Back to Journals » Journal of Inflammation Research » Volume 15
The Pre-Ablation Circulating Tumor-Associated Inflammatory Index Predicts the Prognosis of Patients with Liver Metastasis from Pancreatic Cancer
Authors Li Y ![]() , Peng L, Zhang K, Wu Y, Gao H, Chen H
, Peng L, Zhang K, Wu Y, Gao H, Chen H ![]()
Received 14 July 2022
Accepted for publication 14 October 2022
Published 27 October 2022 Volume 2022:15 Pages 5977—5987
DOI https://doi.org/10.2147/JIR.S381807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yujie Li,1,2 Linjia Peng,1,2 Ke Zhang,1,2 Yong Wu,3 Huifeng Gao,1,2 Hao Chen1,2
1Department of Integrative Oncology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 2Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China; 3Department of Oncology, The Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine, Hefei, People’s Republic of China
Correspondence: Hao Chen, Department of Integrative Oncology, Fudan University Shanghai Cancer Center, 270 Dong’an Road, Shanghai, People’s Republic of China, Tel +86-18017312356, Email [email protected]
Objective: Ablation serves as a common local treatment for liver metastases from pancreatic cancer (PCLM), but the correlation between the prognosis of PCLM and inflammatory cytokines has been rarely reported. This study aimed to establish a cytokine-based prognostic model for patients with PCLM who are receiving ablation.
Patients and Methods: Serum samples from peripheral blood were collected from patients with PCLM before their first ablation. Cytokines were measured using Luminex chips and ELISA. Cox regression and least absolute shrinkage and selection operator regression were used to select prognostic factors for overall survival (OS). Area under the receiver operating characteristic curve (AUC) was applied to compare the ability to predict survival.
Results: The relationship between cytokines and clinical factors was evaluated and their prognostic value was compared. Six optimal predictors were selected, including IL-2, IL-7, HGF, IFN-γ, CA19-9 and CEA. The risk model based on these predictors was built and named circulating tumor-associated inflammatory index (CTII). The CTII (AUCs > 0.90) showed superior performance to systemic immune-inflammation index (SII, AUCs < 0.65) in OS.
Conclusion: A circulating cytokine-based risk model for patients with PCLM before first ablation has been proposed and validated, which has demonstrated superior performance in predicting survival and has the potential to inform clinical treatment strategies.
Keywords: inflammation, cytokines, advanced pancreatic cancer, ablation, prognosis
Introduction
As one of the fourth leading cause of cancer-related death, pancreatic cancer is characterized by its insidious onset and poor prognosis.1 Radical surgery serves as the only treatment strategy that can significantly improve survival, but more than 50% patients were diagnosed with unresectable pancreatic cancer.2 Despite surgical resection, recurrence or metastasis still occur in most patients.3 Liver has been reported as the most common site of metastasis in patients with advanced pancreatic cancer,4 and the prognosis was worse than that in patients with lung or distant lymph node metastasis.5 Among the limited treatment modalities, ablation is an important local treatment method for liver metastases from pancreatic cancer (PCLM), which is expected to be beneficial to achieve long-term survival.
Ablation is a minimally invasive procedure that, under the guidance of an imaging device, directly causes tumor necrosis through a physical or chemical procedure by percutaneous puncture into tumor tissue. Physical ablation can be categorized into thermal ablation and non-thermal ablation, and microwave ablation is a type of thermal ablation.6 Ablation induces tumor cell reduction and anticancer immune activation through a variety of mechanisms.7 Increasing evidences have indicated that ablation-mediated necrosis can modulate the host immune-inflammation response.8,9 Previous studies have shown that a combination of thermal ablation and systemic chemotherapy can lead to a better survival outcome in patients with PCLM.10,11 Currently, ablation has been recommended by the National Comprehensive Cancer Network (NCCN) guidelines for the treatment of various types of cancers.6 However, the prognosis of patients undergoing ablation varies. Therefore, the identification of prognostic risk factors may help to accurately screen the appropriate population.
As effector molecules, cytokines play an essential role in tumor microenvironment and mediate immune activation against cancer cells. Many studies have investigated the role of cytokines as diagnostic, prognostic, or predictive biomarkers of pancreatic cancer.12 However, whether circulating inflammatory factor levels are risk factors in patients with PCLM is poorly reported. The objective of our study was to determine the relationship between pre-ablation cytokines and prognosis in patients with PCLM from readily available peripheral blood samples. In this study, a novel index, termed circulating tumor-associated inflammatory index (CTII), was constructed. The CTII showed an exceptional prognostic value before ablation and has the potential to guide the treatment of PCLM.
Materials and Methods
Patients
A retrospective cohort study (n = 70) consisting of patients who were diagnosed with PCLM and received ablation as an initial treatment was conducted from January 2020 to March 2022 at Fudan University Shanghai Cancer Center (FUSCC). The patients were divided into training cohort (n = 31) and validation cohort (n = 39) according to the time of blood collection before the ablation. Another group of healthy individuals were served as control (n = 8). Patients who met the following criteria were included in this study: 1) Histologically or cytologically diagnosed as pancreatic adenocarcinoma. 2) Radiology confirmed only liver metastases (including distant lymph node metastases) and no other important organ metastases. The exclusion criteria included: 1) Receiving minimally invasive treatments other than microwave ablation (such as irreversible electroporation and cryoablation). 2) A second primary malignancy detected during treatment. 3) Lacking information on serum level of cytokines and tumor markers.
The study was approved by the ethics committee of FUSCC. All procedures are conducted in accordance with the ethical standards of our institution’s Research Committee and the 1964 Declaration of Helsinki and its subsequent amendments or similar ethical standards. Written informed consent was obtained from patients prior to treatment.
