")
Back to Journals » Journal of Inflammation Research » Volume 16
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
Authors He J, Song C, Zhang R, Yuan S, Li J, Dou K
Received 28 July 2023
Accepted for publication 10 November 2023
Published 20 November 2023 Volume 2023:16 Pages 5439—5450
DOI https://doi.org/10.2147/JIR.S428734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Jining He,1– 3 Chenxi Song,1– 3 Rui Zhang,1– 4 Sheng Yuan,1– 3 Jianjun Li,1,3 Kefei Dou1– 4
1Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3State Key Laboratory of Cardiovascular Disease, Beijing, People’s Republic of China; 4National Clinical Research Center for Cardiovascular Diseases, Beijing, People’s Republic of China
Correspondence: Kefei Dou, Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, 167A Beilishi Road, Xi Cheng District, Beijing, 100037, People’s Republic of China, Tel +86-13801032912, Fax +86-10-6831-3012, Email [email protected] Jianjun Li, Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, 167A Beilishi Road, Xi Cheng District, Beijing, 100037, People’s Republic of China, Email [email protected]
Purpose: Neutrophil to lymphocyte ratio (NLR), a novel inflammatory biomarker, has been shown to positively predict prognosis independent of high-sensitivity C-reactive protein (hsCRP) in patients with coronary artery disease (CAD). This study aimed to use discordance analysis to evaluate the effectiveness of NLR and hsCRP to predict adverse events in patients with stable CAD.
Patients and Methods: This observational cohort study included 7827 consecutive CAD patients at Fuwai Hospital from March 2011 to April 2017. Discordant NLR with hsCRP was defined by the highest quartiles and medians. The primary endpoint was major adverse cardiovascular and cerebrovascular events (MACCEs), including cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and unplanned revascularization.
Results: During a median 36-month follow-up, 624 (8.0%) MACCEs occurred. Compared with the lowest NLR quartile, a significantly higher risk of MACCEs was observed in the highest NLR quartile after adjusting for confounding factors (hazard ratio [HR], 1.36; 95% confidence interval [CI], 1.09– 1.71). High NLR and low hsCRP discordance were also associated with an increased risk of MACCEs in the fully adjusted model (HR, 1.39; 95% CI, 1.05– 1.84).
Conclusion: This study demonstrated that discordantly elevated NLR levels were associated with a greater risk of adverse clinical events in patients with stable CAD, suggesting the potential clinical significance of NLR as a goal of inflammatory risk management.
Keywords: coronary artery disease, high-sensitivity C-reactive protein, inflammation, neutrophil to lymphocyte ratio, prognosis
Introduction
Inflammation plays a crucial role in the development and progression of coronary artery disease (CAD).1 As a benchmark biomarker for inflammatory risk, high-sensitivity C-reactive protein (hsCRP) is positively associated with cardiovascular events in both primary and secondary prevention.2,4 In the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) trial, the greatest clinical benefit accrued among participants who attained the lowest tertile of hsCRP levels, whereas individuals with on-treatment hsCRP levels in the highest tertile had comparable clinical outcomes relative to placebo.3–5 Such observations further support hsCRP as a potential biomarker to guide therapeutic decision-making.
Contemporary studies not only increase interest in conventional inflammatory biomarkers including hsCRP but also in awareness of a simple biomarker widely and readily available to the clinical community.5–7 One such biomarker is neutrophil to lymphocyte ratio (NLR), which is derived from the complete blood count.8,9 NLR integrated information from both innate immunity, predominately due to neutrophils, and adaptive immune response, supported by lymphocytes. Increasing studies have demonstrated that baseline NLR is positively associated with cardiovascular events and mortality.9,10 Of note, data from five large randomized clinical trials, including the CANTOS trial, demonstrated that baseline NLR modestly correlated with hsCRP, interleukin (IL)-6 and fibrinogen, and it could consistently and independently predict cardiovascular events and death after adjusting the effect of hsCRP.9 These findings indicated that NLR provide additional insights into the nature of the inflammatory atherosclerotic process, which is not reflected by cytokines or hsCRP. Additionally, NLR has been shown to be stable over time and to be responsive to anti-inflammatory therapy, which may make it an alternative or complementary inflammatory biomarker in clinical practice.9–11
Recently, a previous study by Wada et al12 has shown that the 5-year adverse outcomes of CAD patients with low-grade hs-CRP levels could be independently predicted by increased NLR level, suggesting that NLR could be useful for risk stratification of CAD patients with low inflammatory marker levels. However, to date, there are no studies comparing the predictive values of the NLR levels with hsCRP levels for the risk of adverse clinical events in patients with stable CAD. Accordingly, the objective of this study is to use discordance analysis to investigate the joint or discordant association of NLR and hsCRP levels with adverse clinical events in patients with stable CAD.
Materials and Methods
Study Design
This study was a single-center, observational cohort study. Between March 2011 and April 2017, a total of 9180 patients who underwent coronary angiography examination due to angina-like chest pain or positive non-invasive tests (such as treadmill exercise test or coronary computed tomography angiography) were consecutively recruited at the Fuwai Hospital, Chinese Academy of Medical Sciences. Patients meeting the following criteria were included:1 aged of equal to or more than 18 years,2 diagnosed with CAD. Patients meeting the following criteria were excluded:1 patients with missing detailed information (missing Complete blood counts and/or hsCRP measurements),2 patients with severe hepatic or kidney dysfunction,3 patients with systematic inflammatory disease,4 patients with malignant tumor,5 patients with hematological disorder,6 patients with acute infection,7 patients with acute coronary syndrome (ACS), and8 patients lost to follow-up (Figure 1). ACS was determined according to elevated myocardial enzyme levels, typical electrocardiogram changes, positive findings by angiography and medical history.
This study complied with the Declaration of Helsinki and followed the guidelines for reporting cohort studies of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). The STROBE checklist was provided in the Supplementary Material. The study protocol was approved by Ethics Committee of Fuwai Hospital, Chinese Academy of Medical Sciences (IRB2012-BG-006). All study patients provided written informed consent before enrollment.
