Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Transcatheter Arterial Chemoembolization May Be Selectively Indicated as Postoperative Adjuvant Therapy for Hepatocellular Carcinoma Patients with Microvascular Invasion
Authors Zeng J ![]() , Huang H, Tang M, Tao Z, Mo K, Chen W, Su Y, Su J, Liang R
, Huang H, Tang M, Tao Z, Mo K, Chen W, Su Y, Su J, Liang R ![]() , Lin Y, Li L
, Lin Y, Li L ![]() , Wu G
, Wu G ![]() , Luo X, Ye J, Mai R
, Luo X, Ye J, Mai R
Received 14 August 2025
Accepted for publication 3 December 2025
Published 18 December 2025 Volume 2025:12 Pages 2825—2838
DOI https://doi.org/10.2147/JHC.S560567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Mohamed Shaker
Jie Zeng,1,2,* Hongyang Huang,1,* Minchao Tang,1,* Zheng Tao,1 Kaixiang Mo,1 Weijie Chen,1 Yuejiao Su,3 Jinting Su,3 Rong Liang,3,4 Yan Lin,3,4 Lequn Li,1 Guobin Wu,1 Xiaoling Luo,4,5 Jiazhou Ye,1,4 Rongyun Mai1,4,5
1Department of Hepatobiliary & Pancreatic Surgery, Guangxi Medical University Cancer Hospital, Guangxi Medical University, Nanning, 530021, People’s Republic of China; 2Department of Physiology, School of Basic Medical Sciences, Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 3Department of Digestive Oncology, Guangxi Medical University Cancer Hospital, Guangxi Medical University, Nanning, 530021, People’s Republic of China; 4Guangxi Liver Cancer Diagnosis and Treatment Engineering and Technology Research Center, Nanning, 530021, People’s Republic of China; 5Department of Experimental Research, Guangxi Medical University Cancer Hospital, Guangxi Medical University, Nanning, 530021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiazhou Ye, Email [email protected] Rongyun Mai, Email [email protected]
Background: Microvascular invasion (MVI) serves as a well-established prognostic factor for tumor recurrence and reduced survival following curative hepatectomy in hepatocellular carcinoma (HCC). This investigation aims to assess the therapeutic value of postoperative adjuvant transcatheter arterial chemoembolization (PA-TACE) in HCC patients with MVI and delineate the optimal patient subpopulations for this intervention.
Methods: This retrospective cohort study analyzed patients with MVI in HCC patients who received curative resection from September 2013 to June 2019. After balancing baseline differences between the PA-TACE group and the non-TACE control group using propensity score matching (PSM), the differences in recurrence-free survival (RFS) and overall survival (OS) between the two groups were compared. A multivariate Cox proportional hazards regression model was used to identify independent prognostic factors.
Results: Among 440 evaluable patients, PA-TACE demonstrated statistically significant improvements in both RFS and OS compared to non-TACE management, with consistent results observed in both the entire and propensity score-matched cohorts. Multivariate analysis established PA-TACE as an independent protective predictor for both RFS and OS. Subgroup analyses revealed pronounced clinical benefits in patients exceeding Milan criteria and those presenting with high-risk features including serum AFP ≥ 400 ng/mL, tumor size ≥ 5 cm, Edmondson-Steiner grade III/IV differentiation, M2-type MVI, or major hepatectomy. Notably, no survival advantage was observed in patients within Milan criteria or BCLC-A/B stages.
Conclusion: PA-TACE provides substantial survival enhancement in HCC patients with MVI exceeding Milan criteria or with high-risk features, but offers limited benefit for Milan-eligible cases. Patient selection based on tumor biology is critical for optimizing adjuvant therapy.
Keywords: hepatocellular carcinoma, microvascular invasion, postoperative adjuvant transcatheter arterial chemoembolization, recurrence-free survival, overall survival
Introduction
Hepatocellular carcinoma (HCC), the most prevalent form of liver cancer, persists as a major global health challenge despite recent therapeutic innovations. Curative-intent hepatectomy remains the cornerstone of early-stage HCC management, conferring 5-year survival rates of 50–70% in eligible cohorts.1–4 However, postoperative recurrence rates exceeding 60% persistently undermine long-term prognosis, underscoring the need for optimized adjuvant strategies. Microvascular invasion (MVI), a histopathological hallmark of tumor aggressiveness, emerges as a critical determinant of recurrence dynamics.5–8 Observational studies report MVI prevalence ranging from 15% to 57% in resected HCC specimens, with incidence escalating to 63% in larger tumors.9,10 Mechanistically, MVI facilitates intrahepatic micrometastasis through portal venous dissemination, correlating with elevated recurrence risk and serving as an independent adverse prognostic variable in multivariate analyses.11,12 More importantly, the presence of MVI profoundly reshapes the disease progression and therapeutic landscape of HCC. It not only substantially limits the long-term efficacy of curative resection but also constitutes a critical link in the vicious cycle of “resection-recurrence-treatment failure”. The highly aggressive and early-recurrence biological characteristics of HCC patients with MVI pose severe challenges to existing postoperative adjuvant treatment strategies. Consequently, precisely evaluating and enhancing the efficacy of adjuvant therapies in this specific patient population is crucial for improving their long-term survival.
Postoperative adjuvant transcatheter arterial chemoembolization (PA-TACE) has emerged as crucial strategies for mitigating recurrence in high-risk populations.13–25 Multiple studies demonstrate the efficacy of PA-TACE in reducing recurrence and improving survival for HCC patients with macrovascular invasion.18–20 However, its therapeutic value in HCC patients with MVI remains contentious. Existing retrospective studies have presented conflicting evidence regarding the efficacy of PA-TACE in this population. While several studies have demonstrated significant long-term benefits,26 others have reported no statistically significant clinical advantage.27,28 Additionally, some researchers suggest that PA-TACE may be a selective option for HCC patients with high-risk MVI, but do not recommend its use in those with low-risk MVI.23 These conflicting results, compounded by methodological limitations in case selection and insufficient adjustment for hepatic functional reserve, underscore the imperative for rigorous propensity-adjusted investigations.27
Based on these gaps, we conducted a rigorous propensity score matching (PSM) retrospective cohort study to evaluate the effect of PA-TACE on recurrence-free survival (RFS) and overall survival (OS) in HCC patients with MVI after curative liver resection. Our specific objectives were to quantify survival benefits overall, delineate differential effects across key risk factors, and assess outcomes stratified by tumor stage relative to the Milan criteria, thereby optimizing patient selection for this intervention.
Patients and Methods
Study Population
From September 2013 and June 2019, clinopathological data for HCC patients undergoing curative-intent hepatic resection at Guangxi Medical University Cancer Hospital were systematically analyzed in this retrospective cohort study. Inclusion criteria comprised: (1) initial R0 hepatectomy; (2) histologically confirmed HCC with MVI. Exclusion criteria were: (1) concurrent malignancies; (2) preoperative antitumor therapies; (3) postoperative adjuvant therapies other than TACE; (4) incomplete clinical/imaging records. The flowchart of this study is provided in Supplementary Figure 1.
