Back to Journals » Journal of Inflammation Research » Volume 19
The Impact of Preoperative Inflammatory Activity in Patients with Ankylosing Spondylitis on Postoperative Joint Function: A Retrospective Cohort Study
Authors Man SL, Ji XJ, Ding YY, Li HC, Guo SY, Bian T, Zhang L
Received 30 October 2025
Accepted for publication 5 January 2026
Published 4 February 2026 Volume 2026:19 576376
DOI https://doi.org/10.2147/JIR.S576376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ujjwol Risal
Si-Liang Man,1 Xiao-Jian Ji,2 Ying-Yue Ding,1 Hong-Chao Li,1 Shao-Yi Guo,2 Tao Bian,2 Liang Zhang3
1Department of Rheumatology, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China; 2Department of Rheumatology, Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China; 3Department of Orthopedic Surgery, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China
Correspondence: Liang Zhang, Department of Orthopedic Surgery, Beijing Jishuitan Hospital, Capital Medical University, No. 31 Xinjiekou East Street, Xicheng District, Beijing, 100035, People’s Republic of China, Tel +8601050963066, Email [email protected]
Background: The relationship between preoperative inflammatory activity and postoperative functional outcomes following total hip arthroplasty (THA) in patients with ankylosing spondylitis (AS) has not been fully elucidated. This study aimed to evaluate the predictive value of preoperative inflammatory markers for postoperative functional outcomes in patients with AS undergoing THA.
Methods: Employed a retrospective research method. A total of 541 AS patients (739 hips) who underwent primary THA between 2003 and 2019 were analyzed. Preoperative inflammatory markers, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), fibrinogen (FIB), and D-dimer (D-D), were measured. Functional outcomes were assessed using the Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and Harris Hip Score (HHS).
Results: Patients with higher baseline ESR levels experienced greater functional improvement postoperatively. Specifically, a higher baseline ESR was associated with an increased probability of BASFI improvement, with an adjusted relative risk of 0.72 per unit increase in ln(ESR). Clinically meaningful improvements were observed, with BASFI decreasing by an average of 18.5 points and HHS increasing by 46.2 points, both exceeding minimal clinically important differences.
Conclusion: These findings suggest that elevated preoperative inflammatory markers, particularly ESR, are not contraindications for THA in AS patients. Instead, they may indicate a greater capacity for postoperative functional recovery. The study supports a proactive surgical approach in appropriately selected AS patients, emphasizing the need for individualized assessment and consideration of systemic inflammation as a potential marker of postoperative improvement rather than a barrier to surgical intervention. These insights could refine surgical decision-making and optimize timing for THA in AS patients.
Keywords: ankylosing spondylitis, CRP, D-dimer, ESR, fibrinogen, inflammatory markers, total Hip arthroplasty
Introduction
Ankylosing spondylitis (AS), also referred to as radiographic axial spondyloarthritis, is a chronic inflammatory rheumatic disorder that predominantly affects the axial skeleton and sacroiliac joints. The estimated global prevalence ranges from 0.1% to 1.4%.1 Hip joint involvement has been reported in approximately 24%–36% of patients with AS, often resulting in substantial functional limitation and decreased quality of life.2,3 Multicenter investigations have indicated that hip arthritis in patients with AS is frequently bilateral, occurring in up to 90% of cases, and may progress to end-stage hip joint destruction within 5–10 years of disease onset.4
Total hip arthroplasty (THA) has been established as the most effective surgical intervention for patients with AS and end-stage hip involvement, producing significant improvements in pain relief, functional recovery, and quality of life.5 Recent systematic reviews have reported long-term implant survival rates of 85%–95% at 10 years post-THA in this population.6 However, these patients present unique surgical challenges due to their younger age at surgery, altered hip biomechanics, and persistent systemic inflammation.7
Historically, elevated preoperative inflammatory markers, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), fibrinogen (FIB), and D-dimer (D-D), have been considered relative contraindications for major orthopedic surgeries.8 This is based on the theoretical increased risk of perioperative complications, particularly surgical site infection and impaired wound healing.9 A meta-analysis of orthopedic procedures indicated that preoperative CRP levels exceeding 10 mg/L were associated with a 1.8-fold increased risk of surgical site infection in general orthopedic populations.10
The association between preoperative inflammatory status and postoperative functional outcomes in patients with AS undergoing THA remains poorly characterized. Published evidence is inconsistent, with some studies suggesting that disease activity does not necessarily predict poor surgical outcomes.11 This knowledge gap is particularly relevant, as patients with AS frequently exhibit persistently elevated inflammatory markers, even during periods of clinical remission.12
The influence of inflammatory markers on surgical outcomes in AS represents a critical clinical consideration. Although systemic inflammation is a hallmark of active disease, its role as a predictor of postoperative functional recovery remains unclear. This uncertainty may contribute to delays in surgical intervention, potentially affecting the optimal timing of THA.13
The commonly used inflammatory markers for AS in clinical practice include erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), fibrinogen (FIB), and D-dimer (D-D). ESR and CRP are the most commonly used inflammatory biomarkers in clinical practice for monitoring AS disease activity and are recommended by international guidelines including ASAS-EULAR recommendations.14 They are readily available, cost-effective, and routinely measured in preoperative assessment. Fibrinogen is an acute-phase protein that reflects systemic inflammation and has been shown to correlate with disease activity and radiographic progression in AS patients.15 D-dimer reflects both inflammation and hypercoagulability, which are clinically relevant in AS patients undergoing major orthopedic surgery due to increased perioperative thrombotic risk associated with chronic inflammation.16
Consequently, this large-scale, single-center cohort study was conducted to evaluate the relationship between preoperative inflammatory markers and functional improvement following THA in patients with AS. It was hypothesized that elevated preoperative inflammatory markers do not adversely impact postoperative functional outcomes, thereby challenging the traditional perspective that active inflammation should delay surgical intervention.
Methods
Patient Selection
A retrospective cohort study was conducted at Beijing Jishuitan Hospital, National Center for Orthopedics, a tertiary referral center specializing in musculoskeletal disorders, covering the period from January 2003 to October 2019. Patients were selected based on established indications for THA in AS. All participants fulfilled the Modified New York criteria (1984) for AS diagnosis.17
The primary indications for surgery included (1) persistent hip pain refractory to conservative management, including physiotherapy and pharmacological interventions;18,19 (2) significant functional impairment affecting activities of daily living;20 (3) radiographic evidence of advanced hip joint destruction, irrespective of patient age;19 and (4) severe limitation in hip range of motion (ROM) or hip ankylosis.21
Between 2003 and 2019, 902 patients with AS underwent THA at the institution. Of these, 182 patients (20.2%) were excluded due to incomplete baseline data (n = 145, 16.1%) or prior hip resurfacing arthroplasty (n = 37, 4.1%). An additional 79 patients (8.7%) were lost to follow-up despite multiple contact attempts via telephone, email, and WeChat. During data quality control, 100 patients (11.1%) were further excluded owing to incomplete or inconsistent data (n = 65, 7.2%), missing key laboratory parameters exceeding 20% (n = 23, 2.5%), or follow-up duration shorter than 22 months (n = 12, 1.3%).
