Back to Journals » Journal of Inflammation Research » Volume 19
A Clinical and Biomarker-Based Model for Predicting in-Hospital Mortality in Patients Undergoing Extracorporeal Membrane Oxygenation: A Machine Learning-Based Nomogram Study
Authors Zhu G, Cai Y, Lin L, Chen C, Bi X
Received 17 April 2026
Accepted for publication 27 June 2026
Published 9 July 2026 Volume 2026:19 613742
DOI https://doi.org/10.2147/JIR.S613742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qing Lin
Guangjun Zhu,1,* Yunda Cai,1,* Li Lin,2 Chaochao Chen,1 Xiaojie Bi1
1Department of Laboratory Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, 317000, People’s Republic of China; 2Department of Rehabilitation Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, 317000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaojie Bi, Department of Laboratory Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, No. 150, Ximen Street, Linhai, 317000, People’s Republic of China, Tel +86 13757693182, Email [email protected] Chaochao Chen, Department of Laboratory Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, No. 150, Ximen Street, Linhai, 317000, People’s Republic of China, Tel +86 13757693182, Email [email protected]
Purpose: A nomogram was constructed for predicting in-hospital mortality in patients receiving extracorporeal membrane oxygenation (ECMO) using clinical indicators, to provide a reference for clinical risk stratification.
Patients and Methods: A retrospective cohort of 122 ECMO patients (81 survivors, 41 non-survivors) from Taizhou Hospital of Zhejiang Province (January 2022–December 2024) was used for model development, with 22 patients from the MIMIC-IV database serving as the external validation cohort. A two-step Boruta-LASSO feature selection strategy was applied to identify key predictors, followed by construction of five machine learning models; the best-performing model was used to develop a nomogram, validated internally and externally via ROC analysis, calibration curves, decision curve analysis, and SHAP interpretability analysis.
Results: Four key predictors were identified: malignant tumor, Lactic Acid, monocyte-to-white blood cell ratio (MWR), and activated partial thromboplastin time-to-albumin ratio (AAR). The logistic regression model exhibited the best and most stable predictive performance, with a cross-validated AUC of 0.765 (95% CI: 0.667– 0.863) in the primary cohort. External validation in the MIMIC-IV cohort (n=22) yielded an AUC of 0.838 (95% CI: 0.655– 1.000), suggesting preliminary external validation with acceptable generalizability.
Conclusion: Malignant tumor, elevated Lactic Acid, decreased MWR, and elevated AAR are key predictive factors for in-hospital mortality in ECMO patients. The nomogram model demonstrated satisfactory discriminatory ability, acceptable calibration, and potential clinical utility, serving as a valuable exploratory tool for bedside risk stratification in ECMO patients. Further validation in larger, multicenter, prospective cohorts is warranted before clinical implementation.
Keywords: ECMO, in-hospital mortality, nomogram, LASSO Regression, machine learning, Boruta algorithm, SHAP analysis
Introduction
Extracorporeal membrane oxygenation (ECMO) is a core life-support technology in critical care, simulating cardiopulmonary function to provide gas exchange and circulatory support.1 It is widely used in reversible cardiopulmonary failure caused by severe pneumonia, acute respiratory distress syndrome, and cardiogenic shock2 Despite technological advancements, in-hospital mortality remains high (40%–60%),3 highlighting the need for early identification of high-risk patients and personalized intervention strategies.4
Most existing scoring systems target specific populations and may not cover the full spectrum of modern ECMO indications.5 Single lab markers or empirical clinical judgment fail to integrate multiple risk dimensions.6 General ICU scores lack ECMO-specific features and depend on pre-intubation parameters.7 These gaps highlight the need for a systematic ECMO-tailored framework. Previous studies have identified age,8 prior CPR, and low initial platelet count9 as independent risk factors for in-hospital mortality in ECMO patients. Elevated pre-ECMO lactate10 and comorbidities11 are also associated with poor outcomes.
To address these limitations, current studies on factors influencing the prognosis of patients treated with ECMO are mostly focused on single-center, small-sample analyses, with a lack of unified risk prediction models and external validation data.10,12 This study conducted a retrospective analysis of clinical data from ECMO patients, adopted a two-step feature screening strategy combining Boruta algorithm and LASSO regression to identify core predictive factors, and constructed multiple machine learning prediction models. A risk prediction nomogram was developed based on the optimal model, and SHAP analysis was used to realize the multi-dimensional interpretability of the model from population to individual. The model’s performance was validated using an external cohort from the MIMIC-IV database. It aims to provide clinicians with a standardized, interpretable and generalizable tool for assessing the mortality risk of ECMO patients, and assist critical care teams in optimizing diagnosis and treatment decisions.
