Back to Journals » Journal of Pain Research » Volume 19
The Handgrip Endurance Task as a Simple Clinical Indicator of Mental Fatigue in Patients with Chronic Low Back Pain
Authors Grousset M, Audiffren M, Meklat H, André N ![]()
Received 20 February 2026
Accepted for publication 24 May 2026
Published 9 July 2026 Volume 2026:19 602280
DOI https://doi.org/10.2147/JPR.S602280
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Marine Grousset,1,2 Michel Audiffren,2 Hachemi Meklat,1 Nathalie André2
1Centre Richelieu, French Red Cross, La Rochelle, Nouvelle Aquitaine, France; 2Centre of Research on Cognition and Learning (CeRCA), University of Poitiers, CNRS, Poitiers, Nouvelle Aquitaine, France
Correspondence: Nathalie André, University of Poitiers, MSHS - CeRCA - Bâtiment A5, 5, rue T. Lefebvre, TSA 21103, Poitiers Cedex 9, 86073, France, Tel +33 549454679, Email [email protected]
Purpose: Mental fatigue is highly prevalent in chronic low back pain (cLBP) but rarely assessed in clinical practice. Standard physical capacity tests may underestimate functional abilities when mental fatigue is present. This study investigated whether a simple handgrip endurance task could objectively detect mental fatigue effects on physical performance in cLBP patients.
Patients and Methods: One hundred twenty participants (60 cLBP patients, 60 pain-free controls) performed a handgrip endurance task at 13% of maximal voluntary contraction before and after either a mentally fatiguing Stroop task (30 minutes) or watching a neutral documentary. Time to exhaustion (TTE) was compared between conditions within each group using analysis of variance.
Results: cLBP patients who performed the Stroop task showed significantly greater reduction in endurance (mean decrease: 118 seconds) compared to those who watched the documentary (mean decrease: 71 seconds), p < 0.05. This mental fatigue effect was not observed in pain-free participants (p =0.644). Importantly, both groups performed similarly on the Stroop task itself, indicating that cognitive performance did not differ between populations.
Conclusion: Mental fatigue selectively impairs physical endurance in cLBP patients. The handgrip endurance test offers a practical, low-cost tool to objectively assess mental fatigue in clinical settings. These findings have important implications for functional capacity evaluations and return-to-work assessments, as standard tests may systematically underestimate patients’ true abilities when mental fatigue goes unrecognized.
Keywords: physical endurance, vitality capacity, functional assessment, return to work
Introduction
Mental fatigue is highly prevalent in individuals with chronic low back pain (cLBP), yet it remains rarely assessed in clinical practice. Epidemiological data on the relationship between pain and fatigue are scarce, partly due to the ongoing debates regarding whether fatigue should be considered a comorbidity of chronic conditions such as depression or a distinct construct in its own right.1,2 In the general population, between 6% and 43% of individuals report symptoms of fatigue, whereas prevalence rates appear to be up to 20% higher among people with chronic conditions. In patients with cLBP, fatigue has been identified as a particularly salient symptom. A systematic review by Perry et al1 highlighted fatigue as an important factor to consider in the rehabilitation, and a large Norwegian cohort study reported that 69.7% of patients with cLBP experienced substantial fatigue.3 Similar observations have been reported in French pain care institutions.4 However, despite its prevalence, the functional consequences of mental fatigue on physical performance in cLBP patients remain poorly understood.
Mental fatigue can be defined as a transient psychophysiological state induced by sustained and effortful cognitive activity requiring executive control. It is characterized by a reduced capacity and/or motivation to perform the ongoing or subsequent physical or cognitive task. In chronic pain populations, mental fatigue is often associated with mood disturbances, impaired social functioning, and deficit in attention and planning.5 Previous research also suggests that individuals experiencing pain exhibit reduced capacity for effortful control, which may contribute to the development and maintenance of chronic pain and its associated disorders.6–8 Pain may increase cognitive load through attentional capture, emotional regulation demands, and altered sensory processing, thereby contributing to mental fatigue in chronic pain population.9–13
There is increasing evidence that mental fatigue alters physical performance, particularly endurance-related outcomes (eg., decreased time to exhaustion). A systematic review by Van Cutsem et al14 demonstrated that mental fatigue is associated with reduced endurance performance, such as shorter time to exhaustion, alongside increased perceived exertion, whereas maximal strength is generally preserved. In patients with chronic pain, this raises the possibility that physical endurance may be undermined by mental fatigue induced by the ongoing management of pain. Consequently, conventional measures of muscular endurance commonly used in low back pain assessment (ie., the Biering-Sørensen test for lumbar extensors or the Shirado–Ito test for abdominal muscles) may underestimate actual physical capacity if mental fatigue is not considered. Such underestimation could have important implications for rehabilitation planning and return-to-work decisions.
In most studies examining fatigue in patients with chronic low back pain, assessment relies primarily on self-report questionnaires, including the Chalder Fatigue Scale,12,15 the Checklist of Individual Strength,16 the Fatigue Severity Scale,17 and the Brief Fatigue Inventory.18 However, these instruments present several limitations. Subjective experiences of fatigue vary considerably across individuals, and some may underestimate their fatigue.19 In addition, fatigue is frequently confused with related states such as boredom or sleepiness.20 Importantly, these questionnaires primarily assess chronic or trait fatigue and do not adequately capture acute mental fatigue induced by sustained cognitive effort.
Acute mental fatigue differs from chronic fatigue in both underlying mechanisms and temporal dynamics. Acute mental fatigue arises from prolonged cognitive activity and typically dissipates after a recovery period, whereas chronic fatigue reflects longer-term dysregulation of neuromodulatory systems.21–24 Importantly, chronic fatigue may increase fatigability and amplify acute mental fatigue effects.25 In the present study, we focus on experimentally induced acute mental fatigue, while acknowledging that it may interact with pre-existing fatigue in cLBP patients.
Despite the clinical relevance of mental fatigue in cLBP, objective assessment remains uncommon in rehabilitation settings. Existing objective measures are often time-consuming, costly, or require specialized equipment, limiting their applicability in routine practice. There is thus a clear need for simple and clinically feasible tools to assess mental fatigue in painful populations. The handgrip endurance task represents a promising candidate in this regard. Unlike standard endurance tests used in low back pain assessment (eg., Biering–Sørensen or Shirado–Ito), it does not directly load the lumbar musculature, making it suitable for patients with chronic low back pain. In addition, it has been validated as a measure of vitality capacity in clinical populations and has demonstrated sensitivity to experimentally induced mental fatigue.26,27 Notably, a recent study conducted by Daneshgar-Pironneau et al28 successfully applied this protocol in healthy participants and demonstrated a significant mental fatigue effect on handgrip endurance performance (d = 0.818). Together, these features support its use as a simple and clinically applicable tool to assess mental fatigue. The present study extends this work to a clinical population of patients with chronic low back pain. If validated as an indicator of mental fatigue in patients with cLBP, this task could be readily integrated into standard functional capacity evaluations, potentially improving the accuracy of rehabilitation planning and return-to-work assessments.
The primary aim of the present study was to examine whether a handgrip endurance task could serve as an indicator of acute mental fatigue in patients with chronic low back pain. The primary outcome was time to exhaustion (TTE) during the handgrip endurance task. We hypothesized that (1) TTE would decrease following a mentally fatiguing task compared with a control condition, (2) this decrease would be greater in patients with cLBP than in pain-free participants, and (3) cognitive performance during the Stroop task would deteriorate over time, particularly in patients with cLBP.
