Back to Journals » Journal of Inflammation Research » Volume 19
A Prognostic Model Based on Immune–Inflammatory–Nutritional Indicators for 28-Day Mortality in Sepsis Patients with Acute-on-Chronic Liver Failure
Authors Xin Q
Received 11 December 2025
Accepted for publication 6 February 2026
Published 16 February 2026 Volume 2026:19 505559
DOI https://doi.org/10.2147/JIR.S505559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xin Du
Qi Xin
Department of Emergency Surgery, Shaanxi Provincial People’s Hospital, Xi’an, 710068, People’s Republic of China
Correspondence: Qi Xin, Shaanxi Provincial People’s Hospital, 256 Youyi West Road, Xi’an, 710068, People’s Republic of China, Tel +86-029-85251331, Fax +86-029-85236987, Email [email protected]
Background: Sepsis and acute-on-chronic liver failure (ACLF) constitute a severe clinical interaction, resulting in alarmingly high short-term mortality rates. Current prognostic models, such as the Sequential Organ Failure Assessment (SOFA) score, lack specificity for this distinct patient group. The pathophysiology of both conditions is critically influenced by immune dysfunction, systemic inflammation, and nutritional deficits. This study sought to develop and validate a novel prognostic model that integrates immune-inflammatory-nutritional indicators to enhance the prediction of 28-day mortality in sepsis patients with ACLF.
Methods: A retrospective cohort study was conducted involving 246 sepsis patients with ACLF admitted to Shaanxi Provincial People’s Hospital. Participants were randomly divided into a training cohort (n=185) and a validation cohort (n=61). Least absolute shrinkage and selection operator (LASSO) regression and multivariate logistic regression analyses were utilized to identify independent predictors and construct a prognostic nomogram. The model’s efficacy was thoroughly evaluated based on its discriminative capacity (area under the receiver operating characteristic curve, AUC), calibration (calibration curves), and clinical utility (decision curve analysis, DCA).
Results: The 28-day mortality rate was observed to be 37.0%. Six independent predictors were identified and integrated into the nomogram: hepatic encephalopathy, D-dimer levels, platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), ALBI grade, and the systemic inflammation response index (SIRI). The nomogram exhibited exceptional discriminative ability, with AUC values of 0.907 and 0.862 in the training and validation cohorts, respectively, significantly surpassing the performance of the SOFA score (AUCs: 0.651 and 0.624). Calibration curves indicated excellent concordance between predicted and observed outcomes, while DCA confirmed a substantial clinical net benefit across a broad range of threshold probabilities.
Conclusion: We have successfully developed and validated a robust nomogram that utilizes routinely available immune-inflammatory-nutritional indicators to provide individualized risk estimation of 28-day mortality in sepsis patients with ACLF. This model represents an advanced prognostic instrument when compared to traditional scoring systems, with the potential to enable early detection of high-risk patients and inform individualized therapeutic interventions.
Keywords: sepsis, acute-on-chronic liver failure, nomogram, immune-inflammatory-nutritional indicators, mortality
Introduction
Sepsis, characterized as a life-threatening organ dysfunction resulting from a dysregulated host response to infection, continues to be a predominant cause of mortality in intensive care units globally.1 The clinical progression of sepsis is significantly exacerbated in patients with pre-existing chronic liver disease, leading to the development of acute-on-chronic liver failure (ACLF).2 ACLF is defined by acute hepatic decompensation, severe systemic inflammation, and elevated short-term mortality due to failures in extrahepatic organs.3 The intersection of sepsis and ACLF establishes a detrimental cycle: sepsis frequently triggers ACLF, while the immunocompromised condition associated with ACLF increases susceptibility to severe and recurrent infections.4–6 Furthermore, research indicates a strong association between sepsis and the onset of ACLF, particularly in patients with hepatitis B-related ACLF, where infections substantially elevate disease severity and mortality rates.7 This detrimental synergy contributes to 28-day mortality rates that can surpass 42.9%, posing a significant challenge to clinicians.5
Precise risk stratification is essential for optimizing resource allocation, informing clinical decisions, and potentially guiding novel interventions. The Sequential Organ Failure Assessment (SOFA) score is a widely utilized and validated instrument for evaluating organ dysfunction and predicting mortality in critically ill patients, including those with sepsis.1 Nevertheless, its application in the specific and complex cohort of sepsis patients with ACLF presents pronounced limitations. As a general critical illness score, the SOFA system does not explicitly incorporate crucial liver-specific prognostic determinants, such as the degree of portal hypertension, synthetic liver function, or nuanced indicators of hepatic encephalopathy severity.8,9 More importantly, it fails to capture the essential dynamics of the immune-inflammatory and nutritional axes—dimensions increasingly recognized as pivotal drivers of pathophysiology and outcomes in this unique population.10–13 Other liver-specific scoring systems (eg, Child-Pugh, MELD) also have inherent limitations in this context; they often rely on subjective clinical assessments, may not fully reflect acute-on-chronic pathophysiology, and similarly lack integration of the systemic inflammatory and immunological dysregulation that is central to the sepsis-ACLF synergy.
It is important to acknowledge the inherent methodological considerations and potential limitations of prognostic model development based on routinely collected clinical data, such as electronic medical records. These include challenges related to data completeness (missing values), heterogeneity in measurement timing and clinical documentation, and the potential for unmeasured confounding factors—all of which are common in observational, retrospective cohort studies and must be considered when interpreting model development and performance. Despite these challenges, leveraging such real-world data remains invaluable for developing pragmatic, clinically applicable tools. Immune-inflammatory-nutritional indicators are particularly pertinent in this context. Metrics such as the neutrophil-to-lymphocyte ratio (NLR) and the systemic immune-inflammation index (SII) provide insights into the balance between pro-inflammatory and immunocompetent cells.14,15 Nutritional markers, including the prognostic nutritional index (PNI), serve not only as indicators of nutritional reserves but also as significant predictors of immune competence and overall physiological resilience.16–18 The albumin-bilirubin (ALBI) grade offers an objective and refined assessment of liver functional reserve, which, in certain contexts, surpasses the Child-Pugh score.19–22 These immune-inflammatory-nutritional indicators have demonstrated prognostic value across a range of diseases, including cancers and liver failure.17,18,23,24 Nonetheless, there is a current lack of a comprehensive model that integrates this multifaceted immune-inflammatory-nutritional information specifically for predicting mortality in the high-risk cohort of sepsis patients with ACLF.
