Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Knowledge, Attitudes, and Practices Regarding Chronic Ankle Instability and Its Management Among Ankle Sprain Patients: A Cross-Sectional Study
Authors Wang B, Xue Z, XU W, Li B, Yang Y
Received 28 November 2025
Accepted for publication 14 February 2026
Published 20 February 2026 Volume 2026:19 585206
DOI https://doi.org/10.2147/JMDH.S585206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Bibo Wang,1 Zhaolong Xue,2 WeiFan XU,2 Bing Li,1 Yunfeng Yang1
1Department of Orthopaedics, Shanghai Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China; 2Department of Orthopaedics, Shanghai Nanxiang Hospital, Shanghai, 201802, People’s Republic of China
Correspondence: Bibo Wang, Department of Orthopaedics, Shanghai Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China, Tel +86-13061723369, Email [email protected]
Background and Objective: This study assessed the knowledge, attitudes, and practices (KAP) of patients with ankle sprains regarding chronic ankle instability (CAI) and its management.
Methods: This cross-sectional study was conducted in Shanghai from June 2024 to August 2024 among adults with a history of ankle sprain. Participants completed an electronic self-administered questionnaire assessing knowledge, attitudes, and practices regarding chronic ankle instability and its management. Spearman correlation and structural equation modeling with bootstrap resampling were used to examine associations and pathways among KAP dimensions.
Results: Among the participants, 289 (51.60%) were males, 288 (51.45%) reported occasional exercise, and 207 (36.95%) currently experienced ankle instability. The mean scores for knowledge, attitude, and practice were 9.87± 4.54 (possible range: 0– 16), 24.48± 2.97 (possible range: 8– 40), and 27.17± 7.67 (possible range: 9– 45), respectively. Positive correlations were found between knowledge and practice (r=0.4772, P< 0.001). The mediation analysis demonstrated that knowledge (β=0.81, P < 0.001), attitude (β = − 0.34, P < 0.001), and exercise habits (β= − 2.59, P < 0.001) directly affected practice.
Conclusion: The findings suggest predominantly moderate knowledge, attitudes, and practices toward CAI, with significant room for improvement, highlighting the need for educational interventions to enhance prevention, rehabilitation adherence, and long-term management.
Keywords: rehabilitation, functional assessment, prevention, patient education, questionnaire survey
Introduction
Ankle sprains are one of the most common types of musculoskeletal injuries, accounting for approximately 7% to 10% of sports-related injuries.1 They are prevalent not only among athletes but also in the general population, often requiring significant medical attention due to secondary complications.2 Ankle sprains can cause pain, limited range of motion, functional deficits, and even long-term disability. In some cases, these injuries lead to post-traumatic osteoarthritis and CAI, with up to 44% of patients still experiencing symptoms one year after the injury.3 For indoor sports, the incidence of lateral ankle sprains (LAS) has been reported as 7 per 1000 exposures.4 If rehabilitation for an ankle sprain is delayed or ineffective, the risk of the injury progressing to CAI increases significantly.5 Approximately 40–75% of ankle sprains may eventually result in CAI.1,6,7 CAI is characterized by persistent symptoms such as pain, swelling, and instability, often accompanied by recurrent sprains for at least 12 months post-injury. This condition can lead to long-term absence from work and sports.8,9
In recent years, as the understanding of ankle sprain sequelae has deepened, it has been shown that effective rehabilitation can accelerate recovery, and earlier intervention is associated with better outcomes for restoring functional capacity.6 However, despite the large number of patients with ankle sprains, there remains a significant shortage of medical professionals specializing in rehabilitation in Shanghai and other major cities in China.10 Alarmingly, only around 50% of individuals who sustain a lateral ankle sprain seek medical attention.11,12
The Knowledge, Attitude, and Practices (KAP) survey serves as a diagnostic tool to assess a group’s understanding, beliefs, and behaviors related to specific health issues. It operates on the premise that improved knowledge can positively influence attitudes, which in turn can shape behaviors.13,14 The primary objective of such surveys is to identify information gaps and behavioral barriers, laying the foundation for designing more targeted educational interventions. By quantitatively assessing the actual level of knowledge and practice behaviors in patients with ankle sprains, this study aims to raise health awareness, encourage active participation in rehabilitation, reduce the incidence of CAI, and ultimately improve both the quality of life and physical activity levels in this patient population. This study aims to investigate the current KAP of patients with ankle sprains concerning CAI and its prevention and treatment. However, KAP data regarding CAI and its management among ankle sprain patients in China remain limited, which weakens the evidence base for designing targeted patient education and rehabilitation support in routine care.
