Back to Journals » Nature and Science of Sleep » Volume 17

The Associations Between Depression, Subjective Sleep Quality, and Health-Related Quality of Life in Patients with Meige Syndrome: A Cross-Sectional Study
Authors Li M ![]() , Li J, Li M, Li J, Yu Y, Yang K, Zhou L, Li S, Li Y, Li Q, Wei J
, Li J, Li M, Li J, Yu Y, Yang K, Zhou L, Li S, Li Y, Li Q, Wei J ![]() , Li H
, Li H
Received 20 August 2025
Accepted for publication 21 November 2025
Published 27 November 2025 Volume 2025:17 Pages 3053—3063
DOI https://doi.org/10.2147/NSS.S558119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Meng Li,1,* Jianhua Li,2,* Mengtian Li,1,3,* Jiaxin Li,4 Yuandong Yu,5 Kezhen Yang,1 Linghan Zhou,1 Shen Li,6 Yanhong Li,1 Qiong Li,7 Junfan Wei,2 Huawei Li1
1Nursing Department, The Third People’s Hospital of Henan Province, Zhengzhou, People’s Republic of China; 2Nursing Department, Nanjing Central Hospital, Nanjing, People’s Republic of China; 3School of Nursing, Xinxiang Medical University, Xinxiang, People’s Republic of China; 4School of Medicine, Xi’an International University, Xi’an, People’s Republic of China; 5Health Management Center, The Third People’s Hospital of Henan Province, Zhengzhou, People’s Republic of China; 6School of Rehabilitation Therapy, Henan Vocational College of Tuina, Luoyang, People’s Republic of China; 7School of Nursing, North Hennan Medical University, Xinxiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huawei Li, Nursing Department, The Third People’s Hospital of Henan Province, 198 Funiu Road, Zhengzhou, Henan, People’s Republic of China, Tel +86 13937182631, Email [email protected] Junfan Wei, Nursing Department, Nanjing Central Hospital, No. 116, Chengxian Street, Xuanwu District, Nanjing, Jiangsu, People’s Republic of China, Tel +86 13253369959, Email [email protected]
Objective: This study aimed to assess the health-related quality of life (HRQoL) in patients with Meige syndrome and to explore the associations among socio-demographic factors, depression, sleep quality, and HRQoL.
Methods: A cross-sectional study was conducted using a convenience sampling method. Data were collected between March and June 2025 from six tertiary hospitals located in Henan Province and Guangdong Province. A total of 376 valid questionnaires were collected. Four instruments were used, including the socio-demographic characteristics questionnaire, the Self-Rating Depression Scale, the Pittsburgh sleep quality index, and the Short-From 36 Health Survey.
Results: The current study reported a mean SF-36 score of 49.6 ± 13.2 among patients with Meige syndrome, indicating moderate HRQoL impairment. The present study identified a negative correlation between HRQoL score with depression score and sleep quality score. Multiple linear regression showed that disease duration (β = 0.17, P < 0.001), self-care ability (β = − 0.13, P = 0.013), depression (β = − 0.14, P = 0.006) and sleep quality (β = − 0.12, P = 0.021) were significant factors associated with HRQoL in Meige syndrome patients.
Conclusion: Patients with Meige syndrome exhibited moderate impairment in HRQoL. Depression and poor sleep quality were significantly associated with lower HRQoL.
Keywords: Meige syndrome, health-related quality of life, cross-sectional study, depression, sleep quality
Introduction
Meige syndrome is a segmental cranial dystonia and one of the most common types of facial movement disorders in adults. It is characterized by involuntary muscle contractions involving the eyelids (blepharospasm) and the lower facial region (orofacial dystonia).1 These motor manifestations often lead to abnormal facial expressions, difficulty opening the eyes, speech disorders, and masticatory dysfunction, resulting in physical disability and functional impairment.2 While the disorder has traditionally been defined by its motor features, recent evidence suggests that non-motor symptoms—such as depression and sleep disturbances—may play a critical role in shaping patients’ overall well-being.3–5
In particular, depression is recognized as one of the most frequent psychological disturbances prevalent among patients with dystonias.6 Depression is defined as a mood disorder characterized by persistent sadness, loss of interest, and reduced energy, often accompanied by cognitive and somatic symptoms. In dystonia populations, including Meige syndrome, depression prevalence rates have been reported as high as 30–40%, significantly exceeding those in the general population.7 Depression not only worsens psychological well-being but has been consistently associated with impaired health-related quality of life (HRQoL), a comprehensive measure of physical, psychological, and social health status.
Similarly, poor sleep quality, insomnia, and fatigue are commonly reported in patients with dystonia and have been shown to compound emotional distress and impair daily activities.8–10 Prior studies suggest that depression and sleep problems often co-occur, further deteriorating HRQoL in this patient group.10
The concept of HRQoL provides a comprehensive framework for evaluating the overall well-being of individuals affected by disease. HRQoL is a multidimensional construct encompassing physical, psychological, and social domains of health, as perceived by the patient. It reflects not merely the absence of disease, but also the individual’s ability to perform daily activities, maintain social relationships, and experience emotional well-being.5
Although the detrimental effects of motor and non-motor symptoms on HRQoL have been recognized in various neurological disorders, the complex relationships between depression, sleep quality, and HRQoL in Meige syndrome remain poorly understood. Moreover, existing studies have primarily focused on heterogeneous dystonia populations, limiting the generalizability of findings to this specific disorder.
In our previous study, we focused on the relationships between positive coping style, psychological resilience, and illness stigma in patients with Meige syndrome.11 However, during the course of that research, we also observed that many participants exhibited persistent negative emotions and poor sleep quality—factors that appeared to be closely linked to their overall well-being. Building upon these observations, the present study shifts focus toward HRQoL as a core outcome and systematically explores its associations with depression, sleep quality, and functional status. This extension allows for a more comprehensive understanding of both psychological and physical contributors to patient outcomes, thereby enhancing the clinical relevance of our findings.