Therefore, the primary objective of this study was to develop and validate a novel, user-friendly prognostic nomogram based on a panel of readily available immune-inflammatory-nutritional indicators. We hypothesize that such an integrated model would provide a more accurate and individualized prediction of 28-day mortality than existing scores, thereby offering a valuable tool for improving patient management and outcomes in this complex population.
Materials and Methods
Study Design
This retrospective, single-center cohort study was conducted at Shaanxi Provincial People’s Hospital. We systematically screened all adult patients (aged 18 years and older) who were admitted to the intensive care unit (ICU) from January 2020 to October 2025. The study protocol received approval from the Institutional Review Board of Shaanxi Provincial People’s Hospital (Approval No: 2025R082). This study is reported in accordance with the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) statement.
Population
The study population comprised adult patients (≥18 years) admitted to the ICU with concurrent diagnoses of sepsis and ACLF. The definition of sepsis adhered to the Sepsis-3 International Consensus, which requires a suspected or confirmed infection in conjunction with an acute increase of 2 or more points in the SOFA score.1 The diagnosis of ACLF was based on criteria established by the Chinese Medical Association,25 characterized by an acute or subacute exacerbation of pre-existing chronic liver disease. Key diagnostic criteria included significant jaundice, defined as a serum total bilirubin (TBIL) level of ≥ 171 μmol/L or a daily increase of ≥ 17.1 μmol/L, and severe coagulopathy, indicated by a prothrombin time activity (PTA) of ≤ 40% or an international normalized ratio (INR) of ≥ 1.50. The exclusion criteria were: (1) < 18 years old (n=1); (2) The length of stay in ICU was less than 24 hours (n=6); (3) Presence of severe chronic kidney disease, cardiopulmonary disease, or other significant comorbidities; (4) Hepatocellular carcinoma or other malignant tumors; (5) Patients after liver transplantation.
Data Collection and Variable Definitions
Clinical and laboratory data were systematically extracted from the hospital’s electronic medical records within the first 24 hours of admission. Collected variables included: (1) Demographics and Comorbidities: Age, gender, and pre-existing conditions (eg, hypertension, diabetes); (2) Vital Signs: Body temperature, heart rate, respiratory rate, and mean arterial pressure. (3) Chronic Liver Disease Etiology and Complications: Presence of hepatitis B virus (HBV) infection, decompensated cirrhosis, hepatic encephalopathy (HE), esophagogastric variceal bleeding (EVB), ascites, and acute kidney injury (AKI). (4) Laboratory Parameters: Routine hematological, biochemical, and coagulation profiles; (5) Clinical Scores: SOFA score was calculated for all patients; (6) Immune-Inflammatory-Nutritional Indicators: The following composite scores were calculated from the baseline laboratory data: ALBI Grade: Calculated as (log10 Bilirubin (μmol/L) × 0.66) – (Albumin (g/L) × 0.085); NLR: Absolute neutrophil count/Absolute lymphocyte count; Platelet-to-Lymphocyte Ratio (PLR): Platelet count/Absolute lymphocyte count; Lymphocyte-to-Monocyte Ratio (LMR): Absolute lymphocyte count/Absolute monocyte count; PNI: Calculated as Albumin (g/L) + 5 × (Absolute lymphocyte count (×109/L)); SII: (Platelet count × Neutrophil count)/Lymphocyte count; Systemic Inflammation Response Index (SIRI): (Neutrophil count × Monocyte count)/Lymphocyte count. Patients were classified into three ALBI grades: Grade 1 (≤ −2.60), Grade 2 (> −2.60 to ≤ −1.39), and Grade 3 (> −1.39). All data were independently reviewed by two senior critical care physicians. In case of any disagreement, a third expert would make the final decision.
Sepsis-Specific Data
To characterize the infectious and systemic aspects of sepsis, we collected the following additional information: (1) Primary infection focus, categorized as pulmonary, intra-abdominal, urinary tract, bloodstream, soft tissue, or other; (2) Initial antibiotic therapy, recorded as appropriate (defined as administration of antibiotics covering the identified or suspected pathogen(s) within 24 hours of sepsis recognition) or inappropriate/delayed; (3) Incidence of new extrahepatic organ failures developing, such as heart failure (HF), respiratory failure (RF) and acute renal failure (ARF).
Data Completeness
After applying the exclusion criteria—specifically, the removal of patients lacking complete key data—the final analysis included a cohort of 635 patients, forming a complete-case dataset. A thorough review verified that within this group, all demographic, clinical, laboratory, and immune-inflammatory-nutritional predictors outlined in the Data Extraction section contained no missing values. As a result, no data imputation techniques were necessary or employed.
Sample Size Consideration
With 4–6 potential modeling predictors reported in previous studies and considering the 35% 28-day mortality from preliminary investigation, we estimated that 114–171 patients (with 40–60 28-day mortality outcome) were needed for sufficient precision of model construction to follow the principle of at least ten outcome events per variable in the regression analysis.
Statistical Analysis
The entire cohort was randomly divided into a training set, comprising 75% of the patients, for the purpose of model development, and a validation set, consisting of 25% of the patients, for internal validation. Continuous variables were reported as medians with interquartile ranges (IQR) and analyzed using the Mann–Whitney U-test. Categorical variables were presented as frequencies (percentages) and analyzed using either the Chi-square test or Fisher’s exact test, as appropriate. Survival analysis was performed using the Kaplan-Meier method to estimate the 28-day survival probability over time. Within the training set, univariate logistic regression analysis was conducted to evaluate the association between each variable and 28-day mortality. Variables demonstrating a P-value of less than 0.05 were identified as potential predictors for further analysis. To address multicollinearity and identify the most pertinent features, the least absolute shrinkage and selection operator (LASSO) method was employed on the significant variables from the univariate analysis. Variables with non-zero coefficients from the LASSO regression were subsequently included in a multivariate logistic regression model to construct the final prediction model. It is important to note that all variable selection steps (univariate analysis, LASSO regression, and subsequent multivariable logistic regression) were performed exclusively on the training cohort. A visual nomogram was developed based on the final multivariate logistic regression model to serve as a user-friendly tool for individualized risk prediction. The predictive accuracy of the nomogram was assessed by calculating the Area Under the Receiver Operating Characteristic Curve (AUC) for both the training and validation datasets. Model calibration was evaluated through calibration curves, which depicted the relationship between predicted probabilities and observed mortality frequencies. Decision Curve Analysis (DCA) was conducted to assess the clinical net benefit of the nomogram across various threshold probabilities within both cohorts.
