Back to Journals » Psychology Research and Behavior Management » Volume 18
Association Between Depression, Anxiety, and Stress and Sleep Quality Among University Students from Saudi Arabia: A Cross-Sectional Study
Authors Gosadi IM ![]() , Shnaimer JA
, Shnaimer JA ![]()
Received 11 September 2025
Accepted for publication 6 November 2025
Published 14 November 2025 Volume 2025:18 Pages 2287—2298
DOI https://doi.org/10.2147/PRBM.S562798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Einar Thorsteinsson
Ibrahim M Gosadi,1 Jubran A Shnaimer2
1Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Sleep Medicine Center, Jazan Specialist Hospital, Jazan, Saudi Arabia
Correspondence: Ibrahim M Gosadi, Department of Family and Community Medicine, Faculty of Medicine, Jazan University, P.O. Box: 2349, Jazan, 82621, Saudi Arabia, Tel +00966562137711, Email [email protected]
Introduction: Inadequate sleep is linked to increased mental distress, and mental disorders often impair sleep quality, suggesting a bidirectional relationship. University students are particularly vulnerable to mental health issues due to academic pressures and related personal experiences. This study assesses sleep quality among university students in Jazan, Saudi Arabia, and its association with depression, anxiety, and stress levels.
Methods: A cross-sectional study was conducted among university students in online settings. The questionnaire collected demographic data, assessed anxiety, depression, and stress using the DASS-21, and measured sleep quality with the Pittsburgh Sleep Quality Index (PSQI). Statistical significance was tested using either Chi-squared tests or Fisher’s exact tests and followed up by logistic regression to calculate the odds of poor sleep quality among the students according to the levels of depression, anxiety, and stress.
Results: Of 508 participating students, 74% reported poor sleep quality. A statistically significant association was found between poor sleep quality and the presence of anxiety, depression, and stress (all P< 0.001). Abnormal stress levels were associated with higher odds of poor sleep 4.68 [2.8– 7.7], followed by higher odds of poor sleep quality among students with anxiety 3.62 [2.38– 5.52] and higher odds of poor sleep quality among students with depression 3.31 [2.1– 4.99]. All seven PSQI components were significantly associated with depression, anxiety, and stress (P< 0.05), except for sleep duration and stress, as well as sleep duration and depression, which had a marginally significant association (P=0.065). Depression showed a higher association with subjective sleep quality, daytime dysfunction, and sleep disturbances compared to stress and anxiety.
Conclusion: The majority of university students in this study experienced poor sleep quality, which was significantly associated with higher levels of depression, anxiety, and stress. The study highlights the critical importance of addressing poor mental health in university students and its strong correlation with sleep quality.
Keywords: sleep quality, depression, anxiety, stress, Jazan, Saudi Arabia
Introduction
Mental wellbeing is an important component of health and is often associated with how individuals learn, work, and contribute to their communities. An individual’s mental wellbeing is affected by multiple factors, such as coping skills, substance use, genetics, and socioeconomic determinants.1 Furthermore, according to the American College of Lifestyle Medicine, stress management, avoidance of risky substances, social connections, and restorative sleep are important components of a healthy lifestyle, in addition to good nutrition and physical activity.2
Current evidence indicates that sleep quality is correlated with mental wellbeing, and inadequate sleep is associated with increased risk of mental distress.3 Additionally, mental disorders influence sleep quality, and individuals suffering from stress,4,5 anxiety,6 and depression7 are at higher risk of sleep disturbances and poor sleep quality. This suggests that the association between mental wellbeing and sleep quality is bidirectional, meaning that mental health can affect sleep quality and that poor sleep quality is a risk factor for mental disorders.8,9 While the general association between mental health and sleep quality is well-established, further context-specific research is needed to fully understand the magnitude and contextual determinants of this association among university students in the Middle Eastern region.
One contextual factor that may impact mental wellbeing and sleep quality is education environment. The current evidence suggests that students are at higher risk of mental health problems if they have a negative educational environment and personal experiences relating to it, such as exposure to bullying and substance abuse.10 The prevalence of depression, anxiety, and stress among university students was reported to be high, and some students required access to relevant supportive services.11 Furthermore, academic performance also correlates with mental health, as impaired mental health has been indicated to impact academic performance.12,13
It was found that the impacts of an education environment on the mental wellbeing of students could be buffered by personal characteristics and lifestyle factors. Personality traits, coping strategies, and self-esteem levels were found to be internal characteristics that could alter mental wellbeing among university students.14–16 Additionally, lifestyle choices and social support also act as buffers for students’ mental wellbeing, as exercise, good sleep, and social support were reported to reduce the risk of developing depression, anxiety, and stress.17–20 This highlights the importance of addressing lifestyle factors, including sleep hygiene, among university students and their association with overall mental wellbeing.
Recent studies indicate that poor sleep quality is prevalent among university students and is highly associated with mental wellbeing.21–24 This emphasizes the importance of assessing sleep quality among university students and how it correlates with levels of depression, anxiety, and stress. Ajeebi et al reported in a previous investigation conducted to assess chorontype distribution among university students from Jazan, Saudi Arabia that only 27.4% were morning type and the remaining were either evening type or neither type.25 Ajeebi et al concluded that the university students exhibited certain lifestyle practices that can disturb sleeping chronotype such as dietary habits, caffeine consumption, and smoking and Khat chewing.
In addition to the identified disturbance of the chronotype among the university students, it can be postulated that quality of sleep can be affected. Additionally, disturbance of quality of sleep might be associated with negative impact on mental well-being of the students. Nonetheless, evidence concerning the magnitude of the association between quality of sleep and mental health among university students in the southwest of Saudi Arabia is currently limited. The current study assesses sleep quality in a sample of university students from Jazan, in the southwest of Saudi Arabia, and examines the association between levels of depression, anxiety, and stress with sleep quality.