Clinical Variables Collection and Treatment Procedure
Clinical and pathological data, including age, gender, tumor grade, tumor site, surgery, distant lymph node metastasis and chemotherapy, were acquired from the electronic medical record system of FUSCC. The laboratory measures included C-reactive protein (CRP), white blood cell (WBC) counts, hemoglobin (HGB), neutrophil (NE) counts, lymphocyte (LY) counts, platelet (PLT) counts, serum levels of alanine transaminase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), glutamyl transpeptidase (GGT), albumin (ALB) and total bilirubin (TBIL). And the tumor biomarkers included carbohydrate antigen 19–9 (CA19-9), carbohydrate antigen 125 (CA125) and carcinoembryonic antigen (CEA). All decisions regarding patient selection and regional treatment modalities were agreed upon through multidisciplinary discussions. The primary end point of this study was overall survival (OS), which was defined as the interval between the first ablation treatment and death or last follow-up. Follow-up was terminated in the training cohort on 1 June 2022 and in the validation cohort on 30 September 2022.
Luminex Liquid Bead Suspension Chip Array
All patients had blood samples taken one day before ablation. After centrifugation, cellular debris was removed, serum was obtained and stored at −80°C. Luminex liquid bead suspension chip detection was performed by Wayen Biotechnologies (Shanghai, China). The Bio-Plex Pro Human Chemokine Panel 48-plex kit was used in accordance with the manufacturer’s instructions.
Enzyme-Linked Immunosorbent Assay (ELISA)
For the validation cohort, the concentrations of IL-2, IL-7, HGF and IFN-γ in blood samples were measured by IL-2, IL-7, HGF and IFN-γ ELISA kits (SenBeiJia Biotechnology, Nanjing, China, Cat no.: SBJ-H0297, Cat no.: SBJ-H2148, Cat no.: SBJ-H0268 and Cat no.: SBJ-H2280) according to the manufacturer’s instructions.
Systemic Immune-Inflammation Index
Systemic immune-inflammation index (SII) was defined as an index based on PLT, NE, and LY counts and calculated using the following formula:  13 Based on our previous study, the optimal cutoff for SII in advanced pancreatic cancer was determined to be 440*109 and the patients were divided into high (>440) and low (≤440) SII score groups.14
13 Based on our previous study, the optimal cutoff for SII in advanced pancreatic cancer was determined to be 440*109 and the patients were divided into high (>440) and low (≤440) SII score groups.14
Bioinformatics Screening for Prognostic Factors
To ensure the universality of the selected factors in different cohorts, we first normalized the concentration of the factors by log2 transformation. Pearson correlation analyses was used to analyze the correlation between inflammatory factors and Mantel test was used to analyze the correlation between two matrices by “ggcor” R package. The prognostic factors were selected by univariate Cox regression analysis (P < 0.05). Then, the least absolute shrinkage and selection operator (LASSO) regression model was constructed by “glmnet” R package. Finally, the regression coefficient for each factor used in the construction of the final prognostic signature. The CTII was equal to the sum of the coefficient of each factor multiplied by its concentrations, and the patients were divided into two groups according to the median. The survival curves were analyzed using the Kaplan–Meier (K-M) method and survival differences in terms of OS were compared by the Log rank test by R package “survival”. Univariate and multivariate Cox regression were used to verify whether the inflammation score was an independent prognostic factor. The time-dependent receiver operating characteristic (ROC) analysis was used to assess discrimination of the model using the R package “timeROC”. And area under the ROC curve (AUC) of CTII and SII were compared.
Statistical Analysis
All statistical analyses in this study were conducted by R software (version 4.1.0). Continuous variables were presented as the median and range. Continuous variables and categorical variables were compared by independent sample t-test, Mann–Whitney U-test and chi-square test. A two-sided P value <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 78 subjects were enrolled in this study, including 70 PCLM (31 in training cohort and 39 in validation cohort) and 8 healthy individuals. The clinical characteristics of the patients with PCLM are shown in Table 1. In the patient population of the training cohort, 23 (74.2%) were male and 8 (25.8%) were female, with a median age of 57 years (range 41–76 years). 54.8% of the primary tumors were located in the head of the pancreas, and 35.5% were poorly differentiated. About 29% had undergone radical surgery at the early stage of diagnosis, and 71% had unresectable pancreatic cancer at the time of diagnosis. 45.2% had distant lymph nodes metastasis. 67.7% had received chemotherapy prior to ablation. In this cohort, the median OS was 5 months. Based on Luminex liquid bead suspension chip detection, the baseline cytokine levels of patients in the training cohort are shown in Table 2. Compared with healthy control subjects, the levels of interleukin (IL)-1α, IL-1β, IL-2Rα, IL-4, IL-7, IL-8, IL-17A, hepatocyte growth factor (HGF), macrophage inflammatory protein-1α (MIP-1α), cutaneous T cell-attracting chemokine (CTACK), monocyte chemotactic protein-3 (MCP-3), fibroblast growth factor (FGF), leukemia inhibitory factor (LIF), tumor necrosis factor-α (TNF-α), Eotaxin, interferon (IFN)-γ, IFN-α2, platelet-derived growth factor-BB (PDGF-BB), granulocyte colony-stimulating factor (G-CSF), monokine induced by gamma interferon (MIG) and were significantly increased (P < 0.05) in patients with PCLM (Figure 1).