Diagnosis and Definitions
Histopathological examination confirmed HCC diagnoses following surgical resection. Tumor staging adhered to the Barcelona Clinic Liver Cancer (BCLC) classification system.29 Lesions were stratified according to the Milan criteria. Those fulfilling the criteria were defined as having either a single tumor ≤5 cm in diameter or up to three discrete nodules, each ≤3 cm. Conversely, tumors exceeding the Milan criteria encompassed all lesions not meeting these conditions, such as a single tumor >5 cm, more than three nodules, or any nodule exceeding 3 cm in diameter.30 MVI was rigorously assessed on surgically resected specimens by experienced hepatopathologists. It was defined as the presence of tumor cell nests within endothelial-lined vessels in the peritumoral liver parenchyma, identified under microscopic examination. The MVI status was further categorized into two subtypes: M1, defined as ≤5 microvascular foci located within 1 cm from the tumor edge; and M2, defined as >5 foci or any focus extending beyond 1 cm from the tumor border.31 Edmondson-Steiner (ES) grading criteria were employed to assess tumor differentiation. Major hepatectomy was characterized by resection encompassing ≥3 anatomically defined Couinaud segments. RFS and OS definitions followed our prior methodology.32,33
Hepatectomy and PA-TACE Procedures
Preoperative contrast-enhanced CT/MRI assessed tumor resectability. Hepatic reserve was evaluated via Child-Pugh classification. For major hepatectomy, CT volumetry ensured residual liver volume. Surgical indications included Child-Pugh A/B, ECOG 0–2, and no distant metastasis. The information of surgery has been detailed in our previous studies.32,33
PA-TACE was typically advised for HCC patients deemed at elevated risk of postoperative recurrence, administered around one and two months following surgery. The PA-TACE procedure adhered to a standardized protocol established in our previous work.25 A chemotherapeutic emulsion was prepared using lipiodol (2–10 mL) in combination with either pirarubicin or epirubicin (10–50 mg) and oxaliplatin (25–100 mg). The dosage of each agent was individualized based on comprehensive assessment of the patient’s anthropometric profile, tumor burden and vascularity, as well as hepatic functional reserve. Under angiographic guidance following femoral artery access and celiac trunk catheterization, the tumor-feeding artery (typically segmental or subsegmental branches) was superselectively catheterized for emulsion delivery. This approach aimed to achieve precise tumor embolization while sparing non-target liver tissue; thus, infusion was not performed at the level of the proper hepatic artery.
Follow-Up
Follow-ups occurred every 2–3 months for the first 2 years and every 6 months thereafter. Evaluations included liver and kidney function, serum alpha-fetoprotein (AFP), abdominal ultrasound, and imaging examinations such as CT or MRI. Tumor recurrence was diagnosed by elevated AFP and imaging findings, with management options including TACE, radiofrequency ablation, re-resection, or molecular targeted drug therapy, as appropriate.34
Statistical Analysis
Continuous variables conforming to normal distribution were presented as mean ± standard deviation (SD) and analyzed using Student’s t-test, whereas non-normally distributed data were reported as median (interquartile range) with Mann–Whitney U-test comparisons. Categorical variables underwent comparative analysis via χ2-test or Fisher’s test.
Propensity score matching (PSM) was executed through logistic regression modeling incorporating 17 clinically relevant covariates: demographic factors (age, sex), laboratory parameters (PLT, PT, TBil, ALB, ALT, AST), tumor characteristics (tumor size or number, AFP), liver status (ascites, cirrhosis, HBV), and histopathological grades (ES, MVI), and resection extent. A 1:1 nearest-neighbor matching algorithm was applied with a 0.10 SD caliper. Survival endpoints (RFS, OS) were analyzed using Kaplan–Meier curves and Log rank tests. Multivariable Cox analysis was determined independent outcome predictors. Analyses were conducted in SPSS v26.0 (IBM), with P < 0.05 considered significant.
Results
Patients’ Characteristics
This study comprised 440 patients, with 152 (34.5%) receiving PA-TACE and 288 (65.5%) constituting the non-TACE group. Before PSM, the groups exhibited comparable demographics, laboratory parameters, tumor profiles, and surgical extent, except for significant disparities in age, serum aspartate aminotransferase (AST) levels, cirrhosis prevalence, Child-Pugh grade, and BCLC staging. Post-PSM analysis yielded 146 matched patient pairs with balanced baseline covariates (Table 1 and Supplementary Figure 2).
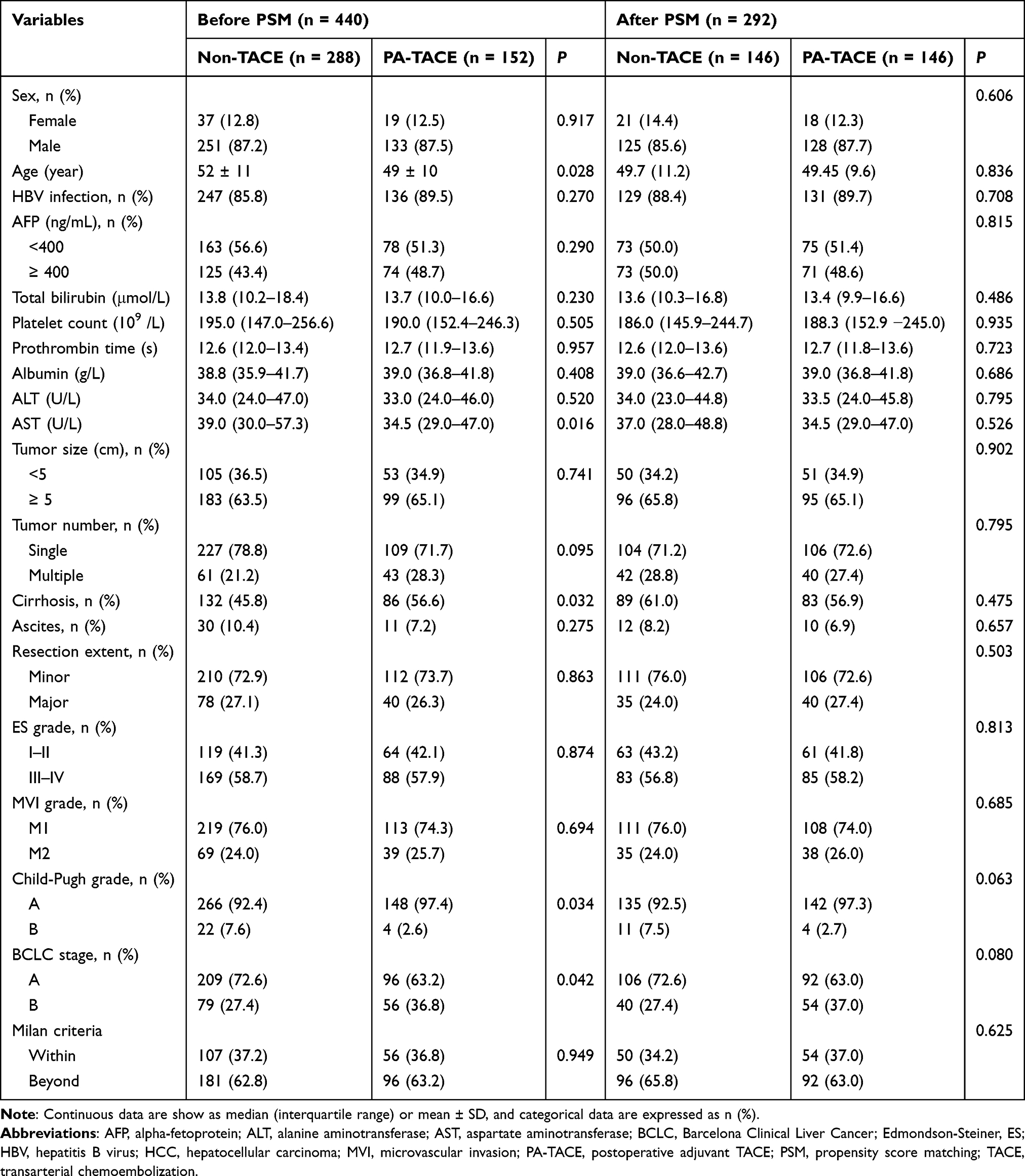 |
Table 1 Demographic and Clinical Characteristics of the Study Population Before and After PSM |
Independent Prognostic Factors for RFS
Univariate analysis identified RFS predictors including AFP ≥400 ng/mL, hepatic function markers (total bilirubin, prothrombin time, albumin, AST), tumor size, resection extent, ES grade III/IV, M2-type MVI, and PA-TACE. Multivariable analysis confirmed independent predictors: AFP ≥400 ng/mL (HR 1.335, 95% CI 1.029–1.733; P = 0.030), albumin (HR 0.975, 95% CI 0.951–0.999; P =0.041), tumor size ≥5 cm (HR 1.334, 95% CI 1.005–1.771; P =0.046), major resection (HR 1.503, 95% CI 1.137–1.987; P =0.004), ES grade III/IV (HR 1.570, 95% CI 1.198–2.057; P =0.001), and PA-TACE (HR 0.660, 95% CI 0.502–0.868; P =0.003) (Table 2). After PSM, it was found to be consistent with these results (Supplementary Table 1).