Method
Participants and Design
Sixty patients suffering from cLBP (35 women, mean age = 43.77, SD = 9.90) and 60 volunteers recruited from the general population who did not suffer from chronic pain (38 women, mean age = 40.47, SD = 12.74) participated in the study.
None of the patients suffered from any serious spinal pathology. As for the volunteers, none of them experienced chronic pain. All volunteers met predefined inclusion and non-inclusion criteria approved by the ethics committee; full details of these criteria are provided in Supplementary Material 6. For instance, non-inclusion criteria included: being colorblind, engaging in muscle-strengthening activities for more than six months, having insufficient visual correction to perform the experimental task, having language or learning difficulties, having a history of severe neurological or metabolic disorders, being retired and/or having a functional impairment involving the dominant hand. Symmetrically, to be included in the study, all patients had to be over eighteen years of age and have French as their native language. Color vision was screened prior to inclusion using the Ishihara Color Vision Test. Participants were required to correctly identify numbers embedded in pseudoisochromatic plates, ensuring normal color vision and the ability to perform the Stroop task. All participants completed the protocol without dropout, likely due to the single-session design, financial compensation (€30), and high levels of engagement.
The sample size was determined via G*Power software, with a moderate effect size (f = 0.25; based on study 3 of Mangin et al,29 alpha =0.05, and power =0.80. The analysis indicated that a sample size of 110 participants was sufficient to detect the effect. To account for potential dropouts, we recruited 120 participants. Informed consent was obtained from each participant following a verbal explanation of the study procedures. All 120 participants completed the full experimental protocol, and no dropouts occurred.
cLBP patients were recruited from the Centre Richelieu in La Rochelle after admission to the Functional Restoration of the Spine (FRS) program. The pain-free controls were recruited through local press announcements. This study was approved by the Ethics Committee of Tours and Poitiers Universities (Ethics Code: CER-TP 2020–06-03) on June 29th, 2020; it was therefore conducted in accordance with the ethical principles of the Declaration of Helsinki, ensuring the protection of the rights, safety, and well-being of the participants. All participants provided written informed consent prior to enrolment in the study. Within each group, participants were randomized in a single-blinded fashion to the fatigue or control conditions. Clinical characteristics of the cLBP participants, including pain intensity (assessed using the Brief Pain Inventory), duration of the condition, and functional capacity (eg., Ito test), were collected to describe the sample and are reported in Table 1 (see Results section).
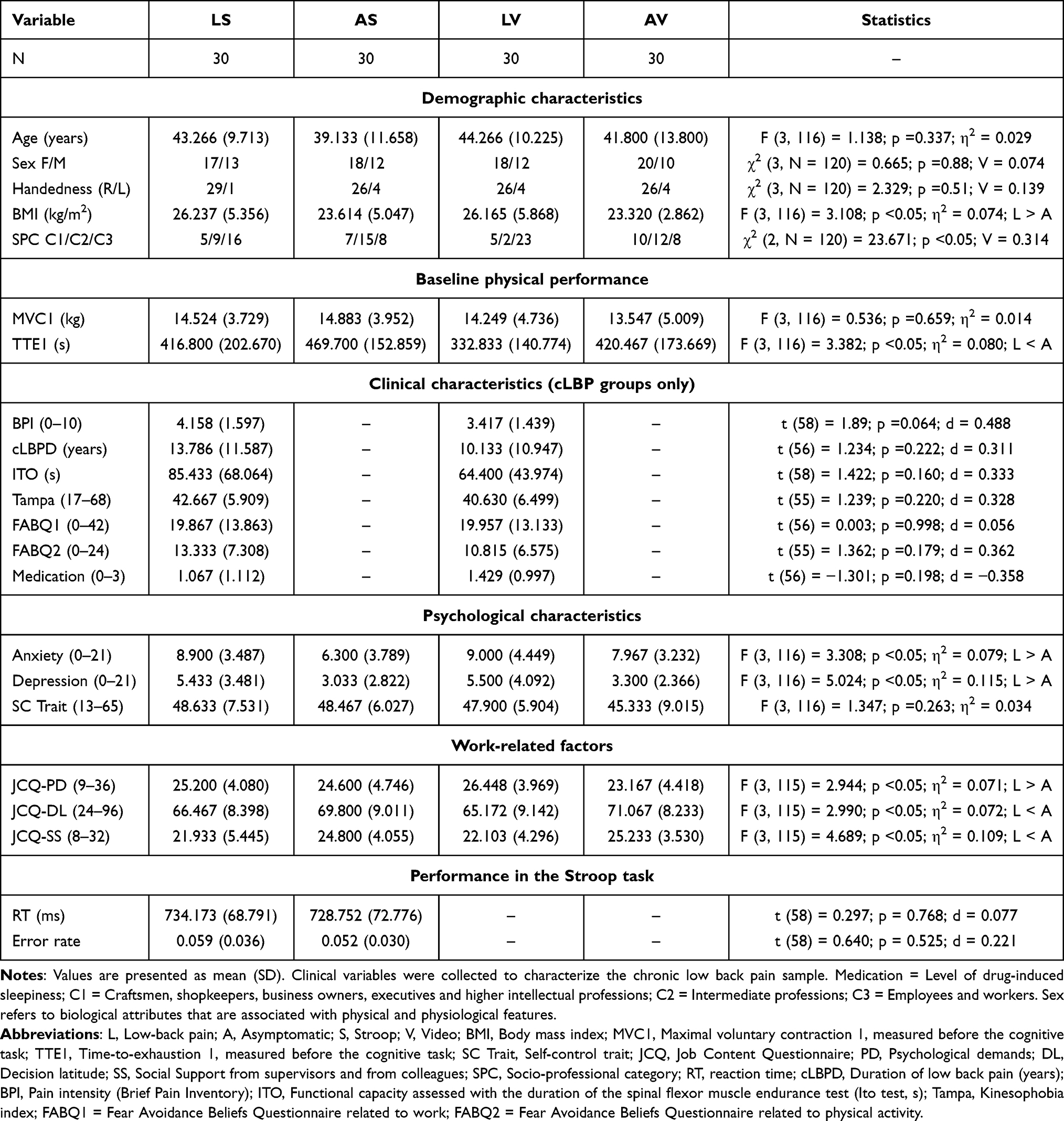 |
Table 1 Demographic, Clinical, and Psychological Characteristics of the Participants |
In addition to age and sex, a comprehensive set of demographics, physical, and psychosocial variables that may influence fatigue was assessed. These included body mass index (BMI), baseline physical performance (MVC and time-to-exhaustion), trait self-control, anxiety and depression (HADS), as well as occupational characteristics such as socio-professional category and work-related stress assessed using the Job Content Questionnaire (psychological demands, decision latitude, and social support). In patients with chronic low back pain, additional clinical variables (eg., pain intensity, duration, fear-avoidance beliefs, and medication use) were also collected. These variables were measured to characterize the sample and to examine the comparability of groups. Differences between groups on these variables are reported in the Results section. Medication use was assessed prior to the experimental session. Participants were screened to ensure that they were not taking medications likely to affect mental fatigue or cognitive performance (eg., antidepressants, anxiolytics, hypnotics, or psychostimulants).