All statistical analyses were executed using SPSS Statistics (version 26.0) and R software (version 4.2.1), with a two-sided P-value of less than 0.05 deemed statistically significant.
Result
Basic Characteristics
A total of 246 sepsis patients with ACLF were included in this study, with 91 (37.0%) experiencing 28-day mortality (Figure 1). Furthermore, the cohort was randomly divided into a training set (n = 185, 75%) and a validation set (n = 61, 25%). As summarized in Table 1, the two groups were well-balanced in terms of demographic characteristics, vital signs, comorbidities, laboratory parameters, immune-inflammatory-nutritional indicators, and clinical outcomes (all P > 0.05). The median age of the overall population was 54 years (IQR: 46–64), with 132 females (53.7%) and 114 males (46.3%). Similar distributions were observed in both the training and validation sets. The overall 28-day survival probability was estimated using Kaplan-Meier analysis. As shown in Supplementary Figure S1, with a cumulative survival probability of 63.0% at 28 days (consistent with the overall mortality rate of 37.0%). The training set contained 65 events (35.1% mortality) and the validation set contained 26 events (42.6% mortality). The event-per-predictor (EPV) ratio in the training set was approximately 10.8, meeting the common threshold of ≥10 EPV recommended for stable multivariable logistic regression model development.
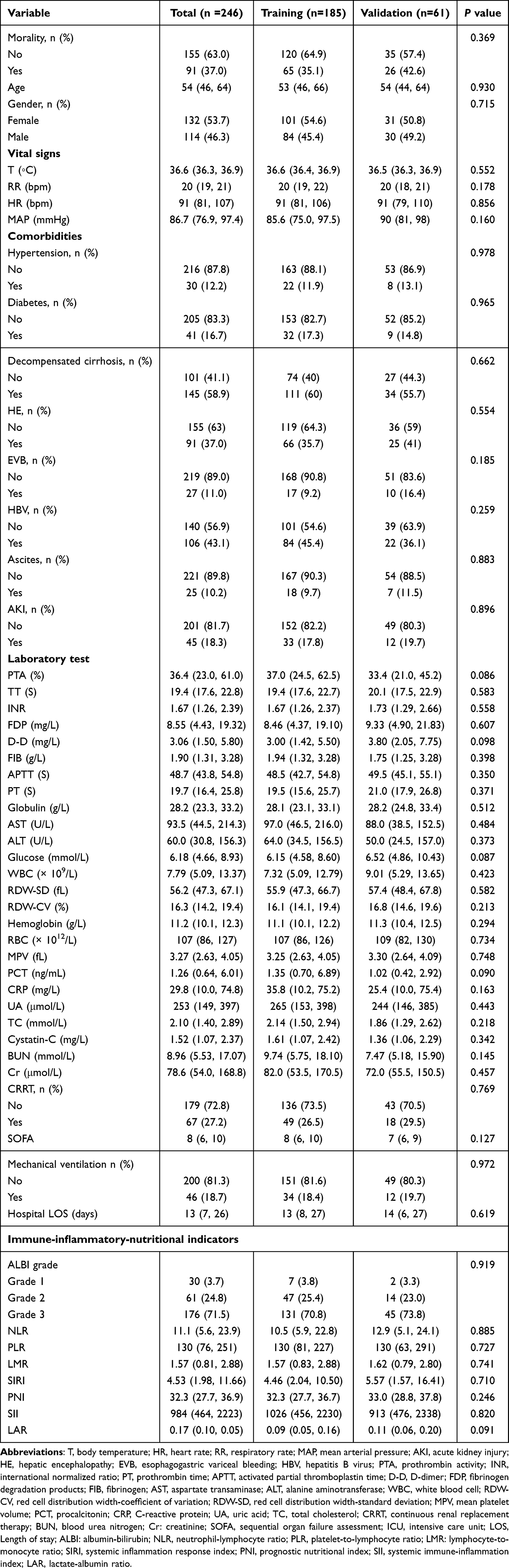 |
Table 1 Baseline Characteristics of Sepsis Patient with Acute-on-Chronic Liver Failure |
 |
Figure 1 The flowchart of patient selection from the Shaanxi Provincial People’s Hospital. |
Sepsis Characteristics and Organ Failures
The primary foci of infection among the 246 patients were: pulmonary (n=98, 39.8%), intra-abdominal (n=74, 30.1%), urinary tract (n=28, 11.4%), bloodstream (n=25, 10.2%), soft tissue (n=10, 4.1%), and other (n=11, 4.5%). Appropriate initial antibiotic therapy was administered to 72.4% (n=178) of patients. In addition to hepatic failure, the most prevalent organ failures were RF in 17.5% (n=43), HF in 24.8% (n=61), and ARF in 9.3% (n=23). A detailed breakdown is provided in Supplementary Table S1.
Univariate Analysis
Univariate logistic regression analysis was performed in the training cohort to identify potential predictors of 28-day mortality (Table 2). Several variables were significantly associated with increased mortality, including HE (OR = 3.349, 95% CI: 1.773–6.329), EVB (OR = 7.250, 95% CI: 2.256–23.299), D-D (OR = 1.125, 95% CI: 1.053–1.202), APTT (OR = 1.039, 95% CI: 1.012–1.067), PT (OR = 1.102, 95% CI: 1.054–1.152), WBC (OR = 1.071, 95% CI: 1.018–1.128), and SOFA score (OR = 1.245, 95% CI: 1.096–1.461). Conversely, globulin (OR = 0.950, 95% CI: 0.913–0.988), and PTA (OR = 0.986, 95% CI: 0.973–1.000) were inversely associated with mortality. Among immune-inflammatory-nutritional indicators, NLR (OR = 1.063), PLR (OR = 1.002), SIRI (OR = 1.133), SII (OR = 1.000), and LAR (OR = 140.856) were significant positive predictors, while LMR (OR = 0.374) and PNI (OR = 0.883) were protective factors.
