Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Clinical Complete Response After Conversion Therapy for Unresectable Hepatocellular Carcinoma: Is Salvage Hepatectomy Necessary?
Authors Wu JY ![]() , Wu JY, Liu DY, Li H, Zhuang SW, Li B, Zhou JY
, Wu JY, Liu DY, Li H, Zhuang SW, Li B, Zhou JY ![]() , Huang JY, Zhang ZB, Li SQ, Yan ML
, Huang JY, Zhang ZB, Li SQ, Yan ML ![]() , Wang YD
, Wang YD
Received 27 September 2023
Accepted for publication 23 November 2023
Published 5 December 2023 Volume 2023:10 Pages 2161—2171
DOI https://doi.org/10.2147/JHC.S442341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Jörg Trojan
Jia-Yi Wu,1,2,* Jun-Yi Wu,1,2,* De-Yi Liu,1,* Han Li,1,* Shao-Wu Zhuang,3 Bin Li,4 Jian-Yin Zhou,5 Jing-Yao Huang,6 Zhi-Bo Zhang,7 Shu-Qun Li,8 Mao-Lin Yan,1,2 Yao-Dong Wang1,2
1Shengli Clinical Medical College of Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 2Department of Hepatobiliary Pancreatic Surgery, Fujian Provincial Hospital, Fuzhou, Fujian Province, People’s Republic of China; 3Department of Interventional Radiology, Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, Fujian Province, People’s Republic of China; 4Department of Hepato-Biliary-Pancreatic and Vascular Surgery, First Affiliated Hospital of Xiamen University, Xiamen, Fujian Province, People’s Republic of China; 5Department of Hepatobiliary Surgery, Zhongshan Hospital of Xiamen University, Xiamen, Fujian Province, People’s Republic of China; 6Department of Interventional Radiology, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, People’s Republic of China; 7Department of Hepatopancreatobiliary Surgery, First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 8Department of Hepatobiliary Pancreatic Surgery, Affiliated Hospital of Guilin Medical University, Guilin, Guangxi Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mao-Lin Yan; Yao-Dong Wang, The Shengli Clinical Medical College of Fujian Medical University, Department of Hepatobiliary Pancreatic Surgery, Fujian Provincial Hospital, Dongjie Road 134, Fuzhou, Fujian Province, 350001, People’s Republic of China, Tel +86 591-88217140 ; +86 591-88217130, Fax +86 591-87557768, Email [email protected]; [email protected]
Background: This study aimed to determine whether salvage hepatectomy offers prognostic advantages for unresectable hepatocellular carcinoma (uHCC) patients with clinical complete response (cCR) after conversion therapy.
Methods: A total of 74 consecutive uHCC patients with cCR after conversion therapy at seven major cancer centers in China between October 2018 and December 2021 were included. One-to-one propensity score matching (PSM) was performed to minimize the influence of potential confounders. Disease-free survival (DFS) and overall survival (OS) rates were compared between the surgical group and the non-surgical group.
Results: Before PSM, 45 patients received salvage hepatectomy, and 29 patients received nonsurgical treatment. The 1-, 2-, and 3-year DFS rates were 77.8%, 61.5%, and 61.5% in the surgical group and 81.2%, 60.9%, and 60.9% in the non-surgical group, respectively. The 1-, 2-, and 3-year OS rates were 92.9%, 92.9%, and 69.7% in the surgical group and 100%, 70%, and 70% in the non-surgical group, respectively. There were no statistical differences in DFS and OS between groups [hazard ratio (HR)=0.715, 95% confidence interval (CI): 0.250– 2.043, p=0.531; HR=0.980, 95% CI: 0.177– 5.418, p=0.982, respectively]. After PSM, 26 pairs of patents were selected; there remained no significant differences in DFS and OS between these two groups (HR=1.547, 95% CI: 0.512– 4.669, p=0.439; HR=1.024, 95% CI: 0.168– 6.242, p=0.979, respectively).
Conclusion: Through the study, it tend to show that salvage hepatectomy may be not essential for uHCC patients with cCR, especially for patients with a high risk of surgical complications. Prospective trials with long term follow-up are warranted to evaluate this treatment option.
Plain Language Summary: To date, there is limited evidence on the prognosis of the unresectable hepatocellular carcinoma (uHCC) patients with clinical complete response (cCR), and the necessity of salvage surgery remains controversial. In this study, they compare and evaluate therapeutic benefits of salvage hepatectomy and nonsurgical treatment in the management of uHCC patients with cCR after conversion therapy. Finally, a total of 74 consecutive uHCC patients with cCR after conversion therapy at seven major cancer centers in China were included. There were no statistically significant differences for disease-free survival and overall survival were observed before and after propensity score matching. They revealed that cCR after conversion therapy led to a good prognosis for patients with uHCC. Furthermore, nonsurgical treatment provided similar survival benefits to those of salvage hepatectomy, suggesting that salvage hepatectomy may be not essential for uHCC patients with cCR.