Materials and Methods
Patients and Study Design
We retrospectively enrolled consecutive ECMO patients from Taizhou Hospital (Jan 2022–Dec 2024). Inclusion criteria: (1) age ≥ 18 years; (2) ECMO support duration ≥ 24 hours; and (3) availability of complete clinical and laboratory data within 24 hours before ECMO initiation. Exclusion criteria: brain death, treatment withdrawal before ECMO, incomplete data. The primary cohort (n=122) was split 8:2 into training (n=98) and test (n=24) sets.
For patient identification in the MIMIC-IV database (2008–2022), we queried ICD-10-PCS procedure code 5A15223 and ICD-9-CM procedure code 3965 to capture ECMO-related records across different data periods. The total number of identified ECMO-related records was 56. Patients were screened using the same inclusion criteria as the primary cohort. A total of 22 patients were ultimately included for validation, comprising 13 survivors and 9 non-survivors (Figure 1). Patient deduplication was performed using unique subject IDs, and data were extracted from the first 24 hours of ECMO support.
 |
Figure 1 Flowchart of patient inclusion and exclusion. |
Samples and Laboratory Measurements
Peripheral venous blood samples were collected from all participants in the study cohort within 24 hours before ECMO initiation. Hematological parameters (WBC, neutrophil, monocyte, lymphocyte, Hb, PLT) were measured using a Mindray BC series automated hematology analyzer (Mindray, Shenzhen, China). Routine coagulation function tests (fibrinogen, APTT, PT, INR) were performed using a Stago STR-Max automated coagulation analyzer (Stago, Cedex, France). Blood gas parameters (Lactic Acid, pH value) and oxygenation index were analyzed using a Siemens Rapid 500 automated blood gas analyzer (Siemens, Munich, Germany). Biochemical indicators (ALT, AST, TP, Alb, ALP, urea, creatinine, eGFR, glucose, total bilirubin) were assayed with a Beckman Coulter AU5800 automated biochemistry analyzer (Beckman Coulter, Brea, California, USA). All measurements were performed per standard protocols. Derived ratios were defined as: MWR (monocyte to WBC ratio), AHR (APTT to HGB ratio), AAR (APTT to Alb ratio), LAR (lactate to Alb ratio). All ratio calculations and feature engineering were conducted on the full dataset prior to train-test splitting.
Collection of Clinical Data and Outcome
Longitudinal clinical indicators were systematically collected from medical records in this study, including demographic data, underlying diseases, comorbidities (eg, cardiac disease, hypertension), organ dysfunction, and in-hospital outcomes (survival/non-survival). Outcome (in-hospital mortality) was defined as all-cause death during the index hospitalization, identified via discharge status codes in both the local electronic medical record system and MIMIC-IV database. Comorbidities including malignant tumor, hypertension, and diabetes were defined using ICD-10 diagnosis codes consistent with prior epidemiological studies of ECMO populations.
Statistical Methods
Data cleaning removed duplicates and implausible values; Missing values were not imputed given the complete case design, and all variables included in the final analysis had <5% missing data. We considered multiple imputation (MICE) as a sensitivity analysis, but given the low missing rate (<5%) and the small sample size, complete-case analysis was chosen to avoid introducing imputation bias. Sample size was pre-calculated (G*Power 3.1, power ≥0.70). The final model achieved an events-per-variable (EPV) of 10.25. Non-normal continuous variables were expressed as median (IQR) and compared via Wilcoxon test; categorical variables used chi-square test. Significance: P<0.05.
Feature Selection
Collinearity among candidate variables was first assessed using the variance inflation factor (VIF), and variables with VIF > 5 were excluded. A two-step feature selection approach was then applied: (1) the Boruta algorithm was used for initial screening, identifying all relevant features by comparing their importance against random shadow variables, thereby reducing dimensionality; (2) LASSO regression with 10-fold cross-validation was subsequently applied to further shrink coefficients and select the most parsimonious set of predictors, minimizing overfitting.
Machine Learning Model Construction and Evaluation
Five models (Logistic regression, LASSO, Random Forest, LightGBM, XGBoost) were built on training data using default hyperparameters. In this cohort, logistic regression outperformed more complex tree-based and boosting models (Random Forest, LightGBM, XGBoost). This is likely attributable to the limited sample size (n=122) and small predictor set: complex models tend to overfit training-set noise in such settings, whereas logistic regression’s lower complexity yields more stable generalization. The approximately linear feature–outcome relationships further favored logistic regression, which was therefore selected as the final model. The area under the receiver operating characteristic curve (AUC) was the primary metric; Calibration plots (1000 bootstrap) and repeated 10-fold cross-validation were performed. All statistical analyses were conducted in R (version 4.4.2), including glmnet (LASSO regression), randomForest (random forest), lightgbm (LightGBM), xgboost (XGBoost), pROC (ROC curves), rms (nomogram and calibration), dca (decision curve analysis), Boruta (feature selection), and shapviz (SHAP analysis). Repeated 10-fold cross-validation was performed to eliminate optimism bias.
Model Interpretability Analysis
The SHAP (SHapley Additive exPlanations) analysis was applied to all five models to quantify individual feature contributions and enable consistent cross-model comparison. For the logistic regression model, SHAP serves a supplementary interpretability role alongside standardized coefficients.