Methods
Study Context
The current investigation utilized a cross-sectional design to recruit a sample of university students. The targeted sample was from Jazan University in the southwest of Saudi Arabia. The students were invited to participate in the study during February and March of 2023. The study setting was online. Approval to conduct the study was secured from the Standing Committee of Scientific Research at Jazan University (approval number: REC-44/04/365, dated November 14, 2022). Additionally, the study has been implemented while adhering to the principles of the Declaration of Helsinki. Participation in the study was voluntary, and students had the right to reject participation and to withdraw at any stage of the study.
Data Collection Tool
The data for the analysis was collected via a questionnaire comprised of three main components. The first component asked the students about their demographic data, including their age, gender, college, year of study, social status, diagnosis with a chronic disease, smoking and khat chewing habits, and latest GPA. The second component assessed levels of anxiety, depression, and stress using the DASS-21 questionnaire. The validity and reliability of the questionnaire were assessed with reference to Antony et al, revealing internal consistencies between 0.87 and 0.94 for depression, anxiety, and stress.26 Additionally, the validity of the DASS-21 questionnaire was tested by comparing the performance of the questionnaire to similar tools measuring depression and anxiety, such as the Beck Depression Inventory and Beck Anxiety Inventory, resulting in positive correlations between 0.51 and 0.85.27 The third component measured quality of sleep via the Pittsburgh Sleep Quality Index (PSQI). The questionnaire included seven main components measuring subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction. The validity and reliability of the PSQI were tested by Buysse et al, and it was concluded that a cut-off score of 5 could distinguish between good and poor sleep quality, with a sensitivity of 89% and a specificity of 85% respectively.28 To meet the language preference of the target population, the Arabic versions of the scales were used.27,29
Data Collection Process
Identification and recruitment of students were conducted within online settings. To secure an adequate sample, the assessment tool was converted to an online format using Google Forms. The online questionnaire was accompanied by a study information sheet that included the study’s objectives and assessment methods and enabled the participants to provide electronic informed consent. Those who refused to participate were directed elsewhere.
Convenient, non-random sampling was performed to recruit the study’s sample. The generated web link was shared on social media platforms, mainly WhatsApp, to recruit students who met the inclusion criteria. Participants were also encouraged to share the generated web link with their colleagues. Students who were registered with the university at the time of the study were included in the study. Additionally, those who were not students or were university alumni at the time of the recruitment were excluded from the study.
The sample size estimation was performed using Epi Info’s StatCal function for surveys to determine the prevalence of depression, anxiety, and stress of 50% with a 95% confidence interval and 5% margin of error. The resulting sample size was increased by 30% to 500 as a procedure to account for cases not meeting the inclusion criteria. Additionally, the estimated sample size was sufficiently powered to detect an association between abnormal mental health and poor sleep quality of a moderate effect size (odds ratio = 1.5) with a significance level of 5% and statistical power of 95%.
Data Analysis
Data analysis was conducted using the Statistical Package for the Social Sciences software (version 25). Descriptive analysis involved the calculation of frequencies and proportions to determine binary and categorical variables. Additionally, it also involved using means and standard deviations to summarize continuous variables. An evaluation of the presence of depression, anxiety, and stress was performed in line with the standardized scoring system described elsewhere.26 Scoring of the PSQI was also performed according to the standardized scoring system described elsewhere.28
A comparison was performed to compare demographic sample characteristics with quality of sleep. Additionally, the sleep quality scores for both the seven PSQI components and the global PSQI were examined according to the presence of depression, anxiety, and stress. For the purpose of conducting cross-tabulation to compare the distributions, age was dichotomized, with the mean age of 22 being the cut-off point. Additionally, the global PSQI was dichotomized based on a score of 5, where scores higher than 5 indicated poor sleep quality and scores lower than 5 indicated good sleep quality. Finally, depression, anxiety, and stress were dichotomized into normal and abnormal levels based on cut-off scores of 9, 7, and 14, respectively. Statistical significance was tested using either Chi-squared tests or Fisher’s exact tests. This was followed up by logistic regression to calculate the odds of poor sleep quality among the students according to the levels of depression, anxiety, and stress. Crude odds ratios (OR) and odds ratios adjusted for measured demographic characteristics were estimated to provide assessment of effect sizes and adjustments for confounders. A P value ≤0.05 was considered statically significant.
Results
A total of 508 students participated in the current study. The distribution of scores for quality of sleep among the sample according to the measured demographic characteristics is displayed in Table 1. In summary, 377 students (74%) suffered from poor sleep quality. The distribution of quality of sleep among the sample was not statistically significant in relation to the measured sample characteristics except for smoking. Higher rates of poor sleep quality were detected for current and previous smokers than for those who had never smoked (P=0.028).