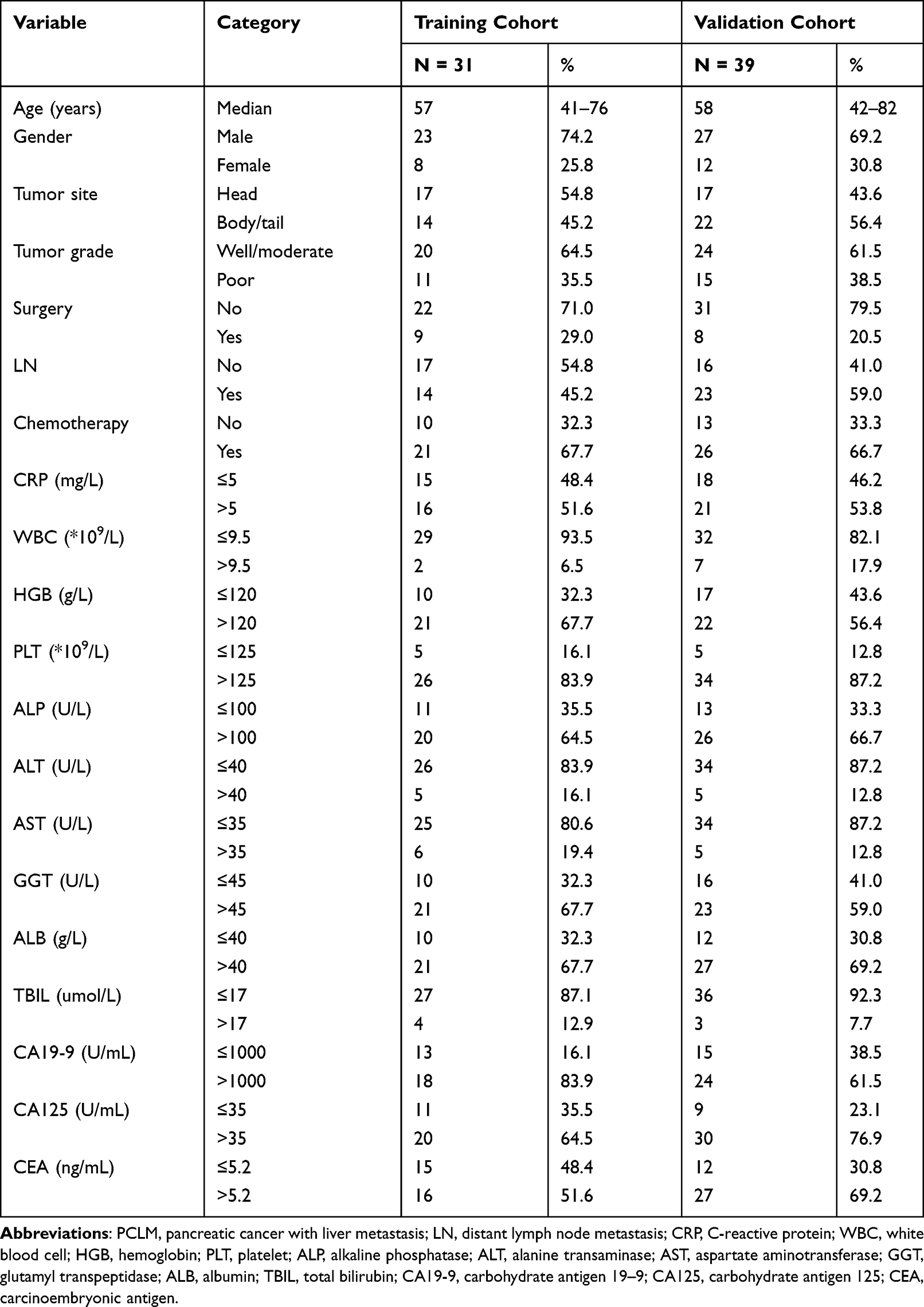 |
Table 1 Clinical Characteristics of Patients with PCLM Undergoing Ablation Therapy |
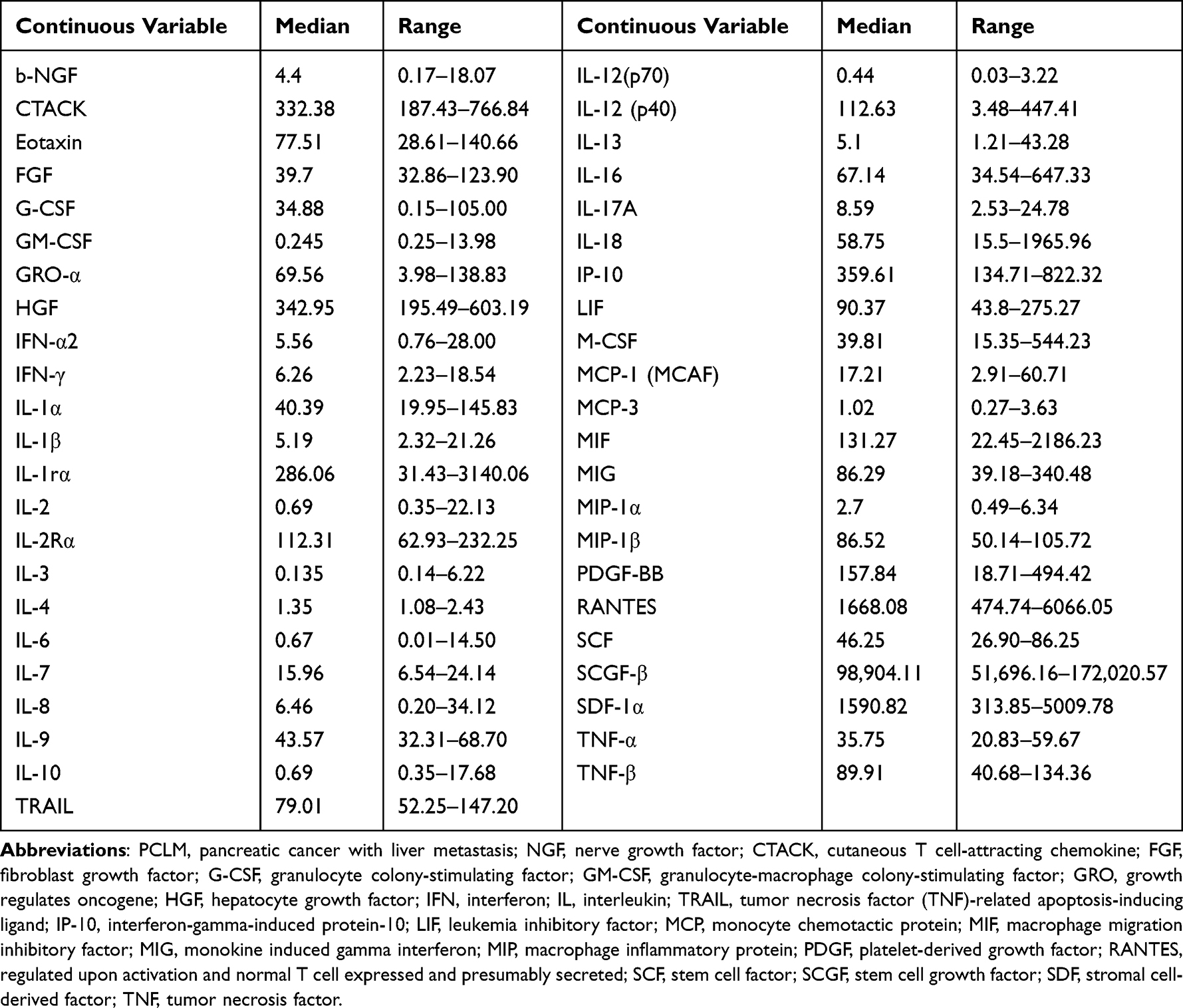 |
Table 2 The Concentration of Cytokines in Training Cohort (Pg/mL) |
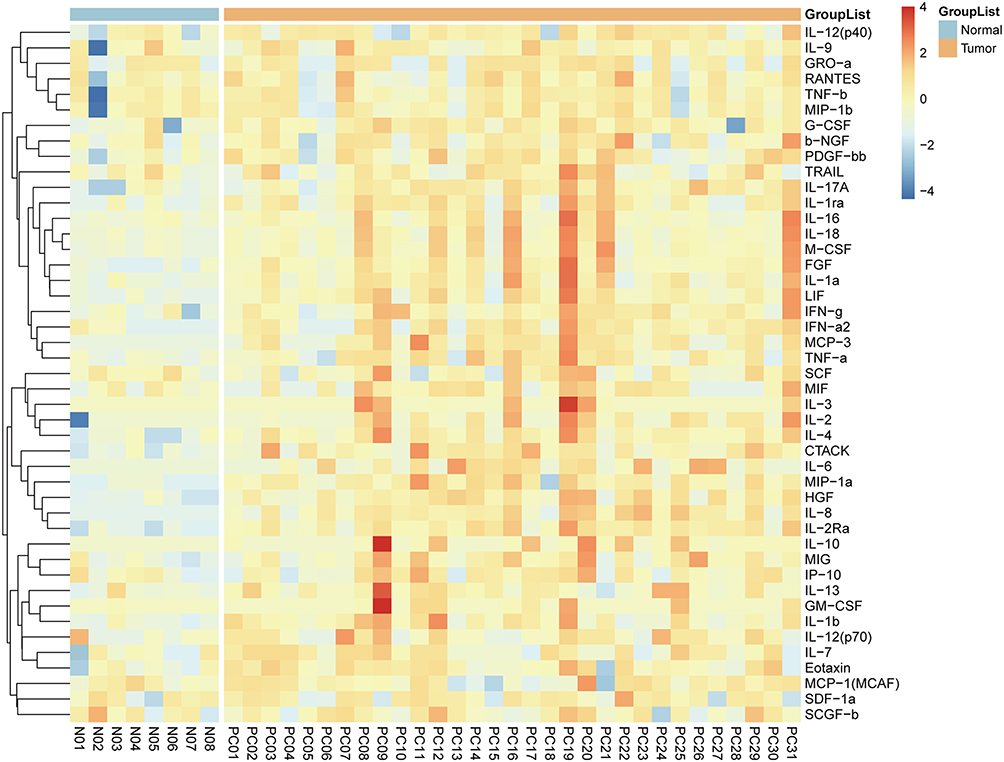 |
Figure 1 The heatmap showed the comparison of cytokines between patients with PCLM and healthy controls. |
Correlation Between the Circulating Cytokines and Clinicopathologic Parameters
The modest associations between circulating cytokines and clinicopathological parameters were observed (Figure 2A). There was a strong correlation network among M-CSF, IL-18, IL-16, FGF, IL-1α and LIF, as well as between IL-4 and IL-2 (Cor > 0.8, P < 0.05). To illustrate the correlation among these factors from different perspectives, blood routine, biochemical routine and tumor biomarkers were included in the separate panels, and the correlations between these three panels and cytokines were analyzed by Mantel test (Figure 2B). The biochemical routine and tumor markers were both correlated with IL-6 and IL-8 (P < 0.05). Positive correlations between IL-2 and IL-4, IL-3, IL-2Rα, were observed respectively. Also, LIF, M-CSF, IL-16 and IL-18 were positively associated with FGF, IFN-α2, IL-1Rα, IL-1α, IL-2, IL-3, and IL-4, respectively.