 |
Table 2 Univariate Analysis of Predictive Variables of the 28-Day Mortality in the Training Cohort |
Variable Selection and Model Development
Based on the results from the training cohort, a LASSO regression analysis was performed to address multicollinearity among the predictors identified as significant (P < 0.05) in the univariate analysis, among which the optimal lambda was selected through 10-fold cross-validation (Figure 2). The following variables were retained for further analysis: HE, EVB, PTA, D-D, PT, globulin, ALBI, PLR, LMR, SIRI, and LAR. Multivariate logistic regression in the training cohort (Table 3) identified HE (OR = 6.100), D-D (OR = 1.160), PLR (OR = 1.001), LMR (OR =0.690), ALBI (OR = 5.901), and SIRI (OR = 1.078) as independent predictors of 28-day mortality. These variables were incorporated into a prognostic nomogram for individualized risk prediction (Figure 3).
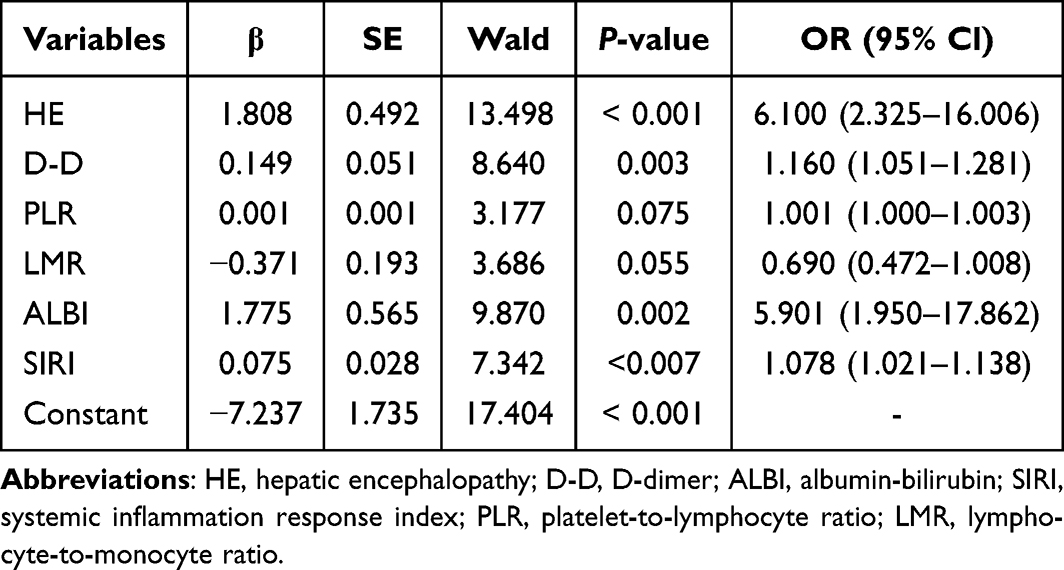 |
Table 3 Multivariate Logistic Regression Analysis in the Training Cohort |
 |
Figure 2 Clinical Predictor Selection by LASSO Regression. (A) The regularization paths show how feature coefficients shrink as the penalty parameter (lambda) increases. (B) Ten-fold cross-validation curve. The optimal lambda (lambda.1se) was selected using the one-standard-error rule, which favors a simpler model while maintaining predictive accuracy, resulting in the final set of predictors. |
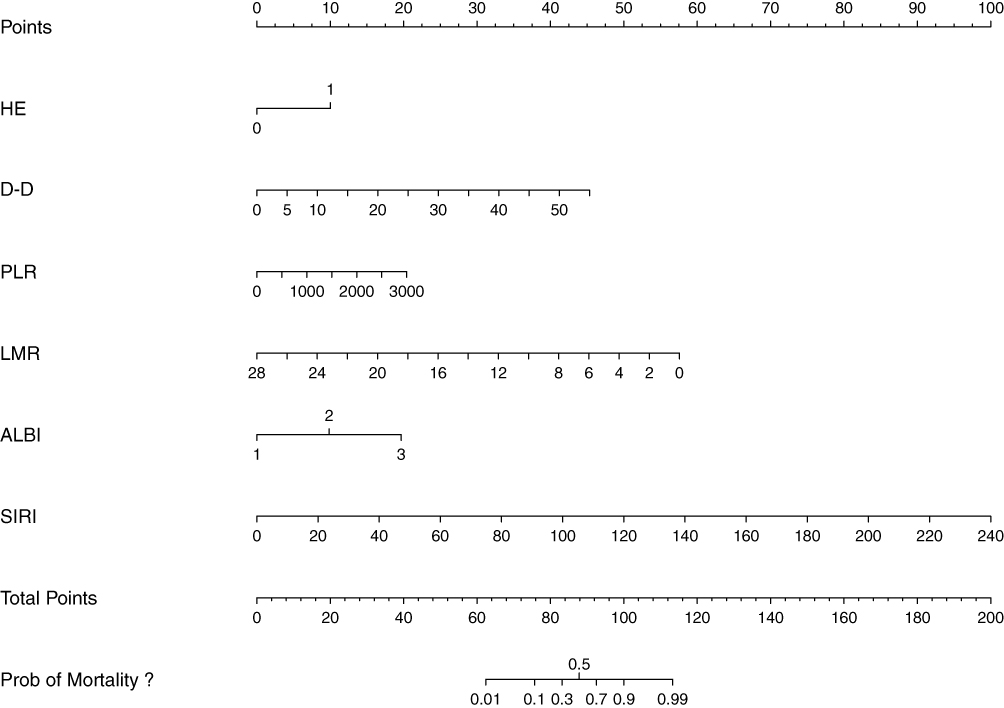 |
Figure 3 Prognostic nomogram for 28-day mortality in sepsis patients with ACLF. Abbreviations: HE, hepatic encephalopathy; D-D, D-dimer; ALBI, albumin-bilirubin; SIRI, systemic inflammation response index; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio. |
Model Validation and Performance
The predictive accuracy of the nomogram was evaluated using ROC curve analysis. In the training cohort, the area under the curve (AUC) was 0.907, while in the validation cohort, the AUC was 0.862 (Figure 4). The model demonstrated superior discriminative ability compared to the SOFA score (training AUC = 0.651, validation AUC = 0.624). Calibration curves showed good agreement between predicted and observed outcomes in both cohorts (Figure 5). Decision curve analysis (DCA) further confirmed the clinical utility of the nomogram, indicating a net benefit across a wide range of threshold probabilities.