The final study cohort comprised 541 patients with AS (739 hips) with complete datasets available for analysis (Figure 1). The mean follow-up duration was 30 months (range: 22–247 months). The study protocol received approval from the Institutional Ethics Committee (project number: K2024015-00), and all participants provided informed consent. Data collection was performed by two independent observers who were not involved in surgical interventions or clinical assessments to minimize potential bias.
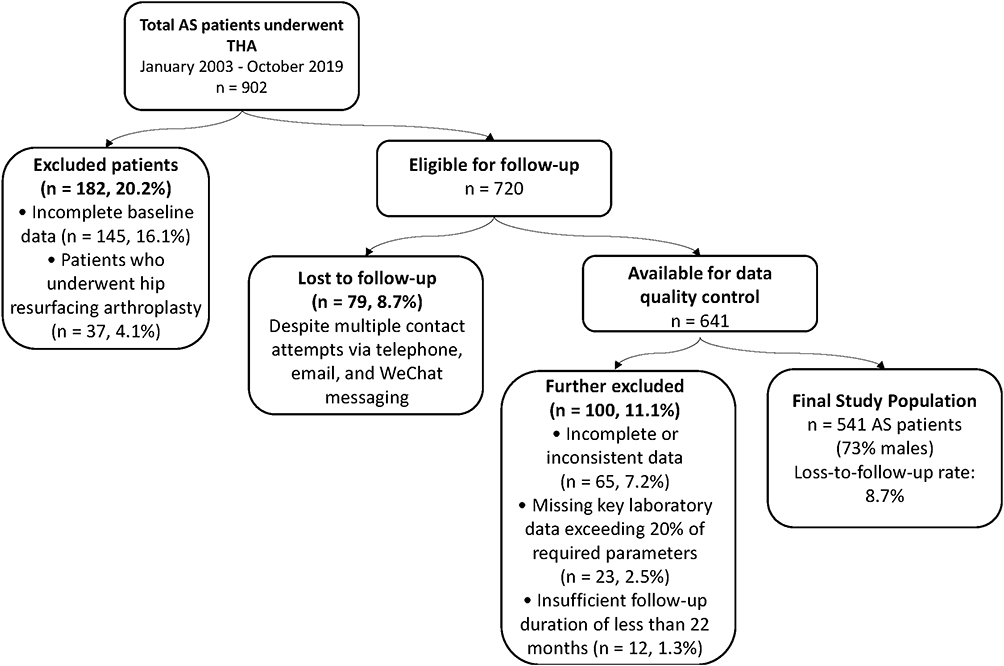 |
Figure 1 Flow diagram illustrating the patient selection process for patients with AS undergoing THA between January 2003 and October 2019. A total of 902 consecutive patients with AS were considered, with final inclusion of 541 patients (739 hips). Abbreviations: AS, ankylosing spondylitis; THA, total hip arthroplasty. |
Clinical and Laboratory Assessments
Demographic variables included age at the time of surgery (years), sex, body mass index (BMI, kg/m2), residence status (urban or rural), employment status, and educational attainment (higher education). Clinical characteristics comprised family history of AS, history of tobacco or alcohol use, age at disease onset (years), age at diagnosis (years), disease duration (years), and extra-articular manifestations including acute anterior uveitis, psoriasis, and inflammatory bowel disease. Prior therapeutic interventions were recorded, including anti-osteoporosis medications, corticosteroids, nonsteroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, and biologic agents.
Preoperative functional status was evaluated through hip flexion contracture (degrees), presence of bony fusion, and ROM (degrees). Disease activity and severity were assessed using standardized instruments, including the Rheumatic Disease Comorbidity Index,22 Bath Ankylosing Spondylitis Disease Activity Index (BASDAI),23 Bath Ankylosing Spondylitis Functional Index (BASFI),24 Physical Component Summary (PCS),25 Mental Component Summary (MCS) of the SF-36,25 Harris Hip Score (HHS),26 and Ankylosing Spondylitis Quality of Life questionnaire (ASQOL).27
Laboratory assessments included white blood cell count (× 109/L), hemoglobin (g/L), lymphocyte count (× 109/L), ESR (mm/hour), CRP (mg/L), serum albumin (g/L), total cholesterol (mmol/L), FIB (g/L), D-D (mg/L), and human leukocyte antigen B27 status.
Surgical parameters documented included surgery type (unilateral, staged bilateral, or simultaneous bilateral), prosthetic femoral head diameter (mm), and bearing surface material combination (ceramic-on-ceramic, ceramic-on-polyethylene, metal-on-polyethylene, or metal-on-metal). All laboratory assessments were conducted according to standardized protocols in the institution’s central laboratory.
Patient Grouping
Patients were categorized into two groups according to the degree of improvement in the BASFI at 24 ± 2 months following total hip arthroplasty. In alignment with clinically meaningful thresholds established in prior studies,28–30 patients who exhibited a BASFI improvement of ≥ 20 were classified as the “good improvement group”, whereas those with a BASFI improvement of < 20 were categorized as the “suboptimal improvement group”. This stratification facilitated the evaluation of variables potentially associated with postoperative functional outcomes following THA in patients with AS. Patients with comorbidities were not excluded; however, laboratory assessments were conducted during clinically stable periods, avoiding acute exacerbations of metabolic, cardiovascular, or other systemic conditions.
Management of Biologic Drug Use
Our institution followed evolving best-practice guidelines for managing immunosuppressive therapies. For surgeries performed before 2017, biologic DMARDs were discontinued at least 1 month prior to surgery. Following publication of the 2017 ACR/AAHKS guideline,31 our practice transitioned to withholding biologic DMARDs for one dosing cycle before surgery and resuming after wound healing. Conventional synthetic DMARDs (csDMARDs) were continued throughout the perioperative period as recommended.
Statistical Analysis
This retrospective cohort study included consecutive patients with AS who underwent primary THA at the institution between January 2003 and October 2019. Of 902 eligible patients, 541 (739 hips) with complete datasets were included in the final analysis after the exclusion of those with incomplete baseline data (n = 145), prior hip resurfacing arthroplasty (n = 37), or loss to follow-up (n = 79).
Statistical analyses were conducted using SPSS software, version 26.0 (IBM Corp., Armonk, NY, USA), and R software, version 4.1.0. The Shapiro–Wilk test was applied to assess the distribution of continuous variables. As most continuous variables did not conform to a normal distribution, they were expressed as medians with interquartile ranges (IQRs) and compared using the Mann–Whitney U-test. Categorical variables were summarized as frequencies and percentages, with comparisons performed using the chi-square test or Fisher’s exact test, as appropriate.
Patients were categorized into two groups according to functional improvement at 24 ± 2 months post-THA: the “good improvement group” (BASFI improvement ≥ 20; n = 337) and the “suboptimal improvement group” (BASFI improvement < 20; n = 402). This cutoff was determined based on previously established thresholds for clinically meaningful improvement in patients with AS.
To examine factors associated with functional improvement, both univariate and multivariate logistic regression analyses were conducted. Variables with a p-value < 0.1 in univariate analysis were included in the multivariate model. Age and gender were retained in the multivariate analysis regardless of statistical significance due to their recognized clinical importance. Results were expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs).