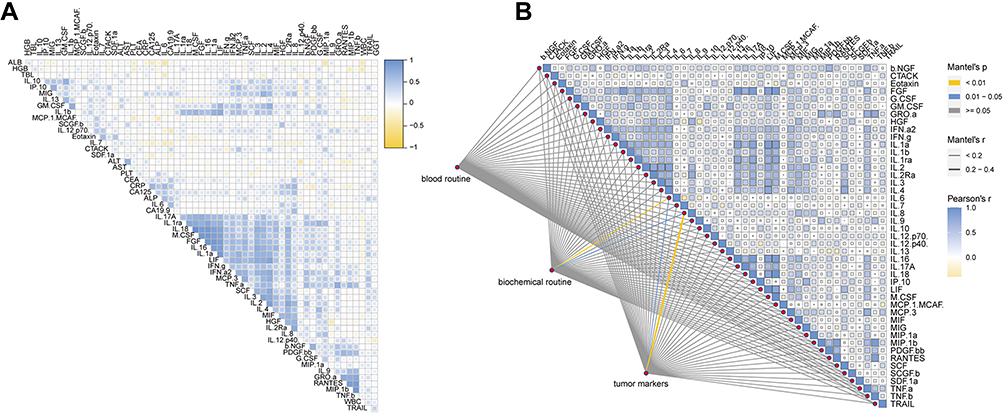 |
Figure 2 The correlation heatmap analysis of the relationship among cytokines and clinical characteristics. (A) Correlation analysis of all cytokines and clinicopathological factors. (B) Mantel test for association analysis between all cytokines and blood routine, biochemical routine, and tumor marker matrices, respectively. |
Screening of Prognostic Factors and Construction of CTII
In order to develop a prognostic model with higher predictive accuracy than previous models, we first selected 10 factors significantly associated with prognosis from all cytokines and clinicopathologic parameters by univariate Cox regression analysis (Figure 3A). The 6 optimal predictors (IL-2, IL-7, HGF, IFN-γ, CA19-9 and CEA) were then selected to compose the CTII using the LASSO regression method (Figure 3B) and ten-fold cross-validation (Figure 3C). The coefficients of the 6 predictors were shown in Table S1. The CTII was arranged in order from low to high, and patients were divided into high or low-CTII groups based on the median value. The K-M analysis showed that high-CTII was significantly associated with inferior OS (P < 0.001, Figure 3D). To compare the predictive ability of CTII and SII, our cohort was also divided into high- and low-SII groups. Similar to our previous results,14 high-SII was significantly associated with poor OS (P = 0.018, Figure 3E).
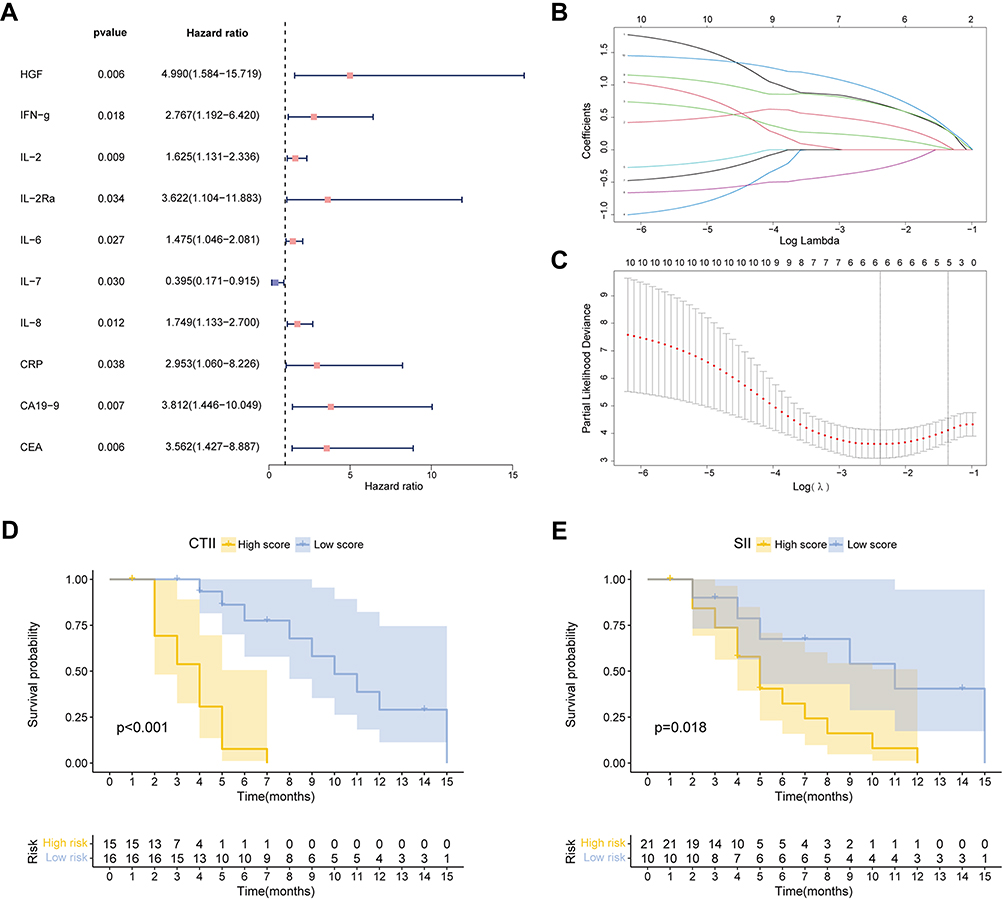 |
Figure 3 Identification of prognostic factors and construction of the circulating tumor-associated inflammatory index (CTII). (A) Forest plot of univariate Cox regression analysis showed that 10 factors were associated with prognosis of PCLM. (B) The coefficient profiles of the least absolute shrinkage and selection operator (LASSO) regression. (C) Selection of the tuning parameter (lambda) in the LASSO model by 10-fold cross-validation based on minimum criteria for OS. The Kaplan–Meier (K–M) curves for the OS of patients in the training cohort based on CTII (D) and SII (E). |
Prognostic Significance of the CTII
According to the univariate Cox analysis, age (HR = 1.060, 95% CI 1.004 to 1.119, P = 0.037) and CTII (HR = 5.771, 95% CI 2.749 to 12.116, P < 0.001) were prognostic factors for OS (Figure 4A). In addition, multivariate Cox validated the CTII as an independent prognostic factor (HR = 4.767, 95% CI 2.088 to 10.885, P < 0.001) in a variety of clinical features (Figure 4B). To describe the accuracy of the predictive index, the prognostic value of CTII and SII on OS were further compared with time-dependent ROC. The AUCs of CTII were 0.95, 0.90 and 0.92 for 4, 6 and 8-month OS, respectively (Figure 4C). However, the AUCs of SII were 0.52, 0.59 and 0.64, which were significantly lower than that of CTII (Figure 4D).