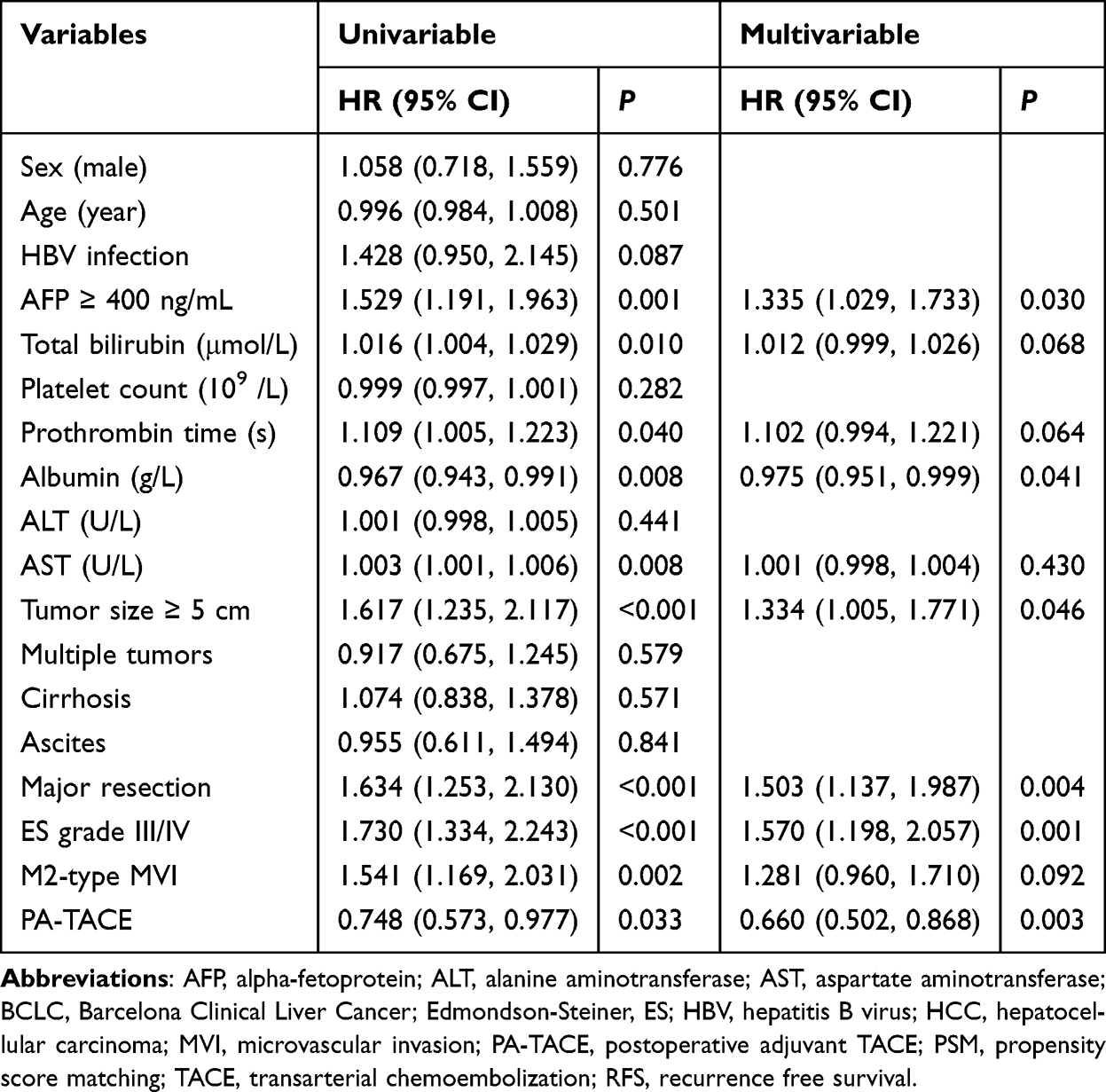 |
Table 2 Univariate and Multivariate Cox-Regression Analyses Predicting RFS in the Before PSM Cohort |
Independent Prognostic Factors for OS
Univariate analysis identified OS predictors: AFP level, total bilirubin, prothrombin time, and AST levels, tumor size, major resection, ES grade III/IV, M2-type MVI and PA-TACE. Multivariable analysis established these independent risk factors: AFP ≥400 ng/mL (HR 1.429, 95% CI 1.045–1.953; P =0.025), total bilirubin (HR 1.016, 95% CI 1.003–1.029; P =0.018), prothrombin time (HR 1.146, 95% CI 1.013–1.297; P =0.031), tumor size ≥5 cm (HR 1.431, 95% CI 1.008–2.033; P =0.045), major resection (HR 1.605, 95% CI 1.162–2.217; P =0.004), ES grade III/IV (HR 1.580, 95% CI 1.135–2.199; P =0.007), M2-type MVI (HR 1.380, 95% CI 0.990–1.923; P =0.057) and PA-TACE (HR 0.647, 95% CI 0.465–0.901; P =0.010) (Table 3). Post-PSM findings aligned with these results (Supplementary Table 2).