Therefore, the present study aimed to investigate the HRQoL of patients with Meige syndrome and to explore the relationship between socio-demographic factors, depression, sleep quality and HRQoL.
Methods
Study Design
This study was conducted with a convenience sampling cross-sectional design. The report complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure methodological transparency and integrity.
Participants
Sample size determination was based on Kendall’s recommendations for cross-sectional studies, using 5 to 10 participants per independent variable.12 This study included 27 variables from four instruments: a sociodemographic questionnaire (8 items), the Self-Rating Depression Scale (4 dimensions), the Pittsburgh Sleep Quality Index (7 dimensions), and the SF-36 Health Survey (8 dimensions). Considering an anticipated 20% non-response rate, we estimated the required sample size to be 169 to 338 participants.
Eligible participants are adults (≥18 years old) with a clinical diagnosis of Meige syndrome. Individuals with primary psychiatric disorders (such as schizophrenia or major depressive disorder with suicidal ideation), cognitive or hearing impairments or insufficient Mandarin proficiency to independently complete study questionnaires are excluded.
Instruments
Socio-Demographic Characteristics Questionnaire
Based on a preliminary study and review, a socio-demographic questionnaire was designed to collect participants’ general information, including gender, age, education level, marriage status, average monthly family income, disease duration, co-morbidity and self-care ability.
The Self-Rating Depression Scale (SDS)
Depression was assessed using the Self-Rating Depression Scale (SDS), a 20-item measure developed by Zung13 in 1965 at the Duke University School of Medicine. He originally designed the scale to provide a self-assessment of depressive symptoms suitable for both clinical screening and research. The scale assesses the participant’s depressive state through 20 items in four domains: affective disturbances, physiological equivalents, psychomotor activities, and psychological equivalents. The SDS consists of 20 questions, rated by the frequency of symptom occurrence, using a four-point Likert scale that categorizes answers from 1–4 into four levels: none or very little time, a little time, quite a lot of time, and the vast majority or all of the time. Questions 1, 3, 4, 7, 8, 9, 10, 13, 15, and 19 were forward scored, while the others were reverse scored. The scores of each of the 20 items were summed up to get the total raw score, and the standardized total score was obtained by taking the entire fraction of the total raw score * 1.25. The higher the total score, the more severe the depressive symptoms of the respondents. The SDS currently demonstrates high reliability and validity in different countries, languages and populations,14,15 and is recognized as suitable for screening and epidemiological studies of depression. The Chinese version of SDS was translated by Mingyuan Zhang et al,16 and has shown acceptable reliability and validity in several studies.17–19 In the present study, the Cronbach’s α was 0.868.
The Pittsburgh Sleep Quality Index (PSQI)
Subjective sleep quality was assessed using the self-reported PSQI, which captures patients’ perceived sleep experiences rather than objective sleep parameters. PSQI was developed by Daniel J. Buysse et al,20 a sleep specialist at the Center for Psychiatric Sleep and Biorhythm Studies at the University of Pittsburgh Medical Center, was used to measure the subjects’ sleep during the last month. The PSQI consists of 24 items including 19 self-assessed and 5 other-assessed items, with the 19th self-assessed and 5 other-assessed items not participating in the scoring process. 18 scores were converted and used to calculate the sleep status score on seven dimensions, including subjective sleep quality (item 6), time to fall asleep (item 2, item 5a), sleep duration (item 4), habitual sleep efficiency (item 1, item 3, item 4), sleep disturbances (items 5b - 5i), use of sleeping pills (item 7), and daytime dysfunction (items 8, 9). A four-point Likert scale was used for each item. A score of “0” means no difficulty, and a score of “3” means great difficulty. All the scores of the dimensions were added together to form the total score of the scale from 0 to 21. The higher the total score, the worse the quality of sleep. In this study, a Cronbach’s α coefficient of 0.906 was calculated for the 14 items by removing the four items of usual time to bed, time to wake up, length of sleep, and actual length of sleep.
The Short-Form 36 Health Survey (SF-36)
The SF-36 questionnaire is a widely used instrument for assessing HRQoL. It was originally developed by John E. Ware Jr. and his team in the Medical Outcomes Study (MOS) in the U.S.21 The SF-36 consists of 8 dimensions including physical functioning, physical role functioning, somatic pain, general health, vitality, social functioning, emotional role functioning, and mental health. The scores for each dimension subscale were calculated according to the scoring manual and then standardized using the formula to obtain a standard score of 0 ~ 100. SF-36 scores (derived by averaging the standardized scores for each subscale) were used as an indicator of quality of life in this study. Higher SF-36 scores indicated a better quality of life for the respondents. The Chinese version of SF-36 was translated by Lu Li et al22 and widely used in several studies.23,24 The Cronbach’s α coefficients for each of the 8 subscales ranged from approximately 0.70 to 0.94, indicating good internal consistency.25
Data Collection
A cross-sectional study was implemented using a convenience sampling approach. Data were collected between March and June 2025 from six tertiary hospitals located in Henan Province and Guangdong Province. Prior to data collection, all investigators were trained in standardized procedures. Eligible patients were recruited from six tertiary hospitals with the assistance of department nurses. Data were collected anonymously via an online questionnaire system between March and June 2025.