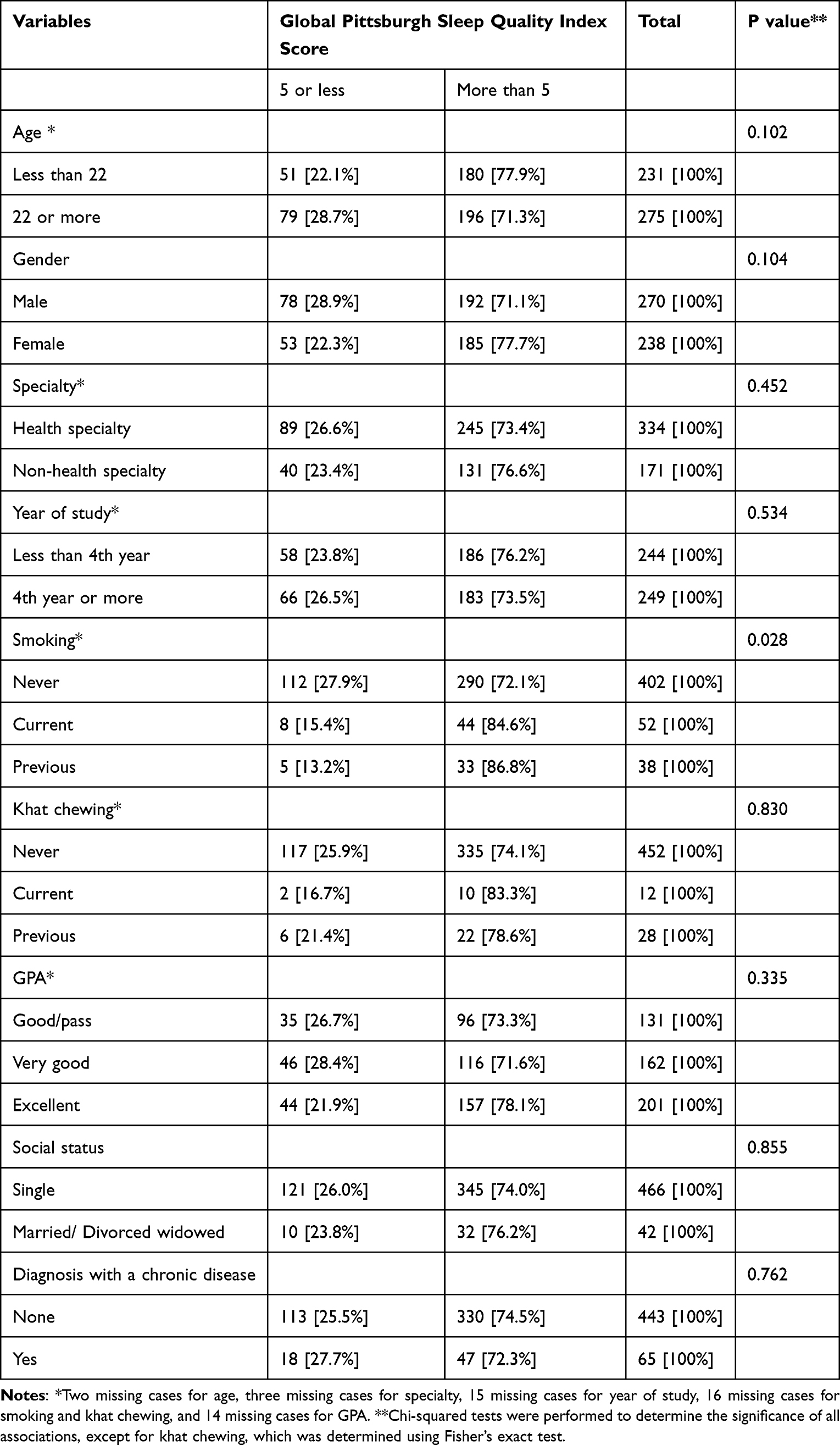 |
Table 1 Distribution of Global Pittsburgh Sleep Quality Index Scores According to the Demographic Variables Among the 508 University Students from Jazan, Saudi Arabia |
Table 2 displays the distribution of quality of sleep scores according to the presence of anxiety, depression, and stress. It is clear that poor sleep quality is more frequent in students with anxiety, depression, or stress (P<0.05). Stress appears to be more associated with poor sleep quality than depression and anxiety, as 89% of those with abnormal levels of stress suffered poor sleep quality.
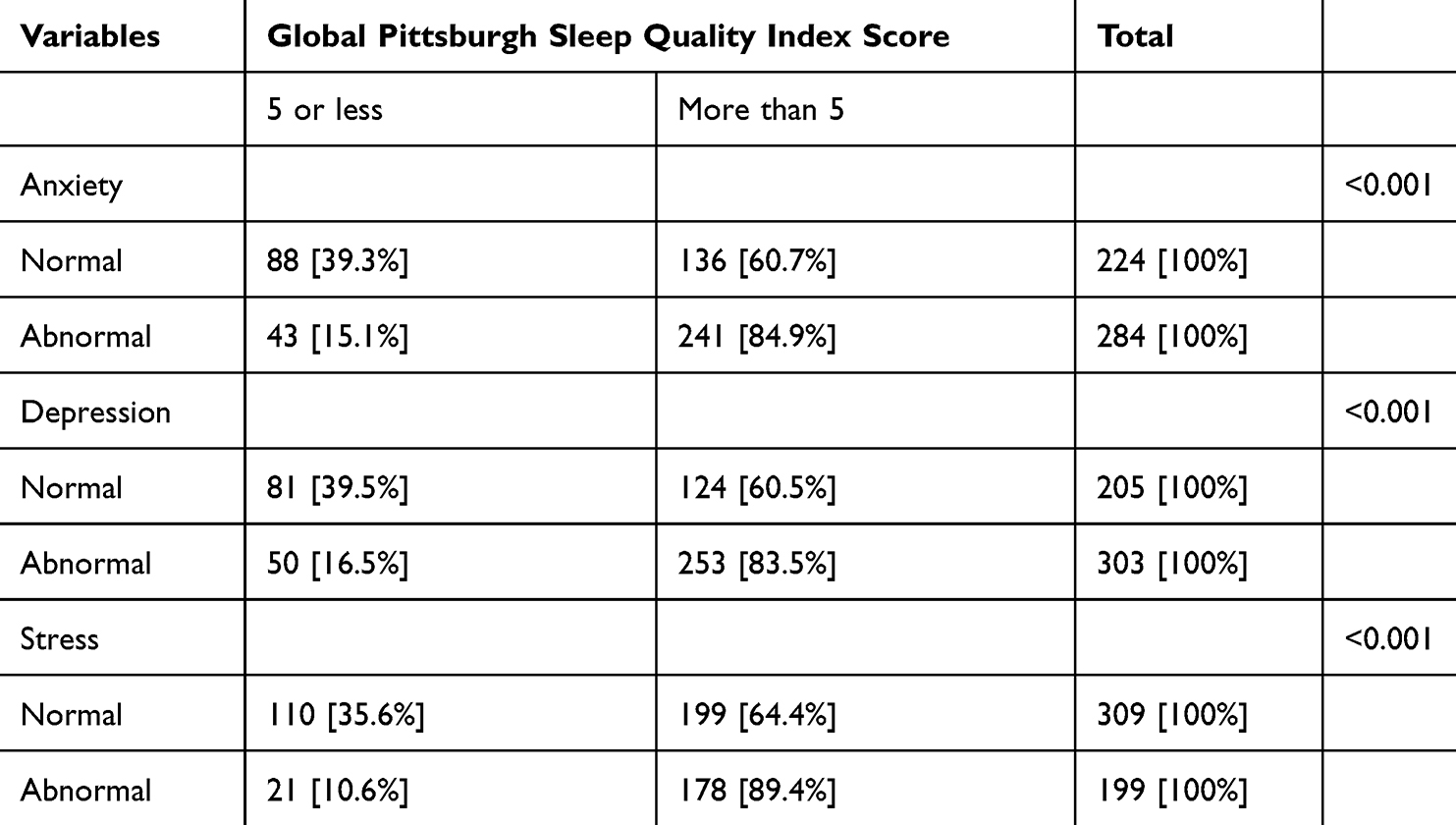 |
Table 2 Distribution of Global Pittsburgh Sleep Quality Index Scores According to the Presence of Anxiety, Depression, and Stress Among the 508 University Students from Jazan, Saudi Arabia |
Table 3 and Figure 1 present the distribution of the seven components of sleep according to the presence of anxiety, depression, and stress. Students with abnormal levels of anxiety, depression, and stress scored higher for all components, indicating positive correlation among the measured components. Nonetheless, the extent to which sleep quality components worsened varied according to mental health status.