Methods
Study Design and Participants
This cross-sectional study was conducted from June 2024 to August 2024 in Shanghai, involving patients with ankle sprains. Eligible participants were consecutively recruited from the orthopaedic outpatient clinics and emergency departments at the participating hospitals during the study period, rather than being randomly sampled across the hospital. All adult patients presenting for an ankle sprain-related visit or reporting a prior ankle sprain history during outpatient or emergency department registration/triage were screened for eligibility by the study team. After eligibility was confirmed, patients were invited to participate, and those who agreed voluntarily completed the electronic questionnaire on-site in the outpatient clinic or emergency department via a QR code or direct link provided by the research staff. The inclusion criteria were: 1) patients who had experienced an ankle sprain, 2) aged 18–70 years, and 3) those who voluntarily signed an informed consent form agreeing to complete the questionnaire. The exclusion criteria were: 1) individuals without a history of ankle sprain, 2) those unable to complete the questionnaire due to psychological, psychiatric, or severe medical conditions, and 3) individuals unwilling to complete the questionnaire. For this survey, current ankle instability was defined for participants as experiencing at least one of the following in the past 6 months: (1) recurring ankle sprains during daily activities or sports, (2) frequent sensation of ankle “giving way”, (3) persistent feeling of ankle weakness or instability, or (4) need to wear ankle support for daily activities. This definition was provided to participants in lay terms at the beginning of the relevant survey section. The study was approved by the Ethics Committee of Shanghai Ruijin Hospital, School of Medicine, Shanghai Jiaotong University (Ethics Approval No: (2024) Lin Lun Shen No. 162), and informed consent was obtained from all participants.
Questionnaire Introduction
The questionnaire was developed through a systematic three-phase process. In Phase 1 (Item Generation), we conducted a comprehensive literature review of ankle sprain and CAI management, followed by expert panel consultation including 3 orthopedic surgeons, 2 physiotherapists, and 1 rehabilitation specialist, which led to initial item pool generation covering knowledge, attitudes, and practices dimensions. In Phase 2 (Content Validation), items underwent expert review for content validity using Content Validity Index (CVI), with items scoring CVI > 0.80 being retained. Language was optimized for lay comprehension, followed by translation and back-translation between English and Simplified Chinese. Phase 3 involved Pilot Testing. A total of 36 pre-test questionnaires were returned, with 1 excluded due to refusal to participate and 9 excluded for failing trap questions, resulting in 26 valid questionnaires. The overall Cronbach’s α coefficient for the questionnaire was 0.760, indicating good internal consistency. The final questionnaire was prepared in Simplified Chinese, the standard written form used in Shanghai region. Medical terminology was minimized and replaced with lay language where possible to ensure comprehension. For example, “talar osteochondral injury and osteoarthritis” was described to participants as “joint surface damage and wear” in the questionnaire. The questionnaire consists of four sections: demographic data, knowledge dimension, attitude dimension, and practice dimension. The knowledge dimension includes 8 questions, with scores of 2 for “very well understood,” 1 for “somewhat understood,” and 0 for “not understood,” yielding a possible score range of 0–16. The attitude dimension comprises 8 questions, using a five-point Likert scale ranging from “strongly agree” (5 points) to “strongly disagree” (1 point), with a score range of 8–40. The practice dimension includes 9 questions, with questions 1–5 using a five-point Likert scale from “always” (5 points) to “never” (1 point), resulting in a score range of 9–45. Different response formats were used across sections because the three constructs required different measurement approaches: the knowledge items assessed self-perceived understanding of CAI-related information (0–2 scale), whereas attitude and practice items captured agreement and behavior frequency, respectively (five-point scales). To allow comparison across domains, total scores were additionally interpreted using the percentage-of-maximum approach (eg, 60–80% as moderate and >80% as adequate) as described below. Participants scoring above 80% of the KAP were categorized as having adequate knowledge, a positive attitude, and proactive practices. Those scoring between 60% and 80% were classified as having moderate knowledge, attitude, and practices, while scores below 60% indicated inadequate knowledge, a negative attitude, and inactive practices.15 The questionnaire was distributed electronically through the WenJuanXing platform (Changsha Ranxing Information Technology Co., Ltd., China), a professional electronic survey system. Participants accessed the survey via QR code or direct link on their mobile devices on-site during their outpatient clinic or emergency department visits. The platform’s built-in logic controls ensured complete responses and prevented duplicate submissions.