Prior to conducting the survey, the research team members introduced the purpose of this study to the participants, explained that the questionnaire content of this study did not involve the privacy of the respondents, guaranteed anonymity, and stated the principle that participants could withdraw at any time for any reason to ensure that each participant had been listened to and understood. The link to the online questionnaire was pre-entered into the Questionnaire Star system (http://www.wjx.cn) and pre-tested. The link was sent face-to-face to respondents who volunteered to participate in the study. Respondents accessed and completed the questionnaire through the link. Respondents were also asked not to send the link to the questionnaire to anyone else without their permission.
The questionnaire included four parts: the socio-demographic characteristics, SDS, PSQI, and SF-36. All responses remained anonymous, and no identifying details (eg, names or addresses) were recorded. To ensure the quality of the returned questionnaires, several measures were implemented.
At the beginning of the questionnaire, a brief description of its purpose and key precautions was provided. The first page contained an informed consent form, and an electronic signature box was placed at the end. Respondents were required to sign this box, either by drawing with a mouse on a computer or by using their finger on a mobile device. To prevent incomplete submissions, all questions were made mandatory. Any unanswered question would prevent the questionnaire from being successfully submitted, and these questions were clearly marked with an asterisk as a reminder for respondents to complete them. All questionnaire items were set as mandatory fields in the online system, which prevented submission of incomplete responses. As a result, no missing data were encountered, and no imputation or exclusion procedures were required. Only participants who met the specified inclusion and exclusion criteria were allowed to proceed with the survey. Furthermore, the questionnaire could only be completed and submitted once per IP address. Ethical approval for the study was granted by the Institutional Review Board, and participants were assured that their responses would remain confidential and anonymous. The collected data were securely stored and accessible only to the research team. See Figure 1 for a flowchart of the participants screening process.
 |
Figure 1 Flowchart of the participant screening and inclusion process. |
Data Analysis
Data were analyzed using SPSS Statistics version 27.0 (IBM Corporation, Armonk, NY, USA). For continuous variables, those with a normal distribution were expressed as mean (standard deviation), while those with skewed distribution were presented as median (interquartile range). Categorical data were reported as percentages. To examine the variations in HRQoL among patients with Meige syndrome across different gender, education level, marriage status, average monthly family income, disease duration, co-morbidity and self-care ability, independent samples t-tests and one-way analysis of variance (ANOVA) were conducted. To examine the association between age and HRQoL, Pearson correlation analysis was conducted. In addition, Pearson correlation analysis was performed to assess the relationships between SDS scores, PSQI scores, and SF-36 scores. Multi-collinearity was evaluated by calculating tolerance and the variance inflation factor (VIF), with the absence of multi-collinearity confirmed when tolerance exceeded 0.1 and VIF remained below 10. Variables that demonstrated statistical significance in the t-test, ANOVA, and Pearson correlation analyses were identified as potential predictors and included in the subsequent regression analysis. Finally, multiple linear regression was conducted, with potential predictors as independent variables and HRQoL as the dependent variable, to further examine the relationship between socio-demographic characteristics, depression, and sleep quality in patients with Meige syndrome. A two-tailed P-value of less than 0.05 was considered statistically significant. No adjustments for multiple comparisons were applied, as the analyses were hypothesis-driven and focused on a predefined set of key variables.
Results
Socio-Demographic Characteristics of Participants and Comparison of Different Variables on HRQoL in Meige Syndrome Patients
We initially invited 600 patients with Meige syndrome who met the inclusion and exclusion criteria to participate in this study, and finally 376 valid questionnaires were collected, which means that the valid response rate was 62.7% in this study. Of these 376 participants, the proportion of females was slightly higher than that of males, with 207 females, accounting for 55.1% of the total. The minimum age of the participants was 29 years and the maximum was 79 years with a mean age of 60.3 ± 7.7. As for the level of education, the largest number of patients among the participants were those with primary school education, 108 (28.7%), and followed by those who held a high school education, 95 (25.3%). The majority of participants were married, with 334 participants, accounting for 88.8% of the total participants. Nearly half of the participants, 155 (41.2%), had a average monthly per person family income of 1000–3000 yuan (in CNY). Only 15 (4.0%) participants had been sick for less than 12 months, 181 (48.1%) had been sick for 12–24 months, and 180 (47.9%) had been sick for more than 24 months. About half of the participants (177, 47.1%) also suffered from other diseases. The majority of participants (157 or 41.8%) were partially dependent on self-care ability. T-tests, Pearson analysis and ANOVA revealed that HRQoL in Meige syndrome patients showed statistically significant differences on marriage status, disease duration, comorbidity with other diseases and self-care ability (P < 0.05). Specifically, married patients had the highest HRQoL scores while unmarried patients had the lowest. In terms of disease duration, patients with a disease duration of more than 24 months had the highest HRQoL scores while those with a disease duration of less than 12 months had the lowest HRQoL scores. For co-morbidities, the HRQoL scores of patients who did not have other co-morbidities were higher than the HRQoL scores of patients who had other co-morbidities. For self-care ability, fully independent patients had the highest HRQoL scores while fully dependent patients had the lowest HRQoL scores. See Table 1 for details.