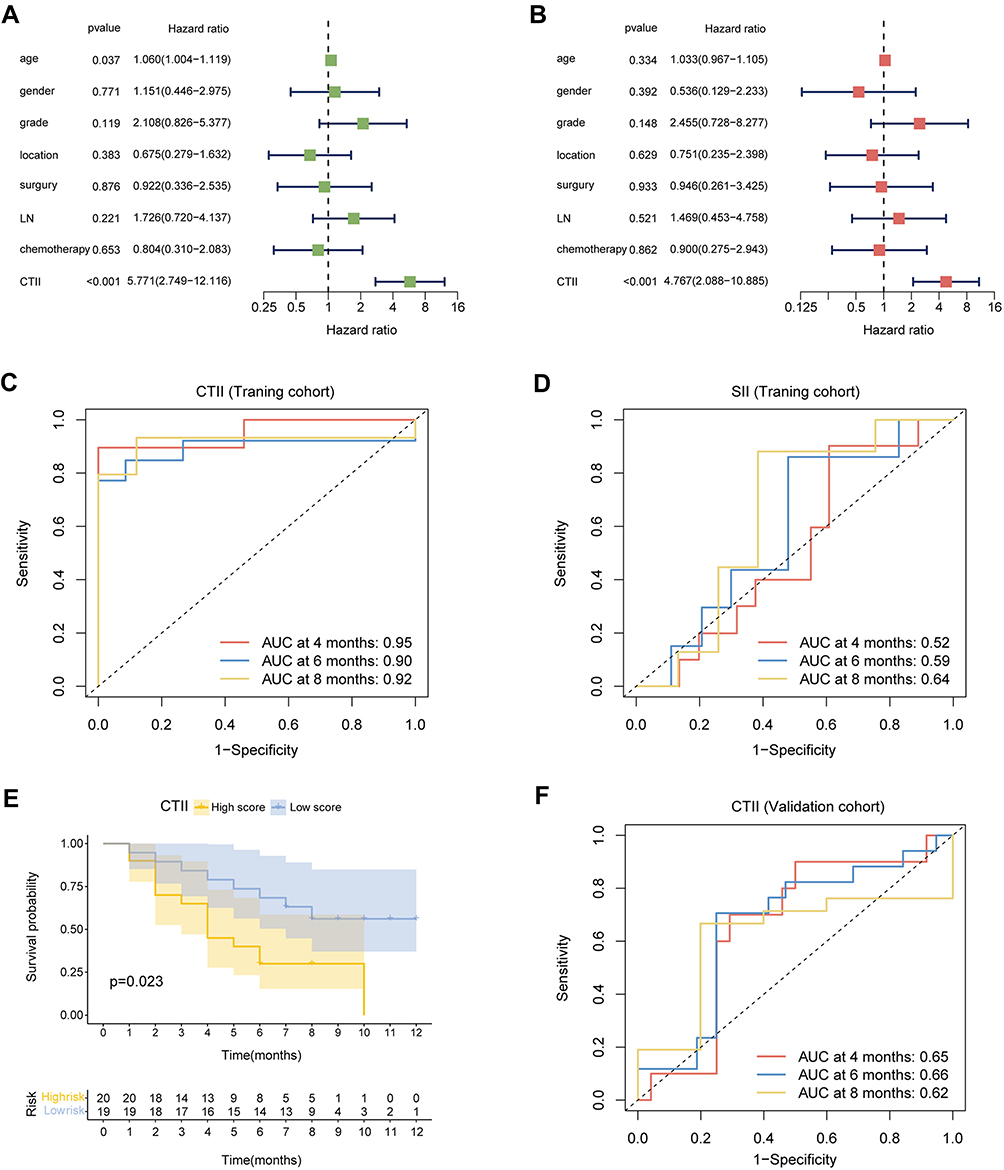 |
Figure 4 Independence and accuracy of the prognostic CTII. Forest plot of univariate (A) and multivariate (B) Cox regression analysis showed that CTII was an independent factor for prognosis. The ROC curves of the CTII (C) and SII (D) in the training cohort. (E) The K–M curves for the OS of patients in the validation cohort based on CTII. (F) The ROC curves of the CTII in the validation cohort. |
Validation of the CTII
The stability of the model was evaluated by a validation cohort based on ELISA data. The K-M analysis showed that CTII was capable of differentiating patients in validation cohorts with different outcomes (P = 0.023, Figure 4E). The AUCs of CTII were 0.65, 0.66 and 0.62 for 4, 6 and 8-month OS, respectively (Figure 4F).
Discussion
In this study, a novel circulating tumor-associated inflammatory index (CTII) was constructed based on inflammatory factors microarray assay and proved to be an independent predictor of OS in patients receiving ablation. The AUC values of CTII were all >0.90, which were higher than that of previous reference model SII based on complete blood counts. Conveniently, CTII measurements are noninvasive and provide the opportunity to be performed routinely in the clinic. Such a model that can distinguish OS is in line with the trend of personalized medicine and can provide optimal decision-making prior to treatment.
Studies have been indicated that the tumor microenvironment in pancreatic cancer showed two main characteristics, including tumor-promoting inflammation and tumor-suppressive immunity, which results in insusceptibility to immunotherapy.15,16 As one of the few local treatments that could be conducted other than systemic chemotherapy in PCLM, ablation has been reported to exhibit immunomodulatory effects on patients with advanced cancer, promoting the expression of pro-inflammatory cytokines and immunosuppressive cytokines and inducing the release of tumor antigens.6 Studies have confirmed that the combination of radiofrequency ablation (RFA) and anti-PD-1 antibody significantly enhances the T-cell immune response.17 Moreover, RFA has an abscopal effect on distal non-RFA tumors, therefore reshaping the tumor immune microenvironment.18 We found that many circulating inflammatory factors were significantly higher in patients with PCLM than in normal controls, suggesting that patients with different levels of circulating inflammation may have different benefits from ablation.