Keywords: conversion therapy, hepatocellular carcinoma, overall survival, disease-free survival, salvage surgery
Introduction
Hepatocellular carcinoma (HCC) is the second leading cause of cancer-related deaths worldwide.1 Surgical resection is one of the most important treatment options for patients with HCC, offering the possibility of cure and the prospect of long-term survival.2–5 However, most patients are diagnosed in advanced stages and often miss the opportunity for surgery, resulting in an expected median survival of only 6–8 months.1,5–7
Notably, with the development of systemic therapy, more patients with unresectable hepatocellular carcinoma (uHCC) are being given the opportunity of salvage surgery, and hence the possibility of long-term survival.8–10 Furthermore, some patients achieve complete response (CR) after conversion therapy.11–13 Current guidelines for the conversion therapy of uHCC recommend salvage surgery for patients with a preoperative assessment of conversion to resectable HCC.8 Salvage surgery can prevent the further progression of incompletely necrotic tumors and provide pathologic data from the resected tumor specimen, which can help to guide subsequent treatment plans. However, salvage surgery inevitably results in perioperative and long-term morbidity. To date, there is limited evidence on the prognosis of uHCC patients with clinical complete response (cCR), and the necessity of salvage surgery is controversial.
The present study aimed to compare the disease-free survival (DFS) and overall survival (OS) rates of uHCC patients with cCR, who received salvage hepatectomy and nonsurgical treatment. To the best of our knowledge, our study is the first to examine the therapeutic benefits of salvage hepatectomy in uHCC patients with cCR.
Patients and Methods
Patients
This retrospective study included consecutive patients with initially uHCC who received conversion therapy between October 2018 and December 2021 at seven major cancer centers in China: Fujian Provincial Hospital, Zhangzhou Affiliated Hospital of Fujian Medical University, First Affiliated Hospital of Xiamen University, Zhongshan Hospital of Xiamen University, Fujian Medical University Union Hospital, First Affiliated Hospital of Fujian Medical University, and Affiliated Hospital of Guilin Medical University. The clinical and pathological data related to this study, which were prospectively entered into a database, were analyzed retrospectively. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of each participating institution. All patients provided written informed consent for their data to be used for research purposes upon the final follow-up.
We excluded patients with extrahepatic metastases (EM), because salvage surgery for patients with EM is controversial and it is difficult to accurately determine whether extrahepatic metastasis achieves CR. Thus, the inclusion criteria were as follows: (1) Patients with a confirmed diagnosis of HCC and assessed as uHCC by multidisciplinary team (MDT); (2) Barcelona Clinic Liver Cancer (BCLC) stage B or C; (3) aged between 18 and 75 years; (4) Eastern Cooperative Oncology Group performance status (ECOG-PS) score 0 or 1; (5) Child-Pugh class A. The exclusion criteria were as follows: (1) patients with EM; (2) combined with other concurrent malignancies; (3) lack of important assessment indicators, such as imaging data or tumor markers; and (4) less than 3 months of follow-up.
Detailed radiological examinations (abdominal contrast-enhanced computed tomography and/or magnetic resonance imaging, physical examination, routine urine, and blood profiles, including complete blood count, blood biochemistry, liver and coagulation function tests, tumor markers [α-fetoprotein (AFP) and protein induced by vitamin K absence-II (PIVKA-II)], and detection of hepatitis B surface antigen (HBsAg) were collected prior to treatment administration.
Conversion Therapy Procedures
Conversion therapy regimens included targeted therapy, immunotherapy, and locoregional treatment. Targeted drugs included oral tyrosine kinase inhibitors [sorafenib (400 mg twice a day) and lenvatinib (8 mg for bodyweight <60 kg or 12 mg for bodyweight ≥60 kg once a day)], and intravenous bevacizumab (15 mg/kg once every 3 weeks). Immunotherapy drugs included intravenous atezolizumab (1200 mg), sintilimab (200 mg), tislelizumab (200 mg), carelizumab (200 mg), toripalimab (240 mg), and pembrolizumab (200 mg) once every 3 weeks. Super-selective transcatheter arterial chemoembolization (TACE) was performed under sterile conditions via the right femoral artery utilizing the Seldinger technique. After identifying the tumor feeding arteries, the radiologist mixed iodized oil and pirarubicin and slowly injected it through the microcatheter into the tumor feeding artery. Finally, gelatin sponge particles were injected until complete stasis of tumor arterial blood flow was achieved. The decision to proceed with TACE treatment or to repeat TACE depended on the opinion of the MDT.
Targeted and immunotherapy drugs were stopped for 3 days before and after TACE. All patients with HBV infection received oral antiviral treatment (entecavir or tenofovir).
Response and Toxicity Evaluation
Tumor assessments were performed every 4–8 weeks. cCR was defined as serum tumor marker normalization (including AFP <7 ng/mL and PIVKA-II <40 mAU/mL) and radiographic CR for ≥4 weeks. Tumor radiographic responses were independently evaluated by two senior diagnostic radiologists (more than 8 years of experience) from each center, according to the modified Response Evaluation Criteria in Solid Tumors.14 The time to cCR was calculated from the start of conversion therapy to the first time when the cCR criteria were met.
Treatment-related Adverse Effects (TRAEs) were retrieved from the hospital’s electronic medical records for analysis, using the Common Terminology Criteria for Adverse Events, Version 5.0.15
Surgical Procedure
When the patient met the criteria of cCR, salvage hepatectomy was determined by MDT discussion based on the difficulty, extent, and risk of the surgery, and patient’s request. Conversion to resectable HCC was defined as: (1) R0 resection with preservation of a sufficient remnant liver volume; (2) no tumor thrombus in the main trunk of portal vein and inferior vena cava; (3) the absence of EM; (4) no contraindications for hepatectomy; (5) Child-Pugh class A; (6) ECOG-PS score 0 or 1. Before salvage hepatectomy, tyrosine kinase inhibitors such as sorafenib and lenvatinib were stopped for 1 week, anti-PD-1 antibodies and TACE for 4 weeks, and bevacizumab for 6 weeks.
