")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Predictive Value of Preoperative Serum AFP, CEA, and CA19-9 Levels in Patients with Single Small Hepatocellular Carcinoma: Retrospective Study
Authors Gan L , Ren S , Lang M, Li G, Fang F, Chen L, Liu Y, Han R , Zhu K, Song T
Received 29 May 2022
Accepted for publication 4 August 2022
Published 13 August 2022 Volume 2022:9 Pages 799—810
DOI https://doi.org/10.2147/JHC.S376607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Leijuan Gan,* Shaohua Ren,* Mengran Lang,* Guangtao Li, Feng Fang, Lu Chen, Yayue Liu, Ruyu Han, Kangwei Zhu, Tianqiang Song
Liver Cancer Center, Tianjin Medical University Cancer Institute & Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tianqiang Song, Liver Cancer Center, Tianjin Medical University Cancer Institute & Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China, Email [email protected]
Purpose: This study aimed to explore the relationship between the tumor marker score (TMS) and the postoperative recurrence of single small hepatocellular carcinoma (HCC).
Patients and Methods: A total of 409 patients with one resectable HCC with a diameter of 3 cm or less who visited Tianjin Medical University Cancer Institute & Hospital from January 2010 to December 2014 were included in this study. Their alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9) levels were classified into low and high groups using X-tile software. Each patients’ TMS was calculated as the sum of each tumor marker (low = 0; high = 1).
Results: A total of 142 patients were classified as TMS0, 171 as TMS1, and 96 as TMS2. Kaplan–Meier analysis illustrated that TMS could divide the patients into groups with remarkably different prognoses, and the patients with high TMS had worse recurrence-free survival (RFS) than those with low TMS. Multivariate analysis showed that TMS, age, and HBeAg positive were the independent predictors of RFS rate. Subgroup analysis revealed that high TMS was a stable risk factor relative to TMS0. Receiver operating curves showed that the 1-, 3-, and 5-year area under curve (AUC) values of TMS were 0.698, 0.662, and 0.673, respectively. The AUC of TMS was higher than that of other common prognostic models in time-dependent receiver operating curve.
Conclusion: TMS was an independent prognostic factor for the postoperative recurrence of a single small HCC and can provide a well-discriminated risk stratification, thus contributing to prognostic prediction and adjuvant therapeutic development.
Keywords: hepatocellular carcinoma, recurrence-free survival, tumor marker score, alpha-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19-9
Introduction
Hepatocellular carcinoma (HCC) was the sixth most common cancer and the third leading cause of cancer death worldwide in 2020.1 Approximately 900,000 new cases of HCC have been reported, and China accounted for more than half of these cases.2 With the enhanced awareness of patients’ physical examination and the improvement of hospitals’ diagnosis, the number of patients diagnosed with early HCC is increasing. In the Barcelona Clinic Liver Cancer (BCLC) system, a single HCC less than 2 cm is classified as a very early stage,3 and a single nodule less than 3 cm is classified as an early stage.4–6 Although surgical treatments, such as transplantation, surgical resection, and ablation, may be effective for BCLC stage A HCC, the 5-year overall survival rate after developing this cancer is only 50%–70%,7–9 and the high incidence of postoperative recurrence remains a major issue.10,11 Thus, biomarkers that can predict postoperative recurrence must be urgently explored.
Alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9) are well-known tumor markers in the diagnosis and prognosis of hepatobiliary pancreatic malignancies and have been incorporated in various prognostic models.12–17 As a common practical clinical biomarker, AFP is widely used in HCC,18 and an increased serum AFP level is usually related to a high risk of HCC development and a poor prognosis.19 CEA is a relatively non-specific antigen widely used in the clinical diagnosis and treatment monitoring of gastrointestinal cancer.20 Its high serum level is considered as an independent predictor of recurrence in patients with HCC.21–23 CA19-9 is mainly used as a sensitive biomarker for pancreatic malignancies,24 and a high level of it is also associated with poor prognosis in patients with HCC.25 CA19-9 was found to be related to severe cirrhosis and liver inflammation,26 leading to a poor prognosis in patients with HCC. Approximately 30% of patients with HCC have an elevated serum level.25,27 The tumor marker score (TMS) based on AFP, CEA, and CA19-9 is correlated with the prognosis of combined hepatocellular-cholangiocarcinoma.23,28,29 However, the relationship between prognosis and TMS in patients with early HCC remains unclear.
To resolve this question, this study retrospectively analyzed the relationship between the recurrence of a single small HCC and TMS to compare the predictive performance of TMS with other prognostic models, including clinical stages.
Materials and Methods
Patients and Data Collection
A total of 546 patients with a single small HCC underwent surgery at Tianjin Medical University Cancer Institute & Hospital from January 2010 to December 2014. Among these patients, 28 received other treatments, 13 received postoperative adjuvant therapy, 1 had an unclear diagnosis, 8 received incomplete radiofrequency ablation (RFA), 47 had incomplete clinical data, and 40 were lost of follow-up. Finally, 409 patients were enrolled in this study (Figure 1).
 |
Figure 1 Flowchart of patient selection. |
The patients received local tumor resection with surgical margin ≥ 1 cm, regular segmental hepatectomy, and radiofrequency ablation. All the patients signed written informed consent before surgery and were examined by multiphase dynamic computed tomography (CT) or magnetic resonance imaging (MRI) before the operation. A multidisciplinary team, including experienced oncology surgeons, radiologists, and ultrasound doctors, determined the patient’s eligibility for invasive treatment and the corresponding treatment plan. All treatments were discussed with the patients, and the patients were allowed to choose the treatment.