As a composite index based on circulating inflammatory factors and tumor biomarkers, the CTII was non-invasive and highly accurate. Combined with inflammatory cytokines HGF, IL-2, IL-7 and IFN-γ and serum tumor biomarkers CA19-9 and CEA, our CTII improved the prediction ability of survival in patients with PCLM. Recent studies have found that IL-2 not only maintains Treg cells to suppress the immunosuppression but also stimulates conventional T cells to promote the immune response.19 And the cytokine IL-7 are essential for the differentiation and maintenance of T cells.20 IFN-γ is associated with tumor immune surveillance and cytotoxicity. Multiple tumor-derived cytokines in pancreatic cancer can be inhibited by IFN-γ, and IFN-γ has been shown to improve the efficacy of PD-1 blocking therapy by blocking the CXCL8-CXCR2 axis and blocking macrophage transport.21 Additionally, HGF was reported to distinguish pancreatic cancer patients from benign disease.22 Elevated serum HGF level is associated with the progression of pancreatic cancer, and HGF/mesenchymal-epithelial transition factor (c-MET) pathway has been found to play a role in metastasis and chemotherapy resistance, as well as in the immune response, mainly by regulating the function of dendritic cells.23,24
A prospective trial found that levels of prediagnostic inflammatory biomarkers including CRP, IL-6 and TNF-αR2 were inversely associated with survival of pancreatic cancer.25 Unlike these studies, we used Lasso regression as machine learning to avoid multicollinearity and model overfitting and used Lasso coefficients as scoring weights rather than averaging the bisection to each factor. To the best of our knowledge, no such large-scale microarray assay has been performed for PCLM.
The universality of SII has been demonstrated in hepatocellular carcinoma,13 colorectal cancer,26 breast cancer,27 gastric cancer,28 renal cell carcinoma29 and advanced non-small cell lung cancer,30 and SII after neoadjuvant therapy was also reported to be a prognostic factor for resectable pancreatic cancer.31 To investigate prognostic biomarkers for patients receiving immune checkpoint blocking treatment, baseline SII, rather than post-treatment SII, was found to be an independent prognostic indicator for patients with pancreatic cancer.32 And our previous studies have also demonstrated the potential of SII in advanced pancreatic cancer.14 In this study, our cohort once again validated the association between SII and prognosis in PCLM. However, its AUC value was much lower than that of our newly developed CTII in this study. This suggested that more comprehensive levels of inflammatory cytokines can reflect patient outcomes more accurately.
This study has several limitations that could be improved. Further large-scale multicenter validation cohort can prove the applicability of the model. A prospective cohort study of changes in circulating inflammatory factors before and after treatment may yield richer conclusions. And the biological analysis of inflammatory factors obtained in this study may further explore the underlying mechanism.
Conclusion
In summary, we identified circulating biomarkers before ablation that predict survival in patients with liver metastases from pancreatic cancer and constructed a circulating tumor-associated inflammatory index. The index could accurately predict the prognosis of PCLM patients and hopefully guide subsequent treatment strategies.
Data Sharing Statement
The data analyzed in this study are available from the corresponding author (Hao Chen) on reasonable requests.
Acknowledgments
The authors thank the participating patients for the source of clinical blood samples.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Nature Science Foundation of China (NO. 81973616).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Khalaf N, El-Serag HB, Abrams HR, Thrift AP. Burden of pancreatic cancer: from epidemiology to practice. Clin Gastroenterol Hepatol. 2021;19(5):876–884. doi:10.1016/j.cgh.2020.02.054
3. Gupta R, Amanam I, Chung V. Current and future therapies for advanced pancreatic cancer. J Surg Oncol. 2017;116(1):25–34. doi:10.1002/jso.24623
4. Liu M, Wang M, Li S. Prognostic factors of survival in pancreatic cancer metastasis to liver at different ages of diagnosis: a SEER population-based cohort study. Front Big Data. 2021;4:654972. doi:10.3389/fdata.2021.654972
5. Oweira H, Petrausch U, Helbling D, et al. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: a Surveillance Epidemiology and End Results database analysis. World J Gastroenterol. 2017;23(10):1872–1880. doi:10.3748/wjg.v23.i10.1872
6. Qian L, Shen Y, Xie J, Meng Z. Immunomodulatory effects of ablation therapy on tumors: potentials for combination with immunotherapy. Biochim Biophys Acta Rev Cancer. 2020;1874(1):188385. doi:10.1016/j.bbcan.2020.188385
7. Yousaf MN, Ehsan H, Muneeb A, et al. Role of radiofrequency ablation in the management of unresectable pancreatic cancer. Front Med. 2020;7:624997. doi:10.3389/fmed.2020.624997
8. Tranberg K-G. Local destruction of tumors and systemic immune effects. Front Oncol. 2021;11:708810. doi:10.3389/fonc.2021.708810
9. Schneider T, Sevko A, Heussel CP, et al. Serum inflammatory factors and circulating immunosuppressive cells are predictive markers for efficacy of radiofrequency ablation in non-small-cell lung cancer. Clin Exp Immunol. 2015;180(3):467–474. doi:10.1111/cei.12596
