Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 12
Sex Differences in Stroke Risk Factors, Clinical Profiles, and In-Hospital Outcomes Among Stroke Patients Admitted to the Medical Ward of Dessie Comprehensive Specialized Hospital, Northeast Ethiopia
Received 4 August 2022
Accepted for publication 17 October 2022
Published 21 October 2022 Volume 2022:12 Pages 133—144
DOI https://doi.org/10.2147/DNND.S383564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Müller
Hussen Abdu,1 Girma Seyoum2
1Department of Anatomy, School of Medicine, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Anatomy, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Hussen Abdu, Department of Anatomy, School of Medicine, College of Medicine and Health Sciences, Wollo University, P.O. Box 1145, Dessie, Ethiopia, Tel +251-910916321, Email [email protected]
Background: A stroke is a vascular accident that affects both men and women. The threat of stroke and outcome status differ between the sexes. Such data are lacking in Ethiopia. Therefore, this study assessed sex differences in stroke risk factors, clinical profiles, and outcomes in the medical ward of Dessie comprehensive specialized hospital.
Methods: A retrospective cross-sectional study was employed among stroke patients. Medical records with complete information and a confirmed diagnosis of stroke using imaging techniques were included in the study. Using simple random sampling, 344 medical records were selected, 312 of which fulfilled the inclusion criteria. Bivariate and multivariate logistic regression analyses and a chi-square test were employed. The frequency, percentage, and mean and standard deviation of the variables were described using descriptive statistics. Findings with a P-value < 0.05 were considered statistically significant.
Results: Most of the patients were above or equal to 45 years old in both sexes. A significantly higher number of male than female patients were aged less than 45 years (p-value-0.001). Younger age (AOR: 2.998, p = 0.000), cigarette smoking (AOR: 2.911, p = 0.009), and Khat chewing (AOR: 3.650, p = 0.001) were risk factors for stroke in males. A higher number of males presented with hemiplegia/hemiparesis 89 (28.5%), aphasia 45 (14.4%), and facial palsy 19 (6.1%). However, more females were unconscious (15.1%). Significant differences were not seen in the stroke outcomes. Furthermore, there were no apparent differences in risk factors for stroke-related mortality.
Conclusion: Males developed stroke at a younger age. Women were older at the time of stroke onset and presented unconscious. More males experienced hemiplegia/hemiparesis, aphasia, and facial palsy. Smoking, drinking, and khat chewing were risk factors for stroke in men. There were no gender differences in the stroke death rate. Therefore, educating the public about stroke risk factors, lifestyle modification, and conducting prospective research is required.
Keywords: clinical profiles, outcome, risk factors, sex difference, stroke, Dessie hospital
Introduction
A stroke or cerebrovascular accident is defined as a vascular problem that is caused either by rapture or blockage of blood vessels that provide the brain with symptoms lasting 24 hours or longer or it may end up with death that only have a vascular origin. It is a rapid, often overwhelming neurological condition that usually puts its victims in danger of passing away or becoming disabled.1–3
Stroke ranks third in the list of causes of mortality and is the second major cause of long-term disability globally.4,5 This vascular problem affects both men and women. However, the incidence rates and outcome status of stroke vary between the sexes.6,7
The main reason for sex-related differences in stroke is because of the differences in the sex steroid hormones, principally estrogen hormone. This explanation is reinforced by sex differences in ischemic stroke in animal models.7 In addition, the hormone, estradiol in females has strong dilation effects on the vascular endothelial and promotes blood flow, whereas testosterone hormone in males has opposite effects that constrict the endothelial and decrease blood flow.8
Genetic and anatomic factors may also contribute to sex-related differences in stroke epidemiology, pathophysiology, and clinical outcomes.9 The sizes of blood vessels are different between men and women. When compared with men, the sizes of arteries and heart are smaller in women. The body size of males is larger when compared with females. This leads to an enlarged left atrium, particularly in humans, and it is associated with an increased risk for the start of a stroke.10 Moreover, in humans, there are differences in the lifestyles such as the status of physical activities, types of food intake, social communications, and cigarette smoking might independently or together contribute to the occurrence of stroke.6,9
Globally, the burden of stroke has been increasing in both males and females, but it has been greater in males. This difference may be because of the improvements of more women from stroke than men in some countries due to the sensitivity of women to health information, health-seeking behaviours, and early access to primary prevention of stroke.2 The other reason why stroke is increased in men than women is that neurovascular risk factors of stroke, such as cigarette smoking, are more common and severe in males and rapidly declined in females.11
Moreover, when compared with their age, the stroke rates are higher in men than women. However, when harmonized with age, a lower risk of stroke has been observed in females than males. When the age approaches 85 years, the risk of stroke is significantly increased in females than males.6,7,12,13 Females are more possibly reach and surpass this age and they need a particular health care system.13,14 Furthermore, after the occurrence of stroke, female patients have poorer treatment outcomes, reduced quality of life, and greater pre- and poststroke disabilities than male patients.6,13,15
Stroke is a condition that considerably lengthens hospital stays and raises the possibility of inpatient mortality. Red cell distribution width (RDW) is a measure of the variability of the size of red blood cells. It is calculated automatically or manually by dividing the standard deviation of red blood cell volume and the volume of red blood cells expressed as a percentage.
