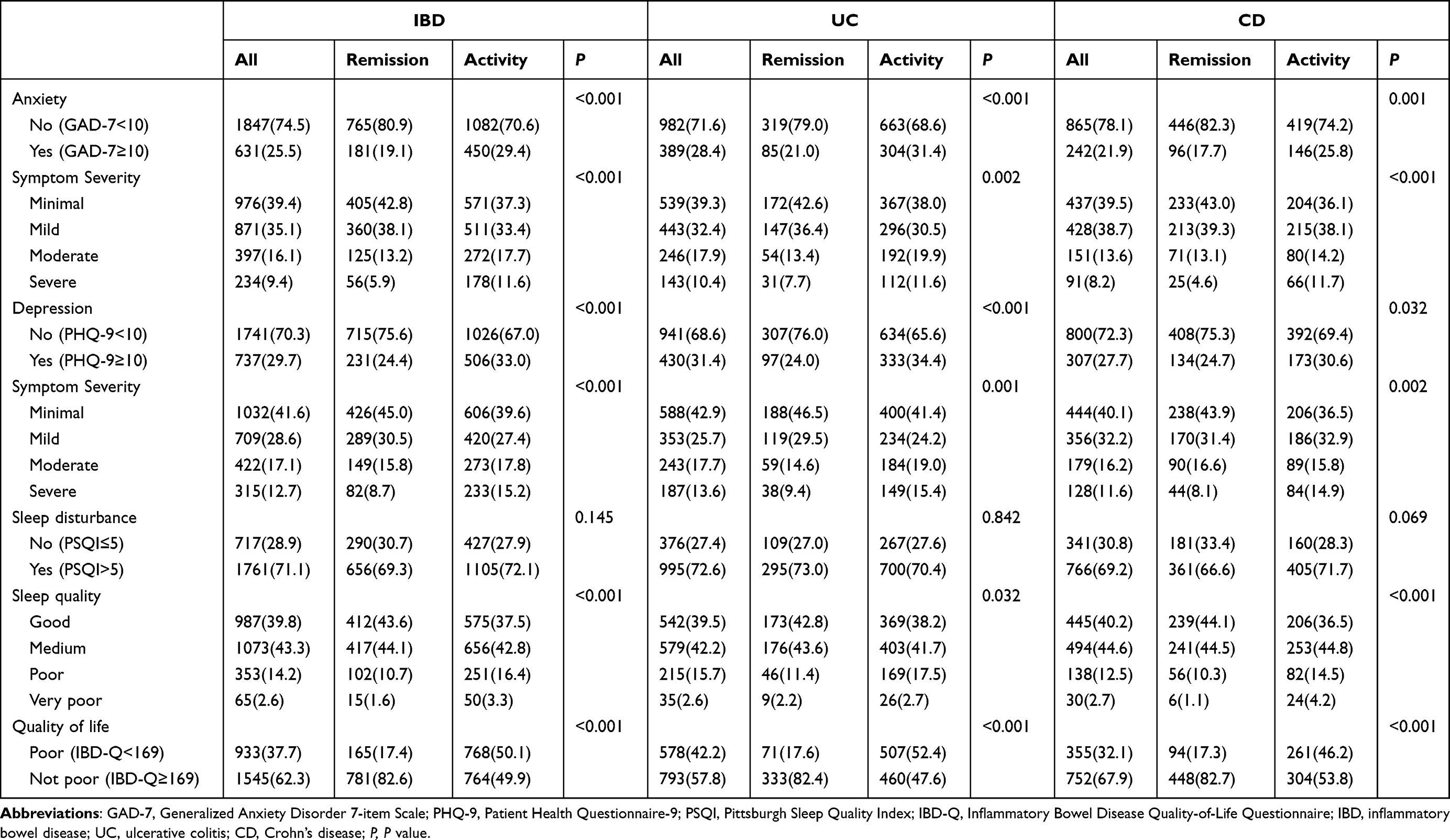 |
Table 2 Anxiety, Depression, Sleep Quality, and Quality of Life in IBD Patients in Activity Compared with in Remission |
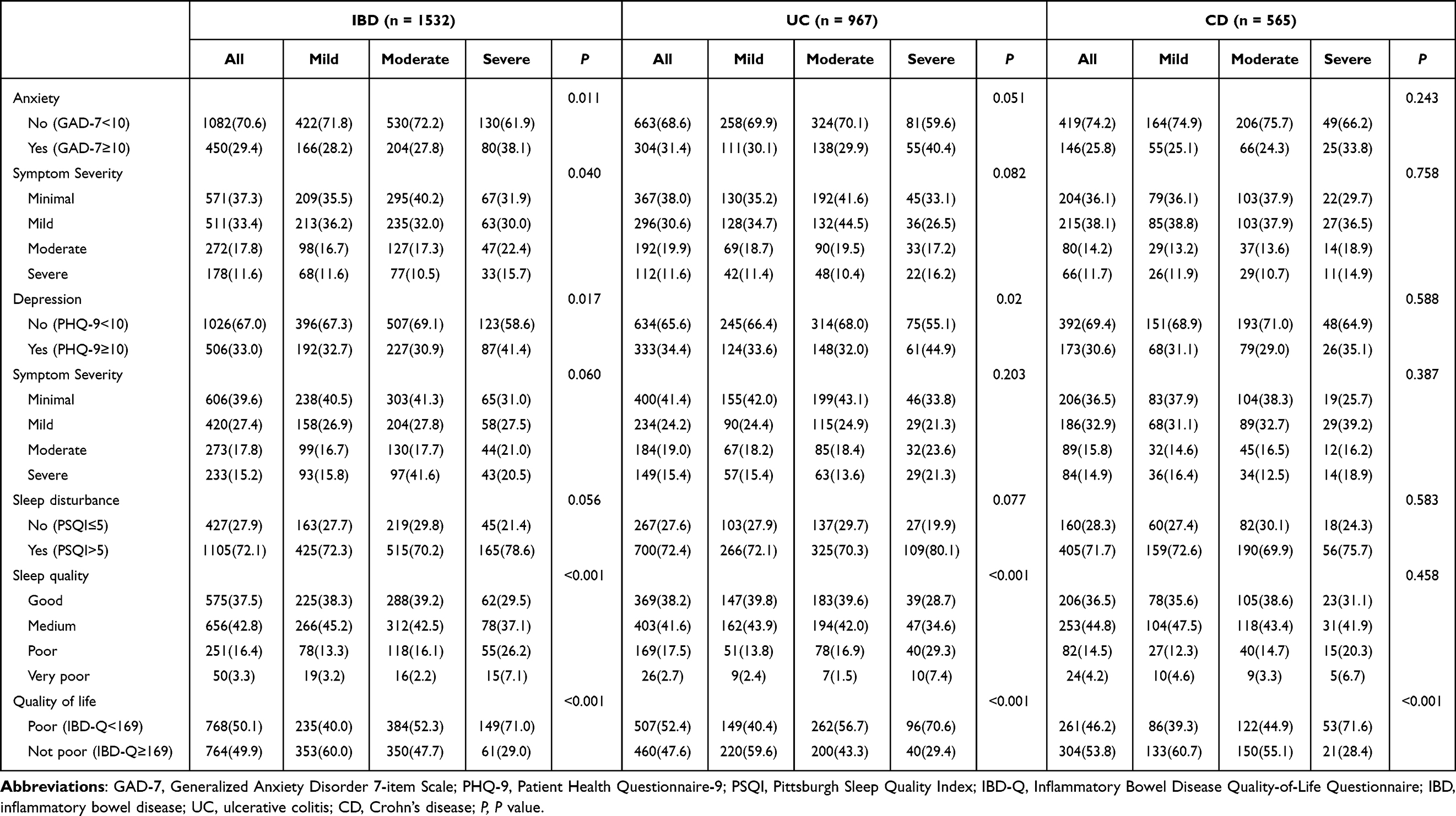 |
Table 3 Anxiety, Depression, Sleep Quality, and Quality of Life in IBD Patients in Mild, Moderate, Severe Activity |
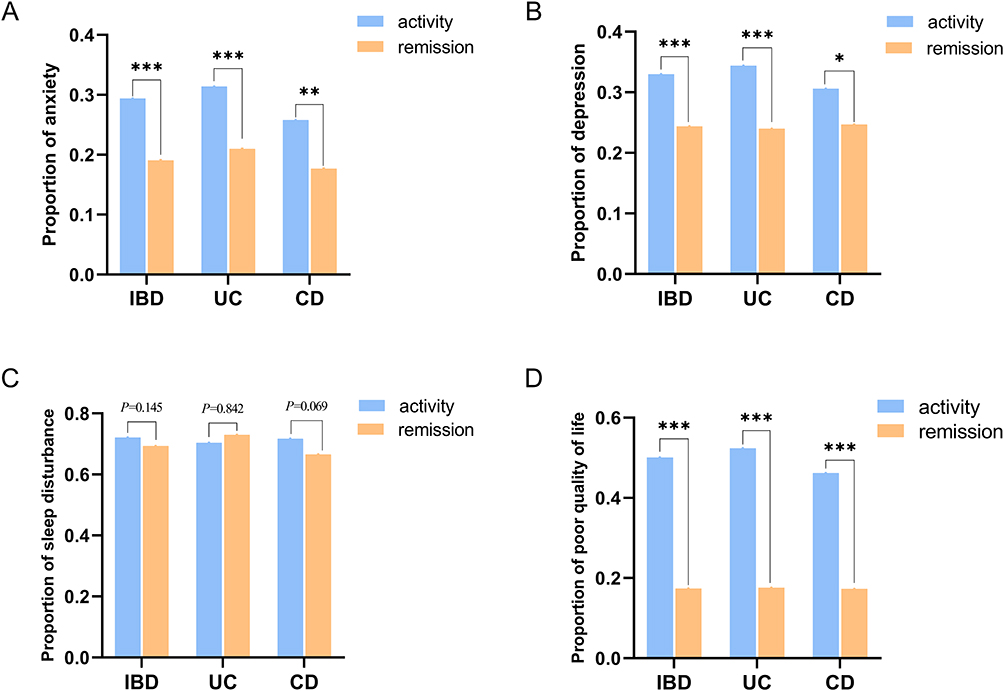 |
Figure 1 Proportions of anxiety (A), depression (B), sleep disturbance (C) and poor quality of life (D) in IBD patients with different disease activity (***P<0.001, **P<0.01, *P<0.05). Abbreviations: IBD, inflammatory bowel disease; UC, ulcerative colitis; CD, Crohn’s disease. |
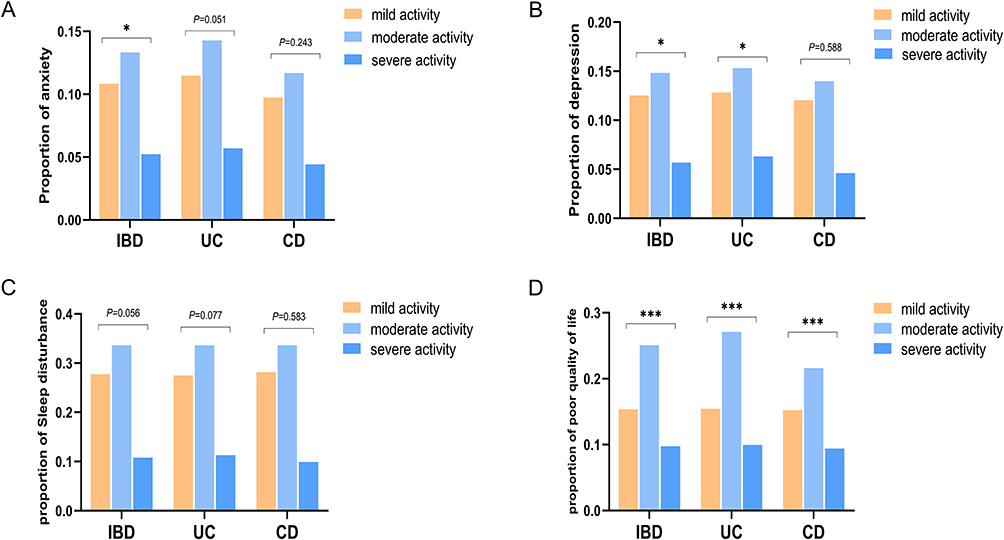 |
Figure 2 Proportions of anxiety (A), depression (B), sleep disturbance (C) and poor quality of life (D) in patients with mild, moderate and moderately active IBD (***P<0.001, *P<0.05). Abbreviations: IBD, inflammatory bowel disease; UC, ulcerative colitis; CD, Crohn’s disease. |
Comorbid Anxiety, Depression, Sleep Disturbances, and Poorer Quality of Life Among IBD Patients of Different Disease Activities