Salvage hepatectomy was performed after consultation and informed consent. The extent of the liver resection was classified into minor (<3 anatomical segments, including multiple non-anatomical resections) or major (≥3 anatomical segments) according to Couinaud’s classification.16 The Clavien–Dindo classification was used to grade postoperative complications, with Clavien–Dindo classification grade ≥IIIb being considered serious.17 Post-hepatectomy liver failure (PHLF) was defined and graded based on the International Study Group of Liver Surgery criteria.18 For pathological response evaluation, pathologic complete response (PCR) was defined as the complete absence of viable tumor cells in the resected tumor specimen and major pathological response (MPR) ≤10%.3
Follow-Up
Postoperative adjuvant systemic therapy was started 2–4 weeks after salvage hepatectomy, which is advised for 3–12 months depending on liver function, TRAEs, and patient performance. Non-surgical patients were advised for 3–12 months of systemic therapy after the diagnosis of cCR.
Patients were followed up every 4–8 weeks. Radiological examination (abdominal contrast-enhanced computed tomography and/or magnetic resonance imaging) data, AFP, PIVKA-II, physical examination, and laboratory profiles were collected at each appointment.
Development of tumor recurrence was classified into three categories including local tumor progression (LTP), intrahepatic distant recurrence (IDR), and EM. LTP was defined as the appearance of a hyper-enhanced nodular portion showing washout on the portal venous or delayed phase within 2 cm of the necrosis area;19 IDR was defined as the development of new HCC lesions away from the necrosis area.
The primary endpoint of this study was DFS. Secondary endpoints included OS and PCR rate in the surgical group. DFS was defined as the time interval from the date of diagnosis of cCR to tumor recurrence, death, or last follow-up. OS was defined as the time interval from the date of diagnosis of cCR to death or last follow-up. The endpoint of follow-up was January 1, 2023.
Statistical Analysis
Continuous data are presented as mean (standard deviation) or as median (range), as appropriate. Variables with a normal distribution were analyzed using an independent t-test. Categorical data are presented as number (percentage) and compared using the chi-square test or Fisher’s exact test. DFS and OS were calculated using Kaplan–Meier curves and compared using the Log rank test. Univariate analyses were performed to identify risk factors for DFS and OS. Since it was a retrospective study, selection bias could not be avoided, we used the propensity score matching (PSM) analysis to overcome the biases introduced by disequilibrium using the logistic regression model. The covariables used to build the propensity score were age, sex, ECOG-PS, HBsAg, pre-treatment platelet-albumin-bilirubin grade, pre-treatment alanine aminotransferase levels, pre-treatment aspartate aminotransferase levels, pre-treatment AFP levels, pre-treatment PIVKA-II levels, tumor number, maximum tumor size, and macrovascular invasion. PSM was performed using 1:1 matching between the nonsurgical treatment and salvage hepatectomy groups with nearest neighbor matching and a 0.2 caliper width.20 The MatchIt R package (version 3.0.2; the CRAN package repository, Vienna, Austria) was used in PSM analyses. Two-tailed P <0.05 were considered significant. All statistical analyses were performed using R version 3.5.0 software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics and Follow-Up
With a median time to cCR of 4.3 months (range, 1.9–17), 74 patients with cCR after conversion therapy were included in this study (Figure 1), including 20 patients with BCLC stage B and 54 patients with BCLC stage C. The mean age was 57.2±11.5 years. A total of 64 patients were males and 67 patients had hepatitis B virus. In terms of tumor markers, 36 patients (48.6%) had baseline AFP ≥400 ng/mL and 57 patients (77.0%) had baseline PIVKA-II ≥400 mAU/mL. Main reason for conversion therapy included bilobar tumor locations (n=18), tumors could not be radically resected (n=46), and anticipated insufficient future liver remnant volume (n=10). Baseline characteristics of patients who achieved cCR are shown in Table 1. Conversion therapy regimens included atezolizumab plus bevacizumab (n=2), lenvatinib plus anti-PD-1 antibodies (n=6), TACE plus atezolizumab and bevacizumab (n=1), TACE plus lenvatinib (n=7), TACE plus sorafenib (n=1), TACE plus sorafenib and anti-PD-1 antibodies (n=5), and TACE plus lenvatinib and anti-PD-1 antibodies (n=52) (Figure 1). Finally, 45 patients received salvage hepatectomy and 29 patients received nonsurgical treatment.
