Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
The Correlation Between Night Shift Work Schedules, Sleep Quality, and Depression Symptoms
Authors Alreshidi SM ![]() , Rayani AM
, Rayani AM ![]()
Received 12 May 2023
Accepted for publication 4 July 2023
Published 7 July 2023 Volume 2023:19 Pages 1565—1571
DOI https://doi.org/10.2147/NDT.S421092
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Salman M Alreshidi, Ahmad M Rayani
Community and Psychiatric Mental Health Nursing Department, College of Nursing, King Saud University, Riyadh City, 12371, Saudi Arabia
Correspondence: Salman M Alreshidi, Tel +9660537737872, Email [email protected]
Purpose: Poor sleep and depressive symptoms are two negative effects of night shift work on physical and mental health. This study evaluated the correlation between sleep quality and depression symptoms among nurses in Saudi Arabia. Specifically, we assessed depressive symptoms and sleep quality observed among nurses who worked night shifts and compared the outcomes with those who worked exclusively day shifts in hospital settings.
Patients and Methods: A total of 191 participants (55.5% men, 44.5% women) participated. The response rate was 63.6%. The hospital anxiety and depression scale (HADS) and Pittsburgh Sleep Quality Index (PSQI) were used to assess depression score and sleep quality, respectively.
Results: Nurses who worked night shifts had substantially higher PSQI ratings (p< 0.05) than those who worked day shifts. In addition, there was a clear relationship between the HADS and PSQI scores. According to the binary logistic regression, longer working hours and inadequate sleep were both independently linked to depressive symptoms among nurses.
Conclusion: Poor sleep quality brought on by night shifts may explain why Saudi nurses who work night shifts experience higher rates of depression than those who work day shifts only.
Keywords: depression, sleep quality, nurse, night shift
Introduction
As a result of rising demand for high-quality treatment, greater public expectations, and increasing financial restrictions, nurses are more frequently exposed to acute and chronic occupational stressors—which puts them at risk for developing psychiatric illnesses, including depression and depressive symptoms.1 The rate at which the nurse population reports symptoms of depression is double that of the general population.2 In the Kingdom of Saudi Arabia (Saudi Arabia), a recent spate of violent assaults on medical personnel has drawn global attention.3 A survey of 738 Saudi nurses found that 11.1% and 32.9% experienced physical and nonphysical violent incidents, respectively.4 The risk of being assaulted puts Saudi nurses under significant psychological strain—the early detection of depression among Saudi nurses facilitates the prevention of negative effects on patients, caregivers, and healthcare organizations.5
Care is provided in hospitals around-the-clock, seven days a week, and nurses’ routines—including night shift work schedules—are largely unchangeable.6 Working a night shift can negatively affect social connections and work–life balance, leading to more emotional anguish,7 and is linked to a higher chance of developing depressive symptoms.8,9
Night shift working practices disrupt cortisol and melatonin cycles,10 which directly impact sleep quality.11 Insufficient sleep following working overnight is a prevalent concern for night shift workers.12 According to one study, nurses who worked night shifts had poorer quality sleep than their counterparts who worked day shifts,13 and the lack of sleep had an adverse effect on their health. Poor sleep quality is also associated with depressive symptoms. According to an epidemiological investigation, up to 90% of those with symptoms of depression had experienced sleep problems.14 Similarly, less sleep over six months is associated with more severe depression in individuals who have experienced a depressive episode.15
Although studies illustrate how poor sleep may play a role in the link between working nights and a disordered state of physical and mental health,16,17 no study has focused on the relevance of sleep quality in terms of the correlation between symptoms of depression and night shift working patterns among nurses. The researcher investigated to determine any correlation between night shifts, sleep quality, and depression symptoms among Saudi nurses, we hypothesized that poor sleep quality might contribute to the link between the two. The current study has two main goals: (1) to investigate the correlation between symptoms of depression and night shift working patterns among nurses, and (2) to understand the correlation between symptoms of depression and sleep quality among the nurse population.
