Back to Journals » Journal of Inflammation Research » Volume 19
The Systemic Immune-Inflammation Index as a Predictor of Clinical Outcomes in Chronic Coronary Syndrome: Influence of Diabetes Mellitus
Authors Gao L, Bai X, Zhao Y, Bao X, Lu J, Yu H ![]() , Xu B, Chen J, Kang L
, Xu B, Chen J, Kang L
Received 22 January 2026
Accepted for publication 23 April 2026
Published 22 May 2026 Volume 2026:19 591353
DOI https://doi.org/10.2147/JIR.S591353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qing Lin
Luwa Gao,1,* Xinbo Bai,1,* Yuqi Zhao,1 Xue Bao,1 Jing Lu,1 Haishen Yu,1 Biao Xu,1 Jianzhou Chen,1 Lina Kang1,2
1Department of Cardiology, Cardiovascular Disease Center, Jiangsu Key Laboratory for Cardiovascular Information and Health Engineering Medicine, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, People’s Republic of China; 2Department of Cardiology, Nanjing Drum Tower Hospital, Clinical College of Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lina Kang, Department of Cardiology, Cardiovascular Disease Center, Jiangsu Key Laboratory for Cardiovascular Information and Health Engineering Medicine, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210008, People’s Republic of China, Email [email protected] Jianzhou Chen, Department of Cardiology, Cardiovascular Disease Center, Jiangsu Key Laboratory for Cardiovascular Information and Health Engineering Medicine, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210008, People’s Republic of China, Email [email protected]
Background: Systemic inflammation plays a critical role in the prognosis of coronary heart disease, and the Systemic Immune-Inflammation Index (SII) reflects both inflammatory status and immune balance. While elevated SII has been associated with adverse outcomes, its prognostic value in chronic coronary syndrome (CCS), particularly among diabetic patients, remains unclear. Hyperglycemia-induced inflammation, which enhances neutrophil activation and platelet reactivity, contributes to a more severe atherosclerosis burden in diabetes. This study investigated the predictive value of SII in CCS patients and examined whether diabetes modifies this relationship.
Methods: From January to December 2022, a cohort of 853 individuals with CCS who underwent coronary angiography was retrospectively analyzed and stratified by SII and glycometabolic status. This retrospective cohort study utilized fully anonymized data from the Coronary Heart Disease Database of Nanjing Drum Tower Hospital. Major adverse cardiovascular and cerebrovascular events (MACCEs), comprising cardiovascular death, nonfatal myocardial infarction, heart failure, ischemia-driven revascularization, and stroke, served as the primary endpoints. Kaplan–Meier analysis, Cox proportional hazard models, and restricted cubic spline (RCS) models were performed to evaluate the independent and combined effects of SII and glycometabolic status on clinical outcomes.
Results: Over a median follow-up period of 36 months, 85 patients (9.96%) experienced MACCEs. Higher log-transformed SII remained an independent predictor of MACCEs in the whole cohort (hazard ratio (HR) 1.63, 95% confidence interval (CI) 1.05– 2.55, P = 0.031) and particularly among patients with diabetes (HR 2.24, 95% CI 1.31– 3.82, P = 0.003) after full adjustment. However, there was no statistical significance among non-diabetic individuals (P = 0.772). Comparable findings were observed when SII was analyzed using the optimal cutoff value or quartiles. RCS analysis showed that MACCEs risk appeared to increase linearly with rising SII levels among diabetic patients. Furthermore, the combination of elevated SII and diabetes identified the subgroup with the poorest prognosis (P< 0.01).
Conclusion: Elevated SII levels independently predict adverse outcomes in patients with CCS, with a stronger prognostic effect among those with diabetes. These findings suggest that SII may serve as a simple and accessible marker for personalized risk stratification in CCS, especially in patients with diabetes.
Keywords: systemic immune-inflammation index, chronic coronary syndrome, diabetes mellitus, inflammation, prognosis, cardiovascular risk
Introduction
Chronic coronary syndrome (CCS), characterized by progressive atherosclerosis, is a major component of the coronary heart disease spectrum and an important contributor to the global burden of disease and cardiovascular mortality.1 Unlike acute coronary syndrome (ACS), CCS requires long-term symptom management and strategies to delay plaque progression and prevent future cardiovascular events. Despite guideline-driven management of traditional risk factors, a considerable number of patients continue to experience adverse cardiovascular outcomes. Increasing evidence suggests that chronic low-grade inflammation plays a significant role in plaque instability and residual cardiovascular risk.2
Lipid accumulation within the arterial wall activates various immune cells, including neutrophils, lymphocytes, and monocyte-macrophages, which promote the release of inflammatory cytokines, endothelial dysfunction, foam cell formation, and plaque rupture.3,4 Previous studies have identified interleukin-6 and high-sensitivity C-reactive protein (hs-CRP) as key biomarkers for coronary artery disease.5,6 Furthermore, large-scale anti-inflammatory trials have confirmed the causal role of inflammation in atherosclerotic cardiovascular diseases.7–9
In recent years, compared to molecular markers, circulating blood cell count-based indices have gained recognition as inexpensive, readily available, and reproducible indicators of the systemic inflammatory response.10–12 Compared with conventional inflammatory biomarkers such as hs-CRP, NLR, PLR, and MLR, the Systemic Immune-Inflammation Index (SII)-an integrated index-may provide a comprehensive view of the inflammatory milieu by capturing the synergistic contributions of neutrophil-driven inflammation, lymphocyte-mediated immune regulation, and platelet activation. Initially introduced by Hu et al for risk stratification in individuals with hepatocellular carcinoma following surgery.13 SII has since been shown to be significantly correlated with worse clinical outcomes in various cardiovascular diseases.14–16 However, evidence from ACS cannot be directly extrapolated to CCS, because ACS is characterized by abrupt plaque disruption and acute cytokine storms, whereas CCS reflects a chronic progressive atherosclerotic state driven by persistent low-grade inflammation. Given these distinct pathobiological and temporal profiles, the prognostic value of SII warrants specific evaluation in patients with CCS.
Diabetes mellitus (DM), driven by chronic hyperglycemia, is a high-risk comorbidity in CCS and further accelerates atherosclerosis through endothelial injury, oxidative stress, and inflammatory activation.17,18 Chronic low-grade inflammation is recognized as the shared pathophysiological mechanism linking DM and atherosclerotic cardiovascular disease.19,20 Based on these findings, the cardiovascular benefits of novel antidiabetic medications, such as sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor (GLP-1R) agonists, partly resulted from modulation of inflammatory pathways in addition to glycemic control.21,22 However, whether SII maintains predictive utility in CCS, particularly in those with DM, remains unclear. Therefore, this study aims to explore the predictive value of SII in CCS and to determine whether DM modifies this association, offering a novel inflammatory biomarker for risk classification.
Methods
Study Design
This retrospective, observational cohort study was conducted at the Department of Cardiology, Nanjing University Medical School Affiliated Drum Tower Hospital. Patients aged >18 years with CCS, as defined by the 2024 European Society of Cardiology (ESC) guidelines, who underwent coronary angiography in 2022, were enrolled.1 Exclusion criteria included missing crucial baseline data, lost to follow-up, history of acute myocardial infarction (MI) within the preceding month, history of coronary artery bypass grafting (CABG), left ventricular ejection fraction <35%, severe cardiac valve disease, severe hepatic or renal insufficiency, acute infection, history of malignancy and autoimmune diseases (Supplementary Figure 1).
