")
Back to Journals » International Journal of General Medicine » Volume 15
Ankylosing Spondylitis Patients Have Lower Risk of Dislocation Following Total Hip Arthroplasty Compared with Patients Undergoing Lumbar Spinal Fusion Surgery
Authors Guan H, Xu C , Fu J, Yang X, Zhang Y, Chen J
Received 12 May 2022
Accepted for publication 1 August 2022
Published 11 August 2022 Volume 2022:15 Pages 6573—6582
DOI https://doi.org/10.2147/IJGM.S373432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Haitao Guan,1,2,* Chi Xu,2,* Jun Fu,2,* Xue Yang,2 Yingze Zhang,3 Jiying Chen2
1School of Medicine, Nankai University, Tianjin, People’s Republic of China; 2Department of Orthopedic Surgery, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Department of Orthopedic Surgery, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiying Chen, Department of Orthopedic Surgery, Chinese PLA General Hospital, No. 28 Fuxing Road, Haidian District, Beijing, 100853, People’s Republic of China, Email [email protected] Yingze Zhang, Department of Orthopedic Surgery, The Third Hospital of Hebei Medical University, No. 139 Ziqiang Road, Qiaoxi District, Shijiazhuang, 050051, Hebei, People’s Republic of China, Email [email protected]
Purpose: Patients undergoing lumbar spinal fusion (LSF) surgery and patients with ankylosing spondylitis (AS) have concomitant pathology of hip and lumbosacral spine. The purpose of our study is to compare the dislocation rate following total hip arthroplasty (THA) between patients with LSF and AS and reveal the differences of lumbar fusion secondary to LSF and AS.
Patients and methods: Fifty-nine patients (73 hips) were included in Group LSF and every patient was matched with two patients in Group AS. Follow-ups were conducted for information of surgical prognosis and dislocation events following THA. Multiple anatomic parameters were measured on preoperative and postoperative radiological images.
Results: The dislocation rate of patients in Group AS (0.68%) was obviously lower than that of patients in Group LSF (4.11%) and the hazard ratio of dislocation events following THA reached 6.1. Considering the low calculated power (1-β, 0.24), we supposed insufficient statistical evidence (p=0.118) could be attributed to small sample size. Postoperative hip flexion range of motion (ROM) in Group AS (102.1°± 24.5°) was significantly lower than that in Group LSF (117.4°± 14.2°) (p< 0.0005). Postoperative flexion ROM of lumbar was also significantly lower in Group AS (p< 0.001). There was no significant difference between two groups concerning postoperative acetabular inclination (p=0.988) and anteversion (p=0.25). However, patients in Group AS had a significantly lower sacral slope (p=0.025) and higher pelvic tilt (p< 0.0005) than patients in Group LSF after THA.
Conclusion: Patients with AS have a lower risk of dislocation after THA compared with patients undergoing LSF. The lower risk is significantly relevant to severer stiffness and lower mobility along the spine–pelvis-–hip axis in AS patients after THA. Acetabular orientation has no significant effect on the difference of dislocation rate between patients with LSF and AS.
Keywords: ankylosing spondylitis, lumbar spinal fusion, total hip arthroplasty, dislocation, range of motion
Introduction
Total hip arthroplasty (THA) is a secure and effective therapeutic method for end-stage hip disease.1,2 With the aging of populations in human society, patients who undergo THA for osteoarthritis or osteonecrosis of the femoral head could suffer from degenerative change of the lumbosacral spine as well.3,4 Lumbar spinal fusion (LSF) surgery is a feasible treatment for patients diagnosed with degenerative lumbar disease. Several studies have recognized that LSF surgery prior to THA has a significant effect on dislocation events and revision surgery following THA.5–7 However, the influence of prior LSF surgery on the outcomes of THA has not been hitherto explained clearly. There is growing evidence that increased dislocation rate could be attributed to subtle changes of spinopelvic biomechanics, the range of lumbar motion, and even acetabular orientation following LSF surgery.5,8,9
Ankylosing spondylitis (AS) is a common chronic spondyloarthritis that progressively affects the axial spine, lumbosacral joints, and hip joints.10,11 The patients who fail to control progression of disease with drugs could eventually suffer from severe hip joint lesions, and THA surgeries are needed for them to improve joint function. Similarly, an elevated dislocation rate following THA among AS patients has been demonstrated in some studies.12 However, some other studies have reported the controversial conclusion that periprosthetic hip dislocation rarely occurs after THA among AS patients.11
We recognized that there is a certain similarity between patients undergoing LSF surgery and that with AS. AS and LSF surgery could both lead to lumbosacral spinal fusion, which would contribute to a certain degree of spinal stiffness and decreased range of lumbar motion universally.9,13,14 The spinal stiffness would certainly change the spinopelvic biomechanics and exert influence on dislocation events following THA.9,15 Nevertheless, the difference between AS and LSF surgery is equally evident. LSF surgery fixes only two segments or some certain segments involved in the surgery and has relatively less impact on other segments. AS would progressively affect all the spinal segments including cervical spine, thoracic spine, and sacroiliac joint, and the autoimmune disease directly invades hip joints pre-operatively and post-operatively.
We hypothesized that the spinal fusion resulting from LSF surgery and AS could exert a similar influence on hip joints and affect the dislocation rate following THA in the same way. Meanwhile, it can be predicted that the fundamental difference in the pattern of lumbar fusion could also make a huge difference in the dislocation rate following THA between LSF and AS patients. Few articles have clarified the relationship between LSF surgery and AS yet. The goal of our study was to compare the dislocation rate following THA between patients with LSF surgery and AS. We sought to reveal the differences and similarities between LSF surgery and AS and explained them as well as possible.
Methods
Patient Population
Between January 2012 and May 2017, there were 4,186 patients who underwent hip surgery in our hospital. Patients aged over 18 who underwent primary THA were included in our study. Patients undergoing hemiarthroplasty, hip resurfacing arthroplasty, dual mobility, constrained THA, and revision surgery were excluded.