During the preliminary analysis, inflammatory markers, including ESR, CRP, FIB, and D-dimer, exhibited right-skewed distributions, which could have affected the validity of the statistical models. To address this non-normality and enhance model performance, natural logarithmic transformations were applied to these variables (denoted as LnESR, LnCRP, LnFIB, and LnDD). This transformation produced approximately normal distributions and enabled more accurate estimation of their associations with functional outcomes.
The logarithmic transformation also facilitated a more meaningful interpretation of effect sizes, as a one-unit increase on the logarithmic scale corresponds to a multiplicative change in the original scale, thereby better reflecting the biological relationships between inflammatory activity and clinical outcomes. For the inflammatory markers, parallel analyses were performed using both untransformed and logarithmically transformed data to assess robustness. The log-transformed variables demonstrated stronger associations with functional outcomes, exhibiting higher odds ratios and improved statistical significance compared to untransformed values. These findings indicated a non-linear relationship between preoperative inflammatory marker levels and postoperative functional improvement.
All statistical tests were two-sided, and a value of p < 0.05 was considered indicative of statistical significance. Effect sizes for regression analyses were expressed as odds ratios. Graphical representations illustrating the distribution of inflammatory markers across the two outcome groups were generated using GraphPad Prism software, version 9.0.
Results
Baseline Characteristics
Among 739 hips in 541 patients with AS who underwent total hip arthroplasty, 337 hips (45.6%) achieved substantial functional improvement (BASFI improvement ≥ 20), whereas 402 hips (54.4%) demonstrated suboptimal improvement. The cohort was predominantly male (84.2%) with a median age of 35.00 years at the time of surgery.
Patients with greater postoperative functional improvement exhibited significantly higher preoperative inflammatory markers, including ESR (27.00 vs 23.00 mm/hour, p = 0.015), CRP (12.40 vs 9.45 mg/L, p = 0.004), FIB (3.31 vs 3.14 g/L, p = 0.012), and D-D (0.43 vs 0.35 mg/L, p < 0.001).
Additionally, patients with better postoperative outcomes had poorer preoperative functional status, as reflected by lower PCS scores (23.45 vs 27.12, p < 0.001; lower HHS: 39.00 vs 43.00, p < 0.001), greater disease activity (BASDAI: 6.00 vs 5.20, p < 0.001), and greater functional impairment (BASFI: 7.20 vs 5.40, p < 0.001).
Surgical strategies differed significantly between groups (p < 0.001), with the good improvement group undergoing a higher proportion of bilateral procedures (staged: 46.6% vs 37.3%; simultaneous: 12.2% vs 8.0%) and receiving larger femoral head prostheses (p = 0.004) (Table 1 and Figure 2).
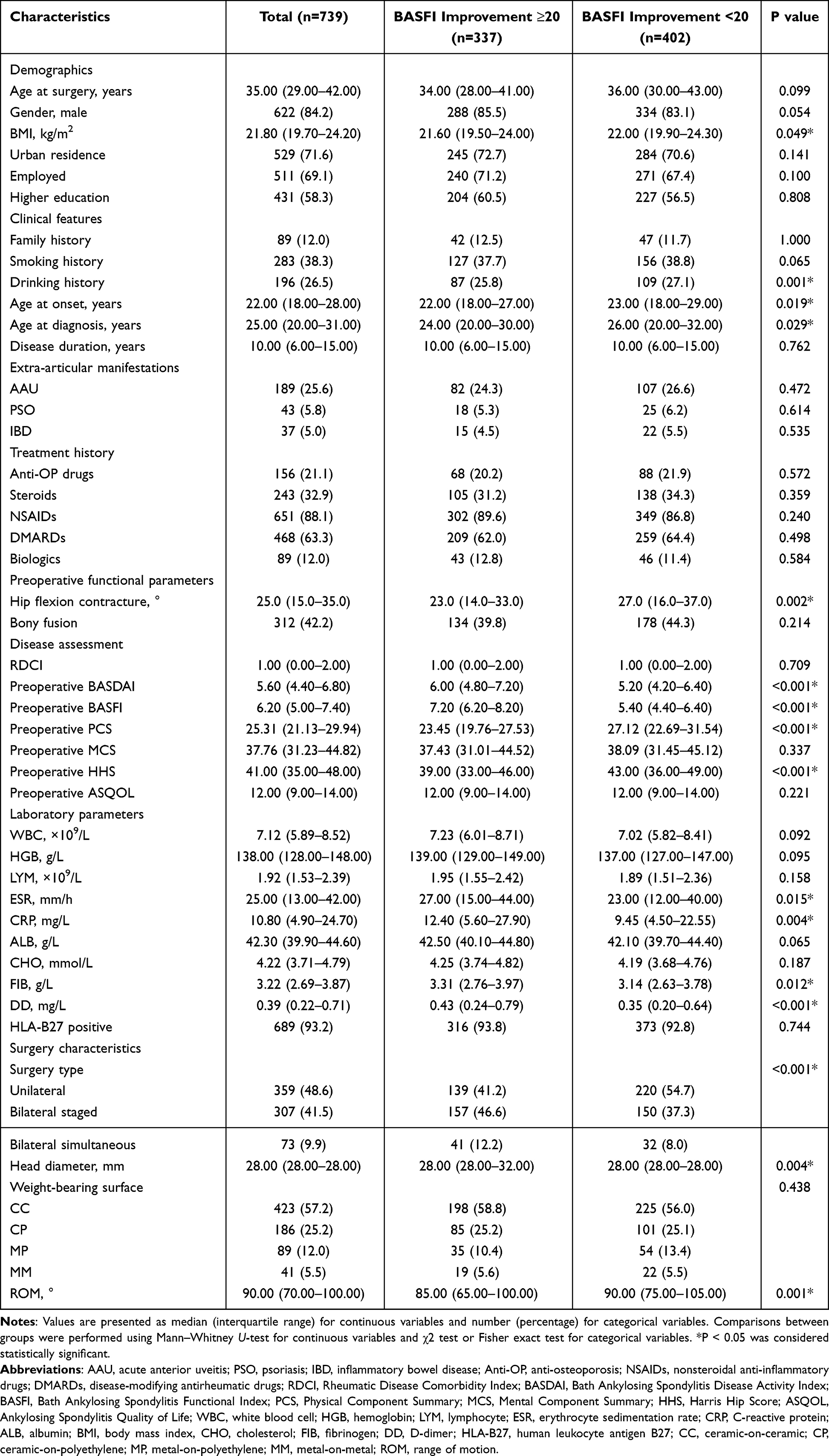 |
Table 1 Baseline Characteristics of Patients According to BASFI Improvement |
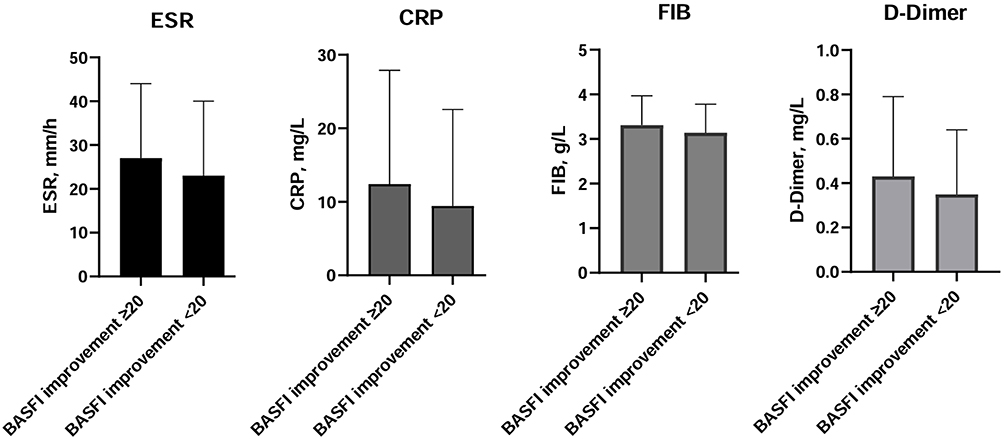 |
Figure 2 Comparison of preoperative inflammatory markers (ESR, CRP, FIB, D-D) between patients achieving good functional improvement (BASFI improvement ≥ 20) and those with suboptimal improvement (BASFI improvement < 20). Abbreviations: ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; FIB, fibrinogen; DD, D-dimer; BASFI, Bath Ankylosing Spondylitis Functional Index. |
The cohort had a median BMI of 21.80 kg/m2 (IQR: 19.70–24.20). Per WHO Asian-Pacific criteria, 12.0% were underweight, 75.0% normal weight, 10.6% overweight, and 2.4% obese. The prevalence of major comorbidities was low: cardiovascular events (4.3%), hypertension (3.8%), fracture history (6.2%), depression (2.0%), and liver disease (2.8%).