Data Acquisition and Gathering
Hospital electronic medical records provided comprehensive clinical and laboratory profiles. Demographic variables contained age, sex, alcohol consumption, smoking status, as well as body mass index (BMI). Comorbidities comprised diabetes mellitus, hypertension, dyslipidemia, stroke, and prior percutaneous coronary intervention (PCI). Laboratory parameters included complete blood count, C-reactive protein (CRP), glucose metabolism, lipid profiles, and renal function parameters. Venous blood samples were collected from all patients under fasting conditions (>8 hours) within 24 hours post-admission and prior to coronary angiography. Echocardiography was used to assess left ventricular structure and left ventricular ejection fraction (LVEF) before coronary angiography. Coronary angiography documented the anatomical location of coronary lesions and the number of vessels involved. Pharmacotherapy profiles were recorded, primarily encompassing anticoagulants, antihypertensive medications, lipid-lowering agents, and hypoglycemic therapies.
Ethical Statement
The study protocol was approved by the Ethics Committee of Nanjing Drum Tower Hospital, affiliated with Nanjing University Medical School (Approval No. 2021-531-02). Given the retrospective nature of this study and the use of fully anonymized clinical data obtained during routine clinical practice, the Ethics Committee exempted the requirement for written informed consent during its review. It approved the use of verbal informed consent and did not issue separate additional approval documentation. This approach was deemed appropriate because the research involved no additional interventions or risks to patients, all data were fully de-identified before analysis, and re-contacting patients for written consent was deemed impractical and liable to introduce selection bias. Verbal informed consent was obtained from participants or their legal representatives during clinical follow-up or via telephone, and the consent process was documented in the patients’ electronic medical records by the attending clinical team. All data were anonymized and coded to ensure confidentiality. This study imposed no additional financial burden or medical risk on the patients and did not influence their clinical management. All procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki. The study was conducted in accordance with the Reporting of Studies Conducted using Observational Routinely-collected Health Data (RECORD) guidelines.
Relevant Definitions
SII was calculated by multiplying the platelet count by the neutrophil-to-lymphocyte ratio. Hypertension was defined by a physician diagnosis, systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, or ongoing antihypertensive treatment. Dyslipidemia was identified based on abnormal lipid profiles. Diabetes was defined by a documented history, a fasting plasma glucose (FPG) level of>126 mg/dL or a glycated hemoglobin A1c (HbA1c) level of>6.5%, or receipt of antidiabetic therapy. Estimated glomerular filtration rate (eGFR) was calculated using the Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, with values <90 mL/min/1.73 m2 serving as the criterion for chronic renal insufficiency.23 BMI was calculated as a standardized anthropometric measure by dividing an individual’s body weight in kilograms by the square of their height in meters (kg/m2).
Outcomes
All participants were followed up by physicians from Nanjing University Medical School Affiliated Drum Tower Hospital via telephone or outpatient visits from the day of discharge until the occurrence of a study endpoint or the last follow-up in July 2025. The primary outcome was the incidence of major adverse cardiovascular and cerebrovascular events (MACCEs), which included cardiovascular death, non-fatal myocardial infarction (MI), heart failure (HF), ischemia-driven revascularization, and stroke. Secondary endpoints were individual MACCEs components. Additional endpoints were disregarded. We further categorized individual endpoints into “hard” and “soft” components. The former classification comprised cardiovascular death, stroke, MI, and HF, whereas the latter included ischemia-driven revascularization. Non-fatal MI was defined by the presence of ischemic symptoms accompanied by a dynamic rise in cardiac biomarkers. Ischemia-driven revascularization referred to any PCI or CABG prompted by objective evidence of ischemia, excluding elective prophylactic procedures. Stroke was characterized as a neurological deficit caused by ischemia or a hemorrhagic event, with symptoms lasting ≥24 hours. All endpoint events were independently adjudicated by two cardiovascular specialists who were blinded to the patients’ baseline characteristics, including SII values. For events identified during telephone follow-up, relevant medical records and procedural reports were reviewed whenever available to confirm the diagnosis. Any disagreements were resolved by consensus with a third senior cardiologist.
Statistical Analysis
Using the “maxstat” package in R, the optimal SII cutoff was determined to stratify patients into two groups: higher and lower. Additionally, participants were further stratified into four quartile subgroups based on SII levels to assess the risk of major adverse cardiovascular and cerebrovascular events (MACCEs) in greater detail. In this study, continuous variables were expressed as means ± standard deviation (SD) or median (interquartile ranges, IQR), based on the results of the Shapiro–Wilk test. Intergroup comparisons of baseline characteristics were performed using Student’s t-test or Mann–Whitney U-test. Frequencies (percentages) were presented for categorical variables, and comparisons were made using χ2 or Fisher’s exact tests.
Cumulative incidence curves for MACCEs were analyzed using the Kaplan-Meier method, with intergroup differences assessed via Log rank tests. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated using multivariable Cox proportional hazards models to assess the association between SII and prognosis in patients with CCS. Covariates were selected based on statistical significance (P < 0.05) from univariate Cox regression analysis (Supplementary Table 1) or established clinical significance. Cox proportional hazards models were employed to evaluate the relationship: Model 1 (unadjusted, including only SII); Model 2 (adjusted for age and sex); and Model 3 (adjusted for age, sex, smoking status, hypertension, prior PCI, multivessel disease, antidiabetic medications, HbA1c, CRP, eGFR, high-density lipoprotein cholesterol (HDL-c), LVEF, and left ventricular end-diastolic diameters (LVEDD)). Variance inflation factors (VIF) were calculated to assess multicollinearity (Supplementary Table 2), with all values < 5, indicating no substantial collinearity. We also performed a supplementary analysis, which repeated the multivariable Cox regression analyses by removing some covariates, to examine the robustness of our findings. Restricted cubic spline (RCS) analysis was used to evaluate potential nonlinear associations between SII and MACCEs risk, adjusting for covariates in Model 3. Furthermore, we analyzed the synergistic impact of glycemic metabolism status and SII on CCS prognosis by stratifying participants into four groups: Lower SII and non-DM, Higher SII and non-DM, Lower SII and DM, as well as Higher SII and DM. The comparative risk of MACCEs across these subgroups was evaluated using Cox proportional hazards modeling, Kaplan-Meier curves, and Log rank tests. Subgroup analyses of MACCE risk were conducted based on age, sex, smoking status, BMI, hypertension, renal impairment, LVEF, and multivessel disease, with results visualized via forest plots. The Schoenfeld residual test was used to check the proportional hazards assumption of the Cox regression model. Statistical analyses were conducted using R (version 4.4.1) and SPSS (version 27.0) software. Statistical significance was determined by bilateral p < 0.05.
Results
A total of 853 participants were included in the final analysis after applying the exclusion criteria and removing cases with missing SII data or loss to follow-up (Supplementary Figure 1). The cohort was predominantly male (65.3%), with a median age of 65 years (IQR 58–71), and was followed for a median of 36 months (IQR 33–39). Using maximal selection rank statistics, the cohort was dichotomized at an optimal SII cut-off of 327 (Supplementary Figure 2) into higher (SII > 327, n = 550) and lower (SII ≤ 327, n = 303) groups.
Baseline Characteristics
Table 1 presents baseline clinical characteristics, laboratory findings, and cardiovascular medication use of the CCS population, categorized by the SII cutoff. Patients with elevated SII levels were more likely to be male. They exhibited higher BMI and blood pressure, as well as a greater prevalence of stroke and hypertension (all P < 0.05). FPG, triglyceride (TG), and serum creatinine were elevated, while HDL-c was lower in the higher SII subgroup (all P < 0.05). Inflammatory indices, comprising white cell count, neutrophil count, platelet count, and CRP, were significantly elevated in the higher SII group, accompanied by a concurrent reduction in lymphocytes (all P < 0.01). Echocardiographic and angiographic measurements showed no significant differences. Statin use differed between groups (P = 0.029), while other medication profiles remained comparable. (Table 1).