Inclusion criteria were as follows: 1) diagnosis of HCC based on the latest clinical guidelines at the time of treatment,4,9,30,31 the pathological diagnosis was made when the clinical diagnosis was not clear; 2) solitary nodular HCC with a maximum diameter of 3 cm or less on CT or MRI scan; 3) HCC discovered for the first time and evaluated by our team as resectable, which was defined as the complete removal of all tumors and the retention of enough liver portion to maintain liver function; 4) Child-Pugh class A or B, and Eastern Cooperative Oncology Group performance status of 0; and 5) more than 1 year follow-up after treatment.
Exclusion criteria were as follows: 1) unclear diagnosis or the presence of any evidence of other tumor lesions rather than confirmed HCC nodules; 2) any preoperative or simultaneous treatment, such as preoperative transcatheter arterial chemoembolization, alcohol injection, or systemic therapy; 3) complicated with other cancers; 4) tumor with macrovascular invasion or distant metastasis; 5) incomplete RFA; 6) incomplete clinical data; and 7) liver transplantation.
All the patients received adequate preoperative preparation and examination before the operation. Blood samples were collected within three days before the operation. All data including age, sex, tumor size, tumor location, preoperative AFP, CEA, and CA19-9 levels, hepatitis, hepatitis B virus e antigen (HBeAg) status, platelet count, prothrombin time, liver cirrhosis, Child-Pugh classification, BCLC stage, TNM eighth stage, albumin–bilirubin (ALBI) grade, and type of surgery were collected. All the patients diagnosed with hepatitis B or C received standard antiviral treatment during the perioperative period. The patients’ liver function reserve before the operation was evaluated using Child-Pugh classification and ALBI grade.32–34 All the researchers were blinded to clinical outcomes at the time of data collection.
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the ethics committee of Tianjin Medical University Cancer Institute & Hospital with the requirement for informed consent waived. And this study complied with the Good Clinical Practice guidelines and applicable local laws. Any patient data that could identify individual patients were anonymized and de-identified before analysis.
Assessment and Follow-Up
All the patients were followed up one month after the first treatment, once every three months for two years after the operation, and once every 4–6 months thereafter. Monitoring included blood routine, liver function, tumor biomarker levels, abdominal ultrasound, or dynamically enhanced CT or MRI. Local tumor recurrence was diagnosed when subsequent follow-up examination showed a new tumor growing along the edge of the ablation or resection area. Neoplasms in other hepatic segments were defined as intrahepatic recurrences. Metastases to other organs were defined as extrahepatic recurrence. All imaging tests were independently reviewed by two or more experienced radiologists. When tumor recurrences occurred during follow-up, second-line treatments, such as radiofrequency ablation, transcatheter arterial chemoembolization, resection, or sorafenib therapy, were performed in accordance with the recommendations of the multidisciplinary cancer committee depending on the patient’s liver function, general condition, and characteristics of tumor recurrence. Given that recurrence is the main cause of death in patients with HCC who undergo surgical treatment,35 recurrence-free survival (RFS) was analyzed to compare long-term outcomes in those cases. RFS was defined as the interval between the successful surgery date and the recurrence or death date. Patients who chose not to attend hospital follow-up underwent a telephone follow-up survey. Long-term follow-up was defined as a follow-up that lasted five years or more from treatment to the last follow-up.
TMS
X-tile software was used to determine optimal cutoff values based on RFS for preoperative serum AFP, CEA, and CA19-9. The patients were then divided into a low-level group (score = 0) or a high-level group (score = 1). The TMS of each patient was defined as the sum of his/her AFP, CEA, and CA19-9 scores.
Statistical Analyses
Continuous variables were expressed as mean ± standard deviation (SD) or median values with interquartile range values (IQRs). The normality hypothesis was used for evaluation. If the normality hypothesis and test of homogeneity of variances were satisfied, then a one-way analysis of variance was used to analyze the continuous variables. Otherwise, the Wilcoxon rank-sum test was employed. All categorical variables were described as numbers and percentages. Intergroup comparisons of categorical variables were analyzed by the chi-square test or Fisher exact test. The RFS rate was estimated by Kaplan–Meier (K–M) analysis and survival curves were statistically compared by Log rank test. A univariate Cox proportional hazards model evaluated RFS-associated variables. Variables with p<0.05 or clinically relevant variables were incorporated into multivariate analyses to identify significant factors that could affect the RFS rate. All statistical analyses were conducted using SPSS version 26.0 (SPSS, Chicago, IL, USA) and R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria). P-value < 0.05 indicated statistical significance.
Results
Demographics
Data of 409 patients with a single tumor with a maximum diameter ≤ 3 cm who received initial diagnosis and treatment in this hospital from January 2010 to December 2014 were retrospectively collected. The average age was 57.12 years, and the patients consisted of 309 (75.6%) men and 100 (24.4%) women. A total of 337 (82.4%) patients were under 65 years, and 72 (17.6%) patients were >65 years. Hepatitis infection and liver cirrhosis were detected in 346 (84.6%), and 333 (81.4%) patients, respectively, and 302 and 44 patients were infected with hepatitis B virus and hepatitis C virus, respectively. Before surgery, 92 (22.5%) patients were found to be HBeAg positive. The median tumor size was 2.3 cm, and 178 (43.5%) patients had tumors less than 2 cm. Tumor in the right lobe of the liver was found in 314 (76.8%) patients. A total of 125 (30.6%) patients accepted anatomical resection (AR), 103 (25.2%) patients received non-anatomical resection (NAR), and 181 (44.3%) patients took RFA. All the enrolled patients were classified as Chinese Liver Cancer stage Ia and R0 resection. Other clinical characteristics of 409 patients are shown in Table 1.