In 1532 active patients, there were 11 (0.72%), 10 (0.65%), 245 (16.01%), and 242 (15.80%) patients with anxiety, depression, sleep disturbance, and poor quality of life only, respectively, and 114 (7.44%) patients with both anxiety, depression, sleep disturbance, and poor quality of life, as shown in Figure 3A. In 946 patients in remission, there were 1 (0.11%), 0 (0%), 56 (5.92%), and 251 (26.53%) patients with anxiety, depression, sleep disturbance, and poor quality of life only, respectively, and 80 (8.46%) patients with both anxiety, depression, sleep disturbance, and poor quality of life, as shown in Figure 3B. Among the 588 patients with mild activity, 54 patients (9.18%) had a combination of anxiety, depression, sleep disturbance and poor quality of life, as shown in Figure 3C. Among the 734 patients with moderate activity, 51 patients (6.95%) had a combination of anxiety, depression, sleep disturbance and poor quality of life, as shown in Figure 3D. Among 210 patients with severe activity, there were 9 patients (4.49%) with combined anxiety, depression, sleep disturbance and poor quality of life, as shown in Figure 3E.
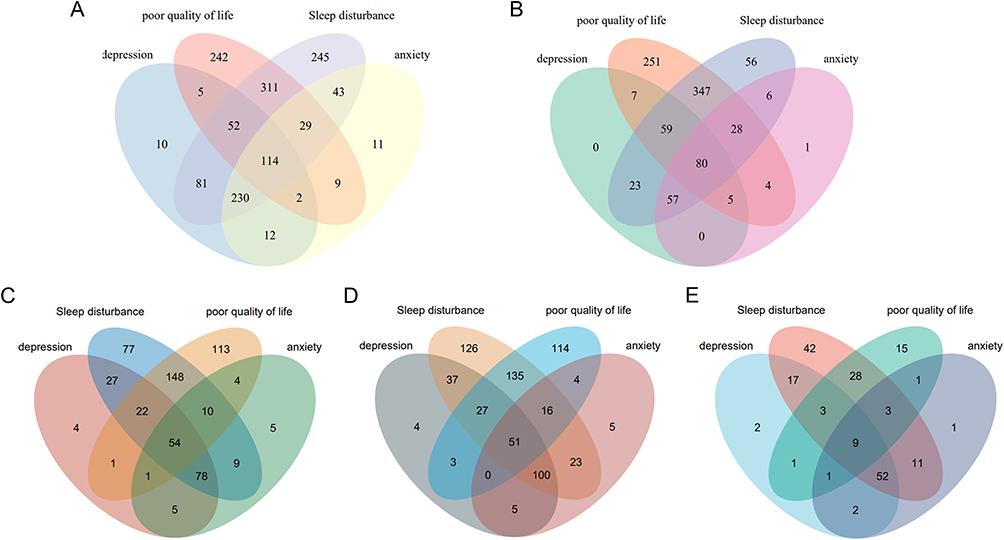 |
Figure 3 Venn diagram of comorbid anxiety, depression, sleep disturbance and poor quality of life in IBD patients with different disease activity (A): active stage, (B): remission stage, (C): mild activity, (D): moderate activity, (E): severe activity. Abbreviation: IBD, inflammatory bowel disease. |
Scores of GAD-7, PHQ-9, PSQI, and IBD-Q in IBD Patients of Different Disease Activity
IBD patients with different degrees of disease activity differed in GAD-7 scores, PHQ-9 scores, PSQI scores, and IBD-Q scores (all P < 0.001). GAD-7 scores, PHQ-9 scores, and PSQI scores were higher in the active stage of IBD (including UC and CD) than in remission (P < 0.001), and total IBD-Q scores were higher in IBD patients in remission (P < 0.001), see Table 4 and Figure 4. Scores of GAD-7, PHQ-9, PSQI, and IBD-Q were significantly different in IBD patients with mild and moderately severe activity (P < 0.001) (Table 5). When anxiety, depression, and sleep disturbance were present together, the three interact with each other to further aggravate disease activity (Table 6).