Procedure
This experiment occurred during a single session with an average duration of 2 hours. All the participants were welcomed individually and given a general description of the procedure before starting the experiment. After signing the informed consent form, the participants completed different questionnaires and tests allowing to check for inclusion criteria. The 120 participants included 60 patients with cLBP and 60 pain-free volunteers. All the participants followed the same protocol regarding the physical and cognitive tasks (see Figure 1). On two occasions, before and after the cognitive task, participants completed the same sequence of physical tasks. First, they performed a series of three maximal voluntary contractions (MVCs), each lasting 3 s, with a 1-minute rest period between contractions, to determine their maximal force. One minute after the last MVC, participants performed a handgrip task until exhaustion at 13% of their MVC. Immediately after this task, they completed a second series of MVCs, following the same procedure as the first series, to verify that the instructions to perform the task “until exhaustion” had been respected. Regarding the cognitive task, participants were randomly assigned to either a fatiguing condition using a modified Stroop task or to a control condition involving watching an animal documentary. The cognitive task and the documentary lasted 30 minutes. Immediately after its completion, participants repeated the same MVC–time-to-exhaustion–MVC sequence under identical conditions. At different times, the state of fatigue, satisfaction with the performance achieved, motivation and perceived difficulty in performing the tasks before and after each sequence were measured via a visual analog scale (VAS) calibrated as a percentage. Figure 1 shows the steps of the protocol.
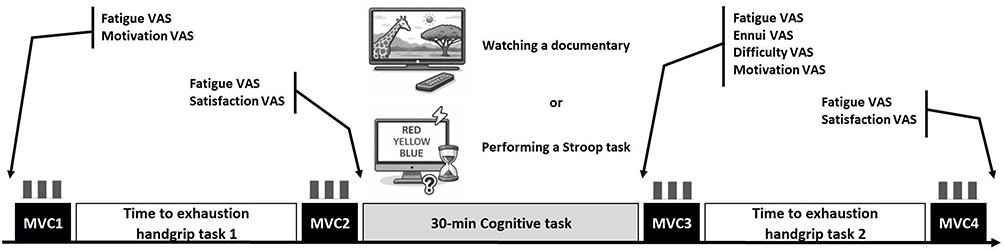 |
Figure 1 Experimental design. Participants first performed a series of 3 maximal voluntary contractions (MVC1), followed by a first handgrip task to exhaustion. After a second MVC (MVC2), they completed a 30-min cognitive task (i.e., watching a documentary or performing a Stroop task, followed by another MVC (MVC 3) and a second handgrip task to exhaustion (TTE-2). A final MVC was performed at the end of the protocol (MVC4). At the beginning of the session, just before the cognitive task, just after the cognitive task and at the end of the session, participants scored their feelings on visual analog scales. |
Tasks
Time-to-Exhaustion Handgrip Task
A time-to-exhaustion (TTE) handgrip task was employed to evaluate acute mental fatigue following either the fatiguing task or the control task, for three main reasons. First, this task has been shown to be a reliable measure of fatigue resistance.26,28,30 Second, previous research has demonstrated that performing isometric handgrip exercises to the point of exhaustion can impair subsequent cognitive performance, as evidenced by reduced scores on a Stroop task.31 Third, the TTE handgrip test was associated with the second largest average effect size (d = 0.63) in the meta-analysis by Hagger et al,32 which examined the impact of ego depletion on task performance. Notably, ego depletion shares conceptual similarities with acute mental fatigue.33 Moreover, to enhance the task’s sensitivity to self-control demands and extend its duration, we reduced the target intensity from 50% to 13% of the participants’ maximal voluntary contraction (MVC). This low-intensity version demonstrated strong reliability based on data from a previous study (n = 55; ICC3 [A, 2] =0.868; 95% CI = [0.774,0.923]). It was selected from a range of intensities during a pilot study, aiming to produce average task durations that were neither too short (< 3 minutes) nor excessively long (> 20 minutes).
A dynamometer (TSD121C, BIOPAC), AcqKnowledge software, version 4.2 (BIOPAC Systems Inc., Goleta, CA, USA) and an MP160WSW data acquisition unit were used to record the force signal in the handgrip tasks. Data were recorded online at a sampling rate of 2000 Hz and later stored and analyzed offline.
The participants started the physical task by performing a maximal voluntary contraction (MVC) while squeezing a hand dynamometer. The highest MVC measured before the first TTE handgrip task was used throughout the session as the reference to calculate the targeted force (ie., 13% MVC) in the TTE handgrip task.
Then, the participants had to squeeze the hand dynamometer and stay between 12% and 14% of the MVC until exhaustion. This TTE handgrip task was used as the dependent task. The end of the TTE task was defined as a failure to maintain the targeted force (ie., force < 12% MVC) for more than 2 s. During the TTE task, every 30s, we asked the participants to rate their perception of effort and their perception of pain. After the TTE handgrip task, the participants repeated the procedure to measure the MVC. This cycle succession of handgrip tasks (ie., the MVC task, TTE task, and MVC task) was repeated after the mental task (see Figure 1).
Incongruent Stroop Task
We used a modified Stroop task implemented on a computer equipped with an S-R response box and E-prime software, version 2.0 (Psychological Software Tools, Pittsburgh, PA, USA), as a fatiguing task for the experimental group. The participants sat in front of a screen and responded orally to the visual stimuli that appeared at the middle of the screen.
The participants underwent 888 trials, each of which lasted for 2 seconds. Fifty percent of the trials were “reading” trials (ie., the participants had to read the word), and the other 50% were “naming ink color” trials (ie., the participants had to name the color of the ink). These two types of trials were presented in a randomized order and primed with a preparatory signal.
Performance in the modified Stroop task was analyzed as a function of time-on-task and type of trial. The data were divided into 4 consecutive periods of 222 trials lasting 7 minutes and 30 seconds. For each period and type of trial, we calculated the mean reaction time (RT) for correct responses and error rate.
Documentary Watching Task
We chose a documentary movie named Earth as a control task for the control groups.34 This documentary was tested as emotionally neutral and weakly boring.29 The participants were subsequently asked to answer three questions related to the content of the documentary to verify whether they were actively watching the movie.
Psychological Measures
Three questionnaires were previously administered by therapists as part of routine clinical care. Of the 3 questionnaires, only the participants’ levels of anxiety and depression (Hospital Anxiety and Depression Scale [HADS])35 were measured in both groups (pain and pain-free) using a 14-item scale with two subscales (7 items each), scored from 0 to 21; a score of 11 or above is considered indicative of a definite symptomatology (HADS-A, α = 0.83; HADS-D, α = 0.82). Kinesiophobia was assessed using the Tampa Scale for Kinesiophobia (TAMPA),36 a 17-item questionnaire rated on a 4-point Likert scale, with scores ranging from 17 to 68. Participants scoring above 40 were classified as presenting with kinesiophobia. Fear-avoidance beliefs were measured using the Fear-Avoidance Beliefs Questionnaire (FABQ),37 with both the physical activity subscale (FABQ-PA, scored from 0 to 24) and the work subscale (FABQ-W, scored from 0 to 42). The TAMPA and the FABQ are two questionnaires that have been validated for patients with chronic pain and it would not have been relevant for pain-free participants to complete these two questionnaires. It should be noted that this asymmetry in questionnaire administration limits direct between-group comparisons on these variables; accordingly, only the HADS, which was administered to both groups, was used for comparative analyses.