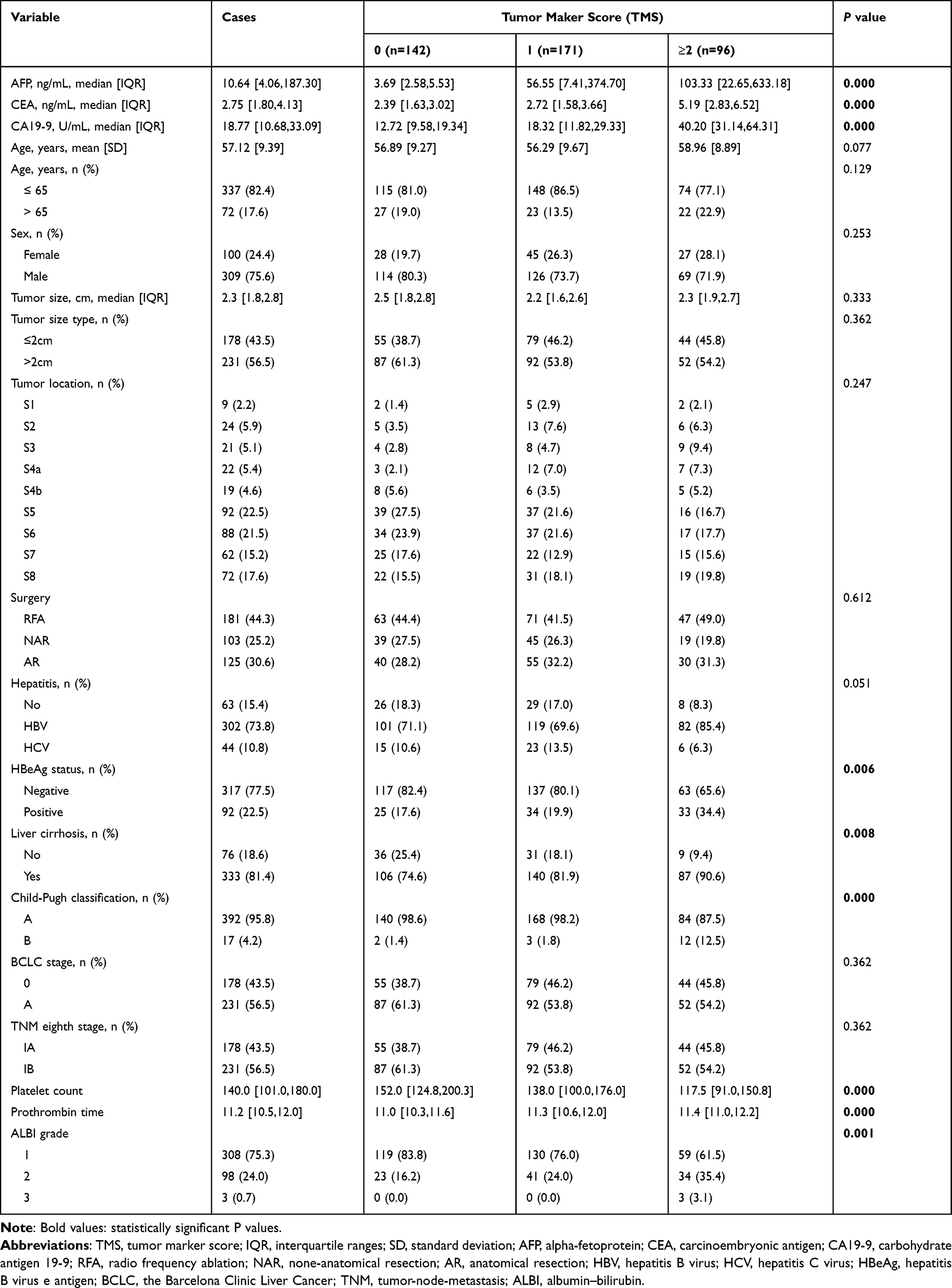 |
Table 1 Characteristics of 409 Enrolled Patients Grouped by TMS |
Tumor Marker Distribution
X-tile was used to determine the optimal cutoff values for the tumor markers. The cutoff values of preoperative AFP, CEA, and CA19-9 were 14.90, 5.30, and 27.70, respectively (the normal upper limits of AFP, CEA, and CA19-9 in our hospital are 7.00 ng/mL, 5.00 ng/mL, and 27.00 U/mL, respectively). The patients with low levels of AFP (≤ 14.90 ng/mL), CEA (≤ 5.30 ng/mL), and CA19-9 (≤ 27.70 U/mL) were given a score of 0. Those with high levels of AFP (> 14.90 ng/mL), CEA (>5.30 ng/mL), and CA19-9 (> 27.70 U/mL) were given a score of 1. After their scores were summed up, all the patients were stratified into TMS scores of 0, 1, 2, or 3 points. Since there were no significant survival differences between TMS2 and TMS3 in this study (p = 0.790, Log rank test), these two strata were merged into one group collectively called TMS2 (Figures 2D and E). According to the above definition, 142 patients were classified as TMS0, 171 as TMS1, and 96 as TMS2. The median values of AFP, CEA, and CA19-9 increased with the TMS. The median values of AFP were 3.69 ng/mL in TMS 0, 56.55 ng/mL in TMS1, and 103.33 ng/mL in TMS2 (p = 0.000). The median values of CEA were 2.39 ng/mL in TMS0, 2.72 ng/mL in TMS1, and 5.19 ng/mL in TMS2 (p = 0.000). The median values of CA19-9 were 12.72 U/mL in TMS0, 18.32 U/mL in TMS1, and 40.20 U/mL in TMS2 (p = 0.000).