Nomogram Development and Validation
The best-performing model was used to build a nomogram (R, rms package). Clinical utility was assessed via decision curve analysis (DCA). Internal validation used ROC curves; external validation used the MIMIC-IV cohort, with AUC comparisons via Z-test.
Results
Baseline Clinical and Laboratory Characteristics of the Primary Cohort
A total of 122 ECMO patients were included in the primary cohort, with a male proportion of 64.75% (79/122) and a median age of 59.00 [46.00;70.00] years. Of these, 93 (76.23%) received VA-ECMO and 29 (23.77%) received VV-ECMO. The median ECMO duration was 3.00 [1.25;7.00] hours, and the overall in-hospital mortality rate was 33.61% (41/122) (Table S1). VA-ECMO and VV-ECMO patients differ in etiology, immune status, metabolism, and coagulation, reflecting their distinct indications (cardiac vs. respiratory support), yet survival rates are similar. There were no statistically significant differences between the survival and non-survival groups in terms of gender, age, and the incidence of underlying diseases including hypertension, diabetes mellitus, hepatic insufficiency and renal insufficiency (all P>0.05). However, the proportion of Malignant Tumor in the non-survival group was significantly higher than that in the survival group (12.2% vs 2.47%, p=0.042).
Liver function: total bilirubin was significantly lower in the non-survival group (7.90 [5.00; 11.50] vs 11.50 [7.80; 15.00] μmol/L, P=0.004); Metabolic indicators: Lactic Acid was markedly higher (11.00 [5.10; 15.40] vs 4.60 [2.50; 8.90] mmol/L, P<0.001) and pH value was lower (7.24 [7.04; 7.37] vs 7.32 [7.24; 7.42], P=0.022) in non-survivors; Coagulation indicators: APTT and INR were significantly higher in non-survivors (57.70 [37.40; 180.00] vs 44.00 [36.50; 62.40] seconds, P=0.043; 1.42 [1.12; 1.92] vs 1.16 [1.08; 1.49], P=0.048); Derived ratio indicators: MWR was significantly lower in non-survivors (0.03 [0.02; 0.05] vs 0.05 [0.03; 0.06], P=0.006), while LAR, AAR, and AHR were significantly higher (all P<0.05) (Table 1).
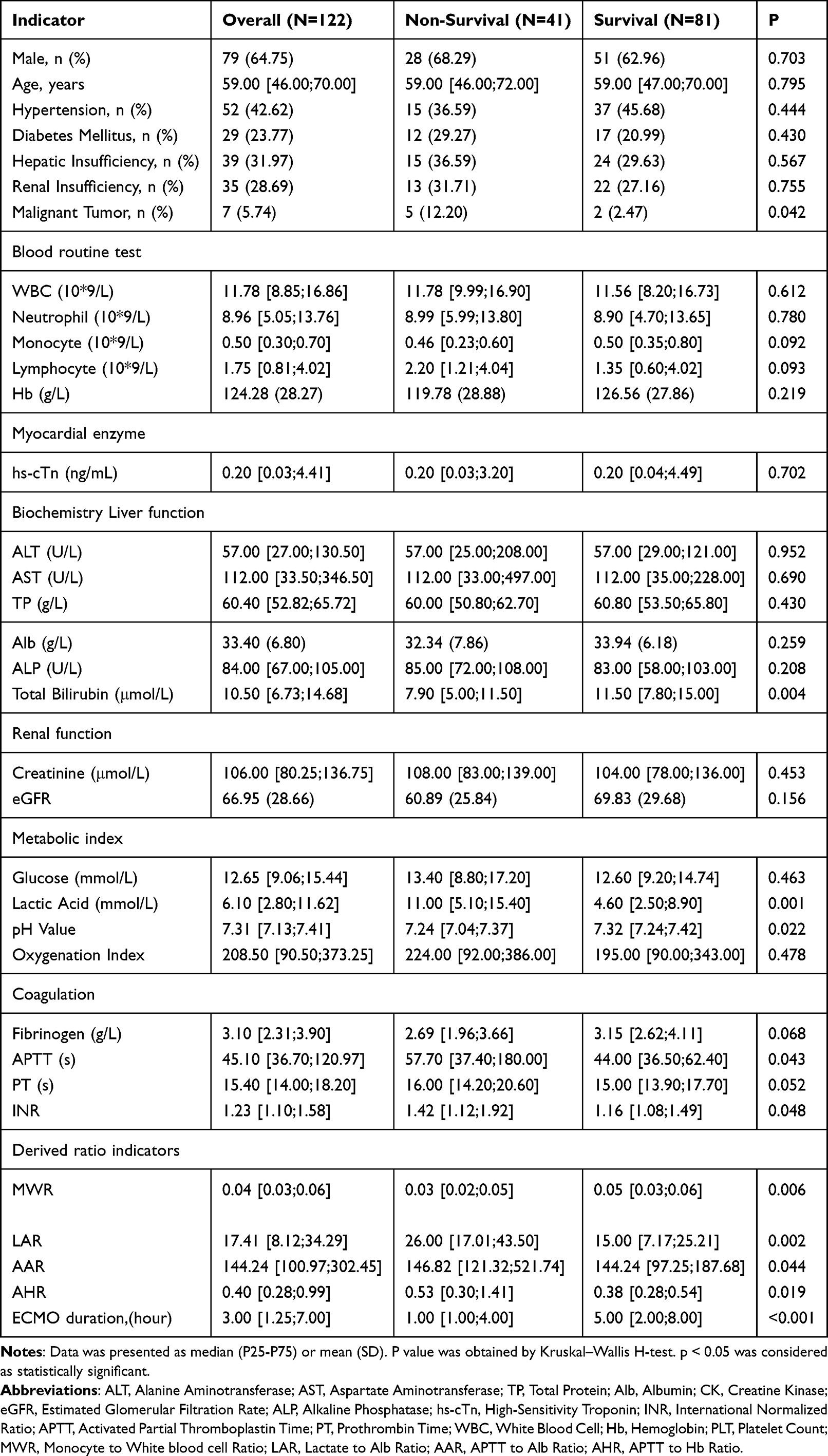 |
Table 1 Baseline Characteristics of ECMO Patients on the Day of Treatment (N=122) |
Baseline Characteristics of the Training an Baseline Characteristics of the Training and Test Groups
Patients were randomly divided into a training group (n=98) and a test group (n=24, comprising 16 survivors and 8 non-survivors, non-survivor proportion 33.3%, consistent with the overall cohort mortality rate of 33.6%). Most baseline characteristics, comorbidities, laboratory parameters, and derived ratio indicators were well balanced between groups (all P>0.05) (Table 2).
 |
Table 2 Baseline Characteristics of ECMO Patients in the Training and Test Groups |
Feature Selection Results
A two-step feature screening was performed using the Boruta algorithm and LASSO regression. The Boruta algorithm (Figure 2A) identified Lactic Acid and MWR as confirmed important features with significant discriminatory ability for survival outcomes, and malignant tumor as a tentative important feature, while AAR and other indicators were initially classified as shadow features without significant predictive value. The box plot of feature importance showed that Lactic Acid had the highest median importance (approximately 7.5), significantly higher than other indicators, indicating its core role in distinguishing survival outcomes, followed by MWR (approximately 5), and the importance of malignant tumor was slightly lower than that of MWR.