 |
Table 4 Scores of GAD-7, PHQ-9, PSQI, and IBD-Q in IBD Patients in Activity Compared with in Remission (Scores, |

 |
Table 5 Scores of GAD-7, PHQ-9, PSQI, and IBD-Q in IBD Patients in Mild, Moderate, Severe Activity (Scores, |



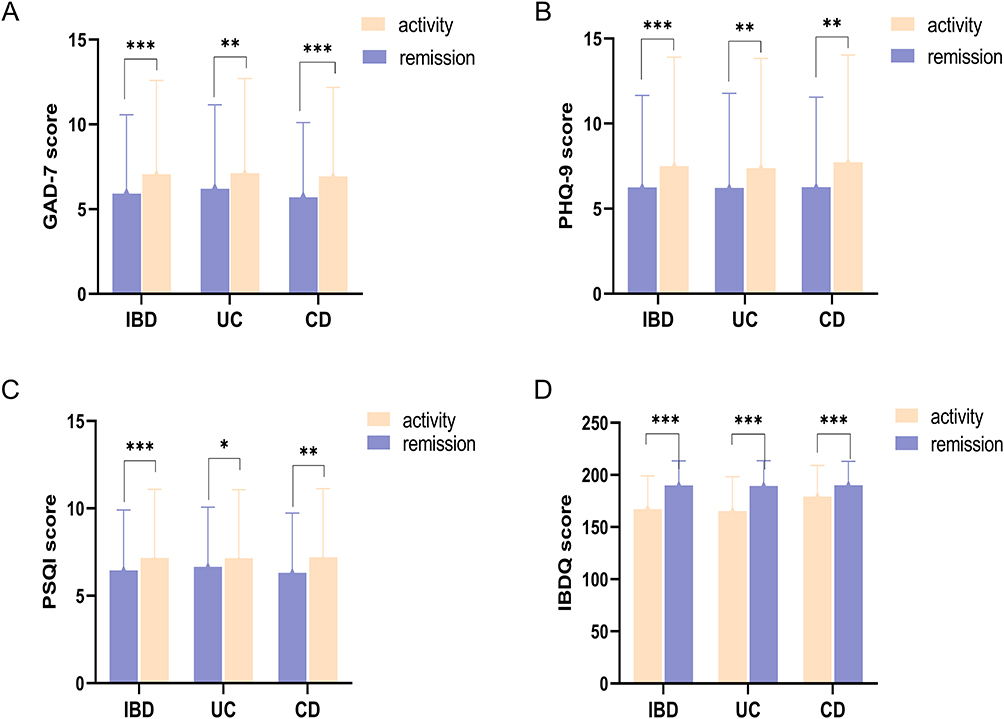 |
Figure 4 GAD-7 score (A), PHQ-9 score (B), PSQI score (C), and IBD-Q score (D) in IBD patients with different disease activity (***P<0.001, **P<0.01, *P<0.05). Abbreviations: IBD, inflammatory bowel disease; UC, ulcerative colitis; CD, Crohn’s disease; GAD-7, Generalized Anxiety Disorder 7-item Scale; PHQ-9, Patient Health Questionnaire-9; PSQI, Pittsburgh Sleep Quality Index; IBD-Q; Inflammatory Bowel Disease Quality-of-Life Questionnaire. |
Discussion
IBD is a chronic disabling disease that affects mental health and overall quality of life, and its prevalence is gradually increasing worldwide.19–22 In this study of 2478 Chinese patients with IBD, it was found that 25.5% and 29.7% of IBD patients were eligible for moderate-to-severe anxiety and depression, and that different levels of anxiety/depression were closely related to different levels of disease activity. It was found that patients with IBD are mostly in the active phase of the disease when there are psychosomatic problems of anxiety, depression, and sleep disturbance. The results of this study are related to the recurrent nature of the IBD disease course, lifelong medication monitoring, adverse drug reactions, and financial burden, which will lead to significant psychological stress in these patients, which was verified by several clinical trials.23–27 In this study, with 38.1% and 41.4% of IBD patients with combined anxiety/depression and at severe activity, respectively. In a study by Lewis et al28 of 242 patients with IBD, it was found that 30.6% and 40.1% of patients met the diagnostic criteria for anxiety and depression, respectively, but about 1/3 and 2/3 were undiagnosed. In this study, the active patients with anxiety and depression accounted for 29.4% and 33.0%, respectively, and none of them was given corresponding psychological treatment. In addition, above an animal experimental study of IBD activity, it was found that a mouse model of colitis in a depressed state reactivated intestinal inflammation,29 and its activity remitted after active psychotherapy.30 Clinical studies have further confirmed that immunotherapy can decrease the PHQ-9 score of IBD patients and significantly improve the risk of moderate and severe depression in IBD patients,31 mainly because there is a bidirectional nature between mental health status and IBD, and the two affect each other.32,33 Patients with IBD with psychological disorders have increased sympathetic autonomic activity and catecholamine secretion from the adrenal medulla, which exacerbates the inflammatory response by stimulating mast cells and macrophages, which in turn leads to increased disease activity.33,34 The bidirectional role of the brain-gut axis plays an important role in the development of disease activity, and the anxiety/depression can increase the activity of IBD disease by reactivating inflammation through multiple pathways,4,35–38 as well as leading to poor patient compliance with treatment and further morbidity and mortality.39–41 In addition, patients with mild anxiety were also in the majority in this study. Therefore, routine psychological assessment is important in the assessment of disease activity to effectively identify patients at higher risk of disease activity at an early stage.42 Improving the distress of psychosocial factors and alleviating anxiety/depression in patients with IBD through psychological state regulation can not only improve disease activity but also optimize quality of life.