Sample Size Calculation
Sample size was calculated using the formula for cross-sectional studies: α=0.05, where
where  =1.96 when α=0.05, the assumed degree of variability of p=0.5 maximises the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size was 480 which includes an extra 20% to allow for subjects lost during the study.
=1.96 when α=0.05, the assumed degree of variability of p=0.5 maximises the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size was 480 which includes an extra 20% to allow for subjects lost during the study.
Statistical Analysis
Data analysis was conducted using STATA 17.0 (Stata Corporation, College Station, TX, USA). Continuous variables are presented as means and standard deviations (SD), and categorical variables are expressed as frequencies and percentages (n, %). Normality of the data was assessed, and for between-group comparisons, ANOVA was applied to normally distributed data, while non-parametric tests were used for non-normally distributed data. Spearman correlation analysis was performed to assess the relationships between knowledge, attitude, and practice scores. A two-sided P-value less than 0.05 was considered statistically significant. Mediation analysis was performed using structural equation modeling (SEM) with maximum likelihood estimation. Variables were selected for the SEM model based on those showing significant between-group differences in KAP scores in Table 1. The model included direct paths from demographic variables to KAP scores, and indirect paths through potential mediators. Model fit was assessed using Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), Tucker-Lewis Index (TLI), and Comparative Fit Index (CFI). Bootstrap analysis with 5000 resamples was used to test the significance of indirect effects.
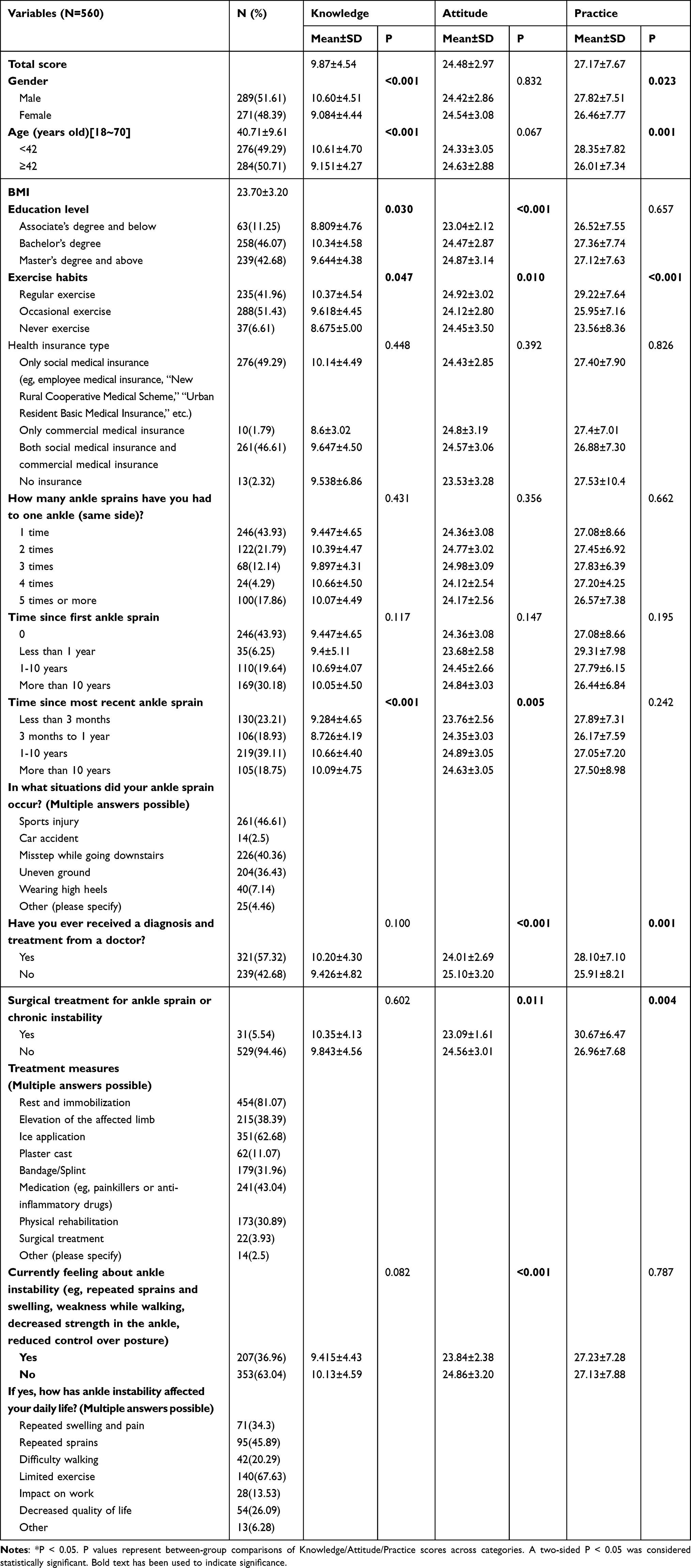 |
Table 1 Demographic Characteristics |
Results
Basic Demographic Characteristics
Of all eligible patients approached during the study period (n=612), 569 agreed to participate (response rate = 93.0%). A total of 569 cases were initially collected in this study. After excluding 9 cases involving individuals under the age of 18, the final dataset comprised 560 valid cases, resulting in an efficiency rate of 98.42%. The formal investigation revealed an overall Cronbach’s α coefficient of 0.905 for the questionnaire, and reliability coefficients of 0.917, 0.854, and 0.881 for knowledge, attitude, and practice respectively, and the KMO value was 0.908 (P < 0.001). Of these, 289 (51.61%) were males, with a mean age of 40.71±9.61 years and a mean BMI of 23.70±3.20 kg/m2. A total of 258 participants (46.07%) held a Bachelor’s degree, 288 (51.43%) reported occasional exercise, 246 (43.93%) had experienced an ankle sprain on the same side at least once, and 207 (36.95%) currently felt ankle instability. Current ankle instability was characterized by participants reporting at least one of the following symptoms in the past 6 months: recurrent sprains (95, 45.89%), ankle weakness during walking (42, 20.29%), limited exercise capacity (140, 67.63%), or impact on daily activities (28, 13.53%).
Knowledge, Attitudes, and Practices Dimensions
The mean scores for knowledge, attitude, and practice were 9.87±4.54, 24.48±2.97, and 27.17±7.67, respectively (Table 1). Knowledge gaps were most evident in three areas: use of ankle braces for prevention (29.64% responded “Not clear”), understanding of potential complications (25.54% responded “Not clear”), and awareness of surgical treatment options (21.43% responded “Not clear”). In the attitude dimension, 28.39% strongly agreed that ankle sprains and CAI severely impact their quality of life (A1), 25.36% expressed significant concern about potential complications and adverse effects (A3), and 18.04% strongly agreed that they felt vulnerable to the effects of ankle sprains and CAI (A2). Regarding practices, 25.71% reported never using assistive devices to reduce ankle load during daily activities (P2), 24.11% never underwent ankle examinations or assessments to monitor rehabilitation progress (P8), and 15.71% never sought help from healthcare professionals to learn about ankle rehabilitation exercises (P3). Based on the scoring criteria, 88 participants (15.71%) were categorized as having adequate knowledge, positive attitude, and proactive practices simultaneously, defined as having all three KAP scores above 80% of their respective maximum scores (knowledge >12.8/16, attitude >32/40, practice >36/45) (Supplementary Table 1).
Correlations Between KAP
Spearman correlation analysis revealed a strong positive correlation between knowledge and practice scores (r = 0.4772, P < 0.001), and a weak but significant correlation between knowledge and attitude scores (r = 0.0888, P = 0.0357). The correlation between attitude and practice scores was not significant (r = −0.0641, P = 0.1300), suggesting that improved attitudes may not directly translate to better practices (Table 2).