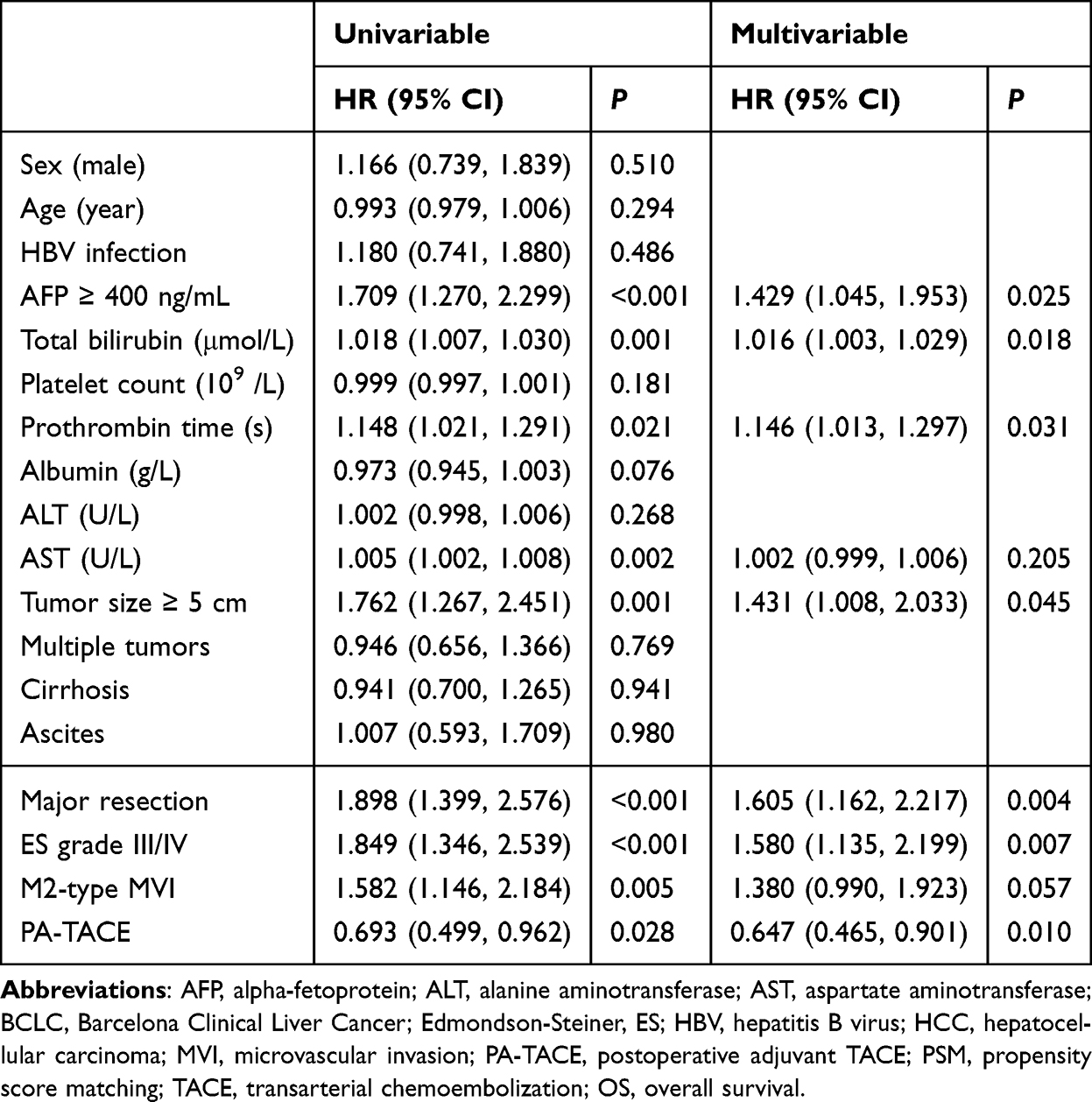 |
Table 3 Univariate and Multivariate Cox-Regression Analyses Predicting OS in the Before PSM Cohort |
Impact of PA-TACE on RFS in HCC Patients with MVI
Prior to PSM, the PA-TACE cohort demonstrated significantly superior RFS outcomes relative to the non-TACE group, evidenced by a higher median RFS (22.0 months, 95% CI: 15.1–28.9 vs 15.0 months, 95% CI: 7.7–22.3) and improved survival rates at 1-year (57.3% vs 48.8%), 3-year (30.5% vs 27.2%), and 5-year (21.9% vs 13.2%; P=0.029). This survival advantage persisted after matching, with the PA-TACE group maintaining greatly higher 1-year (57.4% vs 46.2%), 3-year (30.6% vs 23.4%), and 5-year (21.9% vs 12.3%) RFS rates (P=0.026) (Supplementary Table 3; Figure 1A and B).
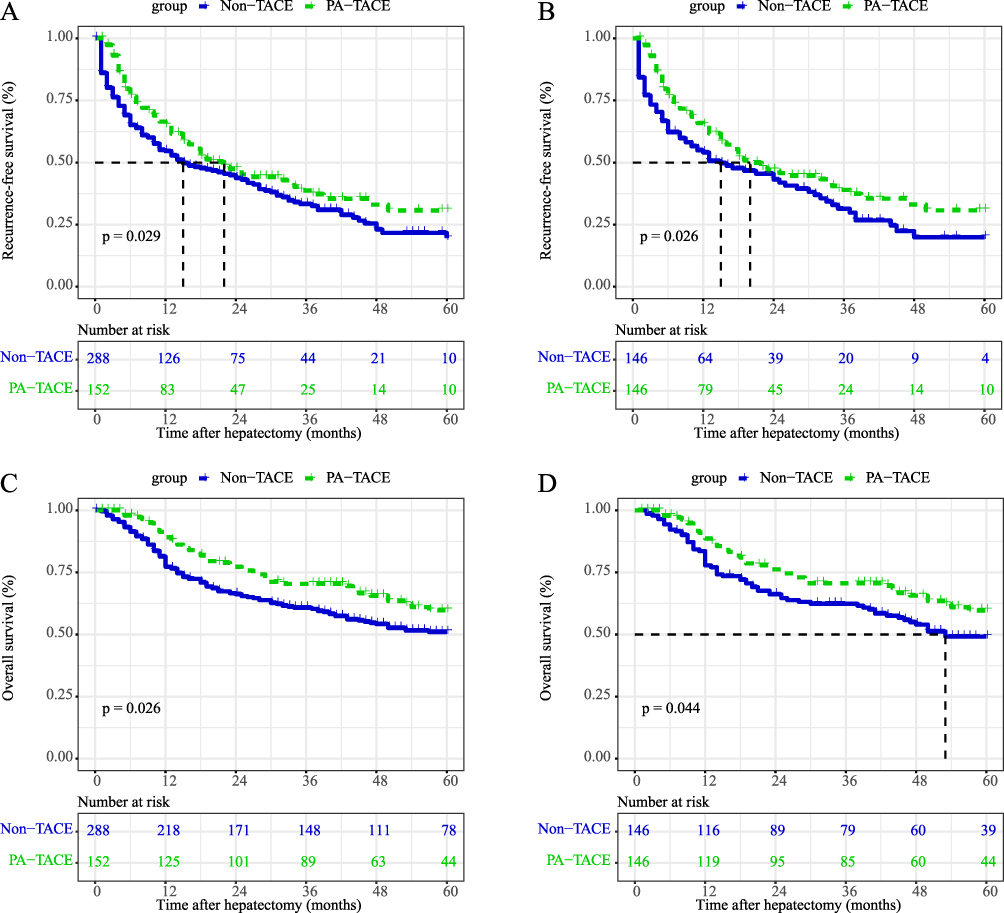 |
Figure 1 Comparative analysis of RFS and OS in HCC patients with MVI receiving PA-TACE versus non-TACE. (A) RFS in entire group; (B) OS in entire group; (C) RFS in PSM group; (D) OS in PSM group. Abbreviations: MVI, microvascular invasion; HCC, hepatocellular carcinoma; PA-TACE, postoperative adjuvant transcatheter arterial chemoembolization; TACE, PSM, transcatheter arterial chemoembolization; PSM, propensity score matching; OS, overall survival; RFS, recurrence free survival. |
Impact of PA-TACE on OS in HCC Patients with MVI
Before PSM, the PA-TACE group demonstrated a significantly longer mean OS compared to the non-TACE cohort (46.1 months, 95% CI: 42.7–49.4 vs 40.3 months, 95% CI: 37.6–43.6; P=0.026). This survival advantage was accompanied by improved survival rates at 1 year (84.1% vs 72.5%), 3 years (63.0% vs 55.1%), and 5 years (61.4% vs 45.0%). Following PSM adjustment, the PA-TACE group maintained superior long-term outcomes with significantly higher 1-/3-/5-year OS rates (83.4%/63.2%/51.2% vs 71.2%/54.0%/41.1%; P=0.044) (Supplementary Table 3; Figure 1C and D).