Study Endpoints and Follow‐Up
Study patients were routinely followed-up at 6-month intervals through clinical visits and/or telephone contact by well-trained coordinators who were blinded to the aims of this study. All clinical events were carefully adjudicated by two independent and experienced cardiologists. Conflicts were resolved by consulting a third experienced cardiologist. The primary endpoint was major cardiovascular and cerebrovascular events (MACCEs), defined as a composite of cardiovascular (CV) death, non-fatal myocardial infarction (MI), non-fatal stroke, and unplanned revascularization. The secondary endpoints of interest were individual components of MACCEs. Cardiovascular death was confirmed by medical records, death certificates, and information provided by the relatives. Non-fatal MI was diagnosed by positive cardiac troponins together with typical chest pain or typical electrocardiogram serial changes. Non-fatal Stroke was defined by persistence of neurological symptoms with acute cerebral infarction as demonstrated by computed tomography and/or magnetic resonance imaging. Unplanned revascularization was defined as any percutaneous coronary intervention or surgical bypass excluding staged procedures.
Clinical Assessment
Baseline information on personal health habits, demographics, medications, and medical history was collected from each participant. According to the American Diabetes Association criteria, diabetes was determined by a fasting blood glucose (FBG) ≥7.0 mmol/L, or 2-h plasma glucose (PG) ≥11.1 mmol/L, or HbA1c ≥6.5%, or currently using hypoglycemic drugs.13 Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, or currently using antihypertensive drugs. Dyslipidemia was defined by triglyceride ≥1.7 mmol/L, total cholesterol ≥5.2 mmol/L, LDL-C ≥3.4 mmol/L, or high-density lipoprotein cholesterol ≤1.0 mmol/L, and/or use of lipid-lowering agents. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared.
Laboratory Tests
On admission, venous blood samples were collected from each participant after at least 12-h fasting and were tested at clinical chemistry department of our hospital. Complete blood counts (including WBC, neutrophils, and lymphocytes) were performed using an automatic blood cell analyzer (XT-1800i; Sysmex Corporation). The NLR value was calculated using the following formula: neutrophils (×109/L)/lymphocytes (×109/L). The hsCRP level was determined using immunoturbidimetry (Beckmann Assay, Bera, California). The HbA1c level was measured by Tosoh Automated Glycohemoglobin Analyser (HLC-723G8, Tokyo, Japan). All other laboratory measurements were performed according to the standard biochemical techniques. Left ventricular ejection fraction (LVEF) was measured using the modified Simpson’s method.
Statistical Analysis
Continuous variables were presented as mean with standard deviation, and categorical variables were expressed as count with percentage. Differences were estimated by Student’s t-test, Mann–Whitney U-test, Chi-square test, and Fisher’s exact test, as appropriate. Distribution of variables was determined by Kolmogorov–Smirnov test. The correlation between NLR and other laboratory parameters was evaluated by Spearman correlation test. Patients were then assigned into the NLR and hsCRP groups according to the quartiles of each measure with the whole population. According to the highest quartile of NLR levels (<2.62 or ≥2.62) and the median of hsCRP levels (<1.30 or ≥1.30 mg/L), patients were subsequently divided into 4 mutually exclusive concordance/discordance groups, as follows: low/low (less than the highest quartile of NLR and less than the median of hsCRP), high/low (greater than or equal to the highest quartile of NLR and less than the median of hsCRP), low/high (less than the highest quartile of NLR and greater than or equal to the median of hsCRP), high/high (greater than or equal to the highest quartile of NLR and greater than or equal to the median of hsCRP). Discordance was defined as high NLR levels and hsCRP levels being low, or vice versa.
In survival analysis, linearity relationship of hsCRP and NLR for the MACCE risk was illustrated by restricted cubic splines (RCS) analysis. Cumulative incidence of adverse events among groups were presented by Kaplan–Meier curves and compared by Log rank test. Patients were censored at the time of death or last contact, whichever came first. The association of NLR and hsCRP levels with study endpoints was explored in univariable and multivariable Cox proportional hazard models. Hazard ratios (HRs) with 95% confidence intervals (CIs) were presented. In multivariable analysis, age, male sex, diabetes, hypertension, previous CABG, previous stroke, creatinine, TG, LVEF, statins use, and aspirin use were included based on their statistical significance in univariable model or clinical importance. Moreover, sensitivity analysis was performed to confirm our findings by classifying 4 concordance/discordance groups using hsCRP guideline-guide target cutoffs of 2 mg/L.14 Furthermore, subgroup analyses were performed to assess the association of 4 concordance/discordance groups with MACCEs in specific subsets. Finally, mediation analysis was performed to evaluate the proportional contribution of NLR and hsCRP on the associations of the counterparts with MACCE risk. Mediation analysis models were adjusted for the same set of confounders as in the multivariable model mentioned above. A two-tailed P value <0.05 indicated statistical significance. All statistical analyses were performed with R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
Among 9180 consecutively recruited patients, we excluded 293 patients with missing detailed information, 56 patients due to severe hepatic or kidney dysfunction, systematic inflammatory disease, malignant tumor, hematological disorder, or acute infection. Besides, we excluded 869 patients with acute coronary syndrome according to elevated myocardial enzyme levels, typical electrocardiogram changes, positive findings by angiography and medical history. Furthermore, 181 patients lost to follow up. Eventually, a total of 7827 patients were included in final analysis (Figure 1).
Generally, a total of 7827 CAD patients (58.02±10.16 years, 70.6% male) were consecutively included in this study. Baseline characteristics of patients with and without MACCEs are presented in Table 1. Patients experiencing any component of MACCEs tended to be older, with higher prevalence of diabetes and prior CABG compared to those in non-MACCE group (all P < 0.05). In addition, higher levels of HbA1c, creatinine, NLR, hsCRP, and lower level of LVEF were noticed in patients with unfavorable prognosis (all P < 0.05). Moreover, there was less use of statins, aspirin, and CCB in patients who suffered from MACCEs than those not (all P < 0.05).