The patients included in our study were divided into two groups. Group LSF was composed of patients undergoing primary THA before or after LSF surgery. Spinal fusion levels of Group LSF’s patients could be allowed to involve in thoracic spine and sacral vertebrae, however, patients only with cervical spinal fusion or thoracic spinal fusion were excluded from Group LSF. Group AS was composed of patients diagnosed with AS prior to THA. AS patients with severe kyphosis (Cobb angle >40°) or undergoing any spinal surgery before THA were excluded from Group AS. AS patients with unaffected lumbar motion were also excluded.
A total of 59 patients (73 hips) were identified in Group LSF. Four hundred patients were in accordance with the inclusive criteria of Group AS. For each joint in Group LSF, it was matched with two joints in Group AS. Matching criteria of Group AS was surgical year, BMI (body mass index), surgical approach, femoral head diameter, and the experience of surgeons. Because patients with AS are obviously more likely to be male and younger at the time of surgery, we had to give up performing matching with Group AS based on gender and age. Surgical year was defined as the year of the later between THA and LSF surgery in Group LSF and the year of THA in Group AS.
Data Collection
For all the patients included in our study, we conducted a retrospective review of medical records and radiological images with the approval of the institutional review board. We did careful follow-up surveys for every patient by telephone to acquire the outcome of dislocation and other prognostic information of THA.
The primary outcome was the incidence of dislocation events following THA. The information of dislocation events could be collected by follow-ups and reviews of medical records. Secondary outcomes included the occurrence of revision surgeries or other hip joint surgeries following THA, and some prognostic information of THA, such as Harris Hip Score (HHS) and postoperative flexion ROM of hip and lumbar.
We made some accurate measurements on radiological images of every patient. All measurements were conducted by two experienced orthopedic surgeons and the repeated measurements were averaged for the final values. The acetabular inclination and anteversion were measured on postoperative standing anteroposterior (AP) pelvis radiograph (Figure 1). Bilateral femoral offset (FO), acetabular offset (AO), and abductor lever arm were measured on preoperative and postoperative standing anteroposterior (AP) pelvis radiograph (Figure 2). The sagittal alignment parameters, including sacral slope (SS), pelvic tilt (PT), and pelvic incidence (PI), were measured on postoperative standing lateral spinopelvic radiographs (Figure 3).5,9,16–19
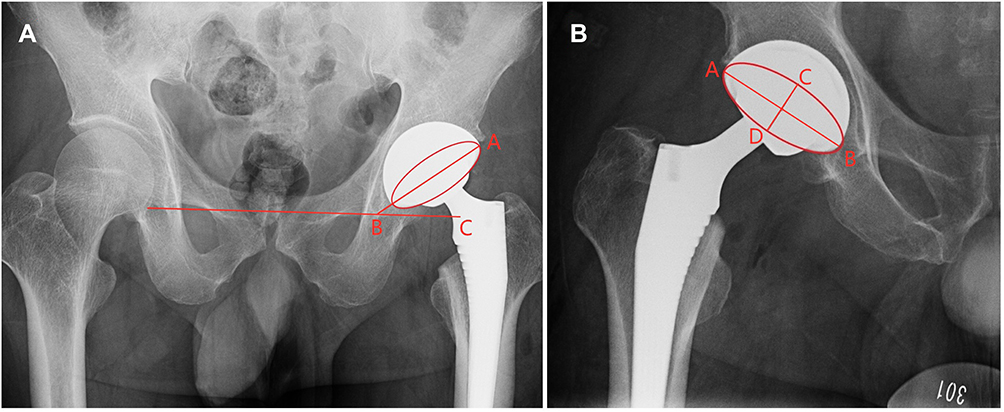 |
Figure 1 (A) Measurement of acetabular inclination. Inclination=∠ABC. ∠ABC is the angle between the line connecting bottoms of two teardrops and the larger diameter of acetabular component. (B) Measurement of acetabular anteversion. Anteversion = arcsin (CD/AB). CD is the short diameter of the acetabular component. AB is the long diameter of the acetabular component. |
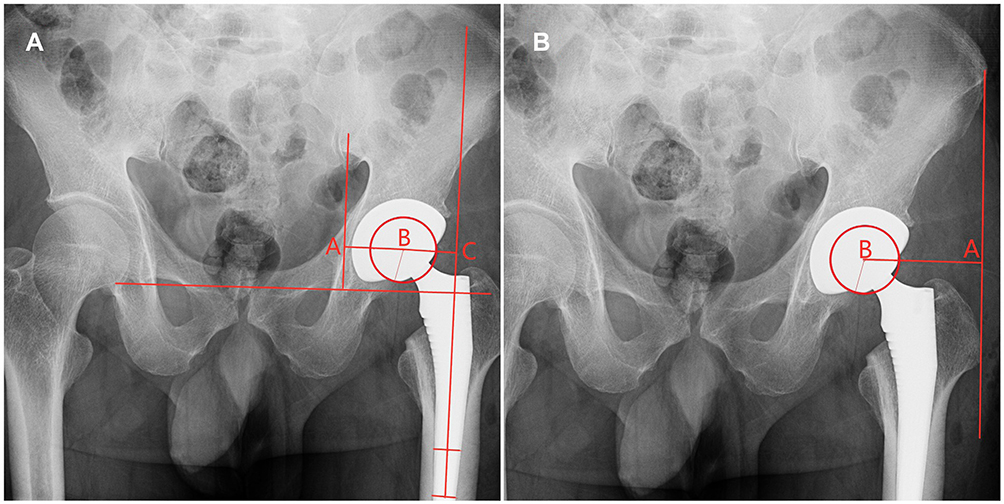 |