10. Park JB, Kim YH, Kim J, et al. Radiofrequency ablation of liver metastasis in patients with locally controlled pancreatic ductal adenocarcinoma. J Vasc Interv Radiol. 2012;23(5):635–641. doi:10.1016/j.jvir.2012.01.080
11. Yan X, Ning Z-Y, Wang P, et al. Combined ablation-chemotherapy versus chemotherapy alone for pancreatic cancer with liver metastasis: a propensity score matching study. Expert Rev Gastroenterol Hepatol. 2021;15(9):1047–1056. doi:10.1080/17474124.2021.1869937
12. Yako YY, Kruger D, Smith M, Brand M. Cytokines as biomarkers of pancreatic ductal adenocarcinoma: a systematic review. PLoS One. 2016;11(5):e0154016. doi:10.1371/journal.pone.0154016
13. Hu B, Yang X-R, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
14. Zhang K, Hua Y-Q, Wang D, et al. Systemic immune-inflammation index predicts prognosis of patients with advanced pancreatic cancer. J Transl Med. 2019;17(1):30. doi:10.1186/s12967-019-1782-x
15. Li Y, Wang J, Wang H, Zhang S, Wei Y, Liu S. The interplay between inflammation and stromal components in pancreatic cancer. Front Immunol. 2022;13:850093. doi:10.3389/fimmu.2022.850093
16. Hamada S, Masamune A, Shimosegawa T. Inflammation and pancreatic cancer: disease promoter and new therapeutic target. J Gastroenterol. 2014;49(4):605–617. doi:10.1007/s00535-013-0915-x
17. Shi L, Chen L, Wu C, et al. PD-1 blockade boosts radiofrequency ablation-elicited adaptive immune responses against tumor. Clin Cancer Res. 2016;22(5):1173–1184. doi:10.1158/1078-0432.CCR-15-1352
18. Fei Q, Pan Y, Lin W, et al. High-dimensional single-cell analysis delineates radiofrequency ablation induced immune microenvironmental remodeling in pancreatic cancer. Cell Death Dis. 2020;11(7):589. doi:10.1038/s41419-020-02787-1
19. Abbas AK, Trotta E, Simeonov RD, Marson A, Bluestone JA. Revisiting IL-2: biology and therapeutic prospects. Sci Immunol. 2018;3(25). doi:10.1126/sciimmunol.aat1482
20. Barata JT, Durum SK, Seddon B. Flip the coin: IL-7 and IL-7R in health and disease. Nat Immunol. 2019;20(12):1584–1593. doi:10.1038/s41590-019-0479-x
21. Zhang M, Huang L, Ding G, et al. Interferon gamma inhibits CXCL8-CXCR2 axis mediated tumor-associated macrophages tumor trafficking and enhances anti-PD1 efficacy in pancreatic cancer. J Immunother Cancer. 2020;8(1):e000308. doi:10.1136/jitc-2019-000308
22. Moosavi F, Giovannetti E, Saso L, Firuzi O. HGF/MET pathway aberrations as diagnostic, prognostic, and predictive biomarkers in human cancers. Crit Rev Clin Lab Sci. 2019;56(8):533–566. doi:10.1080/10408363.2019.1653821
23. Pothula SP, Xu Z, Goldstein D, Pirola RC, Wilson JS, Apte MV. Targeting HGF/c-MET axis in pancreatic cancer. Int J Mol Sci. 2020;21(23):9170. doi:10.3390/ijms21239170
24. Papaccio F, Della Corte CM, Viscardi G, et al. HGF/MET and the immune system: relevance for cancer immunotherapy. Int J Mol Sci. 2018;19(11):3595. doi:10.3390/ijms19113595
25. Yuan C, Morales-Oyarvide V, Khalaf N, et al. Prediagnostic inflammation and pancreatic cancer survival. J Natl Cancer Inst. 2021;113(9):1186–1193. doi:10.1093/jnci/djab040
26. Dong M, Shi Y, Yang J, et al. Prognostic and clinicopathological significance of systemic immune-inflammation index in colorectal cancer: a meta-analysis. Ther Adv Med Oncol. 2020;12:1758835920937425. doi:10.1177/1758835920937425
27. Zhu M, Chen L, Kong X, et al. The systemic immune-inflammation index is an independent predictor of survival in breast cancer patients. Cancer Manag Res. 2022;14:775–820. doi:10.2147/CMAR.S346406
28. Chen L, Yan Y, Zhu L, et al. Systemic immune-inflammation index as a useful prognostic indicator predicts survival in patients with advanced gastric cancer treated with neoadjuvant chemotherapy. Cancer Manag Res. 2017;9:849–867. doi:10.2147/CMAR.S151026
29. Jin M, Yuan S, Yuan Y, Yi L. Prognostic and clinicopathological significance of the systemic immune-inflammation index in patients with renal cell carcinoma: a meta-analysis. Front Oncol. 2021;11:735803. doi:10.3389/fonc.2021.735803
30. Alifano M. Systemic immune-inflammation index and prognosis of advanced non-small cell lung cancer. Ann Transl Med. 2020;8(11):667. doi:10.21037/atm.2020.03.174
31. Murthy P, Zenati MS, Al Abbas AI, et al. Prognostic value of the Systemic Immune-Inflammation Index (SII) after neoadjuvant therapy for patients with resected pancreatic cancer. Ann Surg Oncol. 2020;27(3):898–906. doi:10.1245/s10434-019-08094-0
32. Shang J, Han X, Zha H, et al. Systemic immune-inflammation index and changes of neutrophil-lymphocyte ratio as prognostic biomarkers for patients with pancreatic cancer treated with immune checkpoint blockade. Front Oncol. 2021;11:585271. doi:10.3389/fonc.2021.585271
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Variant Angina is Associated with Myocarditis
Xu X, Wang JJ, Zhao H, Miao K, Cui G, Zhang Y, Yang X, Wang L, Wu J, Wang DW
Journal of Inflammation Research 2022, 15:4939-4949
Published Date: 29 August 2022
Associations of Inflammation with Risk of Cardiovascular and All-Cause Mortality in Adults with Hypertension: An Inflammatory Prognostic Scoring System
Cheang I, Zhu X, Lu X, Yue X, Tang Y, Gao R, Liao S, Yao W, Zhou Y, Zhang H, Yiu KH, Li X
Journal of Inflammation Research 2022, 15:6125-6136
Published Date: 8 November 2022
Special Focus on the Cellular Anti-Inflammatory Effects of Several Micro-Immunotherapy Formulations: Considerations Regarding Intestinal-, Immune-Axis-Related- and Neuronal-Inflammation Contexts
Jacques C, Floris I
Journal of Inflammation Research 2022, 15:6695-6717
Published Date: 13 December 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023