Back to Journals » Clinical Interventions in Aging » Volume 18
External Validation of the Nelson Equation for Kidney Function Decline in Patients with Acute Ischemic Stroke or Transient Ischemic Attack
Authors Zhou H ![]() , Chen W, Suo Y, Meng X, Zhao X
, Chen W, Suo Y, Meng X, Zhao X ![]() , Wang M, Liu L
, Wang M, Liu L ![]() , Li H, Pan Y, Wang Y
, Li H, Pan Y, Wang Y
Received 17 February 2023
Accepted for publication 1 June 2023
Published 6 June 2023 Volume 2023:18 Pages 901—909
DOI https://doi.org/10.2147/CIA.S407338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Hongyu Zhou,1,2 Weiqi Chen,1,2 Yue Suo,1,2 Xia Meng,1,2 Xingquan Zhao,1,2 Mengxing Wang,1,2 Liping Liu,1,2 Hao Li,1,2 Yuesong Pan,1,2 Yongjun Wang1– 4
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China; 4Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
Correspondence: Yongjun Wang; Yuesong Pan, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China, Email [email protected]; [email protected]
Background: There is a close brain–kidney interaction following ischemic cerebrovascular disease. The new-onset kidney injury after stroke leads to severe neurological deficits and poor functional outcomes. We aimed to validate the Nelson equation for predicting the new-onset and long-term kidney function decline in patients with acute ischemic stroke (AIS) or transient ischemic attack (TIA).
Methods: A total of 3169 patients were enrolled in the Third China National Stroke Registry, whose baseline estimated glomerular filtration rate (eGFR) ≥ 60 mL/min/1.73 m2. The outcome of interest was the incident eGFR< 60 mL/min/1.73 m2 at 3 months. The prediction equation of participants with or without diabetes was validated respectively. The receiver operating characteristic curve (AUC) evaluated prediction performance. The Delong test compared the Nelson equation performance with the O’Seaghdha equation and the Chien equation. Continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were determined to evaluate the incremental effect.
Results: During the 3-mo follow-up period, among 1151 patients with diabetes, there were 31 cases (2.7%) of reduced eGFR. Meanwhile, among 2018 non-diabetic patients, there were 23 cases (1.1%) of reduced eGFR. The Nelson equation showed good discrimination and was well-calibrated in patients with diabetes (AUC 0.82, Hosmer-Lemeshow test p = 0.67) or without diabetes (AUC 0.82, Hosmer-Lemeshow test p = 0.09). The performance of the Nelson equation was superior to other equation, as increased continuous NRI (diabetic, 0.64; non-diabetic, 1.13) and IDI (diabetic, 0.10; non-diabetic, 0.13) to the Chien equation.
Conclusion: The Nelson equation reliably predicted the risks of the new-onset and long-term kidney function decline in patients with AIS or TIA, which could help clinicians screen high-risk patients and improve clinical care.
Keywords: stroke, transient ischemic attack, kidney disease, prognosis, risk factors
Introduction
Accumulating evidence from clinical and basic studies indicated a tight interaction between the brain and the kidney.1 Kidney disease is an independent risk factor for the incidence of stroke and has adverse effects on stroke recurrence and disability.2,3 In addition, recent research demonstrated that the new-onset kidney injury after stroke leads to severe neurological deficits and poor functional outcomes.1,4,5 Given the potential for kidney disease prevention and management, the identification of stroke patients at an increased risk of declining kidney function serves to inform targeted risk factor modification and improve stroke prognosis.6
Novel risk equations have been introduced to anticipate the likelihood of kidney disease onset, including the Nelson equation, formulated using community cohort data and exhibited satisfactory performance in the subsequent validation cohort analysis.7–9 Efficient prediction equations have the potential to enable clinicians to promptly identify high-risk patients, thereby facilitating the timely implementation of targeted management and treatment strategies. Despite the availability of various prediction equations for kidney dysfunction, including the Nelson equation, their applicability in stroke patients remains unvalidated. The potential impact of brain-kidney interaction on prediction accuracy remains uncertain.
The present study aimed to assess the validity of the Nelson equation in predicting the incidence of new-onset and long-term kidney function decline in patients with acute ischemic stroke (AIS) or transient ischemic attack (TIA).
Methods
Study Population
The validation cohorts were obtained from the Third China National Stroke Registry (CNSR-III), a nationwide prospective registry that enrolled patients with AIS or TIA within 7 days of symptom onset. The design and methodology of the CNSR-III have been previously delineated.10 The CNSR-III aimed to investigate the pathogenesis and prognostic factors of ischemic cerebrovascular disease by collecting and analyzing the etiology classification, imaging and biology markers. The registry was conducted at 201 hospitals in China between August 2015 and March 2018. All participants or their legal proxies provided written informed consent. The protocol was approved by the ethics committee at each study center. In the validation cohorts, individuals with a baseline eGFR greater than 60 mL/min/1.73m² were considered eligible for participation.
