Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Postoperative Adjuvant Transcatheterarterial Chemoembolization Should Be Considered Selectively for Patients with Cytokeratin-19 Positive Hepatocellular Carcinoma
Authors Mai RY, Tao Z, Huang HY, Zeng C, Mo KX, Zeng DD, Liang R, Lin Y, Wang XB, Bai T, Li LQ ![]() , Ye JZ, Wu GB
, Ye JZ, Wu GB ![]()
Received 8 June 2025
Accepted for publication 26 September 2025
Published 27 October 2025 Volume 2025:12 Pages 2407—2419
DOI https://doi.org/10.2147/JHC.S537915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Rong-Yun Mai,1,* Zheng Tao,1,* Hong-Yang Huang,1,* Can Zeng,1 Kai-Xiang Mo,1 Dan-Dan Zeng,2 Rong Liang,2 Yan Lin,2 Xiao-Bo Wang,1 Tao Bai,1 Le-Qun Li,1 Jia-Zhou Ye,1 Guo-Bin Wu1
1Department of Hepatobiliary & Pancreatic Surgery, Guangxi Medical University Cancer Hospital, Nanning, 530021, People’s Republic of China; 2Department of Digestive Oncology, Guangxi Medical University Cancer Hospital, Nanning, 530021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jia-Zhou Ye; Guo-Bin Wu, Department of Hepatobilliary & Pancreatic Surgery, Guangxi Medical University Cancer Hospital, 71 He Di Road, Nanning, 530021, People’s Republic of China, Email [email protected]; [email protected]
Background: This study aimed to evaluate the clinical efficacy of postoperative adjuvant transarterial chemoembolization (PA-TACE) in cytokeratin 19-positive (CK19+) hepatocellular carcinoma (HCC) patients and to identify cases that may benefit from PA-TACE.
Methods: We conducted a retrospective analysis of 453 CK19+ HCC patients who underwent hepatectomy between November 2013 and June 2019 at our institution. We compared the recurrence-free survival (RFS) and overall survival (OS) between patients who received PA-TACE and those who did not, utilizing propensity score matching (PSM) to balance the groups.
Results: Before and after PSM, both RFS and OS were significantly greater in PA-TACE group compared to the non-TACE group. Multivariable analysis identified PA-TACE as a significantly favorable factor of RFS and OS. In subgroups analyses, PA-TACE significantly improved RFS and OS in patients with CK19+ HCC under the following conditions: alpha-fetoprotein ≥ 400 ng/mL, cirrhosis, tumor size ≥ 5 cm, multiple tumors, major resection, Edmondson-Steiner stage III–IV, macrovascular invasion and microvascular invasion. Similar results were obtained in patients with higher tumor stages. Further recurrence model analyses revealed that PA-TACE significantly reduced early recurrence in patients with high-risk of postoperative recurrence, but had little effect on late recurrence.
Conclusion: Among CK19+ HCC patients with higher recurrence of postoperative risk, PA-TACE could greatly improve RFS and OS.
Keywords: hepatocellular carcinoma, hepatectomy, cytokeratin 19, postoperative adjuvant transarterial chemoembolization, recurrence-free survival, overall survival
Introduction
Hepatocellular carcinoma (HCC) is one of the most common malignancies. Hepatectomy remains the major radical treatment for HCC, which can significantly improve long-term survival in these patients.1,2 However, the high tumor recurrence rate after surgery often leads to poor prognosis for these patients.3 Therefore, identifying high-invasive HCC subtypes and providing adjuvant therapy for specific patient groups will be significant in improving the prognosis of patients with HCC following surgery.
Among the progenitor cells biomarkers of liver malignancies, cytokeratin 19 (CK19) is typically not expressed in hepatocytes, but is highly expressed in liver progenitor cells and cholangiocytes.4 CK19-positive (CK19+) HCC subtypes are generally associated with poorer tumor differentiation, higher tumor recurrence, and poorer outcomes.4–6 Moreover, CK19+ is strongly linked to more aggressive and migratory HCC subtypes, such as “Chiang Proliferation”,7 “Hoshida S2”,8 “Shimada MS1”9 and “iCluster1 subtype”.10 Studies have confirmed that CK19+ HCC has a unique molecular profile that differs from other types of HCC.11–14 Taken together, CK19 should be considered as a unique subtype in the clinical diagnosis and treatment of HCC. Previous studies have shown that CK19 is closely related to the worse prognosis of HCC, but there are currently no effective option specifically targeting this subtype. Notably, previous studies confirmed that CK19+ HCC is resistant to chemotherapy drugs such as 5-fluorouracil and doxorubicin.11,15 Consequently, it is extremely required to determine adjuvant treatment regimes for CK19+ HCC patients following hepetectomy.
Postoperative adjuvant therapy is considered to be an effective measure to reduce tumor recurrence in patients undergoing hepatectomy for HCC.16,17 Recently, transarterial chemoembolization (TACE) is a significant adjuvant option to reduce the recurrence of HCC.18,19 Many evidences have suggested that postoperative adjuvant TACE (PA-TACE) is the main means to prevent recurrence and prolong survival in patients with HCC.20,21 Nevertheless, few researches have estimated the role of PA-TACE in CK19+ HCC patients. Although previous study have suggested that PA-TACE may significantly prolong recurrence-free survival (RFS) in CK19+ HCC patients after surgery,22 as a retrospective study, patient selection bias may limit the credibility of the findings. Thus, whether PA-TACE is helpful for all CK19+ HCC patients remains to be further studied.
The purpose of our research was to assess the clinical value of PA-TACE in patients with CK19+ HCC after liver resection, and to screen for potential beneficiaries who may benefit from PA-TACE.
Patients and Methods
Patients
From November 2013 to June 2019, CK19+ HCC patients undergoing hepatectomy at the Guangxi Medical University Cancer Hospital were included in the retrospective project. The inclusion criteria were: (1) underwent initial R0 hepatectomy; (2) histologically confirmed HCC with CK19+. The exclusion criteria were: (1) accompanied by other malignancies; (2) received other treatments for HCC prior to surgery; (3) received postoperative adjuvant therapy in addition to TACE; (4) incomplete clinical or imaging data. The flow chart of this study was presented in Supplementary Figure 1.