Figure 2 (A) Measurement of FO (femoral offset) and AO (acetabular offset). FO=BC, AO=AB. BC is the perpendicular distance from the long axis of the femoral canal to femoral head rotation center; AB is the perpendicular distance from the line perpendicular to trans-teardrop line to femoral head rotation center. (B) Measurement of abductor lever arm. Abductor lever arm=AB. AB is the distance from the line of abductor muscles’ action to femoral head rotation center. |
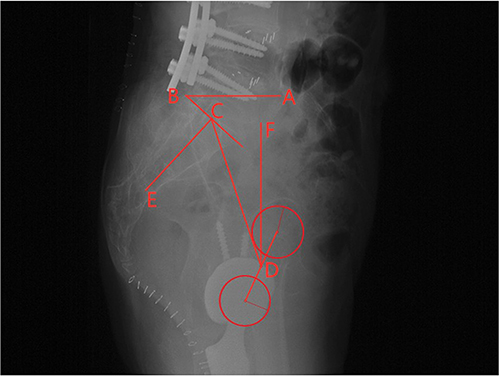 |
Figure 3 Measurement of sacral slope (SS), pelvic tilt (PT), and pelvic incidence (PI). SS=∠ABC, PT=∠CDF, PI=∠DCE. ∠ABC is the angle between the horizontal line and the sacral end plate. ∠CDF is the angle between a vertical line and a line connecting the midpoint of the sacral end plate with the point D. ∠DCE is the angle between the perpendicular line to the sacral end plate and a line connecting point D with midpoint of the sacral end plate. Point D is defined as the midpoint of the line connecting centers of two femoral heads. |
Statistical Analysis
All statistical analyses were performed using IBM SPSS statistic version 22 (SPSS Inc, Armonk, NY). Descriptive statistics were reported as means ± standard deviations, median (lower quartile, upper quartile) and number (frequencies). We used Cox regression to evaluate risk of dislocation. Various risk factors, such as gender, age, BMI, surgical year, and surgical approach, were examined to determine significant variables and subsequently a univariate Cox model was constructed. The comparisons of continuous variables between two groups were conducted by a Student’s t-test and Mann–Whitney U-test. The comparisons of categorical variables between two groups were conducted by Chi-square test and Fisher’s exact probability test. Normality test were conducted to examine all of the data. Statistical significance was defined as p-value <0.05. A power analysis (α=0.05) was conducted with R software 3.6.2.
Results
The mean age of patients in Group LSF and Group AS were 57.3±13.7 and 35.3±9.6, respectively. (p<0.0005, Table 1). There were 25 males (34.2%) in Group LSF and 139 males (95.2%) in Group AS (p<0.0005, Table 1). The surgical year, experience of surgeon, surgical approach, femoral head diameter, and BMI were matching criteria and there were no statistical differences for these variables between two groups (p>0.05, Table 1). All patients had a minimum follow-up of 2 years and the mean follow-ups of patients in two groups were 54 months. The cause of primary THA in Group LSF consisted of osteoarthritis (10, 13.7%), femoral head necrosis (49, 67.1%), and developmental dysplasia of the hip (14, 19.2%).
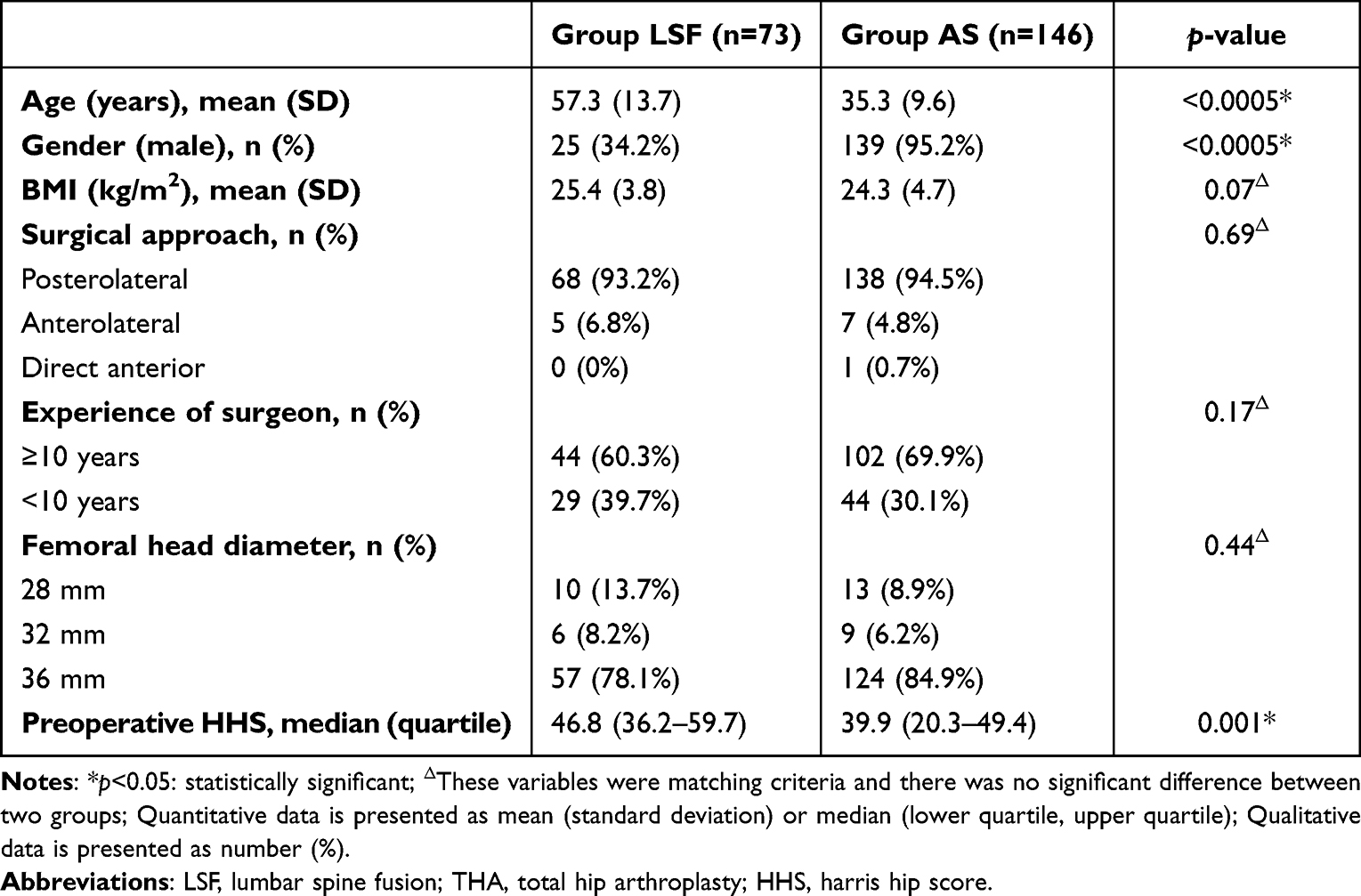 |
Table 1 Demographics and Surgical Factors of Patients in Group LSF (n=73) and Group AS (n=146) |
There were 3/73 hips (4.11%) undergoing dislocation events following THA in Group LSF. There was only 1/146 hip (0.68%) undergoing dislocation events following THA in Group AS. The risk of hip dislocation following THA in Group AS was notably lower than that in Group LSF. However, there was no significant difference for the dislocation rate between two groups (hazard ratio (HR)=6.1, 95% confidence interval (CI)=0.63–58.59; p=0.118, Table 2). No patients in either group underwent revision surgery after THA.