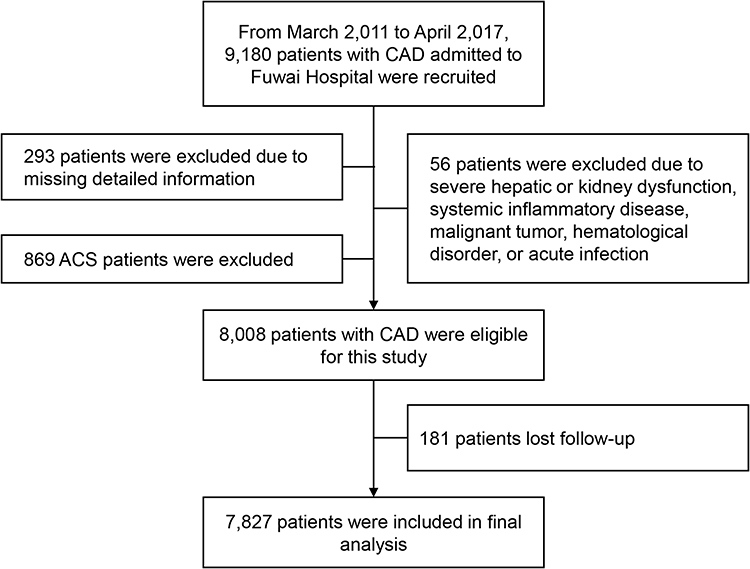 |
Figure 1 Study flowchart. Abbreviations: CAD, coronary artery disease; ACS, acute coronary syndrome. |
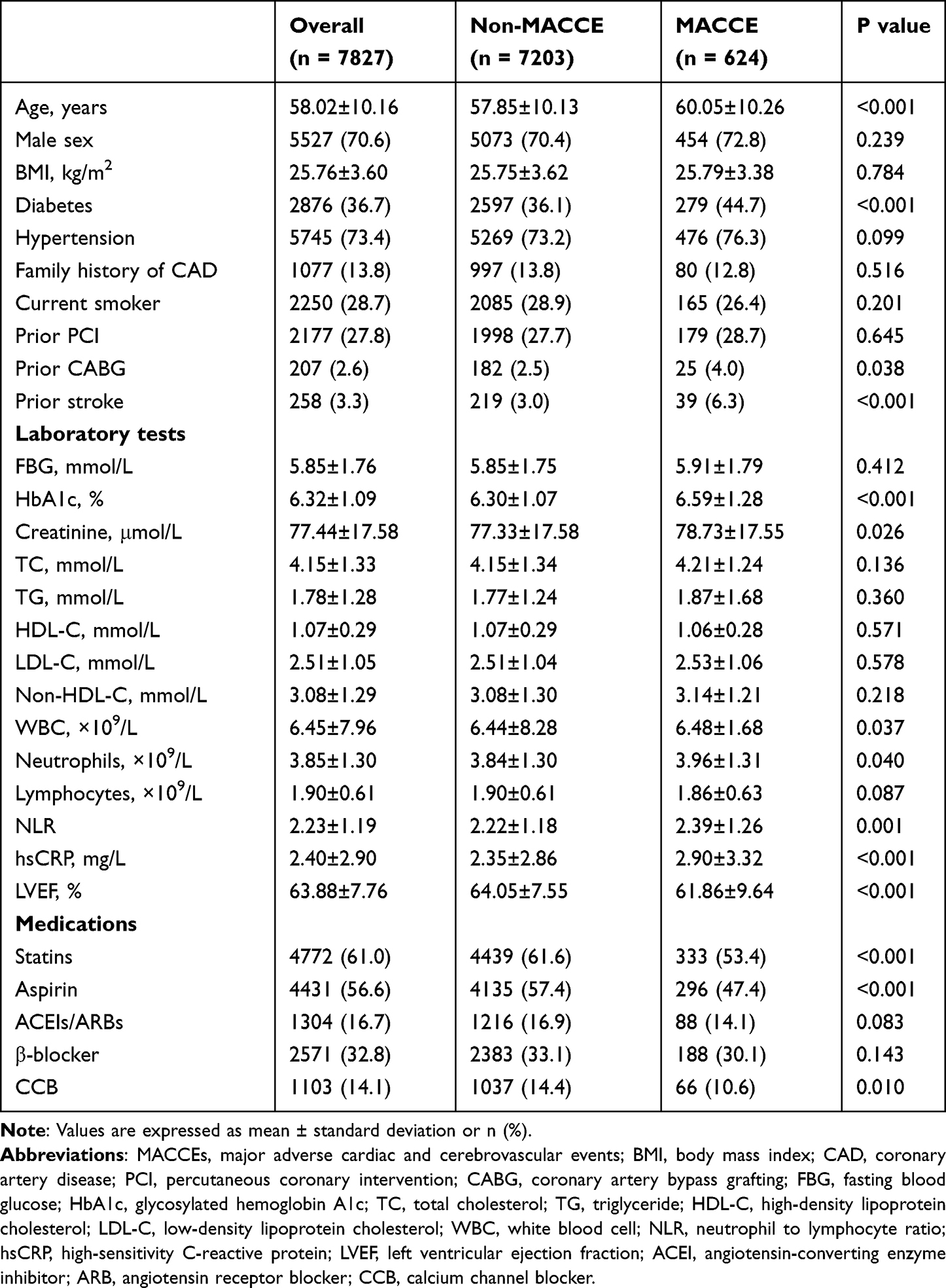 |
Table 1 Baseline Characteristics According to Incidence of MACCEs |
The baseline characteristics across 4 concordance/discordance groups according to low or high NLR and hsCRP levels are listed in Table 2. There were 803 (10.3%) patients had a discordantly high NLR levels. Significant differences were observed regarding age, sex, diabetes, hypertension, family history, smoking status, prior PCI, prior CABG, prior stroke, and medications (statins, aspirin, ACEIs/ARBs, and β-blocker) across 4 groups (all P < 0.05). Moreover, patients with high NLR levels were more likely to have higher levels of FBG, HbA1c, and creatinine (all P < 0.05). Among patients with low hsCRP levels, those with increased NLR values were older and more likely to be male with more prevalent hypertension and prior stroke and less prevalent family history of CAD and current smoker. Meanwhile, there were higher levels of FBG, creatinine, WBC and neutrophils, and lower levels of TC, TG, LDL-C and lymphocytes in those with high NLR levels (all P < 0.05). In addition, among patients with high hsCRP levels, those with increased NLR values were also older and more likely to be male with a higher prevalence of previous PCI or CABG. And these patients had higher levels of creatinine, neutrophils and hsCRP levels, and lower TC, TG, LDL-C and LVEF levels (all P < 0.05). The correlation analysis showed that NLR levels are modestly and positively correlated with hsCRP levels (r = 0.181, P < 0.001) (Supplementary Table 1).