Methods
Participants and Study Design
This cross-sectional study was conducted between March and April 2023 in Medical City in the Province of Riyadh (Central Saudi Arabia). A barcode consisting of the consent form, demographic items, and questionnaire was sent to nurses’ email addresses using Google Forms. A total of 300 nurses were asked to complete a self-administered questionnaire. All responses were anonymous. Nurses were asked to provide written consent to participate in the study and to answer self-administered anonymous surveys. Those who did not consent to participate were excluded from the study. One hundred ninety-one nurses completed the questionnaire (response rate: 63.6%). According to self-report, nurses working day shifts were those whose work shifts did not include night work, as defined by having a work schedule that only included day shift. Nurses who self-reported working night shifts were those whose schedules included night work, which was defined as working after midnight. The night shift spanned from 11:00 p.m. to 8:00 a.m., whereas the day shift spanned 8:00 a.m. to 11:00 p.m.
The Ethics Committee of Medical City approved this study. This study was conducted following the principles of the Declaration of Helsinki. After reading the investigation’s purpose statement, each participant signed an informed consent form.
Evaluation of Clinical Variables
Participants’ sociodemographic information and other clinically significant characteristics were gathered using a study questionnaire. The following tools were used to collect data on clinical variables.
Nurses’ sleep quality was assessed using the Arabic version of the Pittsburgh Sleep Quality Index (PSQI). The PSQI is a 19-item, psychometrically validated approach to measure sleep quality and disruption. The index has a score ranging from 0 to 21. A score cut off < 5 indicates good sleep quality, while a score cut off > 5 indicates poor sleep quality.18,19 In the present study, the seven component scores of the PSQI had an overall Cronbach’s alpha of 0.60.
The Arabic version of the Hospital Anxiety and Depression Scale (HADS) was used to measure depressive symptoms.20,21 The participants were asked to respond to each item on a questionnaire containing questions about how they felt over the past week using a 7-item Likert 4-point scale ranging from 0 (normal) to 3 (severe). Items 2, 4, 6, 8, 10, 12, and 14 relate to the depression subscale. With higher scores indicating higher symptom levels. Participants who received a score of >7 were deemed to have depressed symptoms. Cronbach’s alpha of the HADS Depression subscale in the present study was 0.65.
Statistical Analyses
ANOVA assessed continuous variables, whereas the chi-squared test was performed for categorical variables. Fisher’s exact test was also performed with categorical variables if the underlying assumptions of the chi-square test were unmet. The Pearson correlation coefficient (rp) assessed the bivariate relationship between HADS and PSQI measurements. Binary logistic regression analysis was used to determine the impact of working a night shift on sleep quality and depression symptoms. To limit the impact of potential confounders, we included factors with p<0.05 in the univariate analysis in the logistic regression analysis. Outcomes were represented as an adjusted OR (95% CI). IBM® SPSS® Statistics Version 28.0 (IBM Corp., Armonk NY [USA]) was used to perform the statistical analyses. Statistical significance was set at 0.05. significant.
Results
Among the nurses surveyed, 73.3% (140 out of 191) were revealed to be suffering from depressive symptoms. Compared with nurses who exclusively worked day shifts, nurses who worked night shifts were less likely to be married and younger and self-reported higher PSQI scores (all p<0.05; see Table 1). Moreover, the PSQI and HADS scores were positively correlated (rp = 0.327, p<0.001).