 |
Figure 2 Boruta and LASSO feature selection and model evaluation for ECMO patient mortality prediction. (A) Boruta feature importance: Boxplot of feature importance classified into confirmed, shadow, and tentative groups. (B) 10-Fold CV for LASSO: Binomial deviance curve with λ.min and λ.1se markers for optimal regularization. (C) Lasso coefficient path: Trajectory of coefficients shrinking with increasing λ, with optimal λ marked. (D) Variables importance: Barplot of feature importance based on absolute LASSO coefficients. |
Based on the results of preliminary screening, LASSO regression with 10-fold cross-validation (Figure 2B) selected the optimal λ value at -log(λ)=3.5 (red dashed line) with the minimum binomial deviance, and finally retained four core features: malignant tumor, AAR, Lactic Acid and MWR. The coefficient path plot (Figure 2C) showed that with the decrease of λ (increase of model complexity), the regression coefficients of each feature gradually became non-zero: the coefficient of malignant tumor stabilized to a positive value at the earliest, followed by the increase of AAR and Lactic Acid coefficients, while the MWR coefficient was negative, suggesting that different features had distinct effect directions on in-hospital mortality. The variable importance plot (Figure 2D), measured by the absolute value of LASSO regression coefficients, showed that malignant tumor had the highest contribution (|β|≈1.3), followed by AAR (|β|≈0.3), Lactic Acid (|β|≈0.3) and MWR (|β|≈0.2). The results of Boruta algorithm and LASSO regression formed a complementary effect, in which the former focused on the outcome discrimination ability of features, and the latter emphasized the predictive contribution of features in the model.
Construction and Evaluation of Machine Learning Models
Based on the two-step screened core indicators, five machine learning models were constructed in the training group, and their predictive performance was evaluated in the training set and test set with AUC, optimal cutoff value, sensitivity and specificity as evaluation indices (Table 3). The results showed that all models had good predictive performance (AUC>0.75) in the training set, with XGBoost exhibiting the highest training set AUC (0.827, 95% CI: 0.739–0.915) and satisfactory sensitivity (0.758) and specificity (0.846). Logistic regression showed the best performance in the test set, with an AUC of 0.891 (95% CI: 0.761–1.000), optimal cutoff value of 0.408, sensitivity of 1.000, and specificity of 0.750. LASSO regression achieved a test AUC of 0.844 (95% CI: 0.675–1.000), with a sensitivity of 0.750 and specificity of 0.812. Random forest and LightGBM also showed favorable performance in the test set, with AUCs of 0.832 and 0.816, respectively; while XGBoost presented the lowest test set AUC (0.699, 95% CI: 0.486–0.913) and the lowest specificity (0.438), indicating obvious overfitting and poor generalizability. The cross-validated AUCs, which we now report as the primary performance metrics, are more stable and conservative: logistic regression (0.757±0.097), LASSO regression (0.754±0.096), Random Forest (0.623±0.097), LightGBM (0.679±0.080), and XGBoost (0.687±0.092).