 |
Figure 2 K–M curves of recurrence-free survival after surgery for single small HCC. K–M curves showing RFS of patients grouped by optimal cutoff values of AFP (A), CEA (B), CA19-9 (C) and TMS (D and E (TMS2 and TMS3 were collectively called TMS2 in (E)). Abbreviations: PFS, progression-free survival; K-M, Kaplan–Meier. |
Long-Term Outcomes According to the TMS
The median RFS (mRFS) of the entire cohort was 52 months (IQR 40.8–63.2 months), during which 188 (46.0%) patients relapsed. No recurrence was found in 221 (54.0%) patients at the end of the follow-up, and the 1-, 3-, and 5-year RFS rates were 83.8%, 60.9%, and 45.7%, respectively.
Effect of TMS on RFS
The mRFS rate of TMS0, TMS1, TMS2 was 89%, 52%, and 23%, respectively. The 1-year RFS rate was 94.4% for TMS0, 93.0% for TMS1, and 68.8% for TMS2. The 3-year RFS rate was 79.9% for TMS0, 60.1% for TMS1, and 36.0% for TMS2. The 5-year RFS rate was 68.0% for TMS0, 45.5% for TMS1, and 19.0% for TMS2 (Supplementary Table 1). K–M analysis showed that TMS could divide the patients into groups with significantly different prognoses, and the patients with high AFP, CEA, and CA19-9 scores had worse RFS than those with low scores (Figures 2A–E).
Identification of Prognostic Factors
A Cox proportional hazards model based on RFS was used to estimate the hazard ratio (HR) and its 95% confidence interval (95% CI) (Table 2). Univariate analysis indicated that age, HBeAg positive, platelet count, prothrombin time, ALBI grade, Child–Pugh classification, and TMS were statistically significant. Multivariate analysis revealed that age (HR:1.018, 95% CI: (1.001,1.035), (P=0.041), HBeAg positive (HR: 1.419, 95% CI: (1.015,1.985), P=0.041), and TMS (HR: TMS1=2.015, 95% CI: (1.358,2.990), P = 0.001; TMS2=3.459, 95% CI: (2.276,5.258), P=0.000) were significantly different.
 |
Table 2 Univariate and Multivariate Analyses of Prognostic Factors Based on RFS |
Subgroup Analysis to Examine the Impact of TMS on RFS
The potential confounders for different subgroups are displayed in Figure 3. The HR value increased with the TMS, and a statistically significant difference was found between TMS0 and TMS2. Statistical significance was also found between TMS0 and TMS1 in some subgroups. An example is hepatitis status: for the patients without hepatitis, the risk of recurrence was 2.486 times higher in the TMS1 group than in the TMS0 (HR: 2.486; 95% CI: 0.961 to 6.426; P=0.060) and 5.493 times higher in the TMS2 group than in the TMS0 (HR: 5.493; 95% CI: 1.752 to 17.221; P=0.003). For the patients with hepatitis, the risk of recurrence was 2.001 times higher in the TMS1 group than in the TMS0 (HR: 2.001; 95% CI: 1.300 to 3.079; P=0.002) and 4.010 times higher in the TMS2 group than in the TMS0 (HR: 4.010; 95% CI: 2.616 to 6.147; P=0.000).