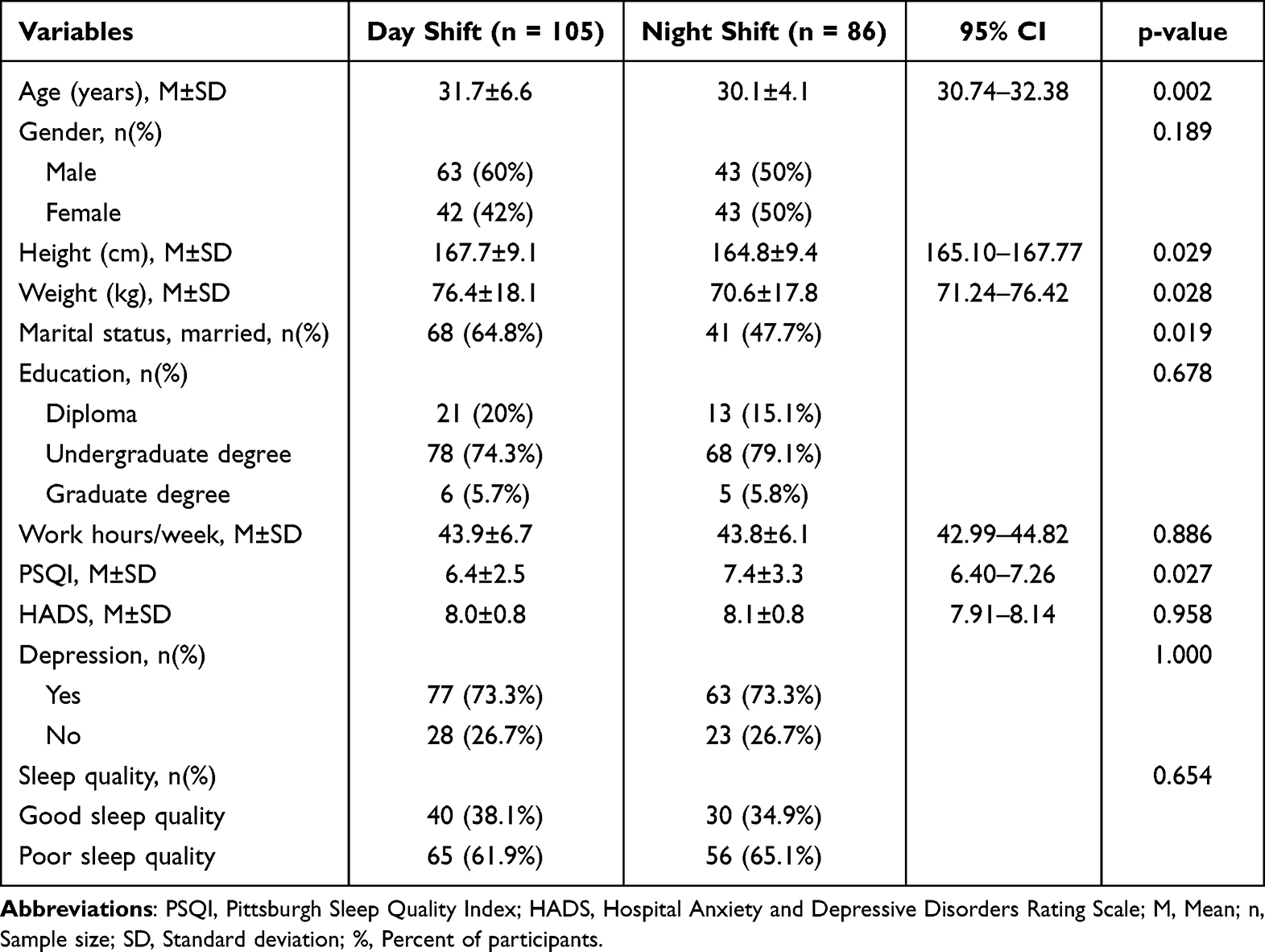 |
Table 1 Demographic, Lifestyle and Clinical Characteristics of Two Groups |
This study used the depression scores among nurses as the dependent variable. Table 2 shows that logistic regression analysis, controlling for age, marital status, and work hours, found no independent association between night shifts and the depression scores (OR, 0.74; 95% CI, 0.36–1.53, p = 0.419). Nurses found to have poor-quality sleep were identified as being at an elevated risk of depressive symptoms (OR, 4.62; 95% CI, 2.26–9.43, p<0.001), as were those who worked longer hours (OR, 0.93; 95% CI, 0.87–1.00, p = 0.049).