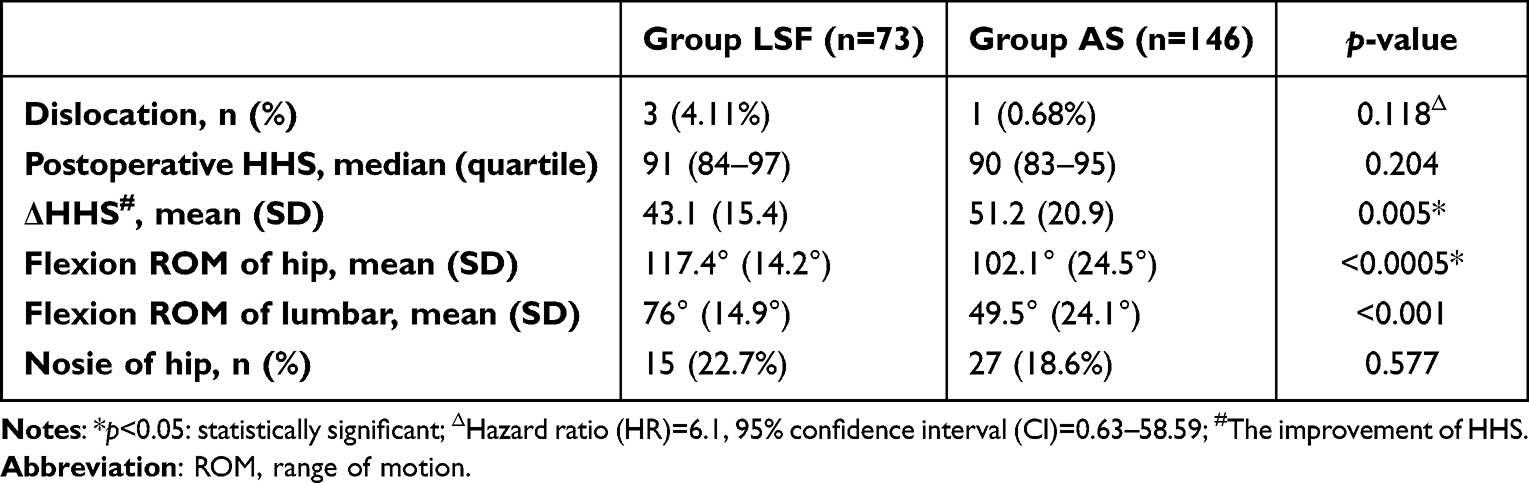 |
Table 2 Postoperative Outcome of Patients in Group LSF (n=73) and Group AS (n=146) |
Three dislocation events in Group LSF occurred within 4 months following THA (2 weeks, 2 months, and 4 months). The dislocation event in Group AS occurred at 3 months following THA. Two patients in Group LSF underwent THA for femoral head necrosis and LSF for lumbar disc herniation. One patient in Group LSF underwent THA for developmental dysplasia of the hip and LSF for scoliosis correction. Only one dislocation in Group LSF was treated by open reduction and the other three patients received closed reduction surgery when dislocation occurred. One patient in Group LSF underwent a second dislocation event at 6 months after surgery and the patient in Group AS suffered from multiple dislocations. One patient in Group LSF dislocated anteriorly and the other three patients underwent posterior dislocation.
The median of preoperative HHS were 46.8 (36.2–59.7) in Group LSF and 39.9 (20.3–49.4) in Group AS (p=0.001, Table 1). At the last follow-up, the median of HHS were 91 (84–97) in Group LSF and 90 (83–95) in Group AS (p=0.204, Table 2). The improvement of HHS (ΔHHS) were 43.1±15.4 in Group LSF and 51.2±20.9 in Group AS (p=0.005, Table 2). At the last follow-up, the flexion ROMs of hip were 117.4°±14.2° in Group LSF and 102.1°±24.5° in Group AS (p<0.0005, Table 2). The postoperative flexion ROMs of lumbar were 76°±14.9° in Group LSF and 49.5°±24.1° in Group AS (p<0.001, Table 2).
Based on measurements of postoperative standing anteroposterior (AP) radiographs, the acetabular inclinations were 39.59°±8.00° in Group LSF and 39.57°±6.44° in Group AS (p=0.988, Table 3). The medians of acetabular anteversion were 19.4° (14.4°–24.7°) in Group LSF and 20.6° (17.7°–23.5°) in Group AS (p=0.25, Table 3). There was no statistical significance in postoperative acetabular inclination and anteversion between the two groups. Postoperative femoral offsets (FO) of the operation side were 38.6 mm (34.5–42.9 mm) in Group LSF and 31.9 mm (25.3–36.1 mm) in Group AS (p<0.0005, Table 3). Postoperative acetabular offsets (AO) of the operation side were 30.1 mm (27.8–33.1 mm) in Group LSF and 32.3 mm (29.4–35.7 mm) in Group AS (p=0.001, Table 3). Postoperative abductor lever arms of the operation side were 65.2 mm±8.6 mm in Group LSF and 61.4 mm±9.3 mm in Group AS (p=0.006, Table 3). Nevertheless, the difference of FO between the operation side and health side (ΔFO, p=0.794, Table 3) revealed no statistical significance between the two groups. A similar statistical result was acquired for abductor lever arm’s difference between the operation and health side (Δabductor lever arm, p=0.902, Table 3). The AO differences (ΔAO) were 3.4 mm (1.3–6.2 mm) in Group LSF and 2.2 mm (1.0–4.2 mm) in Group AS (p=0.04, Table 3).