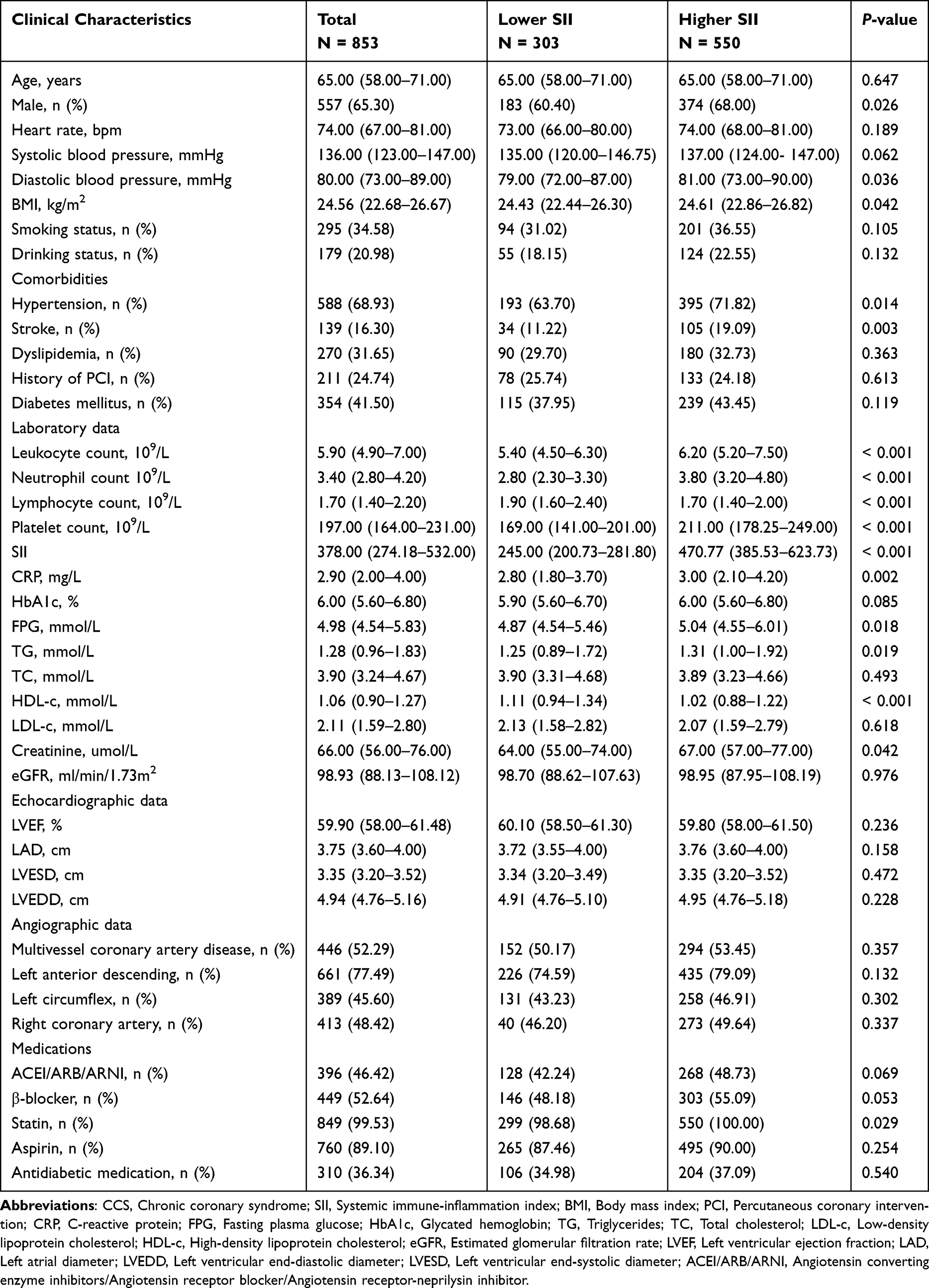 |
Table 1 Baseline Characteristics of the CCS Population Classified by SII Level |
Table S3 presents baseline characteristics stratified by combined SII levels and diabetes status. Patients were categorized into four groups: Higher SII and DM, Lower SII and DM, Higher SII and non-DM, and Lower SII and non-DM. The Higher SII and DM group exhibited a higher inflammatory and metabolic burden, characterized by elevated white cell count, neutrophil count, platelet count, SII, FPG, HbA1c, TG, CRP, creatinine, and lower HDL-c and LVEF compared to the other three groups. These participants also showed higher rates of multivessel disease and more frequent use of aspirin, statins, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor neprilysin inhibitors (ACEI/ARB/ARNI), and antidiabetic agents (all P < 0.05). (Supplementary Table 3).
Clinical Outcomes
A total of 85 MACCEs (9.96%) occurred during the follow-up period, including 4 cardiovascular deaths (0.47%), 7 non-fatal MI events (0.82%), 5 HF events (0.59%), 60 ischemia-driven revascularizations (7.03%), and 9 strokes (1.06%). Kaplan-Meier curves for MACCEs, classified by SII and glycemic status, are shown in Figures 1 and 2. In the overall cohort, SII > 327 corresponded to a significantly higher incidence of MACCEs compared with SII ≤ 327 (Log-rank P = 0.003, Figure 1A), and the highest SII quartile similarly showed a higher risk (Log-rank P = 0.041, Figure 1D). Among individuals with diabetes, SII > 327 was a strong predictor of MACCEs (Log-rank P < 0.001, Figure 1B; Log-rank P = 0.030, Figure 1E), whereas no statistical significance was noted among non-diabetics (all Log-rank P > 0.05, Figure 1C and F).