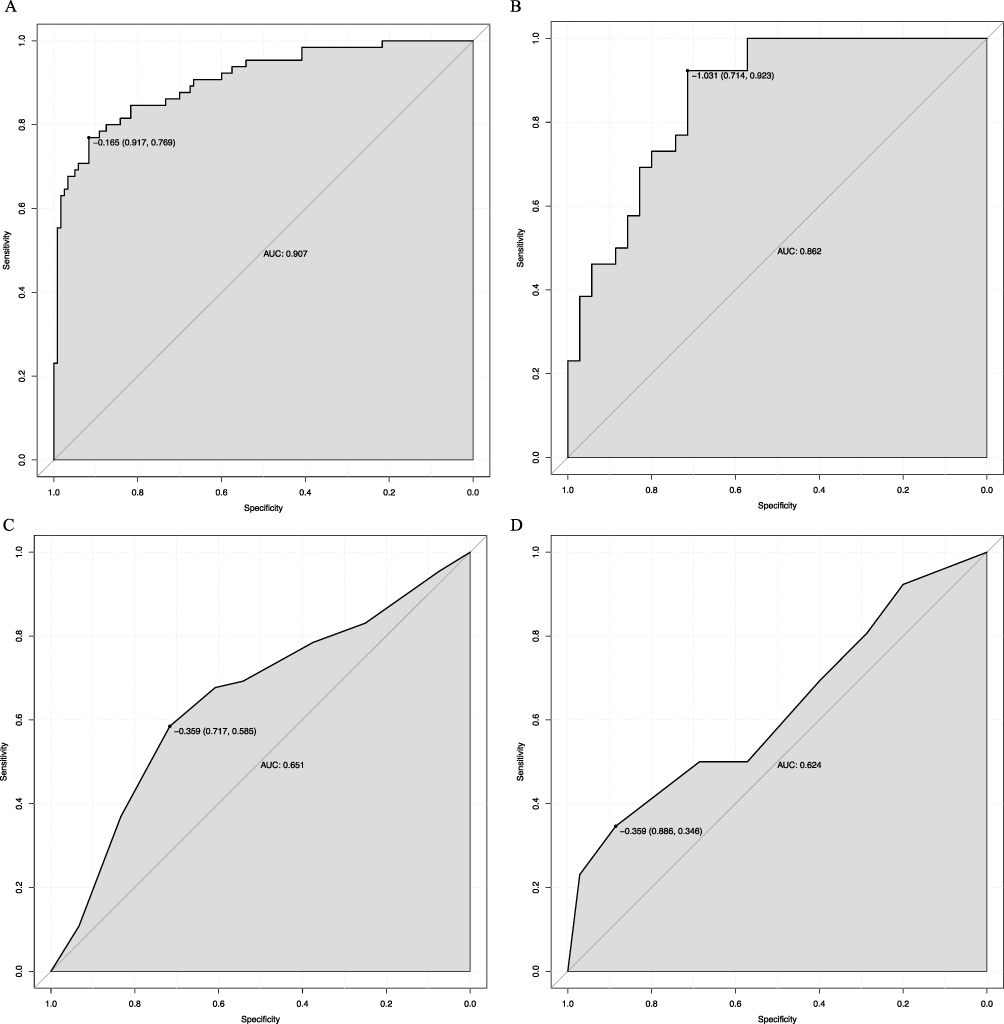 |
Figure 4 Predictive Performance of the Nomogram and SOFA Score. ROC curves evaluating the prediction of 28-day mortality in sepsis patients with ACLF. The nomogram demonstrated AUC of 0.907 in the training cohort (A) and 0.862 in the validation cohort (B). In comparison, the SOFA score yielded AUCs of 0.651 (C) and 0.624 (D) in the training and validation cohorts, respectively. Abbreviations: ROC, receiver operating characteristic; AUC, area under the receiver operating characteristics curve; SOFA, sequential organ failure assessment. |
 |
Figure 5 Model Calibration and Clinical Utility. (A and B) Calibration curves depict the agreement between the nomogram-predicted probability of 28-day mortality and the observed outcome in the training and validation cohorts, respectively. The diagonal dashed line represents the ideal fit. (C and D) DCA evaluates the clinical net benefit of the nomogram across different threshold probabilities in the training and validation sets. Abbreviation: DCA, Decision curve analysis. |
Discussion
In this study, we developed and rigorously validated an innovative prognostic nomogram that integrates hepatic encephalopathy, D-dimer, and four immune-inflammatory-nutritional indicators (PLR, LMR, ALBI and SIRI) to predict 28-day mortality in sepsis patients with ACLF. The model exhibited exceptional discriminative ability, with AUC values exceeding 0.86 in both cohorts, significantly surpassing the performance of the SOFA score. Its robust performance was further substantiated by excellent calibration and a clear net clinical benefit across a wide range of risk thresholds, highlighting its potential for immediate clinical application.