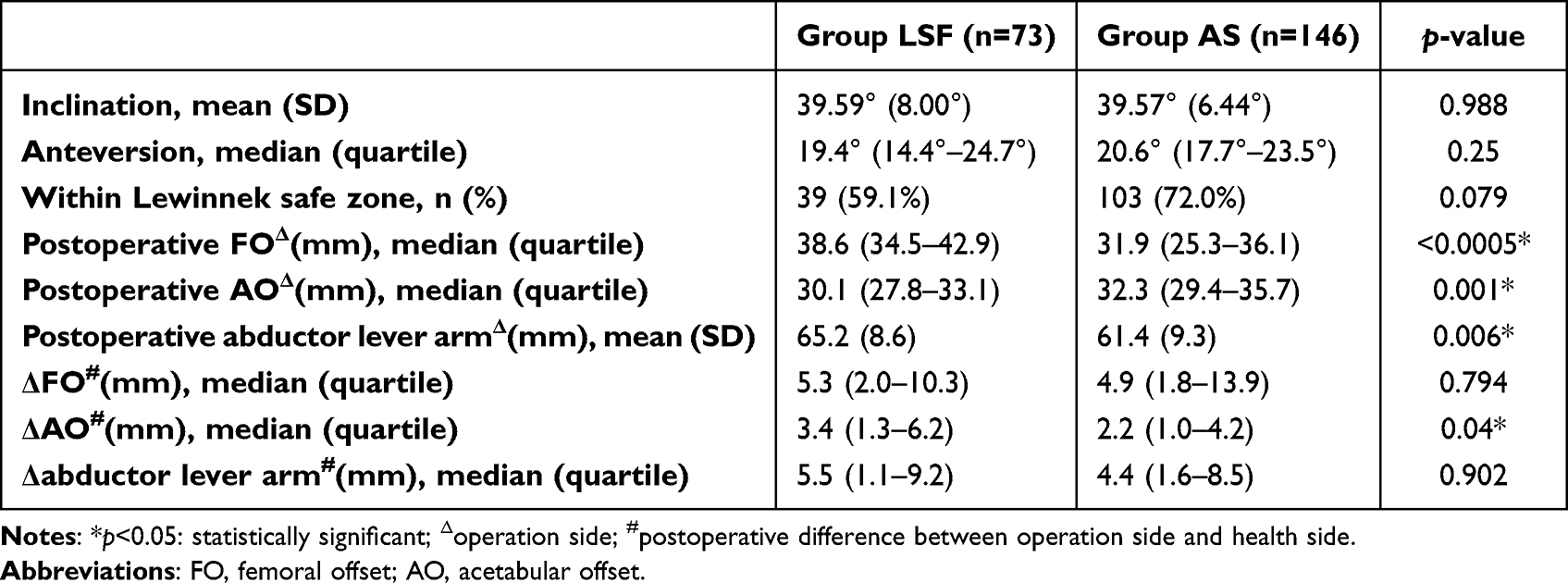 |
Table 3 Measurements of Postoperative Standing Anteroposterior (AP) Spinopelvic Radiographs in Group LSF (n=73) and Group AS (n=146) |
Standing lateral spinopelvic radiographs were available for 30 hips in Group LSF and 55 hips in Group AS. Based on these radiographs, we found the sacral slope (SS) of patients in Group AS was lower than that of patients in Group LSF (25.5° (15.3°–34.1°) versus 33.7° (25.3°–37.8°), p=0.025, Table 4). Moreover, there was a significant difference for pelvic tilt (PT) between Group LSF and Group AS (11.9°±1.6° versus 22.0°±12.2°, p<0.0005, Table 4). No significant difference was found for pelvic incidence (PI) (39.2° (29.4°–45.7°) in Group LSF versus 39.1° (34.1°–52.5°) in Group AS, p=0.158, Table 4).
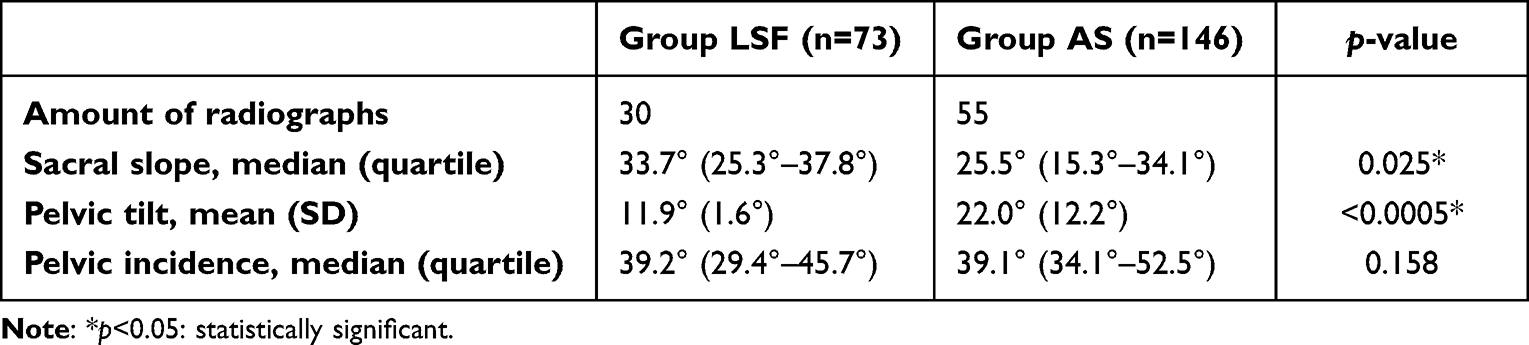 |
Table 4 Measurements of Postoperative Standing Lateral Spinopelvic Radiographs in Group LSF (n=73) and Group AS (n=146) |
Lewinnek et al proposed a safe range to position the cup (5–25° anteversion and 30–50° abduction).20,21 Thirty-nine hips (59.1%) in Group LSF were in the Lewinnek safe zone and 103 hips (72.0%) in Group AS were in the safe zone (p=0.079, Table 3).