Subgroup Analysis
Subgroup analysis was performed to evaluate the efficacy of PA-TACE across various risk factors among HCC patients with MVI. Significant RFS benefits were observed in subgroups with AFP ≥400 ng/mL, tumor diameter ≥5 cm, major resection, ES grade III/IV, or M2-type MVI (Figure 2A–G, P<0.05). Furthermore, significant OS benefits were identified in patients with AFP ≥400 ng/mL, tumor diameter ≥5 cm, or ES grade III/IV (Figure 3A–G, P<0.05). Conversely, in patients lacking these high-risk factors, PA-TACE conferred no significant RFS or OS benefit in remaining subgroups except improved RFS and OS with solitary tumors and improved OS with M2-type MVI (Supplementary Figure 3A–G and Supplementary Figure 4A–G).
 |
Figure 2 Subgroups analyses of RFS among high risk factors in HCC patients with MVI. (A) AFP ≥400 ng/mL; (B) presence of cirrhosis; (C) tumor size ≥ 5cm; (D) multiple tumor numbers; (E) major resection; (F) ES grade III/IV; (G) M2-type MVI. Abbreviations: AFP, alpha-fetoprotein; MVI, microvascular invasion; ES, Edmondson-Steiner; HCC, hepatocellular carcinoma; PA-TACE, postoperative adjuvant transcatheter arterial chemoembolization; TACE, transcatheter arterial chemoembolization; RFS, recurrence free survival. |
 |
Figure 3 Subgroups analyses of OS among high risk factors in HCC patients with MVI. (A) AFP ≥400 ng/mL; (B) presence of cirrhosis; (C) tumor size ≥ 5cm; (D) multiple tumor numbers; (E) major resection; (F) ES grade III/IV; (G) M2-type MVI. Abbreviations: AFP, alpha-fetoprotein; MVI, microvascular invasion; ES, Edmondson-Steiner; HCC, hepatocellular carcinoma; PA-TACE, postoperative adjuvant transcatheter arterial chemoembolization; TACE, transcatheter arterial chemoembolization; OS, overall survival. |
Furthermore, stratified analyses assessed PA-TACE efficacy across tumor stages. In BCLC-A or B stage HCC patients with MVI, PA-TACE showed no significant differences in RFS or OS compared to the non-TACE group (all P > 0.05; Figure 4A–D). Similarly, PA-TACE did not improve RFS or OS in patients meeting the Milan criteria (all P > 0.05; Figure 4E and F). Notably, patients exceeding Milan criteria derived significant clinical benefits from PA-TACE, with improved RFS and OS (RFS: P = 0.021, Figure 4G; OS: P = 0.049, Figure 4H). Multivariable analysis confirmed PA-TACE as an independent favorable prognostic factor specifically in HCC patients with MVI beyond Milan criteria (RFS: HR 0.688, 95% CI 0.495–0.957, P = 0.006; OS: HR 0.643, 95% CI 0.434–0.952, P = 0.027), while showing no significant association in patients within Milan criteria (RFS: HR 0.836, 95% CI 0.529–1.323, P = 0.444; OS: HR 0.671, 95% CI 0.365–1.233, P = 0.198).
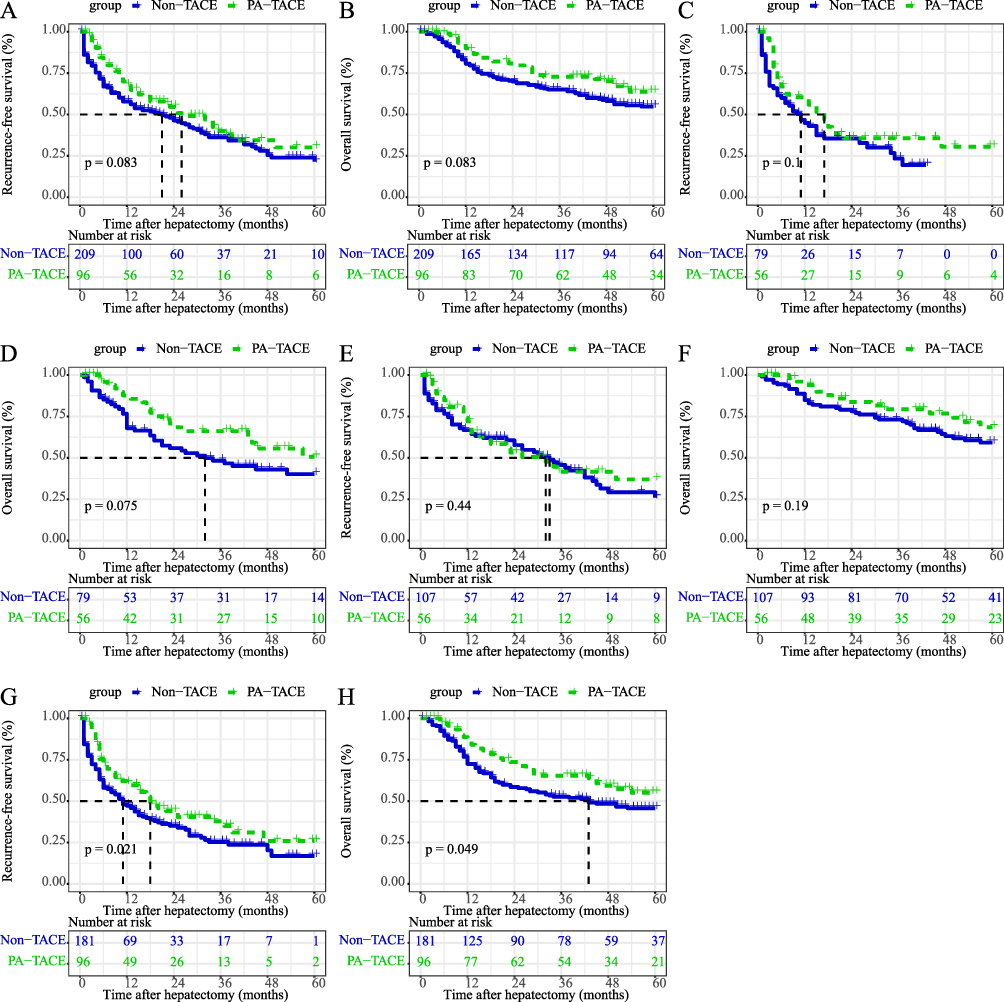 |
Figure 4 Subgroups analyses of RFS and OS in HCC patients with MVI at different tumor stage. (A) RFS, BCLC stage 0 or A; (B) OS, BCLC stage 0 or A; (C) RFS, BCLC stage B or C; (D) OS, BCLC stage B or C; (E) RFS, within Milan criteria; (F) OS, within Milan criteria; (G) RFS, beyond Milan criteria; (H) OS, beyond Milan criteria. Abbreviations: MVI, microvascular invasion; HCC, hepatocellular carcinoma; PA-TACE, postoperative adjuvant transcatheter arterial chemoembolization; TACE, transcatheter arterial chemoembolization; BCLC, Barcelona Clinical Liver Cancer; RFS, recurrence free survival; OS, overall survival. |
Discussion
This study found that PA-TACE was associated with improved RFS and OS in HCC patients with MVI after curative resection. After rigorous PSM to mitigate confounding factors, PA-TACE independently reduced recurrence risk by 34% (HR 0.654, P = 0.002) and mortality risk by 35% (HR 0.647, P = 0.010). Crucially, therapeutic benefits were selective, with pronounced survival advantages restricted to high-risk subgroups: AFP ≥400 ng/mL, tumor size ≥ 5cm, ES grade III/IV, M2-type MVI, or those exceeding Milan criteria.