In this study, 28.4% and 21.9% of UC and CD patients had a moderate anxiety state, respectively, and 31.4% and 27.7% of patients had a moderate depressive state, respectively, and the severity of anxiety/depression also influenced the activity of IBD, and when anxiety was co-morbid with UC or CD, it was more closely associated with disease activity as the level of anxiety increased, which is consistent with the results of previous studies.39,43,44 The main reason may be that the development of depression/anxiety complicates the clinical management of IBD and can increase the frequency of disease activity.26,44 It has also been found that even in disease remission, about 1/3 of IBD patients develop irritable bowel syndrome-like symptoms in response to the brain-gut axis,45 making psychological disturbances more severe and more likely in patients with CD.46,47 In recent years, the incidence of depression in patients with IBD has also increased year by year, with a significant impact on the severity of the disease, both in terms of exacerbating disease activity and increasing the risk of surgery for CD.36,48,49 The earliest prospective studies also confirmed that depressive symptoms are an independent predictor of CD activity.4,42 Therefore, psychosocial status should not be neglected in the treatment of IBD patients, and some patients can control the disease activity by improving their emotions and lifestyle, which is very important for the development of IBD disease and disease prognosis, as well as reducing the economic burden of patients and avoiding the adverse effects caused by medication, improving the quality of life of patients, and relieving the medical burden.
Sleep quality was also strongly associated with disease activity in this study, and impaired sleep may influence the pathogenesis and course of IBD by decreasing systemic immunity.50 This was confirmed by several studies in which patients with sleep-impaired CD had a twofold increased risk of disease activity within a 6-month period.51,52 In this study, the sleep quality of IBD patients was mostly moderate (43.3%) and mostly in remission, when the sleep quality was poor or very poor the disease was mostly in active phase, which may be related to the increase in the number and degree of diarrhea and abdominal pain in active patients, in addition, the proportion of glucocorticoids used in active patients is large, and the side effects of this drug also affect sleep, therefore, sleep disorders can further aggravate the disease activity of the disease. In addition, this study also found that sleep has a greater impact on active CD, and patients with moderate sleep quality are already in the active phase of the disease, which is mainly related to more pronounced systemic symptoms in patients with CD, and prolonged mild sleep disturbance in patients in remission may cause a recurrence of intestinal symptoms. Patients in remission with poor sleep quality were reported to have a higher risk of active disease at 6-month follow-up than those without sleep problems.53 Therefore, sleep quality problems in IBD should be attended to and treated. Studies have shown that although patients with IBD in remission (both UC and CD) have a better quality of life than those in active disease, they still have a lower quality of life compared to healthy individuals,54,55 which requires extensive attention.
In conclusion, anxiety, depression, sleep disturbance and quality of life were strongly associated with disease activity in Chinese patients with IBD, and IBD with varying degrees of psychological disturbance was more often in the active phase of the disease and had a low quality of life. The issue of mental health status of patients with active IBD should receive more attention.
One of the limitations of this study, which was a cross-sectional study, is that it does not provide a causal relationship between psychosomatic mental status and disease activity, and further validation by prospective studies is more needed in the future. Another limitation is that patients’ psychological symptoms were assessed in a retrospective survey, and we did not assess lifetime risk, 12-month risk or changes in psychological status over time, which would be subject to recall bias, and future prospective observational and treatment studies are needed to determine the responsiveness of psychosomatic status in the assessment of changes over time.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
The study complies with the Declaration of Helsinki. The study was approved by the Institutional Review Board of Renmin Hospital of Wuhan University, and informed consent was obtained from all patients. The clinical research Ethics Review approval number of Renmin Hospital of Wuhan University was WDRY2022-K150.