Postoperative Outcomes and Patient Satisfaction
At the 24-month follow-up, patients with substantial functional improvement (BASFI improvement ≥ 20) exhibited superior postoperative outcomes and had higher preoperative inflammatory markers. This group demonstrated enhanced hip function, with a greater proportion achieving satisfactory flexion ability (96.7% vs 89.8%, p < 0.001), greater HHS improvement (ΔHHS: 48.00 vs 38.00, p < 0.001), and more effective disease activity control (84.3% vs 59.0% achieving clinically significant BASDAI reduction, p < 0.001).
Quality of life measures consistently favored this group, with greater improvements in ASQoL, PCS, and MCS scores (all p < 0.001). Patient-reported satisfaction was markedly higher, with 39.5% of patients in the good improvement group reporting being “very satisfied” compared with 25.4% in the suboptimal improvement group (p < 0.001) (Table 2).
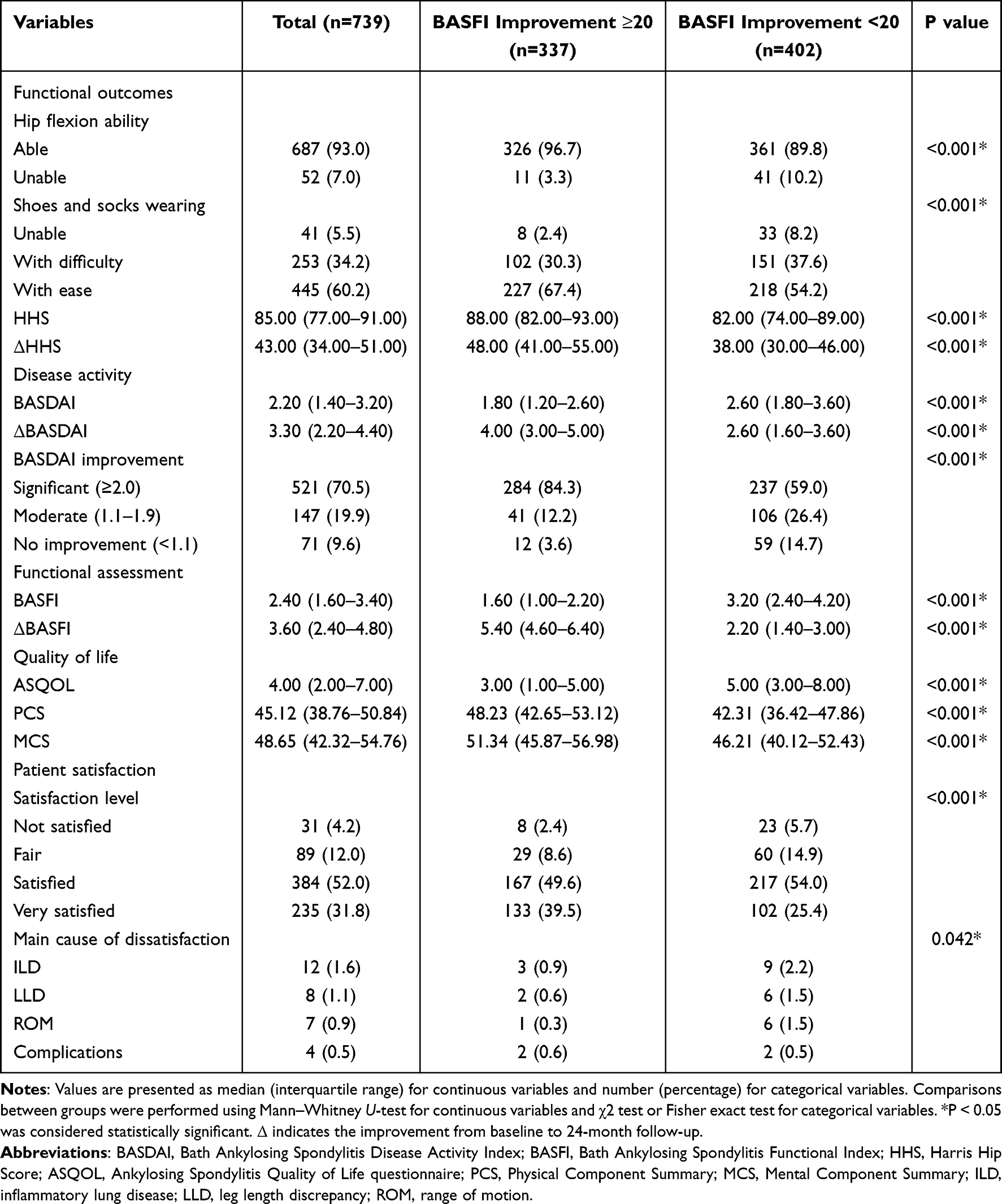 |
Table 2 Postoperative Outcomes at 24-Month Follow-Up According to BASFI Improvement |
These findings indicate that elevated preoperative inflammatory markers, including ESR, CRP, FIB, and D-D, should not be considered contraindications for THA in patients with AS. On the contrary, higher preoperative inflammatory activity may be associated with greater postoperative functional recovery and higher patient satisfaction, challenging conventional assumptions regarding the impact of systemic inflammation on surgical outcomes in this population.
Inflammatory Markers as Predictors of Functional Outcomes
Multivariate regression analysis demonstrated that preoperative inflammatory parameters were independent predictors of functional improvement following THA in patients with AS. Elevated levels of ESR (OR=1.76, 95% CI: 1.28–2.42, p = 0.011), CRP (OR=1.58, 95% CI: 1.17–2.13, p = 0.042), FIB (OR=1.83, 95% CI: 1.31–2.56, p = 0.038), and D-D (OR=1.69, 95% CI: 1.25–2.29, p = 0.035) were each associated with an increased likelihood of achieving a BASFI improvement ≥ 20.