Baseline Data Collection
Trained research coordinators collected baseline data through face-to-face interviews or medical records, including age, sex, body mass index (BMI, the weight in kilograms divided by height in meters, kg/m2), systolic blood pressure (SBP) at admission, smoking status, medical history (ischemic stroke, intracranial hemorrhage (ICH), TIA, coronary heart disease, heart failure, atrial fibrillation or flutter, hypertension, diabetes mellitus (DM), and hypercholesterolemia), medication history (antidiabetic agents, antihypertensive agents, and lipid-lowering agents), stroke types (AIS or TIA), and the National Institutes of Health Stroke Scale (NIHSS) score. The etiological classification was performed according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.11
DM was defined as a self-reported history of physician-diagnosed diabetes, the use of antidiabetic agents, or hemoglobin A1c (HbA1c) ≥6.5% (48 mmol/mol).12 The diagnosis of hypertension was based on blood pressure ≥ 140/90 mmHg, the use of antihypertensive medications, or self-reported hypertension.13 Cardiovascular disease (CVD) included ischemic stroke, ICH, TIA, coronary heart disease, and heart failure.7
Sample Collection and Measurement
Blood and urine specimens were obtained from the participants at admission and during the 3-month follow-up period, then transported through a cold chain to the core laboratory in Beijing Tiantan Hospital. Centralized testing was performed to determine HbA1c, urine creatinine, and urine albumin levels. The estimated glomerular filtration rate (eGFR) was calculated by the Chronic Kidney Disease Epidemiology Collaboration equations (CKD-EPI) with the adjusted coefficient of 1.1 for the Asian population.14–16
Outcomes
The outcome of interest was incident eGFR of less than 60 mL/min/1.73m2 at 3 months.
Prediction Equation
The Nelson equation was developed to predict the 5-year risk of chronic kidney failure (CKD) from 34 multinational cohorts, including more than 5 million individuals. Given the effect of diabetes status on kidney function, the equations were calculated separately for participants with or without diabetes.7 The Nelson equation included age, sex, race, BMI, baseline eGFR, history of CVD and hypertension, smoking status, and urinary albumin/creatinine ratio (ACR). For patients with diabetes, the equation also included diabetes medication and HbA1c levels.
In this study, we compared the performance of the Nelson equation with that of the O’Seaghdha equation and the Chien equation. The O’Seaghdha equation was based on Framingham Heart Study to predict 10-year CKD risk, and consisted of age, diabetes status, baseline eGFR, history of hypertension, and ACR.9 The Chien equation was constructed to estimate CKD risk at 4 years from the National Taiwan University Hospital cohort, including diabetes status, BMI, SBP, and history of stroke.8 The specific formulas of all three prediction equations are shown in Table S1.
Statistical Analysis
Continuous variables were presented as medians with interquartile ranges or mean ± standard deviation and categorical variables as percentages. The characteristics of different groups were compared by Wilcoxon rank-sum test for the continuous variables and χ2 square statistics for the categorical variables. The discriminatory power of the risk prediction equation was assessed by the area under the receiver-operator curve (AUC) and 95% confidence intervals (CIs). The calibration was evaluated by Pearson correlation coefficient and Hosmer–Lemeshow test. The Delong test was used to compare the AUCs of different equations. Moreover, continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were determined to evaluate the incremental effect. Statistical significance was determined as p < 0.05, 2-sided. All statistical analyses were performed with SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Data Availability
Anonymized data are available to other researchers on request for replicating procedures or reproducing the results by directly contacting the corresponding author and their institutions.
Results
Study Participants and Characteristics
A total of 15,166 patients with AIS or TIA were enrolled in the CNSR-III. Upon exclusion of patients with incomplete data on eGFR on admission or at 3 months, HbA1c level at admission, ACR at admission, death at 3 months, or baseline eGFR less than 60 mL/min/1.73m2, a total of 3169 patients were included in the analysis, among which 1151 (36.3%) patients with diabetes and 2018 (63.7%) patients without diabetes (Figure 1). Compared with excluded patients, the eligible patients were younger, less severe at admission, had a lower proportion of stroke, higher BMI, SBP and eGFR, lower HbA1c level and ACR at baseline, more likely to be smokers and have a history of diabetes, less likely to have a history of atrial fibrillation (Table S2).