Two others questionnaires were completed by all the participants. Trait self-control was assessed using the Trait Self-Control Scale,38 which is designed to assess interindividual differences in self-control capacities, with scores ranging from 13 to 65 (α = 0.75). Work-related stress as well as working conditions were evaluated using the Job Content Questionnaire,39 which includes psychological demand (9–36) (α = 0.43), decision latitude (24–96) (α = 0.68), and social support (8–32) (α = 0.64). The questionnaires were completed by the participants in the form of individual interviews that took place before the start of the experiment. In this way, we ensured that there was no problem understanding the statements, that each answer was formulated instinctively and that the conditions for passing were the same. Each session was then designed in three sequences carried out consecutively. The participants benefited from familiarization time with the tasks before each of these sequences.
Pain Assessment
Pain intensity was assessed prior to the experimental session using the short French version of the Brief Pain Inventory (BPI).40 This self-administered 4-item questionnaire uses numeric rating scales from 0 (no pain) to 10 (pain as bad as you can imagine) to evaluate pain intensity across several temporal dimensions, including the most severe, least, usual, and current pain. The BPI is a validated and widely used tool in both clinical and research settings, demonstrating good internal consistency (α =0.93). For the pain-free control group, no pain questionnaire was administered, since the absence of chronic pain was an inclusion criterion. In addition, during the handgrip task, participants reported their perceived pain every 30 seconds using a visual analog scale. This repeated assessment allowed us to monitor fluctuations in pain during the physical task and to ensure that pain levels remained comparable across experimental conditions. Finally, all experimental procedures were conducted within a single session under standardized conditions, thereby limiting potential variability in pain levels across conditions.
Statistical Analysis
Statistical analyses were conducted using fixed-effects models, primarily through univariate analyses of variance (ANOVAs). When applicable, higher-order interactions were examined first, followed by the interpretation of significant lower-order effects. When interactions were not significant, only the main effects relevant to the study hypotheses were reported. For repeated-measures factors with more than two levels, multivariate analyses of variance (MANOVAs) were conducted to avoid violations of the sphericity assumption. Post hoc comparisons were performed using Bonferroni corrections when multiple comparisons were involved. The main analyses were hypothesis-driven and focused on a limited number of planned comparisons directly related to the study objectives, namely the effects of mental fatigue on time-to-exhaustion performance. Separate analyses were conducted for patients with chronic low back pain and pain-free participants due to baseline differences between groups, which could not be adequately controlled without substantially increasing model complexity. To describe group characteristics, one-way ANOVAs and chi-square tests were conducted across the four subgroups. These analyses were considered descriptive and exploratory in nature and were not adjusted for multiple comparisons. Given the number of statistical tests performed, the potential inflation of Type I error was considered. However, this risk was mitigated by the hypothesis-driven nature of the primary analyses and the use of Bonferroni corrections for post hoc tests. Therefore, results from secondary or exploratory analyses should be interpreted with caution. Effect sizes were reported to complement p-values. For ANOVAs, eta squared (η2) was used; for chi square tests, Cramér’s V was reported; and for t-tests, Cohen’s d was calculated. Effect sizes were interpreted according to guidelines for pain research,41 with thresholds of 0.10 (small), 0.30 (medium), and 0.70 (large) for Cohen’s d, 0.10, 0.30 and 0.50 for Cramèr’s V, and 0.01 (small), 0.09 (medium), and 0.50 (large) for η2.
Results
Characteristics of the Participants
A one-way univariate ANOVA was conducted on each characteristic of the participants with Group (cLBP patients allocated to the Stroop task, cLBP patients allocated to the Video task, pain-free participants allocated to the Stroop task, and pain-free participants allocated to the Video task) as a between-subjects factor. The differences among the four groups are summarized in Table 1.
Regarding the socioprofessional category of the participants, Table 1 shows that the group of cLBP patients included fewer intermediary professions and more workers and employees than the group of pain-free participants. This result is consistent with the job-content questionnaire data since cLBP patients perceived more psychological demands and less decisional latitude and social support. Additionally, cLBP patients had higher BMI, anxiety and depression scores and lower performance in the time-to-exhaustion test in the first handgrip task. The two populations (cLBP patients and pain-free participants) clearly presented different profiles in terms of at least four different characteristics. We decided to conduct separate analyses for cLBP patients and pain-free participants because including all four groups in a single ANOVA would have required controlling for too many covariates in an ANCOVA, thereby increasing the risk of a Type II error. However, differences between the two populations will be taken into account when interpreting the results, without making a direct comparison.
Since the initial performance of the LV and AS groups in the handgrip task was not homogeneous, the performance in the TTE task was calculated separately for each participant as follows: TTE delta (s) = time-to-exhaustion in the second handgrip task minus time-to-exhaustion in the first handgrip task. Finally, to highlight the acute mental fatigue effect, a two-way ANOVA on the TTE delta was conducted with Population (cLBP, pain-free) and Task (Stroop, Video) as the between-subject factors.
Manipulation Checks
Maximal Voluntary Contraction
If participants followed the instructions and performed the handgrip task until exhaustion, their maximum voluntary contraction (MVC) should have significantly decreased between the beginning and the end of the handgrip task. Consequently, we conducted a mixed ANOVA on MVC with Session time (before and after the cognitive task) and Handgrip time (before and after the TTE handgrip task) as repeated-measures factors and Task group (Stroop vs. Video) as a between-subjects factor, separately for cLBP patients and pain-free participants.
In cLBP patients, both groups significantly decreased their MVC from before to after the TTE handgrip task. However, we observed a significant interaction effect between task group and handgrip time, showing that the cLBP patients included in the Stroop group presented a greater decrease in MVC (M = 17.67%; SD = 10.07%) than did the cLBP patients included in the video group (M = 12.09%; SD = 7.65%) regardless of the session time: F (1, 58) = 7.643; p <0.05; η2 =0.116 (Figure 2A). In pain-free participants, both groups also significantly decreased their MVC from before to after the TTE handgrip task: F (1, 58) = 162.018; p <0.05; η2 =0.736 (Figure 2B). The interaction effect between task group and handgrip time was not significant. On average, pain-free participants exhibited a 17.69% decrease in MVC (SD = 10.22%). Globally, participants in the four groups followed the instruction of squeezing the handgrip until exhaustion since we observed a significant decrease in MVC at the beginning and at the end of the session.