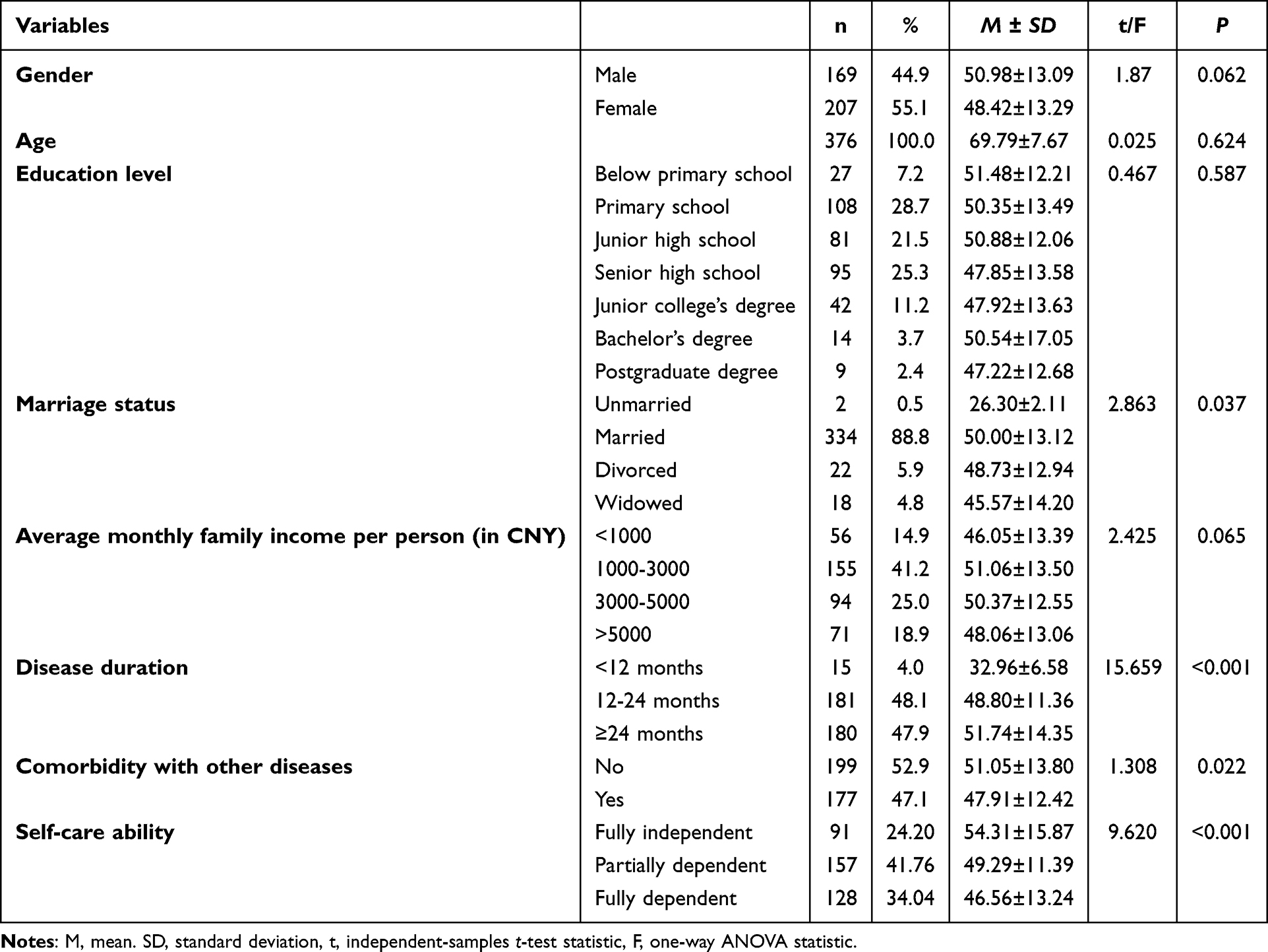 |
Table 1 Socio-Demographic Characteristics and Comparison of Participants Different Variables Regarding HRQoL in Meige Syndrome (N = 376) |
Correlation Analysis of Depression, Sleep Quality, and HRQoL
In this study, HRQoL score was found to be correlated with depression score and sleep quality score. Specifically, the HRQoL score showed a negative correlation with depression score (r = −0.185, P < 0.001), indicating that patients with higher HRQoL scores tend to show lower depression scores. Similarly, the HRQoL score was significantly negatively correlated with sleep quality score (r = −0.175, P < 0.001), suggesting that patients with higher HRQoL scores tend to present better sleep quality. In addition, depression score was positively correlated with sleep quality (r = 0.131, P < 0.05), indicating that individuals with higher levels of depression have poorer sleep quality. See Table 2 for details. See Figure 2 for the correlation heatmap.
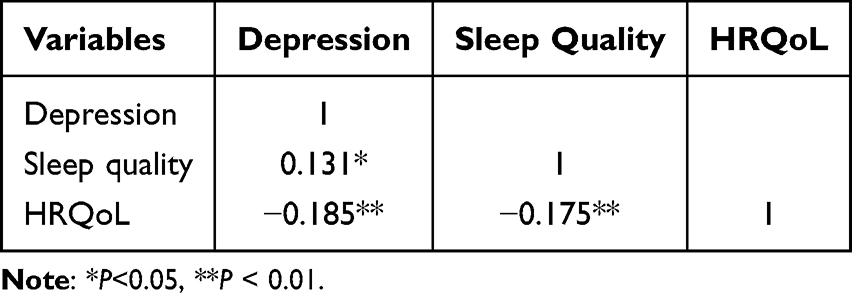 |
Table 2 Pearson Correlation of Depression, Sleep Quality and HRQoL in Patients with Meige Syndrome |
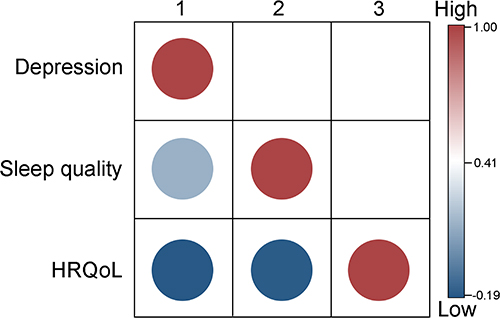 |
Figure 2 Heatmap illustrating the correlations among depression, sleep quality, and HRQoL in patients with Meige syndrome. Abbreviation: HRQoL, Health-related Quality of Life. |
Multiple Linear Regression Analysis of Factors Associated with HRQoL in Meige Syndrome Patients
Multi-collinearity among the independent variables was assessed to verify the basic assumptions of the regression model. Given that the VIF less than 10 and the tolerance was 0.1 or above, no significant multi-collinearity issues were identified. Based on univariate analysis of t-test, ANOVA and Pearson analysis, variables with statistical significance (P < 0.05) were selected as independent variables, with HRQoL as the dependent variable for multiple linear regression analysis. As shown in Table 3, the model explained a significant proportion of the variance in HRQoL among Meige syndrome patients. The results indicated that disease duration (β = 0.17, P < 0.001), self-care ability (β = −0.13, P = 0.013), depression (β = −0.14, P = 0.006), and sleep quality (β = −0.12, P = 0.021) were significant factors associated with HRQoL in Meige syndrome patients.