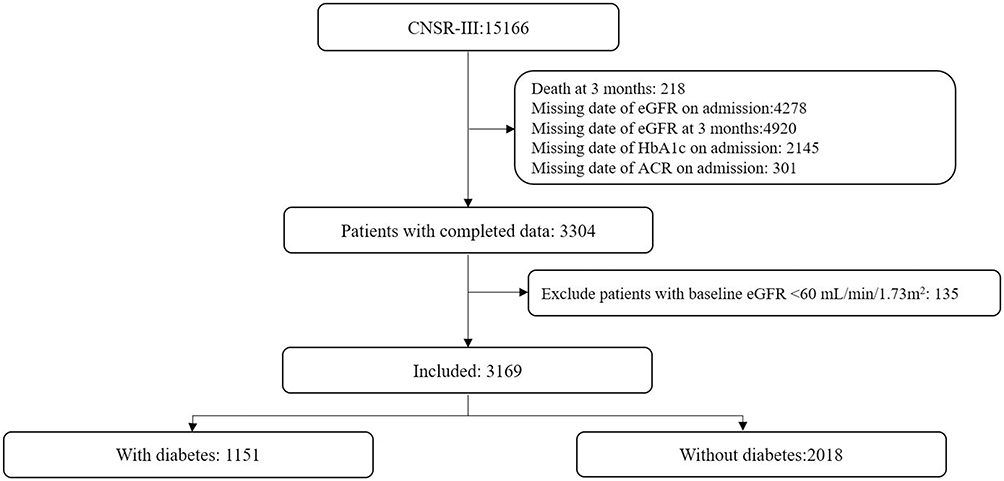 |
Figure 1 Flow chart of study population. Abbreviations: ACR, urinary albumin/creatinine ratio; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1. |
Table 1 shows the demographic and clinical characteristics of enrolled participants. Patients with diabetes were more likely to be female and suffer from ischemic stroke, coronary heart disease, hypertension, and hypercholesterolemia, less likely to be smokers and suffer from TIA and atrial fibrillation, had a higher proportion of large-artery atherosclerosis in TOAST classification, had higher BMI, eGFR, HbA1c level and ACR at baseline (Table 1).
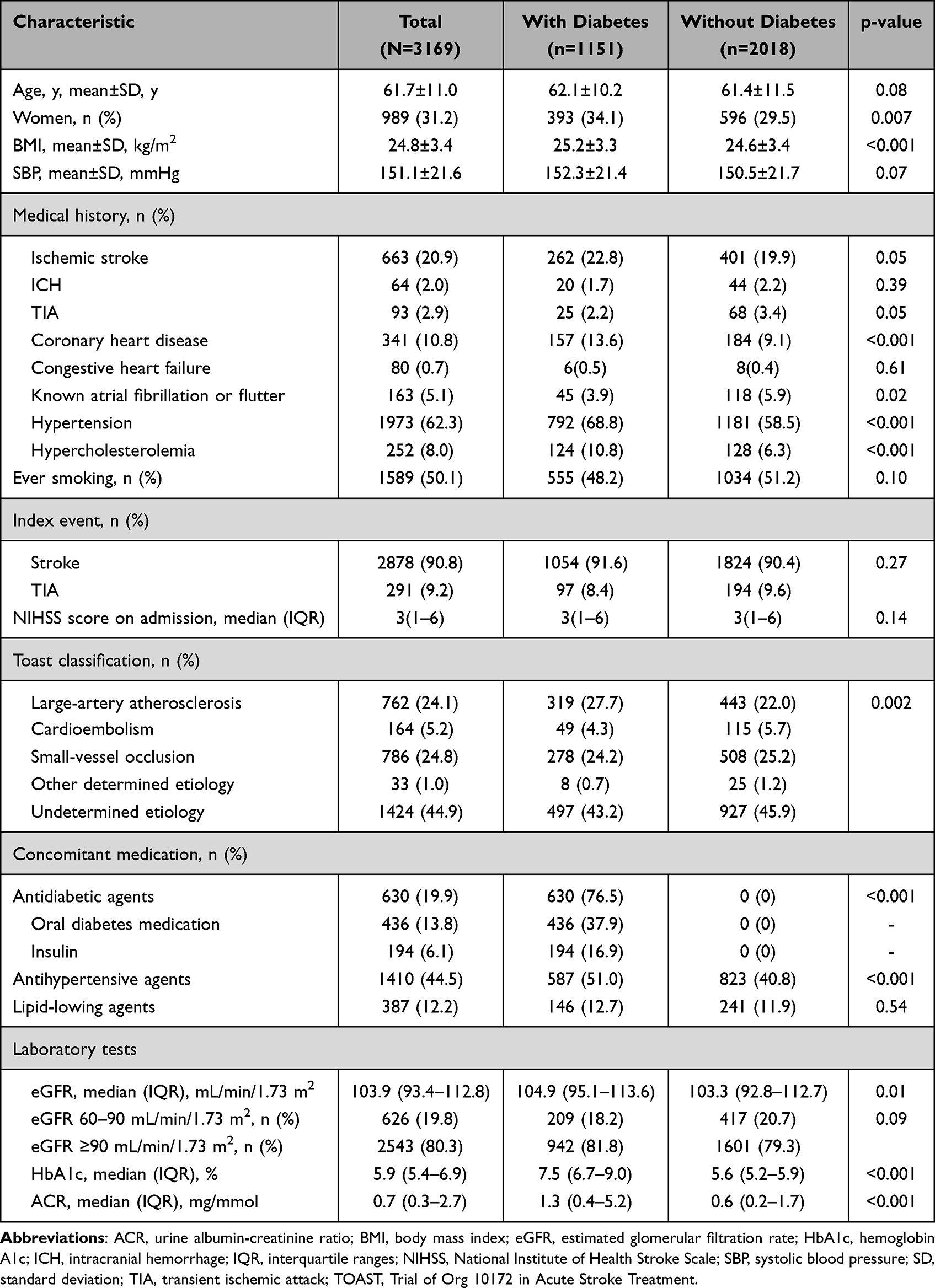 |
Table 1 Baseline Characteristics of the Patients with or Without Diabetes |
Among the patients who survived at 3 months, there were 31 incident cases (2.7%) of reduced eGFR observed in patients with diabetes, while 23 incident cases of reduced eGFR (1.1%) were reported in patients without diabetes (p = 0.001).