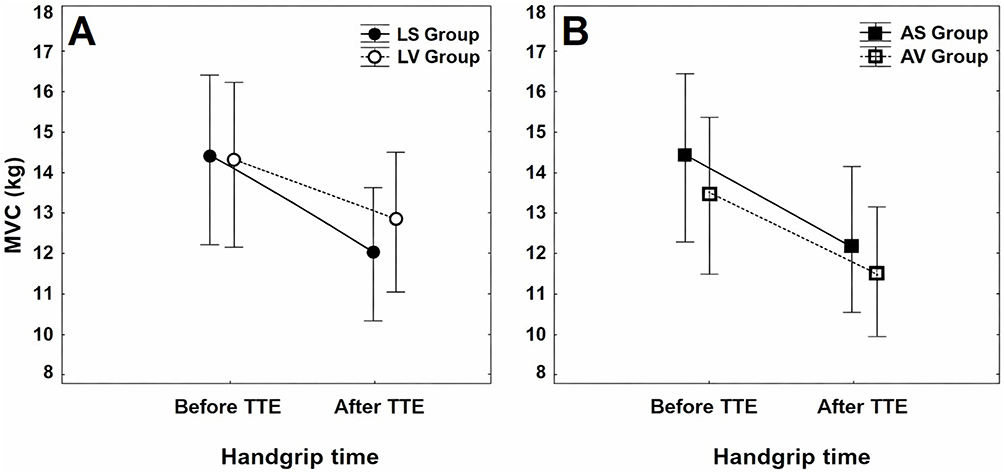 |
Figure 2 Maximal voluntary contraction as a function of Handgrip time measurement (before and after the time-to-exhaustion handgrip task) and Task group. Panel (A) LS = LBP patients Stroop group, LV = LBP patients Video group. Panel (B) AS = Asymptomatic pain-free participants Stroop group, AV = Asymptomatic pain-free participants Video group. Error bars denote 0.95 confidence intervals. |
Perceived Difficulty of the Cognitive Task
The Stroop task involved two executive functions (inhibitory control and cognitive flexibility) that required cognitive control, whereas in the video task, watching the documentary required a low level of cognitive control. A one-way ANOVA showed that the Stroop task was perceived as more difficult (MLS = 75.30) by cLBP patients than the video task (MLV = 7.07): F (1, 58) = 176.017; p <0.05; η2 =0.752. The same results were obtained for the pain-free participants: F (1, 58) = 106.985; p <0.05; η2 =0.648 (MAS = 73.60 vs. MAV = 18.47).
Perceived Fatigue
The Stroop task was designed to induce a high level of mental fatigue, and the video task, as a control task, was designed to induce a low level of mental fatigue. A mixed ANOVA was conducted on perceived fatigue in cLBP patients with Session time (before and after the cognitive task) as a repeated-measures factor and Task group (Stroop vs. Video) as a between-subjects factor. The interaction between session time and task group was significant: F (1, 57) = 9.221; p <0.05; η2 =0.139 (Figure 3A). A Bonferroni post hoc correction revealed that cLBP patients who performed the Stroop task (LS group) perceived a greater level of fatigue after the cognitive task than before, whereas cLBP patients who performed the video task (LV group) did not show a change in their perceived fatigue. The same analysis was conducted in pain-free participants. The interaction between session time and task group was close but did not reach significance: F (1, 56) = 3.146; p =0.088; η2 = 0.053. However, the simple effect of session time was significant: F (1, 56) = 11.900; p <0.05; η2 =0.175 (Figure 3B). A Bonferroni post hoc correction revealed that pain-free participants who performed the Stroop task (AS group) perceived a greater level of fatigue after the cognitive task than before, whereas pain-free participants who performed the Video task (AV group) did not show a change in their perceived fatigue.
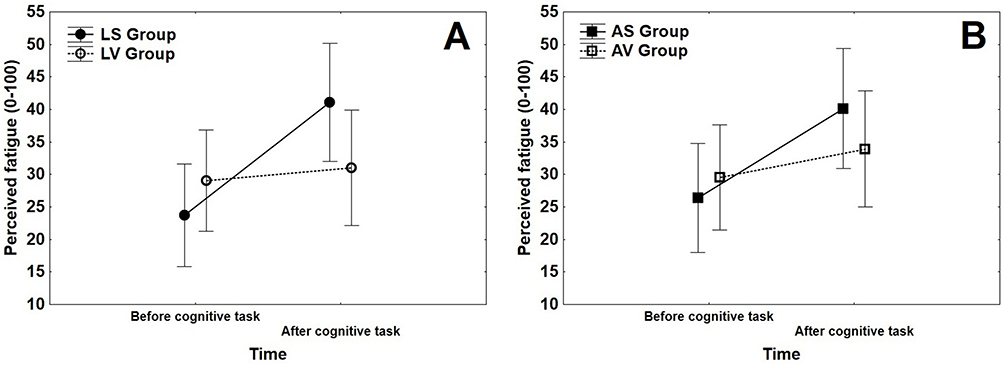 |
Figure 3 Perceived fatigue as a function of time of measurement (before and after the cognitive task) and group of participants. Panel (A) LS = LBP patients Stroop group; LV = LBP patients Video group. Panel (B) AS = Asymptomatic pain-free participants Stroop group; AV = Asymptomatic pain-free participants Video group). Error bars denote 0.95 confidence intervals. |
Induction of Mental Fatigue
To explore changes in performance across time during the Stroop task, we conducted repeated-measures MANOVA with Time-on-Task (T1, T2, T3, and T4) and Type of trials (naming vs. reading) on RT in cLBP patients. The interaction between time-on-task and type of trial did not reach significance: F (3, 27) = 2.335; p =0.096; Wilks’ lambda =0.794; η2 =0.206. Similarly, the simple effect of time-on-task was not significant: F (3, 27) = 2.669; p =0.068; Wilks’ lambda =0.771; η2 =0.229. However, the simple effect of the type of trial reached significance: F (1, 29) = 223.768; p <0.05; η2 =0.885. The RTs for the naming trials were significantly slower (M = 811.738 ms, SD = 81.120 ms) than those for the reading trials (M = 653.053 ms; SD = 69.712 ms). The same analysis was conducted for the error rate. The interaction between time-on-task and type of trial did not reach significance: F (3, 27) = 1.224; p =0.320; Wilks’ lambda =0.880; η2 =0.120. In contrast, the effect of time-on-task reached significance: F (3, 27) = 6.949; p <0.05; Wilks’ lambda =0.564; η2 =0.436 (see Figure 4). A Bonferroni post hoc correction revealed that participants significantly decreased their error rate from part 1 (T1) to parts 3 (T3) and 4 (T4). cLBP patients showed a practice effect: they improved their performance over time. Finally, there was a significant effect of trial type: F (1, 29) = 52.301; p <0.05; Wilks’ lambda =0.357; η2 =0.643. cLBP patients made more errors in naming trials (M = 0.075; SD = 0.057) than in reading trials (M = 0.019; SD = 0.023). Naming trials led to slower RT and a greater number of errors. The same MANOVAs were conducted for RT and the error rate in pain-free participants, and we obtained exactly the same results as those for cLBP patients. Detailed performance metrics for the cognitive task (reaction times and error rates) are provided in Table 1 and Table S2.
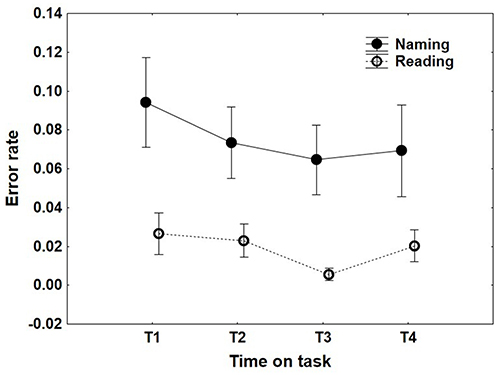 |
Figure 4 Effect of Time-on-task on error rate in the Stroop task for the low-back pain patients. Naming = trials in which participants had to name the color of the word; Reading = trials in which participants had to read the word. |
Effects of Mental Fatigue on the TTE Handgrip Task
We first conducted a Student’s t test on the TTE delta in the handgrip task with Task group (Stroop vs. Video) as a between-subjects factor in cLBP patients. We excluded one participant (ie., outlier) who had data that were more than two standard deviations away from the mean. The results of this participant disfavored the hypothesis. The effect of the task group reached significance: t (57) = −2.406; p <0.05; d = −0.627 (see Figure 5). The difference between the second and the first time-to-exhaustion tasks was significantly greater after the Stroop task (M = −124.448 s, SD = 86.133 s) than after the documentary (M = −71.133 s, SD = 80.047 s), indicating that the cLBP patients dropped out earlier after the Stroop task than after the documentary.