Acknowledgment
The authors would like to thank 42 participating institutions and associated IBD physicians for their help in this study, listed below (in no particular order): Renmin Hospital of Wuhan University (Ping An, Jixiang Zhang), Xijing Hospital, Air Force Medical University (Min Chen), Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (Hong Lyv), the Second Affiliated Hospital of Xi’an Jiaotong University (Fenrong Chen, Sumei Sha), Peking University First Hospital (Tian Yuling), Peking University Third Hospital (Jun Li), Beijing Friendship Hospital, Capital Medical University (Ye Zong, Haiying Zhao), Ruijin Hospital, Shanghai Jiaotong University School of Medicine (Tianyu Zhang), First Affiliated Hospital of Sun Yat-sen University (Baili Chen, Ren Mao, Yao He, Shenghong Zhang), General Hospital, Tianjin Medical University (Hailong Cao, Shuai Su, Wenyao Dong, Lili Yang), Second Hospital of Hebei Medical University (Qian Liu, Rongrong Zhan), Sir Run-Run Shaw Hospital, Zhejiang University School of Medicine (Jing Liu), the First Affiliated Hospital of Wenzhou Medical University (Xiangrong Chen, Xiaowei Chen, Lingyan Shi), the Affiliated Hospital of Medical School of Ningbo University (Jinfeng Wen), Jiangsu Province Hospital, the First Affiliated Hospital of Nanjing Medical University (Jingjing Ma), Jiangsu Province Hospital of Chinese Medicine (Lei Zhu), General Hospital of Eastern Theater Command of Chinese People’s Liberation Army (Juan Wei), the Second Affiliated Hospital of Soochow University (Han Xu), Shengjing Hospital of China Medical University (Nan Nan, Feng Tian), the First Affiliated Hospital of Dalian Medical University (Xiuli Chen, Jingwei Mao), Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Liangru Zhu), Zhongnan Hospital of Wuhan University (Mei Ye), Xiangya Hospital of Central South University (Shuijiao Chen), the Second Xiangya Hospital of Central South University (Hanyu Wang), Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China (Xue Yang, Yinghui Zhang), the First Affiliated Hospital of Anhui Medical University (Juan Wu), Qilu Hospital, Shandong University (Xiaoqing Jia), the Affiliated Hospital of Qingdao University (Xueli Ding, Jing Guo, Ailing Liu), the First Hospital of Jilin University (Haibo Sun, Jing Zhan), the First Affiliated Hospital of Kunming Medical University (Yating Qi), General Hospital of Ningxia Medical University (Shaoqi Yang, Ting Ye), the Second Affiliated Hospital of Zhengzhou University (Sumin Wang, Dandan Wang), the First Affiliated Hospital of Guangxi Medical University (Xiaoping Lyu, Junhua Fan, Shiquan Li), Chongqing General Hospital (Chongqing Hospital, University of Chinese Academy of Sciences) (Lingya Xiang), the First Affiliated Hospital of Xinjiang Medical University (Ping Yao, Hongliang Gao), the Second Affiliated Hospital of Harbin Medical University (Wanying Li), the First Affiliated Hospital of the University of Science and Technology of China, Anhui Provincial Hospital (Xuemei Xu), Daping Hospital, Army Medical University (Zhuqing Qiu), Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine (Wen Lyu), the Affiliated Hospital of Southwest Medical University (Xiaolin Zhong), General Hospital of Southern Theater Command of People’s Liberation Army (Ang Li, Xiangqiang Liu, Yanchun Ma), Suzhou Municipal Hospital (North District), Nanjing Medical University Affiliated Suzhou Hospital (Zhi Pang). In addition, the authors would like to thank editors and the anonymous reviewers for their valuable comments and suggestions to improve the quality of the paper.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The National Natural Science Foundation of China (No. 82170549) funded this manuscript.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Ananthakrishnan AN, Bernstein CN, Iliopoulos D, et al. Environmental triggers in IBD: a review of progress and evidence. Nat Rev Gastroenterol Hepatol. 2018;15(1):39–49. doi:10.1038/nrgastro.2017.136
2. Alatab S, Sepanlou SG, Ikuta K, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi:10.1016/S2468-1253(19)30333-4
3. Drossman DA. Gastrointestinal illness and the biopsychosocial model. J Clin Gastroenterol. 1996;22(4):252–254.
4. Mikocka-Walus A, Pittet V, Rossel J-B, von Känel R. Symptoms of depression and anxiety are independently associated with clinical recurrence of inflammatory bowel disease. Clin Gastroenterol Hepatol. 2016;14(6). doi:10.1016/j.cgh.2015.12.045
5. Alexakis C, Kumar S, Saxena S, Pollok R. Systematic review with meta-analysis: the impact of a depressive state on disease course in adult inflammatory bowel disease. Aliment Pharmacol Ther. 2017;46(3):225–235. doi:10.1111/apt.14171
6. Mikocka-Walus A, Andrews JM. It is high time to examine the psyche while treating IBD. Nat Rev Gastroenterol Hepatol. 2018;15(6):329–330. doi:10.1038/s41575-018-0004-y
7. Mikocka-Walus A, Knowles SR, Keefer L, Graff L. Controversies revisited: a systematic review of the comorbidity of depression and anxiety with inflammatory bowel diseases. Inflamm Bowel Dis. 2016;22(3):752–762. doi:10.1097/MIB.0000000000000620
8. Sepehri S, Kotlowski R, Bernstein CN, Krause DO. Microbial diversity of inflamed and noninflamed gut biopsy tissues in inflammatory bowel disease. Inflamm Bowel Dis. 2007;13(6):675–683.
9. Kelly JR, Kennedy PJ, Cryan JF, Dinan TG, Clarke G, Hyland NP. Breaking down the barriers: the gut microbiome, intestinal permeability and stress-related psychiatric disorders. Front Cell Neurosci. 2015;9:392. doi:10.3389/fncel.2015.00392
10. D’Haens G, Sandborn WJ, Feagan BG, et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Gastroenterology. 2007;132(2):763–786.
11. Best WR, Becktel JM, Singleton JW, Kern F. Development of a Crohn’s disease activity index. national cooperative Crohn’s disease study. Gastroenterology. 1976;70(3):439–444.
12. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the Gad-7. Arch Intern Med. 2006;166(10):1092–1097.