Prediction Performance
The prediction performance of each equation for the new-onset and long-term kidney function decline was assessed and compared by receiver operating characteristic (ROC) curve analysis (Table 2, Figure 2). For patients with diabetes, the AUC of the Nelson equation (0.82, 95% CI 0.72–0.93) was similar to the O’Seaghdha equation (0.82, 95% CI 0.75–0.89, p for comparison = 0.94) and the Chien equation (0.76, 95% CI 0.67–0.85, p for comparison = 0.28). For the patients without diabetes, the Nelson equation displayed a relatively higher prediction ability manifested as the maximum AUC (0.82, 95% CI 0.69–0.95). In comparison, the O’Seaghdha equation yielded an AUC of 0.78 (95% CI 0.68–0.88, p for comparison = 0.07), while the Chien equation exhibited a lower AUC of 0.68 (95% CI 0.57–0.79, p for comparison = 0.0006). Additionally, the cut-off value, sensitivity, and specificity for each equation were calculated, respectively (details shown in Table 2).
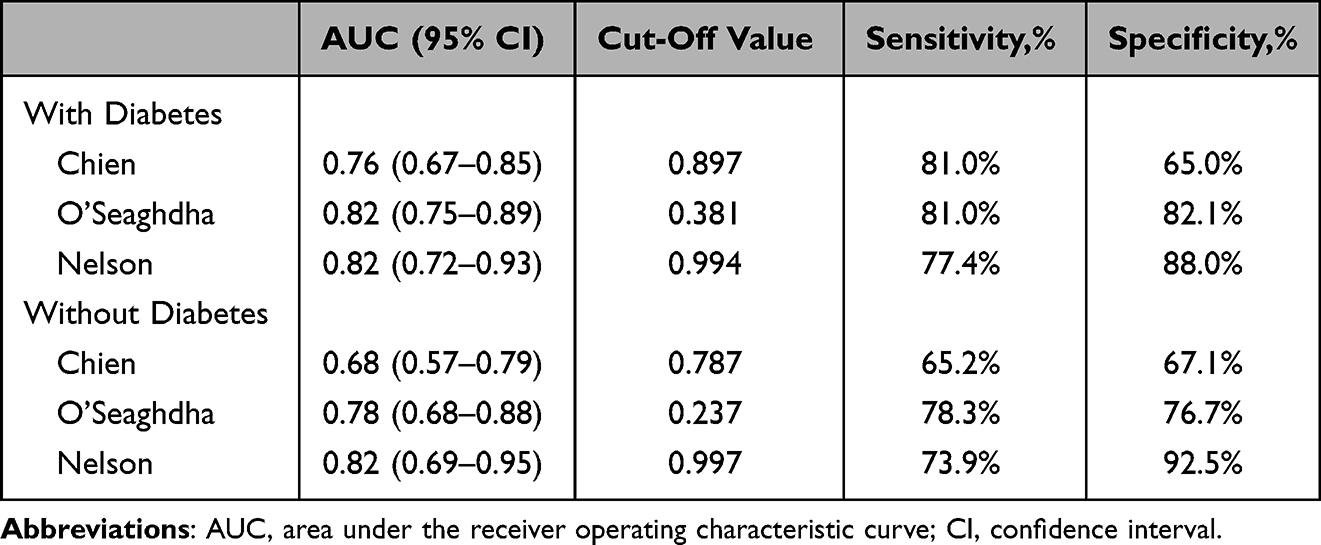 |
Table 2 Prediction Performance of the Nelson Equation, the O’Seaghdha Equation and the Chien Equation |
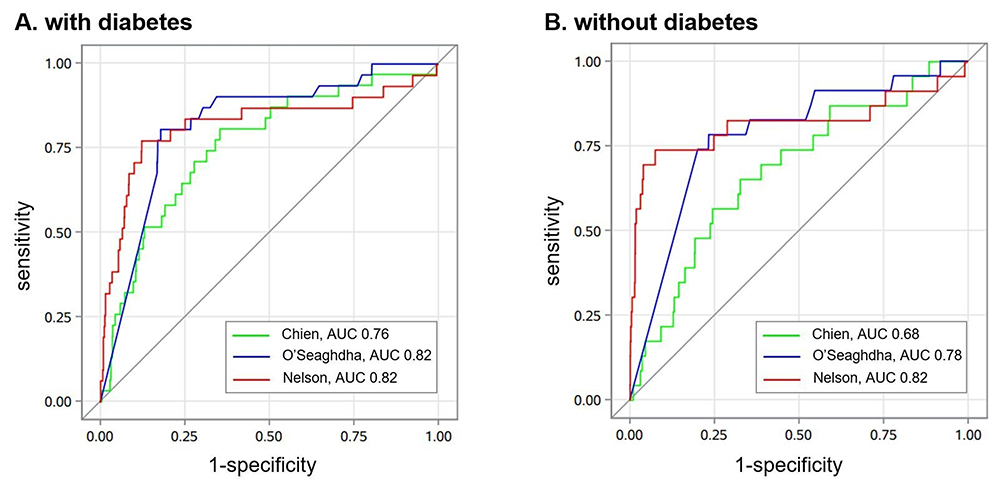 |
Figure 2 Receiver operating characteristic (ROC) curve analysis comparing the Nelson equation with other equations in patients with (A) or without (B) diabetes. Abbreviation: AUC, area under the receiver operating characteristic curve. |
Calibration Ability
Calibration analysis showed a high correlation between the predicted and observed probability of the new-onset and long-term kidney function decline, for the Nelson equation (diabetic r = 0.33, p < 0.0001; non-diabetic r = 0.36, p < 0.0001), the O’Seaghdha equation (diabetic r = 0.22, p < 0.0001; non-diabetic r = 0.14, p < 0.0001) and the Chien equation (diabetic r = 0.15, p < 0.0001; non-diabetic r = 0.07, p = 0.002).