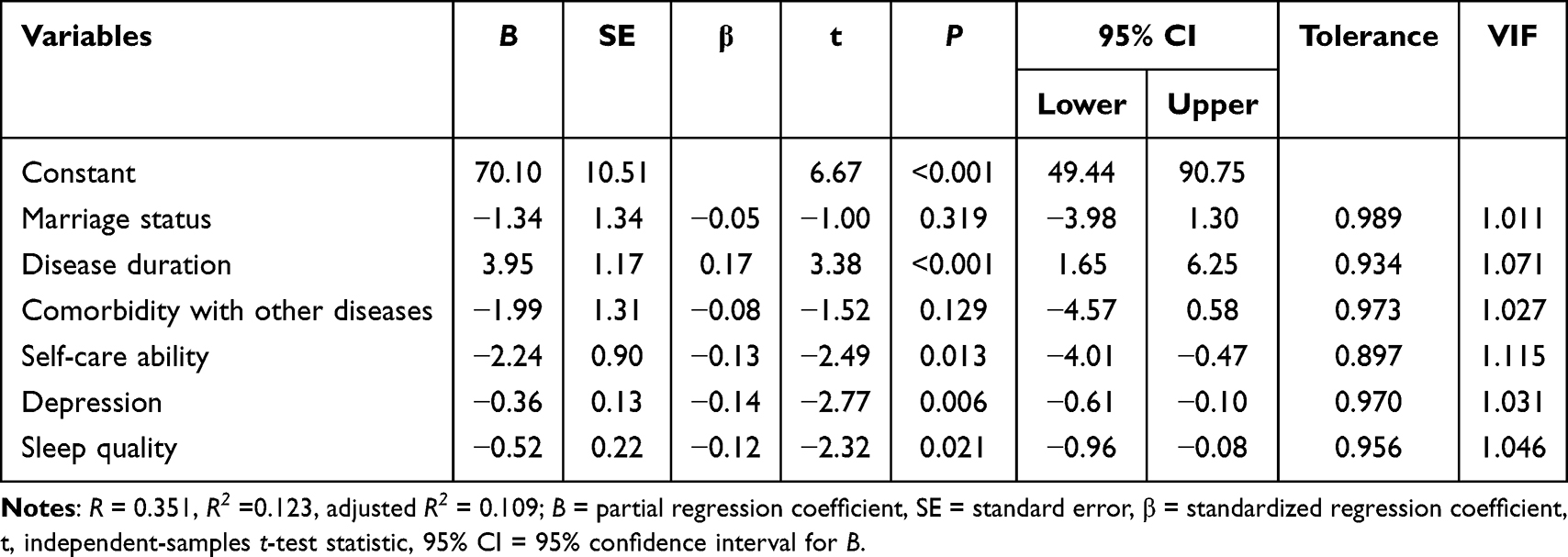 |
Table 3 Multiple Linear Regression Analysis for Factors Associated with HRQoL in Patients with Meige Syndrome |
Discussion
The aim of this study was to investigate the HRQoL of patients with Meige syndrome. This group has been noted relatively little in the existing literature. By simultaneously examining patients’ sociodemographic characteristics, depression, and sleep quality, this study provides a more comprehensive understanding of the factors associated with HRQoL in patients with a rare movement disorder, Meige syndrome. Unlike previous studies that have tended to focus exclusively on motor symptoms, our findings expand the existing knowledge base within the field of neuromotor disorders by emphasizing the multidimensional factors that influence HRQoL and highlighting the crucial role of psychosocial variables.
In the present study, there were more female patients with Meige syndrome than male patients, which is consistent with previous clinical studies on Meige syndrome that showed a higher percentage of female patients.26,27 This discrepancy may be attributed to regional differences in health-seeking behavior, sampling strategies, or diagnostic criteria variations. Additionally, the possibility of selection bias and statistical variability should not be overlooked, especially given the modest sample size.
Patients with Meige syndrome in this study had a relatively advanced mean age compared with previous reports.28,29 Such differences may stem from variations in sampling methods, referral patterns, diagnostic delays, or population characteristics across studies. Therefore, the age profile of our cohort should be interpreted cautiously and viewed as contextual information rather than a central finding.
The current study reported a mean SF-36 score of 49.6 ± 13.2 among patients with Meige syndrome, indicating moderate HRQoL impairment. This result is comparable to prior findings in Meige patients30 and similar to scores reported in cervical dystonia and moderate-stage Parkinson’s disease, where total SF-36 scores often range between 40 and 50.31 In contrast, patients with essential tremor typically report higher SF-36 scores (55–60),32 reflecting milder disability and better preserved functioning. These comparisons suggest that Meige syndrome imposes a substantial HRQoL burden, on par with other disabling movement disorders.