 |
Table 3 Model Performance in Training and Test Sets for ECMO Mortality Prediction |
Nomogram Development and Validation
A nomogram model integrating the four core predictive features (malignant tumor, Lactic Acid, MWR, AAR) was developed based on the optimal Logistic regression model (Figure 3A). Internal validation showed that the calibration curve of the nomogram with 1000 bootstrap resamples had a good agreement between predicted and observed probabilities of death (Figure 3B), indicating acceptable calibration of the model. DCA demonstrated that the nomogram model had a positive clinical net benefit across a range of high-risk thresholds (Figure 3C), which was significantly higher than the all-treat and no-treat strategies, suggesting potential clinical utility across a range of threshold probabilities. ROC curve analysis showed that the nomogram model had good discriminatory ability in the training set (AUC=0.765), test set (AUC=0.891) (Figure 3D).
 |
Figure 3 Development and validation of the nomogram for predicting in-hospital mortality in ECMO patients. (A) Nomogram integrating four key predictors (Lactic Acid, MWR, AAR, and Malignant Tumor) to estimate individual mortality risk. (B) Calibration curve of the nomogram with 1000 bootstrap resamples, showing reasonable agreement between predicted and observed probabilities of death. (C) Decision curve analysis (DCA) demonstrating the clinical net benefit of the prediction model across a range of high-risk thresholds. (D) Receiver operating characteristic (ROC) curves of the nomogram in the training, test, and external validation cohorts, with corresponding area under the curve (AUC) values. |
SHAP Model Interpretability Analysis
SHAP analysis confirmed Lactic Acid as the dominant predictor across all models (mean |SHAP| ≈0.10 for logistic regression; Figure 4A and B). Dependence and waterfall plots further illustrated individual-level risk contributions (Figure 4C and D).
 |
Figure 4 SHAP analysis of the logistic regression model for ECMO patient mortality prediction. (A) Global feature importance: Ranked by mean absolute SHAP values. (B) SHAP bee swarm plot: Distribution of SHAP values showing feature impact direction and magnitude. (C) SHAP dependence plot: Linear association between Lactic Acid and its SHAP values. (D) High-risk waterfall plot: SHAP contribution decomposition for a representative high-mortality patient. |
External Validation of the Prediction Model
External validation was conducted in the MIMIC-IV cohort (n=22). Lactic Acid were significantly higher in the non-survival group (both P<0.05), consistent with the primary cohort. No significant differences were observed for AAR, MWR or malignant tumor (both P>0.05), likely due to the small external sample size (Table 4). The model maintained good discrimination in external validation, with an AUC of 0.838 (0.655–1.000), indicating preliminary external validation with acceptable generalizability (Figure 3D).
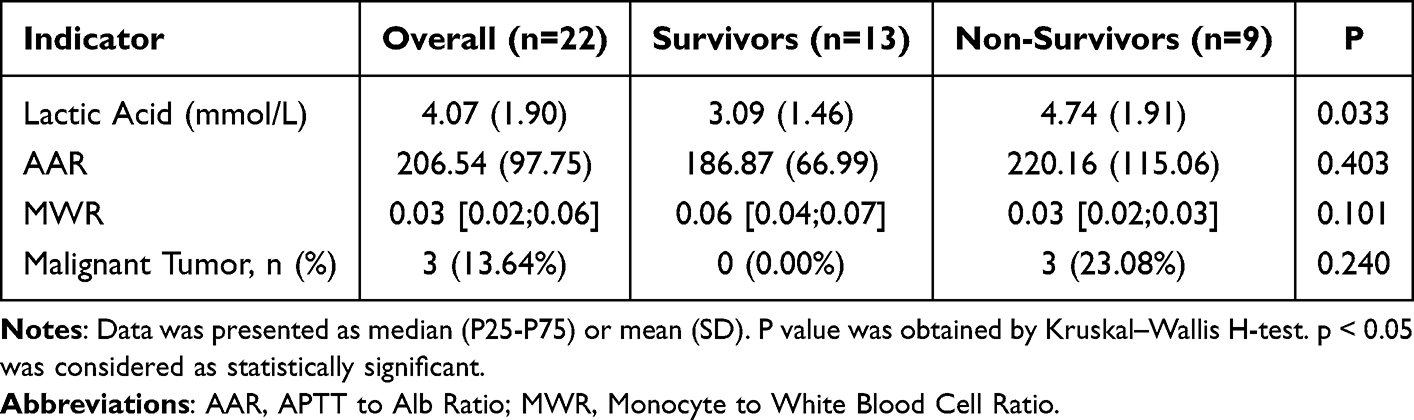 |
Table 4 Comparison of Clinical Characteristics Between Survival and Non-Survival Patients in the External Validation Cohort |
Discussion
This study employed a two-step Boruta-LASSO approach for feature screening and four machine learning algorithms for model development to identify key predictors of in-hospital mortality in patients ECMO. A parsimonious prediction model with favorable discrimination and generalizability was subsequently established.