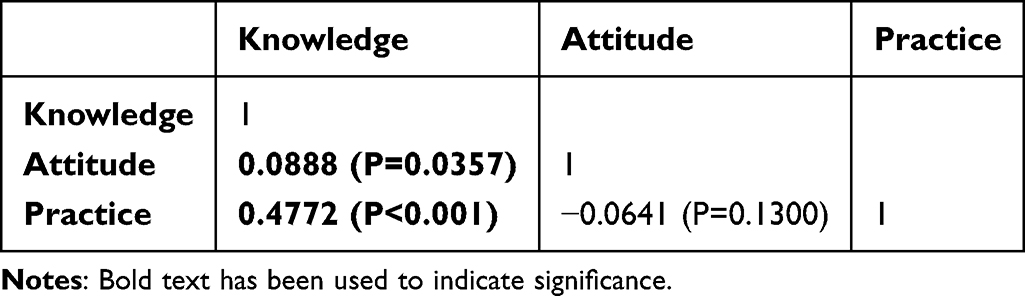 |
Table 2 Spearman Correlation Analysis |
Mediation Analysis
The mediation analysis indicated a highly favorable model fit, with an RMSEA of 0.030, SRMR of 0.017, TLI of 0.957, and CFI of 0.987, suggesting the model fit well (Supplementary Table 2). The results demonstrated that gender (β = −1.24, P = 0.001), age (β = −1.61, P = 0.000), exercise habits (β = −0.64, P = 0.040), and time since the most recent ankle sprain (β = 0.40, P = 0.002) directly affected knowledge. Knowledge (β = 0.05, P = 0.026), education level (β = 0.33, P = 0.001), exercise habits (β = −0.46, P = 0.021), and treatment measures (β = 0.86, P = 0.001) directly affected attitude. Knowledge (β = 0.81, P < 0.001), attitude (β = −0.34, P < 0.001), and exercise habits (β = −2.59, P < 0.001) directly affected practice. In addition, age (β = −0.09, P = 0.048) indirectly affected attitude. Gender (β = −0.98, P = 0.001), age (β = −1.28, P < 0.001), time since the first ankle sprain (β = 0.28, P = 0.014), and treatment measures (β = −0.29, P = 0.012) indirectly affected practice (Table 3 and Figure 1).
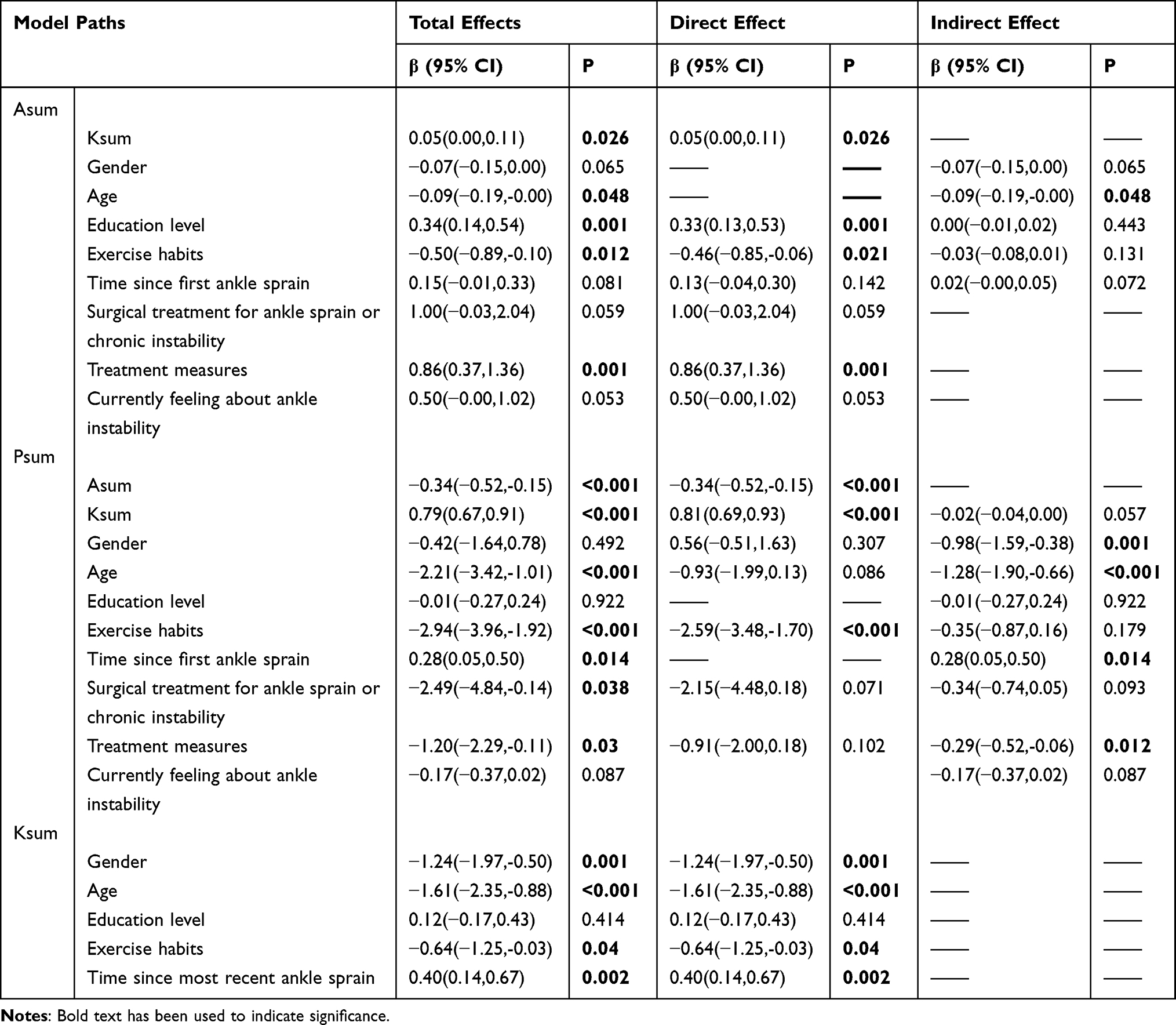 |
Table 3 Mediation Analysis |
 |
Figure 1 Mediation analysis. |
Discussion
This study identified key areas for improvement in patients’ knowledge, attitudes, and practices regarding CAI and its management. The strong correlation between knowledge and practices suggests that targeted educational interventions could effectively enhance patient outcomes in clinical settings.