Greater preoperative functional improvement was also observed in patients with poorer preoperative functional status, including higher BASFI scores: OR = 1.86, 95% CI: 1.24–2.78, p = 0.003; higher BASDAI scores: OR = 1.45, 95% CI: 1.07–1.96, p = 0.028; lower HHS: OR = 0.93, 95% CI: 0.87–0.99, p = 0.045). Younger age at surgery (OR = 0.95, 95% CI: 0.91–0.99, p = 0.042) was also significantly associated with better functional outcomes (Table 3). Detailed univariate analysis results are provided in Supplementary Table 1.
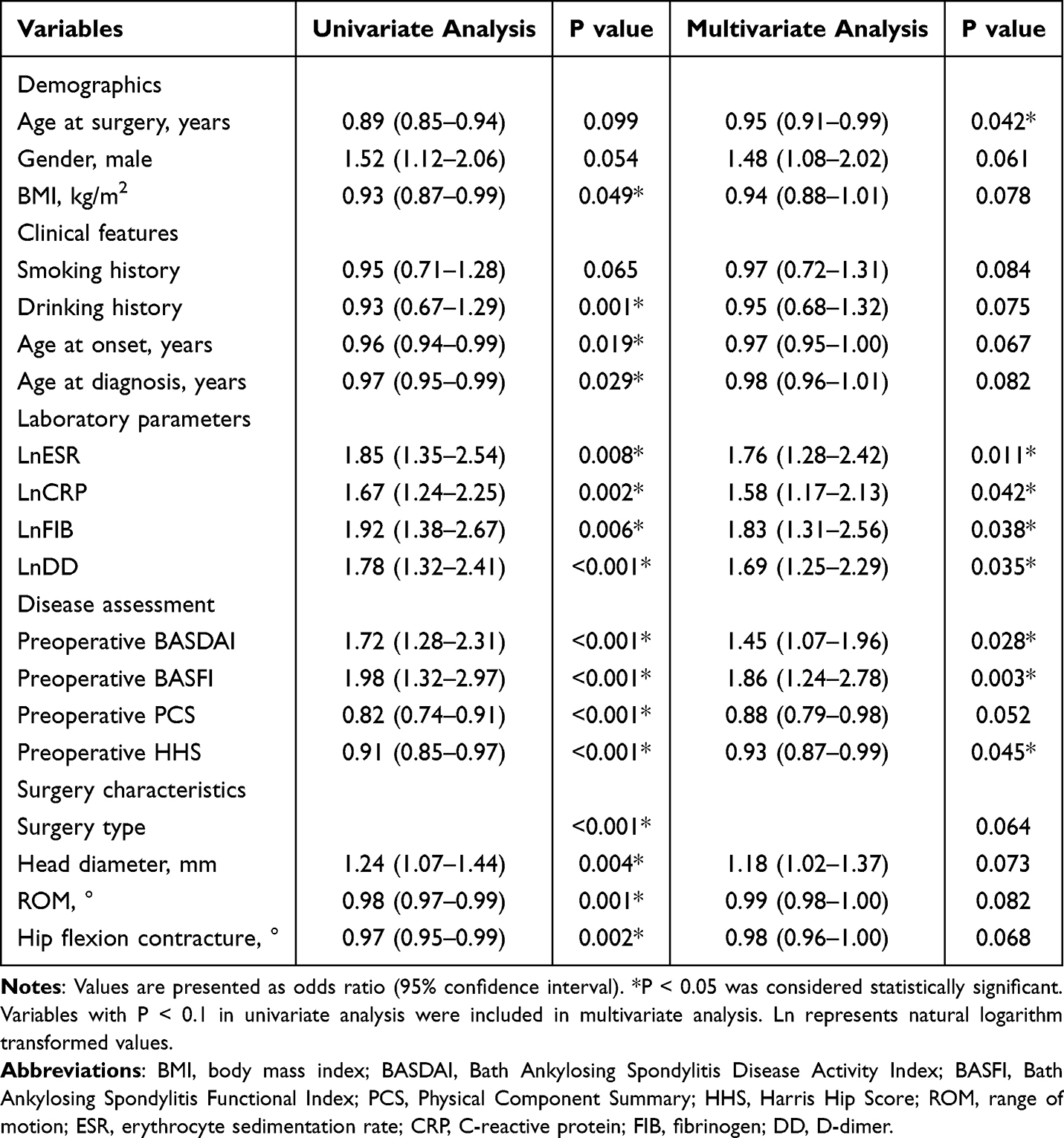 |
Table 3 Univariate and Multivariate Analysis of Factors Associated with BASFI Improvement (Using Natural Logarithm Transformed Variables) |
Subgroup analysis according to biologic therapy use demonstrated consistent functional improvement patterns across treatment profiles. Among patients receiving biologic therapy (n=89, 12.0%), functional outcomes were comparable to those not receiving biologics (n=650, 88.0%). The median BASFI improvement was 3.8 points (IQR: 2.6–5.0) in the biologic group versus 3.5 points (IQR: 2.4–4.7) in the non-biologic group (p=0.612). Similarly, HHS improvement was 44.0 points (IQR: 35.0–52.0) versus 43.0 points (IQR: 34.0–51.0), respectively (p=0.721). The proportion achieving BASFI improvement ≥20 was 48.3% in biologic users and 45.2% in non-users (p=0.584) (Supplementary Table 2).
These functional improvements represent clinically meaningful gains in daily living capacity. A median BASFI improvement of 3.6 points translates to enhanced ability to perform fundamental activities: patients who previously struggled to bend forward to pick up objects from the floor or reach overhead shelves regained these abilities. The median HHS improvement of 43 points reflects transformation from severe functional limitation (preoperative median: 41 points, indicating dependence on assistive devices for ambulation and inability to perform self-care activities) to good functional recovery (postoperative median: 85 points, representing independent ambulation and self-care). Among patients in the good improvement group, 96.7% achieved satisfactory hip flexion ability, and 67.4% could wear shoes and socks with ease—activities that were severely restricted or impossible before surgery.
Discussion
This retrospective cohort study of 541 patients with AS undergoing THA demonstrated an unexpected association between preoperative inflammatory markers and postoperative functional outcomes. Elevated preoperative levels of ESR, CRP, FIB, and D-D were associated with greater functional improvement following THA, thereby challenging conventional assumptions regarding the role of systemic inflammation in surgical decision-making.