 |
Table 1 Baseline Demographic Characteristics of Patients Who Achieved Clinical Complete Response |
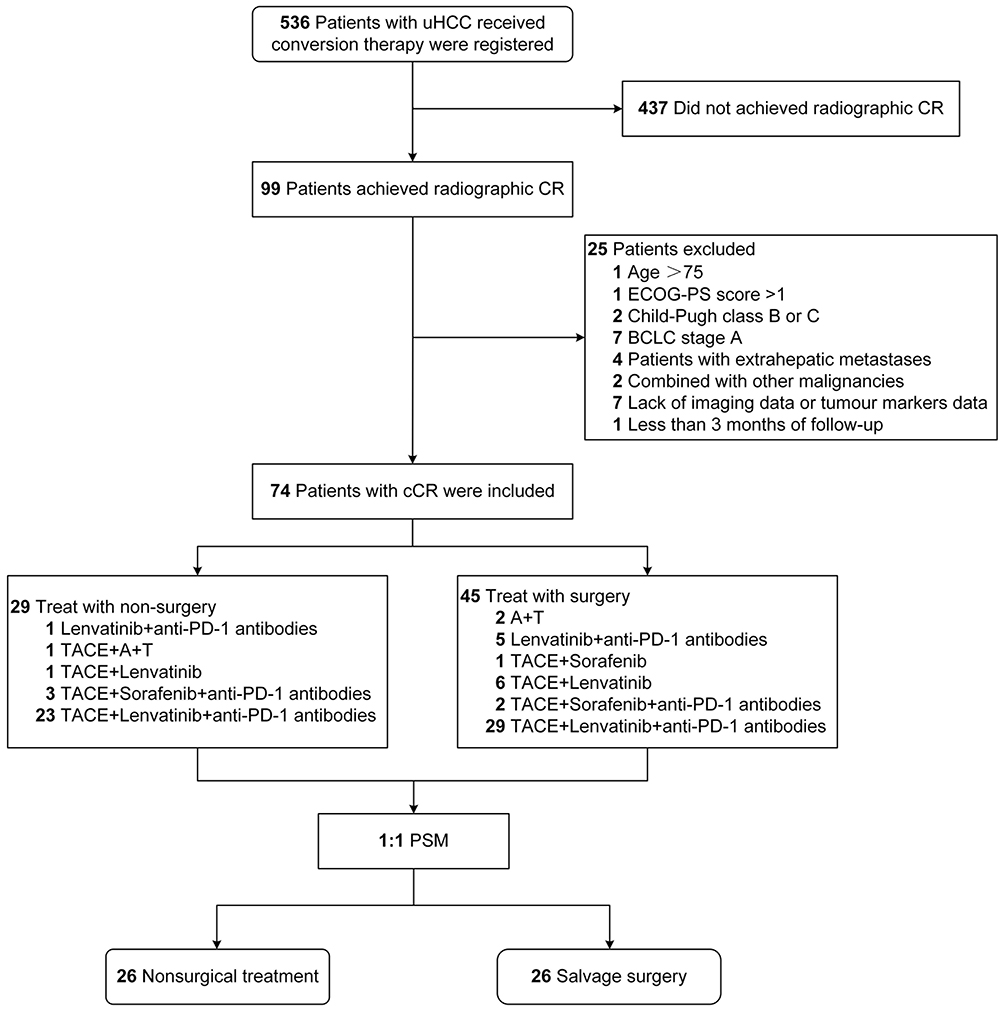 |
Figure 1 Flowchart of patient selection. Abbreviations: uHCC, unresectable hepatocellular carcinoma; CR, complete response; ECOG-PS, Eastern Cooperative Oncology Group performance status; BCLC, Barcelona Clinic Liver Cancer; cCR, clinical complete response; TACE, transarterial chemoembolization; A+T, atezolizumab plus bevacizumab; PSM, propensity score matching. |
With a median follow-up of 18.6 months (range 6–47.9), the median DFS and OS were not reached. The 1-, 2-, and 3-year DFS rates were 79.4%, 58.8%, and 58.8%, and the corresponding OS rates were 95.6%, 87.3%, and 72.7%, respectively (Figure S1). Tumor recurrence occurred in 17 patients, including LTP in 2 patients (11.8%), IDR in 14 patients (82.4%), and EM in 2 patients (11.8%) (Figure 2). A total of 6 patients (8.1%) died for different reasons, including 3 for tumor recurrence, 2 for portal hypertensive hemorrhage, and 1 for PHLF. In the nonsurgical group, 5 patients experienced IDR without LTP.