The study revealed specific knowledge gaps, particularly in understanding preventive measures such as ankle brace usage and recognizing potential complications. These findings align with previous research indicating that improved patient education could enhance prevention strategies and reduce the risk of CAI development.16,17 The lack of adequate KAP among this patient population might contribute to the ongoing challenges in managing and preventing chronic conditions associated with ankle sprains. Therefore, improving patient education and addressing gaps in attitudes and practices should be a key focus in clinical settings to enhance treatment outcomes and prevent future injury recurrence.
Clinically, patients who better understand CAI and its management appear more likely to translate this understanding into preventive and rehabilitation-related behaviors, supporting education as a practical entry point for improving self-management. Patients with better knowledge were more likely to engage in preventive practices and hold positive attitudes toward managing their condition. These results align with prior research, which has demonstrated that increased knowledge correlates with more proactive health behaviors and better self-management of chronic conditions.18,19 Interestingly, the mediation analysis revealed a significant negative direct effect of attitude on practice. This counter-intuitive result suggests that patients with more positive attitudes might not necessarily translate their intentions into actual preventive practices. This may indicate an intention–behavior gap, where favorable perceptions do not necessarily translate into sustained protective or rehabilitation behaviors. From a clinical perspective, structured guidance and follow-up may be needed even for patients who report positive attitudes. For example, the significant association between exercise habits and KAP scores, supported by SEM, indicates that patients who engage in regular exercise tend to have better knowledge, attitudes, and practices. This finding aligns with previous studies in ankle sprain rehabilitation,20,21 showing that regular exercisers demonstrate better adherence to prevention protocols and rehabilitation programs.
The analysis also found significant differences in KAP based on demographic variables, such as gender and age, with males and younger patients exhibiting better knowledge and practices, a result that was supported by SEM outcomes. This could be due to differences in health-seeking behaviors or access to educational resources between these groups. The lack of significant differences in attitudes across age groups suggests that factors such as previous injury experience, access to healthcare resources, and understanding of rehabilitation importance may be more influential in shaping patient attitudes than age alone.22,23
The knowledge dimension revealed that participants lacked clarity on several key aspects of CAI, including its complications and the use of ankle braces. To address this, healthcare providers should prioritize patient education, emphasizing the importance of using braces and other preventive measures. Educational interventions could involve practical demonstrations on how to properly use braces and information on the complications associated with CAI. Tailored educational programs, particularly for patients who have experienced multiple sprains, would be beneficial in improving knowledge and reducing recurrence rates.21,24,25
Attitudes toward ankle instability varied, with many patients not expressing a strong concern for the complications that might arise. This finding suggests a need for targeted psychological and motivational interventions to shift patient perceptions about the severity of ankle instability. Encouraging patients to take ankle sprain prevention seriously, possibly through peer-support programs or behavior change strategies, could improve attitudes.17,26 Implementing strategies that engage patients more actively in their treatment planning and rehabilitation may help increase their sense of responsibility and concern regarding ankle sprain outcomes.