All four inflammatory markers—ESR, CRP, FIB, and D-D—exhibited positive associations with postoperative functional recovery. Following logarithmic transformation to account for non-normal distributions, multivariate analysis indicated that higher preoperative levels of these markers were independently associated with an increased likelihood of achieving clinically significant functional improvement (BASFI improvement ≥ 20). These findings contrast with traditional surgical practice, where elevated inflammatory markers have historically been regarded as relative contraindications for elective procedures.32,33
Several potential mechanisms may explain the observed association. First, patients with higher inflammatory activity may constitute a subgroup in which joint destruction is predominantly driven by inflammatory processes rather than mechanical or degenerative changes.12 Braun et al reported that patients with AS and elevated systemic inflammation frequently exhibit functional limitations that are more likely to be reversible compared with those whose impairments result mainly from structural joint damage.34 Second, elevated preoperative inflammatory markers may reflect a greater capacity for functional recovery once a major source of inflammation—the affected hip joint—is surgically addressed.35 This concept aligns with findings by Goodman et al, who observed that patients with inflammatory arthritis and higher preoperative disease activity experienced greater relative functional improvement following arthroplasty, although their study focused primarily on rheumatoid arthritis rather than AS.36
These findings contribute to the growing body of evidence on perioperative management in inflammatory arthritis. Similarly, Zhang et al observed that patients with AS who exhibited distinct inflammatory profiles showed variable functional outcomes following THA, highlighting the complex interactions between systemic inflammation and surgical recovery.37
These observations may have potential clinical implications, suggesting that delaying THA solely based on elevated preoperative inflammatory markers may not always be warranted. Furthermore, preoperative inflammatory profiles could potentially serve as one of several factors to inform discussions regarding expected postoperative functional outcomes.38 However, these potential implications require validation through prospective studies before being applied in clinical practice.
In addition to inflammatory markers, other factors were associated with postoperative functional improvement. Patients with poorer preoperative functional status (higher BASFI, higher BASDAI, lower HHS) experienced greater postoperative gains.
Younger age at surgery was also associated with better functional outcomes, consistent with previous studies indicating that younger patients generally achieve superior recovery following arthroplasty.39 This effect of age may be particularly relevant in AS, in which disease onset typically occurs in early adulthood, and hip involvement often develops within the first decade of disease.40
The relationship between inflammatory markers and other predictors warrants careful consideration. Patients with elevated preoperative inflammatory markers frequently exhibited poorer functional status prior to surgery, indicating a complex interplay of predictive factors. These findings imply that systemic inflammation may function both as a marker of disease severity and, paradoxically, as an indicator of potential for postoperative functional improvement.28
Obesity is known to independently elevate inflammatory markers irrespective of disease activity. However, our cohort was predominantly of normal weight (75.0%), with only 2.4% classified as obese—this demographic distribution minimizes potential obesity-related confounding. Multivariate regression analyses adjusting for BMI were performed, and the results demonstrated that the associations between preoperative inflammatory markers and postoperative functional outcomes remained statistically significant. These findings indicate that the observed relationships primarily reflect AS-related inflammation rather than confounding by obesity-driven systemic inflammation.
Several limitations of this study should be acknowledged when interpreting the findings. The retrospective design introduces potential selection and information biases. Although standardized data collection procedures and consecutive patient inclusion were employed to minimize bias, the retrospective nature precludes definitive causal inference. The cohort comprised patients from a single tertiary referral center specializing in AS, which may limit the generalizability of findings to other clinical settings or populations. The predominance of male patients (84.2%), while reflective of the typical sex distribution in AS, may further restrict extrapolation of the results to female patients. We note key limitations of our inflammatory biomarker panel: ESR, CRP, fibrinogen, and D-dimer are non-specific, unable to differentiate AS-related from other systemic inflammation (eg, infection, obesity). We excluded acute illness/infection and used stable-state measurements, but chronic comorbidity-related inflammation may persist. Future prospective studies with AS-specific biomarkers (IL-17, TNF-α, MMP-3) and imaging could clarify disease-specific inflammation-surgical outcome mechanisms. The extended study period (2003–2019) encompasses evolution in both surgical techniques and medical management strategies, which may introduce heterogeneity.
Although multiple potential confounders were included in the multivariate models, unmeasured factors such as genetic variables, medication adherence, and psychosocial determinants could have influenced outcomes. While adjustments were made for medical therapies, the cumulative effects and interactions of these treatments were not fully captured. Inflammatory markers were assessed at a single preoperative timepoint; serial measurements would have provided greater insight into the dynamic nature of inflammation and its impact on postoperative recovery. Postoperative changes in inflammatory markers were not evaluated, limiting understanding of the relationship between resolution of inflammation and functional improvement. While patients with comorbidities were not excluded, laboratory assessments were performed during clinically stable periods. The low prevalence of major comorbidities (<7% for each condition) minimizes their confounding effect on inflammatory markers. The BASFI used in this study is a comprehensive functional assessment indicator that cannot distinguish whether the postoperative functional improvement is due to hip joint replacement (the target site) or the control of spinal inflammation (an inherent manifestation of AS). This may overestimate the enhancement effect of THA on specific hip joint functions. Future studies can further verify this by combining hip joint-specific scales (such as HOOS). Patients with high preoperative inflammation often have more severe functional impairments (such as higher BASFI scores and lower HHS scores). Their greater postoperative functional improvement may partly result from the “regression to the mean” effect - the natural trend of extreme baseline values approaching the group mean, rather than the inflammation itself promoting recovery. Although multivariate regression adjusted the baseline function, it still could not completely eliminate this confounding factor. The sensitivity analysis of this study for the two subgroups from 2003–2010 and 2011–2019 showed that the association trend between inflammation and functional improvement was consistent (data not shown), but it could not rule out the independent effects of different era prosthesis designs (such as the widespread use of ceramic bearings) and the increase in the use of biological agents on postoperative recovery, which may lead to an overestimation or underestimation of the overall effect.
The definition of “good improvement” (BASFI improvement ≥ 20) was based on established literature; alternative thresholds may yield different results. The BASFI, although widely used, has recognized limitations as an outcome measure, including potential floor and ceiling effects.24 Finally, as with all observational studies, causality between preoperative inflammatory markers and functional outcomes cannot be established. The observed associations may be confounded by unmeasured variables or represent complex relationships that cannot be fully addressed through the applied analytical methods.
These findings underscore several directions for future research. Prospective studies with pre-planned protocols are warranted to further evaluate the relationship between preoperative inflammatory status and postoperative functional outcomes. Such studies should incorporate serial measurements of inflammatory markers both before and after surgery to assess their trajectory and correlation with recovery. Investigating the biological mechanisms underlying these associations may provide insight into the pathophysiology of functional improvement following THA in AS, including analyses of synovial fluid biomarkers, genetic factors, and cellular immune responses. Comparative studies evaluating outcomes in patients with differing inflammatory profiles who undergo early versus delayed surgical intervention could inform optimal timing of THA. Furthermore, examination of the impact of perioperative anti-inflammatory therapies on postoperative outcomes across varying baseline inflammatory states may offer additional guidance for clinical management.
Conclusion
The findings of this study suggest a potential association between elevated preoperative inflammatory markers and improved functional outcomes following THA in patients with AS. Elevated levels of ESR, CRP, FIB, and D-D levels may not necessarily constitute contraindications to surgery. However, in clinical decision-making, it is necessary to avoid relying solely on inflammatory markers. Individualized assessment should be conducted by integrating the patient’s infection risk, the extent of spinal involvement, the use of biologics, and subjective needs. Particularly in long-term follow-up, it is crucial to monitor whether inflammation remains in remission to balance short-term functional benefits with long-term prosthesis survival.