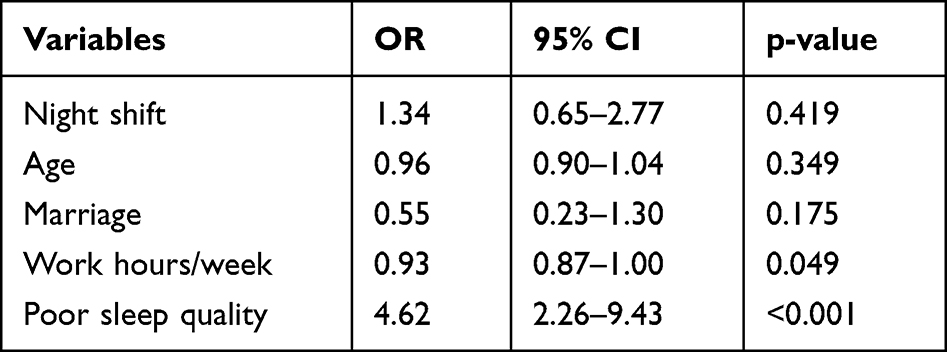 |
Table 2 Binary Logistic Model of the Clinical Determinants of Depressive Symptoms Among Nurses |
Discussion
This study has three key findings. First, the depressive symptoms experienced by nurses who worked night shifts were similar to those observed among nurses who worked day shifts exclusively. Second, poor sleep quality was associated with a higher prevalence of depressive symptoms among nurses. Third, nurses who worked night shifts experienced poorer sleep quality than those who worked exclusively day shifts. Thus, the higher prevalence of depressive symptoms among nurses who work night shifts may be attributed to poor sleep quality resulting from working night shifts.
Our study’s findings of prevalence of depressive symptoms among Saudi Arabian nurses (73.3%) follow the findings reported in other studies.22,23 This prevalence is higher than that reported in Western nations, including the United States and France.24,25 This discrepancy may include Saudi Arabian nurses’ heavy workload, the poor nurse–patient relationships arising from medical disputes, and increasingly high public expectations of nurses in Saudi Arabia.26
Studies have explored the relationships between sleep and physical and mental health in various settings. For example, shift work can result in poor sleep quality and health conditions, including coronary heart disease and diabetes.27,28 Among older workers (those aged 45 and over), studies have found that good sleep quality potentially enhances cognitive abilities and lessens depressive symptoms.29 Furthermore, research conducted in various settings has linked shift work among nurses with poor-quality sleep, fatigue, and depressive symptoms.30–32 Similarly, the nurses in our study who worked night shifts experienced poorer quality sleep and were 462% more likely to suffer from depressive symptoms than their counterparts who worked day shifts. This study contributes to the literature primarily by analyzing the role of sleep quality in the prevalence of depressive symptoms among Saudi Arabian nurses. One possible explanation for the current study’s findings is that night shifts disrupt nurses’ circadian rhythms, negatively impacting sleep and thus inducing depressive symptoms;33 previous studies have established a correlation between disturbances in circadian rhythms, sleep quality, and depressive symptoms.31,34,35 This phenomenon may result from disrupted social routines and abnormal cortisol secretion patterns.36 Other studies have shown that depressive symptoms are reduced when disturbances in circadian rhythms are addressed.37
In accordance with the existing literature, this study identified a positive relationship between depressive symptoms and poor sleep quality.38,39 The sleep quality of those with depressive symptoms also predicted treatment results. Poor sleep quality predicts a poor response to pharmacological, or non-pharmacological interventions, or both to treat depressive symptoms.40,41 In the context of Saudi Arabian nurses, this can be inferred from the correlation between working night shifts, depressive symptoms, and sleep quality, which mediates the relationship between depressive symptoms and working night shifts. The role played by poor-quality sleep may be the result of disturbances to circadian rhythms or inadequate rest and recuperation by nurses caused by sleep disorders,42 and clinical observations have demonstrated that circadian dysregulation may induce different manifestations of mood disorders.42,43 Individuals experiencing depressive symptoms demonstrate irregularities in the timing of the phases of the diurnal (24-hour) cycle. Specifically, the nocturnal body temperature increased earlier than expected. Individuals experiencing depressive symptoms also secrete more cortisol and experience a phase advance of their circadian rhythms.44 In healthy individuals, maximal cortisol secretion occurs in the morning, progressively decreasing during the day until it reaches its lowest point in the evening. Individuals with depressive symptoms display reduced melatonin secretion and experience delays in the phases of their circadian rhythms regarding this secretion.45,46 Other studies report a link between disturbances in social routines and depressive symptoms.36,47
Nonetheless, research findings in this area are inconsistent. For example, research conducted among nurses in Norway did not identify any significant correlation between sleepiness and working night shifts.48 Variations in national healthcare systems, work environments, and workloads may partially explain these contradictory findings.