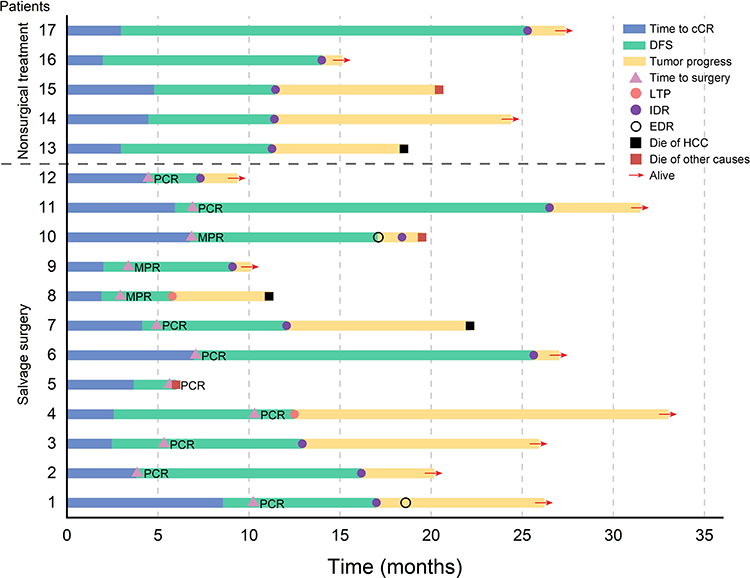 |
Figure 2 Swimmer’s plot of the clinical course and current status of 17 progressing patients. Abbreviations: cCR, clinical complete response; DFS, disease-free survival; LTP, Local tumor progression; IDR, intrahepatic distant recurrence; EDR, extrahepatic distant recurrence; HCC, hepatocellular carcinoma; PCR, pathologic complete response; MPR, major pathologic response. |
Salvage Hepatectomy and Perioperative Conditions
With a median interval between conversion therapy and salvage hepatectomy of 4.8 months (range, 2.3–14.2 months), 45 patients underwent salvage hepatectomy (Table S1). The median operative time was 183 minutes (range, 90–415 minutes), and median blood loss volume was 200 mL (range, 100–6000 mL). Thirteen patients (28.9%) underwent blood transfusion. PCR was achieved in 39 patients (86.7%). Three patients (6.7%) experienced serious post-hepatectomy complications, including PHLF (n=2) and pulmonary embolism (n=1). One patient died of PHLF 9 days after salvage hepatectomy, with a 90-day mortality rate of 2.2% (1/45). The prevalence of PHLF was 22.2% (17.8% for grade A, 2.2% for grade B, and 2.2% for grade C). The median postoperative hospital stay was 9 days (range, 6–38 days). During the follow-up period, 12 patients (26.7%) experienced tumor recurrence after surgery, including LTP in 2 patients (4.4%), IDR in 9 patients (20%), and EM in 2 patients (4.4%) (Figure 2).
Treatment-Related Adverse Effects
The incidence of TRAEs was 91.9% (68/74), of which grade I–III accounted for 83.8%, grade IV for 8.1%, and there were no grade V TRAEs. The most common (≥10%) TRAEs, in order of prevalence, were abnormal liver function, decreased appetite, fever, fatigue, hypertension, abdominal pain, hypothyroidism, hand-foot skin reaction, thrombocytopenia, skin rash, weight loss, diarrhea, proteinuria, and anemia (Table S2). Grade IV TRAEs occurred in 3 patients (10.3%) in the nonsurgical group and 3 patients (6.7%) in the surgical group. No statistical difference was observed between the two groups in terms of incidence of grade I–III or grade IV TRAEs (p=0.603 and p=0.897, respectively). All TRAEs were manageable during follow-up.
Comparison of DFS and OS
Before PSM, patients treated with salvage surgery had a better ECOG-PS than patients treated with non-surgical treatment (p=0.032, Table 1). The 1-,2-, and 3-year DFS rates were 77.8%, 61.5%, and 61.5% in the surgical group and 81.2%, 60.9%, and 60.9% in the non-surgical group, respectively. The 1-, 2-, and 3-year OS rates were 92.9%, 92.9%, and 69.7% in the surgical group and 100%, 70%, and 70% in the non-surgical group, respectively. There were no statistical differences in DFS and OS between these two groups (p=0.531 and p=0.982, respectively; Figure 3A and B).
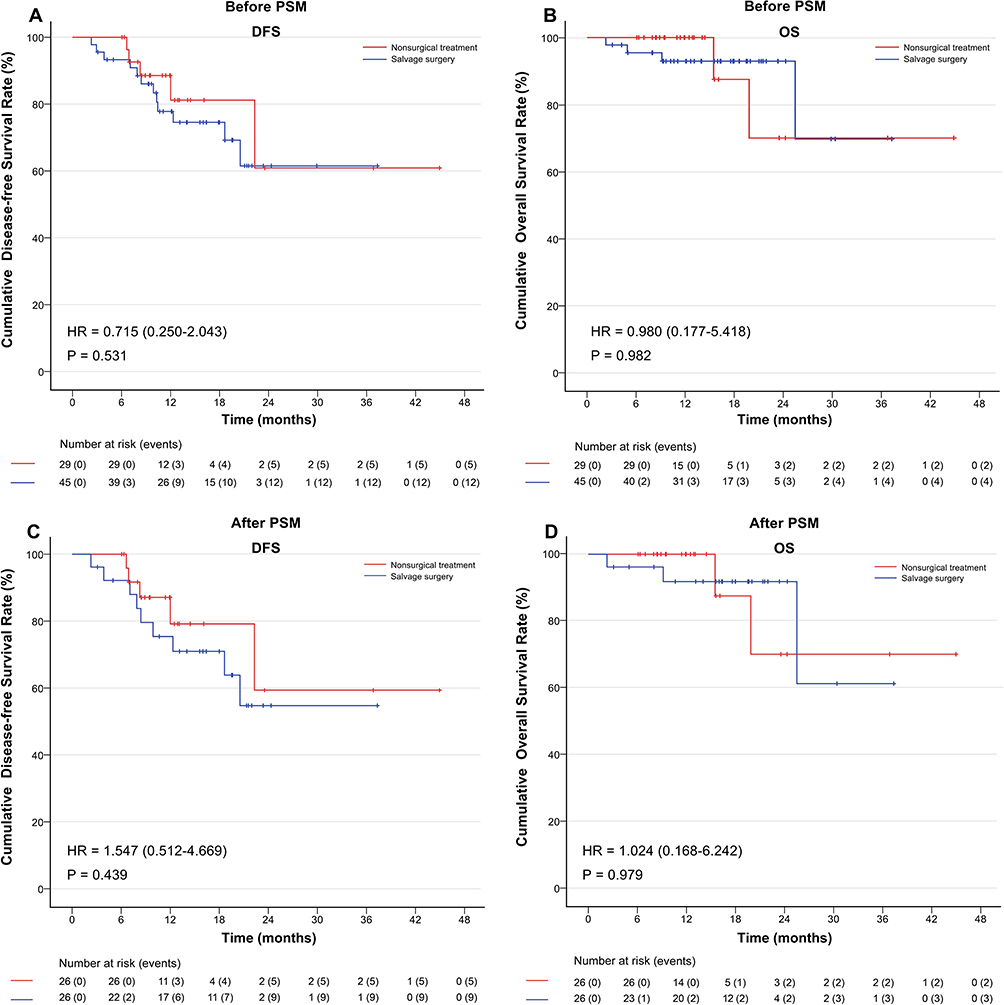 |
Figure 3 Kaplan–Meier analysis of the DFS and OS before (A and B) and after PSM (C and D). Abbreviations: DFS, disease-free survival; OS, overall survival; HR, hazard ratio; PSM, propensity score matching. |
After PSM, 26 pairs of patients were selected. The demographic characteristics were balanced and comparable between the two groups (Table S3). The 1-,2-, and 3-year DFS rates were 75.4%, 54.7%, and 54.7% in the surgical group and 79.2%, 59.4%, and 59.4% in the non-surgical group, respectively. The 1-,2-, and 3-year OS rates were 91.8%, 91.8%, and 61.2% in the surgical group and 100%, 70%, and 70% in the non-surgical group, respectively (Figure 3C and D). There were no significant differences in DFS and OS between these two groups (p=0.439 and p=0.979, respectively).
Risk Factor Analysis for DFS and OS