Discussion
LSF and AS
The coexistence of degenerative lumbar spinal disease and end-stage hip osteoarthritis is common now.22–24 The hip-spine syndrome proposed by Offierski and Macnab25 has attracted much attention of many orthopedic surgeons. Researchers increasingly suggested that LSF prior to or after THA increased the risk of complications following THA, especially for dislocation event. Sing et al3 collected data of 598,995 patients and finally concluded that patients undergoing THA with prior LSF were at increased risk of dislocation events following THA. Diebo et al22 demonstrated that patients who underwent spinal fusion after primary THA had 340% higher odds of hip dislocation events and 220% higher odds of a revision surgery.
Ankylosing spondylitis also invades spine and hip joints simultaneously. However, it is still controversial whether AS could elevate the risk of dislocation following THA. Xu et al11 reported a cohort of 54 AS patients (81 THAs) and demonstrated that there were no signs of dislocation, periprosthetic fractures, or aseptic loosening following THA. Blizzard et al12 supposed that the risk ratio of dislocation events was elevated at 90-days (1.44, 95% CI0.93–2.22) with no statistical significance, but significantly increased at 2-years (1.67, 95% CI1.25–2.23). We found the outcome of THA patients with LSF and AS seemed to be different, though LSF and AS could all lead to various degrees of spinal fusion. However, no previous study has confirmed and analyzed the difference between “pathological” spinal fusion (AS) and “artificial” spinal fusion (LSF). We believed that our study was groundbreaking and valuable.
Dislocation and ROM
In our study, we found the dislocation rate of patients in Group AS (0.68%) was obviously lower than that of patients in Group LSF (4.11%) and the HR value reached 6.1. However, the difference has not reached statistical significance (p=0.118). Considering the low calculated power (1-β, 0.24), we supposed insufficient statistical evidence could be attributed to small sample size and a retrospectively designed study. We looked forward to prospective, large-scale trials to statistically validate the difference of dislocation rate between two groups.
Though there was no significant difference for postoperative HHS (p=0.204) between two groups in our study, it demonstrated that postoperative hip flexion–extension ROM in Group AS was significantly lower than that in Group LSF. Researchers have reported that the dislocation event was related to postoperative hip ROM. Peak et al26 believed that postoperative education remained necessary to avoid dislocation events. Though several restrictions (the use of a higher stool and a pillow between two legs, the avoidance of driving and lying on operative side, etc.) proved ineffective for rehabilitation in their study, Peak et al26 still asked all patients in their department to obey the restrictive rules of ROM (the avoidance of flexion >90°, hip adduction, external and internal rotation >45°) for 6 weeks postoperatively. Patients in Group AS had significantly lower hip joint motion than patients in Group LSF in the early stage of rehabilitation or after complete recovery. Therefore, AS patients had fewer opportunities to exceed the limitation of hip ROM, so that they had fewer opportunities to undergo dislocation events. Our research has also demonstrated that postoperative lumbar flexion ROM of AS patients was significantly lower than that of patients in Group LSF. Previous studies have revealed that the spine–pelvis–hip complex functions in coordination in the sagittal plane and lumbar stiffness is closely related to decreased pelvic motion.9,27 We supposed that the decreased lumbar flexion ROM in AS patients was also associated with the limitation of hip ROM and lower risk of dislocation events.
Acetabular Orientation
Multiple studies have demonstrated that the inclination and anteversion were key elements of initial stability and long-term survival of the implant and inappropriate orientation of the acetabular cup can lead to dislocation events.5,16,20,21 Since history of LSF and AS would change the ROM and sagittal balancing of the spine, the pelvis tended to be hyperextension and acetabular orientation would change with spine and pelvis.11,16,28,29 Thus, it was conventional for surgeons to adjust inclination and anteversion of the implant intraoperatively in case routine acetabular positioning and orientation would lead to increased risk of dislocation.11,28,29
However, our study revealed that there was no significant difference between two groups concerning postoperative acetabular inclination (p=0.988) and anteversion (p=0.25). Moreover, the mean acetabular inclination and anteversion of two groups were all located in the Lewinnek safe zone and the proportion of patients in the safe zone was not significantly different between two groups (p=0.079). We believed that the difference of dislocation rate between two groups was not associated with acetabular inclination and anteversion and there would be no need for surgeons to specially adjust positioning and orientation of the implant intraoperatively.
Standing Lateral Spinopelvic Radiographs
With the measurement of standing lateral spinopelvic radiographs, we found the sacral slope of patients in Group LSF and Group AS was, respectively, 33.7° and 25.5°, and they were all below the mean value of the general population (40°). That demonstrated that the pelvis tended to be hyperextended in patients with LSF and AS. Meanwhile, our data suggested that patients in Group AS had a significantly lower SS (p=0.025) and higher PT (p<0.0005) than patients in Group LSF. Lower SS and higher PT in patients with AS demonstrated that AS patients suffered from more serious spinopelvic stiffness compared with LSF patients.30–32 The decreased lumbar ROM and increased spinopelvic stiffness in AS patients could be attributed to severer spinal ankylosis and sagittal imbalance, which was known to be associated with the decreased hip ROM.30,33–35 Therefore, compared with LSF patients, AS patients suffered from severer stiffness and lower mobility along the spine–pelvis–hip axis. The lower mobility restricted movement along the spine–pelvis–hip axis and reduced the possibility of risky movement which could result in dislocation events. We will design and carry out a prospective study with a large sample size to validate our conclusion. The standing and sitting lateral spinopelvic radiographs will be acquired preoperatively and postoperatively for all patients enrolled in the prospective study, so that we could dynamically analyze the mobility and sagittal balance along the spine–pelvis–hip axis.