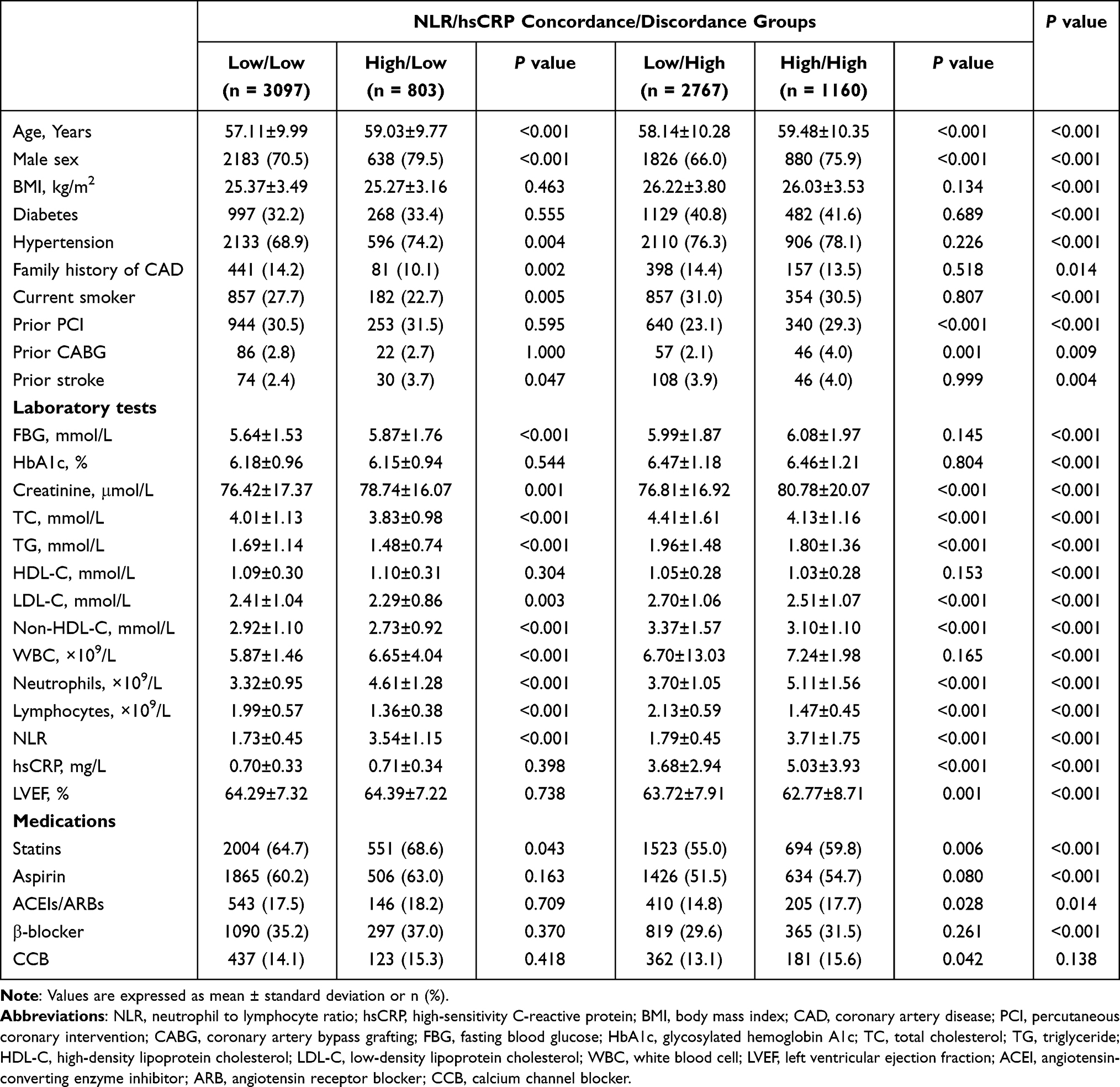 |
Table 2 Baseline Characteristics of the Concordance/Discordance Groups According to Low or High NLR and hsCRP Categories |
Association of Inflammatory Status with Adverse Clinical Events
During a median follow-up of 36 months, 107 (1.4%) CV death, 79 (1.0%) non-fatal MI, 155 (2.0%) non-fatal stroke, 330 (4.2%) unplanned revascularization, and 624 (8.0%) MACCEs was documented.
Kaplan–Meier analysis showed that patients with hsCRP levels in the third and fourth quartile had a higher probability of MACCEs compared with those with hsCRP levels in the lowest quartile (P < 0.001, Figure 2A), and that subjects in fourth quantile of NLR had a higher probability of MACCEs than those in first quantile of NLR (P = 0.002, Figure 2B). The crude and adjusted HRs and 95% CIs of MACCEs according to hsCRP or NLR quantiles are listed in Table 3. Patients with Q3 or Q4 of hsCRP or Q4 of NLR had significantly higher risk of MACCEs (adjusted HR, 1.29; 95% CI, 1.02–1.64; adjusted HR, 1.38; 95% CI, 1.09–1.74; adjusted HR, 1.36; 95% CI, 1.09–1.71; respectively, all P < 0.05) after adjusting confounding factors including age, male sex, diabetes, hypertension, previous CABG, previous stroke, creatinine, TG, LVEF, statins, and aspirin. RCS analysis suggested that there was a linear relationship of hsCRP and NLR with MACCEs after adjusting confounding factors (both P for non-linearity >0.05) (Supplementary Figure 1).