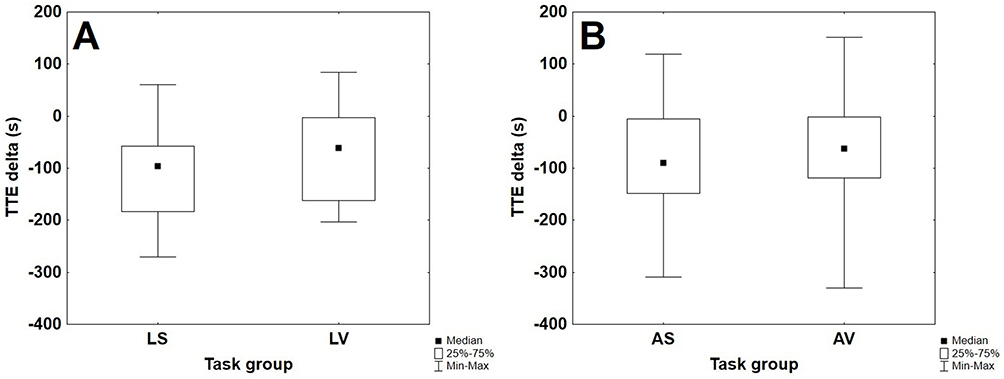 |
Figure 5 Box and whisker plot for the four groups of participants illustrating the distributions of time-to-exhaustion delta as a function of group. Panel (A) LS = Low-back pain patients performing the Stroop task; LV = Low-back pain patients watching the documentary. Panel (B) AS = Asymptomatic pain-free participants performing the Stroop task; AV = Asymptomatic pain-free participants watching the documentary. TTE delta = TTE in the second handgrip task – TTE in the first handgrip task). |
Another Student’s t test was conducted for the pain-free participants. We excluded three participants (ie., outliers) whose data deviated from the mean by more than two standard deviations: one favoring the hypothesis and the two others disfavoring the hypothesis. The effect of the task group was not significant: t (55) = −0.464; p =0.644; d = −0.123.
Discussion
This study aimed to examine whether mental fatigue could reduce engagement in a long and demanding effortful task among cLBP patients compared with a pain-free group. The results revealed that patients with cLBP disengaged earlier from the TTE handgrip task after the Stroop task than after the control task, whereas pain-free participants showed no difference between conditions. In addition, both populations showed comparable performance during the 30-min Stroop task, indicating that inhibitory control was not altered for either group. Notably, and contrary to our hypothesis, this comparable performance reflected stable or improved performance over time, suggesting a practice effect rather than cognitive deterioration. This dissociation between objective cognitive performance and subjective fatigue states indicates that cognitive decline is not a necessary marker of mental fatigue. The discussion will focus primarily on the cLBP group results.
Within the cLBP group, a significant mental fatigue effect emerged under depletion conditions than under the control condition, with a medium effect size, consistent with prior research in chronic pain populations.28,29,42,43 The handgrip time-to-exhaustion task primarily measures the ability to sustain physical effort (see Supplementary Material 3 [Figure S1 Panel A – Figure S1 Panel B]). The earlier disengagement cannot be attributed to reduced motivation (see Supplementary Material 2), greater boredom (see Supplementary Material 1), or higher pain levels during the handgrip task (see Supplementary Material 4). It is thus plausible to argue that acute mental fatigue contributed to reduced physical performance, although other factors such as physical fitness, BMI, or activity level cannot be entirely ruled out.
According to Nes et al,43 self-regulatory fatigue constitutes a distinct construct, independent of anxiety and depression, a view supported by the absence of correlations between depression and anxiety symptoms and handgrip task performance in our data. They suggest that self-regulatory fatigue may be a critical yet underrecognized dimension in understanding chronic multisymptomatic illnesses. Similarly, Holmqvist et al44 posited that mental fatigue, closely related to self-regulatory fatigue, may serve as a specific hallmark of chronic pain.
Two complementary theoretical interpretations may help contextualize these findings, although both remain speculative. First, individuals with cLBP often exhibit heightened sensitivity to physical fatigue, and impairments in muscular endurance have been consistently associated with the condition.45 Mental fatigue has furthermore been shown to impair muscular endurance more than maximal strength,14 and fatigued participants may increasingly rely on interoceptive cues that are likely altered in chronic pain populations.46 This underscores the importance of incorporating body‒mind connections in research on mental fatigue and pain.47
Second, prior cognitive fatigue may bias the subjective cost-benefit ratio, leading to earlier disengagement from subsequent physical effort, a tendency likely amplified in cLBP patients by heightened self-regulatory demands, maladaptive pain beliefs (eg., fear of movement), and mood-related factors.48 Future studies should test these interpretations using direct measures of interoception and effort-based decision-making.
The observed correlation between the Shirado-Ito test and performance on handgrip performance (r =0.36; p <0.05; medium effect size; see Supplementary Material 5 and Table S1) suggests these two measures share common underlying construct related to vitality capacity,49 despite assessing different muscle groups. Further research could examine whether handgrip endurance constitutes a valid proxy for vitality capacity in cLBP populations.
The present findings should be interpreted carefully given several contextual factors. cLBP patients reported more stressful and controlling work environments, predominantly belonging to working-class and employee’s socio-occupational categories. They also presented with higher BMI than pain-free controls (small effect size). These psychosocial and physical factors may partly explain earlier effort disengagement, and their respective contributions cannot be fully disentangled from those of chronic pain and mental fatigue.
Several limitations warrant acknowledgment. First, the emotional bonds between the experimenter and the patients who were enrolled in a rehabilitation program differed from those with volunteers, which may have influenced commitment to the fatiguing tasks.
Second, the absence of a mental fatigue effect in pain-free participants may reflect lower engagement, and learning effect may have obscured trait fatigue effects in both groups.49 Future studies should include a familiarization session and assess baseline fatigue before cognitive induction.42 The handgrip test’s specificity as a mental fatigue indicator also warrants further study; whole-body endurance tasks (eg., cycling or walking at fixed aerobic load) may provide complementary validation.
Third, significant baseline differences between groups (ie., BMI, time to exhaustion in the handgrip task at baseline, anxiety, depression, subscales of the job content questionnaire) limit the ability to isolate the unique contribution of chronic pain. Importantly, chronic low back pain and other musculoskeletal disorders are associated with multiple comorbidities and lifestyle factors, including anxiety, depression, and sedentariness.50,51 The use of different psychological questionnaires across groups (TAMPA and FABQ administered to cLBP patients only) further restricts direct between-group comparisons.
An additional limitation concerns the assessment of pain. Although pain intensity was measured prior to the experimental session and repeatedly during the handgrip task, it was not systematically assessed immediately before each experimental condition. Therefore, we cannot entirely rule out the possibility that fluctuations in momentary pain may have influenced performance. Future studies should include real-time assessment of pain before each task to better control for its potential confounding effects.
Finally, in accordance with the principle of data minimization, we relied on existing psychological assessments previously administered by therapists as part of routine clinical care. As these assessments were not conducted for research purposes, it is not possible to verify the psychometric properties or administration conditions of the scales used. However, to reduce participant burden and avoid redundant data collection, we opted not to re-administer the same questionnaires. This approach aligns with ethical and legal standards. Future studies with prospective designs would benefit from standardized administration of validated measures.