13. Litster B, Bernstein CN, Graff LA, et al. Validation of the Phq-9 for suicidal ideation in persons with inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(8):1641–1648. doi:10.1093/ibd/izy032
14. Liu Y, Chen H, Zhang N, et al. Anxiety and depression symptoms of medical staff under Covid-19 epidemic in China. J Affect Disord. 2021;278:144–148. doi:10.1016/j.jad.2020.09.004
15. Liao J, Kang J, Li F, et al. A cross-sectional study on the association of anxiety and depression with the disease activity of systemic lupus erythematosus. BMC Psychiatry. 2022;22(1):591. doi:10.1186/s12888-022-04236-z
16. Gong Y, Zhou H, Zhang Y, et al. Validation of the 7-item generalized anxiety disorder scale (Gad-7) as a screening tool for anxiety among pregnant Chinese women. J Affect Disord. 2021:282. doi:10.1016/j.jad.2020.12.129
17. Tong X, An D, McGonigal A, Park S-P, Zhou D. Validation of the Generalized Anxiety Disorder-7 (Gad-7) among Chinese people with epilepsy. Epilepsy Res. 2016;120:31–36. doi:10.1016/j.eplepsyres.2015.11.019
18. Chen X-L, Zhong L-H, Wen Y, et al. Inflammatory bowel disease-specific health-related quality of life instruments: a systematic review of measurement properties. Health Qual Life Outcomes. 2017;15(1):177. doi:10.1186/s12955-017-0753-2
19. Tarar ZI, Zafar MU, Farooq U, et al. Burden of depression and anxiety among patients with inflammatory bowel disease: results of a nationwide analysis. Int J Colorectal Dis. 2022;37(2):313–321. doi:10.1007/s00384-021-04056-9
20. Bernstein CN, Hitchon CA, Walld R, et al. Increased burden of psychiatric disorders in inflammatory bowel disease. Inflamm Bowel Dis. 2019;25(2):360–368. doi:10.1093/ibd/izy235
21. Williet N, Sarter H, Gower-Rousseau C, et al. Patient-reported outcomes in a French nationwide survey of inflammatory bowel disease patients. J Crohns Colitis. 2017;11(2):165–174. doi:10.1093/ecco-jcc/jjw145
22. Walker JR, Ediger JP, Graff LA, et al. The Manitoba IBD cohort study: a population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am J Gastroenterol. 2008;103(8):1989–1997. doi:10.1111/j.1572-0241.2008.01980.x
23. Geiss T, Schaefert RM, Berens S, Hoffmann P, Gauss A. Risk of depression in patients with inflammatory bowel disease. J Dig Dis. 2018;19(8):456–467. doi:10.1111/1751-2980.12644
24. Sexton KA, Walker JR, Graff LA, et al. Evidence of bidirectional associations between perceived stress and symptom activity: a prospective longitudinal investigation in inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(3):473–483. doi:10.1097/MIB.0000000000001040
25. Mawdsley JE, Macey MG, Feakins RM, Langmead L, Rampton DS. The effect of acute psychologic stress on systemic and rectal mucosal measures of inflammation in ulcerative colitis. Gastroenterology. 2006;131(2):410–419.
26. Marrie RA, Graff LA, Fisk JD, Patten SB, Bernstein CN. The relationship between symptoms of depression and anxiety and disease activity in IBD over time. Inflamm Bowel Dis. 2021;27(8):1285–1293. doi:10.1093/ibd/izaa349
27. Tabatabaeian M, Afshar H, Roohafza HR, et al. Psychological status in Iranian patients with ulcerative colitis and its relation to disease activity and quality of life. J Res Med Sci. 2015;20(6):577–584. doi:10.4103/1735-1995.165962
28. Lewis K, Marrie RA, Bernstein CN, et al. The prevalence and risk factors of undiagnosed depression and anxiety disorders among patients with inflammatory bowel disease. Inflamm Bowel Dis. 2019;25(10):1674–1680. doi:10.1093/ibd/izz045
29. Ghia J-E, Blennerhassett P, Deng Y, Verdu EF, Khan WI, Collins SM. Reactivation of Inflammatory bowel disease in a mouse model of depression. Gastroenterology. 2009;136(7). doi:10.1053/j.gastro.2009.02.069
30. Ghia J-E, Blennerhassett P, Collins SM. Impaired parasympathetic function increases susceptibility to inflammatory bowel disease in a mouse model of depression. J Clin Invest. 2008;118(6):2209–2218. doi:10.1172/JCI32849
31. Horst S, Chao A, Rosen M, et al. Treatment with immunosuppressive therapy may improve depressive symptoms in patients with inflammatory bowel disease. Dig Dis Sci. 2015;60(2):465–470. doi:10.1007/s10620-014-3375-0
32. Gracie DJ, Guthrie EA, Hamlin PJ, Ford AC. Bi-directionality of brain-gut interactions in patients with inflammatory bowel disease. Gastroenterology. 2018;154(6). doi:10.1053/j.gastro.2018.01.027
33. Mawdsley JE, Rampton DS. Psychological stress in IBD: new insights into pathogenic and therapeutic implications. Gut. 2005;54(10):1481–1491.
34. Gracie DJ, Hamlin PJ, Ford AC. The influence of the brain–gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol Hepatol. 2019;4(8):632–642. doi:10.1016/s2468-1253(19)30089-5
35. Luo X-P, Mao R, Chen B-L, et al. Over-reaching beyond disease activity: the influence of anxiety and medical economic burden on health-related quality of life in patients with inflammatory bowel disease. Patient Prefer Adherence. 2017;11:23–31. doi:10.2147/PPA.S118589
36. Gao X, Tang Y, Lei N, et al. Symptoms of anxiety/depression is associated with more aggressive inflammatory bowel disease. Sci Rep. 2021;11(1):1440. doi:10.1038/s41598-021-81213-8
37. Graff LA, Walker JR, Lix L, et al. The relationship of inflammatory bowel disease type and activity to psychological functioning and quality of life. Clin Gastroenterol Hepatol. 2006;4(12):1491–1501.