The practice dimension results were moderate, with a significant portion of participants not engaging in preventive measures such as using assistive devices or seeking professional help. These findings highlight areas where clinical practice can be improved, particularly in encouraging routine rehabilitation and the use of protective devices like ankle braces. Specific recommendations include implementing standardized patient education protocols during initial clinical visits, providing visual demonstrations of proper ankle brace usage, establishing regular follow-up schedules to monitor compliance, and developing mobile health applications to support home-based rehabilitation programs. These practical interventions could address the identified knowledge gaps while promoting better self-management practices. Targeted interventions should also focus on older patients, who demonstrated lower practice scores, possibly due to barriers such as physical limitations or lack of access to rehabilitation services.27,28
This study has several limitations. First, the cross-sectional design limits our ability to establish causal relationships between KAP and CAI outcomes. Second, the use of self-reported questionnaires may introduce recall bias, particularly regarding past injury experiences and treatment adherence. Third, while the study was conducted at a major medical center in Shanghai, the findings may not fully represent the situation in other regions of China or different healthcare systems. Future longitudinal studies with objective measures of ankle function and rehabilitation adherence would provide stronger evidence for the relationship between KAP and clinical outcomes.
Conclusions
In conclusion, this study identified specific areas for improvement in patients’ knowledge, attitudes, and practices regarding CAI management. Our findings highlighted the strong relationship between knowledge and preventive practices, suggesting that targeted educational interventions could effectively enhance patient outcomes. Future clinical practice should focus on implementing structured patient education programs, particularly emphasizing proper use of preventive measures, early recognition of complications, and the importance of rehabilitation adherence. Multi-center studies with longitudinal follow-up are needed to evaluate the long-term impact of such educational interventions on CAI outcomes. Further studies are also warranted to confirm the generalizability of these findings in non-urban patients.
Abbreviations
KAP, knowledge, attitudes, and practices; CAI, chronic ankle instability; LAS, lateral ankle sprains.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval and Informed Consent Statements
The study was approved by the Ethics Committee of Shanghai Ruijin Hospital, School of Medicine, Shanghai Jiaotong University (Ethics Approval No: (2024) Lin Lun Shen No. 162), and informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations and complied with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Herzog MM, Kerr ZY, Marshall SW, Wikstrom EA. Epidemiology of ankle sprains and chronic ankle instability. J Athl Train. 2019;54(6):603–10. doi:10.4085/1062-6050-447-17
2. Gribble PA, Bleakley CM, Caulfield BM, et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016;50(24):1496–1505. doi:10.1136/bjsports-2016-096189
3. Valderrabano V, Hintermann B, Horisberger M, Fung TS. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34(4):612–620. doi:10.1177/0363546505281813
4. Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123–140. doi:10.1007/s40279-013-0102-5
5. Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. 2017;51(2):113–125. doi:10.1136/bjsports-2016-096178
6. Attenborough AS, Hiller CE, Smith RM, Stuelcken M, Greene A, Sinclair PJ. Chronic ankle instability in sporting populations. Sports Med. 2014;44(11):1545–1556. doi:10.1007/s40279-014-0218-2
7. Roos KG, Kerr ZY, Mauntel TC, Djoko A, Dompier TP, Wikstrom EA. The epidemiology of lateral ligament complex ankle sprains in national collegiate athletic association sports. Am J Sports Med. 2017;45(1):201–209. doi:10.1177/0363546516660980
8. Delahunt E, Coughlan GF, Caulfield B, Nightingale EJ, Lin CW, Hiller CE. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc. 2010;42(11):2106–2121. doi:10.1249/MSS.0b013e3181de7a8a
9. Gribble PA, Delahunt E, Bleakley C, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. J Orthop Sports Phys Ther. 2013;43(8):585–591. doi:10.2519/jospt.2013.0303
10. Zheng -J-J, Shen L-Y, Duan L-R, et al. Investigatation of rehabilitation human resources in Shanghai, China. Chin J Rehab Theor Pract. 2020;1471–1476.