Diagnosis and Definitions
Histopathological evidence was used to determine the diagnosis of HCC, CK19, microvascular invasion (MiVI), macrovascular invasion (MaVI), and Edmondson-Steiner (ES) grade. CK19 expression in tissue biopsies was assessed via immunohistochemistry according to established protocols.23 A semi-quantitative scoring system evaluated staining intensity (0=absent, 1=faint yellow, 2=moderate brown, 3=strong tan) and positive cell proportion (0=<5%, 1=5-25%, 2=26-50%, 3=51-75%, 4≤75%). The composite score, derived from multiplying intensity and proportion scores, defined CK19 status as follows: 0–4=negative and 5–12=positive. Barcelona Clinical Liver Cancer (BCLC) staging system and Milan criteria were used to evaluate HCC stages. Curative hepatectomy was defined as the removal of all visible tumors, with microhistopathology showing no tumor cells at the surgical margin. Major hepatectomy was defined as the removal of more than three Couinaud hepatic segments.24
Hepatectomy and PA-TACE
The patients enrolled in this project all had good hepatic function and underwent R0 liver resection. The information of surgery has been detailed in our previous studies.25,26
PA-TACE was generally recommended for HCC patients with high risk of postoperative recurrence at 1 and 2 months after surgery. Adjuvant TACE was administered our per established protocols,27 employing a chemotherapeutic emulsion comprising pirarubicin or epirubicin (10–50 mg) combined with oxaliplatin (25–100 mg) and lipiodol (2–10 mL). This therapeutic cocktail was selectively delivered through catheterization of the target hepatic arterial branch, with individual dosages meticulously calibrated according to patient-specific anthropometric parameters.
Follow-Up
After discharge, all patients were followed up every 2–3 months for the first 2 years, and then every 6 months thereafter. Routine tests include liver and kidney function tests, serum alpha-fetoprotein (AFP) levels, abdominal ultrasound, chest and abdominal CT, or abdominal MRI at each follow-up visit. Recurrent HCC may be treated with repeat liver resection, radiofrequency ablation, TACE, or molecular targeted drug therapy, depending on the situation. The definitions of recurrence-free survival (RFS) and overall survival (OS) were consistent with our previous studies.25,26
Statistical Analysis
Continuous data were presented as mean ± standard deviation (SD) or median (interquartile range) and were compared using a two-tailed unpaired T-test or Mann–Whitney U-test. Categorical data were presented as as frequencies (proportions) and compared using Chi-square test or Fisher exact test.
Propensity score matching (PSM) analysis was performed by logistic regression to eliminate confounding factors. Specifically, age, sex, hepatitis B virus (HBV) infection, AFP, platelet count, prothrombin time, total bilirubin, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), tumor size, tumor number, ascites, cirrhosis, ES grade, MiVI, MaVI, and resection extent may affect PA-TACE selection and survival factors were included in the PSM analysis. A one-to-one nearest neighbor matching between groups was carried out by a 0.05 caliper.
RFS and OS were measured by Kaplan-Meier method and compared by Log rank test. Survival prognostic factors were identified through sequential Cox regression, with significant univariate predictors (P<0.05) advanced to multivariate analysis. All results were analyzed using SPSS (v26.0) software, and a p value < 0.05 was considered statistically significant.
Results
Patients’ Characteristics
Of the 413 patients included in the study, 136 (32.9%) patients were treated with PA-TACE and were assigned to the PA-TACE group, and the remaining 277 (67.1%) were assigned to the non-TACE group. As presented in Table 1, many factors were similar between the two groups, including gender, AFP levels, levels of TBIL, PLT, PT, ALB, ALT and AST, tumor size, cirrhosis, ascites, MaVI, MiVI, ES grade, Child-Pugh grade, resection extent and Milan criteria. Nevertheless, there were significant differences between the two groups in age, HBV infection, tumors number, and BCLC stage B HCC. After PSM analysis, 121 matched patients were selected, and all baseline indicators were not different between the two groups (Table 1 and Supplementary Figure 2).
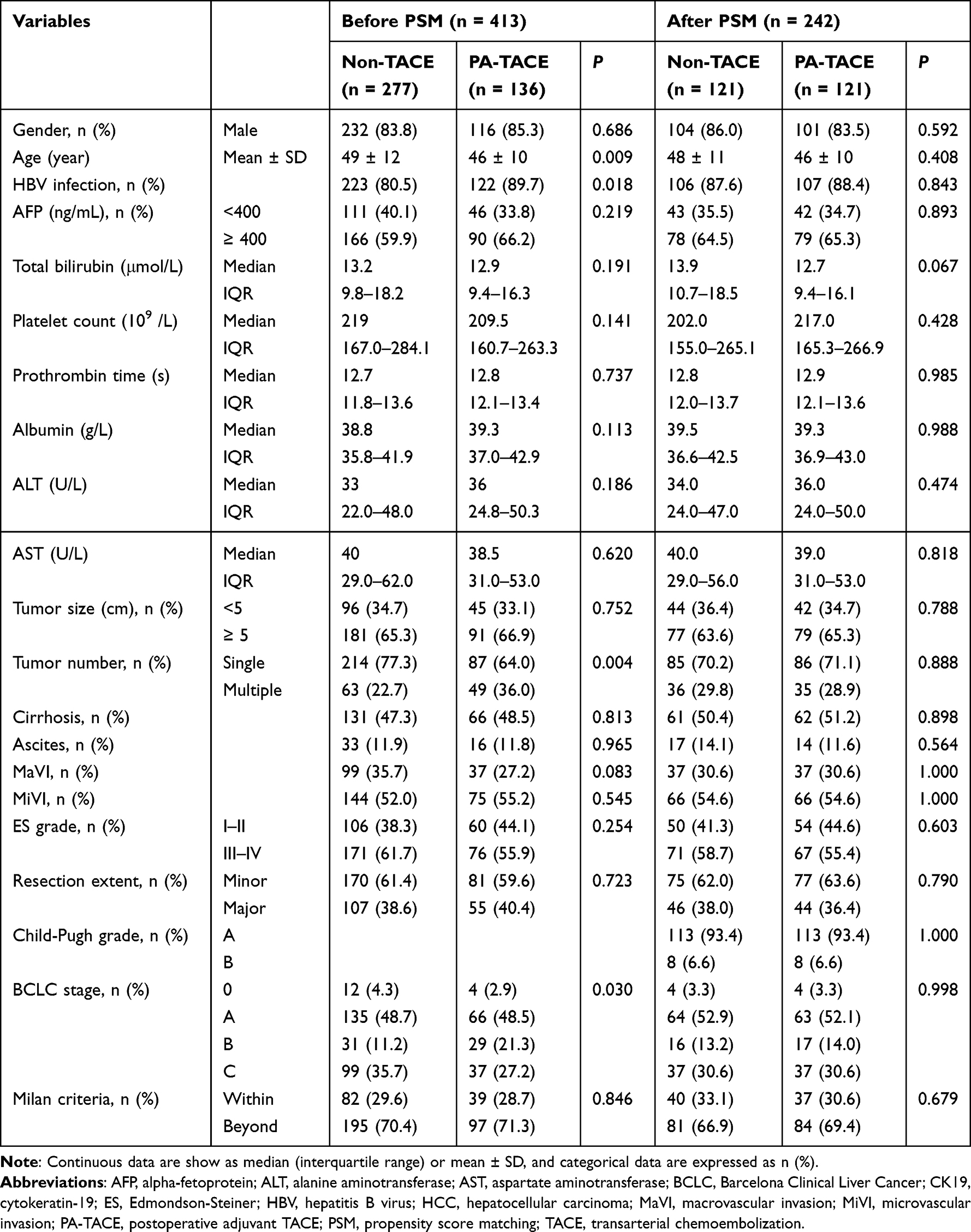 |
Table 1 Clinicopathologic Characteristics of the Non-TACE and PA-TACE Groups in Included CK19+ HCC Patients Before and After PSM |
Role of PA-TACE on the RFS
In the entire cohort, the median follow-up time (interquartile range) for RFS was 5.0 (2.0–15.5) months in the non-TACE group and 12.0 (4.0–23.0) months in the PA-TACE group. During follow-up, 255 patients (61.7%) occurred HCC recurrence, including 177 (63.9%) non-TACE patients and 78 (57.4%) PA-TACE patients. The 1, 3, and 5-year RFS in the PA-TACE group (51.7%, 24.1%, and 16.8%) was significantly higher than those in the non-TACE group (34.3%, 23.9% and 11.5%; P = 0.0036; Figure 1A).