MVI, present in 60–90% of HCCs >5 cm, is a histopathologic hallmark of aggressive biology and a powerful predictor of early recurrence.35 MVI signifies aggressive tumor biology and heightened risk of occult metastases. As MVI can only be diagnosed post-resection, adjuvant therapies are critical for mitigating recurrence risk.5,6,9–12 TACE delivers localized chemotherapy and ischemia, potentially eradicating residual micrometastases or circulating tumor cells after liver resection.25 While PA-TACE is established for high-risk HCC, its role in HCC patients with MVI cohorts remained uncertain. Our data confirmed that PA-TACE independently improves both RFS and OS in HCC patients with MVI, aligns with mechanistic understanding. Subsequent multivariate modeling consistently identified PA-TACE as an independent favorable prognostic determinant, demonstrating significant protective associations with both RFS (before PSM, HR 0.660, P=0.010; After PSM, HR 0.627, P=0.003) and OS (before PSM, HR 0.647, P=0.010; After PSM, HR 0.668, P=0.035), thereby supporting its pathophysiological rationale in this therapeutic context. The consistency of these results before and after PSM underscores their reliability, mitigating concerns about selection bias.
However, the true clinical value emerges from our granular subgroup and stratification analyses. Our finding showed that the significant RFS and OS benefit of PA-TACE in HCC patients with MVI with specific high-risk biological features including AFP ≥400 ng/mL, tumor size ≥ 5cm, ES III/IV grade, M2-type MVI reflects a multidimensional therapeutic alignment between tumor pathophysiology and treatment mechanisms. Elevated AFP concentrations establish an immunosuppressive pro-angiogenic microenvironment36–38 that PA-TACE effectively reverses through dual mechanisms: selective vascular disruption of VEGF-dependent neovessels combined with localized tumor necrosis that releases endogenous antigens, thereby converting the treated lesion into an immunogenic reservoir that counteracts AFP-mediated immune tolerance.39–41 Large tumors demonstrate heightened therapeutic vulnerability due to their distinct hemodynamic characteristics,42 where hypoxia-induced peripheral arterialization enhances susceptibility to ischemia from embolization while elevated proliferative activity increases intracellular uptake of cytotoxic agents, creating synergistic therapeutic effects through combined ischemic and chemotherapeutic cytotoxicity.43,44 Poorly differentiated tumors exhibit two complementary therapeutic vulnerabilities: inherent genomic instability amplifies chemotherapy-induced apoptosis while their disorganized vasculature paradoxically improves therapeutic agent retention through enhanced lipiodol deposition and sustained drug release.45 For aggressive M2-type MVI, PA-TACE achieves micrometastatic control through concurrent spatial and biological effects: direct chemotherapy delivery to radiologically undetectable satellite lesions combined with embolization-induced endothelial stabilization, which collectively inhibit circulating tumor cell colonization.46 These high-risk biological parameters create a unique therapeutic context where PA-TACE’s triad of vascular occlusion, cytotoxic delivery, and immune modulation converge to disrupt critical pathways in metastatic progression, establishing its selective superiority in this molecularly defined patient subset over those with less aggressive biological profiles.
Stratification based on tumor staging revealed critical clinical implications. The pronounced improvement in RFS and OS with PA-TACE was specifically observed in patients exceeding Milan criteria, while no comparable benefit emerged for those meeting Milan criteria or classified as BCLC-A/B stages. This differential response highlights the critical interplay between tumor biology and tumor burden in therapeutic efficacy. Patients beyond Milan criteria typically exhibit higher-risk features including larger tumor dimensions, multifocal presentations, and an intrinsically elevated recurrence potential.47,48 In this population, PA-TACE appears effective in addressing the biological limitations of surgical resection alone by controlling micronodular spread. The multivariable analysis specifically identified PA-TACE as an independent prognostic enhancer specific to this subpopulation, underscoring the rationale for precision deployment in this disease context. These findings necessitate reevaluation of conventional TACE selection criteria that prioritize technical resectability over comprehensive biological risk assessment, advocating for more sophisticated stratification models in treatment algorithms.
The histopathological confirmation of MVI status and grading remains exclusively dependent on surgical specimen analysis, underscoring the critical importance of postoperative adjuvant strategies for recurrence mitigation. Clinically, while PA-TACE constitutes the most prevalent adjuvant intervention, our findings revealed its therapeutic limitations in HCC patients with MVI meeting Milan criteria, a population paradoxically excluded from demonstrated benefits. Building upon these findings, we propose several directions for future research. First, there is an urgent need to develop novel diagnostic biomarkers (eg, liquid biopsy, radiomics) to enable accurate preoperative MVI prediction. Second, individualized treatment strategies should be constructed based on distinct risk profiles—particularly integrating our observation that PA-TACE benefits are confined to patients exceeding Milan criteria. Finally, the role of PA-TACE in future precision medicine frameworks requires redefinition: rather than a universal adjuvant, it should be reserved for selected high-risk subgroups, potentially in combination with systemic therapies. This refined therapeutic perspective emphasizes the imperative for enhanced preoperative MVI prediction and optimized surgical strategies. The novel nomogram developed by Lei et al,49 incorporating seven clinicopathological parameters for preoperative MVI risk stratification in HBV-related Milan-criteria HCC, enables individualized surgical planning. For high-risk candidates, procedural optimization through anatomical resection paradigms and extended resection margins (≥1 cm) may confer survival advantages.
Several limitations warrant acknowledgment. Firstly, the retrospective, single-center design carries inherent risks of bias and unmeasured confounding, despite statistical adjustments, which may limit the generalizability of our findings to institutions with different patient demographics or healthcare practices. Secondly, the high prevalence of HBV infection defines the specific etiological context of our cohort, reflecting the regional epidemiology of an endemic area; consequently, the applicability of our results to populations with different predominant causes of liver disease (such as HCV or alcohol-related) requires further validation. Finally, the inability to analyze individualized TACE regimens (eg, specific chemotherapeutic agents and embolic materials) in relation to key baseline characteristics may have influenced the observed outcomes. Future prospective, multi-center studies encompassing diverse epidemiological backgrounds and standardized treatment protocols are needed to address these limitations and refine patient selection.
Conclusion
Our analysis found that PA-TACE was associated with improved RFS and OS in HCC patients with MVI following curative liver resection, particularly among those exhibiting aggressive tumor biological features (eg, higher AFP level, larger tumor size, poorer differentiation) or those with tumor burden exceeding the Milan criteria. However, its survival benefit is limited in patients meeting Milan criteria or BCLC-A/B stages. Clinical implementation should prioritize personalized risk stratification incorporating tumor pathology, staging, and liver function to optimize patient selection.
Abbreviations
AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinical Liver Cancer; ES, Edmondson-Steiner; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; MVI, microvascular invasion; TACE, transcatheter arterial chemoembolization; PA-TACE, postoperative adjuvant transcatheter arterial chemoembolization; PSM, propensity score matching; RFS, recurrence-free survival; OS, overall survival.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved and supervised by the Ethics Committee of Guangxi Medical University Cancer Hospital and conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was waived by the ethics committee owing to the retrospective nature of the research. We confirm that all patient data were kept confidential. All procedures were performed in compliance with relevant guidelines and regulations.