Interestingly, although previous studies on dystonia have observed an association between longer disease duration and higher HRQoL scores, this relationship should be interpreted with caution. This is because the observed pattern may be partially influenced by unmeasured confounding factors such as coping strategies, treatment history, symptom severity, or selection bias and survival bias associated with recruiting patients from tertiary hospitals.30 This seemingly paradoxical trend may reflect adaptive psychological mechanisms such as acceptance and emotional adjustment, which have been described in chronic movement disorders.32 Over time, patients may develop coping strategies and modify daily routines to accommodate symptoms, which may be associated with better-perceived well-being.33 Furthermore, individuals with longer disease duration are more likely to have engaged with multiple treatment modalities, including botulinum toxin therapy or behavioral interventions, which may be associated with better outcomes in both physical and mental health domains.31 Although similar findings have been reported in previous dystonia studies, suggesting that long-term patients may experience psychological adaptation or benefit from accumulated treatment exposure, this interpretation should still be viewed with caution.
The self-care ability is another important associated factor; specifically, patients with stronger self-care abilities exhibited higher HRQoL scores. This relationship has been observed across various movement disorders, where greater independence in daily activities contributes to better perceptions of health and emotional stability.34 Similarly, Drexel et al found that even among dystonia patients receiving optimized botulinum toxin therapy, those with preserved self-care function reported better physical and mental HRQoL outcomes.35 Moreover, the dimension of self-care in HRQoL assessment tools such as the EQ-5D-5L has shown high discriminatory value in dystonia populations, underlining its critical role in perceived well-being.36 Furthermore, there was a empirical study showed that improvements in self-care often co-occur with functional gains from therapeutic interventions like deep brain stimulation (DBS), which not only reduce motor disability but also restore autonomy in activities of daily living.37 As such, greater self-care capacity is associated with better HRQoL, highlighting the relevance of rehabilitation, assistive devices, and caregiver support in the overall management of patients with Meige syndrome.
Depression plays a significant role in HRQoL among Meige syndrome patients. In a study conducted at AIIMS, India, 50% of patients with Meige syndrome exhibited signs of depression, with 21.4% experiencing moderate levels, which strongly correlated with lower SF-36 scores across emotional and social domains.30 Similarly, Zheng et al31 demonstrated that botulinum toxin type A significantly reduced depression and anxiety levels in Meige patients, and the improvements in mental health were closely associated with enhancements in HRQoL, independent of motor symptom relief. Furthermore, a study by Xie et al38 examining the effects of subthalamic deep brain stimulation on Meige syndrome reported that reductions in depression and anxiety were associated with higher HRQoL scores, indicating that neuropsychiatric symptoms are closely linked to patients’ overall quality of life. These findings underscore that beyond motor dysfunction, psychological burden—particularly depression—constitutes a critical determinant of HRQoL in this patient population.
Furthermore, the present study found that sleep quality is also an important factor associated with the HRQoL of patients with Meige syndrome. This is consistent with the findings of Liu et al,39 who reported significant improvements in both sleep quality and HRQoL 12 months after deep brain stimulation in Meige syndrome patients, suggesting a tight interplay between restorative sleep and overall well-being. Sleep disturbances such as insomnia and fragmented sleep are common in dystonia and have been associated with increased mood symptoms and fatigue, which may in turn relate to greater difficulty in daily functioning.40,41
Although multiple variables including disease duration, self-care ability, depression status, and sleep quality were statistically significant predictors of HRQoL, the overall explanatory power of the regression model remained relatively low (R2 ≈ 0.12). This indicates that the included predictors accounted for only a small fraction of the variance in HRQoL. The modest effect sizes of these factors further suggest that HRQoL in patients with Meige Syndrome may be influenced by a broader range of factors, such as social support, coping strategies, treatment history, access to healthcare services, and other psychological factors not examined in this study. Future research could incorporate additional biopsychosocial variables and adopt more comprehensive modeling frameworks to better elucidate the complexity of HRQoL in this patient population.
Several limitations should be considered when interpreting these findings. First, although data were collected from multiple centers, a convenience sampling strategy was used and not all geographic regions were represented, which may introduce selection bias. The exclusion of patients with major psychiatric comorbidities may also have led to an underestimation of the true burden of depression, thereby limiting the generalizability of the results to the broader Meige syndrome population. Second, the cross-sectional design restricts our ability to determine the directionality or causality of the associations observed between clinical and psychosocial variables and HRQoL. Third, the study focused primarily on patient-level characteristics such as mood and functional status, whereas potentially influential external factors—including family support, treatment accessibility, and economic circumstances—were not systematically evaluated. In addition, several subgroup categories contained very few participants (eg, only two unmarried individuals), which reduces statistical stability and may exaggerate observed group differences. Therefore, subgroup findings should be interpreted with caution. Additionally, sleep quality was measured using a subjective self-report scale, which may not fully capture objective sleep disturbances and could introduce reporting bias. Future studies should employ multi-site, longitudinal designs and incorporate broader contextual and clinical variables to provide a more comprehensive understanding of the determinants of HRQoL in this population.
Conclusion
The findings of this study suggest that Meige syndrome places a greater burden on patients’ HRQoL. Longer illness duration, greater self-care ability, better subjective sleep quality, and fewer depressive symptoms were observed to be associated with higher HRQoL, indicating that mental health and functional functioning are closely related to patients’ perceived quality of life. These findings highlight the need for comprehensive, multidisciplinary interventions, and given that health-related quality of life encompasses multiple aspects of physical functioning, emotional well-being, self-care competence, sleep quality, and depression, the concerted efforts of neurologists, rehabilitation physicians, nurses, psychologists, occupational therapists, and physical therapists are critical. In addition, the observed association between longer disease duration and higher HRQoL may be confounded by unmeasured factors—including treatment exposure, pain or motor severity, coping adaptations, and selection/survivorship bias arising from convenience sampling in tertiary centers. In addition, improving patients’ mental resilience and functional autonomy may also significantly enhance overall health and daily functioning. A targeted, holistic approach to care should be prioritized in the long-term disease management of Meige syndrome in order to improve the health-related quality of life and health status of patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Third People’s Hospital of Henan Province in Zhengzhou, China (Ethical Review NO.: 2025SZSYLCYJ0302), based on the principles of the Declaration of Helsinki. Informed consent was obtained in written electronic form from all participants prior to enrolment via an electronic signature within the online questionnaire system. All eligible participants were informed of the study and its ethical principles (eg, voluntary participation, withdrawal, anonymity, and confidentiality).