Limitations
This study has limitations. First, given that this was a cross-sectional study, causation regarding the relationship between working night shifts, depressive symptoms, and sleep quality could not be established. Future studies should adopt a longitudinal design to establish this relationship. Although the causation was not proven, the higher prevalence of poor sleep quality among nurses who work night shifts presents a significant health concern. Second, the questionnaire design separated work shifts into two binary categories-day and night-without considering more subtle work patterns. Further research should also assess diverse work patterns. Third, selection bias and its impact on the findings is a concern, given that the nurses surveyed in this study who worked night shifts were typically younger than their day shift counterparts. However, these potential confounders were adjusted for in logistic regression analysis. Finally, this study did not measure violence or aggression among nurses.
Conclusion
The results of this study suggest a link between a higher prevalence of depressive symptoms among nurses who work night shifts and poor sleep quality, which is the result of night shift working patterns. This study contributes to the literature in its analysis of the role of sleep quality in the depression scores among Saudi Arabian nurses. In future research, longitudinal studies should be used to establish a causal relationship between working night shifts, depressive symptoms, and sleep quality.
Data Sharing Statement
Upon request to corresponding author.
Acknowledgments
The authors are thankful to the Deanship of Scientific Research, College of Nursing Research Center at King Saud University for funding this research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rudman A, Arborelius L, Dahlgren A, Finnes A, Gustavsson P. Consequences of early career nurse burnout: a prospective long-term follow-up on cognitive functions, depressive symptoms, and insomnia. EClinicalMedicine. 2020;27:100565. doi:10.1016/j.eclinm.2020.100565
2. Letvak S, Ruhm CJ, McCoy T. Depression in hospital-employed nurses. Clin Nurse Specialist. 2012;26(3):177–182. doi:10.1097/NUR.0b013e3182503ef0
3. Ministry of Health. Sentencing offenders against health practitioners. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2018-07-30-003.aspx.
4. Alsaleem SA, Alsabaani A, Alamri RS, et al. Violence towards healthcare workers: a study conducted in Abha City, Saudi Arabia. J Family Community Med. 2018;25(3):188. doi:10.4103/jfcm.JFCM_170_17
5. Brown P, Fraser K, Wong CA, Muise M, Cummings G. Factors influencing intentions to stay and retention of nurse managers: a systematic review. J Nurs Manag. 2013;21(3):459–472. doi:10.1111/j.1365-2834.2012.01352.x
6. Korompeli A, Muurlink O, Tzavara C, Velonakis E, Lemonidou C, Sourtzi P. Influence of shiftwork on Greek nursing personnel. Saf Health Work. 2014;5(2):73–79. doi:10.1016/j.shaw.2014.03.003
7. Horton Dias C, Dawson RM. Hospital and shift work influences on nurses’ dietary behaviors: a qualitative study. Workplace Health Saf. 2020;68(8):374–383. doi:10.1177/2165079919890351
8. Lee A, Myung S-K, Cho JJ, Jung Y-J, Yoon JL, Kim MY. Night shift work and risk of depression: meta-analysis of observational studies. J Korean Med Sci. 2017;32(7):1091–1096. doi:10.3346/jkms.2017.32.7.1091
9. Bara A-C, Arber S. Working shifts and mental health–findings from the British Household Panel Survey (1995–2005). Scand J Work Environ Health. 2009;35(5):361–367. doi:10.5271/sjweh.1344
10. Brum MCB, Senger MB, Schnorr CC, Ehlert LR, da Costa Rodrigues T. Effect of night-shift work on cortisol circadian rhythm and melatonin levels. Sleep Sci. 2022;15(2):143. doi:10.5935/1984-0063.20220034