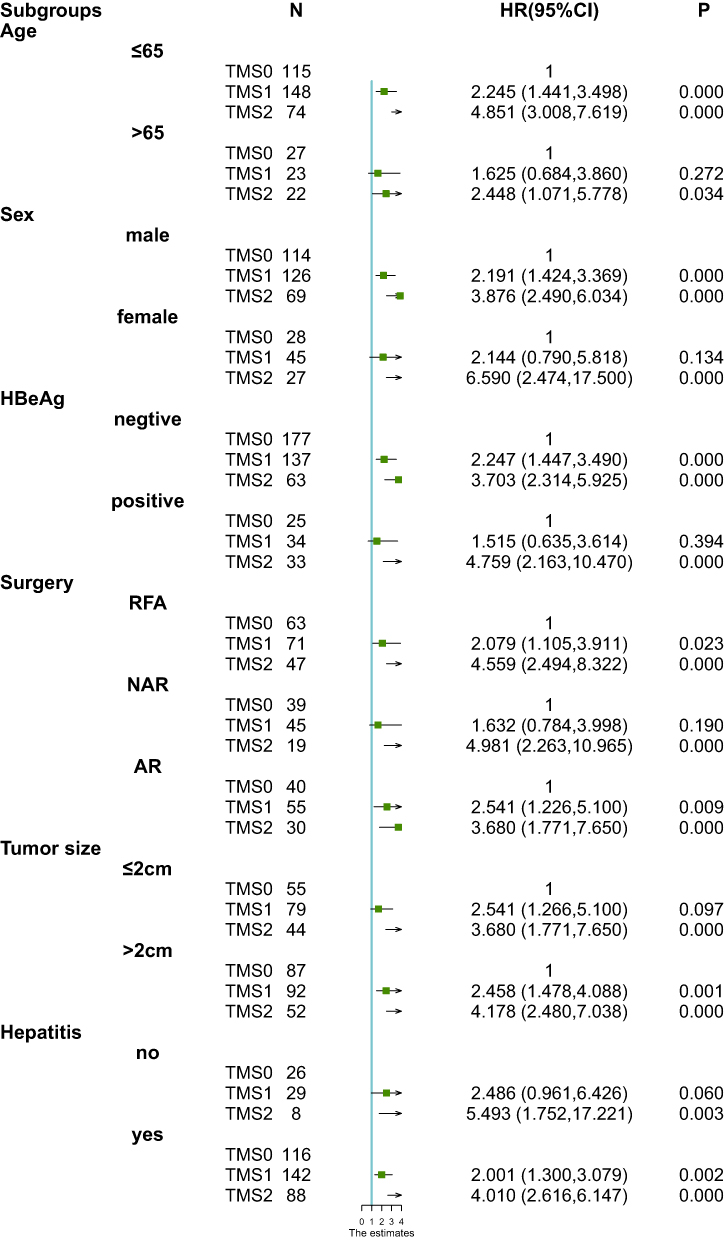 |
Figure 3 HR of univariable Cox regression analysis for postoperative recurrence comparing TMS in different subgroups of some group. Abbreviation: HR; hazard ratios. |
Comparison of TMS and Other Predictive Models
The 1-, 3-, 5-year area under curve (AUC) values of TMS were 0.698 (95% CI: 0.634 to 0.762), 0.662 (95% CI: 0.605 to 0.718), and 0.673 (95% CI: 0.596 to 0.749), respectively (Figure 4). The following models, including TMS, AFP, CEA, CA19-9, TNM, Child-Pugh classification, and ALBI grade, were developed to compare a single small HCC prognosis (Figure 5). As shown in the time-dependent ROC (td-ROC), the AUC of TMS was higher than that of other models such as AFP, CEA, CA19-9, TNM, Child-Pugh classification, and ALBI grade, indicating that TMS was the best among these predictive models.
 |
Figure 4 Receiver operating characteristic curve of TMS at 1-, 3-, and 5-year recurrence-free survival. |
 |
Figure 5 Time-dependent ROC curves of the seven models for predicting recurrence-free survival. Abbreviations: TMS, tumor marker score; AFP, alpha-fetoprotein; CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19-9; ALBI, albumin–bilirubin; TNM, tumor-node-metastasis. |
Discussion
In this work, we developed a simple, easily applicable TMS based on the serum indices AFP, CEA and CA19-9 and can stratify patients with single small HCC who underwent surgery into groups with statistically different prognoses. Compared with patients with an AFP of more than 14.9 ng/mL, a CEA of more than 5.30 ng/mL, and a CA19-9 of more than 27.70 U/mL, the patients who met none of these criteria had a beneficial survival, and the patients who met only one criterion still had a protective outcome. The predictive power of TMS was also evident in all the subgroups considered in this work. To our knowledge, this study is the first to present the prognostic value of TMS in patients with a single small HCC after surgery, suggesting its essential role in recurrence assessment in these patients.
As the “gold standard” biomarker of HCC, AFP has been widely used in treatment monitoring, therapeutic decision making, and prognosis predicting.36,37 A high level of AFP is closely associated with postoperative recurrence and poor prognosis.19 However, no standard cutoff value has been set for dividing patients into high or low recurrence groups. Although several studies have reported the ideal cutoff value of CEA or CA 19–9 for predicting HCC prognosis,21,25,38 their optimal cutoff values have also not been established. Most studies chose the clinical standard upper limit of the tumor markers as their cutoff value,21,22,25,38 but statistical evidence does not support this strategy. According to X-tile statistical analysis, our novel cutoff values are 14.90 ng/mL for AFP, 5.30 ng/mL for CEA, and 27.70 U/mL for CA19-9 are close to the upper limits of the current clinical norms of our hospital.
This study also clarified the prognostic significance of TMS for patients with a single small HCC. TMS can distinguish poor prognosis from good prognosis. Patients with high TMS were found to have a significantly poor prognosis than those with low TMS. Tumor differentiation has been used to predict the prognosis of malignant tumors; however, recent studies revealed the lack of significant prognosis effect of tumor differentiation.39,40 Several serum markers, such as prognostic nutritional index,41 rapid turnover proteins (RTPs),42 and some inflammation indicators, like systemic immune inflammation index (SII),43 neutrophil-to-lymphocyte ratio (NLR),44 lymphocyte-to-monocyte ratio (LMR),45 and platelet-to-lymphocyte ratio (PLR) were found to contribute to tumor progression.46 However, only a few studies compared AUC with other prognostic systems, such as TNM stage and Child-Pugh classification. The subgroups analysis in our study provided additional details for TMS and the variable groups.