Increased red blood cell destruction, such as that caused by haemolysis, or red blood cell production dysfunction brought on by deficiency of iron, vitamin B12, folic acid, or chronic inflammation are the causes of elevated RDW.16 Recent publications have also shown the RDW’s value as a prognostic factor for a variety of cardiovascular diseases, including postoperative stroke.17
According to the reports of the National Institute of Health Stroke Scale, a significantly higher number of females have experienced severe stroke than males.9,18 Furthermore, the occurrence of complications and deaths after stroke are less in men than women; and if enduring, the outcome statuses have become more severe in females than males.9,19,20 This might be because females are elder at the time of stroke onset and are more likely to live without help. Consequently, women may be delayed longer to reach health institutions and the outcome statuses worsen.7 These sex variances of stroke outcomes are detected for the inability of the victims to food intake, dress, grooming, and move from bed to chair which could also be accountable for the prolonged hospitalization of women than men.9,21
According to the reports of the American Heart Association’s 2021, age-specific incidence rates of stroke in younger and middle-aged groups are considerably lower in females than males.22 Stroke epidemiologists supposed that females have a lower rate of stroke in all age groups until they become very elder. In addition, men have better functional outcomes than women after the occurrence of stroke.23,24
There is a shortage of data about sex differences in stroke-related antecedent risk factors, clinical profiles, and outcomes, as well as prevention and management strategies for stroke. In addition, having better and more thoughtful information about these differences could be imperative to be able to devise approaches to prevent and manage stroke more successfully. Consequently, it is necessary to examine whether sex-related differences in the risk factors, clinical presentations, and outcome statuses of stroke exist between the two sexes. Thus, the current study was intended to assess sex-related differences in stroke risk factors, clinical profiles, outcomes, and risk factors for in-hospital mortality among stroke patients at Dessie Comprehensive Specialized Hospital (DCSH).
Materials and Methods
The method and materials portion of the current study shares similarities with our previous study that was conducted to compare ischemic and hemorrhagic strokes in the same institution, on the same population, and following the same protocol.25
Study Setting and Period
The current study was carried out in the medical ward of DCSH from January 2016 to December 2019. Dessie city administration is in the eastern parts of Amhara national regional state, which is about 401 km far from Addis Ababa, the capital city of Ethiopia. The city has one comprehensive specialized public hospital which is named, Dessie Comprehensive Specialized Hospital. Currently, the hospital is serving more than 10 million people in the Amhara, Afar, and other nearby regions.
Study Design
A document-based, retrospective, cross-sectional study design was done amongst patients that were admitted to the medical department of DCSH.
Source and Study Population
The source population for the current study included all stroke patients who were admitted to the medical department of DCSH during the study period, whereas the study population included all stroke patients who were systematically chosen and admitted to the medical department of DCSH during the study period.
Inclusion and Exclusion Criteria
Inclusion Criteria
For the purpose of this study, medical records of stroke patients with diagnoses made by computed tomography, magnetic resonance imaging, or both were taken into consideration.
Exclusion Criteria
Patient files that missed at least 20% of the compulsory information or had no imaging findings were excluded from the study.
Sampling Method and Sample Size Determination
The sample size of the current study was designed using Epi Info 7 through the help of single population proportion formula considering a 13% of mortality rate among admitted stroke patients with a 95% confidence interval, and 3% of marginal error.26 About 1200 patients were expected to visit the hospital during the study period. Considering this assumption, the total sample size of the study subjects was adjusted to 344. Therefore, about 344 patient charts were nominated from the whole 1371 admitted stroke patients, using simple random sampling. Three hundred and twelve medical records fulfilled the inclusion criteria and were incorporated into the study.
Data Extraction Techniques
After evaluating a few medical records, the checklist was created to retain the data’s clarity and quality. The checklist comprised information on patient sociodemographic characteristics, clinical presentation, risk factors, and outcomes for stroke patients. Finally, using checklists, trained medical interns collected the data from nominated medical records.
Variables
Dependent Variables
The dependent variables in the current study were the outcome statuses of the stroke patients from the hospital at the time of discharge.
Independent Variables
The sociodemographic characteristics of the study participants, such as age, sex, marriage, religion, and place of residence, served as the independent variables. Additionally, the study took into account risk factors for strokes such as prior stroke history, hypertension, structural heart disease, diabetes mellitus, atrial fibrillation, family history of stroke, obesity, HIV/AIDS, and headaches. Smoking, drinking, and khat chewing were all factors taken into consideration while analyzing the patients’ behavioral characteristics.
Definition of Terminologies
- Taking of at all quantity of alcohol is considered alcohol consumption.
- Stroke is stated as “rapidly developing clinical signs of focal (or global) disturbance of cerebral function lasting longer than 24 hours unless interrupted by death with no apparent cause other than that of vascular origin” and diagnosed using computed tomography scan/magnetic resonance imaging.
Outcome Statuses of Stroke Patients
- If a stroke patient was fully free of neurological problems during discharge, it was considered completely resolved from neurological deficit.
- If a stroke patient was discharged from the hospital with stroke problems but had improved sign and symptoms, it was stated as discharged with neurologic deficit.
- If the patient died due to stroke and its complications, it was described as death.
- If the patient refused the advice of the professionals and left the hospital without consent, it was stated as discharged against medical advice:
- Glasgow Coma Scale (GCS): It is a clinical method used to measure the level of awareness of patients to the environment, people and time.27
- GCS is good when it ranges from 13 to 15 that indicates a mild brain injury, or the patient is aware to environment, people, and time.
- GCS is moderate when it ranges from 9 to 12 that indicates a moderate brain injury, or lethargic.
- GCS is poor when it is less than or equal to 8 that indicates a severe brain injury, or comatose.
- Sex: It is a biological categorization based primarily on reproductive potential. In this description, a person is considered based on the observable external genitalia they have at birth.28
- Gender: It is a description that the society categorizes a person and recompenses our understandings of femaleness and maleness.29
Analysis of the Data
In this study, the collected data were cleaned, prepared, fed, and analyzed using SPSS software version 24.0. The study subjects were stated using frequency, percentage, mean and standard deviation. To find factors connected to the dependent variables, bivariate and multivariate logistic regression analyses were used. Variables that had a P-value of less than 0.25 in the bivariate analysis were kept in the multivariate analysis. Variables having a P-value of less than 0.05 in the multivariate analysis were determined to be factors substantially linked with stroke variance between sexes. The findings were stated in the form of texts and summary tables.