 |
Figure 2 Kaplan–Meier (KM) curves for MACCEs according to different inflammatory biomarkers levels (A) KM curves for MACCEs according to hsCRP levels; (B) KM curves for MACCEs according to NLR levels MACCEs were defined as a composite of CV death, non-fatal MI, non-fatal stroke, and unplanned revascularization. Abbreviations: MACCE, major adverse cardiovascular and cerebrovascular events; CV death, cardiovascular death; MI, myocardial infarction; NLR, neutrophil to lymphocyte ratio; hsCRP, high-sensitivity C-reactive protein. |
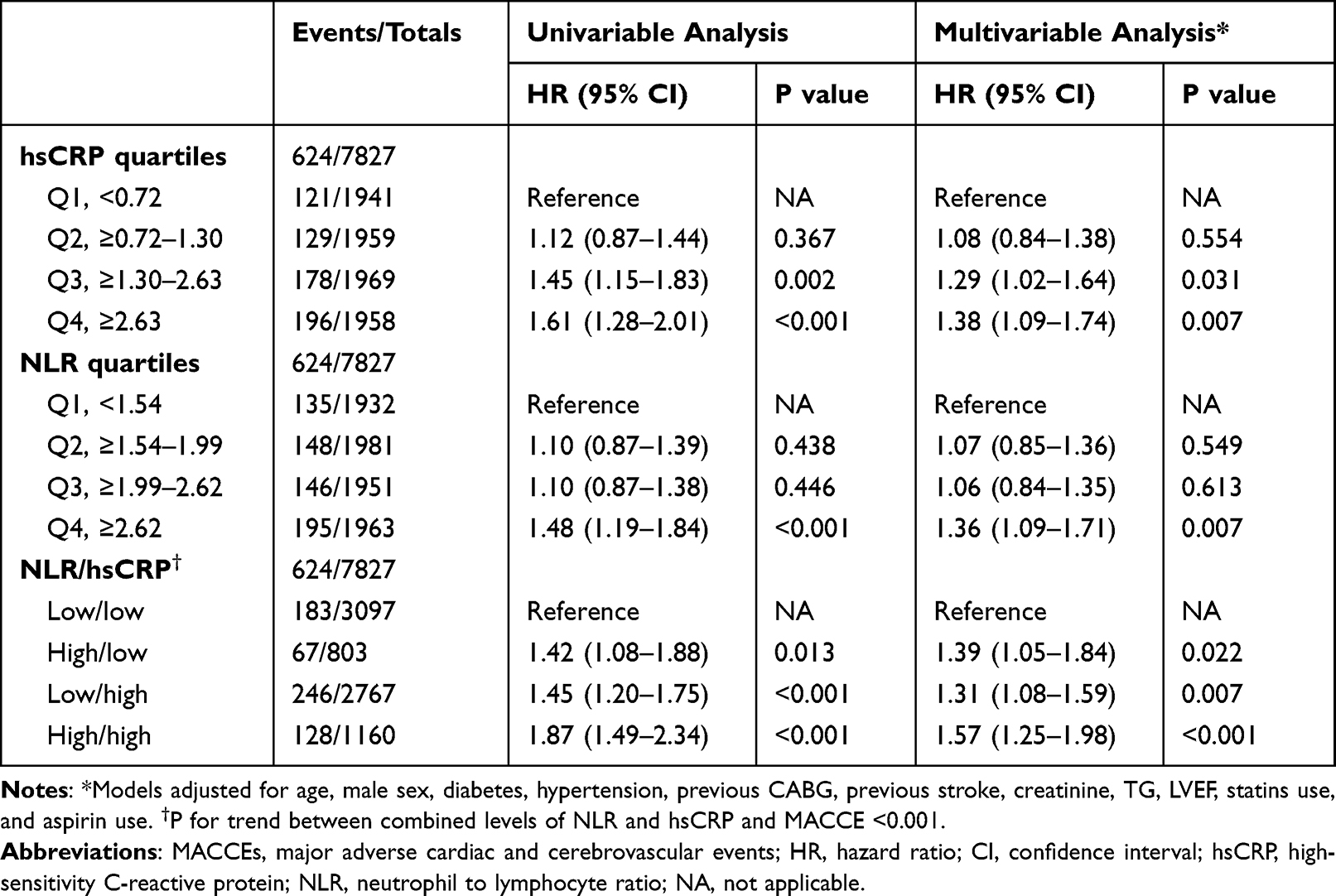 |
Table 3 Univariable and Multivariable Cox Proportional Hazard Analyses for MACCEs |
Association of 4 Concordance/Discordance Groups According to Low or High NLR and hsCRP Levels with Adverse Clinical Events
Patients in the concordant high /high group had the highest incidence of MACCEs, CV death, non-fatal stroke, and unplanned revascularization during follow-up. Meanwhile, no significant difference was observed with regard to the incidence of non-fatal MI across four risk groups (Figure 3).
Univariable Cox regression analysis showed that patients in the high/low, low/high, and high/high groups encountered a 42%, 45%, and 87% increase in MACCE risk, respectively, compared to the reference group (the low/low group; all P < 0.05, Table 3). Consistently, in the fully adjusted model, the adjusted HRs for MACCEs were 1.39 (95% CI, 1.05–1.84), 1.31 (95% CI, 1.08–1.59), and 1.57 (95% CI,1.25–1.98) when NLR and hsCRP were elevated discordantly or concordantly, respectively, compared with the reference group (all P < 0.05) (Supplementary Table 2). In addition, multivariable Cox proportional hazard analysis revealed that patients with concordant elevations of NLR and hsCRP had the highest risk of MACCEs (P for trend <0.001). Cox regression analyses for secondary endpoints are listed in the Supplementary Table 3. NLR and hsCRP elevated concordantly were associated with a 1.73-fold (95% CI, 1.02–2.92), 1.72-fold (95% CI, 1.07–2.76), and 1.45-fold (95% CI, 1.05–2.00) higher risk for CV death, non-fatal stroke, and unplanned revascularization, respectively, compared to the reference group (all P < 0.05).
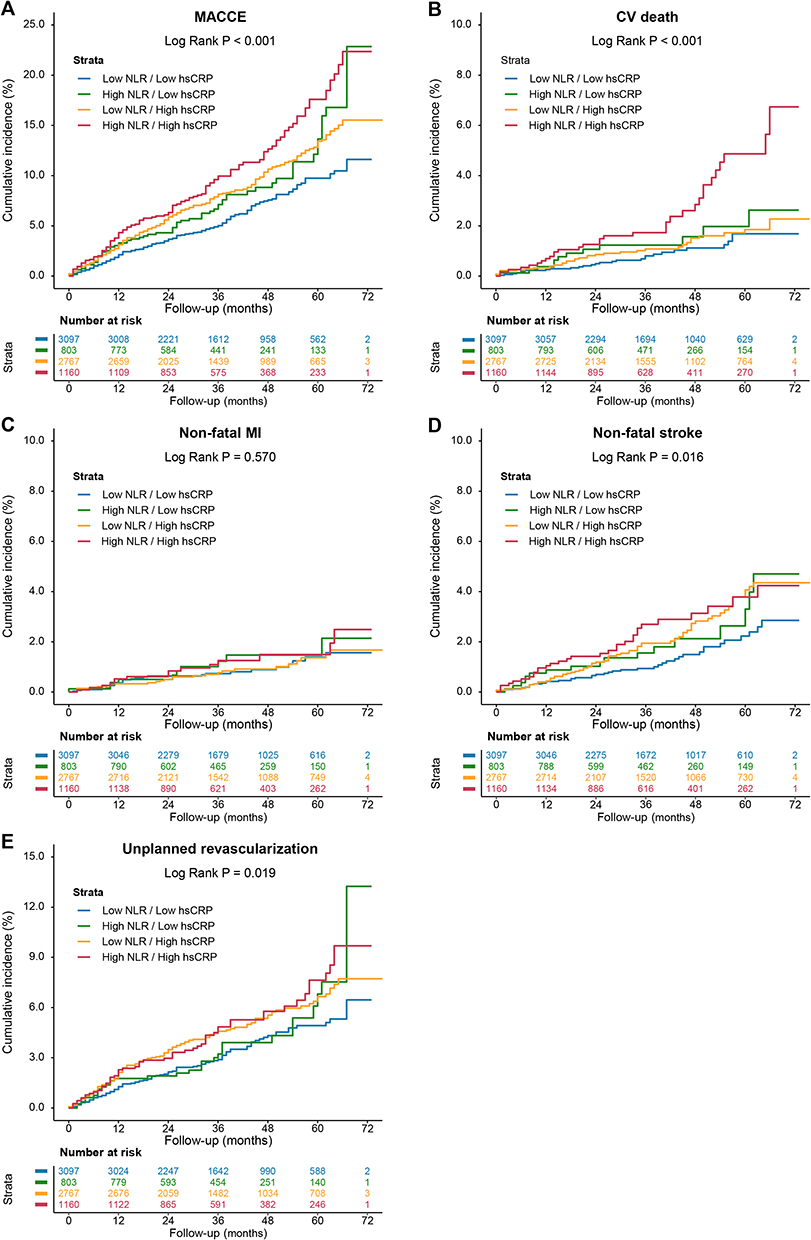 |
Figure 3 Kaplan–Meier (KM) curves for adverse clinical events according to 4 concordance/discordance groups by NLR and hsCRP levels KM curves for MACCEs (A), CV death (B), non-fatal MI (C), non-fatal stroke (D), and unplanned revascularization (E) according to 4 concordance/discordance groups by NLR and hsCRP levels MACCEs were defined as a composite of CV death, non-fatal MI, non-fatal stroke, and unplanned revascularization. Abbreviations: NLR, neutrophil to lymphocyte ratio; hsCRP, high-sensitivity C-reactive protein; MACCE, major adverse cardiovascular and cerebrovascular events; CV, cardiovascular; MI, myocardial infarction. |
Sensitivity, Subgroup and Mediation Analyses
In an exploratory step, the association of 4 concordance/discordance groups using hsCRP guideline-guide target cutoffs of 2 mg/L with the risk of MACCEs was estimated to test the robustness of our findings. As a result, in fully adjusted models, patients with discordantly increased NLR levels were still at a 1.30-fold higher risk of MACCE (95% CI, 1.03–1.64) (Supplementary Table 4).
Moreover, As illustrated in Supplementary Tables 5 and 6, subgroup analyses demonstrated that the association between four risk groups and MACCEs remained consistent regardless of age (age ≥65 years or age <65 years), sex (male or female), BMI (BMI ≥ 25 kg/m2 or BMI < 25 kg/m2), diabetes (with or without diabetes), and hypertension (with or without hypertension) in both crude and fully adjusted models (all P for interaction >0.05).
In mediation analyses (Supplementary Table 7), NLR accounted for 13.1% (95% CI, 1.5%–42.0%, P = 0.020) of the associations between hsCRP and MACCEs. Besides, hsCRP also played a significant mediating role in the associations of NLR with MACCEs (proportions mediated, 17.1%; 95% CI, 4.0%–60.0%, P = 0.008).
Discussion