Univariate Cox proportional hazards regression analysis showed that surgery type was not a significant prognostic factor in patients with a single small HCC who received RFA, NAR, or AR as initial treatment. K–M analysis also showed no statistical significance among the different surgical groups (P=0.74) (Supplementary Figure 1). However, several retrospective studies have reported an improvement in the long-term survival rate of AR compared with NAR.47–51 The NAR group usually includes patients with severe liver disease; hence, the expected survival time is low, affecting the outcome. Among the six propensity score analyses that have been published, three have reported better results after AR than those with NAR.10,52,53 The other three have reported no difference among the groups.54–56 According to a Phase III prospective, randomized, controlled study presented at the annual meeting of the 2021 American Society of Clinical Oncology, no statistical difference in RFS can be found between patients with surgical resection and those with RFA. Subgroup analysis showed a significant statistical difference in TMS1 vs TMS0 and TMS2 vs TMS0 in the RFA and AR subgroups and TMS2 vs TMS0 in the NAR subgroup. Although no statistical significance was found in TMS1 vs TMS0 in the NAR subgroup, the HR value increased with the TMS in all subgroups, indicating that TMS plays an instructive role in distinguishing good prognosis from poor prognosis.
A high TMS may indicate a high recurrence incidence in patients with a single small HCC who undergo RFA, AR, or NAR. In addition to shortening the time of regular follow-up, adjuvant targeting therapy with or without immunotherapy should be considered in these patients with a high possibility of recurrence after surgery. Further research is needed to provide additional details.
Compared with the other models, the TMS had better AUC performance. Although the 1-, 3-, and 5-year AUC values of TMS were close to 0.70, TMS may better predict the prognosis of a single small HCC than TNM stage, Child-Pugh classification, ALBI grade, and single tumor marker.
Several limitations exist in our research. First, given its retrospective nature, this study was inevitably exposed to selection bias. Accordingly, the cohort is heterogeneous in baseline values, such as platelet count, ALBI grade, and liver cirrhosis. Second, this research is a single-centre study. A large-scale multiple-centre study is necessary to verify our conclusions. Moreover, only a small number of patients in the RFA group were confirmed by biopsy, thus possibly affecting the outcome of treatment. Finally, though we pointed out that TMS could accurately predict the recurrence of a single small HCC after surgery, we failed to make internal and external validations. Despite these limitations, we believe this study provides valuable insights into the current trend of predicting the prognosis of patients with a single small HCC.
In conclusion, we developed a TMS combining AFP, CEA, and CA19-9 that can accurately predict recurrence in patients with a single small HCC undergoing RFA, AR, or NAR. The results contribute to the decision-making in daily clinical practice. The TMS is based on three ubiquitously available laboratory values, making it objective and widely applicable. However, a large-scale prospective clinical study is warranted to verify our conclusions.
Funding
This work is supported by the grant from the National Natural Science Foundation of China (82173317).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
3. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;362(9822):1245–1255. doi:10.1016/S0140-6736(11)61347-0
4. Bruix J, Sherman M; American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
5. Kudo M. The 2008 Okuda lecture: management of hepatocellular carcinoma: from surveillance to molecular targeted therapy. J Gastroenterol Hepatol. 2010;25(3):439–452. doi:10.1111/j.1440-1746.2009.06207.x
6. Yamamoto J, Okada S, Shimada K, et al. Treatment strategy for small hepatocellular carcinoma: comparison of long-term results after percutaneous ethanol injection therapy and surgical resection. Hepatology. 2001;34(4):707–713. doi:10.1053/jhep.2001.27950
7. Jiang Y, Sun A, Zhao Y, et al. Proteomics identifies new therapeutic targets of early-stage hepatocellular carcinoma. Nature. 2019;567(7747):257–261. doi:10.1038/s41586-019-0987-8
8. Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150(4):835–853. doi:10.1053/j.gastro.2015.12.041
9. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
10. Shindoh J, Makuuchi M, Matsuyama Y, et al. Complete removal of the tumor-bearing portal territory decreases local tumor recurrence and improves disease-specific survival of patients with hepatocellular carcinoma. J Hepatol. 2016;64(3):594–600. doi:10.1016/j.jhep.2015.10.015
11. Poon RT, Fan ST, Lo CM, Liu CL, Wong J. Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg. 2002;235(3):373–382. doi:10.1097/00000658-200203000-00009
12. Qin C, Gao Y, Li J, Huang C, He S. Predictive effects of preoperative serum CA125 and AFP levels on post-hepatectomy survival in patients with hepatitis B-related hepatocellular carcinoma. Oncol Lett. 2021;21(6):487. doi:10.3892/ol.2021.12748
13. Galle PR, Foerster F, Kudo M, et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. 2019;39(12):2214–2229. doi:10.1111/liv.14223
14. Sachan A, Saluja SS, Nekarakanti PK, et al. Raised CA19-9 and CEA have prognostic relevance in gallbladder carcinoma. BMC Cancer. 2020;20(1):826. doi:10.1186/s12885-020-07334-x
15. Kim M, Kim H, Han Y, et al. Prognostic Value of Carcinoembryonic Antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9) in gallbladder cancer; 65 IU/mL of CA 19-9 is the new cut-off value for prognosis. Cancers. 2021;13(5):1089.
16. Edoo MIA, Chutturghoon VK, Wusu-Ansah GK, et al. Serum biomarkers AFP, CEA and CA19-9 combined detection for early diagnosis of hepatocellular carcinoma. Iran J Public Health. 2019;48(2):314–322.