Results
Socio-Demographic Characteristics of Study Subjects
Of all the study subjects, 150 (48.1%) of them were male and 162 (51.9%) were female. Most of the patients were above or equal to 45 years of age in both sexes. The mean age of the male and female patients was 60.8 ±12.3 and 69.6±11.7 years, respectively. The age of the patients ranged from 20 to 86 and 22 to 90 years in men and women, respectively. Female patients were significantly older than male patients. A higher number of 122 (39.1) women were married than men. Additionally, more females 96 (30.8%) had no formal education than males (26.3%). However, it is not statistically significant. In both sexes, most of the patients were rural residents (Table 1).
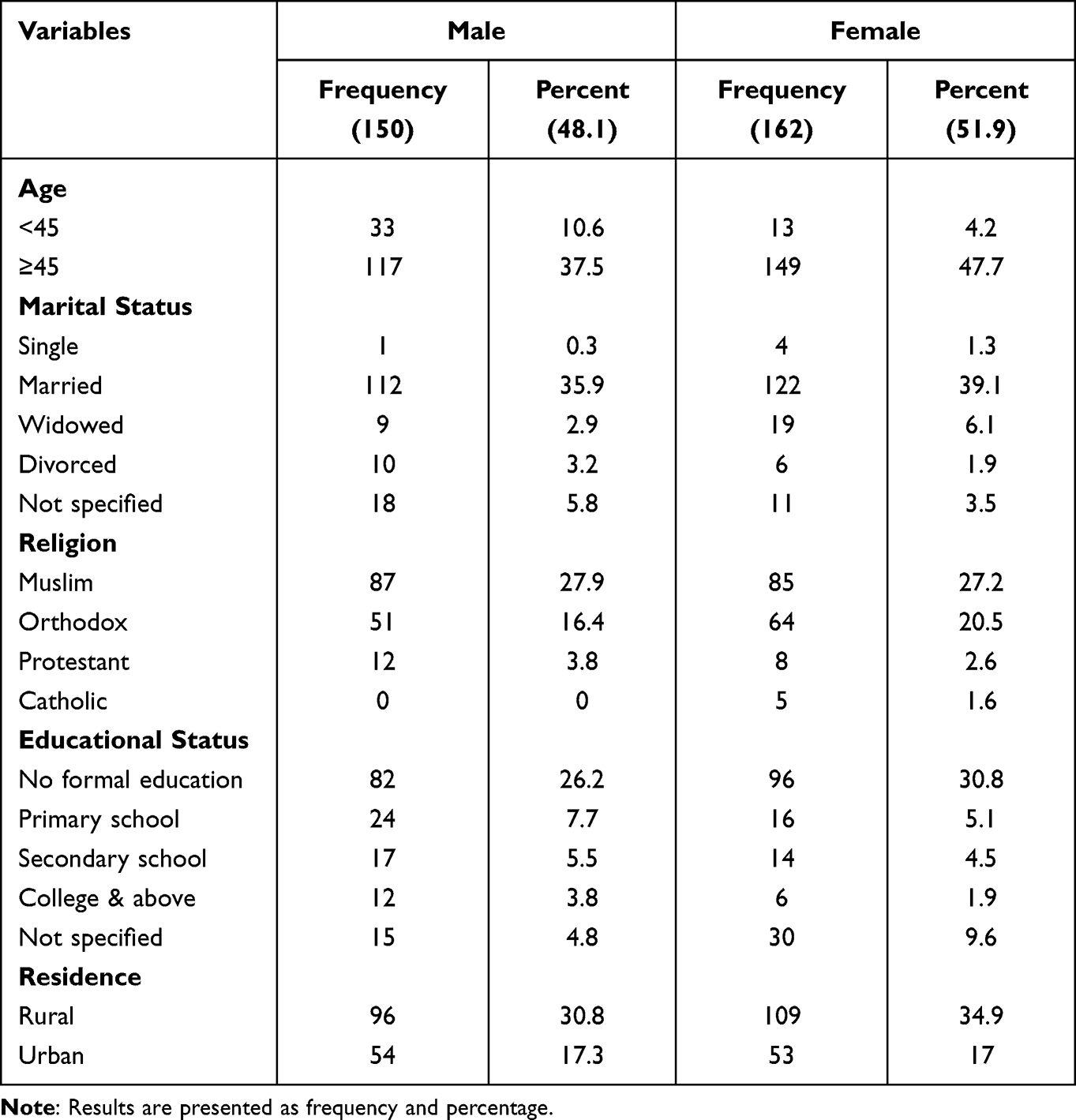 |
Table 1 Comparison of Socio-Demographic Characteristics of Subjects by Sex in the Medical Ward of DCSH from January 2016 to December 2019 |
Distribution of Stroke Risk Factors by Sex
In the current study, a significantly higher number of male patients were smokers 27 (8.7%), alcohol consumers 22 (7.1%), and Khat chewers 33 (10.6%) than female patients. However, hypertension, atrial fibrillation, structural heart diseases, obesity, headache as well as both hypertension and diabetes mellitus were more frequent risk factors in female patients.
A p-value of 0.25 was utilized as the cut-off point to allow for more candidate variables in binary logistic regression. Thus, the multivariable logistic regression was proposed to include age, DM, smoking, drinking, structural heart problems, chewing khat, obesity, headaches, and migraines. According to multivariable logistic regression with 95% CI, age (AOR: 2.998), cigarette smoking (AOR: 2.911), and khat chewing (AOR: 3.650) were statistically significant risk factors for stroke in male patients compared to female patients. Males are roughly three times more likely than females to get a stroke at a younger age. Males had higher stroke risk factors than females for smoking cigarettes and chewing khat, respectively, by 2.911 and 3.650 times. However, with a p-value of <0.05, structural heart disease (AOR: 0.420) was less likely to be a risk factor for stroke in men than in women (Table 2).
 |
Table 2 Binary and Multivariable Logistic Regression for Comparison of Stroke Risk Factors Distribution of Subjects by Sex in the Medical Ward of DCSH from January 2016 to December 2019 |
Clinical Profile of Patients
During admission to the hospital, a significantly higher number of male patients presented with hemiplegia/hemiparesis 89 (28.5%), aphasia 45 (14.4%), and facial palsy 19 (6.1%) than female patients. In addition, more males experienced headache 7 (2.2%), visual perceptual deficits 8 (2.6%), ataxia, and in-coordination 12 (3.8%) than females. Yet, it was not statistically significant.