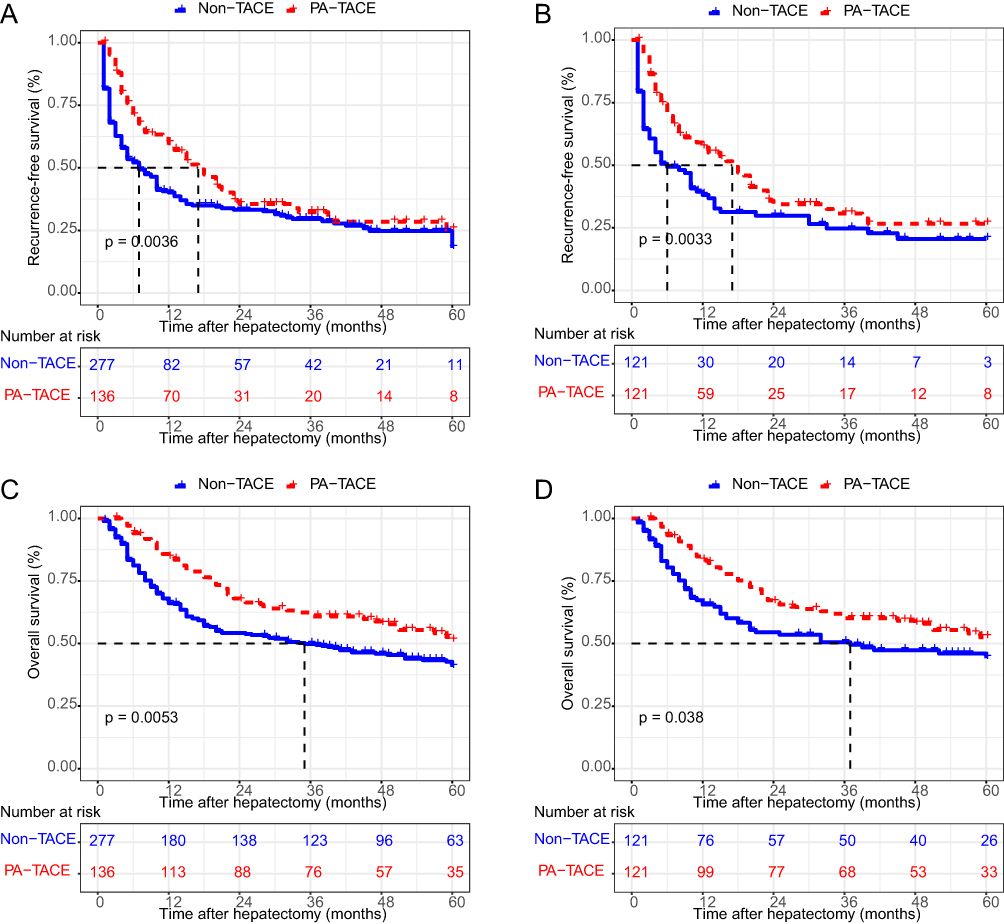 |
Figure 1 Comparison of RFS and OS between CK19+ HCC patients who received PA-TACE and those who did not. (A) RFS in before PSM group; (B) OS in before PSM group; (C) RFS in after PSM group; (D) OS in after PSM group. Abbreviations: CK19, cytokeratin-19; HCC, hepatocellular carcinoma; PA-TACE, postoperative adjuvant TACE; PSM, propensity score matching; OS, overall survival; RFS, recurrence free survival. |
Similarly, after PSM, the 1, 3, and 5-year RFS in the PA-TACE group (48.2%, 22.2%, and 18.2%) also remarkably greater than those in the non-TACE group (29.6%, 16.8%, and 12.9%; P = 0.0033; Figure 1B).
Independent Prognosis Predictors of RFS
As shown in Table 2, univariate analysis showed that lower albumin levels, larger tumor size, MaVI, MiVI, major resection, and absence of PA-TACE were significantly associated with poorer RFS. Subsequent multivariate analysis confirmed MiVI, major resection, and absence of PA-TACE as independent risk factors for poor RFS in patients with CK19+ HCC (all p < 0.05, Table 2).
 |
Table 2 Uni- and Multivariable Analyses to Identify Independent Risk Factors Affecting the RFS of CK19+ HCC Patients After Curative Hepatectomy |
Role of PA-TACE on the OS
The median follow-up for OS was 21.0 (8.0–56.5) months in the non-TACE group and 40.0 (15.8–60.0) months in the PA-TACE group. Among these patients, there were 59 deaths (43.4%) in the PA-TACE group and 151 deaths (54.5%) in the non-TACE group. The 1, 3, and 5 -years OS of PA-TACE group (78.2%, 52.9%, 42.5%) was greatly higher than that of non-TACE group (60.7%, 44.2%, 34.8%; P = 0.0053; Figure 1C).
After PSM, the 1, 3, and 5-year OS in the PA-TACE group in the PA-TACE group (76.6%, 51.8%, and 43.6%) also remarkably greater than those in the non-TACE group (57.5%, 42.0%, and 35.5%; P = 0.038; Figure 1D).