Clinical and Research Implications
The present findings have meaningful implications for clinical practice and future research. From a clinical standpoint, routine assessments of cLBP patients should extend beyond physical capabilities to include mental fatigue as a core symptom, as it may impact patients’ capacity to engage in rehabilitation programs and daily activities, even when physical capacity appears adequate. The handgrip endurance task represents a simple, low-cost tool that could be integrated into functional capacity evaluations to objectively detect mental fatigue and inform personalized treatment planning.
Physical activity programs aimed at increasing tolerance or resistance to fatigue could be particularly beneficial for cLBP patients. These programs should be designed with consideration of mental fatigue, potentially incorporating strategies to enhance self-regulatory capacity and interoceptive awareness. Given the documented relationship between mental fatigue and physical endurance, rehabilitation protocols that address both dimensions may yield superior outcomes compared to those targeting physical restoration alone.
From a research perspective, future studies should distinguish fatigue as a comorbidity of depression or anxiety from fatigue arising directly from chronic pain and its management demands. Longitudinal designs could clarify temporal relationships between pain chronicity, mental fatigue, and functional outcomes. Research examining the mechanisms underlying heightened susceptibility to mental fatigue in cLBP—particularly the roles of altered interoception, biased effort-cost evaluation, and compromised self-regulatory resources—would advance theoretical understanding and inform targeted interventions.
Finally, validation of handgrip endurance as a proxy for vitality capacity in chronic pain populations could facilitate more comprehensive functional assessment where whole-body testing is impractical or contraindicated.
Conclusions
Mental fatigue is rarely assessed in patients with cLBP, yet it significantly impacts their ability to sustain physical effort. Standard endurance tests used in low back pain assessment (eg., the Biering-Sorensen test or Shirado-Ito test) do not capture this dimension, and self-reported fatigue measures appear insufficiently sensitive to detect it. The present study demonstrates that mental fatigue selectively impairs physical endurance in cLBP patients, an effect not observed in pain-free individuals, and that the handgrip endurance task offers a simple, low-cost, and objective means of detecting this impairment. Standard functional capacity evaluations may therefore systematically underestimate patients’ true capabilities when mental fatigue goes unrecognized.
These findings support integrating mental fatigue assessment into comprehensive pain evaluation protocols. The handgrip endurance task could help identify patients with increased susceptibility to mental fatigue and monitor fatigue-related changes over the course of rehabilitation, thereby allowing clinicians to better tailor intervention programs. These findings also highlight the importance of considering mental fatigue as a relevant dimension contributing to inter-individual variability in functional performance. Rehabilitation programs may also benefit from incorporating fatigue management strategies, such as cognitive load reduction, pacing techniques, and self-regulation skills training, alongside traditional physical interventions. However, these clinical perspectives require confirmation in future intervention studies.
Further research should establish normative values, examine test-retest reliability, and evaluate the task’s sensitivity to clinical change. Given the high prevalence of mental fatigue in cLBP and its impact on functional performance, developing validated assessment tools represents an important step toward more comprehensive, patient-centered pain management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank the American Journal Experts for their evaluation of the English version of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the French National Association for Research and Technology (ANRT) under grant number CIFRE Convention No. 2019/0559, and by the Regional Council of New Aquitaine (convention n° AAPR2022-2021-17359910).
Disclosure
The authors report no conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Perry M, Dean S, Devan H. The relationship between chronic low back pain and fatigue: a systematic review. Phys Ther Rev. 2016;21(3–6):173–14. doi:10.1080/10833196.2016.1264665
2. Zengarini E, Ruggiero C, Pérez-Zepeda MU, et al. Fatigue: relevance and implications in the aging population. Exp Gerontol. 2015;70:78–83. doi:10.1016/j.exger.2015.07.011
3. Snekkevik H, Eriksen HR, Tangen T, Chalder T, Reme SE. Fatigue and depression in sick-listed chronic low back pain patients. Pain Med. 2014;15(7):1163–1170. doi:10.1111/pme.12435
4. Barfety-Servignat V. Douleur et fatigue. Douleur Analg. 2022;35:1. doi:10.3166/dea-2022-0210
5. Silvestrini N. Implication de la capacité de contrôle cognitif dans l’expérience de la douleur. Rev Med Suisse. 2014;10:1378–1381. doi:10.53738/REVMED.2014.10.436.1378
6. Beaupré M, McKerral M. Impact of chronic pain on cognition and concomitant psychological factors. Rev Neuropsychol. 2012;1:53–59. doi:10.1684/nrp.2012.0203
7. Fishbain DA, Cole B, Cutler RB, Lewis J, Rosomoff HL, Rosomoff RS. Is pain fatiguing? A structured evidence-based review. Pain Med. 2003;4:51–62. doi:10.1046/j.1526-4637.2003.03008.x
8. Yamada K, Adams H, Ellis T, et al. The temporal relation between pain and fatigue in individuals receiving treatment for chronic musculoskeletal pain. BMC Musculoskelet Disord. 2022;23:219. doi:10.1186/s12891-022-05162-7
9. Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 2013;14:502–511. doi:10.1038/nrn3516
10. André N, Baumeister RF. Three Pathways Into Chronic Lack of Energy as a Mental Health Complaint. European Journal of Health Psychology. 2023;30(2):87–101. doi:10.1027/2512-8442/a000123
11. Elman I, Borsook D. Threat Response System: parallel Brain Processes in Pain vis-à-vis Fear and Anxiety. Front Psychiatry. 2018;9:29. doi:10.3389/fpsyt.2018.00029
12. Druce KL, McBeth J. Central sensitization predicts greater fatigue independently of musculoskeletal pain. Rheumatology. 2019;58(11):1923–1927. doi:10.1093/rheumatology/kez028
13. Louati K, Berenbaum F. Fatigue in chronic inflammation—a link to pain pathways. Arthritis Res Ther. 2015;17:254. doi:10.1186/s13075-015-0784-1
14. Van Cutsem J, Marcora S, De Pauw K, Bailey S, Meeusen R, Roelands B. The Effects of Mental Fatigue on Physical Performance: a Systematic Review. Sports Med. 2017;47:1569–1588. doi:10.1007/s40279-016-0672-0
15. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–153. doi:10.1016/0022-3999(93)90081-p
16. Adnan R, Van Oosterwijck J, Danneels L, et al. Differences in psychological factors, disability and fatigue according to the grade of chronification in non-specific low back pain patients: a cross-sectional study. J Back Musculoskelet Rehabil. 2020;33(6):919–930. doi:10.3233/BMR-191548