Author Contributions
All authors have reviewed the final version to be published and agreed to be accountable for all aspects of the work. Concept and design: Jie Zeng, Xiaoling Luo, Jiazhou Ye, Rongyun Mai. Acquisition, analysis, or interpretation of data: Jie Zeng, Minchao Tang, Hongyang Huang, Zheng Tao, Kaixiang Mo, Weijie Chen, Yuejiao Su, Jinting Su. Drafting of the manuscript: Jie Zeng, Minchao Tang, Hongyang Huang, Rongyun Mai. Critical review of the manuscript for important intellectual content: Xiaoling Luo, Jiazhou Ye, Rongyun Mai. Supervision: Rong Liang, Yan Lin, Lequn Li.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Guangxi Natural Science Foundation (No. 2025GXNSFBA069552, 2025GXNSFDA069007, 2024GXNSFDA010046, 2024GXNSFAA010401); National Natural Science Foundation of China (No.82460611, 82060427, 82103297); Project for Enhancing Young and Middle-aged Teacher’s Research Basis Ability in Colleges of Guangxi (NO. 2024KY0133); Youth Program of Scientific Research Foundation of Guangxi Medical University Cancer Hospital (NO.2023-7); Guangxi First Batch Qingmiao Young Talents Universal Support Policy Program; Guangxi Bagua Youth Outstanding Talent Training Program; Guangxi Medical and health key discipline construction project; Guangxi Medical and health key cultivation discipline construction project; Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University; Guangxi Scholarship Fund of Guangxi Education Department; Guangxi Medical University Outstanding Young Talents Training Program; Guangxi Medical University Cancer Hospital Outstanding Doctoral Support Project; Nanning Qingxiu District Science and Technology Project (No.2021010, 2021007, 2021012).
Disclosure
The authors declare that they have no competing interests.
References
1. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
2. Chidambaranathan-Reghupaty S, Fisher PB, Sarkar D. Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification. Adv Cancer Res. 2021;149:1–61.
3. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
4. Rezaee-Zavareh MS, Liang J, Yang JD. Ethnic disparities in the epidemiology, treatment, and outcome of patients with hepatocellular carcinoma in the United States. Hepatoma Res. 2023;9:10. doi:10.20517/2394-5079.2023.10
5. Zhang XP, Zhang TC, Wu FF, et al. Patterns and outcomes of early and late recurrence after hepatectomy for hepatocellular carcinoma with microvascular invasion: a multicenter study in China. Hepatol Int. 2025;19(4):903–914. doi:10.1007/s12072-025-10802-w
6. Fuster-Anglada C, Mauro E, Ferrer-Fàbrega J, et al. Histological predictors of aggressive recurrence of hepatocellular carcinoma after liver resection. J Hepatol. 2024;81(6):995–1004. doi:10.1016/j.jhep.2024.06.018
7. Chen W, Rong Y, Ma T, Shi W, Chen W, Jiang H. Classification of microvascular invasion of hepatocellular carcinoma: different standards, common goals: letter to the editor on “Classification of microvascular invasion of hepatocellular carcinoma: correlation with prognosis and magnetic resonance imaging”. Clin Mol Hepatol. 2025;31(3):e249–e251. doi:10.3350/cmh.2025.0167
8. Zhang X, Hu M, Liu R. Recognizing significant role of microvascular invasion in postoperative aggressive recurrence of early hepatocellular carcinoma. J Hepatol. 2025;82(4):e197–e198.
9. Pawlik TM, Delman KA, Vauthey JN, et al. Tumor size predicts vascular invasion and histologic grade: implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transpl. 2005;11(9):1086–1092. doi:10.1002/lt.20472
10. Li K, Zhang R, Wen F, et al. Single-cell dissection of the multicellular ecosystem and molecular features underlying microvascular invasion in HCC. Hepatology. 2024;79(6):1293–1309. doi:10.1097/HEP.0000000000000673
11. Li SH, Mei J, Cheng Y, et al. Postoperative adjuvant hepatic arterial infusion chemotherapy with FOLFOX in hepatocellular carcinoma with microvascular invasion: a multicenter, Phase III, randomized study. J Clin Oncol. 2023;41(10):1898–1908. doi:10.1200/JCO.22.01142
12. Shi C, Li Y, Geng L, et al. Adjuvant stereotactic body radiotherapy after marginal resection for hepatocellular carcinoma with microvascular invasion: a randomised controlled trial. Eur J Cancer. 2022;166:176–184. doi:10.1016/j.ejca.2022.02.012
13. Wang H, Du PC, Wu MC, Cong WM. Postoperative adjuvant transarterial chemoembolization for multinodular hepatocellular carcinoma within the Barcelona clinic liver cancer early stage and microvascular invasion. Hepatobiliary Surg Nutr. 2018;7(6):418–428. doi:10.21037/hbsn.2018.09.05
14. He K, Xiao Y, Tu S, et al. Efficacy evaluation of postoperative adjuvant transarterial chemoembolization in preventing hepatocellular carcinoma recurrence within the Milan criteria: a multicenter propensity score matching analysis based on pathologic indicators. J Gastrointest Surg. 2025;29(4):101978. doi:10.1016/j.gassur.2025.101978
15. Zhang XP, Liu YC, Chen ZH, et al. Postoperative adjuvant transarterial chemoembolization improves outcomes of hepatocellular carcinoma associated with hepatic vein invasion: a propensity score matching analysis. Ann Surg Oncol. 2019;26(5):1465–1473. doi:10.1245/s10434-019-07223-z
16. Yang XW, Chen J, Yang MQ, et al. Postoperative adjuvant transarterial chemoembolization prolongs overall survival in alpha-fetoprotein-negative hepatocellular carcinoma with bile duct tumor thrombosis: a long-term retrospective cohort study. World J Surg Oncol. 2025;23(1):260. doi:10.1186/s12957-025-03917-9
17. Tao M, Xueli B, Qi Z, et al. Adjuvant transarterial chemoembolization for hepatocellular carcinoma following curative resection: a randomized, open-label, Phase 3 trial. Hepatology. 2025;82(5):1112–1121. doi:10.1097/HEP.0000000000001233
18. Liang L, Li C, Diao YK, et al. Survival benefits from adjuvant transcatheter arterial chemoembolization in patients undergoing liver resection for hepatocellular carcinoma: a systematic review and meta-analysis. Therap Adv Gastroenterol. 2020;13:1756284820977693. doi:10.1177/1756284820977693
19. Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg. 2009;198(3):313–318. doi:10.1016/j.amjsurg.2008.09.026
20. Zheng Z, Liang W, Wang D, et al. Adjuvant chemotherapy for patients with primary hepatocellular carcinoma: a meta-analysis. Int J Cancer. 2015;136(6):E751–9. doi:10.1002/ijc.29203
21. Leng Z, Zhu T, Huang Z, et al. Adjuvant TACE improves prognosis after resection in dual-phenotype hepatocellular carcinoma: a propensity score-matched study. J Hepatocell Carcinoma. 2025;12:2213–2224. doi:10.2147/JHC.S549670
22. Li Y, Wang K, Qin H, et al. Whether adjuvant TACE plus TKI therapy is more effective than TACE alone in HCC patients at high risks of recurrence following radical hepatectomy. J Hepatocell Carcinoma. 2025;12:1767–1780. doi:10.2147/JHC.S534143
23. Lu J, Feng J, Zhao Y, et al. Grading risk of microvascular invasion impacts survival in hepatocellular carcinoma patients undergoing adjuvant transarterial chemoembolization: a multicenter study. Eur J Surg Oncol. 2025;51(8):110102. doi:10.1016/j.ejso.2025.110102