17. Wang YF, Feng FL, Zhao XH, et al. Combined detection tumor markers for diagnosis and prognosis of gallbladder cancer. World J Gastroenterol. 2014;20(14):4085–4092. doi:10.3748/wjg.v20.i14.4085
18. Zheng Y, Zhu M, Li M. Effects of alpha-fetoprotein on the occurrence and progression of hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(10):2439–2446. doi:10.1007/s00432-020-03331-6
19. Bai DS, Zhang C, Chen P, Jin SJ, Jiang GQ. The prognostic correlation of AFP level at diagnosis with pathological grade, progression, and survival of patients with hepatocellular carcinoma. Sci Rep. 2017;7(1):12870. doi:10.1038/s41598-017-12834-1
20. Yang W, Luo Y, Hu S, Li Y, Liu Q. Value of combined detection of serum carcino-embryonic antigen, carbohydrate antigen 19-9 and cyclooxygenase-2 in the diagnosis of colorectal cancer. Oncol Lett. 2018;16(2):1551–1556. doi:10.3892/ol.2018.8792
21. Yoshikawa M, Morine Y, Ikemoto T, et al. Elevated preoperative serum CEA level is associated with poor prognosis in patients with hepatocellular carcinoma through the epithelial-mesenchymal transition. Anticancer Res. 2017;37(3):1169–1175.
22. Qi F, Zhou A, Yan L, et al. The diagnostic value of PIVKA-II, AFP, AFP-L3, CEA, and their combinations in primary and metastatic hepatocellular carcinoma. J Clin Lab Anal. 2020;34(5):e23158. doi:10.1002/jcla.23158
23. Hou GM, Liu HL, Wu H, Zeng Y. Prediction of prognosis for cHCC-CC patients after surgery: comparison of tumor marker score based on AFP, CEA, CA19-9, and other clinical stages. Ann Surg Oncol. 2021;28(12):7647–7660. doi:10.1245/s10434-021-09949-1
24. Singh S, Tang SJ, Sreenarasimhaiah J, Lara LF, Siddiqui A. The clinical utility and limitations of serum carbohydrate antigen (CA19-9) as a diagnostic tool for pancreatic cancer and cholangiocarcinoma. Dig Dis Sci. 2011;56(8):2491–2496. doi:10.1007/s10620-011-1709-8
25. Zhang W, Wang Y, Dong X, et al. Elevated serum CA19-9 indicates severe liver inflammation and worse survival after curative resection in hepatitis B-related hepatocellular carcinoma. Biosci Trends. 2022;15(6):397–405. doi:10.5582/bst.2021.01517
26. Liu W, Li X, Zheng W, Yao R, Zheng J. Preoperative evaluation of the degree of liver fibrosis based on matter-element analysis using serological indicators in patients with hepatocellular carcinoma. Biosci Trends. 2019;13(1):70–76. doi:10.5582/bst.2018.01311
27. Tsuji M, Kashihara T, Terada N, Mori H. An immunohistochemical study of hepatic atypical adenomatous hyperplasia, hepatocellular carcinoma, and cholangiocarcinoma with alpha-fetoprotein, carcinoembryonic antigen, CA19-9, epithelial membrane antigen, and cytokeratins 18 and 19. Pathol Int. 1999;49(4):310–317. doi:10.1046/j.1440-1827.1999.00865.x
28. Wakizaka K, Yokoo H, Kamiyama T, et al. Clinical and pathological features of combined hepatocellular-cholangiocarcinoma compared with other liver cancers. J Gastroenterol Hepatol. 2019;34(6):1074–1080. doi:10.1111/jgh.14547
29. Kim KH, Lee SG, Park EH, et al. Surgical treatments and prognoses of patients with combined hepatocellular carcinoma and cholangiocarcinoma. Ann Surg Oncol. 2009;16(3):623–629. doi:10.1245/s10434-008-0278-3
30. Yang JD, Heimbach JK. New advances in the diagnosis and management of hepatocellular carcinoma. BMJ. 2020;371:m3544. doi:10.1136/bmj.m3544
31. Bruix J, Sherman M; Practice Guidelines Committee AAftSoLD. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–1236. doi:10.1002/hep.20933
32. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-The ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
33. Hiraoka A, Kumada T, Tsuji K, et al. Validation of modified ALBI grade for more detailed assessment of hepatic function in hepatocellular carcinoma patients: a multicenter analysis. Liver Cancer. 2019;8(2):121–129.