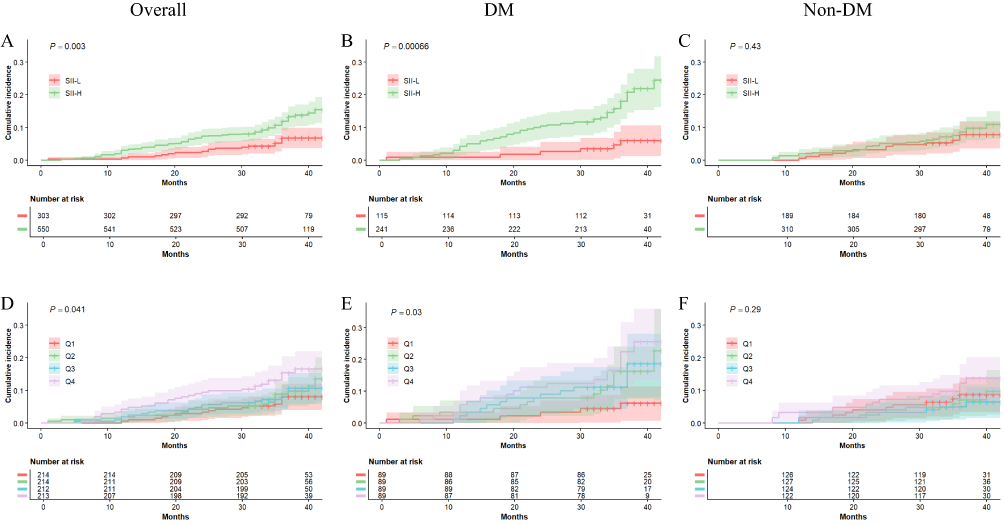 |
Figure 1 Kaplan-Meier survival curves for composite events stratified by the cutoff point of SII and SII quartiles in the whole cohort (A and D), in the diabetic cohort (B and E), and in the nondiabetic cohort (C and F). Abbreviation: SII, systemic immune-inflammation index. |
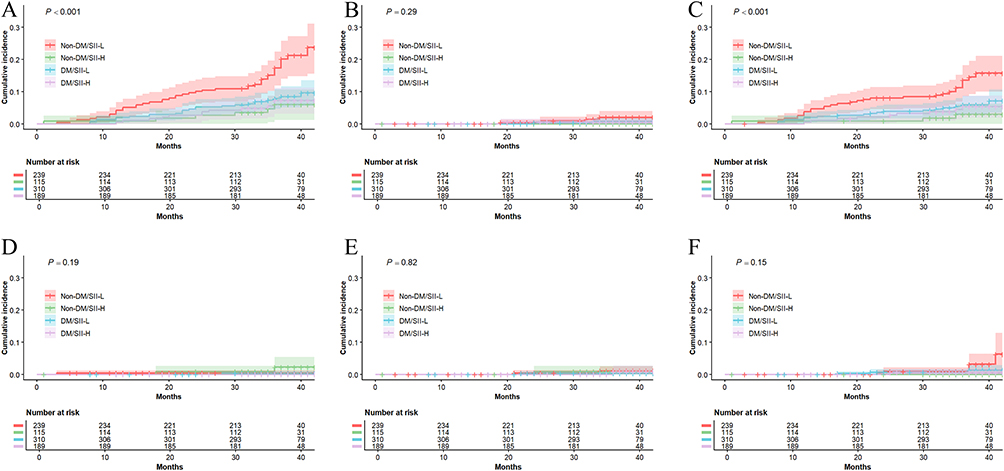 |
Figure 2 Kaplan–Meier curves for cumulative incidence of MACCE according to glycemic metabolism SII levels and glycemic metabolism. (A) Major adverse cardiovascular and cerebrovascular events (MACCEs); (B) Nonfatal myocardial infarction; (C) Ischemia-driven revascularization; (D) Cardiovascular death; (E) Heart failure; (F) Stroke. |
Cox regression results are summarized in Table 2. After full adjustment (Model 3), higher log-transformed SII, analyzed as a continuous variable, continued to independently predict MACCEs in the whole cohort (HR 1.63, 95% CI 1.05–2.55, P = 0.031) and particularly in diabetics (HR 2.24, 95% CI 1.31–3.82, P = 0.003), but not in non-diabetics (HR 1.10, 95% CI 0.57–2.11, P = 0.772). When dichotomized at the optimal cut-off, a higher SII level remained significantly associated with MACCEs in the general population (adjusted HR 1.98, 95% CI 1.16–3.36, P = 0.012) as well as the diabetic subgroup (adjusted HR 4.04, 95% CI 1.66–9.83, P = 0.002). Quartile analysis further reinforced the aforementioned findings: the highest SII quartile independently predicted poorer clinical outcomes in the overall cohort both before (unadjusted HR 2.24, 95% CI 1.21–4.15, P = 0.010) and after full adjustment (adjusted HR 1.93, 95% CI 1.02–3.65, P = 0.043). This relationship was particularly pronounced in diabetics (unadjusted HR 4.16, 95% CI 1.54–11.22, P = 0.005; adjusted HR 4.23, 95% CI 1.50–11.91, P = 0.006), whereas no significant association was found in individuals without diabetes (adjusted HR 1.35, 95% CI 0.59–3.05, P = 0.478). A significant interaction between SII and diabetes was detected (P for interaction = 0.004). Schoenfeld residual tests showed no violation of proportional hazards (global P = 0.253; Supplementary Figure 3). As a supplementary analysis, we refitted the multivariable model with fewer covariates, the results of which were similar to those in the main analysis (Supplementary Table 4). In component-specific analyses, the association between SII and individual endpoint components was most consistent for ischemia-driven revascularization (Supplementary Figure 4 and Supplementary Table 6), while no significant associations were observed for nonfatal MI, heart failure, cardiovascular death, or stroke (Supplementary Tables 5–8). Additionally, when endpoint components were regrouped into hard and soft endpoints, the observed association between SII and MACCEs appeared to be driven predominantly by the soft endpoint component (Supplementary Table 7).
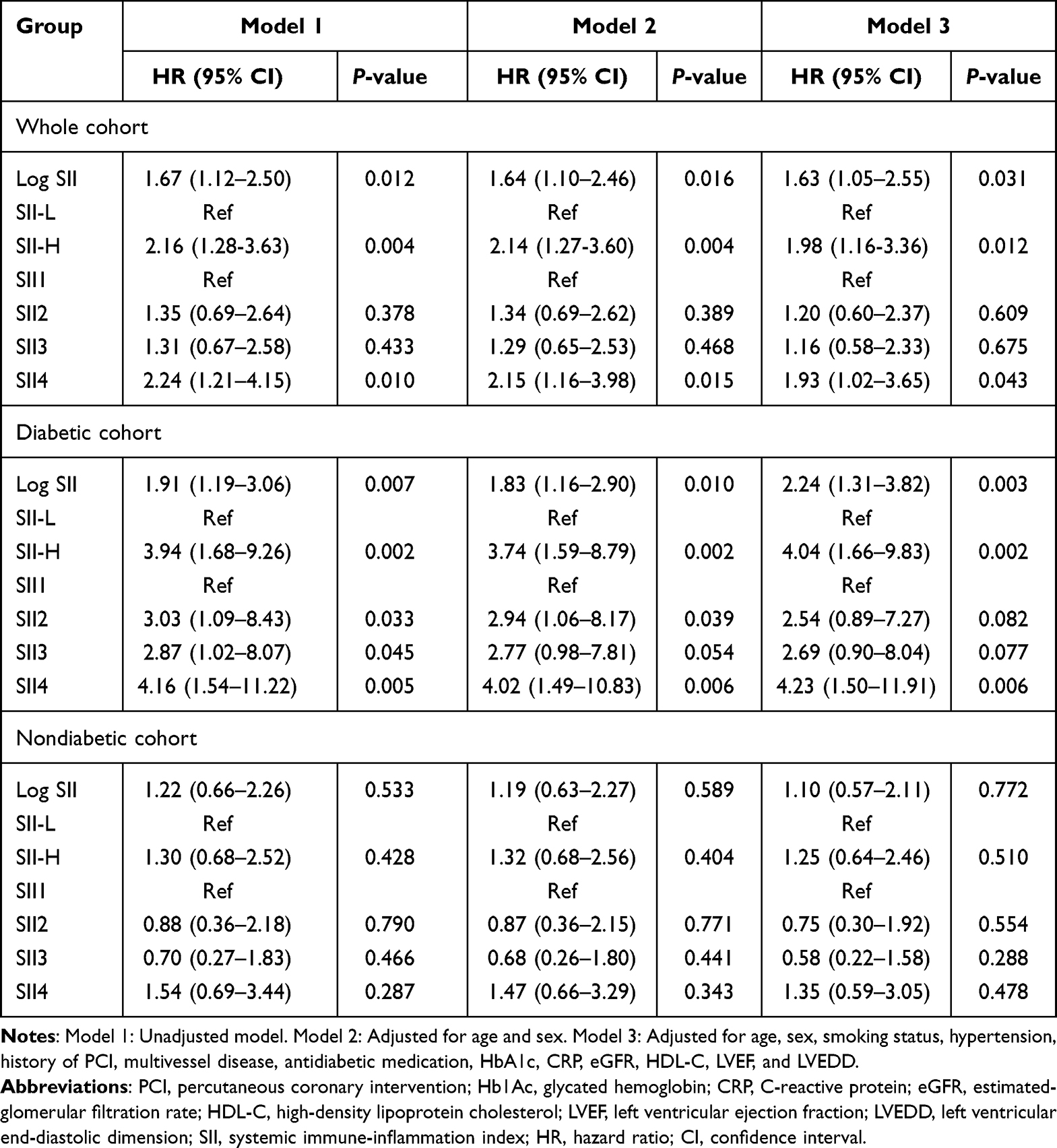 |
Table 2 Multivariate-Adjusted Cox Regression Models of SII for Clinical Outcomes in Overall, Diabetic, and Non-Diabetic CCS Patients |
Restricted cubic spline analysis further demonstrated a linear, dose-response, positive association between SII and MACCEs risk exclusively among diabetics (overall P = 0.0211, non-linear P = 0.375; Figure 3).