17. Kauffman BY, Manning K, Rogers AH, Matoska CT, Zvolensky MJ. Anxiety sensitivity and fatigue severity among adults with chronic low back pain. Fatigue. 2021;9(4):227–235. doi:10.1080/21641846.2021.2009684
18. Saravanan A, Bajaj P, Matthews HL, Tell D, Starkweather A, Janusek L. Fatigue and depressive mood in chronic low back pain. Pain Manag Nurs. 2024;25(3):225–230. doi:10.1016/j.pmn.2024.02.003
19. Purto H, Anabalon H, Vargas K, Jara DC, de la Vega R. Self-perceptual blindness to mental fatigue in mining workers. Front Neuroergon. 2024;5:1441243. doi:10.3389/fnrgo.2024.1441243
20. Weiler H, Russell S, Spielmann J, Englert C. Mental Fatigue: is It Real? J Appl Sport Exerc Psychol. 2025. doi:10.1026/2941-7597/a000033
21. André N, Audiffren M, Baumeister RF. An integrative model of effortful control. Front Syst Neurosci. 2019;13:79. doi:10.3389/fnsys.2019.00079
22. Holroyd CB. The controllosphere: the neural origin of cognitive effort. Psychol Rev. 2024;132:603–631. doi:10.1037/rev0000467
23. Pessiglione M, Blain B, Wiehler A, Naik S. Origins and consequences of cognitive fatigue. Trends Cognit Sci. 2025;29(8):730–749. doi:10.1016/j.tics.2025.02.005
24. Chaudhuri A, Behan PO. Fatigue in neurological disorders. Lancet. 2004;363(9413):978–988. doi:10.1016/S0140-6736(04)15794-2
25. Walker LA, Berard JA, Berrigan LI, Rees LM, Freedman MS. Detecting cognitive fatigue in multiple sclerosis: method matters. J Neurol Sci. 2012;316(1–2):86–92. doi:10.1016/j.jns.2012.01.021
26. Bautmans I, Mets T. A fatigue resistance test for elderly persons based on grip strength: reliability and comparison with healthy young subjects. Aging Clin Exp Res. 2005;17(3):217–222. doi:10.1007/BF03324600
27. Bautmans I, Knoop V, Thiyagarajan A, et al. Banerjee AWHO working definition of vitality capacity for healthy longevity monitoring. Lancet Healthy Longev. 2022;3:e789–96. doi:10.1016/S2666-7568(22)00200-8
28. Daneshgar-Pironneau S, Audiffren M, Benraïss A, Métais A, André N. Mental fatigue impairs endurance performance in a time-to-exhaustion handgrip task: psychophysiological markers of effort engagement dynamics. Front Psychol. 2025;16:1611135. doi:10.3389/fpsyg.2025.1611135
29. Mangin T, André N, Benraïss A, Pageaux B, Audiffren M. No ego-depletion effect without a good control task. Psychol Sport Exerc. 2021;57:102033. doi:10.1016/j.psychsport.2021.102033
30. De Dobbeleer L, Beyer I, Njemini R, et al. Force-time characteristics during sustained maximal handgrip effort according to age and clinical condition. Exp Gerontol. 2017;98:192–198. doi:10.1016/j.exger.2017.08.033
31. Brown DM, Bray SR. Isometric exercise and cognitive function: an investigation of acute dose-response effects during submaximal fatiguing contractions. J Sports Sci. 2015;33(5):487–497. doi:10.1080/02640414.2014.947524
32. Hagger MS, Wood C, Stiff C, Chatzisarantis NL. Ego depletion and the strength model of self-control: a meta-analysis. Psychol Bull. 2010;136(4):495–525. doi:10.1037/a0019486
33. Forestier C, de Chanaleilles M, Boisgontier MP, Chalabaev A. From ego depletion to self-control fatigue: a review of criticisms along with new perspectives for the investigation and replication of a multicomponent phenomenon. Motiv Sci. 2022;8(1):19–32. doi:10.1037/mot0000262
34. Fothergill A, Linfield M. Earth [Documentary]. Disneynature, BBC Worldwide, Greenlight Media AG; 2009.
35. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
36. Miller RP, Kori SH, Todd DD. The Tampa Scale: a Measure of Kinisophobia. Clin J Pain. 1991;7(1):51.
37. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–168. doi:10.1016/0304-3959(93)90127-B
38. Tangney JP, Baumeister RF, Boone AL. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J Pers. 2004;72(2):271–324. doi:10.1111/j.0022-3506.2004.00263.x
39. Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an Instrument for Internationally Comparative Assessments of Psychosocial Job characteristics. J Occup Health Psychol. 1998;3:322–355. doi:10.1037//1076-8998.3.4.322
40. Agence Nationale d’Accréditation et d’Evaluation en Santé. Évaluation et suivi de la douleur chronique chez l’adulte en médecine ambulatoire. Paris: Service des Recommandations et Références Professionnelles; 1999.
41. Zieliński G. Getting to Know Pain Effect Sizes-Guidelines for Effect Size and Sample Size in Global Pain Research. Arch Phys Med Rehabil. 2026;107(4):726–733. doi:10.1016/j.apmr.2026.01.006
42. Lorcery A, André N, Benraïss A, Pingault M, Mirabelli F, Audiffren M. Engagement of mental effort in response to mental fatigue: a psychophysiological analysis. Psychol Sport Exerc. 2024;74:102660. doi:10.1016/j.psychsport.2024.102660
43. Nes LS, Ehlers SL, Whipple MO, Vincent A. Self-Regulatory Fatigue: a Missing Link in Understanding Fibromyalgia and Other Chronic MultiSymptom Illnesses. Pain Pract. 2017;17(4):460–469. doi:10.1111/papr.12480
44. Holmqvist A, Berginström N, Löfgren M, Stalnacke BM, Möller MC. Fatigue and cognitive fatigability in patients with chronic pain. Scand J Pain. 2024;24:20230085. doi:10.1515/sjpain-2023-0085
45. Pincus T, Santos R, Breen A, Burton AK, Underwood M. A review and proposal for a core set of factors for prospective cohorts in low back pain: a consensus statement. Arthritis Rheumatol. 2008;59:14–24. doi:10.1002/art.23251
46. Horsburgh A, Summers SJ, Lewis A, Keegan RJ, Flood A. The relationship between pain and interoception: a systematic review and meta-analysis. J Pain. 2024;25:104476. doi:10.1016/j.jpain.2024.01.341
47. Oliveira I, Vaz Garrido M, Carvalho H, Figueira Bernardes S. Sensing the body matters: profiles of interoceptive sensibility in chronic pain adjustment. Pain. 2024;165:412–422. doi:10.1097/j.pain.0000000000003032
48. Løke D, Løvstad M, Andelic N, Andersson S, Ystrom E, Vassend O. The role of pain and psychological distress in fatigue: a co-twin and within-person analysis of confounding and causal relations. Health Psychol Behav Med. 2022;10:160–179. doi:10.1080/21642850.2022.2033121
49. Skau S, Sundberg K, Kuhn HG. A proposal for a unifying set of definitions of fatigue. Front Psychol. 2021;12:739764. doi:10.3389/fpsyg.2021.739764
50. Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Association of depression and anxiety alone and in combination with chronic musculoskeletal pain in primary care patients. Psychosom Med. 2008;70(8):890–897. doi:10.1097/PSY.0b013e318185c510
51. Park HJ, Choi JY, Lee WM, Park SM. Prevalence of chronic low back pain and its associated factors in the general population of South Korea: a cross-sectional study using the National Health and Nutrition Examination Surveys. J Orthop Surg Res. 2023;18(1):29. doi:10.1186/s13018-023-03509-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Regarding Chronic Ankle Instability and Its Management Among Ankle Sprain Patients: A Cross-Sectional Study
Wang B, Xue Z, XU W, Li B, Yang Y
Journal of Multidisciplinary Healthcare 2026, 19:585206
Published Date: 20 February 2026
Return to Work Status and Influencing Factors Among Young and Middle-Aged Patients with Stanford Type A Aortic Dissection After Cardiac Surgery: A Random Forest Model Analysis
Chen S, Huang Y, Cheng Y, Chen H, You T
International Journal of General Medicine 2026, 19:582277
Published Date: 11 March 2026