11. Verhagen EA, van Mechelen W, de Vente W. The effect of preventive measures on the incidence of ankle sprains. Clin J Sport Med. 2000;10(4):291–296. doi:10.1097/00042752-200010000-00012
12. Hubbard-Turner T. Lack of medical treatment from a medical professional after an ankle sprain. J Athl Train. 2019;54(6):671–675. doi:10.4085/1062-6050-428-17
13. Almohammed OA, Aldwihi LA, Alragas AM, Almoteer AI, Gopalakrishnan S, Alqahtani NM. Knowledge, attitude, and practices associated with COVID-19 among healthcare workers in hospitals: a cross-sectional study in Saudi Arabia. Front Public Health. 2021;9:643053. doi:10.3389/fpubh.2021.643053
14. Corbett RO, Harris PC, Vela L, Saliba SA, Hertel J. Athletic trainers’ perceptions of treating and managing patients with ankle sprains. J Athl Train. 2021;56(9):967–972. doi:10.4085/325-20
15. BF AL, Thirunavukkarasu A, Alsaidan AA, et al. Knowledge, attitude, and practice towards evidence-based medicine among northern saudi primary care physicians: a cross-sectional study. Healthcare. 2022;10(11). doi:10.3390/healthcare10112285
16. Elbahri HMH, Abd-Elmaged HMA, Abdulkarim M. Osteosarcoma of the distal fibula and reconstruction of the ankle using inverted fibula, a case report. Int J Surg Case Rep. 2022;96:107310. doi:10.1016/j.ijscr.2022.107310
17. Khan B, Ikram M, Rehman SSU, Un Nisa Z. Urdu translation and cross-cultural validation of Cumberland Ankle Instability Tool (CAIT). BMC Musculoskelet Disord. 2022;23(1):443. doi:10.1186/s12891-022-05408-4
18. Lu J, Liu L, Wang Y, Zhou Z. Social engagement and urban-rural disparity in self-management behaviors: study of middle-aged and older chinese hypertension patients. Front Public Health. 2021;9:801307. doi:10.3389/fpubh.2021.801307
19. Oster C, Schoo A, Litt J, et al. Supporting workforce practice change: protocol for a pilot study of a motivational interviewing virtual client software tool for health professionals. BMJ Open. 2020;10(2):e033080. doi:10.1136/bmjopen-2019-033080
20. Ruiz-Sánchez FJ, Ruiz-Muñoz M, Martín-Martín J, et al. Management and treatment of ankle sprain according to clinical practice guidelines: a PRISMA systematic review. Medicine. 2022;101(42):e31087. doi:10.1097/md.0000000000031087
21. Wagemans J, Bleakley C, Taeymans J, et al. Exercise-based rehabilitation reduces reinjury following acute lateral ankle sprain: a systematic review update with meta-analysis. PLoS One. 2022;17(2):e0262023. doi:10.1371/journal.pone.0262023
22. Dai W, Leng X, Wang J, Hu X, Ao Y. Rehabilitation regimen for non-surgical treatment of Achilles tendon rupture: a systematic review and meta-analysis of randomised controlled trials. J Sci Med Sport. 2021;24(6):536–543. doi:10.1016/j.jsams.2020.12.005
23. Marvulli R, Ianieri G, Pignatelli G, Santagati D, Ranieri M, Megna M. Electronic method (Pro-Kin) for improving and speeding up the recovery after ankle sprain. Endocr Metab Immune Disord Drug Targets. 2024;24(13):1572–1580. doi:10.2174/1871530322666220523155452
24. Corte-Real N, Caetano J. Ankle and syndesmosis instability: consensus and controversies. EFORT Open Rev. 2021;6(6):420–431. doi:10.1302/2058-5241.6.210017
25. Gogate N, Satpute K, Hall T. The effectiveness of mobilization with movement on pain, balance and function following acute and sub acute inversion ankle sprain - A randomized, placebo controlled trial. Phys Ther Sport. 2021;48:91–100. doi:10.1016/j.ptsp.2020.12.016
26. Ziaei Ziabari E, Haghpanahi M, Razi M, Lubberts B, Ashkani-Esfahani S, DiGiovanni CW. The effects of chronic ankle instability on the biomechanics of the uninjured, contralateral ankle during gait. Orthop Surg. 2022;14(9):2238–2244. doi:10.1111/os.13307
27. Halabchi F, Hassabi M. Acute ankle sprain in athletes: clinical aspects and algorithmic approach. World J Orthop. 2020;11(12):534–558. doi:10.5312/wjo.v11.i12.534
28. Sarcon AK, Heyrani N, Giza E, Kreulen C. Lateral ankle sprain and chronic ankle instability. Foot Ankle Orthop. 2019;4(2):2473011419846938. doi:10.1177/2473011419846938
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Utility of SpeedCourt System: A Novel Study of 100 Professional Footballers at FIFA Medical Centre of Excellence Dubai UAE
Ghrairi M, Dalal S, Esteban-García E, Chomier P, Valle X, Pruna R
Open Access Journal of Sports Medicine 2023, 14:79-87
Published Date: 31 October 2023
The Handgrip Endurance Task as a Simple Clinical Indicator of Mental Fatigue in Patients with Chronic Low Back Pain
Grousset M, Audiffren M, Meklat H, André N
Journal of Pain Research 2026, 19:602280
Published Date: 9 July 2026