Author Contributions
M.L.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review and editing.
J.L.: Conceptualization, Formal analysis, Investigation, Visualization, Validation, Writing – original draft, Writing – review and editing.
M.L.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
J.L.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
Y.Y.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
K.Y.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
L.Z.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
S.L.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
Y.L.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
Q.L.: Formal analysis, Investigation, Validation, Writing – original draft, Writing – review and editing.
J.W.: Conceptualization, Methodology, Formal analysis, Validation, Writing – original draft, Writing – review and editing.
H.L.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft.
All authors agreed on the journal to which the article will be submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, agrees to take responsibility and be accountable for the contents of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Defazio G, Abbruzzese G, Livrea P, Berardelli A. Epidemiology of primary dystonia. Lancet Neurol. 2004;3(11):673–678. doi:10.1016/S1474-4422(04)00907-X
2. Klein C, Ozelius LJ. Dystonia: clinical features, genetics, and treatment. Curr Opin Neurol. 2002;15(4):491–497. doi:10.1097/00019052-200208000-00014
3. Peall KJ, Waite AJ, Blake DJ, Owen MJ, Morris HR. Psychiatric disorders, myoclonus dystonia, and the epsilon-sarcoglycan gene: a systematic review. Mov Disord. 2011;26(10):1939–1942. doi:10.1002/mds.23791
4. Peall KJ, Berman BD, Bruggemann N, et al. Non-motor symptoms in dystonia: from diagnosis to treatment. Dystonia. 2023;2:11860.
5. Nutt JG, Siderowf AD, Guttman M, et al. Mobility, mood and site of care impact health related quality of life in Parkinson’s disease. Parkinsonism Relat Disord. 2014;20(3):274–279. doi:10.1016/j.parkreldis.2013.10.004
6. Ray S, Kutty B, Pal PK, Yadav R. Sleep and other non-motor symptoms in patients with idiopathic oromandibular dystonia and Meige syndrome: a questionnaire-based study. Ann Indian Acad Neurol. 2021;24(3):351–355. doi:10.4103/aian.AIAN_906_20
7. Medina Escobar A, Pringsheim T, Goodarzi Z, Martino D. The prevalence of depression in adult onset idiopathic dystonia: systematic review and metaanalysis. Neurosci Biobehav Rev. 2021;125:221–230. doi:10.1016/j.neubiorev.2021.02.036
8. Ray S, Kumar G, Kutty B, Pal PK, Yadav R. Patients with primary cervical dystonia have significant sleep impairment and polysomnographic abnormalities. Sleep Vigilance. 2021;5(1):119–126. doi:10.1007/s41782-021-00144-6
9. Wagle Shukla A, Brown R, Heese K, et al. High rates of fatigue and sleep disturbances in dystonia. Int J Neurosci. 2016;126(10):928–935. doi:10.3109/00207454.2015.1085035
10. Paus S, Gross J, Moll-Müller M, et al. Impaired sleep quality and restless legs syndrome in idiopathic focal dystonia: a controlled study. J Neurol. 2011;258(10):1835–1840. doi:10.1007/s00415-011-6029-6
11. Li M, Li M, Zhang N, et al. The relationships between positive coping style, resilience, and illness stigma in patients with Meige syndrome: a cross-sectional study. Front Psychiatry. 2025;16:1646084. doi:10.3389/fpsyt.2025.1646084
12. Zhang W, Pan Z, Zhu Y, et al. Illness uncertainty, resilience, and perceived social support among patients with moyamoya disease: a cross-sectional study. Front Psychiatry. 2024;15:1405594. doi:10.3389/fpsyt.2024.1405594
13. ZUNG WWK. A Self-Rating Depression Scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
14. Mammadova F, Sultanov M, Hajiyeva A, Aichberger M, Heinz A. Translation and adaptation of the Zung self- rating depression scale for application in the bilingual Azerbaijani population. Eur Psychiatry. 2012;27 Suppl 2:S27–31. doi:10.1016/S0924-9338(12)75705-X
15. Aragonès Benaiges E, Masdèu Montalà RM, Cando Guasch G, Coll Borràs G. Diagnostic validity of Zung’s self-rating depression scale on primary care patients. Actas Esp Psiquiatr. 2001;29(5):310–316.
16. Yuan J, Chen J, Zhu Z, Zhang M, Jin H. A study of the validity of the flow call depression self-rating scale for use in the community. Shanghai Psychiatry. 1998;1998(03):150–151+153.
17. Lu J, Xu X, Huang Y, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2021;8(11):981–990. doi:10.1016/S2215-0366(21)00251-0
18. Hou L, Huang K, Gong C, et al. Long-term pegylated GH for children with GH deficiency: a large, prospective, real-world study. J Clin Endocrinol Metab. 2023;108(8):2078–2086. doi:10.1210/clinem/dgad039
19. Liao DD, Dong M, Ding KR, et al. Prevalence and patterns of major depressive disorder and subthreshold depressive symptoms in south China. J Affect Disord. 2023;329:131–140. doi:10.1016/j.jad.2023.02.069
20. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
21. Ware J, Snoww K, Kosinski MA, Gandek BG. SF-36. Health survey: manual and interpretation guide. Health Assessment Lab. 1993;1993:6.