The prognostic efficacy of our model is partially attributed to its integration of pivotal clinical complications, specifically HE. This condition is direct manifestations of advanced liver dysfunction, fundamental pathophysiological characteristics of ACLF. The occurrence of HE indicates not only impaired ammonia clearance due to liver failure but also significant systemic neuroinflammation and altered cerebral perfusion, often intensified by the systemic inflammatory response associated with sepsis.26,27 Consequently, the inclusion of HE in our model encapsulates a crucial aspect of illness severity, rooted in the fundamental hemodynamic and metabolic disturbances of ACLF, which are exacerbated in the context of sepsis.26,28,29 Moreover, our model highlights the critical importance of coagulopathy by incorporating D-dimer as a key indicator. In patients with sepsis and ACLF, coagulopathy embodies a complex duality. APTT prolongation signifies impaired hepatic synthesis of essential clotting factors, directly resulting from synthetic liver failure.30 Conversely, elevated D-dimer levels suggest heightened fibrinolytic activity and microthrombus formation, arising from widespread endothelial injury, disseminated intravascular coagulation (DIC), and systemic inflammation induced by sepsis.31,32 This concurrent state of bleeding predisposition and pro-thrombotic tendency establishes a precarious haemostatic balance. Our findings corroborate that these readily accessible coagulation markers are sensitive indicators of this pathological condition, consistent with existing literature that identifies hyperfibrinolysis and prolonged coagulation times as significant independent predictors of mortality in both liver failure and sepsis.33–36
The primary innovation of our model lies in the effective integration of immune-inflammatory-nutritional indicators. The ALBI grade offers a more objective and nuanced evaluation of liver synthetic function compared to traditional scores, as it is not influenced by the subjective grading of ascites and encephalopathy.37 Its robust predictive capability underscores the importance of baseline liver reserve as a critical determinant of survival in the event of new insults such as sepsis.38 The SIRI, a comprehensive index that includes neutrophils, monocytes, and lymphocytes, provides an overview of the systemic inflammatory environment. An elevated SIRI indicates a predominant pro-inflammatory condition characterized by increased levels of neutrophils and monocytes, alongside immune exhaustion marked by reduced lymphocyte counts. This phenotype is closely associated with tissue damage and adverse outcomes in both sepsis and cancer.39,40 Within the context of sepsis-associated ACLF, a high SIRI likely represents the unchecked cytokine storm that precipitates multiorgan failure.
Additionally, PLR and LMR further refine our assessment of the immune-inflammatory and thrombotic milieu. PLR serves as a composite marker reflecting both the degree of inflammatory stress and the compensatory capacity of the host. Thrombocytopenia, a key component of PLR, is common in ACLF due to portal hypertension-induced splenic sequestration and reduced thrombopoietin production from the failing liver. Concurrent lymphopenia, often observed in sepsis, indicates immune paralysis and adrenal stress response. Thus, an elevated PLR encapsulates a state of heightened inflammation coupled with impaired immune competence, which has been consistently linked to poor outcomes in critical illnesses including sepsis and liver failure.41 Conversely, a decreased LMR, typically driven by lymphocytopenia and monocytosis, offers distinct prognostic information. Lymphocytopenia indicates impaired adaptive immunity, whereas an elevated monocyte count reflects persistent activation of the innate immune system and ongoing tissue inflammation. In patients with sepsis-associated ACLF, a low LMR has been specifically linked to an increased risk of secondary infections and organ failure, encapsulating the double hit of immune paralysis and sustained inflammatory burden.42 The integration of PLR and LMR thus allows for a more granular assessment of the immune-inflammatory axis, complementing the information provided by SIRI and offering a holistic view of the patient’s immunologic status.
Compared to the SOFA score, our nomogram provides distinct advantages for this particular patient cohort. Although the SOFA score is a well-established and effective prognostic tool for general sepsis, its primary limitation in sepsis-induced ACLF is its lack of specificity. It inadequately incorporates critical liver-specific parameters and fails to capture the essential dynamics of the immune-inflammatory-nutritional axis, which are pivotal to the pathophysiology of ACLF. Conversely, our model explicitly integrates these dimensions, thereby enhancing its predictive accuracy. Moreover, the nomogram format offers a user-friendly interface that enables clinicians to calculate individualized mortality risk at the bedside, which can be invaluable for communicating prognosis with families, triaging patients to higher levels of care, or identifying candidates for salvage therapies.
Limitations
Despite its promising results, our study has several limitations that require acknowledgment. Firstly, the retrospective and single-center design inherently introduces the potential for selection bias and limits the generalizability of our findings. External validation in multi-center, prospective cohorts is essential to confirm the model’s robustness and transportability. Secondly, although we included a comprehensive set of variables, data on certain potential confounders, such as the specific microbiological etiology of sepsis, the use of specific vasopressors, or detailed pharmacological interventions, were not available for analysis. Thirdly, although our sample size and event rate met commonly recommended thresholds for prognostic model development, the number of predictors retained in the final model warrants caution regarding potential overfitting. Internal validation via bootstrap resampling or a larger independent cohort would provide more robust estimates of model performance. Fourthly, this was a single-center study, and the model has not yet been externally validated in other populations or healthcare settings. Therefore, its generalizability remains to be established, and we recommend external validation before widespread clinical implementation. Finally, the application of region-specific diagnostic criteria for ACLF (Chinese Medical Association criteria) represents an important consideration. As there is currently no universally accepted definition of ACLF—with notable differences existing between European (EASL-CLIF), North American (NACSLD), and Asian (APASL/CMA) guidelines—the generalizability of our findings to populations diagnosed under other criteria may be limited. Future validation studies in cohorts defined by different diagnostic standards are needed to assess the model’s broader applicability.
Conclusion
We have successfully developed and validated an innovative prognostic nomogram that integrates clinical complications, coagulation parameters, and immune-inflammatory-nutritional indicators to predict 28-day mortality in sepsis patients with ACLF. This model exhibits superior performance compared to the SOFA score and provides a practical, individualized risk assessment tool. Our model has been internally validated and demonstrates promising performance; however, it is important to note that external validation in independent, multicenter cohorts is necessary to confirm its generalizability and clinical utility before it can be recommended for broader application. The nomogram holds promise for enhancing clinical decision-making, enabling early intervention for high-risk patients, and serving as a valuable instrument for risk stratification in both clinical practice and future research endeavors.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the author, without undue reservation.
Ethics Statement
We received approval from the Institutional Review Board (approval number: 2025R082).
Acknowledgments
We appreciate the nurses and physicians who assisted with the study. We thank the Information Department of Shaanxi Provincial People’s Hospital for providing clinical data.
Author Contributions
Qi Xin: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. Qi Xin took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author declares that no financial support was received for the research, authorship, and/or publication of this article.