11. Labad J, Salvat-Pujol N, Armario A, et al. The role of sleep quality, trait anxiety and hypothalamic-pituitary-adrenal axis measures in cognitive abilities of healthy individuals. Int J Environ Res Public Health. 2020;17(20):7600. doi:10.3390/ijerph17207600
12. Torsvall L, Akerstedt T, Gillander K, Knutsson A. Sleep on the night shift: 24-hour EEG monitoring of spontaneous sleep/wake behavior. Psychophysiology. 1989;26(3):352–358. doi:10.1111/j.1469-8986.1989.tb01934.x
13. Feng H, Xx Q, Xia CL, Xiao S, Fan L. Association between night shift and sleep quality and health among Chinese nurses: a cross‐sectional study. J Nurs Manag. 2021;29(7):2123–2131. doi:10.1111/jonm.13351
14. Tsuno N, Besset A, Ritchie K. Sleep and depression. J Clin Psychiatry. 2005;66(10):1254–1269. doi:10.4088/JCP.v66n1008
15. Perlman CA, Johnson SL, Mellman TA. The prospective impact of sleep duration on depression and mania. Bipolar Disord. 2006;8(3):271–274. doi:10.1111/j.1399-5618.2006.00330.x
16. Vallières A, Azaiez A, Moreau V, LeBlanc M, Morin CM. Insomnia in shift work. Sleep Med. 2014;15(12):1440–1448. doi:10.1016/j.sleep.2014.06.021
17. Silva-Costa A, Griep R, Rotenberg L. Disentangling the effects of insomnia and night work on cardiovascular diseases: a study in nursing professionals. Brazil J Med Biol Res. 2014;48(2):120–127. doi:10.1590/1414-431x20143965
18. Suleiman KH, Yates BC, Berger AM, Pozehl B, Meza J. Translating the Pittsburgh Sleep Quality Index into Arabic. West J Nurs Res. 2010;32(2):250–268. doi:10.1177/0193945909348230
19. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
20. Snaith RP. The Hospital Anxiety and Depression Scale. Health Qual Life Outcomes. 2003;1(1):29. doi:10.1186/1477-7525-1-29
21. El-Rufaie O, Absood G. Validity study of the hospital anxiety and depression scale among a group of Saudi patients. Br J Psychiatry. 1987;151(5):687–688. doi:10.1192/bjp.151.5.687
22. Al-Maddah EM, Al-Dabal BK, Khalil MS. Prevalence of sleep deprivation and relation with depressive symptoms among medical residents in King Fahd University Hospital, Saudi Arabia. Sultan Qaboos Univ Med J. 2015;15(1):e78. doi:10.2466/pr0.1989.65.2.355
23. Almarhapi SA, Khalil TA. Depression among healthcare workers in North West Armed Forces hospital-Tabuk, Saudi Arabia: prevalence and associated factors. Ann Med Surg. 2021;68:102681. doi:10.1016/j.amsu.2021.102681
24. Nourry N, Luc A, Lefebvre F, Sultan-Taïeb H, Béjean S. Psychosocial and organizational work environment of nurse managers and self-reported depressive symptoms: cross-sectional analysis from a cohort of nurse managers. Int J Occup Med Environ Health. 2014;27(2):252–269. doi:10.2478/s13382-014-0264-x
25. Welsh D. Predictors of depressive symptoms in female medical-surgical hospital nurses. Issues Ment Health Nurs. 2009;30(5):320–326. doi:10.1080/01612840902754537
26. Alsadaan N, Jones LK, Kimpton A, DaCosta C. Challenges facing the nursing profession in Saudi Arabia: an integrative review. Nurs Rep. 2021;11(2):395–403. doi:10.3390/nursrep11020038
27. Kecklund G, Axelsson J. Health consequences of shift work and insufficient sleep. BMJ. 2016;355:i5210. doi:10.1136/bmj.i5210
28. Guo Y, Liu Y, Huang X, et al. The effects of shift work on sleeping quality, hypertension and diabetes in retired workers. PLoS One. 2013;8(8):e71107. doi:10.1371/journal.pone.0071107
29. Giuntella O, Han W, Mazzonna F. Circadian rhythms, sleep, and cognitive skills: evidence from an unsleeping giant. Demography. 2017;54(5):1715–1742. doi:10.1007/s13524-017-0609-8
30. Son Y-J, Park Y-R. Relationships between sleep quality, fatigue and depression on health promoting behavior by shift-work patterns in university hospital nurses. J Korean Biol Nurs Sci. 2011;13(3):229–237.
31. H-S KIM, Choi K-S, Eom M, Joo E-J. Role of circadian types and depressive mood on sleep quality of shift work nurses. Korean J Psychopharmacol. 2011;2011:96–104.