Limitations
There were two limitations in this study. First, the study was a retrospective study and that made it difficult to obtain data and conduct follow-ups. We will further conduct a relevant prospective study and collect more abundant data to validate our opinions more exactly. Second, our study was limited by the small sample size. The patients with LSF and THA coexisting only contributed a minor part of THA patients and dislocation events following THA are events with low probabilities. Therefore, the amount of dislocation events occurring in two groups was relatively small and the rare amount of dislocation events had a great effect on the statistical result. Further studies need a larger sample size which could help reduce the effect as far as possible.
Conclusion
Patients with AS have a lower risk of dislocation following THA than patients undergoing LSF, though prospective and large-sample trials are further needed to statistically validate the difference between the two groups. The lower risk is significantly relevant to severer stiffness and lower mobility along the spine–pelvis–hip axis in AS patients after THA, including lower hip ROM, lower lumbar ROM, and severer spinopelvic stiffness. There is no significant evidence that acetabular orientation has an effect on the difference of dislocation rate between patients with LSF and AS. Therefore, we propose that there is no need for surgeons to specially adjust positioning and orientation of the implant among patients with various lumbar fusion.
Abbreviations
LSF, lumbar spinal fusion; AS, ankylosing spondylitis; ROM, range of motion; THA, total hip arthroplasty; BMI, body mass index; HHS, Harris Hip Score; AP, anteroposterior; FO, femoral offset; AO, acetabular offset; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; HR, hazard ratio; CI, confidence intervals.
Data Sharing Statement
All data and materials were in full compliance with the journal’s policy.
Ethics Approval and Informed Consent
This study was completely approved by the institutional review board of Chinese PLA General Hospital (IRB number: S2021-066-01). This study is a retrospective study and we could not obtain written informed consent from the patients who have been discharged from hospital. Therefore, we obtained verbal informed consent from all participants during the telephone follow-up with the approval of the institutional review board of Chinese PLA General Hospital. All data that could indicate the identity of the patients were kept strictly confidential in this study. Work on human beings is conducted in accordance with the Declaration of Helsinki.
Consent for Publication
We have obtained consent to publish from all the participants.
Acknowledgments
The authors would like to thank Dr Zhiwei Liu, Dr Minzhi Yang, Dr Jizhe Li and Dr Taiyang Shu for the guidance of the manuscript preparation.
Funding
This study is financially supported by the National Key Research and Development Program of China (No.2020YFC2004900).
Disclosure
All authors declare that they have no conflict of interest.
References
1. Loh JLM, Jiang L, Chong HC, Yeo SJ, Lo NN. Effect of spinal fusion surgery on total hip arthroplasty outcomes: a matched comparison study. J Arthroplasty. 2017;32(8):2457–2461. doi:10.1016/j.arth.2017.03.031
2. Mariconda M, Galasso O, Costa GG, Recano P, Cerbasi S. Quality of life and functionality after total Hip arthroplasty: a long-term follow-up study. BMC Musculoskelet Disord. 2011;12(1):222. doi:10.1186/1471-2474-12-222
3. Sing DC, Barry JJ, Aguilar TU, et al. Prior lumbar spinal arthrodesis increases risk of prosthetic-related complication in total hip arthroplasty. J Arthroplasty. 2016;31(9):227–232.e1. doi:10.1016/j.arth.2016.02.069
4. Ben-Galim P, Ben-Galim T, Rand N, et al. Hip-spine syndrome: the effect of total hip replacement surgery on low back pain in severe osteoarthritis of the Hip. Spine. 2007;32(19):2099–2102. doi:10.1097/BRS.0b013e318145a3c5
5. Salib CG, Reina N, Perry KI, Taunton MJ, Berry DJ, Abdel MP. Lumbar fusion involving the sacrum increases dislocation risk in primary total Hip arthroplasty. Bone Jt J. 2019;101-B(2):198–206. doi:10.1302/0301-620X.101B2.BJJ-2018-0754.R1
6. Barry JJ, Sing DC, Vail TP, Hansen EN. Early outcomes of primary total hip arthroplasty after prior lumbar spinal fusion. J Arthroplasty. 2017;32(2):470–474. doi:10.1016/j.arth.2016.07.019
7. Buckland AJ, Puvanesarajah V, Vigdorchik J, et al. Dislocation of a primary total Hip arthroplasty is more common in patients with a lumbar spinal fusion. Bone Jt J. 2017;99-B(5):585–591. doi:10.1302/0301-620X.99B5.BJJ-2016-0657.R1
8. Blizzard DJ, Sheets CZ, Seyler TM, et al. The impact of lumbar spine disease and deformity on total hip arthroplasty outcomes. Orthopedics. 2017;40(3):e520–e525. doi:10.3928/01477447-20170327-03
9. Heckmann N, McKnight B, Stefl M, Trasolini NA, Ike H, Dorr LD. Late dislocation following total hip arthroplasty: spinopelvic imbalance as a causative factor. J Bone Jt Surg. 2018;100(21):1845–1853. doi:10.2106/JBJS.18.00078
10. Gu M, Zhang Z, Kang Y, et al. Roles of sagittal anatomical parameters of the pelvis in primary total hip replacement for patients with ankylosing spondylitis. J Arthroplasty. 2015;30(12):2219–2223. doi:10.1016/j.arth.2015.06.027
11. Xu J, Zeng M, Xie J, Wen T, Hu Y. Cementless total Hip arthroplasty in patients with ankylosing spondylitis: a retrospective observational study. Medicine. 2017;96(4):e5813. doi:10.1097/MD.0000000000005813
12. Blizzard DJ, Penrose CT, Sheets CZ, Seyler TM, Bolognesi MP, Brown CR. Ankylosing spondylitis increases perioperative and postoperative complications after total hip arthroplasty. J Arthroplasty. 2017;32(8):2474–2479. doi:10.1016/j.arth.2017.03.041
13. Yim SJ, Park YB, Kim J, Park SH. Long-term outcomes of cemented total hip arthroplasty in patients with ankylosing spondylitis at a minimum follow-up of 10 years. Hip Pelvis. 2018;30(3):175. doi:10.5371/hp.2018.30.3.175
14. Perfetti DC. Prosthetic dislocation and revision after primary total hip arthroplasty in lumbar fusion patients: a propensity score matched-pair analysis. J Arthroplasty. 2017;32:1635–1640.