The Hosmer-Lemeshow test was not significant with the Nelson equation in diabetic (p = 0.67) and in non-diabetic (p = 0.09), the O’Seaghdha equation in non-diabetic (p = 0.85), and the Chien equation in diabetic (p = 0.32) and in non-diabetic (p = 0.16), except for the O’Seaghdha equation in diabetic (p = 0.0003).
Incremental Effect
In patients with diabetes, although the AUC of the Nelson equation was not significantly increased (p = 0.28), the continuous NRI (0.64, 95% CI 0.31–0.96, p = 0.0004) and IDI (0.10, 95% CI 0.05–0.15, p < 0.0001) in comparision with the Chien equation was statistically significant. Meanwhile, in patients without diabetes, the Nelson equation exhibited the significant enhancement (p = 0.0006), as the continuous NRI (1.13, 95% CI 0.75–1.50, p < 0.0001) and IDI (0.13, 95% CI 0.07–0.18, p < 0.0001) to the Chien equation (Table 3).
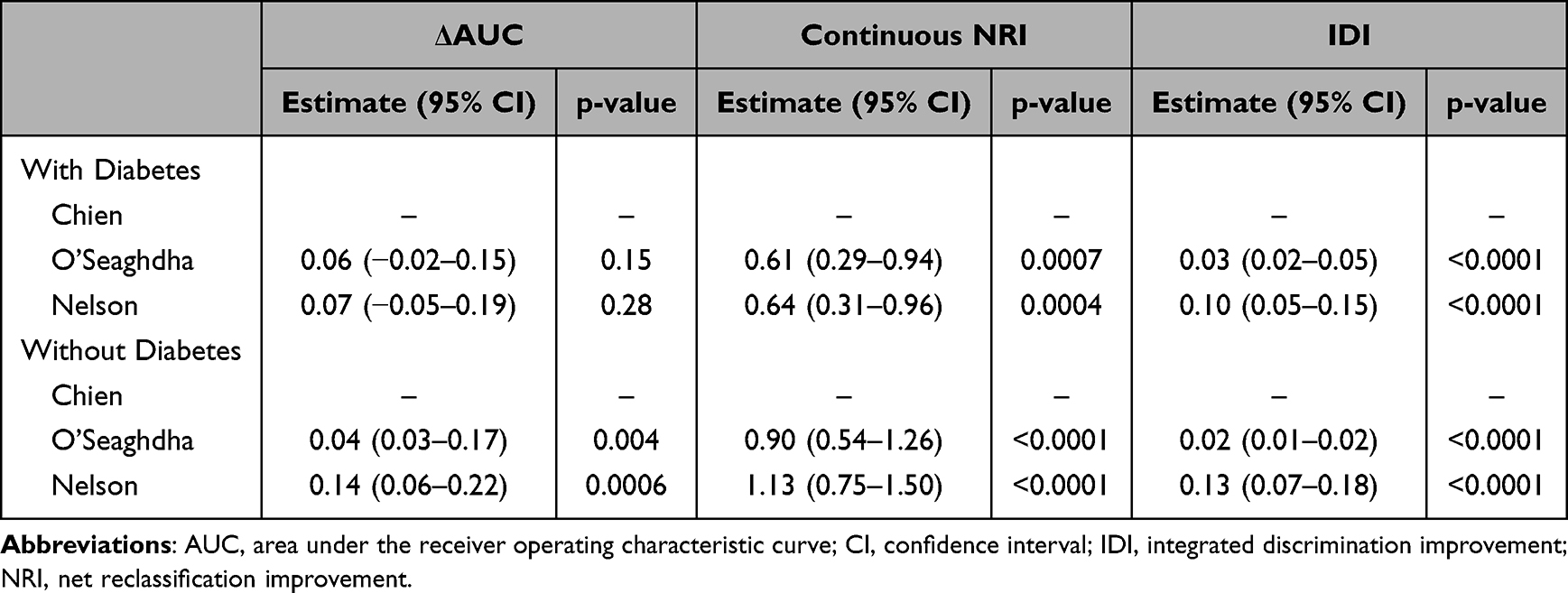 |
Table 3 Incremental Ability of Various Equation on the Prediction of the New-Onset and Long-Term Kidney Function Decline |
Discussion
In this study, we found that a few patients had a new-onset and long-term kidney function decline after AIS or TIA. It is the first study to report the external validation of the kidney dysfunction prediction equations in patients with acute ischemic cerebrovascular disease. The Nelson equation demonstrated high discrimination and variable calibration in predicting the risk of the new-onset and long-term kidney function decline after AIS or TIA, and has an improvement in other prediction models.