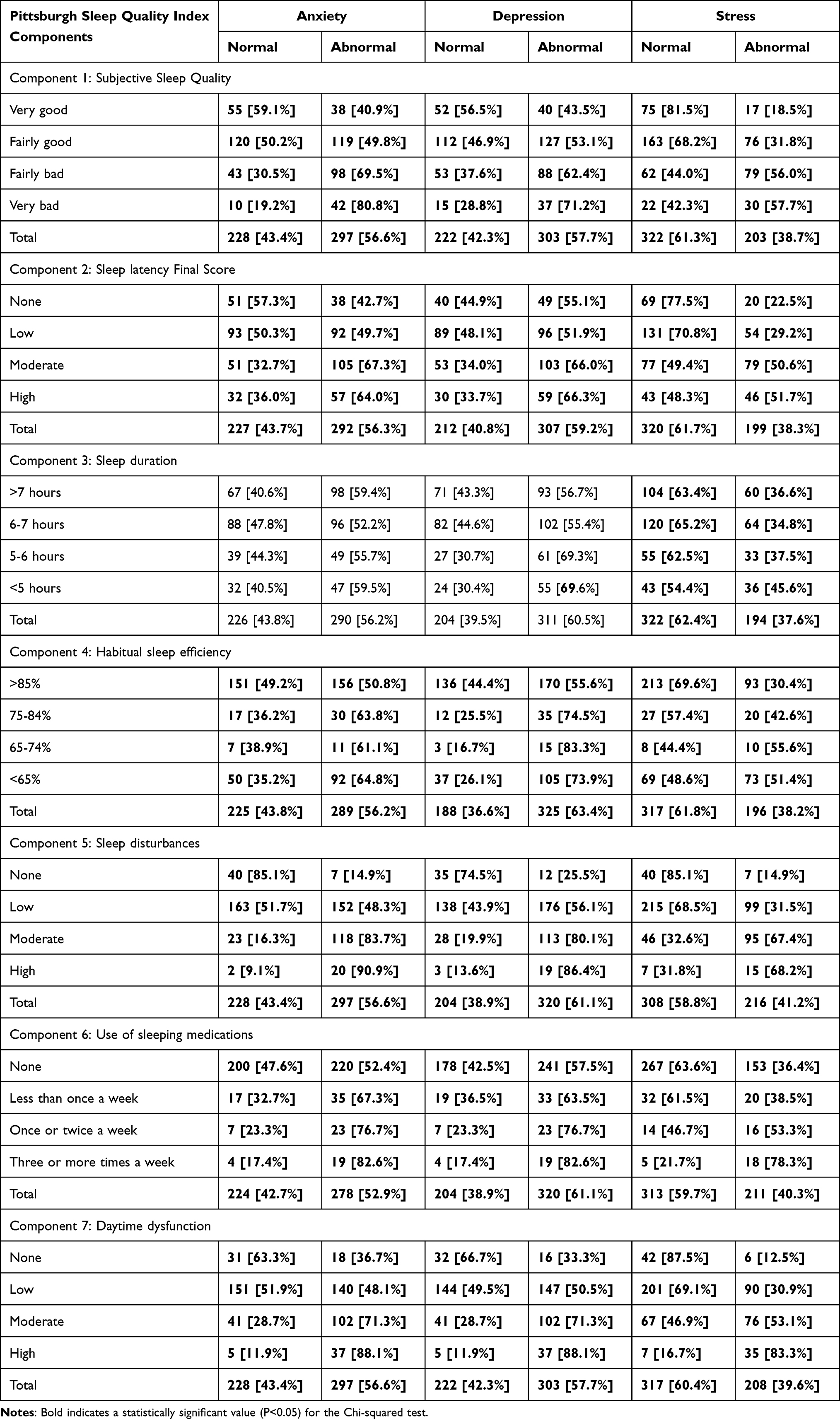 |
Table 3 Distribution of Pittsburgh Sleep Quality Index Components According to the Presence of Anxiety, Depression, and Stress Among the 508 University Students from Jazan, Saudi Arabia |
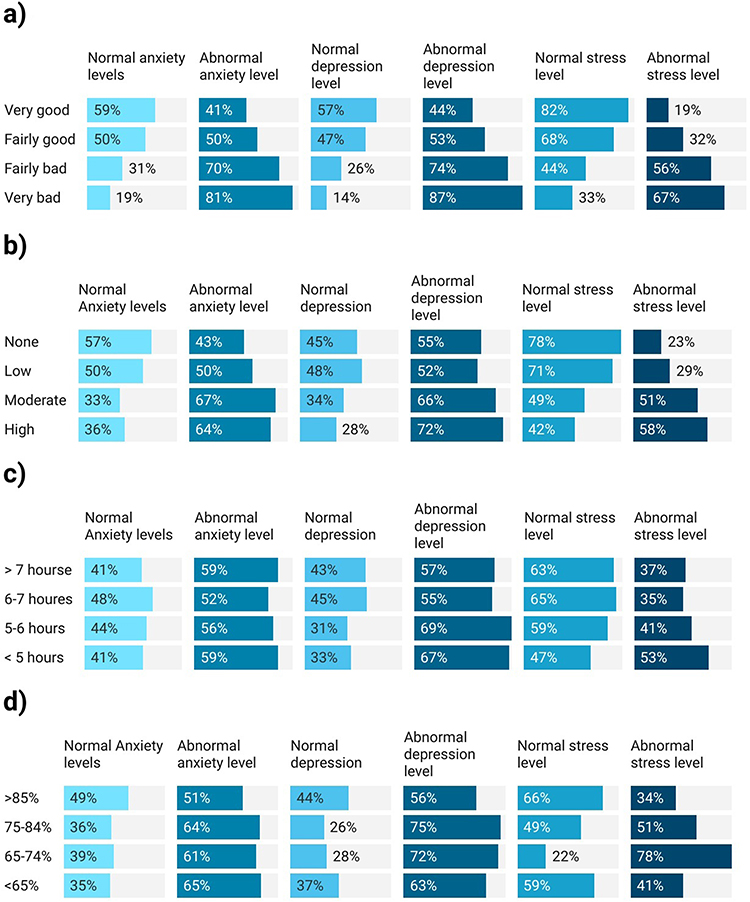 |
Figure 1 Continued. |
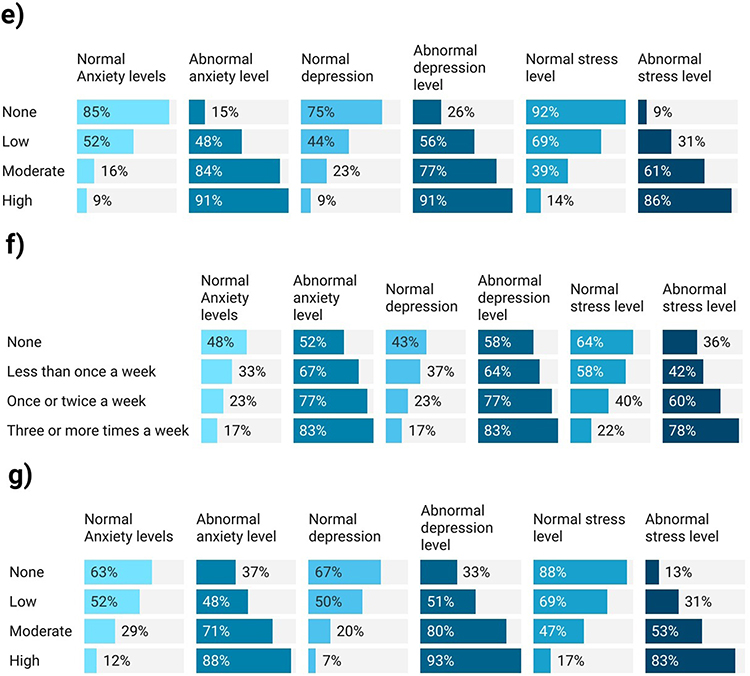 |
Figure 1 Distribution of Pittsburgh Sleep Quality Index components according to the presence of anxiety, depression, and stress among the 508 university students from Jazan, Saudi Arabia ((a) Subjective Sleep Quality, (b) Sleep Latency, (c) Sleep Duration, (d) Habitual Sleep Efficiency, (e) Sleep Disturbances, (f) Use of Sleeping Medications, (g) Daytime Dysfunction). |
All seven components were statistically significant in their association with depression, anxiety, and stress in the study sample (P<0.05), excluding the association between sleep duration and stress. Additionally, the association between sleep duration and depression was marginally significant (P=0.065). Observing the distributions, depression appears to have a higher association with subjective sleep quality in comparison to stress and anxiety. Similarly, daytime dysfunction and sleep disturbances were frequently present in those with abnormal anxiety or depression levels in comparison to other sleep quality components. Although the global PQSI score suggests that stress had a higher impact on sleep quality among this sample, the assessment of each component suggests that depression has a higher impact on certain sleep quality components.
Table 4 illustrates the findings of the univariate and multivariate logistic regression to estimate the odds of poor sleep quality as measured via PSQI according to the presence of abnormal levels of anxiety, depression, and stress. Abnormal stress levels were associated with higher odds of poor sleep 4.68 [2.8–7.7], followed by higher odds of poor sleep quality among students with anxiety 3.62 [2.38–5.52] and higher odds of poor sleep quality among students with depression 3.31 [2.1–4.99]. The associates remained statistically significant (p values <0.001) upon adjusting for the effect of age, gender, specialty, year of study, smoking, khat chewing, GPA, social status, and diagnosis with a chronic disease. This indicates the potential strong association between mental health and sleep quality among the university students despite the variation of other demographic and health characteristics.