Independent Prognosis Predictors of OS
Univariate analysis found that large tumor size, MaVI, MiVI, major resection, and absence of PA-TACE were significantly associated with poorer OS (all p < 0.05, Table 3). Multivariate analysis further found that MiVI, major resection, and absence of PA-TACE were independent risk variables for worse OS in patients with CK19+ HCC (all p < 0.05, Table 3).
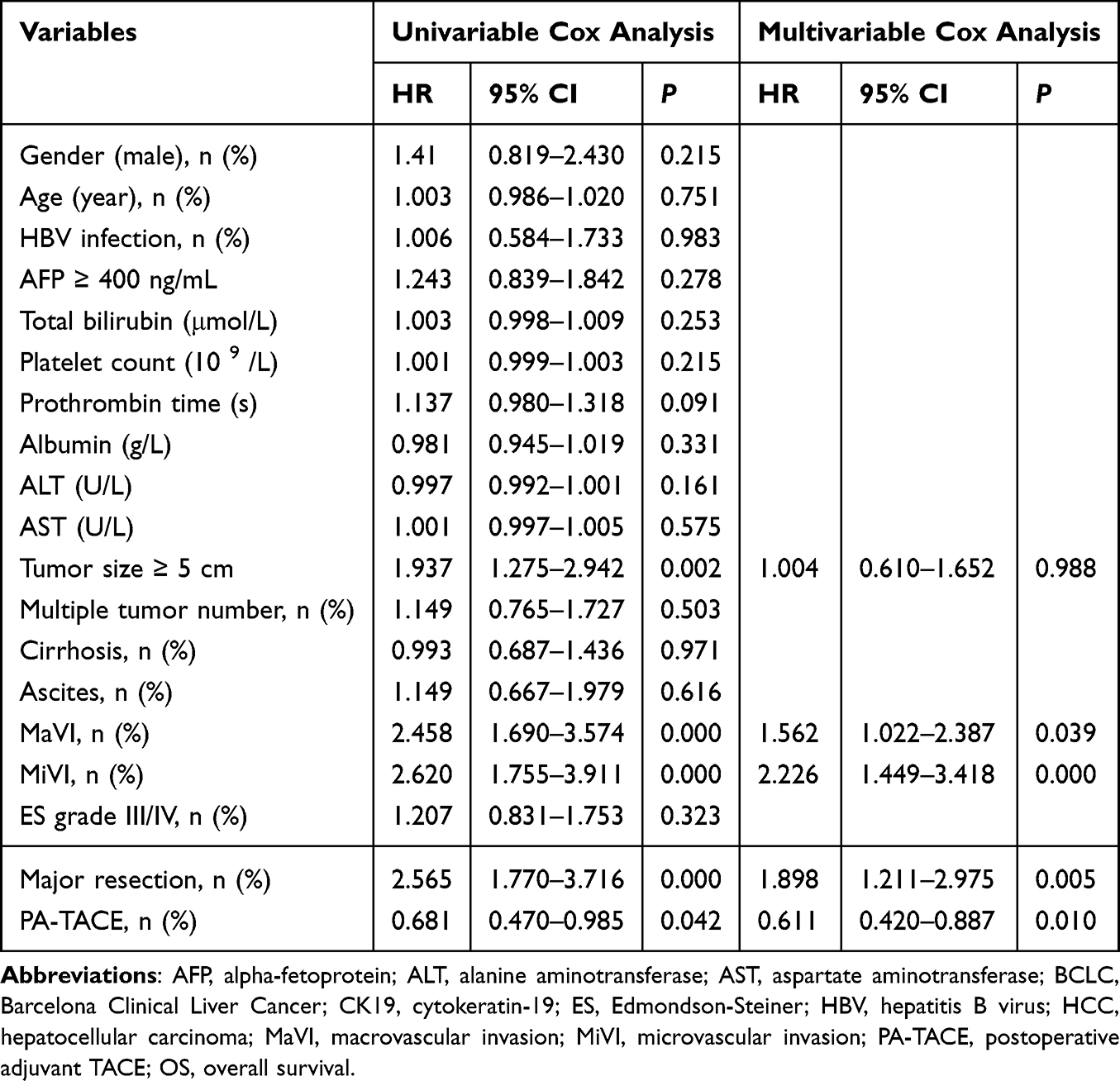 |
Table 3 Uni- and Multivariable Analyses to Identify Independent Factors Affecting the OS of Patients with CK19-Positive HCC After Curative Liver Resection |
Subgroups Analyses
Further investigation revealed the clinical value of PA-TACE in distinct recurrence-risk subgroups of CK19+ HCC patients stratified by AFP levels, presence of cirrhosis, tumor size, tumor numbers, extent of resection, pathological grade, and presence of MaVI or MiVI. We demonstrated that CK19+ HCC patients with AFP ≥400 ng/mL, cirrhosis, tumor size ≥5 cm, multiple tumors, major hepatectomy, ES grade III–IV, MaVI, or MiVI derived significant RFS (Figure 2A–H) and OS benefits (Figure 3A–H) from PA-TACE treatment. However, when the patient did not suffer the high risks of postoperative recurrence factors, PA-TACE did not show a prognostic benefit for these patients (Supplementary Figures 3 and 4). Similarly, for CK19+ HCC patients at higher tumor stages (BCLC stage B or C, and beyond Milan criteria), PA-TACE also provides significant benefits in terms of RFS and OS, but it is ineffective for lower tumor stages (Figure 4A–H). Further recurrence pattern subgroups analyses indicated that the beneficial role of PA-TACE on CK19+ HCC patients with high risk of postoperative recurrence was mainly due to reduce recurrence within 3 months after operation (Supplementary Table 1).