Previous studies clarified that 29.7% of patients were diagnosed with CKD among 3-mo survivors after AIS or TIA, whose eGFR was less than 60 mL/min/1.73m2 last 3 months, and 7.2% of patients recovered from the baseline kidney dysfunction.17 In light of our study findings, which indicated that 1.7% of patients experienced a new-onset and long-term decline in kidney function, the kidney injury and recovery processes after stroke were dynamic. Indeed, both pre-existing and post-stroke kidney diseases exacerbate the pathological progression of stroke, limit access to essential therapeutics, and adversely impact the recovery outcomes of stroke patients.5,18–20 An accurate prediction tool to identify patients at risk of kidney function decline would assist clinicians in implementing targeted preventative measures and determining the appropriate frequency of kidney health monitoring.
Our study identified that the prediction efficiency of the Nelson equations in patients with stroke is equivalent to that in the community population (diabetic, AUC, 0.82 vs 0.80; non-diabetic, AUC, 0.82 vs 0.85).7 Furthermore, considering the complex interplay between the brain and kidney, specific modifiable or preventable risk factors for kidney function decline in stroke patients may exist that differ from those in the community cohort. Namely, recent literature has demonstrated that some biomarkers, including proteinuria and urinary liver-type fatty-acid binding protein, could predict kidney function decline after stroke independently.21,22 Intensive blood pressure lowering increases the possibility of kidney function decline.23 Drugs play a double-edged role in kidney injury after stroke, as mannitol exacerbates the damage and edaravone prevents the function.24,25 Surprisingly, there was no significant correlation between acute kidney injury and computed tomography angiography, intravascular therapy and intravenous thrombolysis.26–28 Further investigations on the association between kidney dysfunction and risk factors are warranted to diminish the prevalence of kidney function decline, aid in selecting suitable therapeutic interventions, and circumvent the inadvertent dismissal of critical treatments stemming from preconceptions.
Some pathological mechanisms might partly mediate the brain-kidney interaction following stroke. Inflammation and immune responses controlled by the spleen play a central role in kidney dysfunction after stroke, including C-reactive protein, interleukin-6, reactive oxygen species and matrix metalloproteinase-9.29–33 The central autonomic network might influence kidney injury through the sympathetic nervous system, hypothalamic-pituitary-adrenal axis and renin-angiotensin-aldosterone system.34–36 Besides, miRs and extracellular vesicles, such as microparticles and exosomes, are likely mediators of kidney dysfunction after stroke.37–39 More depth research on the brain-kidney cross-talk might promote the discovery of new therapeutic targets, further improving the clinical prognosis and reducing complications.
Our study has some limitations. First, our study only included baseline and 3-month eGFR. Given the constraints of our study design, we were unable to ascertain the precise timing of initial eGFR decline or determine the duration of kidney function decline. Second, given the missing data in our cohort, there may be selection bias in the included population. Third, none of the three prediction equations included imaging features and other biomarkers that might be associated with impaired renal function, such as uric acid and cerebral microbleeds.28,40
Conclusions
The present study indicated that the Nelson equation is of high predictive value for the new-onset and long-term kidney function decline in patients with AIS or TIA, which could help clinicians screen high-risk patients, determine the frequency of kidney health monitoring, facilitate efforts to take targeted management and treatment in time, and improve stroke prognosis.
Ethics Approval
The ethics committee at Beijing Tiantan Hospital, with IRB approval number KY2015-001-01, along with all participating study centers, provided ethical approval for the study protocol.
Consent to Participate
All participants or their legal proxies provided written informed consent.
Acknowledgments
We appreciate the staff and participants of CNSR-III studies for their contributions.
Funding
This study was supported by grants from the Capital’s Funds for Health Improvement and Research (2020-1-2041), the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), and the National Natural Science Foundation of China (81870905, U20A20358).
Disclosure
The authors declare that they do not have a conflict of interest.