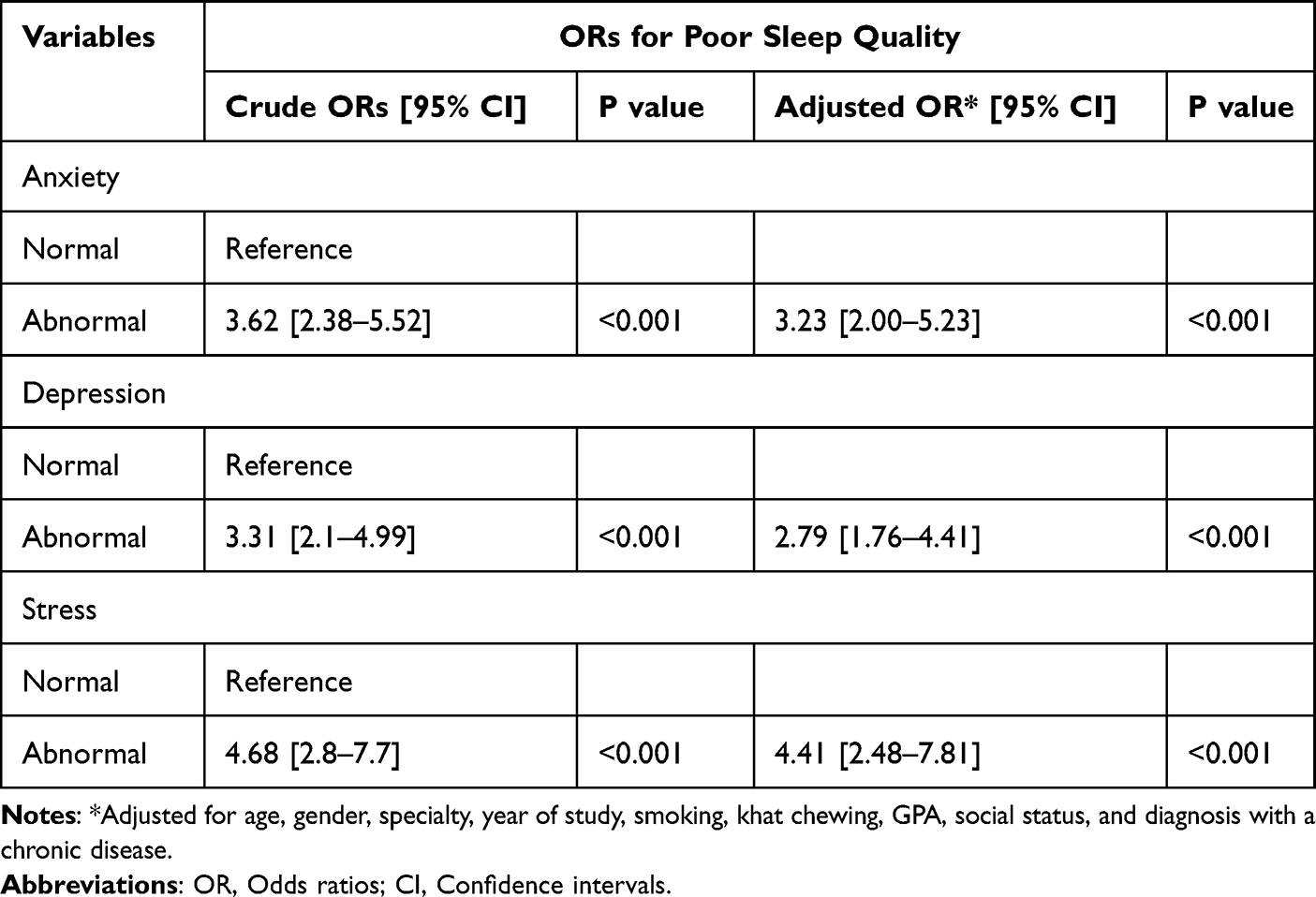 |
Table 4 Odds Ratios of Poor Sleep Quality Measured via Pittsburgh Sleep Quality Index According to the Presence of Anxiety, Depression, and Stress Among the 508 University Students from Jazan, Saudi Arabia |
Discussion
The current study measured sleep quality among university students from Saudi Arabia and evaluated the association between sleep quality and depression, anxiety, and stress. The findings indicate that the majority of the sample suffered from poor sleep quality (74%). Lower sleep quality was found in participants with abnormal levels of depression, anxiety, and stress. Poor sleep quality was more frequently reported among students with abnormal stress levels compared to depression and anxiety. Univariate analysis showed abnormal stress had the highest odds of poor sleep (OR=4.68), followed by anxiety (OR=3.62) and depression (OR=3.31), and these strong associations remained statistically significant (p<0.001) after adjusting for demographic and health characteristics. However, when assessing the associations between depression, anxiety, and stress and the components of the PSQI, the frequency of poor sleep quality varied depending on the presence of these mental health conditions. All seven components of sleep quality were statistically significant with regard to their correlations with depression, anxiety, and stress, excluding the relationship between sleep duration, anxiety, and depression.
The findings of the study can be compared to similar local or international investigations. In a similar cross-sectional study conducted by Sayed et al, which recruited a sample of 347 university medical students and used the PSQI to measure sleep quality, it was concluded that 46.6% of participants experienced moderate sleep quality.30 Additionally, it was concluded that gender and marital status were associated with sleep quality, though these were not measured in the current study. The main differences between the study conducted by Sayed et al and the current study are the different cut-off points for sleep quality and the study sample, which was restricted to medical students in Sayed et al’s study, whereas the current analysis involved students from different specialties.
In a similar study conducted by Almojali et al, with a sample of 756 medical students from Riyadh, Saudi Arabia, it was concluded that 76% of the students suffered poor sleep quality, which is similar to the findings of the current analysis.31 Additionally, Almojali et al found that students suffering from stress were more likely to suffer from low sleep quality, which is consistent with the findings of the current study. Similarly, in another study conducted in Abha, Saudi Arabia, involving a sample of 514 students, it was also concluded that 88% of the students suffered poor sleep quality and that sleep quality was not associated with demographic factors, similar to the findings of the current study.32
Similarly, international studies also indicate a positive correlation between the presence of depression, anxiety, and stress and poor sleep quality. A study conducted in Iran involving a sample of 471 freshman university students noted that risk of poor sleep quality was higher for those with depression or anxiety compared to for those without these conditions.33 A Turkish study involving a sample of 704 university students also reported similar findings, indicating positive correlations between depression, anxiety, and stress and poor sleep quality.34 In a Croatian study that involved a sample of 386 medical students, it was similarly concluded that depression, anxiety, and stress were correlated with poor sleep quality.21
The current study assessed the association between depression, anxiety, and stress and the seven components of the PSQI. It was noted that the associations varied according to each measured component. Nonetheless, studies that assess sleep quality components and mental health are limited. In a study that assessed the association between the seven components of sleep quality and the presence of depression, stress, and anxiety among a sample of 1552 participants from Portugal, Spain, and Brazil, it was concluded that all components were associated with the measured mental conditions except for subjective sleep quality.35 This is similar to the findings of the current study, except that all seven components were associated with depression, anxiety or stress, although sleep duration was only associated with the latter.