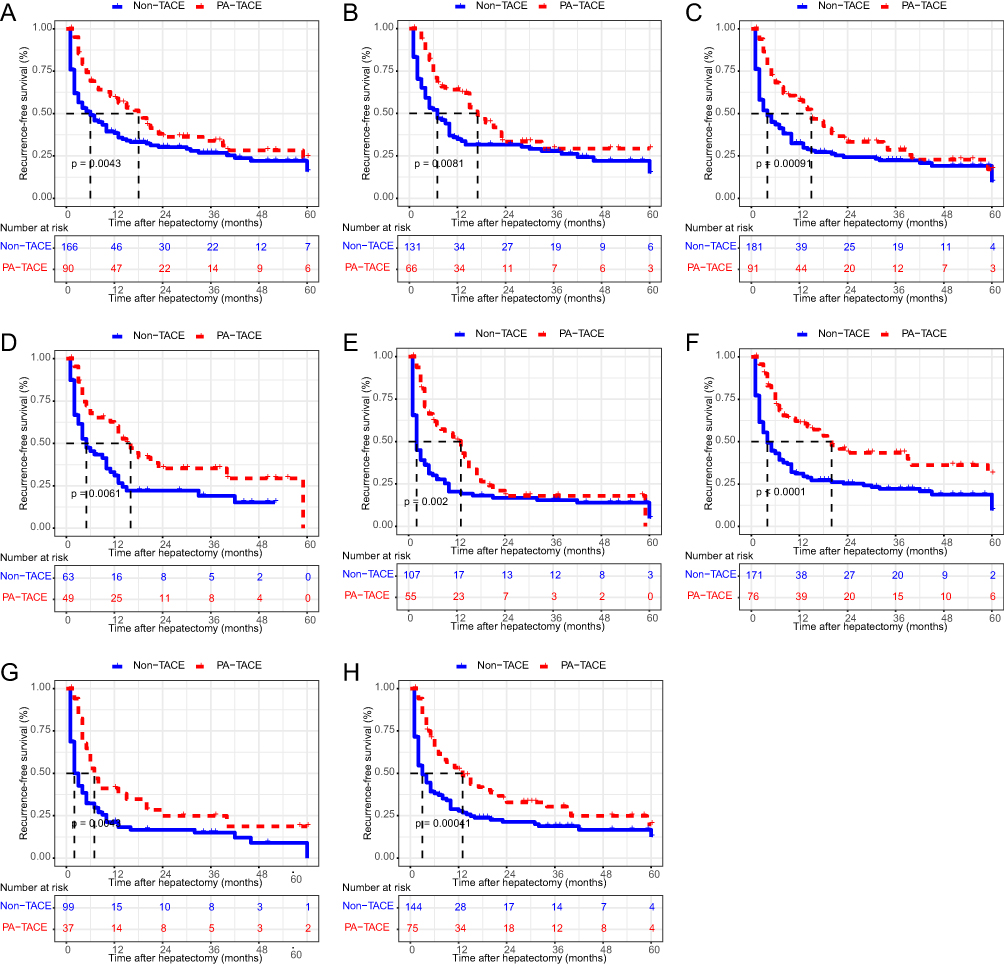 |
Figure 2 Subgroups analyses of RFS among high risk of postoperative recurrence in CK19+ HCC patients. (A) AFP ≥400 ng/mL; (B) presence of cirrhosis; (C) tumor size ≥ 5cm; (D) multiple tumor numbers; (E) major resection; (F) ES grade III–IV; (G) presence of MaVI; (H) presence of MiVI. Abbreviations: AFP, alpha-fetoprotein; CK19, cytokeratin-19; ES, Edmondson- Steiner; HCC, hepatocellular carcinoma; MaVI, macrovascular invasion; MiVI, microvascular invasion; RFS, recurrence free survival. |
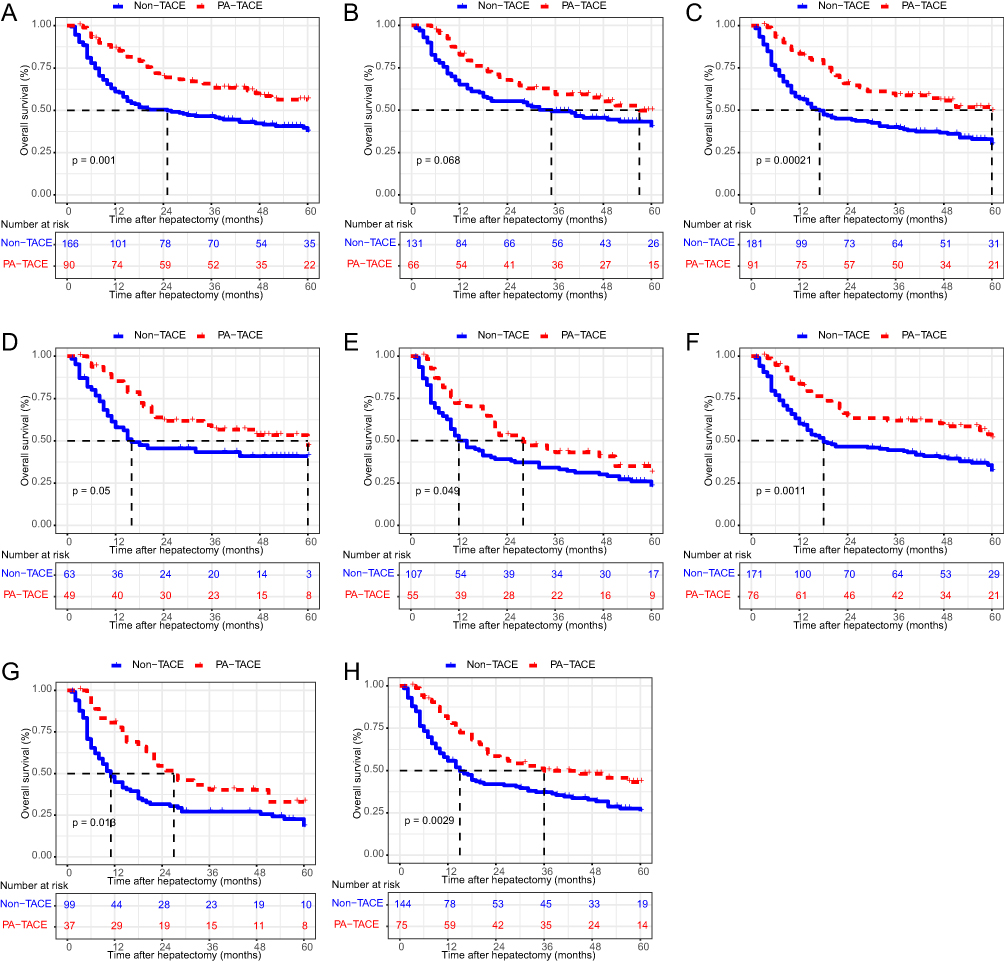 |
Figure 3 Subgroups analyses of OS among high risk factors in CK19+ HCC patients. (A) AFP ≥400 ng/mL; (B) presence of cirrhosis; (C) tumor size ≥ 5cm; (D) multiple tumor numbers; (E) major resection; (F) ES grade III–IV; (G) presence of MaVI; (H) presence of MiVI. Abbreviations: AFP, alpha-fetoprotein; CK19, cytokeratin-19; ES, Edmondson- Steiner; HCC, hepatocellular carcinoma; MaVI, macrovascular invasion; MiVI, microvascular invasion; OS, overall survival. |
 |
Figure 4 Subgroups analyses of RFS and OS in CK19+ HCC patients at different tumor stage. (A) RFS, BCLC stage 0 or A; (B) OS, BCLC stage 0 or A; (C) RFS, BCLC stage B or C; (D) OS, BCLC stage B or C; (E) RFS, within Milan criteria; (F) OS, within Milan criteria; (G) RFS, beyond Milan criteria; (H) OS, beyond Milan criteria. Abbreviations: BCLC, Barcelona Clinical Liver Cancer; CK19, cytokeratin-19; HCC, hepatocellular carcinoma; OS, overall survival; RFS, recurrence free survival. |
Discussion
In this study, we assessed the clinical role of PA-TACE on the prognosis of CK19+HCC patients who subjected to hepatectomy. Our study found that PA-TACE can significantly prolong RFS and OS in CK19+ HCC patients, and PA-TACE was a greatly favorable variable for prognosis evaluation. In addition, subgroups analyses showed that the beneficial effects of PA-TACE on prognosis in those patients mainly occurred in patients with high risks of postoperative recurrence, but were not effective in patients without high risk factors. Therefore, we can definitely suggest that patients with CK19+ HCC should be considered selectively for PA-TACE.