References
1. Zhao Q, Yan T, Chopp M, et al. Brain-kidney interaction: renal dysfunction following ischemic stroke. J Cereb Blood Flow Metab. 2020;40(2):246–262. doi:10.1177/0271678X19890931
2. Wang D, Liu M, Hao Z, et al. Association between reduced kidney function and clinical outcomes after ischaemic stroke with atrial fibrillation. Eur J Neurol. 2014;21(1):160–166. doi:10.1111/ene.12293
3. Wu VC, Wu PC, Wu CH, et al. The impact of acute kidney injury on the long-term risk of stroke. J Am Heart Assoc. 2014;3:e000933. doi:10.1161/JAHA.114.000933
4. Zorrilla-Vaca A, Ziai W, Connolly ES, et al. Acute kidney injury following acute ischemic stroke and intracerebral hemorrhage: a meta-analysis of prevalence rate and mortality risk. Cerebrovasc Dis. 2018;45(1–2):1–9. doi:10.1159/000479338
5. Tsagalis G, Akrivos T, Alevizaki M, et al. Long-term prognosis of acute kidney injury after first acute stroke. Clin J Am Soc Nephrol. 2009;4(3):616–622. doi:10.2215/CJN.04110808
6. Tummalapalli SL, Estrella MM. Predicting risk of kidney disease: is risk-based kidney care on the horizon? JAMA. 2019;322(21):2079–2081. doi:10.1001/jama.2019.17378
7. Nelson RG, Grams ME, Ballew SH, et al. Development of risk prediction equations for incident chronic kidney disease. JAMA. 2019;322(21):2104–2114. doi:10.1001/jama.2019.17379
8. Chien KL, Lin HJ, Lee BC, et al. A prediction model for the risk of incident chronic kidney disease. Am J Med. 2010;123(9):836–846.e832. doi:10.1016/j.amjmed.2010.05.010
9. O’Seaghdha CM, Lyass A, Massaro JM, et al. A risk score for chronic kidney disease in the general population. Am J Med. 2012;125(3):270–277. doi:10.1016/j.amjmed.2011.09.009
10. Wang Y, Jing J, Meng X, et al. The Third China National Stroke Registry (CNSR-III) for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics. Stroke Vasc Neurol. 2019;4(3):158–164. doi:10.1136/svn-2019-000242
11. Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24:35–41. doi:10.1161/01.STR.24.1.35
12. Draznin B, Aroda VR, Bakris G, et al. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45:S17–S38.
13. Carey RM, Wright JT, Taler SJ, et al. Guideline-driven management of hypertension: an evidence-based update. Circ Res. 2021;128(7):827–846. doi:10.1161/CIRCRESAHA.121.318083
14. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
15. Luo Y, Wang X, Wang Y, et al. Association of glomerular filtration rate with outcomes of acute stroke in type 2 diabetic patients: results from the China National Stroke Registry. Diabetes Care. 2014;37:173–179. doi:10.2337/dc13-1931
16. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713–735. doi:10.1053/j.ajkd.2014.01.416
17. Hayden D, McCarthy C, Akijian L, et al. Renal dysfunction and chronic kidney disease in ischemic stroke and transient ischemic attack: a population-based study. Int J Stroke. 2017;12(7):761–769. doi:10.1177/1747493017701148
18. Putaala J, Haapaniemi E, Gordin D, et al. Factors associated with impaired kidney function and its impact on long-term outcome in young ischemic stroke. Stroke. 2011;42(9):2459–2464. doi:10.1161/STROKEAHA.110.612721
19. Fandler-Höfler S, Odler B, Kneihsl M, et al. Acute and chronic kidney dysfunction and outcome after stroke thrombectomy. Transl Stroke Res. 2021;12(5):791–798. doi:10.1007/s12975-020-00881-2
20. Kelly DAO, Li L, Burgess AI, et al. Associations of blood biomarkers with glomerular filtration rate in patients with TIA and stroke: population-based study. Stroke Vasc Neurol. 2021;6(1):48–56. doi:10.1136/svn-2020-000422
21. Shimoyama T, Sato T, Sakamoto Y, et al. Urinary biomarkers of kidney tubule injury, risk of acute kidney injury, and mortality in patients with acute ischaemic stroke treated at a stroke care unit. Eur J Neurol. 2020;27(12):2463–2472. doi:10.1111/ene.14448
22. Tao Y, Dong W, Li Z, et al. Proteinuria as an independent risk factor for contrast-induced acute kidney injury and mortality in patients with stroke undergoing cerebral angiography. J Neurointerv Surg. 2017;9:445–448. doi:10.1136/neurintsurg-2016-012349
23. Ikeme JC, Pergola PE, Scherzer R, et al. Cerebral white matter hyperintensities, kidney function decline, and recurrent stroke after intensive blood pressure lowering: results from the secondary prevention of small subcortical strokes (SPS 3) trial. J Am Heart Assoc. 2019;8:e010091. doi:10.1161/JAHA.118.010091
24. Lin SY, Tang SC, Tsai LK, et al. Incidence and risk factors for acute kidney injury following mannitol infusion in patients with acute stroke: a retrospective cohort study. Medicine. 2015;94:e2032. doi:10.1097/MD.0000000000002032
25. Kamouchi M, Sakai H, Kiyohara Y, et al. Acute kidney injury and edaravone in acute ischemic stroke: the Fukuoka Stroke Registry. J Stroke Cerebrovasc Dis. 2013;22(8):e470–e476. doi:10.1016/j.jstrokecerebrovasdis.2013.05.018