Nevertheless, a significantly higher number of females were presented as unconscious, 47 (15.1%). Furthermore, more females were presented with an inability to detect sensory stimuli and decreased ability of body movements 84 (26.9%), urinary incontinence 49 (15.7%), and vomiting 14 (4.5%) than male patients. So far, it has not been statistically significant. In addition, the average systolic blood pressure (SBP) and diastolic blood pressure (DBP) in female patients (SBP = 167.4±17.3 mmHg; DBP = 95.6±23.5 mmHg) were higher than those in male patients (SBP = 161.4±19.6 mmHg; DBP = 93.7±22.8 mmHg). During admission, the mean GCS in most male and female patients ranged from 9 to 12 (Table 3).
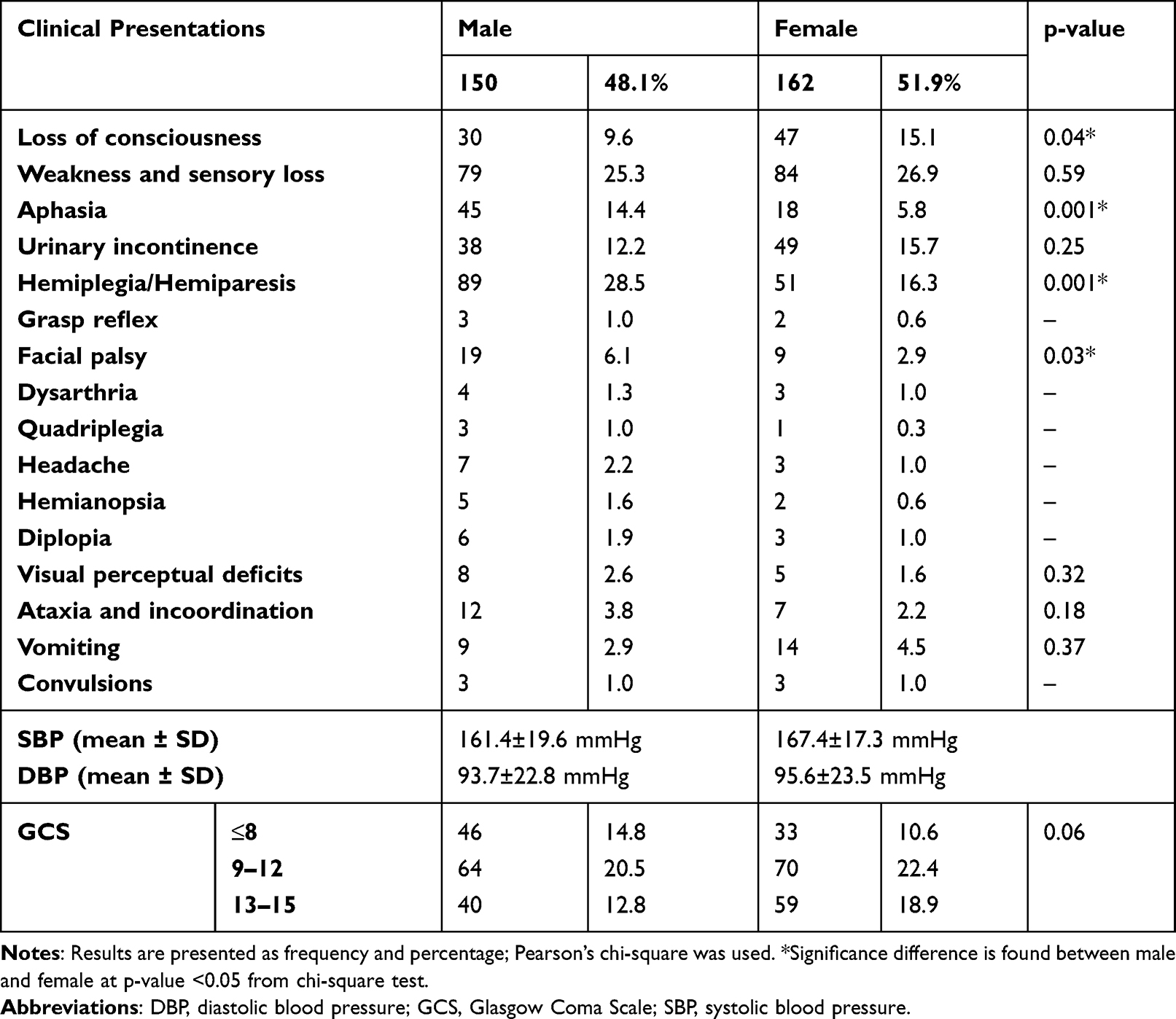 |
Table 3 Sex Distribution of Clinical Presentations of Stroke at the Time of Admission in the Medical Ward of DCSH from January 2016 to December 2019 |
Comparison of Stroke Outcomes Between Men and Women
In this study, the outcome status of five (1 male and 4 female) stroke patients was not specified in their corresponding medical records and excluded from the analysis. Subsequently, the outcome status of 307 (149 (48.5%) male and 158 (51.5%) female) patients were analyzed. Fifty-seven (18.6%) male and 53 (17.3%) female patients were completely improved from any clinical neurological manifestations and discharged from the hospital. However, more females 24 (7.8%) than males 18 (5.9%) were discharged with neurological deficits. Similarly, to some extent, a higher number of 37 (12.0%) male patients were in a paradox of the consultation of the professionals and left the hospital without agreement. However, a higher proportion of deaths, 36 (11.7%), occurred in females than in males, but not statistically significant (Table 4).
 |
Table 4 Comparison of Stroke Outcomes by Sex in the Medical Ward of DCSH from January 2016 to December 2019 |
Of the total 31 (10.1%) deaths in males, 22 (7.2%) of them were hypertensive and 9 (2.9%) of them had AF. Similarly, nearly the same proportion of females was hypertensive (22 (7.2%)) and had AF (10 (3.3%)). In both sexes, an increased number of deaths were noted in the patients with a GCS of 8 or less (Table 5).