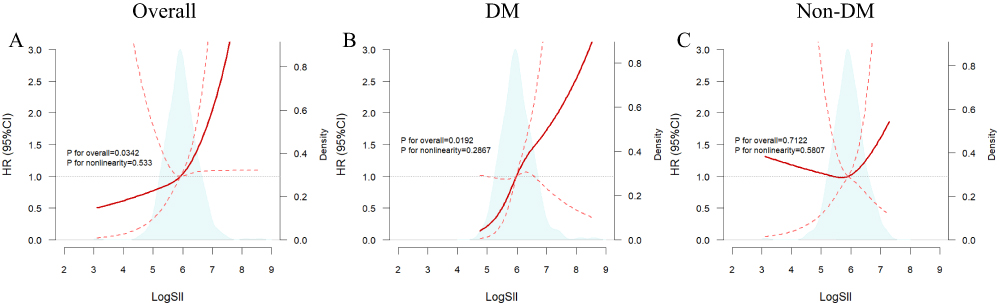 |
Figure 3 The association between SII with composite outcomes in the whole cohort (A), and in the diabetic (B) and nondiabetic (C) cohorts, was analyzed using restricted cubic splines (RCS). Blue areas show the distribution of SII levels. The solid red line in each figure indicates the HR, and the dashed red lines indicate the 95% CI. Covariates in the multivariable RCS model included: age, sex, smoking status, hypertension, history of PCI, multivessel coronary artery disease, antidiabetic medication, HbA1c, CRP, eGFR, HDL-C, LVEF, and LVEDD. Abbreviations: Log SII, Log-transformed systemic immune-inflammation index; HR, hazard ratio; CI, confidence interval. |
Integrated Assessment of SII and Diabetes
When patients were further classified into four groups according to SII level and diabetes status, Kaplan-Meier curves (Figure 2) showed that the Higher SII and DM group had the highest risk of MACCEs (Log-rank P < 0.001). The hazard ratios, using the Higher SII and DM group as a reference, were presented in Table 3. In the unadjusted analysis, patients in the Lower SII and DM, Higher SII and non-DM, as well as Lower SII and non-DM groups all demonstrated significantly reduced risk for MACCEs (unadjusted HR 0.27, 95% CI 0.11–0.63, P = 0.002; unadjusted HR 0.42, 95% CI 0.26–0.69, P = 0.001; unadjusted HR 0.33, 95% CI 0.17–0.62, P = 0.001; respectively). After multivariable adjustment, these findings remained significant (adjusted HR 0.30, 95% CI 0.13–0.72, P = 0.007; adjusted HR 0.32, 95% CI 0.14–0.76, P = 0.010; adjusted HR 0.26, 95% CI 0.10–0.67, P = 0.006; respectively), underscoring the strong link between elevated SII and MACCEs in the context of metabolic stress. Supplementary analysis further confirmed this finding after adjusting for covariates (Supplementary Table 5). For secondary endpoints, Kaplan-Meier curves revealed a significant difference in ischemia-driven revascularization across the four groups, whereas other components showed no statistically meaningful distinctions (Figure 2 and Supplementary Table 6). The association between SII and the composite outcome was largely attributable to the soft endpoint component (Supplementary Table 7).
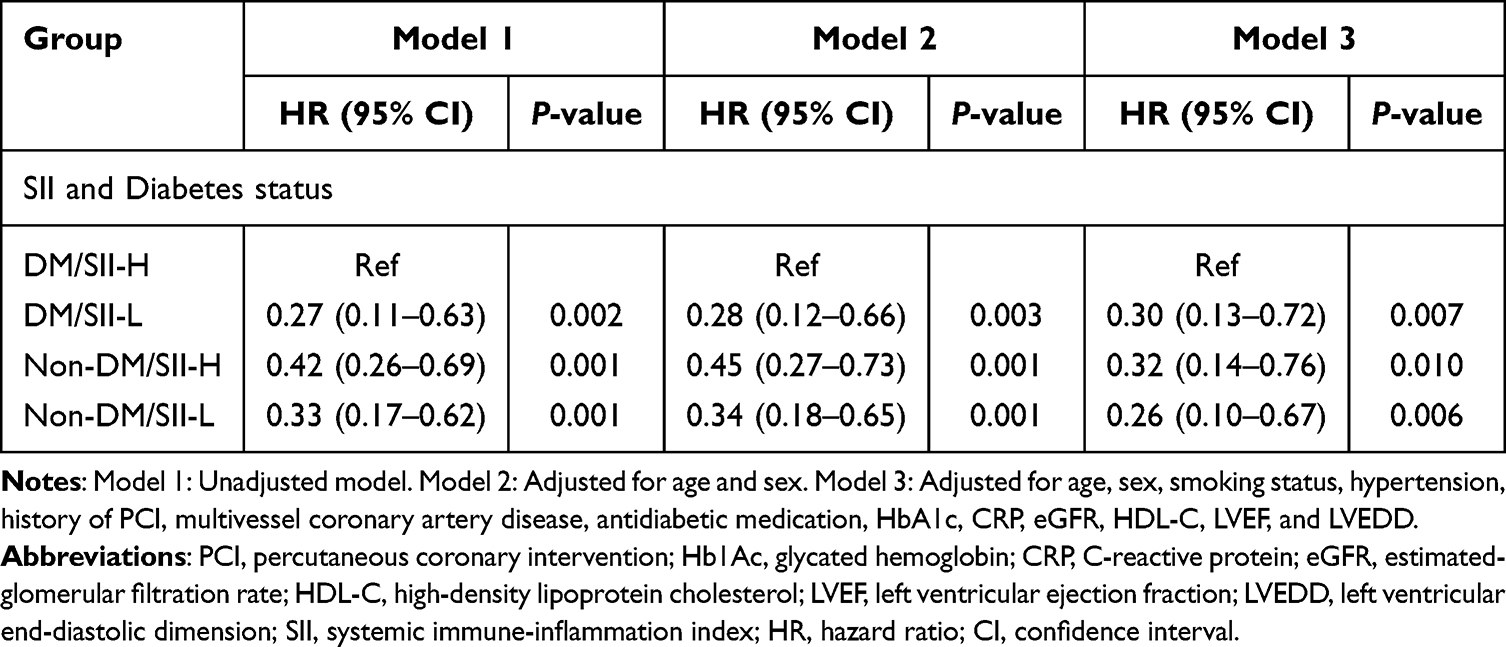 |
Table 3 Association Between risks of Composite Endpoints and Groups Based on SII Levels and Diabetes Status |
Subgroup Analysis
The association between SII level, diabetes status, and MACCEs risk remained consistent across subgroups, including sex, age, smoking status, hypertension, renal impairment, LVEF, prior PCI, and multivessel disease (all P for interaction > 0.05). In contrast, a significant interaction was identified for BMI after full adjustment (P for interaction = 0.036; Figure 4).