Abbreviations
AS, Ankylosing spondylitis; r-axSpA, Radiographic axial spondyloarthritis; THA, Total hip arthroplasty; ESR, Erythrocyte sedimentation rate; CRP, C-reactive protein; FIB, Fibrinogen; D-D, D-dimer; BASFI, Bath Ankylosing Spondylitis Functional Index; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; HHS, Harris Hip Score; PCS, Physical Component Summary (of SF-36); MCS, Mental Component Summary (of SF-36); ASQoL, Ankylosing Spondylitis Quality of Life; WBC, White blood cell; HGB, Hemoglobin; LYM, Lymphocyte; ALB, Albumin; CHO, Cholesterol; HLA-B27, Human leukocyte antigen B27; BMI, Body mass index; ROM, Range of motion; RDCI, Rheumatic Disease Comorbidity Index; NSAIDs, Nonsteroidal anti-inflammatory drugs; DMARDs, Disease-modifying antirheumatic drugs; OR, Odds ratio; CI, Confidence interval; IQR, Interquartile range; AAU, Acute anterior uveitis; PSO, Psoriasis; IBD, Inflammatory bowel disease; ASDAS, Ankylosing Spondylitis Disease Activity Score; SF-36, 36-Item Short Form Health Survey.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. However, these data are not publicly available due to privacy and ethical restrictions, as they contain information that could compromise research participant privacy/consent. Requests to access the datasets should be directed to the corresponding author ([email protected]), and will require approval from the institutional ethics committee of Beijing Jishuitan Hospital.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University (approval number: K2024015-00). Written informed consent was obtained from all participants before their enrollment in the study.
Acknowledgments
We would like to thank the medical record staff for their assistance with data collection. We appreciate the statistical consultation provided by the Clinical Research Center of Beijing Jishuitan Hospital. We are also grateful to all the patients who participated in this study.
Author Contributions
Si-Liang Man: Conceptualization, Formal analysis, Funding acquisition, Writing – original draft. Xiao-Jian Ji: Formal analysis, Funding acquisition, Writing – review and editing. Ying-Yue Ding: Data curation, Formal analysis, Writing – review and editing. Hong-Chao Li: Data curation, Formal analysis, Writing – review and editing. Shao-Yi Guo: Data curation, Formal analysis, Writing – review and editing. Tao Bian: Data curation, Formal analysis, Writing – review and editing. Liang Zhang: Conceptualization, Writing – review and editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Chronic Disease Management Research Project of National Health Commission Capacity Building and Continuing Education Center (GWJJMB202510025034), the Beijing Natural Science Foundation [number L242143] and the Beijing JST Research Funding [number ZR202416].
Disclosure
None of the authors have any financial disclosure or conflict of interest.
References
1. Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73–14. doi:10.1016/S0140-6736(16)31591-4
2. Ward MM, Deodhar A, Akl EA, et al. American college of rheumatology/spondylitis association of america/spondyloarthritis research and treatment network 2015 recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Rheumatol. 2016;68(2):282–298. doi:10.1002/art.39298
3. Raychaudhuri SP, Deodhar A. The classification and diagnostic criteria of ankylosing spondylitis. J Autoimmun. 2014;48–49:128–133. doi:10.1016/j.jaut.2014.01.015
4. Abdelaal MS, Restrepo C, Sharkey PF. Global perspectives on arthroplasty of hip and knee joints. Orthop Clin North Am. 2020;51(2):169–176. doi:10.1016/j.ocl.2019.11.003
5. Goodman SM, Springer B, Guyatt G, et al. 2017 american college of rheumatology/american association of hip and knee surgeons guideline for the perioperative management of antirheumatic medication in patients with rheumatic diseases undergoing elective total hip or total knee arthroplasty. Arthritis Care Res. 2017;69(8):1111–1124. doi:10.1002/acr.23274
6. Tsai SHL, Lau NC, Chen WC, et al. Total Hip arthroplasty has higher complication rates in stiff spine patients: a systematic review and network meta-analysis. J Orthop Surg Res. 2022;17(1):353. doi:10.1186/s13018-022-03237-8
7. Ahrengart L. Periarticular heterotopic ossification after total hip arthroplasty: Risk factors and consequences. Clin Orthop Relat Res. 1991;263(263):49–58. doi:10.1097/00003086-199102000-00005
8. George MD, Baker JF, Winthrop K, et al. Risk for serious infection with low-dose glucocorticoids in patients with rheumatoid arthritis: a cohort study. Ann Intern Med. 2020;173(11):870–878. doi:10.7326/M20-1594
9. Schnaser EA, Browne JA, Padgett DE, Figgie MP, D’Apuzzo MR. Perioperative complications in patients with inflammatory arthropathy undergoing total hip arthroplasty. J Arthroplasty. 2016;31(10):2286–2290. doi:10.1016/j.arth.2016.03.023
10. Workgroup Convened by the Musculoskeletal Infection Society. New definition for periprosthetic joint infection. J Arthroplasty. 2011;26(8):1136–1138. doi:10.1016/j.arth.2011.09.026
11. Laiho K, Mäenpää H, Kautiainen H, et al. Rise in serum C reactive protein after hip and knee arthroplasties in patients with rheumatoid arthritis. Ann Rheum Dis. 2001;60(3):275–277. doi:10.1136/ard.60.3.275
12. Danve A, O’Dell J. The ongoing quest for biomarkers in Ankylosing Spondylitis. Int J Rheum Dis. 2015;18(8):826–834. doi:10.1111/1756-185X.12779
13. Jämsen E, Varonen M, Huhtala H, et al. Incidence of prosthetic joint infections after primary knee arthroplasty. J Arthroplasty. 2010;25(1):87–92. doi:10.1016/j.arth.2008.10.013
14. Ramiro S, Nikiphorou E, Sepriano A, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. 2023;82(1):19–34. doi:10.1136/ard-2022-223296
15. Cyrus N, Isenberg DA. Biomarkers in axial spondyloarthritis: what is new? Curr Opin Rheumatol. 2021;33(4):322–328. doi:10.1097/BOR.0000000000000804
16. Ungprasert P, Srivali N, Thongprayoon C. Patients with ankylosing spondylitis have an increased risk of deep vein thrombosis and pulmonary embolism: a systematic review and meta-analysis. Mod Rheumatol. 2022;32(2):430–436. doi:10.1093/mr/roab008
17. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984;27(4):361–368. doi:10.1002/art.1780270401
18. Putnis SE, Wartemberg GK, Khan WS, Agarwal S. A literature review of total hip arthroplasty in patients with ankylosing spondylitis: perioperative considerations and outcome. Open Orthop J. 2015;9(1):483–488. doi:10.2174/1874325001509010483
19. Saglam Y, Ozturk I, Cakmak MF, Ozdemir M, Yazicioglu O. Total hip arthroplasty in patients with ankylosing spondylitis: midterm radiologic and functional results. Acta Orthop Traumatol Turc. 2016;50(4):443–447. doi:10.1016/j.aott.2016.06.010
20. Singh A, Telagareddy K, Kumar P, Singh S. Robotic total hip arthroplasty for fused hips in ankylosing spondylitis patients: our experience with robotic arm technology. SICOT J. 2022;8:30. doi:10.1051/sicotj/2022024
21. Joshi AB, Markovic L, Hardinge K, Murphy JC. Total hip arthroplasty in ankylosing spondylitis: an analysis of 181 hips. J Arthroplasty. 2002;17(4):427–433. doi:10.1054/arth.2002.32170
22. Fatima S, Pope JE, Chen LR, et al. Higher comorbidities associated with less improvement in disease activity in early rheumatoid arthritis: results from CATCH cohort. Rheumatology. 2025;64(11):5785–5792. doi:10.1093/rheumatology/keaf350
23. Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A. A new approach to defining disease status in ankylosing spondylitis: the bath ankylosing spondylitis disease activity index. J Rheumatol. 1994;21(12):2286–2291. PMID: 7699630.