At present, many evidences confirmed that CK19 is a specific marker of tumor stem cells, biliary tract and progenitor cells, which can significantly promote the malignant progression of HCC.28 CK19+ HCC patients often have the characteristics of stronger tumor invasion and metastasis, higher recurrence rate of intrahepatic lymph node metastasis and worse prognosis, which are closely related to clinical aggressiveness.29,30 It is of great significance to determine the expression status of CK19 in HCC patients for better clinical decision-making and improving prognosis. However, it cannot be detected prior to operation and can only be diagnosed by histology of the excised specimen.31 Therefore, in order to reduce HCC recurrence, it is very necessary to emphasize adjuvant therapy for CK19+HCC patients after surgery. PA-TACE, as the primary adjunctive therapy after hepatectomy, has been shown to be an effective regime for preventing recurrence in HCC patients with high risk of recurrences. Although previous study also have proposed that PA-TACE may greatly improve RFS in CK19+ HCC patients,22 the clinical value of PA-TACE in CK19+HCC patients is still unclear and more studies are needed.
In this study, survival analyses suggested that PA-TACE greatly prolong the RFS and OS of CK19+ HCC patients. Moreover, Cox univariate and multivariate analyses revealed that PA-TACE was an independent favorable factor for RFS and OS. Furthermore, subgroups analyses suggested that the protective role of PA-TACE on CK19+ HCC cases mainly occurred when there were high risks of postoperative recurrence, such as high AFP level, cirrhosis, large tumor, multiple tumors, major resection, high ES grade, MaVI and MiVI. These indicators have been extensively studied as high risk factors for postoperative recurrence in HCC patients.32–34 However, for patients without these factors, PA-TACE had little difference on their prognosis. Similarly, for CK19+ HCC patients at higher tumor stages (BCLC stage B or C and beyond Milan criteria), PA-TACE also provides significant benefits in terms of RFS and OS, but it is ineffective for lower tumor stages.
Many reports suggested that most HCC patients often experience recurrence within 2 years after surgery (early recurrence), and the recurrent lesions usually originate from intrahepatic micrometastases.35–37 Current research has confirmed that PA-TACE is an effective treatment option for intrahepatic micrometastasis. In our research, the recurrence rate of CK19+HCC patients with high risk of postoperative recurrence within 3 months after surgery was significantly higher in patients who did not receive PA-TACE than in patients who did (p<0.05 for both). After 3 months, the difference had narrowed significantly. This suggests that the beneficial effect of PA-TACE in CK19+ HCC patients with a high risk of postoperative recurrence is primarily in reducing recurrences within the first 3 months after surgery. This may be related to the fact that early recurrence mostly results from subclinical dissemination during the operation, and PA-TACE can effectively clear it.38,39 However, in patients with a low risk of postoperative recurrence, PA-TACE was not effective in reducing early or late recurrences, and the recurrence rates were similar between the two groups. Thus, for CK19+HCC patients with a low risk of postoperative recurrence, the limited effect of PA-TACE might be due to the low recurrence rate within 3 months after hepatectomy.
Currently, CK19 can only be definitively diagnosed by histopathology of surgical specimens. Consequently, postoperative adjuvant therapy plays a crucial role in preventing tumors recurrences. Unfortunately, in our results, PA-TACE failed to show significant effect in low-risk CK19+HCC patients, including AFP < 400 ng/mL, absence of cirrhosis, tumor size < 5 cm, single tumors, minor resection, ES I–II stage, absence of MaVI and MiVI. It is also ineffective in patients with low tumor stages, including BCLC stage 0 or A, CNLC stage Ia or Ib, and with Milan criteria. To mitigate the adverse effects of CK19, preoperative evaluation of CK19 status and timely surgical intervention are paramount in ensuring favorable outcomes. Notably, many current studies are enthusiastic about combining radiomics signatures and clinical indicators to predict CK19 expression and evaluate the prognosis of these patients. For example, Choi et al40 suggested that gadoxetic acid–enhanced and diffusion-weighted magnetic resonance imaging (MRI) may help to predict early recurrence in CK19+ HCC patients after hepatectomy. Zhao et al41 further developed a nomogram based on radiomics and serum AFP levels for individualized preoperative prediction of CK19 expression in HCC. These models can assess the probability of CK19 expression in HCC patients. For HCC patients with high probability of CK19 expression, expanded surgical resection margins, anatomical resection, and appropriate postoperative adjuvant therapy may be important measures to improve the prognosis of these patients.
This study has several notable limitations that should be acknowledged. Firstly, although PSM was implemented to minimize selection bias, residual confounding factors between compared groups may persist due to inherent methodological constraints. Secondly, the clinical relevance of our findings may be geographically constrained as the cohort predominantly comprised HBV-associated HCC cases, potentially limiting generalizability to populations with different etiological profiles. Thirdly, preoperative assessment of CK19 status currently remains impractical for clinical decision-making as it relies on postoperative histopathological confirmation, necessitating empirical selection criteria for PA-TACE candidate stratification. Furthermore, the absence of standardized PA-TACE protocols introduces potential variability, as the therapeutic agents and dosage regimens employed in this study may differ from those used at other institutions. Finally, while this retrospective single-center analysis provides preliminary insights, future multi-center prospective studies with protocol harmonization will be necessary to validate our findings and establish broader clinical applicability.
Conclusion
In summary, PA-TACE effectively extends the RFS and OS of CK19+ HCC patients following hepatic resection, particularly among those at high risks of postoperative recurrence. Therefore, it is crucial to prioritize comprehensive adjuvant therapies for CK19+ HCC patients following hepatic resection to enhance their prognosis.
Abbreviations
AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinical Liver Cancer; CK19, cytokeratin-19; ES, Edmondson-Steiner; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; MaVI, macrovascular invasion; MiVI, microvascular invasion; PA-TACE, postoperative adjuvant TACE; PSM, propensity score matching; TACE, transarterial chemoembolization.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Guo-Bin Wu) on reasonable request.