22. Li L, Wang H, Shen Y. Development of the Chinese version of the SF-36 Health Survey Scale and its performance testing. Chin J Prevent Med. 2002;36(2):5.
23. Lin Y, Yu Y, Zeng J, Zhao X, Wan C. Comparing the reliability and validity of the SF-36 and SF-12 in measuring quality of life among adolescents in China: a large sample cross-sectional study. Health Qual Life Outcomes. 2020;18(1):360. doi:10.1186/s12955-020-01605-8
24. Mei J, Ju C, Wang B, et al. The efficacy and safety of Bazi Bushen Capsule in treating premature aging: a randomized, double blind, multicenter, placebo-controlled clinical trial. Phytomedicine. 2024;130:155742. doi:10.1016/j.phymed.2024.155742
25. Hu ZY, Hu XC, Zhu AA, et al. Application of SF-36 scale in the survey of quality of life of occupational disease patients. Chin J Labor Health Occup Dis. 2020;38(11):846–848.
26. Liu G, Xu T, Guo QY, et al. The efficacy and safety of nerve loop blocking in the treatment of blepharospasm in Meige syndrome. Zhonghua Yan Ke Za Zhi. 2023;59(1):31–36. doi:10.3760/cma.j.cn112142-20220726-00361
27. Poungvarin N, Devahastin V, Chaisevikul R, Prayoonwiwat N, Viriyavejakul A. Botulinum A toxin treatment for blepharospasm and Meige syndrome: report of 100 patients. J Med Assoc Thai. 1997;80(1):1–8.
28. Sharma AK, Behari M, Ahuja GK. Clinical and demographic features of Meige’s syndrome. J Assoc Physicians India. 1996;44(9):645–647.
29. Horisawa S, Ochiai T, Goto S, et al. Long-term outcome of pallidal stimulation for Meige syndrome. J Neurosurg. 2019;130(1):84–89. doi:10.3171/2017.7.JNS17323
30. Verma A, Singh PK, Agarwal S, Gupta B. Assessment of health related quality of life (HRQol) in patients with Meige’s syndrome. Int J Res Med Sci. 2018;6:1956. doi:10.18203/2320-6012.ijrms20181961
31. Zheng H, Wu L, Tian S, et al. Effect of botulinum toxin type A on non-motor symptoms and quality of life in Meige syndrome. Front Neurol. 2023;14:1115482. doi:10.3389/fneur.2023.1115482
32. Lorenz D, Schwieger D, Moises H, Deuschl G. Quality of life and personality in essential tremor patients. Mov Disord. 2006;21(8):1114–1118. doi:10.1002/mds.20884
33. Nguyen HV, Ngian V, Cordato D, Shen Q, Chan DK. Quality of life in a random sample of community dwelling older patients with essential tremor. Acta Neurol Scand. 2007;116(5):289–292. doi:10.1111/j.1600-0404.2007.00863.x
34. Băjenaru OL, Nuță CR, Băjenaru L, et al. Health-related quality of life in romanian patients with dystonia: an exploratory study. J Clin Med. 2024;13(12):3403. doi:10.3390/jcm13123403
35. Drexel SC, Klietz M, Kollewe K, et al. Caregiver burden and health-related quality of life in idiopathic dystonia patients under botulinum toxin treatment: a cross-sectional study. J Neural Transm. 2020;127(1):61–70. doi:10.1007/s00702-019-02109-6
36. Skogseid IM. Pallidal deep brain stimulation is effective, and improves quality of life in primary segmental and generalized dystonia. Acta Neurol Scand Suppl. 2008;188:51–55. doi:10.1111/j.1600-0404.2008.01032.x
37. Tsuboi T, Wong JK, Okun MS, Ramirez-Zamora A. Quality of life outcomes after deep brain stimulation in dystonia: a systematic review. Parkinsonism Relat Disord. 2020;70:82–93. doi:10.1016/j.parkreldis.2019.11.016
38. Xie H, Shan M, Wang S, et al. Deep brain stimulation of the subthalamic nucleus for primary Meige syndrome: clinical outcomes and predictive factors. J Neurosurg. 2024;140(6):1650–1663. doi:10.3171/2023.11.JNS232075
39. Liu J, Ding H, Xu K, et al. Pallidal versus subthalamic deep-brain stimulation for Meige syndrome: a retrospective study. Sci Rep. 2021;11(1):8742. doi:10.1038/s41598-021-88384-4
40. Smit M, Kamphuis ASJ, Bartels AL, et al. Fatigue, sleep disturbances, and their influence on quality of life in cervical dystonia patients. Mov Disord Clin Pract. 2017;4(4):517–523. doi:10.1002/mdc3.12459
41. Soeder A, Kluger BM, Okun MS, et al. Mood and energy determinants of quality of life in dystonia. J Neurol. 2009;256(6):996–1001. doi:10.1007/s00415-009-5060-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
The Correlation Between Night Shift Work Schedules, Sleep Quality, and Depression Symptoms
Alreshidi SM, Rayani AM
Neuropsychiatric Disease and Treatment 2023, 19:1565-1571
Published Date: 7 July 2023
Anxiety and Depression in People with Eczema or Psoriasis: A Comparison of Associations in UK Biobank and Linked Primary Care Data
Matthewman J, Mansfield KE, Hayes JF, Adesanya EI, Smith CH, Roberts A, Langan SM, Henderson AD
Clinical Epidemiology 2023, 15:891-899
Published Date: 7 August 2023