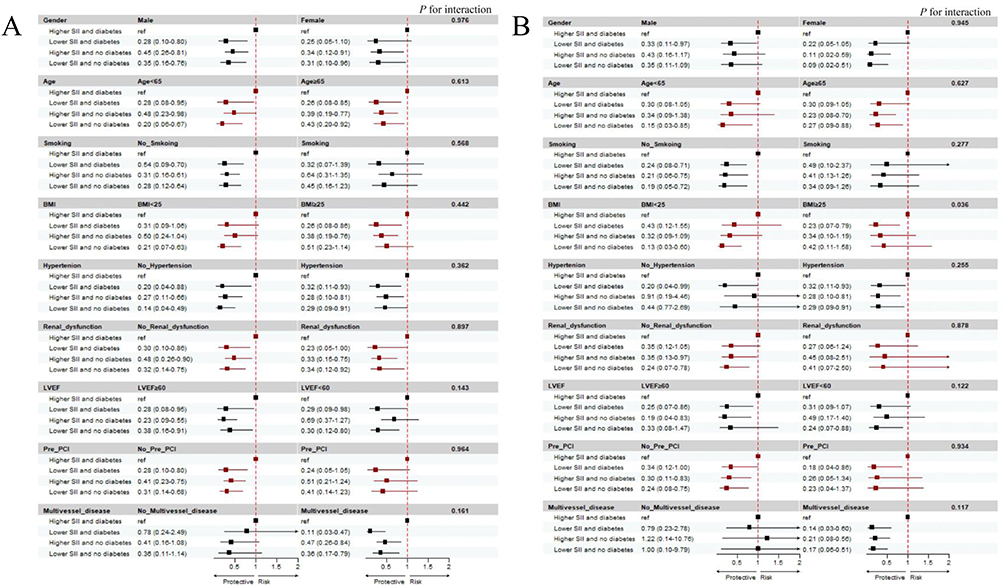 |
Figure 4 Subgroup analysis of the associations among SII, glycemic status, and MACCEs in patients with CCS. (A) Unadjusted; (B) Adjusted. |
Discussion
This study provides evidence that baseline SII, an easily obtainable biomarker derived from the complete blood count, independently predicts MACCEs in patients with CCS. Importantly, SII demonstrated robust predictive value, particularly in diabetic patients, where elevated SII predicted substantially increased clinical risk, even after multivariable adjustment. However, no significant relationship was found among non-diabetic individuals. The coexistence of high SII and diabetes identified a distinct subgroup that represents a high-risk phenotype with substantial inflammatory burden and adverse outcomes. Consequently, SII can serve as a readily available and clinically meaningful biomarker to refine risk stratification in this high-risk subgroup.
Despite advances in revascularization and secondary prevention, a substantial subset of CCS patients continues to experience recurrent ischemic episodes. Growing evidence indicates that persistent low-grade inflammation is a significant determinant of this residual risk, even after optimal control of lipids and glucose. SII integrates three hematologic parameters that collectively reflect the balance between inflammatory activation and immune regulation. Mechanistically, recruited neutrophils release proteolytic enzymes, myeloperoxidase, and neutrophil extracellular traps (NETosis), which injure the vascular endothelium, promote low-density lipoprotein oxidation and foam-cell formation, and accelerate lipid-core expansion and fibrous-cap degradation, thereby contributing to plaque instability.24 Lymphopenia, notably a reduction in CD4⁺ T cells, reflects impaired immune homeostasis that impedes inflammation resolution and endothelial repair.25 Elevated platelet counts promote platelet adhesion and aggregation, fueling thrombus formation; importantly, inflammatory and thrombotic pathways are tightly interconnected, with inflammation amplifying thrombosis under pathological conditions.4 By capturing these integrated elements, SII offers a holistic measure of vascular inflammatory activity.
Accumulating evidence supports the prognostic utility of SII across the coronary artery disease spectrum. Babes et al retrospectively showed that elevated SII significantly correlated with worse cardiovascular events and mortality in ACS, and further improved the predictive performance of the GRACE score.26 Zhu et al demonstrated significantly elevated SII levels among ST-segment elevation myocardial infarction (STEMI) patients experiencing unfavorable outcomes.27 Orhan et al identified that higher SII independently predicted adverse hospital outcomes and poorer future survival in elderly non-STEMI (NSTEMI) patients, after adjusting for age and key comorbidities.28 This present study extends these findings to the chronic phase of coronary disease. Our study confirmed that higher SII, whether analyzed dichotomously or as a continuous variable, was significantly correlated with elevated MACCEs risk in CCS patients, and this association remained robust after multivariable adjustment. These results reinforce SII as a robust prognostic tool across the diverse clinical manifestations of coronary artery disease, encompassing both acute presentations and chronic coronary syndromes. Importantly, existing evidence suggests that systemic inflammation may indirectly contribute to myocardial damage through several interconnected mechanisms, such as cytokine-mediated cellular toxicity, microvascular dysfunction, and increased cardiomyocyte membrane permeability.29,30 However, given the incomplete data and the limited dispersion of the available values in our cohort, further prospective studies with systematic biomarker collection are needed to validate this.
Moreover, this work identified that SII interacted significantly with glycemic status. Previous studies indicate that diabetes amplifies the prognostic impact of SII. As evidenced by Luo et al, an elevated SII independently predicted mortality in myocardial infarction, with the effect being most prominent among diabetic patients.15 Similarly, Cao et al demonstrated that high SII levels markedly increased the risk of mortality and rehospitalization in heart failure with preserved ejection fraction (HFpEF), particularly within the high-risk diabetic subgroup.14 Consistently, elevated SII independently predicts MACCEs after PCI in ACS patients with diabetes.31 Chronic hyperglycemia triggers a pathogenic cascade featuring the accumulation of advanced glycation end-products, activation of the NF-κB pathway and NLRP3 inflammasome, increased interleukin-6 and interleukin-1β release, and excessive generation of reactive oxygen species. These abnormalities amplify insulin resistance and perpetuate a vicious cycle of metabolic inflammation.32 Critically, hyperglycemia directly primes neutrophils to undergo NETosis through NADPH oxidase-dependent ROS production, providing a platelet-adhesive scaffold that accelerates atherosclerosis and destabilizes plaque. Simultaneously, hyperglycemia increases platelet reactivity through nonenzymatic glycation of membrane proteins, activation of protein kinase C, and mitochondrial superoxide overproduction, thereby elevating platelet counts and baseline activation. The coexistence of hyperglycemia-induced neutrophil priming and platelet hyperactivity creates a self-perpetuating cycle of inflammation and thrombosis that is quantitatively captured by elevated SII, explaining its enhanced prognostic value in diabetic patients.17,33,34 By contrast, non-diabetic patients generally carry fewer cardiovascular risk factors, making their prognosis less susceptible to milder inflammatory or metabolic perturbations. In addition, non-diabetic patients typically exhibit lower basal inflammatory tone, a narrower dynamic range of inflammation, and lower event density, which may limit the ability of inflammatory biomarkers like SII to demonstrate significant associations with clinical outcomes.35 These mechanistic differences could explain the divergent prognostic value of SII in diabetic versus non-diabetic patients.
Consistent with previous reports, this study confirmed the potential predictive utility of SII for worse outcomes in CCS, with its prognostic value markedly amplified among diabetics. Restricted cubic spline analysis further revealed a linear increase in the risk of MACCEs with rising SII among diabetic patients, without an apparent threshold effect. The combination of high SII and diabetes is a strong, independent predictor of MACCEs beyond traditional risk factors. Collectively, by capturing the systemic inflammation burden, SII serves as a powerful tool for prognostic refinement in diabetic CCS patients, enabling more accurate risk stratification and earlier identification of individuals at the highest risk.