In this cohort, logistic regression outperformed more complex tree-based and boosting models (Random Forest, LightGBM, XGBoost). This is likely attributable to the limited sample size (n=122) and small predictor set: complex models tend to overfit training-set noise in such settings, whereas logistic regression’s lower complexity yields more stable generalization. The approximately linear feature–outcome relationships further favored logistic regression, which was therefore selected as the final model.
Malignant Tumor was an independent risk factor, likely due to the poor functional status, immune impairment, and advanced organ dysfunction often present in these patients. The invasive nature of ECMO may further exacerbate systemic stress and inflammatory responses.
Lactic Acid emerged as the most powerful predictor of in‑hospital mortality in this cohort. The persistent elevation of lactate despite ECMO may further suggest ongoing microcirculatory dysfunction, irreversible cellular injury, or sepsis-related metabolic disturbances, all of which are associated with higher mortality in critically ill patients13,14 As a direct marker of tissue hypoperfusion and hypoxia, elevated lactate levels, which were more than double in non-survivors compared to survivors, strongly indicate unfavorable outcomes during ECMO support.15
The AAR (APTT-to-Albumin Ratio), a novel composite indicator, integrates and reflects concurrent coagulation dysfunction (prolonged APTT) and nutritional/metabolic compromise (hypoalbuminemia). Notably, APTT has long been recognized as a key indicator for anticoagulation monitoring during ECMO support, as it directly assesses the integrity of the intrinsic coagulation pathway and the efficacy of anticoagulant agents such as heparin16 When combined with hypoalbuminemia—a marker of nutritional depletion, systemic inflammation, and impaired synthesis—the elevated AAR synergistically integrates two independent adverse prognostic factors. In the context of ECMO, hypoalbuminemia can exacerbate endothelial dysfunction, alter drug pharmacokinetics (eg, of heparin),17 and reflect a severe systemic inflammatory state.18 An elevated AAR indicates a synergistic increase in mortality risk by reflecting the cumulative burdens of coagulation impairment and metabolic/inflammatory dysregulation in ECMO patients. The use of composite biomarkers like the HALP score (Hemoglobin, Albumin, Lymphocyte, Platelet), which integrates albumin as a marker of nutritional status and inflammation, is supported by evidence predicting adverse events after coronary bypass surgery.19 This growing body of literature underscores the clinical value of albumin-related composite indices in patients undergoing extracorporeal circulation support.
In our cohort, the MWR (Monocyte-to-White cell Ratio) was identified as a protective factor against in-hospital mortality. This finding aligns with emerging evidence highlighting the prognostic role of monocyte function in critical care settings. Specifically, a prospective study by Siegel et al demonstrated that monocyte dysfunction effectively predicts mortality in patients receiving VA-ECMO.20 A low MWR may reflect a state of immune exhaustion, impaired monocyte function, and overwhelming systemic inflammation, all of which can hinder recovery in critically ill ECMO patients.21 Thus, MWR serves not only as a simple hematologic index but also as an integrative marker of immune competence and inflammatory balance. Its identification as a protective factor underscores the importance of monitoring immune cell profiles in ECMO patients, potentially informing strategies aimed at modulating immune responses and improving outcomes in this high-risk population.
A nomogram was developed based on the logistic regression model for clinical application. Internal validation indicated good calibration, and decision‑curve analysis demonstrated favorable clinical net benefit. External validation in the MIMIC‑IV cohort (n=22) yielded an AUC of 0.838 (95% CI: 0.655–1.000), suggesting acceptable generalizability.
Existing ECMO mortality scores including SAVE and RESP were established for specific patient groups, so they do not apply to our heterogeneous cohort (76% VA-ECMO, 24% VV-ECMO).22 Direct AUC comparison would lead to spectrum bias and lack clinical value. Further studies with stratified, larger cohorts are required to compare our model with existing tools. Although individual predictors did not show statistically significant differences in the external cohort, the full model integrating all four indicators still demonstrated reasonable discriminative performance in external validation. This tool facilitates bedside risk assessment and supports individualized clinical decision‑making.