This observational study including large-scale secondary prevention cohort of CAD participants demonstrated that systemic inflammation assessed by elevated NLR levels was strongly associated with an increased risk for MACCEs during long-term follow-up. NLR levels are significantly but modestly correlated with hsCRP levels, and the discordance existed in more than 10% of patients with stable CAD. Discordantly elevated NLR levels were associated with a higher risk of MACCEs in patients with CAD during follow-up. Meanwhile, patients could encounter an increased risk of CV death and non-fatal stroke only when NLR and hsCRP increased concordantly. Specifically, the risk for adverse events may underestimate or overestimate when using hsCRP alone. To our knowledge, this study is the first comparing the effectiveness of NLR and hsCRP to predict the risk of adverse clinical events in patients with stable CAD, and our findings suggested a promising clinical significance for NLR as a goal of inflammatory risk management.
Plasma TC levels in many resource-rich populations have been in steady decline in response to lifestyle interventions and pharmacological treatments by targeting LDL-C.15 However, despite such efforts, CV events continue to occur frequently, even among subjects with controlled LDL-C.16,17 In the recent FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Patients With Elevated Risk) trial using evolocumab, a PCSK9 inhibitor, for secondary prevention after ACS, composite event rates during the median follow-up of 26 months remained at 9.8% in the evolocumab group despite an achieved median LDL-C of 0.78mmol/L.17 Although current evidence supports aggressively reducing LDL-C to reduce CV events, further therapeutic strategies may be needed to appropriately reduce remaining CV risk. And systemic inflammation is one of the most mainly focused risk factors among residual CV risk.1,5 In secondary prevention of stable atherosclerotic vascular disease, extensive studies demonstrated that hsCRP is also informative and has a positive relationship with adverse cardiovascular events such as MI, revascularization, stroke, heart failure, and mortality.1,2,18 Similarly, our findings also indicated that patients with the higher hsCRP levels encountered increased risk of MACCEs compared to those with the lowest hsCRP level during follow-up. In the FOURIER trial, participants with the highest hsCRP levels had the highest event rates and, in turn, the greatest absolute risk reductions.2 Supporting this clinical observation, intravascular ultrasonography demonstrated on-statin reductions in hsCRP are significantly associated with the rate of plaque progression after adjusting for changes in lipids.19 These studies support hsCRP as a reliable biomarker to assess inflammatory risk, and potential biomarker to guide-related therapies.
Although the role of hsCRP as an inflammatory biomarker has been widely studied, contemporary studies have also increased awareness of a simple biomarker that is widely and readily available to the clinical community, such as NLR.8,9 Observational studies have suggested that high NLR levels were associated with increased atherosclerotic plaque vulnerability and lesion severity.10,20 Besides, previous studies have demonstrated baseline NLR independently predict future adverse events and CV death after adjusting confounding factors.21–23 Of note, a recent analysis of five large contemporary trials, including the CANTOS trial, studies of PCSK9 Inhibition and the Reduction of Vascular Events (SPIRE)-1, SPIRE-2, and Cardiovascular Inflammation Reduction Trial, demonstrated that the association between NLR and clinical outcomes remained significant even after adjusting for hsCRP. Meanwhile, previous studies have reported that NLR levels were modestly correlated with hsCRP levels,9,22 which was also observed in this study. Collectively, these observations convey the information that NLR, as an inflammatory biomarker, has important prognostic value and provides additional information on the nature of the inflammatory process, which is not mirrored by hsCRP or cytokines.9 And our study provided additional information to support previous research, indicating the clinical significance of NLR for predicting the risk of adverse events in CAD patients.