Notably, in our study, MACCEs included cardiovascular death, non-fatal MI, HF, ischemia-driven revascularization, and stroke, which differ in clinical severity, pathophysiological relation to inflammation, and susceptibility to treatment decision-making. Prior work has described that, in cardiovascular composite end points, the overall signal is often driven disproportionately by more frequent and less severe component events.36 Supplementary analyses indicated that the overall association between SII and MACCEs was influenced mainly by the soft endpoint component, particularly ischemia-driven revascularization, whereas the analyses of individual hard endpoints were limited by the small number of events, which needs to be further addressed.
The prognostic synergy between SII and diabetes highlights the importance of targeting both inflammation and metabolic dysfunction. Beyond glycemic and lipid control, therapies with anti-inflammatory or cardiometabolic benefits, such as colchicine, interleukin-1β inhibitors, GLP-1 receptor agonists, or SGLT2 inhibitors, may be of particular importance in patients with elevated SII; however, their potential influence on the association between SII and clinical outcomes requires further investigation.7–9
Obesity is known to impair insulin sensitivity, increase free fatty acid turnover, enhance basal sympathetic activity, and promote a pro-thrombotic state, thereby elevating the risk of coronary artery disease and adverse cardiovascular events.37 Nevertheless, previous studies have described an “obesity paradox” in patients with type 2 diabetes or cardiovascular disease, wherein overweight or mildly obese individuals appear to experience more favorable outcomes.38,39 Notably, this work observed that the combined impact of high SII and diabetes was most pronounced in patients with BMI < 25 kg/m2 (P for interaction = 0.036). However, this finding should be interpreted prudently. BMI is a crude anthropometric measure that neither distinguishes fat from lean mass, nor captures regional fat distribution—particularly visceral adiposity, which more closely correlates with metabolic and cardiovascular dysfunction. In addition, disease progression, cardiorespiratory fitness, duration of obesity, and differences in clinical treatment may all modulate the prognostic implications of BMI.40–42 Therefore, although the effect appeared more pronounced in patients with lower BMI, this finding should be interpreted cautiously. Future studies using more precise indices of adiposity—such as waist circumference, hip circumference, or waist-to-hip ratio—are needed to clarify the physiological mechanisms underlying the obesity paradox.
Clinical Implications
These findings have potential implications for clinical risk assessment. SII, calculated from a routine complete blood count, offers an inexpensive and accessible measure of residual inflammatory risk in CCS. It may serve as an adjunct biomarker to complement conventional risk markers such as hs-CRP. Incorporating SII into clinical assessment may help identify CCS patients, particularly those with diabetes, who remain vulnerable despite guideline-directed therapy.
Limitations
This research has certain limitations. First, as a single-center, retrospective observational study, it cannot establish causality and may be influenced by selection bias and unmeasured confounders. These findings should be confirmed in prospective, multicenter cohorts before broader application. Moreover, given the clinically heterogeneous components and the limited number of individual hard events, further studies are needed to explore the association between SII and clinical endpoints. In addition, SII was assessed only at a single time point, which precluded assessment of the prognostic value of SII trajectories. Third, BMI was used as a crude adiposity indicator; more accurate assessments of body composition are needed in future studies to elucidate the underlying physiology. Moreover, cardiac biomarkers such as troponin T and NT-proBNP were available only in a subset of patients and were not collected systematically; the correlation between SII and biomarkers of myocardial damage should be further explored in future prospective studies with more complete data collection and a more rigorous study design. Finally, as an observational study, this work demonstrates only an association between SII and prognosis. Mechanistic studies are required to clarify how SII contributes to plaque progression, rupture, and immune-thrombosis.
Conclusions
SII independently predicts MACCEs in CCS, and this risk is further amplified by the presence of diabetes. Hyperglycemia drives neutrophil activation and NETosis, as well as platelet hyperreactivity, all of which contribute to the pathogenesis of atherothrombosis in diabetic patients. This interaction underscores the central roles of inflammation and metabolic dysfunction in disease progression. As a low-cost and accessible biomarker, SII may enhance risk stratification in this high-risk phenotype. BMI is commonly used as an obesity measure; its prognostic value is complicated by the “obesity paradox”, which may be driven by visceral adiposity. Future studies using more precise adiposity indices are needed to clarify this relationship. Meanwhile, some clinical trials are required to evaluate the incremental prognostic value of SII to further validate its applicability.
Data Sharing Statement
The datasets used during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Nanjing Drum Tower Hospital (approval number: 2021-531-02). Verbal informed consent was obtained from all individual participants included in the study.
Consent for Publication
The manuscript was approved by all authors for publication.
Author Contributions
Luwa Gao: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing–original draft, Writing–review & editing; Xinbo Bai: Conceptualization, Investigation, Software, Writing – original draft, Writing–review & editing; Yuqi Zhao: Investigation, Data curation, Formal analysis, Writing–original draft; Xue Bao: Formal analysis, Methodology, Software, Writing – original draft; Jing Lu: Data curation, Formal analysis, Writing–original draft; Haishen Yu: Data curation, Validation, Writing–original draft; Biao Xu: Conceptualization, Resources, Supervision, Funding acquisition, Project administration, Writing–review & editing; Jianzhou Chen: Conceptualization, Formal analysis, Methodology, Visualization, Software, Writing–review & editing; Lina Kang: Conceptualization, Resources, Funding acquisition, Project administration, Supervision, Writing–review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Luwa Gao and Xinbo Bai contributed equally to this work and share first authorship. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Program of China (2024YFF0508604), the National Natural Science Foundation of China (82570460), and the Natural Science Foundation of Jiangsu Province (BK20222002).
Disclosure
The authors declare that they have no competing interests in this article.