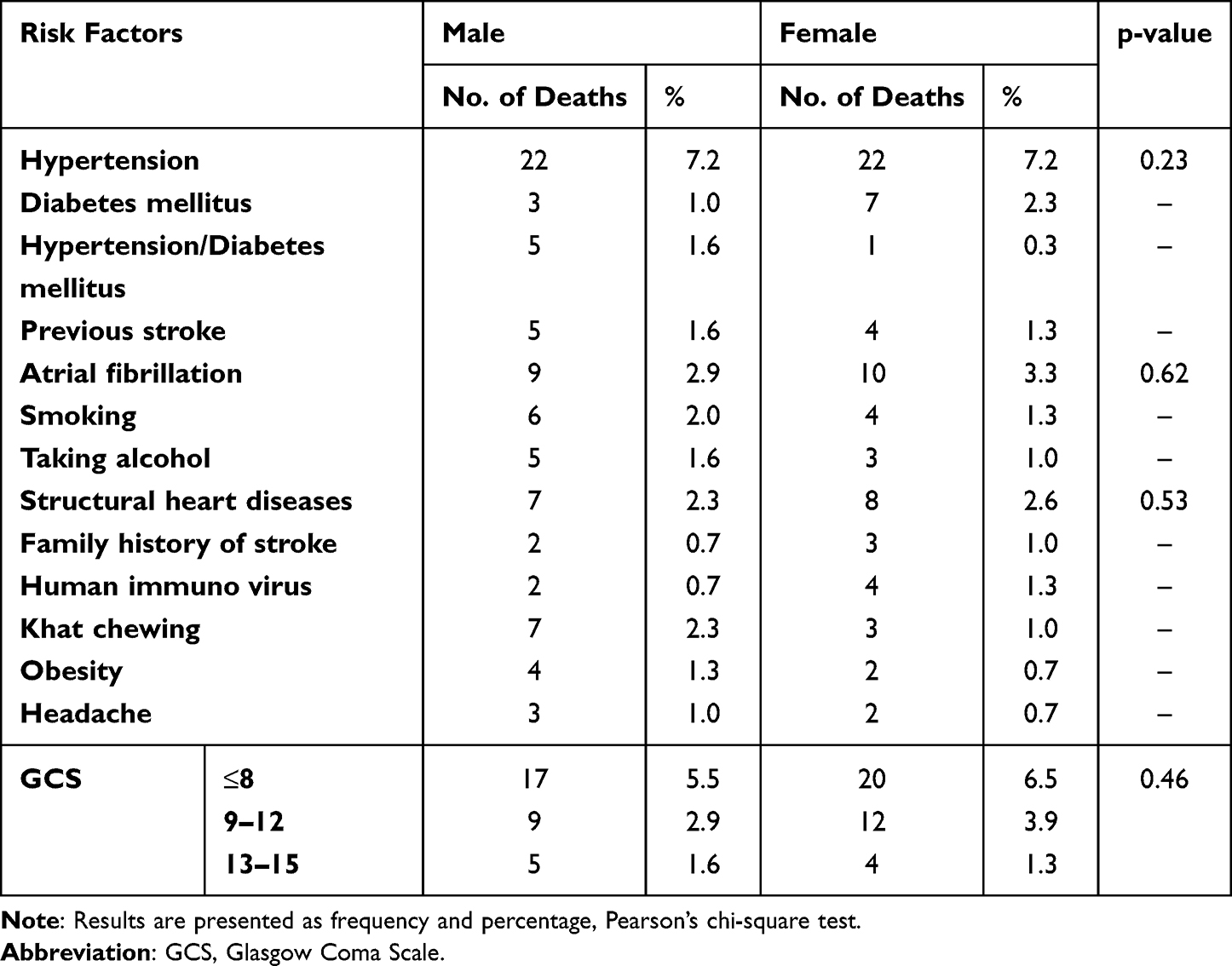 |
Table 5 Comparison of the Proportion of Risk Factors for Stroke-Related Deaths by Sex in the Medical Ward of DCSH from January 2016 to December 2019 |
Discussion
To our understanding, the current study is the first study that describes sex differences in clinical presentations, antecedent factors, and outcome statuses of stroke in the medical department of DCSH. The foremost results in this study show that women were significantly older and presented unconscious during admission than men. Men were more probably to be educated, involved in cigarette smoking, alcohol consumption, khat chewing, and experience hemiplegia, aphasia, and facial palsy than women.
In the current study, many of the stroke patients were 45 years and older. Compared with female patients, males experienced stroke nearly three times than females at a younger age. The mean age of male and female patients was 60.8±12.3 and 69.6±11.7 years, respectively. This is consistent with other previous studies that stated significant age differences between male and female stroke patients.13,30–32 However, the findings of our study varied from the previous studies studied in China, which established stroke occurs at an elder age in males when compared with females.33
In the current study, women were less formally educated than men, and this may indicate that less educational status may have a significant effect on the stroke status in women. Less formal education in females may have a negative effect on their economic status. In addition, less educational status in females may affect the use of stroke drugs and may decrease the quality of health care15 and these patients might be missing follow-up health care, which might increase the risk of stroke relapse.25
In the current study, more women than men were comatose when they were admitted. This is consistent with other studies that found female stroke patients were more likely than male patients to be unconscious at arrival and to have altered levels of consciousness.15,34–36 This might contribute to stroke severity, delays in seeking medical care, delays in prompt diagnosis, and delays in admission to acute care. However, males were more likely than females to have hemiplegia/hemiparesis, aphasia, and facial palsy. Similar to another earlier study, this one also found that gait problems were more common in male patients than in female patients.32 In terms of other clinical symptoms, such as swallowing, vomiting, and headaches, there were no significant differences between the sexes.