26. Qureshi AI, Aslam H, Zafar W, et al. Acute kidney injury in acute ischemic stroke patients in clinical trials. Crit Care Med. 2020;48:1334–1339. doi:10.1097/CCM.0000000000004464
27. Demel SL, Grossman AW, Khoury JC, et al. Association between acute kidney disease and intravenous dye administration in patients with acute stroke: a population-based study. Stroke. 2017;48:835–839. doi:10.1161/STROKEAHA.116.014603
28. Gadalean F, Simu M, Parv F, et al. The impact of acute kidney injury on in-hospital mortality in acute ischemic stroke patients undergoing intravenous thrombolysis. PLoS One. 2017;12:e0185589. doi:10.1371/journal.pone.0185589
29. Stuveling EM, Hillege HL, Bakker SJ, et al. C-reactive protein is associated with renal function abnormalities in a non-diabetic population. Kidney Int. 2003;63(2):654–661. doi:10.1046/j.1523-1755.2003.00762.x
30. Wang HR, Chen DL, Zhao M, et al. C-reactive protein induces interleukin-6 and thrombospondin-1 protein and mRNA expression through activation of nuclear factor-ĸB in HK-2 cells. Kidney Blood Press Res. 2012;35:211–219. doi:10.1159/000332402
31. Lee BT, Ahmed FA, Hamm LL, et al. Association of C-reactive protein, tumor necrosis factor-alpha, and interleukin-6 with chronic kidney disease. BMC Nephrol. 2015;16:77. doi:10.1186/s12882-015-0068-7
32. Rhyu DY, Yang Y, Ha H, et al. Role of reactive oxygen species in TGF-beta1-induced mitogen-activated protein kinase activation and epithelial-mesenchymal transition in renal tubular epithelial cells. J Am Soc Nephrol. 2005;16:667–675. doi:10.1681/ASN.2004050425
33. Tan RJ, Liu Y. Matrix metalloproteinases in kidney homeostasis and diseases. Am J Physiol Renal Physiol. 2012;302:F1351–F1361. doi:10.1152/ajprenal.00037.2012
34. Krowicki ZK, Kapusta DR. Microinjection of glycine into the hypothalamic paraventricular nucleus produces diuresis, natriuresis, and inhibition of central sympathetic outflow. J Pharmacol Exp Ther. 2011;337:247–255. doi:10.1124/jpet.110.175398
35. Mracsko E, Liesz A, Karcher S, et al. Differential effects of sympathetic nervous system and hypothalamic-pituitary-adrenal axis on systemic immune cells after severe experimental stroke. Brain Behav Immun. 2014;41:200–209. doi:10.1016/j.bbi.2014.05.015
36. Zhang W, Wang W, Yu H, et al. Interleukin 6 underlies angiotensin II-induced hypertension and chronic renal damage. Hypertension. 2012;59:136–144. doi:10.1161/HYPERTENSIONAHA.111.173328
37. Puddu P, Puddu GM, Cravero E, et al. The involvement of circulating microparticles in inflammation, coagulation and cardiovascular diseases. Can J Cardiol. 2010;26(4):140–145. doi:10.1016/S0828-282X(10)70371-8
38. Venkat P, Chen J, Chopp M. Exosome-mediated amplification of endogenous brain repair mechanisms and brain and systemic organ interaction in modulating neurological outcome after stroke. J Cereb Blood Flow Metab. 2018;38:2165–2178. doi:10.1177/0271678X18782789
39. Zhang W, Zhou X, Zhang H, et al. Extracellular vesicles in diagnosis and therapy of kidney diseases. Am J Physiol Renal Physiol. 2016;311(5):F844–F851. doi:10.1152/ajprenal.00429.2016
40. van Overbeek EC, Staals J, van Oostenbrugge RJ. Decreased kidney function relates to progression of cerebral microbleeds in lacunar stroke patients. Int J Stroke. 2016;11(6):695–700. doi:10.1177/1747493016641966
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sex Differences in Stroke Risk Factors, Clinical Profiles, and In-Hospital Outcomes Among Stroke Patients Admitted to the Medical Ward of Dessie Comprehensive Specialized Hospital, Northeast Ethiopia
Abdu H, Seyoum G
Degenerative Neurological and Neuromuscular Disease 2022, 12:133-144
Published Date: 21 October 2022
Risk Factors and Prognosis of Carbapenem-Resistant Organism Colonization and Infection in Acute Cholangitis
Li K, Jiang S, Fu H, Hao Y, Tian S, Zhou F
Infection and Drug Resistance 2022, 15:7777-7787
Published Date: 28 December 2022
Prognostic Factors of Adrenocortical Carcinoma: Experience from a Regional Medical Center in Eastern China
Li P, Su X, Zhang X, Sun L, Zhang G
International Journal of General Medicine 2023, 16:453-465
Published Date: 3 February 2023
Analysis of Pathogenic Bacteria Distribution and Related Factors in Recurrent Acute Cholangitis
Li K, Hu X, Lu Q, Zhang H, Zhou J, Tian S, Zhou F
Infection and Drug Resistance 2023, 16:4729-4740
Published Date: 20 July 2023
Knowledge of Cardiovascular Disease Risk Factors and Its Primary Prevention Practices Among the Saudi Public – A Questionnaire-Based Cross-Sectional Study
Bashatah A, Syed W, Al-Rawi MBA
International Journal of General Medicine 2023, 16:4745-4756
Published Date: 20 October 2023