38. Larsson K, Lööf L, Rönnblom A, Nordin K. Quality of life for patients with exacerbation in inflammatory bowel disease and how they cope with disease activity. J Psychosom Res. 2008;64(2):139–148. doi:10.1016/j.jpsychores.2007.10.007
39. Neuendorf R, Harding A, Stello N, Hanes D, Wahbeh H. Depression and anxiety in patients with inflammatory bowel disease: a systematic review. J Psychosom Res. 2016;87:70–80. doi:10.1016/j.jpsychores.2016.06.001
40. Nigro G, Angelini G, Grosso SB, Caula G, Sategna-Guidetti C. Psychiatric predictors of noncompliance in inflammatory bowel disease: psychiatry and compliance. J Clin Gastroenterol. 2001;32(1):66–68.
41. Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):1.
42. Mardini HE, Kip KE, Wilson JW. Crohn’s disease: a two-year prospective study of the association between psychological distress and disease activity. Dig Dis Sci. 2004;49(3):492–497.
43. Iglesias M, Barreiro de Acosta M, Vázquez I, et al. Psychological impact of Crohn’s disease on patients in remission: anxiety and depression risks. Rev Esp Enferm Dig. 2009;101(4):249–257.
44. Barberio B, Zamani M, Black CJ, Savarino EV, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–370. doi:10.1016/S2468-1253(21)00014-5
45. Jonefjäll B, Strid H, Ohman L, Svedlund J, Bergstedt A, Simren M. Characterization of Ibs-like symptoms in patients with ulcerative colitis in clinical remission. Neurogastroenterol Motil. 2013;25(9). doi:10.1111/nmo.12163
46. Henriksen M, Høivik ML, Jelsness-Jørgensen L-P, Moum B. Irritable bowel-like symptoms in ulcerative colitis are as common in patients in deep remission as in inflammation: results from a population-based study [the Ibsen study]. J Crohns Colitis. 2018;12(4):389–393. doi:10.1093/ecco-jcc/jjx152
47. Gracie DJ, Williams CJM, Sood R, et al. Negative effects on psychological health and quality of life of genuine irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2017;15(3). doi:10.1016/j.cgh.2016.05.012
48. Blackwell J, Saxena S, Petersen I, et al. Depression in individuals who subsequently develop inflammatory bowel disease: a population-based nested case-control study. Gut. 2021;70(9):1642–1648. doi:10.1136/gutjnl-2020-322308
49. Kochar B, Barnes EL, Long MD, et al. Depression is associated with more aggressive inflammatory bowel disease. Am J Gastroenterol. 2018;113(1):80–85. doi:10.1038/ajg.2017.423
50. Eissa N, Mujawar Q, Alabdoulsalam T, Zohni S, El-Matary W. The immune-sleep crosstalk in inflammatory bowel disease. Sleep Med. 2020;73:38–46. doi:10.1016/j.sleep.2020.04.020
51. Hao G, Zhu B, Li Y, Wang P, Li L, Hou L. Sleep quality and disease activity in patients with inflammatory bowel disease: a systematic review and meta-analysis. Sleep Med. 2020;75:301–308. doi:10.1016/j.sleep.2020.08.032
52. Ali T, Madhoun MF, Orr WC, Rubin DT. Assessment of the relationship between quality of sleep and disease activity in inflammatory bowel disease patients. Inflamm Bowel Dis. 2013;19(11):2440–2443. doi:10.1097/MIB.0b013e3182a0ea54
53. Ananthakrishnan AN, Long MD, Martin CF, Sandler RS, Kappelman MD. Sleep disturbance and risk of active disease in patients with Crohn’s disease and ulcerative colitis. Clin Gastroenterol Hepatol. 2013;11(8):965–971. doi:10.1016/j.cgh.2013.01.021
54. Knowles SR, Keefer L, Wilding H, Hewitt C, Graff LA, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses-part Ii. Inflamm Bowel Dis. 2018;24(5):966–976. doi:10.1093/ibd/izy015
55. Knowles SR, Graff LA, Wilding H, Hewitt C, Keefer L, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses-part I. Inflamm Bowel Dis. 2018;24(4):742–751. doi:10.1093/ibd/izx100
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relation Among Anxiety, Depression, Sleep Quality and Health-Related Quality of Life Among Patients with Systemic Lupus Erythematosus: Path Analysis
Chen HJ, Wang H, Qiu LJ, Ling HY, Wu LL, Wang TR, Zhou Y, Xue Y, Ye DQ, Wang B
Patient Preference and Adherence 2022, 16:1351-1358
Published Date: 25 May 2022
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
A Cross-Sectional Study on the Relationship Between Rosacea Severity and Quality of Life or Psychological State
Yang F, Zhang Q, Song D, Liu X, Wang L, Jiang X
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2807-2816
Published Date: 20 December 2022
Analyzing Role Overload, Mental Health, and Quality of Life Among Jordanian Female Healthcare Professionals: A Cross-Sectional Study
Alnazly EK, Allari R, Alshareef BE, Abu Al-khair F
International Journal of Women's Health 2023, 15:1917-1930
Published Date: 4 December 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024