Nearly in 77% of the people with an episode of stroke, blood pressure was more than 140/90 mmHg.37 Studies showed that about 26% of ischemic stroke is caused because of hypertension.38 Globally, in adults older than 25 years of age, the prevalence of hypertension was 40%, affecting about 29.2% of men and 24.8% of women.39
The current study showed that SBP and DBP were high in both sexes. This indicated that most of the patients were hypertensive. However, females were more to be expected to have higher SBP and DBP levels than males. This agrees with the other previous study that reported a higher SBP in women than men and women taking anti-hypertensive drugs.40 This might be because of physical inactivity in most of the females that may increase the rates of blood pressure as females are more likely than males to be not engaged in physical activity in all age groups.5,41
Previous studies showed an association between smoking34,42–44 and alcohol intake34,43–46 with stroke morbidity and mortality. In addition, studies also showed that alcohol consumption and cigarette smoking were more common in males than females.43,47,48 Consistent with these studies, a higher proportion of men were cigarette smokers and alcohol drinkers than women in this study, and males should withhold themselves from smoking and alcohol intake.
Nevertheless, the current study did not find any significant sex differences in the other stroke risk factors. Significant gender differences in stroke risk factors, such as hypertension,15,43,44 atrial fibrillation,44,49 dyslipidemia, and obesity,43,44 have been reported in several studies. These are more common in women than in men. All of these risk factors for stroke are modifiable risk factors; they can be prevented, and the community may be advised to change their way of life.
In this study, the in-hospital outcome status of the stroke patients revealed that more male patients than female patients were completely free of any clinical neurological symptoms and were discharged from the hospital. Furthermore, fewer males than women were discharged from the hospital with neurological impairments. This suggests that women experienced more severe strokes than men, which is in line with other studies.50–52 These sex disparities in stroke outcome status may be caused by the later onset of stroke in females than in men, as well as the higher expectation that females would be able to live independently, which delays hospitalization and worsens outcome status.7
In line with other earlier studies,15,53 there was no discernible difference in the death rate from stroke between the two sexes. However, according to other studies,34,54 women die at a greater rate than men do. In terms of risk factors for stroke mortality, the majority of patients had a history of hypertension and atrial fibrillation. No significant disparities between men and women were found. This could be due to a relatively small sample size that has been used in the current study.
Conclusion and Recommendations
In conclusion, the present investigation revealed sex-related differences in clinical profiles and stroke risk factors among patients admitted to the study hospital during the study period. Males developed stroke at a younger age than females. Males more frequently than females experienced hemiplegia/hemiparesis, aphasia, and facial palsy. Additionally, men are more likely than women to experience stroke risk factors such as smoking, consuming alcohol, and chewing khat. But compared to men, women more frequently arrived unconscious and were older at the time of stroke onset. Additionally, there was a higher likelihood that structural heart disease was linked to female stroke risk factors. The mortality rate from stroke did not differ by gender. In terms of in-hospital mortality from stroke, there were no independent factors that varied by gender. Therefore, it is critical to educate the general population about the risk factors for stroke and the significance of altering lifestyle choices and habits like stopping smoking, drinking alcohol, and chewing khat.
Strength of the Study
The study was the first attempt to look at sex-related variations in stroke in the study hospital. The study sought to understand clinical and risk variables as well as patient outcome statuses that assist doctors, hospital administration, and the general public in adapting themselves to prevent, treat, and provide rehabilitation for victims who have been left with a neurological squeal.
Limitations of the Study
In this kind of retrospective study, it was challenging to avoid prejudices. Additionally, broad population inferences from institution-based research findings were not possible.
Future Line of the Study
To overcome biases and establish inferences about the population, community-based prospective surveys on stroke risk factors, clinical profile, and prognosis should be encouraged. In addition, community-based prospective studies on sex differences in stroke risk factors, clinical profile, and prognosis should be promoted. In addition to understand the variability of prognosis of stroke patients’, studies on RDW examination is recommended.
Patient and Public Involvement
The data of the current study were extracted from the patient charts. Therefore, the study subjects and their caregivers were not directly participated in the design of the study protocols. However, the directors of the hospital were involved in the development of data extraction tools. Before data collection, they also reviewed the objectives of the study.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DBP, diastolic blood pressure; DCSH, Dessie Comprehensive Specialized Hospital; GCS, Glasgow Coma Scale; RDW, red cell distribution width; SBP, systolic blood pressure; SPSS, Statistical Package for Social Science.
Availability of the Data
All the necessary data that help the results of the current study are incorporated in the manuscript.
Ethics Approval and Consent to Participate
The study complies with the Declaration of Helsinki. Since the study was retrospective, a waiver for ethical approval and consent to participate was obtained from the Institutional Review Board of Wollo University. We received a letter of support from Wollo University’s College of Medicine and Health Sciences to carry out the present study. The director of DCSH was provided with the letter of support, and consent was acquired to view the necessary medical information. Patient confidentiality was guaranteed by ensuring the patient data was “de-identified and anonymous.”
Acknowledgment
It is our great pleasure to thank the record staff and the leaders of DCSH who permitted us to contact documents of the admitted patients. We are also thanking the data collectors and all the study subjects whose information was used for the present study.
Author Contributions
All the authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was not obtained from any individual or institution for the study.
Disclosure
The current study does not contain any conflicts of interest that the authors have declared.