Univariate analysis indicated that none of the factors, including sex, age, ECOG-PS, HBsAg, pre-treatment platelet-albumin-bilirubin grade, alanine aminotransferase, aspartate aminotransferase, pre-treatment AFP, pre-treatment PIVKA-II, tumor number, maximum tumor size, macrovascular invasion, and salvage hepatectomy had a statistically significant impact on DFS and OS (Table S4).
Discussion
Conversion therapy provides patients with initial uHCC the opportunity to undergo radical resection.8,21 However, whether conversion surgery can result in additional survival benefits for uHCC patients with CR remains controversial. In the present study, we retrospectively analyzed the prognosis of patients with cCR after conversion surgery. At a median follow-up of 18.6 months, the 1-, 2-, and 3-year DFS rates were 79.4%, 58.8%, and 58.8%, respectively, and the corresponding OS rates were 95.6%, 87.3%, and 72.7%, respectively. When comparing salvage surgery with nonsurgical treatment, no statistically significant differences for DFS and OS were observed before and after PSM. Therefore, patients with cCR had a good survival prognosis, and nonsurgical treatment achieved similar oncologic outcomes as those who underwent salvage surgery.
Currently, there are various conversion therapy regimens for uHCC, including atezolizumab plus bevacizumab, lenvatinib, sorafenib, TACE, and transarterial radioembolization.8–13,21–27 With the development of systemic therapy, there are more studies reporting patients with HCC that achieve CR. In randomized controlled trials, the rate of CR after systemic therapy ranges from 1–12.5% per modified Response Evaluation Criteria in Solid Tumors (1% for sintilimab plus bevacizumab,28 2% for lenvatinib,29 5% for lenvatinib plus pembrolizumab,30 8.9% for camrelizumab plus apatinib,31 and 12.5% for atezolizumab plus bevacizumab32). In a retrospective study,13 10 out of 101 patients with uHCC achieved PCR after conversion therapy with tyrosine kinase inhibitors plus an anti-PD-1 antibody, and 1- and 2-year recurrence-free survival rates were 90.0% and 73.6%, respectively. However, studies on survival prognosis for patients with CR are limited.
Conversion surgery offers the possibility of radical treatment and subsequently provides longer tumor-free survival and OS.8,21 In our previous study,33 70 patients with uHCC received salvage surgery after conversion therapy by TACE combined with lenvatinib plus anti-PD-1 antibodies, and the 1- and 2-year OS rates were 97.1% and 94.4%, respectively, and the PCR rate was 16% (29/181). However, the perioperative complications should be considered, especially PHLF; 4 out of our 70 patients presented with PHLF grade B or C. Luo et al found that hepatectomy after conversion therapy was more difficult than direct hepatectomy, as it led to a higher risk of PHLF (14.6%) and grade III–IV complications (26.8%).34 In this study, the risk of PHLF and serious post-hepatectomy complications were 22.2% and 6.7% in the surgical group, respectively. Thus, perioperative complications can not be ignored and may restrict the clinical application of salvage hepatectomy.
In rectal cancer patients with cCR, the “watch and wait” strategy is recommended to preserve anorectal function and avoid permanent colostomy,35 Several studies had confirmed that the “watch and wait” strategy can achieve long-term survival similar to radical surgery for rectal cancer patients with cCR.36–39 Therefore, the “watch and wait” strategy maybe applicable to uHCC patients with cCR, based on our results, especially for patients with high risk of perioperative complications or fear of surgery. Prospective trials with long term follow-up periods are warranted to evaluate this promising treatment option.