24. Su JY, Huang DJ, Liu SP, et al. Adjuvant transarterial chemoembolization after truly curative resection does not improve survival of patients with hepatocellular carcinoma at high risk of recurrence: a target trial emulation study. Hepatol Res. 2025;55(9):1263–1273. doi:10.1111/hepr.14219
25. Mai RY, Tao Z, Huang HY, et al. Postoperative adjuvant transcatheterarterial chemoembolization should be considered selectively for patients with cytokeratin-19 positive hepatocellular carcinoma. J Hepatocell Carcinoma. 2025;12:2407–2419. doi:10.2147/JHC.S537915
26. Sun JJ, Wang K, Zhang CZ, et al. Postoperative adjuvant transcatheter arterial chemoembolization after R0 hepatectomy improves outcomes of patients who have hepatocellular carcinoma with microvascular invasion. Ann Surg Oncol. 2016;23(4):1344–1351. doi:10.1245/s10434-015-5008-z
27. Ke-Wei L, Tian-Fu W, Xi L, et al. The effect of postoperative TACE on prognosis of HCC with microscopic venous invasion. Hepatogastroenterology. 2012;59(118):1944–1946. doi:10.5754/hge11845
28. Peng Y, Shen S, Feng Y, et al. Prognostic analysis and limited efficacy of adjuvant TACE in hepatocellular carcinoma following hepatectomy: a propensity score-matched study. Langenbecks Arch Surg. 2025;410(1):92. doi:10.1007/s00423-025-03663-2
29. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
30. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699. doi:10.1056/NEJM199603143341104
31. Roayaie S, Blume IN, Thung SN, et al. A system of classifying microvascular invasion to predict outcome after resection in patients with hepatocellular carcinoma. Gastroenterology. 2009;137(3):850–855. doi:10.1053/j.gastro.2009.06.003
32. Mai R, Bai T, Luo X, Wu G. Preoperative fibrinogen-to-albumin ratio predicts the prognosis of patients with hepatocellular carcinoma subjected to hepatectomy. BMC Gastroenterol. 2022;22(1):261. doi:10.1186/s12876-022-02328-4
33. Mai RY, Lu TL, Lu RJ, et al. C-reactive protein-albumin ratio (CAR): a more promising inflammation-based prognostic marker for patients undergoing curative hepatectomy for hepatocellular carcinoma. J Inflamm Res. 2024;17:919–931. doi:10.2147/JIR.S441623
34. Zeng J, Lu R, Tao Z, et al. A CART-based prognostic model for risk stratification of postoperative early recurrence in hepatocellular carcinoma with microvascular invasion. Front Oncol. 2025;15. doi:10.3389/fonc.2025.1655739
35. de Lope CR, Tremosini S, Forner A, Reig M, Bruix J. Management of HCC. J Hepatol. 2012;56 Suppl 1:S75–87. doi:10.1016/S0168-8278(12)60009-9
36. Meng W, Bai B, Bai Z, et al. The immunosuppression role of alpha-fetoprotein in human hepatocellular carcinoma. Discov Med. 2016;21(118):489–494.
37. Santos PM, Menk AV, Shi J, Tsung A, Delgoffe GM, Butterfield LH. Tumor-derived α-fetoprotein suppresses fatty acid metabolism and oxidative phosphorylation in dendritic cells. Cancer Immunol Res. 2019;7(6):1001–1012. doi:10.1158/2326-6066.CIR-18-0513
38. Yang X, Zhang Y, Zhang L, Zhang L, Mao J. Silencing alpha-fetoprotein expression induces growth arrest and apoptosis in human hepatocellular cancer cell. Cancer Lett. 2008;271(2):281–293. doi:10.1016/j.canlet.2008.06.017
39. Wang Y, Chen Y, Ge N, et al. Prognostic significance of alpha-fetoprotein status in the outcome of hepatocellular carcinoma after treatment of transarterial chemoembolization. Ann Surg Oncol. 2012;19(11):3540–3546. doi:10.1245/s10434-012-2368-5
40. Pinto E, Pelizzaro F, Cardin R, et al. HIF-1α and VEGF as prognostic biomarkers in hepatocellular carcinoma patients treated with transarterial chemoembolization. Dig Liver Dis. 2024;56(5):872–879. doi:10.1016/j.dld.2023.09.019
41. Schicho A, Hellerbrand C, Krüger K, et al. Impact of different embolic agents for transarterial chemoembolization (TACE) procedures on systemic vascular endothelial growth factor (VEGF) levels. J Clin Transl Hepatol. 2016;4(4):288–292.
42. Choi GH, Han DH, Kim DH, et al. Outcome after curative resection for a huge (>or=10 cm) hepatocellular carcinoma and prognostic significance of gross tumor classification. Am J Surg. 2009;198(5):693–701. doi:10.1016/j.amjsurg.2008.09.019
43. Chung SW, Kim JS, Choi WM, et al. Synergistic effects of transarterial chemoembolization and lenvatinib on HIF-1α ubiquitination and prognosis improvement in hepatocellular carcinoma. Clin Cancer Res. 2025;31(10):2046–2055. doi:10.1158/1078-0432.CCR-24-1228
44. Lin ZH, Jiang JR, Ma XK, et al. Prognostic value of serum HIF-1α change following transarterial chemoembolization in hepatocellular carcinoma. Clin Exp Med. 2021;21(1):109–120. doi:10.1007/s10238-020-00667-8
45. Nakachi K, Tamai H, Mori Y, et al. Prediction of poorly differentiated hepatocellular carcinoma using contrast computed tomography. Cancer Imag. 2014;14(1):7. doi:10.1186/1470-7330-14-7
46. Sheng X, Ji Y, Ren GP, et al. A standardized pathological proposal for evaluating microvascular invasion of hepatocellular carcinoma: a multicenter study by LCPGC. Hepatol Int. 2020;14(6):1034–1047. doi:10.1007/s12072-020-10111-4
47. Tsilimigras DI, Ntanasis-Stathopoulos I, Moris D. Recurrence beyond Milan criteria following liver resection for early-stage hepatocellular carcinoma: incidence, prediction and implications for treatment selection. Hepatobiliary Surg Nutr. 2025;14(2):305–307. doi:10.21037/hbsn-2025-45
48. Ferrer-Fàbrega J, Sampson-Dávila J, Forner A, et al. Limited tumour progression beyond Milan criteria while on the waiting list does not result in unacceptable impairment of survival. J Hepatol. 2021;75(5):1154–1163. doi:10.1016/j.jhep.2021.06.015
49. Lei Z, Li J, Wu D, et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis B virus-related hepatocellular carcinoma within the milan criteria. JAMA Surg. 2016;151(4):356–363. doi:10.1001/jamasurg.2015.4257
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Preoperative Serum AFP, CEA, and CA19-9 Levels in Patients with Single Small Hepatocellular Carcinoma: Retrospective Study
Gan L, Ren S, Lang M, Li G, Fang F, Chen L, Liu Y, Han R, Zhu K, Song T
Journal of Hepatocellular Carcinoma 2022, 9:799-810
Published Date: 13 August 2022
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023
Clinical Complete Response After Conversion Therapy for Unresectable Hepatocellular Carcinoma: Is Salvage Hepatectomy Necessary?
Wu JY, Wu JY, Liu DY, Li H, Zhuang SW, Li B, Zhou JY, Huang JY, Zhang ZB, Li SQ, Yan ML, Wang YD
Journal of Hepatocellular Carcinoma 2023, 10:2161-2171
Published Date: 5 December 2023
Negative Impact of Intra-Operative Blood Transfusion on Survival Outcomes of Hepatocellular Carcinoma Patients
Teng L, Zhao L, Shao H, Dai J, Zou H
Cancer Management and Research 2024, 16:385-393
Published Date: 25 April 2024
Postoperative Adjuvant Transcatheterarterial Chemoembolization Should Be Considered Selectively for Patients with Cytokeratin-19 Positive Hepatocellular Carcinoma
Mai RY, Tao Z, Huang HY, Zeng C, Mo KX, Zeng DD, Liang R, Lin Y, Wang XB, Bai T, Li LQ, Ye JZ, Wu GB
Journal of Hepatocellular Carcinoma 2025, 12:2407-2419
Published Date: 27 October 2025