References
1. Bennett DA, Krishnamurthi RV, Barker-Collo S, et al. The global burden of ischemic stroke: findings of the GBD 2010 study. Glob Heart. 2014;9(1):107–112. doi:10.1016/j.gheart.2014.01.001
2. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
3. Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990–2010: findings from the global burden of disease study 2010. lancet. 2014;383(9913):245–255. doi:10.1016/S0140-6736(13)61953-4
4. Girijala RL, Sohrabji F, Bush RL. Sex differences in stroke: review of current knowledge and evidence. Vasc Med. 2017;22(2):135–145. doi:10.1177/1358863X16668263
5. Samai AA, Martin-Schild S. Sex differences in predictors of ischemic stroke: current perspectives. Vasc Health Risk Manag. 2015;11:427. doi:10.2147/VHRM.S65886
6. Hiraga A. Gender differences and stroke outcomes. Neuroepidemiology. 2017;48(1–2):61–62. doi:10.1159/000475451
7. Reeves MJ, Bushnell CD, Howard G, et al. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008;7(10):915–926. doi:10.1016/S1474-4422(08)70193-5
8. Krause DN, Duckles SP, Pelligrino DA. Influence of sex steroid hormones on cerebrovascular function. J Appl Physiol. 2006;101(4):1252–1261. doi:10.1152/japplphysiol.01095.2005
9. Haast RA, Gustafson DR, Kiliaan AJ. Sex differences in stroke. J Cereb Blood Flow Metab. 2012;32(12):2100–2107. doi:10.1038/jcbfm.2012.141
10. Abhayaratna WP, Seward JB, Appleton CP, et al. Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol. 2006;47(12):2357–2363. doi:10.1016/j.jacc.2006.02.048
11. Barker-Collo S, Bennett DA, Krishnamurthi RV, et al. Sex differences in stroke incidence, prevalence, mortality and disability-adjusted life years: results from the global burden of disease study 2013. Neuroepidemiology. 2015;45(3):203–214. doi:10.1159/000441103
12. Bonita R. Epidemiology of stroke. Lancet. 1992;339(8789):342–344. doi:10.1016/0140-6736(92)91658-U
13. Caso V, Paciaroni M, Agnelli G, et al. Gender differences in patients with acute ischemic stroke. Womens Health. 2010;6(1):51–57. doi:10.2217/whe.09.82
14. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18–e209. doi:10.1161/CIR.0b013e3182009701
15. Di Carlo A, Lamassa M, Baldereschi M, et al. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke. 2003;34(5):1114–1119. doi:10.1161/01.STR.0000068410.07397.D7
16. Duchnowski P, Hryniewiecki T, Stokłosa P, et al. Number of erythrocytes as a prognostic marker in patients undergoing heart valve surgery. Kardiol Pol. 2018;76(4):791–793. doi:10.5603/KP.2018.0076
17. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, et al. Red cell distribution width is a prognostic marker of perioperative stroke in patients undergoing cardiac valve surgery. Interact Cardiovasc Thorac Surg. 2017;25(6):925–929. doi:10.1093/icvts/ivx216
18. Gall S, Donnan G, Dewey HM, et al. Sex differences in presentation, severity, and management of stroke in a population-based study. Neurology. 2010;74(12):975–981. doi:10.1212/WNL.0b013e3181d5a48f
19. Roquer J, Campello AR, Gomis M. Sex differences in first-ever acute stroke. Stroke. 2003;34(7):1581–1585. doi:10.1161/01.STR.0000078562.82918.F6
20. Arboix A, Oliveres M, García-Eroles L, et al. Acute cerebrovascular disease in women. Eur Neurol. 2001;45(4):199–205. doi:10.1159/000052130
21. Petrea RE, Beiser AS, Seshadri S, et al. Gender differences in stroke incidence and poststroke disability in the Framingham heart study. Stroke. 2009;40(4):1032–1037. doi:10.1161/STROKEAHA.108.542894
22. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254–e743. doi:10.1161/CIR.0000000000000950
23. Bushnell CD, Chaturvedi S, Gage KR, et al. Sex differences in stroke: challenges and opportunities. J Cereb Blood Flow Metab. 2018;38(12):2179–2191. doi:10.1177/0271678X18793324
24. Carcel C, Woodward M, Wang X, et al. Sex matters in stroke: a review of recent evidence on the differences between women and men. Front Neuroendocrinol. 2020;59:100870. doi:10.1016/j.yfrne.2020.100870
25. Abdu H, Tadese F, Seyoum G. Comparison of Ischemic and hemorrhagic stroke in the medical ward of Dessie Referral Hospital, Northeast Ethiopia: a retrospective study. Neurol Res Int. 2021;2021:34.
26. Greffie ES, Mitiku T, Getahun S. Risk factors, clinical pattern and outcome of stroke in a referral hospital, Northwest Ethiopia. Clin Med Res. 2015;4(6):182–188. doi:10.11648/j.cmr.20150406.13
27. Jain S, Iverson LM. Glasgow coma scale. University of Glasgow; 2018.
28. Marchbank J, Letherby G. Introduction to Gender: Social Science Perspectives. Routledge; 2014.
29. Shaw S, Lee J. Women’s Voices, Feminist Visions: Classic and Contemporary Readings (B&B). McGraw-Hill Education; 2009.
30. Berglund A, Schenck-Gustafsson K, von Euler M. Sex differences in the presentation of stroke. Maturitas. 2017;99:47–50. doi:10.1016/j.maturitas.2017.02.007
31. Jerath NU, Reddy C, Freeman WD, et al. Gender differences in presenting signs and symptoms of acute ischemic stroke: a population-based study. Gend Med. 2011;8(5):312–319. doi:10.1016/j.genm.2011.08.001
32. Stuart-Shor EM, Wellenius GA, DelloIacono DM, et al. Gender differences in presenting and prodromal stroke symptoms. Stroke. 2009;40(4):1121–1126. doi:10.1161/STROKEAHA.108.543371
33. Wang J, Ning X, Yang L, et al. Sex differences in trends of incidence and mortality of first-ever stroke in rural Tianjin, China, from 1992 to 2012. Stroke. 2014;45(6):1626–1631. doi:10.1161/STROKEAHA.113.003899
34. Watila M, Bwala S, Ibrahim A. Gender variation in risk factors and clinical presentation of acute stroke, Northeastern Nigeria. J Neurosci Behavior Health. 2011;3(3):38–43.