There are several potential mechanisms for the positive association between NLR and poor prognosis. First, activated neutrophils secrete inflammatory mediators. These molecules could initiate atherosclerosis and promote plaque progression by upregulating inflammatory response, myeloid cell recruitment, oxidative stress, and foam cell formation.24,25 In addition, the presence of neutrophils in the arterial intima was positively associated with traits of plaque instability in humans and mice.26 Activate neutrophils release neutrophil extracellular traps (NETs) containing cytotoxic histone H4 and matrix metalloproteinases eventually resulting in the fibrous cap thinning.24 Furthermore, lymphopenia may occur in response to an increase level of cortisol, catecholamines, and proinflammatory cytokines.27,28 Besides, lymphocyte apoptosis was shown to be present in atherosclerotic plaques and becomes increasingly frequent with the progression and destabilization of the atherosclerotic lesion.29 The redistribution of T cells from the circulation to lymphoid tissues potentially exacerbate lymphopenia, which could promote compensatory proliferation of antigen-experienced T cells, further resulting in risk of CV events.30,31
In this study, we adopted discordance analysis to compare the effectiveness of NLR and hsCRP levels for the prediction of CAD prognosis. Although the C-statistics have been widely used to evaluate the discriminative performance and could identify diseased patients by sensitivity and specificity, it might be suboptimal and could mistakenly exclude pivotal risk factors. Meanwhile, the improvement in C-statistics by adding new risk factors to the clinical risk models might be small, despite statistically significant.32 By contrast, discordance analysis mainly focused on the clinical consequences, rather than the prediction accuracy. This method is a new approach,33,34 which could discriminate additional positive cases and help the clinicians to understand the consequences of NLR through the disagreements between the NLR and hsCRP levels. In this study, there were more than 10% of patients exhibiting discordant elevation in NLR levels who were also at higher inflammatory risk which was underestimated by hsCRP alone. Since previous research has demonstrated that NLR levels markedly decreased during anti-inflammatory treatment with canakinumab,9 future prospective studies are also warranted to examine whether monitoring anti-inflammatory treatment response by targets of NLR levels could further reduce CV risks among CAD patients. Furthermore, in the present study, reduced rates of aspirin and statins use were observed in patients experiencing MACCE. According to current guideline, patients with stable CAD could benefit from adequate therapy for secondary prevention (such as aspirin and statins).35 Aspirin acts via irreversible inhibition of platelet cyclooxygenase-1 and thus thromboxane production, and current evidence suggests a daily low-dose aspirin for the prevention of ischemic events in CAD patients with or without a history of MI.36,37 Consistently, in this study, univariable Cox proportional hazard model shown that aspirin use and statins use were both inversely associated with the risk of MACCE. And after multivariable adjustment including aspirin use and statins use, high NLR levels remained to predict MACCE in CAD patients, even in those with low hsCRP levels, indicating the association of NLR and hsCRP with risk of MACCE independent of medications for secondary prevention.
Clinical Translations
This study with a sizeable sample size confirmed that increased levels were associated with increased risk of adverse clinical events in CAD populations, even in those with low hsCRP levels. The CANTOS trial illustrated that participants who achieved on-treatment hsCRP in the lowest tertile had a 29% reduction in CV events, whereas participants with on-canakinumab hsCRP in the highest tertile had comparable outcomes with the placebo group.3 The findings support hsCRP as a potential marker of the adequacy of relative therapies. Meanwhile, a post-hoc analysis of the CANTOS trial showed that canakinumab significantly reduced the NLR in a dose-dependent manner, mimicking that for CRP and IL-6.9 Since there was an increased risk of adverse events in patients with low hsCRP levels who had high NLR levels, patients could benefit from anti-inflammatory therapies by targeting both NLR and hsCRP levels. Further prospective studies are needed to investigate such hypothesis.
Study Limitations
Several limitations of this study need to be addressed. First, due to the nature of observational study design, potential confounding factors could not be fully eradicated.38,39 Second, information on hsCRP and NLR was not available during follow-up, which possibly provide incremental value for prediction of adverse clinical events. Third, this study only included Chinese patients, and further studies are warranted among individuals from other ethnicities. Fourth, per observation study design, the effect of pharmacological treatments on CV outcomes by targeting NLR levels could not be determined in this study. Further prospective studies are needed to investigate the effect of pharmacological treatments. Fifth, the mechanism between NLR and events remained unclear. Further mechanistic studies aiming to investigate the association between NLR and events are needed.
Conclusion
This study demonstrated discordantly elevated NLR levels were associated with a greater risk of adverse clinical events in patients with stable CAD, suggesting a potential clinical significance for NLR as a goal of inflammatory risk management.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
This work was supported by the CAMS Innovation Fund for Medical Sciences (CIFMS) [grant number, 2021-I2M-1-008].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lawler PR, Bhatt DL, Godoy LC, et al. Targeting cardiovascular inflammation: next steps in clinical translation. Eur Heart J. 2021;42(1):113–131. doi:10.1093/eurheartj/ehaa099
2. Bohula EA, Giugliano RP, Leiter LA, et al. Inflammatory and Cholesterol Risk in the Fourier Trial. Circulation. 2018;138(2):131–140. doi:10.1161/CIRCULATIONAHA.118.034032
3. Ridker PM, MacFadyen JG, Everett BM, et al. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: a secondary analysis from the CANTOS randomised controlled trial. Lancet. 2018;391(10118):319–328. doi:10.1016/S0140-6736(17)32814-3