Ethics Approval and Consent to Participate
This study was approved and supervised by the Ethics Committee of Guangxi Medical University Cancer Hospital and conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was waived by the ethics committee due to the retrospective nature of the study. We confirm that all patient data was treated confidentially. All methods were carried out in accordance with relevant guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Guangxi Natural Science Foundation (No. 2025GXNSFBA069552, 2025GXNSFDA069007, 2024GXNSFDA010046, 2024GXNSFAA010401); National Natural Science Foundation of China (No.82460611, 82060427, 82103297); Project for Enhancing Young and Middle-aged Teacher’s Research Basis Ability in Colleges of Guangxi (NO. 2024KY0133); Youth Program of Scientific Research Foundation of Guangxi Medical University Cancer Hospital (NO.2023-7); Guangxi First Batch Qingmiao Young Talents Universal Support Policy Program; Guangxi Bagua Youth Outstanding Talent Training Program; Guangxi Medical and health key discipline construction project; Guangxi Medical and health key cultivation discipline construction project; Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University; Guangxi Scholarship Fund of Guangxi Education Department; Guangxi Medical University Outstanding Young Talents Training Program; Guangxi Medical University Cancer Hospital Outstanding Doctoral Support Project; Nanning Qingxiu District Science and Technology Project (No.2021010, 2021007, 2021012).
Disclosure
The authors declare that they have no competing interests.
References
1. Park S, Davis AM, Pillai AA. Prevention, diagnosis, and treatment of hepatocellular carcinoma. JAMA. 2024;332(12):1013–1014. doi:10.1001/jama.2024.14101
2. Liver EAftSot. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
3. Su JY, Liu SP, Xu XL, et al. Treatment duration of adjuvant immune checkpoint inhibitors in hepatocellular carcinoma patients at high risk of recurrence after resection: a prospective, multicentric cohort study. Liver Cancer. 2025;14(4):378–390. doi:10.1159/000542954
4. Wang F, Yan C, Huang X, He J, Yang M, Xian D. Radiomics and deep learning as important techniques of artificial intelligence - diagnosing perspectives in cytokeratin 19 positive hepatocellular carcinoma. J Hepatocell Carcinoma. 2025;12:1129–1140. doi:10.2147/JHC.S526887
5. Zhu D, Yang W, Zhou HF, et al. Prognostic implications of CK19 positivity in patients with early recurrent hepatocellular carcinoma after hepatic resection undergoing transarterial chemoembolization. BMC Gastroenterol. 2024;24(1):347. doi:10.1186/s12876-024-03417-2
6. Ou Z, Fu S, Yi J, Huang J, Zhu W. Diagnostic value of expressions of cancer stem cell markers for adverse outcomes of hepatocellular carcinoma and their associations with prognosis: a Bayesian network meta‑analysis. Oncol Lett. 2024;28(5):536. doi:10.3892/ol.2024.14669
7. Chiang DY, Villanueva A, Hoshida Y, et al. Focal gains of VEGFA and molecular classification of hepatocellular carcinoma. Cancer Res. 2008;68(16):6779–6788. doi:10.1158/0008-5472.CAN-08-0742
8. Hoshida Y, Nijman SM, Kobayashi M, et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. 2009;69(18):7385–7392. doi:10.1158/0008-5472.CAN-09-1089
9. Shimada S, Mogushi K, Akiyama Y, et al. Comprehensive molecular and immunological characterization of hepatocellular carcinoma. EBioMedicine. 2019;40:457–470. doi:10.1016/j.ebiom.2018.12.058
10. Ally A, Balasundaram M, Carlsen R. Comprehensive and integrative genomic characterization of hepatocellular carcinoma. Cell. 2017;169(7):1327–1341.e23. doi:10.1016/j.cell.2017.05.046
11. Govaere O, Komuta M, Berkers J, et al. Keratin 19: a key role player in the invasion of human hepatocellular carcinomas. Gut. 2014;63(4):674–685. doi:10.1136/gutjnl-2012-304351
12. Yang CL, Song R, Hu JW, et al. Integrating single-cell and bulk RNA sequencing reveals CK19 + cancer stem cells and their specific SPP1 + tumor-associated macrophage niche in HBV-related hepatocellular carcinoma. Hepatol Int. 2024;18(1):73–90. doi:10.1007/s12072-023-10615-9
13. Zhuo JY, Lu D, Tan WY, Zheng SS, Shen YQ, Xu X. CK19-positive hepatocellular carcinoma is a characteristic subtype. J Cancer. 2020;11(17):5069–5077. doi:10.7150/jca.44697
14. Yang C, Xiang W, Wu Z, et al. CK19 protein expression: the best cutoff value on the prognosis and the prognosis model of hepatocellular carcinoma. BMC Cancer. 2025;25(1):55. doi:10.1186/s12885-024-13399-9
15. Kawai T, Yasuchika K, Ishii T, et al. Keratin 19, a cancer stem cell marker in human hepatocellular carcinoma. Clin Cancer Res. 2015;21(13):3081–3091. doi:10.1158/1078-0432.CCR-14-1936
16. Xiang C, Shen X, Zeng X, et al. Effect of transarterial chemoembolization as postoperative adjuvant therapy for intermediate-stage hepatocellular carcinoma with microvascular invasion: a multicenter cohort study. Int J Surg. 2024;110(1):315–323. doi:10.1097/JS9.0000000000000805
17. Li ZX, Zhang QF, Huang JM, et al. Safety and efficacy of postoperative adjuvant therapy with atezolizumab and bevacizumab after radical resection of hepatocellular carcinoma. Clin Res Hepatol Gastroenterol. 2023;47(7):102165. doi:10.1016/j.clinre.2023.102165
18. Yang XW, Chen J, Yang MQ, et al. Postoperative adjuvant transarterial chemoembolization prolongs overall survival in alpha-fetoprotein-negative hepatocellular carcinoma with bile duct tumor thrombosis: a long-term retrospective cohort study. World J Surg Oncol. 2025;23(1):260. doi:10.1186/s12957-025-03917-9
19. Lu JP, Feng JK, Zhao Y, et al. Grading risk of microvascular invasion impacts survival in hepatocellular carcinoma patients undergoing adjuvant transarterial chemoembolization: a multicenter study. Eur J Surg Oncol. 2025;51(8):110102. doi:10.1016/j.ejso.2025.110102
20. Liu J, Ding X, Zhang Y, Li H. A clinical-imaging nomogram for predicting early recurrence in patients with solitary hepatocellular carcinoma after postoperative adjuvant TACE. J Hepatocell Carcinoma. 2025;12:1835–1847. doi:10.2147/JHC.S544127
21. Qian J, Shen Y, Cui L, et al. Survival effects of postoperative adjuvant TACE in early-HCC patients with microvascular invasion: a multicenter propensity score matching. J Cancer. 2024;15(1):68–78. doi:10.7150/jca.87435
22. Wu MS, Zhong JH, Chen K, et al. Association of CK19 expression with the efficacy of adjuvant transarterial chemoembolization after hepatic resection in hepatocellular carcinoma patients at high risk of recurrence. J Clin Trans Res. 2022;8(1):71–79.