35. Lisabeth LD, Brown DL, Hughes R, et al. Acute stroke symptoms: comparing women and men. Stroke. 2009;40(6):2031–2036. doi:10.1161/STROKEAHA.109.546812
36. Ali M, van Os HJA, van der Weerd N, et al. Sex differences in presentation of stroke: a systematic review and meta-analysis. Stroke. 2022;53(2):345–354. doi:10.1161/STROKEAHA.120.034040
37. Association, AH. High blood pressure. (Statistical Fact Sheet 2013 Update); 2014.
38. Whisnant JP. Modeling of risk factors for ischemic stroke: the Willis Lecture. Stroke. 1997;28(9):1840–1844. doi:10.1161/01.STR.28.9.1840
39. Selection, W.E.C.o.t., U.o.E. Medicines, and W.H. Organization. The selection and use of essential medicines: report of the WHO expert committee, 2013 (including the 18th WHO Model List of Essential Medicines and the 4th WHO Model List of Essential Medicines for Children). World Health Organization; 2014.
40. Wang Y, Xiao B-Q, Li B-H, et al. Sex difference in the incidence of stroke and its corresponding influence factors: results from a follow-up 8.4 years of rural China hypertensive prospective cohort study. Lipids Health Dis. 2019;18(1):1–10. doi:10.1186/s12944-018-0950-y
41. Doumas M, Papademetriou V, Faselis C, et al. Gender differences in hypertension: myths and reality. Curr Hypertens Rep. 2013;15(4):321–330. doi:10.1007/s11906-013-0359-y
42. Peters SA, Suxley RR, Sattar N, et al. Sex differences in the excess risk of cardiovascular diseases associated with type 2 diabetes: potential explanations and clinical implications. Curr Cardiovasc Risk Rep. 2015;9(7):1–7. doi:10.1007/s12170-015-0462-5
43. Yu C, An Z, Zhao W, et al. Sex differences in stroke subtypes, severity, risk factors, and outcomes among elderly patients with acute ischemic stroke. Front Aging Neurosci. 2015;7:174. doi:10.3389/fnagi.2015.00174
44. Yan L, Huangfu C, Yang N, et al. Sex-related differences in the factors associated with outcomes among patients with strokes of undetermined source: a hospital-based follow-up study. Postgrad Med. 2021;133(4):428–435. doi:10.1080/00325481.2021.1886770
45. Zhang C, Qin -Y-Y, Chen Q, et al. Alcohol intake and risk of stroke: a dose–response meta-analysis of prospective studies. Int J Cardiol. 2014;174(3):669–677. doi:10.1016/j.ijcard.2014.04.225
46. Emdin CA, Wong CX, Hsiao AJ, et al. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men: systematic review and meta-analysis of cohort studies. BMJ. 2016;2016:352.
47. Li Z, Bai Y, Guo X, et al. Alcohol consumption and cardiovascular diseases in rural China. Int J Cardiol. 2016;215:257–262. doi:10.1016/j.ijcard.2016.04.095
48. Tolibova N, Vakhabova N. Gender differences in stroke subtypes, severity, risk factors, and outcomes among elderly patients with acute ischemic stroke in Uzbekistan. J Neurol Sci. 2017;381:377.
49. Rathfoot C, Edrissi C, Sanders CB, et al. Gender differences in comorbidities and risk factors in ischemic stroke patients with a history of atrial fibrillation. BMC Neurol. 2021;21(1):1–15. doi:10.1186/s12883-021-02214-8
50. Ong C-T, Wong Y-S, Sung S-F, et al. Sex-related differences in the risk factors for in-hospital mortality and outcomes of ischemic stroke patients in rural areas of Taiwan. PLoS One. 2017;12(9):e0185361. doi:10.1371/journal.pone.0185361
51. Santalucia P, Pezzella FR, Sessa M, et al. Sex differences in clinical presentation, severity and outcome of stroke: results from a hospital-based registry. Eur J Intern Med. 2013;24(2):167–171. doi:10.1016/j.ejim.2012.10.004
52. Irie F, Kamouchi M, Hata J, et al. Sex differences in short-term outcomes after acute ischemic stroke: the Fukuoka Stroke Registry. Stroke. 2015;46(2):471–476. doi:10.1161/STROKEAHA.114.006739
53. Forster A, Gass A, Kern R, et al. Gender differences in acute ischemic stroke: etiology, stroke patterns and response to thrombolysis. Stroke. 2009;40(7):2428–2432. doi:10.1161/STROKEAHA.109.548750
54. Reeves MJ, Fonarow GC, Zhao X, et al. Quality of care in women with ischemic stroke in the GWTG program. Stroke. 2009;40(4):1127–1133. doi:10.1161/STROKEAHA.108.543157
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pediatric Stroke from Bench to Bedside: A Single-Center Experience in Saudi Arabia
Al-Sharydah AM, Al-Arfaj HK, Al-Suhibani SS, Al-Safran FS, Al-Abdulwahhab AH, Al-Jubran SA, AlSaflan AA
Vascular Health and Risk Management 2022, 18:529-540
Published Date: 13 July 2022
Risk Factors and Outcomes of Patients with Carbapenem-Resistant Pseudomonas aeruginosa Bloodstream Infection
Wei X, Li L, Li M, Liang H, He Y, Li S
Infection and Drug Resistance 2023, 16:337-345
Published Date: 19 January 2023
External Validation of the Nelson Equation for Kidney Function Decline in Patients with Acute Ischemic Stroke or Transient Ischemic Attack
Zhou H, Chen W, Suo Y, Meng X, Zhao X, Wang M, Liu L, Li H, Pan Y, Wang Y
Clinical Interventions in Aging 2023, 18:901-909
Published Date: 6 June 2023
Knowledge of Cardiovascular Disease Risk Factors and Its Primary Prevention Practices Among the Saudi Public – A Questionnaire-Based Cross-Sectional Study
Bashatah A, Syed W, Al-Rawi MBA
International Journal of General Medicine 2023, 16:4745-4756
Published Date: 20 October 2023
Navigating the Knowledge of Risk Factors, Warning Signs, of Stroke - A Community-Based Cross-Sectional Study Among Saudi Adults in Riyadh Saudi Arabia
Syed W, AlHarbi AA, Samarkandi OA, Alobaid AM, Alsulaihim IN
International Journal of General Medicine 2023, 16:5869-5883
Published Date: 12 December 2023