Disclosure
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–16. doi:10.1001/jama.2016.0287
2. Kumar R, Mehta G, Jalan R. Acute-on-chronic liver failure. Clin Med. 2020;20(5):501–504. doi:10.7861/clinmed.2020-0631
3. Ghalayini M, Zylberfajn C, Nahon P, Lobo D, Lescat M, Amathieu R. Cirrhosis is an independent risk factor for candidemia in critically ill patients: a 6-year single-center observational study. Anaesth Crit Care Pain Med. 2025;45(1):101611. doi:10.1016/j.accpm.2025.101611
4. Khanam A, Kottilil S. Abnormal innate immunity in acute-on-chronic liver failure: immunotargets for therapeutics. Front Immunol. 2020;11:2013. doi:10.3389/fimmu.2020.02013
5. Su H, Tong J, Liu X, et al. Characteristics and outcome of nosocomial bloodstream infection in patients with acute-on-chronic liver failure. Eur J Gastroenterol Hepatol. 2021;33(1):83–88. doi:10.1097/MEG.0000000000001699
6. Wong F, Piano S, Singh V, et al. Clinical features and evolution of bacterial infection-related acute-on-chronic liver failure. J Hepatol. 2021;74(2):330–339.
7. Zhai XR, Tong JJ, Wang HM, et al. Infection deteriorating hepatitis B virus related acute-on-chronic liver failure: a retrospective cohort study. BMC Gastroenterol. 2020;20(1):320. doi:10.1186/s12876-020-01473-y
8. Saraiva IE, Ortiz-Soriano VM, Mei X, et al. Continuous renal replacement therapy in critically ill patients with acute on chronic liver failure and acute kidney injury: a retrospective cohort study. Clin Nephrol. 2020;93(4):187–194. doi:10.5414/CN109983
9. Zhang Y, Nie Y, Liu L, Zhu X. Assessing the prognostic scores for the prediction of the mortality of patients with acute-on-chronic liver failure: a retrospective study. PeerJ. 2020;8:e9857. doi:10.7717/peerj.9857
10. Philips CA, Ahamed R, Rajesh S, George T, Mohanan M, Augustine P. Update on diagnosis and management of sepsis in cirrhosis: current advances. World J Hepatol. 2020;12(8):451–474. doi:10.4254/wjh.v12.i8.451
11. Bernsmeier C, Cavazza A, Fatourou EM, et al. Leucocyte ratios are biomarkers of mortality in patients with acute decompensation of cirrhosis and acute-on-chronic liver failure. Aliment Pharmacol Ther. 2020;52(5):855–865. doi:10.1111/apt.15932
12. Song R, Wang X, Li Z, et al. ALTA: a simple nutritional prognostic score for patients with hepatitis B virus-related acute-on-chronic liver failure. Front Nutr. 2024;11:1370025. doi:10.3389/fnut.2024.1370025
13. Kulkarni AV, Anand L, Vyas AK, et al. Omega-3 fatty acid lipid emulsions are safe and effective in reducing endotoxemia and sepsis in acute-on-chronic liver failure: an open-label randomized controlled trial. J Gastroenterol Hepatol. 2021;36(7):1953–1961. doi:10.1111/jgh.15400
14. Liu K, Yang L, Liu Y, et al. Systemic Immune-Inflammation Index (SII) and Neutrophil-to-Lymphocyte Ratio (NLR): a strong predictor of disease severity in Large-Artery Atherosclerosis (LAA) stroke patients. J Inflamm Res. 2025;18:195–202. doi:10.2147/JIR.S500474
15. Zhang X, Chen Y, Fan Y, Gao D, Zhang Z. NLR (neutrophil to lymphocyte ratio), PLR (platelet to lymphocyte ratio), and SII (systemic immune-inflammation index) reflect disease activity and renal remission in patients with lupus nephritis. Front Immunol. 2025;16:1646276. doi:10.3389/fimmu.2025.1646276
16. Park IH, Ko NG, Jin M, Lee YJ. Lower prognostic nutritional index is associated with a greater decline in long-term kidney function in general population. Nutr J. 2024;23(1):146. doi:10.1186/s12937-024-01047-8
17. Keskinkilic M, Semiz HS, Ataca E, Yavuzsen T. The prognostic value of immune-nutritional status in metastatic colorectal cancer: Prognostic Nutritional Index (PNI). Support Care Cancer. 2024;32(6):374. doi:10.1007/s00520-024-08572-6
18. Mathold K, Nobin R, Brudin L, Carlsson M, Wanby P. Albumin-to-alkaline phosphatase ratio may be a better predictor of survival than sclerostin, dickkopf-1, osteopontin, osteoprotegerin and osteocalcin. Heliyon. 2024;10(8):e29639.
19. Feng D, Wang M, Hu J, et al. Prognostic value of the albumin-bilirubin grade in patients with hepatocellular carcinoma and other liver diseases. Ann Transl Med. 2020;8(8):553. doi:10.21037/atm.2020.02.116
20. da Fonsecaa LG, de Melob MAZ, da Silveirac THM, Yamamotod VJ, Hashizumee PHS, Sabbagaf J. Prognostic role of albumin-bilirubin (ALBI) score and Child-Pugh classification in patients with advanced hepatocellular carcinoma under systemic treatment. Ecancermedicalscience. 2024;18:1748. doi:10.3332/ecancer.2024.1748
21. Zhao S, Zhang T, Li H, et al. Comparison of albumin-bilirubin grade versus Child-Pugh score in predicting the outcome of transarterial chemoembolization for hepatocellular carcinoma using time-dependent ROC. Ann Transl Med. 2020;8(8):538. doi:10.21037/atm.2020.02.124
22. Zou H, Wen Y, Yuan K, Miao XY, Xiong L, Liu KJ. Combining albumin-bilirubin score with future liver remnant predicts post-hepatectomy liver failure in HBV-associated HCC patients. Liver Int. 2018;38(3):494–502. doi:10.1111/liv.13514
23. Liu J, Li S, Zhang S, et al. Systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio can predict clinical outcomes in patients with metastatic non-small-cell lung cancer treated with nivolumab. J Clin Lab Anal. 2019;33(8):e22964. doi:10.1002/jcla.22964
24. Ao Z, Chen X, Zhu W, Long H, Wang Q, Wu Q. The prognostic nutritional index is an effective prognostic and nutritional status indicator for cirrhosis. BMC Gastroenterol. 2025;25(1):107. doi:10.1186/s12876-025-03599-3