The long-term survival of nonsurgical treatment was similar to that of salvage surgery for patients with cCR, which may be attributed to the reasons below: first, although cCR is not equivalent to pCR, patients with cCR also had a deep tumor response. PCR rate reached 86.7% and only 2 patients (2.7%) developed LTP in the surgical group. Second, most patients who received conversion therapy had a high tumor burden, resulting in a high risk of recurrence after salvage hepatectomy. Consequently, the advantage of salvage hepatectomy may be challenged.
This study had some limitations. First, due to the retrospective analysis with a relatively small sample size and short follow-up time, further long-term randomized controlled trials are needed to confirm our conclusions. However, this study represents the largest reported case series on cCR after conversion therapy for uHCC patients to date. Second, the regimens and treatment durations of conversion therapy in our study were not uniform, which may have had different effects on patient survival. Third, most patients included in this study had HBV-related HCC, and the results of our study may not be applicable to HCC patients of other etiologies.
In conclusion, cCR after conversion therapy led to a good prognosis for patients with uHCC. Furthermore, nonsurgical treatment provided similar survival benefits to those of salvage hepatectomy. It tend to show that salvage hepatectomy may be not essential for uHCC patients with cCR, especially in patients with a high risk of surgical complications. Prospective trials with long-term follow-up periods are warranted to evaluate this promising treatment modality.
Data Sharing Statement
The data supporting the fundings of this study are available within the article.
Ethics Statement
This study was conducted in accordance with the World Medical Association Declaration of Helsinki and with approval from the Institutional Review Board (IRB) of Fujian Provincial Hospital (approval number: K2022-06-032).
Acknowledgments
We thank all the staff of the participating hospitals for their efforts, as well as all of the patients for their participation.
Funding
This study was funded by the Natural Science Foundation of Fujian Province (Grant number: 2022J011021) and the Medical Innovation Project of Health and Family Planning Commission of Fujian Province (Grant number: 2022CXA002).
Disclosure
All authors declare that they have no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
3. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of Hepatocellular carcinoma (2019 edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
4. Roayaie S, Jibara G, Tabrizian P, et al. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology. 2015;62(2):440–451. doi:10.1002/hep.27745
5. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
6. Bruix J, Gores G, Mazzaferro V. Hepatocellular carcinoma: clinical frontiers and perspectives. Gut. 2014;63(5):844–855. doi:10.1136/gutjnl-2013-306627
7. Villanueva A, Longo DL. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
8. Sun H, Zhou J, Wang Z, et al. Chinese expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobiliary Surg Nutr. 2022;11(2):227–252. doi:10.21037/hbsn-21-328
9. Kudo M. Combination cancer immunotherapy in hepatocellular carcinoma. Liver Cancer. 2018;7(1):20–27. doi:10.1159/000486487
10. Luo X, Wu K, He X. Advances in drug development for hepatocellular carcinoma: clinical trials and potential therapeutic targets. J Exp Clin Cancer Res. 2021;40(1):172. doi:10.1186/s13046-021-01968-w
11. Wu J, Yin Z, Bai Y, et al. Lenvatinib combined with anti-PD-1 antibodies plus transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: a multicenter retrospective study. J Hepatocell Carcinoma. 2021;8:1233–1240. doi:10.2147/JHC.S332420
12. Zhu X, Huang C, Shen Y, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and anti-PD-1 antibody combinations. Liver Cancer. 2021;10(4):320–329. doi:10.1159/000514313
13. Zhu X, Huang C, Shen Y, et al. Hepatectomy after conversion therapy using tyrosine kinase inhibitors plus anti-PD-1 antibody therapy for patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2023;30(5):2782–2790. doi:10.1245/s10434-022-12530-z
14. Lencioni R, Llovet J. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
15. US Department of Health and Human Services. Common terminology criteria for adverse events version 5.0. Available from: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50.