References
1. Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415–14. doi:10.1093/eurheartj/ehae177
2. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401(10384):1293–1301. doi:10.1016/s0140-6736(23)00215-5
3. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. doi:10.1056/nejmra043430
4. Waksman R, Merdler I, Case BC, et al. Targeting inflammation in atherosclerosis: overview, strategy and directions. EuroIntervention. 2024;20(1):32–44. doi:10.4244/EIJ-D-23-00606
5. Bay B, Tanner R, Gao M, et al. Residual cholesterol and inflammatory risk in statin-treated patients undergoing percutaneous coronary intervention†. Eur Heart J. 2025;46(32):3167–3177. doi:10.1093/eurheartj/ehaf196
6. Ridker PM. From C-reactive protein to interleukin-6 to interleukin-1: moving upstream to identify novel targets for atheroprotection. Circ Res. 2016;118(1):145–156. doi:10.1161/circresaha.115.306656
7. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383(19):1838–1847. doi:10.1056/NEJMoa2021372
8. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
9. Tardif JC, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
10. Oliva A, Vogel B, Sartori S, et al. Association of neutrophil-to-lymphocyte ratio with clinical outcomes after percutaneous coronary intervention. Eur J Prev Cardiol. 2025. doi:10.1093/eurjpc/zwaf597
11. He J, Bian X, Song C, et al. High neutrophil to lymphocyte ratio with type 2 diabetes mellitus predicts poor prognosis in patients undergoing percutaneous coronary intervention: a large-scale cohort study. Cardiovasc Diabetol. 2022;21(1):156. doi:10.1186/s12933-022-01583-9
12. Kalhor P, Mahmoudi Hamidabad N, Hellou E, et al. Association of monocyte-to-lymphocyte ratio with coronary endothelial dysfunction and cardiovascular events in patients with angina and nonobstructive coronary artery disease. Atherosclerosis. 2025;410:120539. doi:10.1016/j.atherosclerosis.2025.120539
13. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.Ccr-14-0442
14. Mohammed A-Q, Luo Y, Chen Y, et al. Association of systemic immune-inflammation index with adverse outcomes in heart failure and preserved ejection fraction. J Transl Med. 2025;23(1):957. doi:10.1186/s12967-025-06964-8
15. Luo J, Qin X, Zhang X, et al. Prognostic implications of systemic immune-inflammation index in myocardial infarction patients with and without diabetes: insights from the NOAFCAMI-SH registry. Cardiovasc Diabetol. 2024;23(1):41. doi:10.1186/s12933-024-02129-x
16. Ekizler F, Kaplan E, Cay S, et al. Usefulness of the systemic immune inflammation index to predict atrial fibrillation recurrence after cryoablation. EP Europace. 2023;25(Supplement_1). doi:10.1093/europace/euad122.679
17. Li Y, Liu Y, Liu S, et al. Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Signal Transduct Target Ther. 2023;8(1):152. doi:10.1038/s41392-023-01400-z
18. Guariguata L, Whiting DR, Hambleton I, et al. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137–149. doi:10.1016/j.diabres.2013.11.002
19. Pradhan AD, Manson JE, Rifai N, et al. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 2001;286(3):327–334. doi:10.1001/jama.286.3.327
20. Sharif S, Van der Graaf Y, Cramer MJ, et al. Low-grade inflammation as a risk factor for cardiovascular events and all-cause mortality in patients with type 2 diabetes. Cardiovasc Diabetol. 2021;20(1):220. doi:10.1186/s12933-021-01409-0
21. Bray JJH, Foster-Davies H, Salem A, et al. Glucagon-like peptide-1 receptor agonists improve biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis of randomised controlled trials. Diabetes Obesity Metab. 2021;23(8):1806–1822. doi:10.1111/dom.14399
22. Yoo TT, Baek IH, Stoletniy L, et al. Impact of sodium–glucose transport protein-2 (SGLT2) inhibitors on the inflammasome pathway in acute myocardial infarction in type 2 diabetes mellitus: a comprehensive review. Cardiovasc Diabetol. 2025;24(1). doi:10.1186/s12933-025-02777-7
23. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Internal Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
24. Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17(6):327–340. doi:10.1038/s41569-019-0326-7
25. Swirski FK, Nahrendorf M. Leukocyte behavior in atherosclerosis, myocardial infarction, and heart failure. Science. 2013;339(6116):161–166. doi:10.1126/science.1230719
26. Babes EE, Radu AF, Cretu NA, et al. Risk stratification in acute coronary syndromes: the systemic immune-inflammation index as prognostic marker. Med Sci. 2025;13(3). doi:10.3390/medsci13030116
27. Zhu Y, He H, Qiu H, et al. Prognostic value of systemic immune-inflammation index and NT-proBNP in patients with acute ST-elevation myocardial infarction. Clin Interv Aging. 2023;18:397–407. doi:10.2147/cia.S397614
28. Orhan AL, Şaylık F, Çiçek V, et al. Evaluating the systemic immune-inflammation index for in-hospital and long-term mortality in elderly non-ST-elevation myocardial infarction patients. Aging Clin Exper Res. 2022;34(7):1687–1695. doi:10.1007/s40520-022-02103-1
29. Erbay I, Kokturk U, Eris Gudul N, et al. Prognostic role of systemic immune-inflammation index versus other cardiac markers in acute myocarditis in young adults. Biomarker Med. 2024;18(20):889–897. doi:10.1080/17520363.2024.2403321
30. Ostermann M, Ayis S, Tuddenham E, et al. Cardiac troponin release is associated with biomarkers of inflammation and ventricular dilatation during critical illness. Shock. 2017;47(6):702–708. doi:10.1097/shk.0000000000000811
31. Zhang L, Wang S, Wang Y, et al. Prognostic value of systemic immune-Inflammatory index in patients with diabetes mellitus and acute coronary syndrome after percutaneous coronary intervention: a prospective cohort study. BMC Cardiovasc Disord. 2025;25(1):612. doi:10.1186/s12872-025-04990-4
32. Weinberg Sibony R, Segev O, Dor S, et al. Overview of oxidative stress and inflammation in diabetes. J Diabetes. 2024;16(10):e70014. doi:10.1111/1753-0407.70014
33. Wong SL, Demers M, Martinod K, et al. Diabetes primes neutrophils to undergo NETosis, which impairs wound healing. Nat Med. 2015;21(7):815–819. doi:10.1038/nm.3887
34. Poznyak A, Grechko AV, Poggio P, et al. The diabetes mellitus-atherosclerosis connection: the role of lipid and glucose metabolism and chronic inflammation. Int J Mol Sci. 2020;21(5). doi:10.3390/ijms21051835
35. Bao X, Borné Y, Johnson L, et al. Comparing the inflammatory profiles for incidence of diabetes mellitus and cardiovascular diseases: a prospective study exploring the ‘common soil’ hypothesis. Cardiovasc Diabetol. 2018;17(1):87. doi:10.1186/s12933-018-0733-9
36. Shaikh A, Ochani RK, Khan MS, et al. Contribution of individual components to composite end points in contemporary cardiovascular randomized controlled trials. Am Heart J. 2020;230:71–81. doi:10.1016/j.ahj.2020.09.001
37. Lavie CJ, Arena R, Alpert MA, et al. Management of cardiovascular diseases in patients with obesity. Nat Rev Cardiol. 2018;15(1):45–56. doi:10.1038/nrcardio.2017.108
38. Thakker J, Khaliq I, Ardeshna NS, et al. The obesity paradox of cardiovascular outcomes in patients with diabetes mellitus. Curr Diabetes Rep. 2025;25(1):35. doi:10.1007/s11892-025-01592-4
39. Pagidipati NJ, Zheng Y, Green JB, et al. Association of obesity with cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease: insights from TECOS. Am Heart J. 2020;219:47–57. doi:10.1016/j.ahj.2019.09.016
40. Simati S, Kokkinos A, Dalamaga M, et al. Obesity paradox: fact or fiction? Curr Obes Rep. 2023;12(2):75–85. doi:10.1007/s13679-023-00497-1
41. Tutor AW, Lavie CJ, Kachur S, et al. Updates on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis. 2023;78:2–10. doi:10.1016/j.pcad.2022.11.013
42. Yang L, Ge Y, Zhu Q, et al. The combination of fat distribution and bmi redefines obesity: result from NHANES. J Cachexia Sarcopenia Muscle. 2025;16(4):e70013. doi:10.1002/jcsm.70013
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Associations of Inflammation with Risk of Cardiovascular and All-Cause Mortality in Adults with Hypertension: An Inflammatory Prognostic Scoring System
Cheang I, Zhu X, Lu X, Yue X, Tang Y, Gao R, Liao S, Yao W, Zhou Y, Zhang H, Yiu KH, Li X
Journal of Inflammation Research 2022, 15:6125-6136
Published Date: 8 November 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
Association of the Systemic Immune-Inflammation Index with Outcomes in Acute Coronary Syndrome Patients with Chronic Kidney Disease
Shi S, Kong S, Ni W, Lu Y, Li J, Huang Y, Chen J, Lin K, Li Y, Ke J, Zhou H
Journal of Inflammation Research 2023, 16:1343-1356
Published Date: 27 March 2023
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
He J, Song C, Zhang R, Yuan S, Li J, Dou K
Journal of Inflammation Research 2023, 16:5439-5450
Published Date: 20 November 2023