25. Lin S, Wang X, Xu Z, et al. Construction of a prediction model for hepatic encephalopathy in acute-on-chronic liver failure patients. Ann Med. 2024;56(1):2410403. doi:10.1080/07853890.2024.2410403
26. Verma N, Dhiman RK, Choudhury A, et al. Dynamic assessments of hepatic encephalopathy and ammonia levels predict mortality in acute-on-chronic liver failure. Hepatol Int. 2021;15(4):970–982. doi:10.1007/s12072-021-10221-7
27. Aldridge DR, Tranah EJ, Shawcross DL. Pathogenesis of hepatic encephalopathy: role of ammonia and systemic inflammation. J Clin Exp Hepatol. 2015;5(Suppl 1):S7–s20. doi:10.1016/j.jceh.2014.06.004
28. Shin J, Yu JH, Jin YJ, et al. Acute-on-chronic liver failure as a major predictive factor for mortality in patients with variceal bleeding. Clin Mol Hepatol. 2020;26(4):540–553. doi:10.3350/cmh.2020.0034
29. Martin Mateos R, Albillos A. Sepsis in patients with cirrhosis awaiting liver transplantation: new trends and management. Liver Transpl. 2019;25(11):1700–1709. doi:10.1002/lt.25621
30. Bowyer A, Smith J, Woolley AM, et al. The investigation of a prolonged APTT with specific clotting factor assays is unnecessary if an APTT with Actin FS is normal. Int J Lab Hematol. 2011;33(2):212–218. doi:10.1111/j.1751-553X.2010.01266.x
31. Kim SM, Kim SI, Yu G, et al. Role of thromboelastography as an early predictor of disseminated intravascular coagulation in patients with septic shock. J Clin Med. 2020;9(12):3883. doi:10.3390/jcm9123883
32. Tao J, Guo X, Li D, Li Y. Increased level of thrombomodulin is associated with endothelial injury in patients with sepsis-induced disseminated intravascular coagulation. Clin Lab. 2021;67(8). doi:10.7754/Clin.Lab.2020.201204
33. Blasi A, Patel VC, Adelmeijer J, et al. Mixed fibrinolytic phenotypes in decompensated cirrhosis and acute-on-chronic liver failure with hypofibrinolysis in those with complications and poor survival. Hepatology. 2020;71(4):1381–1390. doi:10.1002/hep.30915
34. Lisman T, Arefaine B, Adelmeijer J, et al. Global hemostatic status in patients with acute-on-chronic liver failure and septics without underlying liver disease. J Thromb Haemost. 2021;19(1):85–95. doi:10.1111/jth.15112
35. Panigada M, Zacchetti L, L’Acqua C, et al. Assessment of fibrinolysis in sepsis patients with urokinase modified thromboelastography. PLoS One. 2015;10(8):e0136463. doi:10.1371/journal.pone.0136463
36. Onishi T, Ishihara T, Nogami K. Coagulation and fibrinolysis balance in disseminated intravascular coagulation. Pediatr Int. 2021;63(11):1311–1318. doi:10.1111/ped.14684
37. Hiraoka A, Kumada T, Kudo M, et al. Albumin-Bilirubin (ALBI) grade as part of the evidence-based clinical practice guideline for HCC of the Japan Society of Hepatology: a comparison with the liver damage and child-pugh classifications. Liver Cancer. 2017;6(3):204–215. doi:10.1159/000452846
38. Murray LJ, Sykes J, Brierley J, et al. Baseline Albumin-Bilirubin (ALBI) score in western patients with hepatocellular carcinoma treated with Stereotactic Body Radiation Therapy (SBRT). Int J Radiat Oncol Biol Phys. 2018;101(4):900–909. doi:10.1016/j.ijrobp.2018.04.011
39. Wei L, Xie H, Yan P. Prognostic value of the systemic inflammation response index in human malignancy: a meta-analysis. Medicine. 2020;99(50):e23486. doi:10.1097/MD.0000000000023486
40. Xu T, Song S, Zhu K, et al. Systemic inflammatory response index improves prognostic predictive value in intensive care unit patients with sepsis. Sci Rep. 2025;15(1):1908. doi:10.1038/s41598-024-81860-7
41. Wang G, Mivefroshan A, Yaghoobpoor S, et al. Prognostic value of platelet to lymphocyte ratio in sepsis: a systematic review and meta-analysis. Biomed Res Int. 2022;2022:9056363. doi:10.1155/2022/9056363
42. Zhang B, Han Y, Chen X, et al. Association of monocyte-to-lymphocyte and neutrophil-to-lymphocyte ratios with persistent critical illness in patients with severe trauma. J Trauma Nurs. 2022;29(5):240–251. doi:10.1097/JTN.0000000000000672
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Procalcitonin in Predicting Mortality and Organ Dysfunction at Intensive Care Admission
Suranadi IW, Sinardja CD, Suryadi IA
International Journal of General Medicine 2022, 15:4917-4923
Published Date: 12 May 2022
Resistin Concentration in Early Sepsis and All-Cause Mortality at a Safety-Net Hospital in Riverside County
Bonenfant J, Li J, Nasouf L, Miller J, Lowe T, Jaroszewski L, Qiu X, Thapamagar S, Mittal A, Godzik A, Klein W, Nair MG
Journal of Inflammation Research 2022, 15:3925-3940
Published Date: 13 July 2022
Albumin Level is Associated with Short-Term and Long-Term Outcomes in Sepsis Patients Admitted in the ICU: A Large Public Database Retrospective Research
Cao Y, Su Y, Guo C, He L, Ding N
Clinical Epidemiology 2023, 15:263-273
Published Date: 3 March 2023
Multidrug-Resistant Bacteria on Critically Ill Patients with Sepsis at Hospital Admission: Risk Factors and Effects on Hospital Mortality
Maia MDO, da Silveira CDG, Gomes M, Fernandes SES, Bezerra de Santana R, de Oliveira DQ, Amorim FFP, Neves FDAR, Amorim FF
Infection and Drug Resistance 2023, 16:1693-1704
Published Date: 23 March 2023
A Practical Nomogram Based on RDW-CV for Predicting Clinical Outcome in Elderly Septic Patients
Hong C, Liu Z, Nan C, Xie Y, Xia J, Jiang Y, Liu X, Xu Z, Hui K, Xiong Y, Wang W, Chen H
Infection and Drug Resistance 2025, 18:4799-4809
Published Date: 9 September 2025