This study has several limitations. The small retrospective single-center cohort (n=122, 41 in-hospital deaths) may cause inadequate statistical power and biases. Dynamic clinical parameters during ECMO, imaging and genetic markers were not included. External validation relied on a small MIMIC-IV subgroup (n=22), restricting model generalizability. Moreover, we did not compare our model with other prediction models. It should be seen as an exploratory tool, not a definitive clinical aid, until further model optimization through large multicenter studies with complete data and rigorous validation.
Conclusion
In this study, we identified Malignant Tumor, elevated Lactic Acid, AAR, and decreased MWR as potential predictors of in-hospital mortality in ECMO patients. A nomogram was built using two-step Boruta-LASSO feature selection and logistic regression, showing reasonable discrimination, acceptable calibration, and modest generalizability. SHAP analysis added clinical interpretability. This tool may help address a current gap in ECMO-specific risk assessment and support bedside mortality stratification and personalized decision-making. Larger external validation is still needed to confirm its reliability.
Statement
This study was conducted and reported in adherence to the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) reporting guidelines. All authors meet the journal’s authorship criteria. All authors have read and approved the final manuscript to be published, agreed on the target journal for submission, and take full responsibility for all aspects of this work.
Data Sharing Statement
The authors confirm that all data supporting the findings of this study are available from the corresponding author upon reasonable request. Prof. Zhu had full access to all data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Supplemental Materials, including the study protocol, programming code, and analysis scripts, are also available by contacting the corresponding author at [[email protected]].
Ethics Approval and Informed Consent
This study involved a retrospective analysis of de-identified historical laboratory data from patients. Prior to admission, all patients were informed and provided written informed consent for the following: “To advance medical research and education, your medical records and residual biological specimens (including blood, body fluids, tissues, etc.) may be used for relevant research. During this process, your personal information will be strictly confidential”. This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Taizhou Hospital of Zhejiang Province (Approval No.: K20251042).
Author Contributions
Guangjun Zhu: Conceptualization, Methodology, Supervision, Project Administration, Funding Acquisition, Writing – Review & Editing;
Yunda Cai: Conceptualization, Investigation, Formal Analysis, Software, Writing – Original Draft, Visualization;
Li Lin: Resources, Validation, Formal Analysis, Data Curation, Writing – Review & Editing;
Chaochao Chen: Investigation, Data Curation, Software, Visualization, Writing–Review & Editing;
Xiaojie Bi: Investigation, Resources, Validation, Writing – Review & Editing.
Funding
Medical Science and Technology Project of Zhejiang Province 2024KY522.
Disclosure
The authors declare no competing interests in this work.
References
1. Qadir N, Sahetya S, Munshi L, et al. An update on management of adult patients with acute respiratory distress syndrome: an Official American Thoracic Society Clinical Practice Guideline. Am J Resp Crit Care. 2024;209(1):24–14. doi:10.1164/rccm.202311-2011ST
2. Thiele H, Zeymer U, Akin I, et al. Extracorporeal life support in infarct-related cardiogenic shock. New Engl J Med. 2023;389(14):1286–1297. doi:10.1056/NEJMoa2307227
3. Teng Y, Li Y, Li K, et al. Risk factors for acute kidney injury in adult patients under veno-arterial extracorporeal membrane oxygenation support. J Cardiothor Vasc an. 2024;38(10):2231–2237. doi:10.1053/j.jvca.2024.03.038
4. Lüsebrink E, Binzenhöfer L, Kellnar A, et al. Venting during venoarterial extracorporeal membrane oxygenation. Clin Res Cardiol. 2023;112(4):464–505. doi:10.1007/s00392-022-02069-0
5. Condella A, Lentz S, Upchurch C, Badulak J, Long B, Gottlieb M. Extracorporeal membrane oxygenation (ECMO): a narrative review for the emergency clinician. Am J Emergency Med. 2025;96:6–14. doi:10.1016/j.ajem.2025.06.007
6. Chad T, Yusuff H, Zochios V, et al. Right ventricular injury increases mortality in patients with acute respiratory distress syndrome on veno-venous extracorporeal membrane oxygenation: a systematic review and meta-analysis. Asaio J Am Soci Artificial Internal Organs. 2023;69(1):e14–e22. doi:10.1097/MAT.0000000000001854
7. Pratt EH, Morrison S, Green CL, Rackley CR. Ability of the respiratory ECMO survival prediction (RESP) score to predict survival for patients with COVID-19 ARDS and non-COVID-19 ARDS: a single-center retrospective study. J Intensive Care. 2023;11(1):37. doi:10.1186/s40560-023-00686-z