32. Lin SH, Liao WC, Chen MY, Fan JY. The impact of shift work on nurses’ job stress, sleep quality and self‐perceived health status. J Nurs Manag. 2014;22(5):604–612. doi:10.1111/jonm.12020
33. McClung CA. How might circadian rhythms control mood? Let me count the ways. Biol Psychiatry. 2013;74(4):242–249. doi:10.1016/j.biopsych.2013.02.019
34. Hori H, Koga N, Hidese S, et al. 24-h activity rhythm and sleep in depressed outpatients. J Psychiatr Res. 2016;77:27–34. doi:10.1016/j.jpsychires.2016.02.022
35. Bumb J, Enning F, Mueller J, et al. Differential melatonin alterations in cerebrospinal fluid and serum of patients with major depressive disorder and bipolar disorder. Compr Psychiatry. 2016;68:34–39. doi:10.1016/j.comppsych.2016.03.005
36. Peeters F, Nicolson NA, Berkhof J. Levels and variability of daily life cortisol secretion in major depression. Psychiatry Res. 2004;126(1):1–13. doi:10.1016/j.psychres.2003.12.010
37. Jones SG, Benca RM. Circadian disruption in psychiatric disorders. Sleep Med Clin. 2015;10(4):481–493. doi:10.1016/j.jsmc.2015.07.004
38. Klumpp H, Roberts J, Kapella MC, Kennedy AE, Kumar A, Phan KL. Subjective and objective sleep quality modulate emotion regulatory brain function in anxiety and depression. Depress Anxiety. 2017;34(7):651–660. doi:10.1002/da.22622
39. Joo HJ, Kwon KA, Shin J, Park S, Jang S-I. Association between sleep quality and depressive symptoms. J Affect Disord. 2022;310:258–265. doi:10.1016/j.jad.2022.05.004
40. Lowe A, Rajaratnam SM, Hoy K, Taffe J, Fitzgerald PB. Can sleep disturbance in depression predict repetitive transcranial magnetic stimulation (rTMS) treatment response? Psychiatry Res. 2013;210(1):121–126. doi:10.1016/j.psychres.2013.04.028
41. Manglick M, Rajaratnam SM, Taffe J, Tonge B, Melvin G. Persistent sleep disturbance is associated with treatment response in adolescents with depression. Austr N Z J Psychiatry. 2013;47(6):556–563. doi:10.1177/0004867413481630
42. Walker WH, Walton JC, DeVries AC, Nelson RJ. Circadian rhythm disruption and mental health. Transl Psychiatry. 2020;10(1):28. doi:10.1038/s41398-020-0694-0
43. Monteleone P, Maj M. The circadian basis of mood disorders: recent developments and treatment implications. Eur Neuropsychopharmacol. 2008;18(10):701–711. doi:10.1016/j.euroneuro.2008.06.007
44. Cervantes P, Gelber S, Kin F, Nair VN, Schwartz G. Circadian secretion of cortisol in bipolar disorder. J Psychiatry Neurosci. 2001;26(5):411.
45. Hong W, Zhang Q. Biological rhythms advance in depressive disorder. In: Fang Y, editor. Depressive Disorders: Mechanisms, Measurement and Management. Singapore: Springer; 2019:117–133.
46. Claustrat B, Chazot G, Brun J, Jordan D, Sassolas G. A chronobiological study of melatonin and cortisol secretion in depressed subjects: plasma melatonin, a biochemical marker in major depression. Biol Psychiatry. 1984;19(8):1215–1228.
47. Haynes PL, Ancoli‐Israel S, McQuaid J. Illuminating the impact of habitual behaviors in depression. Chronobiol Int. 2005;22(2):279–297. doi:10.1081/CBI-200053546
48. Øyane NM, Pallesen S, Moen BE, Åkerstedt T, Bjorvatn B, Tranah G. Associations between night work and anxiety, depression, insomnia, sleepiness and fatigue in a sample of Norwegian nurses. PLoS One. 2013;8(8):e70228. doi:10.1371/journal.pone.0070228
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
Associations Between Sleep Duration, Sleep Quality, and Depressive Symptoms: Evidence from Medical Graduate Students in China
He H, Zeng Y, Chen Z, Wu M, Wang Y
Nature and Science of Sleep 2025, 17:1853-1862
Published Date: 16 August 2025