24. Calin A, Garrett S, Whitelock H, et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the bath ankylosing spondylitis functional index. J Rheumatol. 1994;21(12):2281–2285. PMID: 7699629.
25. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. PMID: 1593914. doi:10.1097/00005650-199206000-00002
26. Harris WH. Traumatic arthritis of the Hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51(4):737–755. PMID: 5783851. doi:10.2106/00004623-196951040-00012
27. Doward LC, Spoorenberg A, Cook SA, et al. Development of the ASQoL: a quality of life instrument specific to ankylosing spondylitis. Ann Rheum Dis. 2003;62(1):20–26. PMID: 12480664; PMCID: PMC1754293. doi:10.1136/ard.62.1.20
28. Assessment of SpondyloArthritis international Society; Machado P, Landewé R, Lie E, et al. Ankylosing spondylitis disease activity score (ASDAS): defining cut-off values for disease activity states and improvement scores. Ann Rheum Dis. 2011;70(1):47–53. PMID: 21068095. doi:10.1136/ard.2010.138594
29. GO-RAISE investigators; van der Heijde D, Deodhar A, Braun J, et al. The effect of golimumab therapy on disease activity and health-related quality of life in patients with ankylosing spondylitis: 2-year results of the GO-RAISE trial. J Rheumatol. 2014;41(6):1095–1103. PMID: 24737912. doi:10.3899/jrheum.131003
30. Zhao J, Zheng W, Zhang C, Li J, Liu D, Xu W. Radiographic hip involvement in ankylosing spondylitis: factors associated with severe hip diseases. J Rheumatol. 2015;42(1):106–110. PMID: 25362650. doi:10.3899/jrheum.140428
31. Goodman SM, Springer B, Guyatt G, et al. 2017 american college of rheumatology/american association of hip and knee surgeons guideline for the perioperative management of antirheumatic medication in patients with rheumatic diseases undergoing elective total hip or total knee arthroplasty. Arthritis Rheumatol. 2017;69(8):1538–1551. doi:10.1002/art.40149
32. Battistelli S, Fortina M, Carta S, Guerranti R, Nobile F, Ferrata P. Serum C-reactive protein and procalcitonin kinetics in patients undergoing elective total hip arthroplasty. Biomed Res Int. 2014;2014:565080. doi:10.1155/2014/565080
33. Wirtz DC, Heller KD, Miltner O, Zilkens KW, Wolff JM. Interleukin-6: a potential inflammatory marker after total joint replacement. Int Orthop. 2000;24(4):194–196. doi:10.1007/s002640000136
34. Braun J, Baraliakos X, Heldmann F, Kiltz U. Tumor necrosis factor alpha antagonists in the treatment of axial spondyloarthritis. Expert Opin Investig Drugs. 2014;23(5):647–659. PMID: 24654630. doi:10.1517/13543784.2014.899351
35. Baraliakos X, Listing J, Rudwaleit M, Brandt J, Sieper J, Braun J. Radiographic progression in patients with ankylosing spondylitis after 2 years of treatment with the tumour necrosis factor alpha antibody infliximab. Ann Rheum Dis. 2005;64(10):1462–1466. PMID: 15778240; PMCID: PMC1755223. doi:10.1136/ard.2004.033472
36. Goodman SM, Mirza SZ, DiCarlo EF, et al. Rheumatoid arthritis flares after total hip and total knee arthroplasty: outcomes at one year. Arthritis Care Res. 2020;72(7):925–932. doi:10.1002/acr.24091
37. Zhang L, Yang D, Yin X, Zhou Y. Risk factors for poor hip flexion after total hip arthroplasty for the treatment of ankylosing spondylitis a multivariateanalysis. Clin Rheumatol. 2014;33(9):1295–1301. PMID: 24651916. doi:10.1007/s10067-014-2575-5
38. Greidanus NV, Masri BA, Garbuz DS, et al. Use of erythrocyte sedimentation rate and C-reactive protein level to diagnose infection before revision total knee arthroplasty. A prospective evaluation. J Bone Joint Surg Am. 2007;89(7):1409–1416. doi:10.2106/JBJS.D.02602
39. Galloway R, Monnington K, Moss R, Donaldson J, Skinner J, McCulloch R. Satisfaction rates, function, and return to activity following young adult total hip arthroplasty. Bone Jt Open. 2024;5(4):304–311. doi:10.1302/2633-1462.54.BJO-2024-0005.R1
40. Bose VC, Kalaivanan K, Manohar M, Kumar A, Patil S, Suryanarayan P. Is the revision rate higher after hip arthroplasty in teenage patients? A prospective study with long-term follow-up of more than 10 years. Indian J Orthop. 2021;55(4):993–1002. doi:10.1007/s43465-021-00370-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ankylosing Spondylitis Patients Have Lower Risk of Dislocation Following Total Hip Arthroplasty Compared with Patients Undergoing Lumbar Spinal Fusion Surgery
Guan H, Xu C, Fu J, Yang X, Zhang Y, Chen J
International Journal of General Medicine 2022, 15:6573-6582
Published Date: 11 August 2022
Value of Laboratory Indicators in Predicting Pneumonia in Symptomatic COVID-19 Patients Infected with the SARS-CoV-2 Omicron Variant
Zhu K, Ma S, Chen H, Xie J, Huang D, Fu C, Ma G, Huang Y
Infection and Drug Resistance 2023, 16:1159-1170
Published Date: 28 February 2023
The Diagnostic Value of Inflammatory Markers (CRP, IL6, CRP/IL6, CRP/L, LCR) for Assessing the Severity of COVID-19 Symptoms Based on the MEWS and Predicting the Risk of Mortality

Wolszczak-Biedrzycka B, Dorf J, Milewska A, Łukaszyk M, Naumnik W, Kosidło JW, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:2173-2188
Published Date: 22 May 2023
Changes in Anxiety and Depression After THA in Patients with Ankylosing Spondylitis and the Affecting Factors
Qian H, Wang X, Wang P, Zhang G, Liu J, Dang X, Guo J, Liu R
Therapeutics and Clinical Risk Management 2023, 19:675-684
Published Date: 15 August 2023
Inflammatory Markers as Predictors of Diabetes Mellitus in Patients with Pulmonary Tuberculosis: A Retrospective Analysis of Hematological Parameters and Clinical Features
He X, Jiang Y, Hou H, Wu W
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2203-2212
Published Date: 5 July 2025