In a Chinese study that assessed the association between sleep pattern and duration and depression among a sample of 8775 adolescents, it was concluded that depression was associated with shorter periods of sleep.36 This is similar to the findings of the current study, with students having shorter periods of sleep among those suffering from abnormal levels of depression. However, the association detected in the current study exhibited marginal statistical significance (P=0.065), which can be partially explained by the smaller sample size of the current study in comparison to the Chinese study.
The findings of the current study, which illustrate a strong association between mental health and sleep quality among university students, have multiple clinical and public health implications. The presence of abnormal levels of depression, anxiety, and stress among the students suggests the presence of contextual factors influencing mental well-being of the university students. This necessitates the provision of supporting services within the university campus, such as better access to mental healthcare services and the provision of courses or workshops for stress management. Additionally, students can be offered access to sleep medicine clinics within the university healthcare services, which can then apply targeted interventions to improve sleep hygiene. Finally, a policy of faculty-targeted programs can be implemented to increase awareness among the university faculty about the importance of detecting signs of psychological distress and the possible association with impaired sleep quality.
The current study has several strengths and limitations. Its main strength lies in its recruitment of a sample of university students with varying levels of anxiety, depression, and stress to measure associations with sleep quality. Additionally, the assessment of these associations with sleep quality components provided further evidence of how mental health might be related to each sleep quality component. Its main limitation is the nature of the assessment tool used, which may have resulted in measurement bias. Nonetheless, the assessment was performed using validated tools with strong reliability. Since the sample was limited to university students, the generalizability is limited, meaning the study is less applicable to the general population and people of older ages. Additionally, selection bias might have been incurred by targeting students who have access to the internet and the WhatsApp application, potentially excluding those with no internet access or those without the application. Finally, the cross-sectional design inherently limits the ability to establish causality between sleep quality and mental health. This necessitates the use of future longitudinal research to provide stronger evidence for causal inference.
Conclusion
The findings of the current study revealed that the majority of the sample suffered from poor sleep quality. Lower sleep quality was associated with abnormal levels of depression, anxiety, and stress. All seven components of quality of sleep were statistically significant in their association with depression, anxiety, and stress, except for the association between sleep duration, anxiety, and depression. This study indicates the importance of addressing mental health issues in university students and how they correlate with sleep quality. Additionally, the findings suggest the need to conduct future longitudinal research to investigate specific mechanisms related to sleep quality and its contribution to the severity of mental health outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from any funding agency.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Mental health. 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
2. American College of Lifestyle Medicine. What is lifestyle medicine? Available from: https://lifestylemedicine.org/#:~:text=Applying%20the%20six%20pillars%20of%20lifestyle%20medicine%E2%80%94a,connections%E2%80%94also%20provides%20effective%20prevention%20for%20these%20conditions.
3. Blackwelder A, Hoskins M, Huber L. Effect of inadequate sleep on frequent mental distress. Prev Chronic Dis. 2021;18:E61. doi:10.5888/pcd18.200573
4. Zhang J, Xiang S, Li X, Tang Y, Hu Q. The impact of stress on sleep quality: a mediation analysis based on longitudinal data. Front Psychol. 2024;15:1431234. doi:10.3389/fpsyg.2024.1431234
5. Kalmbach DA, Anderson JR, Drake CL. The impact of stress on sleep: pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J Sleep Res. 2018;27(6):e12710. doi:10.1111/jsr.12710
6. Staner L. Sleep and anxiety disorders. Dialogues Clin Neurosci. 2003;5(3):249–258. doi:10.31887/DCNS.2003.5.3/lstaner
7. Jiang Y, Jiang T, Xu LT, Ding L. Relationship of depression and sleep quality, diseases and general characteristics. World J Psychiatry. 2022;12(5):722–738. doi:10.5498/wjp.v12.i5.722
8. Stafford A, Oduola S, Reeve S. How sleep in patients with serious mental illness is recorded and treated, and its impact on service engagement. Sleep Med. 2024;124:58–69. doi:10.1016/j.sleep.2024.09.002
9. Yasugaki S, Okamura H, Kaneko A, Hayashi Y. Bidirectional relationship between sleep and depression. Neurosci Res. 2025;211:57–64. doi:10.1016/j.neures.2023.04.006
10. Donato F, Triassi M, Loperto I, et al. Symptoms of mental health problems among Italian adolescents in 2017-2018 school year: a multicenter cross-sectional study. Environ Health Prev Med. 2021;26(1):67. doi:10.1186/s12199-021-00988-4
11. Bayram N, Bilgel N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc Psychiatry Psychiatr Epidemiol. 2008;43(8):667–672. doi:10.1007/s00127-008-0345-x
12. Chu T, Liu X, Takayanagi S, Matsushita T, Kishimoto H. Association between mental health and academic performance among university undergraduates: the interacting role of lifestyle behaviors. Int J Methods Psychiatr Res. 2023;32(1):e1938. doi:10.1002/mpr.1938