34. Hiraoka A, Kumada T, Michitaka K, et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J Gastroenterol Hepatol. 2016;31(5):1031–1036. doi:10.1111/jgh.13250
35. Wang XH, Long LH, Cui Y, et al. MRI-based radiomics model for preoperative prediction of 5-year survival in patients with hepatocellular carcinoma. Br J Cancer. 2020;122(7):978–985. doi:10.1038/s41416-019-0706-0
36. Chen T, Dai X, Dai J, et al. AFP promotes HCC progression by suppressing the HuR-mediated Fas/FADD apoptotic pathway. Cell Death Dis. 2020;11(10):822. doi:10.1038/s41419-020-03030-7
37. Sauzay C, Petit A, Bourgeois AM, et al. Alpha-foetoprotein (AFP): a multi-purpose marker in hepatocellular carcinoma. Clin Chim Acta. 2016;463:39–44. doi:10.1016/j.cca.2016.10.006
38. Hsu CC, Goyal A, Iuga A, et al. Elevated CA19-9 is associated with increased mortality in a prospective cohort of hepatocellular carcinoma Patients. Clin Transl Gastroenterol. 2015;6(2):e74. doi:10.1038/ctg.2014.22
39. Zhao H, Hua Y, Lu Z, et al. Prognostic value and preoperative predictors of microvascular invasion in solitary hepatocellular carcinoma ≤ 5 cm without macrovascular invasion. Oncotarget. 2017;8(37):61203–61214. doi:10.18632/oncotarget.18049
40. Oishi K, Itamoto T, Amano H, et al. Clinicopathologic features of poorly differentiated hepatocellular carcinoma. J Surg Oncol. 2007;95(4):311–316. doi:10.1002/jso.20661
41. Pan J, Chen S, Tian G, Jiang T. Preoperative albumin-bilirubin grade with prognostic nutritional index predicts the outcome of patients with early-stage hepatocellular carcinoma after percutaneous radiofrequency ablation. Front Med. 2020;7:584871. doi:10.3389/fmed.2020.584871
42. Yanagaki M, Haruki K, Yasuda J, et al. The significance of the rapid turnover protein score as a predictor of the long-term outcomes in hepatocellular carcinoma after hepatic resection. Ann Surg Oncol. 2021;28(13):8130–8139. doi:10.1245/s10434-021-10704-9
43. Yang J, Bao Y, Chen W, Duan Y, Sun D. Nomogram based on systemic immune inflammation index and prognostic nutrition index predicts recurrence of hepatocellular carcinoma after surgery. Front Oncol. 2020;10:551668. doi:10.3389/fonc.2020.551668
44. Shen Y, Wang H, Li W, Chen J. Prognostic significance of the CRP/Alb and neutrophil to lymphocyte ratios in hepatocellular carcinoma patients undergoing TACE and RFA. J Clin Lab Anal. 2019;33(9):e22999. doi:10.1002/jcla.22999
45. Yang YT, Jiang JH, Yang HJ, Wu ZJ, Xiao ZM, Xiang BD. The lymphocyte-to-monocyte ratio is a superior predictor of overall survival compared to established biomarkers in HCC patients undergoing liver resection. Sci Rep. 2018;8(1):2535. doi:10.1038/s41598-018-20199-2
46. He C, Zhang Y, Cai Z, Lin X. The prognostic and predictive value of the combination of the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio in patients with hepatocellular carcinoma who receive transarterial chemoembolization therapy. Cancer Manag Res. 2019;11:1391–1400. doi:10.2147/CMAR.S190545
47. Minagawa M, Mise Y, Omichi K, et al. Anatomic resection for hepatocellular carcinoma: prognostic impact assessed from recurrence treatment. Ann Surg Oncol. 2022;29(2):913–921. doi:10.1245/s10434-021-10380-9
48. Tanaka K, Shimada H, Matsumoto C, et al. Anatomic versus limited nonanatomic resection for solitary hepatocellular carcinoma. Surgery. 2008;143(5):607–615. doi:10.1016/j.surg.2008.01.006
49. Cucchetti A, Cescon M, Ercolani G, Bigonzi E, Torzilli G, Pinna AD. A comprehensive meta-regression analysis on outcome of anatomic resection versus nonanatomic resection for hepatocellular carcinoma. Ann Surg Oncol. 2012;19(12):3697–3705. doi:10.1245/s10434-012-2450-z
50. Eguchi S, Kanematsu T, Arii S, et al. Comparison of the outcomes between an anatomical subsegmentectomy and a non-anatomical minor hepatectomy for single hepatocellular carcinomas based on a Japanese nationwide survey. Surgery. 2008;143(4):469–475. doi:10.1016/j.surg.2007.12.003
51. Wakai T, Shirai Y, Sakata J, et al. Anatomic resection independently improves long-term survival in patients with T1-T2 hepatocellular carcinoma. Ann Surg Oncol. 2007;14(4):1356–1365. doi:10.1245/s10434-006-9318-z
52. Ishii M, Mizuguchi T, Kawamoto M, et al. Propensity score analysis demonstrated the prognostic advantage of anatomical liver resection in hepatocellular carcinoma. World J Gastroenterol. 2014;20(12):3335–3342. doi:10.3748/wjg.v20.i12.3335
53. Cucchetti A, Qiao GL, Cescon M, et al. Anatomic versus nonanatomic resection in cirrhotic patients with early hepatocellular carcinoma. Surgery. 2014;155(3):512–521. doi:10.1016/j.surg.2013.10.009
54. Hirokawa F, Kubo S, Nagano H, et al. Do patients with small solitary hepatocellular carcinomas without macroscopically vascular invasion require anatomic resection? Propensity score analysis. Surgery. 2015;157(1):27–36. doi:10.1016/j.surg.2014.06.080
55. Okamura Y, Ito T, Sugiura T, Mori K, Uesaka K. Anatomic versus nonanatomic hepatectomy for a solitary hepatocellular carcinoma: a case-controlled study with propensity score matching. J Gastrointest Surg. 2014;18(11):1994–2002. doi:10.1007/s11605-014-2646-6
56. Marubashi S, Gotoh K, Akita H, et al. Anatomical versus non-anatomical resection for hepatocellular carcinoma. Br J Surg. 2015;102(7):776–784. doi:10.1002/bjs.9815
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.