15. Malkani AL, Himschoot KJ, Ong KL, et al. Does timing of primary total hip arthroplasty prior to or after lumbar spine fusion have an effect on dislocation and revision rates? J Arthroplasty. 2019;34(5):907–911. doi:10.1016/j.arth.2019.01.009
16. Buckland AJ, Vigdorchik J, Schwab FJ, et al. Acetabular anteversion changes due to spinal deformity correction: bridging the gap between hip and spine surgeons. J Bone Jt Surg-Am Vol. 2015;97(23):1913–1920. doi:10.2106/JBJS.O.00276
17. Flecher X, Ollivier M, Argenson JN. Lower limb length and offset in total Hip arthroplasty. Orthop Traumatol Surg Res. 2016;102(1):S9–S20. doi:10.1016/j.otsr.2015.11.001
18. Matsuda K, Nakamura S, Matsushita T. A simple method to minimize limb-length discrepancy after Hip arthroplasty. Acta Orthop. 2006;77(3):375–379. doi:10.1080/17453670610046280
19. Bjørdal F, Bjørgul K. The role of femoral offset and abductor lever arm in total Hip arthroplasty. J Orthop Traumatol. 2015;16(4):325–330. doi:10.1007/s10195-015-0358-7
20. Banaszkiewicz PA. Dislocations after total hip-replacement arthroplasties. In: Banaszkiewicz PA, Kader DF, editors. Classic Papers in Orthopaedics. London: Springer; 2014:113–115.
21. Tezuka T, Heckmann ND, Bodner RJ, Dorr LD. Functional safe zone is superior to the lewinnek safe zone for total hip arthroplasty: why the lewinnek safe zone is not always predictive of stability. J Arthroplasty. 2019;34(1):3–8. doi:10.1016/j.arth.2018.10.034
22. Diebo BG, Beyer GA, Grieco PW, et al. Complications in patients undergoing spinal fusion after THA. Clin Orthop. 2018;476(2):412–417. doi:10.1007/s11999.0000000000000009
23. King CA, Landy DC, Martell JM, Luu HH, Shi LL, Lee MJ. Time to dislocation analysis of lumbar spine fusion following total hip arthroplasty: breaking up a happy home. J Arthroplasty. 2018;33(12):3768–3772. doi:10.1016/j.arth.2018.08.029
24. Eneqvist T, Nemes S, Brisby H, Fritzell P, Garellick G, Rolfson O. Lumbar surgery prior to total Hip arthroplasty is associated with worse patient-reported outcomes. Bone Jt J. 2017;99-B(6):759–765. doi:10.1302/0301-620X.99B6.BJJ-2016-0577.R2
25. Offierski CM, Macnab I. Hip-Spine Syndrome. Spine. 1983;8(3):316–321. doi:10.1097/00007632-198304000-00014
26. Peak EL, Parvizi J, Ciminiello M, et al. The role of patient restrictions in reducing the prevalence of early dislocation following total hip arthroplasty. JBJS. 2005;87:247–253.
27. Esposito CI, Miller TT, Kim HJ, et al. Does degenerative lumbar spine disease influence femoroacetabular flexion in patients undergoing total hip arthroplasty? Clin Orthop. 2016;474(8):1788–1797. doi:10.1007/s11999-016-4787-2
28. Seagrave KG, Troelsen A, Malchau H, Husted H, Gromov K. Acetabular cup position and risk of dislocation in primary total Hip arthroplasty: a systematic review of the literature. Acta Orthop. 2017;88(1):10–17. doi:10.1080/17453674.2016.1251255
29. Stefl M, Lundergan W, Heckmann N, et al. Spinopelvic mobility and acetabular component position for total Hip arthroplasty. Bone Jt J. 2017;99-B(1_Supple_A):37–45. doi:10.1302/0301-620X.99B1.BJJ-2016-0415.R1
30. Bukowski BR, Clark NJ, Taunton MJ, Freedman BA, Berry DJ, Abdel MP. Primary total hip arthroplasty in patients with ankylosing spondylitis. J Arthroplasty. 2021;36(7):S282–S289. doi:10.1016/j.arth.2021.01.054
31. Oommen AT, Hariharan TD, Kandagaddala M, Chandy VJ, Poonnoose PM, Shankar AA. Spinopelvic mobility pattern and acetabular anteversion in stiff hips with ankylosing spondylitis after total hip arthroplasty. Arthroplasty Today. 2022;16:182–191. doi:10.1016/j.artd.2022.05.006
32. Esposito CI, Carroll KM, Sculco PK, Padgett DE, Jerabek SA, Mayman DJ. Total hip arthroplasty patients with fixed spinopelvic alignment are at higher risk of hip dislocation. J Arthroplasty. 2018;33(5):1449–1454. doi:10.1016/j.arth.2017.12.005
33. Sariali E, Lazennec JY, Khiami F, Gorin M, Catonne Y. Modification of pelvic orientation after total hip replacement in primary osteoarthritis. HIP Int. 2009;19(3):257–263. doi:10.1177/112070000901900312
34. Baraliakos X, Braun J. Hip involvement in ankylosing spondylitis. Rheumatology. 2010;49(1):3–4. doi:10.1093/rheumatology/kep298
35. Stolwijk C, Ramiro S, Vosse D, Landewé R, van der Heijde D, van Tubergen A. Comparison of tests for lumbar flexion and hip function in patients with and without axial spondyloarthritis: mobility tests in patients with and without axial SpA. Arthritis Care Res. 2015;67(4):538–545. doi:10.1002/acr.22464
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.