8. Wang J, Huang S, Feng K, et al. Risk factors for mortality in patients receiving extracorporeal membrane oxygenation. Renal Failure. 2024;46(2):2395450. doi:10.1080/0886022X.2024.2395450
9. Byun E, Kang PJ, Jung SH, et al. Impact of extracorporeal membrane oxygenation-related complications on in-hospital mortality. PLoS One. 2024;19(3):e0300713. doi:10.1371/journal.pone.0300713
10. Lee H, Song MJ, Cho YJ, et al. Supervised machine learning model to predict mortality in patients undergoing venovenous extracorporeal membrane oxygenation from a nationwide multicentre registry. BMJ Open Respir Res. 2023;10(1). doi:10.1136/bmjresp-2023-002025
11. Jeong JH, Kook H, Lee SH, et al. Predictors of in-hospital mortality after successful weaning of venoarterial extracorporeal membrane oxygenation in cardiogenic shock. Sci Rep-Uk. 2023;13(1):17529. doi:10.1038/s41598-023-44679-2
12. Lesouhaitier M, Belicard F, Tadié J. Cardiopulmonary bypass and VA-ECMO induced immune dysfunction: common features and differences, a narrative review. Critical Care. 2024;28(1):300. doi:10.1186/s13054-024-05058-z
13. Slottosch I, Liakopoulos O, Kuhn E, et al. Lactate and lactate clearance as valuable tool to evaluate ECMO therapy in cardiogenic shock. J Crit Care. 2017;42:35–41. doi:10.1016/j.jcrc.2017.06.022
14. Qian S, Li P, Hou X, Dong N. Development and internal validation of the PROFIT and POSITIVE prognostic nomograms for patients undergoing VA-ECMO therapy. Sci Rep-Uk. 2025;15(1):20573. doi:10.1038/s41598-025-06607-4
15. Levy B, Girerd N, Baudry G, et al. Serial daily lactate levels association with 30-day outcome in cardiogenic shock patients treated with VA-ECMO: a post-hoc analysis of the HYPO-ECMO study. Ann Intensive Care. 2024;14(1):43. doi:10.1186/s13613-024-01266-6
16. Rajsic S, Treml B, Jadzic D, et al. aPTT-guided anticoagulation monitoring during ECMO support: a systematic review and meta-analysis. J Crit Care. 2023;77:154332. doi:10.1016/j.jcrc.2023.154332
17. Laimoud M, Alanazi M. The clinical significance of blood lactate levels in evaluation of adult patients with veno-arterial extracorporeal membrane oxygenation. Egypt Heart J. 2020;72(1):74. doi:10.1186/s43044-020-00108-7
18. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/CCM.0000000000005337
19. Zhen K, Li J, Jiang H. The relationship between hemoglobin, albumin, lymphocyte, and platelet (HALP) score and prognosis in patients with heart failure: a retrospective analysis of the MIMIC-IV database. Medicine. 2026;105(19):e48530. doi:10.1097/MD.0000000000048530
20. Martucci G, Giani M, Schmidt M, et al. Anticoagulation and bleeding during veno-venous extracorporeal membrane oxygenation: insights from the PROTECMO study. Am J Resp Crit Care. 2024;209(4):417–426. doi:10.1164/rccm.202305-0896OC
21. Raja KM, Plazak M, Rabin J, et al. Hypoalbuminemia is a predictor of mortality in patients with cardiogenic shock requiring veno-arterial extracorporeal membrane oxygenation. Perfusion-Uk. 2025;40(5):1193–1201. doi:10.1177/02676591241288793
22. Biancari F, Juvonen T, Cho S, et al. External validation of the PC-ECMO score in postcardiotomy veno-arterial extracorporeal membrane oxygenation. Int J Artificial Organs. 2024;47(4):313–317. doi:10.1177/03913988241237701
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nomogram for Predicting the Risk of Pulmonary Hypertension for Patients with Chronic Obstructive Pulmonary Disease
Wang N, Guo Z, Gong X, Kang S, Cui Z, Yuan Y
International Journal of General Medicine 2022, 15:5751-5762
Published Date: 22 June 2022
A Nomogram for Predicting the Risk of Critical Limb Ischemia in Adults with Hypertension: A Retrospective Study
Xu D, Zhu X, Huo J, Xie X, Huang C, Fang X, Yin T
International Journal of General Medicine 2022, 15:8205-8216
Published Date: 18 November 2022
Radiomics Nomogram Model Based on TOF-MRA Images: A New Effective Method for Predicting Microaneurysms
Kong D, Li J, Lv Y, Wang M, Li S, Qian B, Yu Y
International Journal of General Medicine 2023, 16:1091-1100
Published Date: 27 March 2023
Prediction of the Risk of Bone Mineral Density Decrease in Type 2 Diabetes Mellitus Patients Based on Traditional Multivariate Logistic Regression and Machine Learning: A Preliminary Study
Zhang J, Xu Z, Fu Y, Chen L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2885-2898
Published Date: 19 September 2023
Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Monocyte-to-Lymphocyte Ratio (MLR), and Eosinophil-to-Lymphocyte Ratio (ELR) as Biomarkers in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD)
Liao QQ, Mo YJ, Zhu KW, Gao F, Huang B, Chen P, Jing FT, Jiang X, Xu HZ, Tang YF, Chu LW, Huang HL, Wang WL, Wei FN, Huang DD, Zhao BJ, Chen J, Zhang H
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:501-518
Published Date: 23 February 2024