16. Chen K, Pan Y, Hu G-Y, et al. Laparoscopic versus open major hepatectomy for hepatocellular carcinoma: a meta-analysis. Surg Laparosc Endosc Percutan Tech. 2018;28(5):267–274. doi:10.1097/SLE.0000000000000567
17. Clavien P, Barkun J, de Oliveira M, et al. The Clavien–Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
18. Rahbari N, Garden O, Padbury R, et al. Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery. 2011;149(5):713–724. doi:10.1016/j.surg.2010.10.001
19. Dioguardi Burgio M, Sartoris R, Libotean C, et al. Lipiodol retention pattern after TACE for HCC is a predictor for local progression in lesions with complete response. Cancer Imaging. 2019;19(1):75. doi:10.1186/s40644-019-0260-2
20. Austin P. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–161. doi:10.1002/pst.433
21. Zhao H, Cai J. Chinese expert consensus on neoadjuvant and conversion therapies for hepatocellular carcinoma. World J Gastroenterol. 2021;27(47):8069–8080. doi:10.3748/wjg.v27.i47.8069
22. Shindoh J, Kawamura Y, Kobayashi Y, et al. Prognostic impact of surgical intervention after lenvatinib treatment for advanced hepatocellular carcinoma. Ann Surg Oncol. 2021;28(12):7663–7672. doi:10.1245/s10434-021-09974-0
23. Zhang Y, Huang G, Wang Y, et al. Is salvage liver resection necessary for initially unresectable hepatocellular carcinoma patients downstaged by transarterial chemoembolization? Ten years of experience. Oncologist. 2016;21(12):1442–1449. doi:10.1634/theoncologist.2016-0094
24. Chung T, Leung T, Chung C, et al. Ablative-transarterial radioembolization resulting in complete histopathological response of hepatocellular carcinoma in the resected liver specimen after salvage hepatectomy. Int J Surg Case Rep. 2022;90:106679. doi:10.1016/j.ijscr.2021.106679
25. Kudo M, Aoki T, Ueshima K, et al. Achievement of complete response and drug-free status by atezolizumab plus bevacizumab combined with or without curative conversion in patients with transarterial chemoembolization-unsuitable, intermediate-stage hepatocellular carcinoma: a multicenter proof-of-concept study. Liver Cancer. 2023;12(4):321–338. doi:10.1159/000529574
26. Gan L, Lang M, Tian X, et al. A retrospective analysis of conversion therapy with lenvatinib, sintilimab, and arterially-directed therapy in patients with initially unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:673–686. doi:10.2147/JHC.S404675
27. Shimose S, Iwamoto H, Shirono T, et al. The impact of curative conversion therapy aimed at a cancer-free state in patients with hepatocellular carcinoma treated with atezolizumab plus bevacizumab. Cancer Med. 2023;12(11):12325–12335. doi:10.1002/cam4.5931
28. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
29. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
30. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol. 2020;38(26):2960–2970. doi:10.1200/JCO.20.00808
31. Xu JM, Shen J, Gu SZ, et al. Camrelizumab in combination with apatinib in patients with advanced hepatocellular carcinoma (RESCUE): a nonrandomized, open-label, Phase II trial. Clin Cancer Res. 2021;27(4):1003–1011. doi:10.1158/1078-0432.CCR-20-2571
32. Qin S, Ren Z, Feng YH, et al. Atezolizumab plus bevacizumab versus sorafenib in the Chinese subpopulation with unresectable hepatocellular carcinoma: phase 3 randomized, open-label IMbrave150 study. Liver Cancer. 2021;10(4):296–308. doi:10.1159/000513486
33. Wu JY, Zhang ZB, Zhou JY, et al. Outcomes of salvage surgery for initially unresectable hepatocellular carcinoma converted by transcatheter arterial chemoembolization combined with lenvatinib plus anti-PD-1 antibodies: a multicenter retrospective study. Liver Cancer. 2023;12(3):229–237. doi:10.1159/000528356
34. Luo L, He Y, Zhu G, et al. Hepatectomy after conversion therapy for initially unresectable HCC: what is the difference? J Hepatocell Carcinoma. 2022;9:1353–1368. doi:10.2147/JHC.S388965
35. Habr-Gama A, Perez R, Nadalin W, et al. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: long-term results. Ann Surg. 2004;240(4):711–717; discussion 717–718. doi:10.1097/01.sla.0000141194.27992.32
36. Wang QX, Zhang R, Xiao WW, et al. The watch-and-wait strategy versus surgical resection for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy. Radiat Oncol. 2021;16(1):16. doi:10.1186/s13014-021-01746-0
37. Dattani M, Heald RJ, Goussous G, et al. Oncological and survival outcomes in watch and wait patients with a clinical complete response after neoadjuvant chemoradiotherapy for rectal cancer: a systematic review and pooled analysis. Ann Surg. 2018;268(6):955–967. doi:10.1097/SLA.0000000000002761
38. Renehan AG, Malcomson L, Emsley R, et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol. 2016;17(2):174–183. doi:10.1016/S1470-2045(15)00467-2
39. Dossa F, Chesney TR, Acuna SA, et al. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2017;2(7):501–513. doi:10.1016/S2468-1253(17)30074-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Preoperative Serum AFP, CEA, and CA19-9 Levels in Patients with Single Small Hepatocellular Carcinoma: Retrospective Study
Gan L, Ren S, Lang M, Li G, Fang F, Chen L, Liu Y, Han R, Zhu K, Song T
Journal of Hepatocellular Carcinoma 2022, 9:799-810
Published Date: 13 August 2022
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023
Negative Impact of Intra-Operative Blood Transfusion on Survival Outcomes of Hepatocellular Carcinoma Patients
Teng L, Zhao L, Shao H, Dai J, Zou H
Cancer Management and Research 2024, 16:385-393
Published Date: 25 April 2024
Postoperative Adjuvant Transcatheterarterial Chemoembolization Should Be Considered Selectively for Patients with Cytokeratin-19 Positive Hepatocellular Carcinoma
Mai RY, Tao Z, Huang HY, Zeng C, Mo KX, Zeng DD, Liang R, Lin Y, Wang XB, Bai T, Li LQ, Ye JZ, Wu GB
Journal of Hepatocellular Carcinoma 2025, 12:2407-2419
Published Date: 27 October 2025
Transcatheter Arterial Chemoembolization May Be Selectively Indicated as Postoperative Adjuvant Therapy for Hepatocellular Carcinoma Patients with Microvascular Invasion
Zeng J, Huang H, Tang M, Tao Z, Mo K, Chen W, Su Y, Su J, Liang R, Lin Y, Li L, Wu G, Luo X, Ye J, Mai R
Journal of Hepatocellular Carcinoma 2025, 12:2825-2838
Published Date: 18 December 2025