4. Kaptoge S, Di Angelantonio E, Lowe G, et al. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–140.
5. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
6. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383(19):1838–1847. doi:10.1056/NEJMoa2021372
7. Tardif J-C, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
8. Agarwal R, Aurora RG, Siswanto BB, et al. The prognostic value of neutrophil-to-lymphocyte ratio across all stages of coronary artery disease. Coron Artery Dis. 2022;33(2):137–143. doi:10.1097/MCA.0000000000001040
9. Adamstein NH, MacFadyen JG, Rose LM, et al. The neutrophil-lymphocyte ratio and incident atherosclerotic events: analyses from five contemporary randomized trials. Eur Heart J. 2021;42(9):896–903. doi:10.1093/eurheartj/ehaa1034
10. He J, Bian X, Song C, et al. High neutrophil to lymphocyte ratio with type 2 diabetes mellitus predicts poor prognosis in patients undergoing percutaneous coronary intervention: a large-scale cohort study. Cardiovasc Diabetol. 2022;21(1):156. doi:10.1186/s12933-022-01583-9
11. Sager HB, Koenig W. Immune cell-based cardiovascular risk assessment: spotlight on the neutrophil-lymphocyte ratio. Eur Heart J. 2021;42(9):904–906. doi:10.1093/eurheartj/ehaa1104
12. Wada H, Dohi T, Miyauchi K, et al. Neutrophil to Lymphocyte Ratio and Long-Term Cardiovascular Outcomes in Coronary Artery Disease Patients with Low High-Sensitivity C-Reactive Protein Level. Int Heart J. 2020;61(3):447–453. doi:10.1536/ihj.19-543
13. Association AD. 2. Classification and Diagnosis of Diabetes: standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–S38. doi:10.2337/dc22-S002
14. Grundy SM, Stone NJ, Bailey AL, et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73(24):e285–e350. doi:10.1016/j.jacc.2018.11.003
15. Rosinger A, Carroll MD, Lacher D, et al. Trends in total cholesterol, triglycerides, and low-density lipoprotein in US adults, 1999–2014. JAMA Cardiol. 2017;2(3):339–341. doi:10.1001/jamacardio.2016.4396
16. He J, Yang M, Song C, et al. Lipoprotein(a) is associated with recurrent cardiovascular events in patients with coronary artery disease and prediabetes or diabetes. J Endocrinol Invest. 2023. doi:10.1007/s40618-023-02203-3
17. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
18. Held C, White HD, Stewart RAH, et al. Inflammatory Biomarkers Interleukin-6 and C-Reactive Protein and Outcomes in Stable Coronary Heart Disease: experiences From the STABILITY (Stabilization of Atherosclerotic Plaque by Initiation of Darapladib Therapy) Trial. J Am Heart Assoc. 2017;6(10). doi:10.1161/JAHA.116.005077.
19. Nissen SE, Tuzcu EM, Schoenhagen P, et al. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med. 2005;352(1):29–38. doi:10.1056/NEJMoa042000
20. Xu N, Tang X-F, Yao Y, et al. Predictive value of neutrophil to lymphocyte ratio in long-term outcomes of left main and/or three-vessel disease in patients with acute myocardial infarction. Catheter Cardiovasc Interv. 2018;91(S1):551–557. doi:10.1002/ccd.27495
21. Papa A, Emdin M, Passino C, et al. Predictive value of elevated neutrophil-lymphocyte ratio on cardiac mortality in patients with stable coronary artery disease. Clin Chim Acta. 2008;395(1–2):27–31. doi:10.1016/j.cca.2008.04.019
22. Wada H, Dohi T, Miyauchi K, et al. Pre-procedural neutrophil-to-lymphocyte ratio and long-term cardiac outcomes after percutaneous coronary intervention for stable coronary artery disease. Atherosclerosis. 2017;265:35–40. doi:10.1016/j.atherosclerosis.2017.08.007
23. Bressi E, Mangiacapra F, Ricottini E, et al. Impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio on 5-year clinical outcomes of patients with stable coronary artery disease undergoing elective percutaneous coronary intervention. J Cardiovasc Transl Res. 2018;11(6):517–523. doi:10.1007/s12265-018-9829-6
24. Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17(6):327–340. doi:10.1038/s41569-019-0326-7
25. Burn GL, Foti A, Marsman G, et al. The Neutrophil. Immunity. 2021;54(7):1377–1391. doi:10.1016/j.immuni.2021.06.006
26. Warnatsch A, Ioannou M, Wang Q, et al. Neutrophil extracellular traps license macrophages for cytokine production in atherosclerosis. Science. 2015;349(6245):316–320. doi:10.1126/science.aaa8064
27. Gordon AS. Some aspects of hormonal influences upon the leukocytes. Ann N Y Acad Sci. 1955;59(5):907–927. doi:10.1111/j.1749-6632.1955.tb45990.x
28. Ulich TR, Keys M, Ni RX, et al. The contributions of adrenal hormones, hemodynamic factors, and the endotoxin-related stress reaction to stable prostaglandin analog-induced peripheral lymphopenia and neutrophilia. J Leukoc Biol. 1988;43(1):5–10. doi:10.1002/jlb.43.1.5
29. Hofmann U, Frantz S. Role of lymphocytes in myocardial injury, healing, and remodeling after myocardial infarction. Circ Res. 2015;116(2):354–367. doi:10.1161/CIRCRESAHA.116.304072
30. Zafrir B, Hussein S, Jaffe R, et al. Lymphopenia and mortality among patients undergoing coronary angiography: long-term follow-up study. Cardiol J. 2022;29(4):637–646. doi:10.5603/CJ.a2020.0141
31. Le Campion A, Gagnerault M-C, Auffray C, et al. Lymphopenia-induced spontaneous T-cell proliferation as a cofactor for autoimmune disease development. Blood. 2009;114(9):1784–1793. doi:10.1182/blood-2008-12-192120
32. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115(7):928–935. doi:10.1161/CIRCULATIONAHA.106.672402
33. Su X, Cai X, Pan Y, et al. Discordance of apolipoprotein B with low-density lipoprotein cholesterol or non-high-density lipoprotein cholesterol and coronary atherosclerosis. Eur J Prev Cardiol. 2022;29(18):2349–2358. doi:10.1093/eurjpc/zwac223
34. Hu C, Zhang J, Liu J, et al. Discordance between the triglyceride glucose index and fasting plasma glucose or HbA1C in patients with acute coronary syndrome undergoing percutaneous coronary intervention predicts cardiovascular events: a cohort study from China. Cardiovasc Diabetol. 2020;19(1):116. doi:10.1186/s12933-020-01091-8
35. Knuuti J, Wijns W, Saraste A, et al. ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
36. Collaboration AT. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71–86. doi:10.1136/bmj.324.7329.71
37. Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849–1860.
38. He J, Yuan S, Song C, et al. High triglyceride-glucose index predicts cardiovascular events in patients with coronary bifurcation lesions: a large-scale cohort study. Cardiovasc Diabetol. 2023;22(1):289. doi:10.1186/s12933-023-02016-x
39. He J, Song C, Wang H, et al. Diabetes mellitus with mild or moderate kidney dysfunction is associated with poor prognosis in patients with coronary artery disease: a large-scale cohort study. Diabetes Res Clin Pract;2023:110693. doi:10.1016/j.diabres.2023.110693
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.