13. Zhang J, Peng C, Chen C. Mental health and academic performance of college students: knowledge in the field of mental health, self-control, and learning in college. Acta Psychol. 2024;248:104351. doi:10.1016/j.actpsy.2024.104351
14. Slimmen S, Timmermans O, Mikolajczak-Degrauwe K, Oenema A. How stress-related factors affect mental wellbeing of university students A cross-sectional study to explore the associations between stressors, perceived stress, and mental wellbeing. PLoS One. 2022;17(11):e0275925. doi:10.1371/journal.pone.0275925
15. Ahmad B, Ali chughtai S, Rauf A. Relationship between personality traits and mental health among graduate students. Pakistan Languages Humanities Rev. 2022;6(2):959–973. doi:10.47205/plhr.2022(6-II)81
16. Effandi K, Bahari MI, Haji Md Said HSR. Effect of emotional intelligence and personality traits on the psychological well-being of university students in Malaysia. Int J Learning Teaching Educ Res. 2023;22(9):592–616. doi:10.26803/ijlter.22.9.32
17. Roldán-Espínola L, Riera-Serra P, Roca M, et al. Depression and lifestyle among university students: a one-year follow-up study. Eur J Psych. 2024;38(3):100250. doi:10.1016/j.ejpsy.2024.100250
18. Ghali H, Ghammem R, Baccouche I, et al. Association between lifestyle choices and mental health among medical students during the COVID-19 pandemic: a cross-sectional study. PLoS One. 2022;17(10):e0274525. doi:10.1371/journal.pone.0274525
19. Bahri AA, Korairi HA, Gosadi IM, Othathi FA, Shami MO, Jareebi MA. The relationship between walking and depression, anxiety, and stress among a sample from Jazan, Saudi Arabia: a cross-sectional investigation. Medicine. 2022;101(38):e30718. doi:10.1097/MD.0000000000030718
20. Gosadi IM. Protective effect of exercise against depression, anxiety, and stress among university students based on their level of academic performance. Medicina. 2024;60(10):1706. doi:10.3390/medicina60101706
21. Vidović S, Rakić N, Kraštek S, et al. Sleep quality and mental health among medical students: a cross-sectional study. J Clin Med. 2025;14(7):2274. doi:10.3390/jcm14072274
22. Daud A, Hasmat N, Othman H. Association between sleep quality and mental illness among undergraduate students. Int J Case Scholars. 2023;6(3):7–14.
23. Moeis RM, Kuswiyanto RB, Tarigan R, Pandia V, Dhamayanti M. Correlation between adolescent mental health and sleep quality: a study in Indonesian rural areas during the COVID-19 pandemic. Int J Gen Med. 2023;16:3203–3210. doi:10.2147/IJGM.S416076
24. Verma P, Jani H, Bhanderi P, Patel B, Parlewar R. Association between sleep quality and mental health among medical students: a college based study in Himachal Pradesh, India. J Pharm Bioallied Sci. 2025;17(Suppl 1):S363–s365. doi:10.4103/jpbs.jpbs_310_25
25. Ajeebi Y, Oberi IA, Al-Hulaibi M, et al. Assessment of chronotype distribution among university students and its association with lifestyle characteristics and academic performance. Cureus. 2024;16(8):e67678. doi:10.7759/cureus.67678
26. Antony MM, Cox BJ, Enns MW, Bieling PJ, Swinson RP. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol Assess. 1998;10(2):176–181. doi:10.1037/1040-3590.10.2.176
27. Ali AM, Ahmed A, Sharaf A, Kawakami N, Abdeldayem SM, Green J. The Arabic version of the depression anxiety stress scale-21: cumulative scaling and discriminant-validation testing. Asian J Psychiatr. 2017;30:56–58. doi:10.1016/j.ajp.2017.07.018
28. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
29. Suleiman K, Yates B, Berger A, Pozehl B, Meza J. Translating the pittsburgh sleep quality index into Arabic. West J Nurs Res. 2009;32(2):250–268. doi:10.1177/0193945909348230
30. Sayed AI, Mobarki SJ, Oberi IA, et al. Effect of stress on sleep quality among medical students: a cross-sectional study at Jazan University, Saudi Arabia. Ann Afr Med. 2024;23(4):586–593. doi:10.4103/aam.aam_7_24
31. Almojali AI, Almalki SA, Alothman AS, Masuadi EM, Alaqeel MK. The prevalence and association of stress with sleep quality among medical students. J Epidemiol Glob Health. 2017;7(3):169–174. doi:10.1016/j.jegh.2017.04.005
32. Khaled A, Almaghaslah D, Siddiqua A, Kandasamy G, Orayj K. Impact of sleep quality on academic achievements of undergraduate medical students: a cross-sectional study from Saudi Arabia. BMC Med Educ. 2025;25(1):59. doi:10.1186/s12909-025-06664-3
33. Garmabi M, Andishmand Z, Naderi F, et al. The prevalence of depression and anxiety and its association with sleep quality in the first-year medical science students. Depression Res Treatment. 2024;2024:7102081. doi:10.1155/2024/7102081
34. Dülger H, Ayaz-Alkaya S. Prevalence of stress, anxiety, depression, and sleep quality among young adults in Turkiye: a cross-sectional study. J Eval Clin Pract. 2025;31(1):e70002. doi:10.1111/jep.70002
35. Del Rio João KA, de Jesus SN, Carmo C, Pinto P. Sleep quality components and mental health: study with a non-clinical population. Psychiatry Res. 2018;269:244–250. doi:10.1016/j.psychres.2018.08.020
36. Zhang X, Dou Z, Yang F, Luo L, Yang J. Exploring the relationship between sleep patterns and depression among Chinese middle school students: a focus on sleep quality vs. sleep duration. Front Public Health. 2024;12:1383884. doi:10.3389/fpubh.2024.1383884
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19
Hamka, Suen MW, Ramadhan YA, Yusuf M, Wang JH
Psychology Research and Behavior Management 2022, 15:3013-3025
Published Date: 17 October 2022
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mental Health, Sleep, and Physical Activity Among Young Saudi Women During Ramadan: A Comparative Cohort Study
Balasubramanian K, Sanjeevi RR, Alshehri MM, Alothman SA
Nature and Science of Sleep 2026, 18:583610
Published Date: 11 June 2026