23. Bader BL, Magin TM, Hatzfeld M, Franke WW. Amino acid sequence and gene organization of cytokeratin no. 19, an exceptional tail-less intermediate filament protein. EMBO J. 1986;5(8):1865–1875. doi:10.1002/j.1460-2075.1986.tb04438.x
24. Pol B, Campan P, Hardwigsen J, Botti G, Pons J, Le Treut YP. Morbidity of major hepatic resections: a 100-case prospective study. Eur J Surg. 1999;165(5):446–453. doi:10.1080/110241599750006686
25. Mai R, Bai T, Luo X, Wu G. Preoperative fibrinogen-to-albumin ratio predicts the prognosis of patients with hepatocellular carcinoma subjected to hepatectomy. BMC Gastroenterol. 2022;22(1):261. doi:10.1186/s12876-022-02328-4
26. Mai RY, Lu TL, Lu RJ, et al. C-Reactive Protein-Albumin Ratio (CAR): a more promising inflammation-based prognostic marker for patients undergoing curative hepatectomy for hepatocellular carcinoma. J Inflamm Res. 2024;17:919–931. doi:10.2147/JIR.S441623
27. Wang YY, Wang LJ, Xu D, et al. Postoperative adjuvant transcatheter arterial chemoembolization should be considered selectively in patients who have hepatocellular carcinoma with microvascular invasion. HPB. 2019;21(4):425–433. doi:10.1016/j.hpb.2018.08.001
28. Rhee H, Kim H, Park YN. Clinico-radio-pathological and molecular features of hepatocellular carcinomas with keratin 19 expression. Liver Cancer. 2020;9(6):663–681. doi:10.1159/000510522
29. Fatourou E, Koskinas J, Karandrea D, et al. Keratin 19 protein expression is an independent predictor of survival in human hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2015;27(9):1094–1102. doi:10.1097/MEG.0000000000000398
30. Lee SH, Lee JS, Na GH, You YK, Kim DG. Immunohistochemical markers for hepatocellular carcinoma prognosis after liver resection and liver transplantation. Clin Transplant. 2017;31(1). doi:10.1111/ctr.12852
31. Mehrpouya M, Pourhashem Z, Yardehnavi N, Oladnabi M. Evaluation of cytokeratin 19 as a prognostic tumoral and metastatic marker with focus on improved detection methods. J Cell Physiol. 2019;234(12):21425–21435. doi:10.1002/jcp.28768
32. Tung-Ping Poon R, Fan ST, Wong J. Risk factors, prevention, and management of postoperative recurrence after resection of hepatocellular carcinoma. Ann Surg. 2000;232(1):10–24. doi:10.1097/00000658-200007000-00003
33. Xu XF, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from China. JAMA Surg. 2019;154(3):209–217. doi:10.1001/jamasurg.2018.4334
34. Niu ZS, Wang WH, Niu XJ. Recent progress in molecular mechanisms of postoperative recurrence and metastasis of hepatocellular carcinoma. World J Gastroenterol. 2022;28(46):6433–6477. doi:10.3748/wjg.v28.i46.6433
35. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
36. Chidambaranathan-Reghupaty S, Fisher PB, Sarkar D. Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification. Adv Cancer Res. 2021;149:1–61.
37. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
38. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/S0168-8278(02)00360-4
39. Fuster-Anglada C, Mauro E, Ferrer-Fàbrega J, et al. Histological predictors of aggressive recurrence of hepatocellular carcinoma after liver resection. J Hepatol. 2024;81(6):995–1004. doi:10.1016/j.jhep.2024.06.018
40. Choi SY, Kim SH, Park CK, et al. Imaging features of gadoxetic acid-enhanced and diffusion-weighted MR imaging for identifying cytokeratin 19-positive hepatocellular carcinoma: a retrospective observational study. Radiology. 2018;286(3):897–908. doi:10.1148/radiol.2017162846
41. Zhao Y, Tan X, Chen J, et al. Preoperative prediction of cytokeratin-19 expression for hepatocellular carcinoma using T1 mapping on gadoxetic acid-enhanced MRI combined with diffusion-weighted imaging and clinical indicators. Front Oncol. 2022;12:1068231. doi:10.3389/fonc.2022.1068231
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Complete Response After Conversion Therapy for Unresectable Hepatocellular Carcinoma: Is Salvage Hepatectomy Necessary?
Wu JY, Wu JY, Liu DY, Li H, Zhuang SW, Li B, Zhou JY, Huang JY, Zhang ZB, Li SQ, Yan ML, Wang YD
Journal of Hepatocellular Carcinoma 2023, 10:2161-2171
Published Date: 5 December 2023
A Longitudinal Study of AFP Trajectories and Clinical Outcomes in Intermediate-Stage Hepatocellular Carcinoma After Hepatectomy
Yang H, Lu L, Guo W, Gong B, Wang X, Chen Y, Chen X
Journal of Hepatocellular Carcinoma 2024, 11:219-228
Published Date: 25 January 2024
Negative Impact of Intra-Operative Blood Transfusion on Survival Outcomes of Hepatocellular Carcinoma Patients
Teng L, Zhao L, Shao H, Dai J, Zou H
Cancer Management and Research 2024, 16:385-393
Published Date: 25 April 2024
Transcatheter Arterial Chemoembolization May Be Selectively Indicated as Postoperative Adjuvant Therapy for Hepatocellular Carcinoma Patients with Microvascular Invasion
Zeng J, Huang H, Tang M, Tao Z, Mo K, Chen W, Su Y, Su J, Liang R, Lin Y, Li L, Wu G, Luo X, Ye J, Mai R
Journal of Hepatocellular Carcinoma 2025, 12:2825-2838
Published Date: 18 December 2025
Comparable Long-Term Survival After Curative Hepatectomy for Solitary Large (5–10 cm) versus Giant (≥10 cm) Hepatocellular Carcinoma: A Retrospective Study
Jiang K, Li J, Zhang D, Wang W, Chang J
Journal of Hepatocellular Carcinoma 2026, 13:607722
Published Date: 8 June 2026