")
Back to Journals » International Journal of General Medicine » Volume 16
Navigating the Knowledge of Risk Factors, Warning Signs, of Stroke - A Community-Based Cross-Sectional Study Among Saudi Adults in Riyadh Saudi Arabia
Authors Syed W , AlHarbi AA, Samarkandi OA, Alobaid AM, Alsulaihim IN
Received 14 September 2023
Accepted for publication 1 December 2023
Published 12 December 2023 Volume 2023:16 Pages 5869—5883
DOI https://doi.org/10.2147/IJGM.S437941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wajid Syed,1 Asma Awadh AlHarbi,2 Osama A Samarkandi,3 Abdullah M Alobaid,4 Ibrahim Nasser Alsulaihim5
1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia; 2Department of Nursing, College of Nursing King Saud University, Riyadh, 11451, Saudi Arabia; 3Department of Basic Sciences, Prince Sultan College for Emergency Medical Services, King Saud University, Riyadh, 11466, Saudi Arabia; 4Department of Accident and Trauma, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh,Saudi Arabia; 5Department of Pharmacology and Toxicology, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Wajid Syed, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia, Email [email protected]
Background: The incidence of stroke is increasing in everyday life as a result of modifiable cerebrovascular risk factors and aging. Therefore, the goal of this study was to assess knowledge of the risk factors, and warning signs, of stroke and to determine associated demographic factors among individuals living in Riyadh, Saudi Arabia.
Methods and Materials: A cross-sectional online study using a convenience sampling of general population living in Riyadh was carried out over three months in 2023 using a series of questionnaires that was adopted from the previous study. Before data collection, the study tool was subjected to pilot testing among a small sample of individuals to validate for consistency and reliability. The data was collected using social media platforms. A statistical package for the social science (SPSS version 27) was used.
Results: Four hundred and sixty-two individuals completed the survey. Among those 69.5%, identified hypertension as a risk factor for stroke followed by hyperlipidemia (42.9%), heart disease (44.8%). In addition, most of the respondents (n = 332, 71.9%) knew that numbness or weakness of the face and/or limbs of the body was a warning sign of stroke. In this, 73.5% (n=249) of the respondents agreed that if they saw an individual suffering from a stroke, they would like to take the patient to the hospital immediately. However, there was a significant association between the knowledge of the respondents about the risk factor of stroke and educational degree (p=0.011), and parents working in healthcare settings (p =0.015).
Conclusion: In conclusion it was observed that a significant respondents had an adequate knowledge of stroke risk factors, while most were unaware of the early warning signs of a stroke. To promote primary prevention and early management/outcomes, we advise that future regional campaigns focus on raising knowledge and recognition of stroke symptoms.
Keywords: risk factors, hypertension, warning signs, treatment, stroke, sedentary life style
Introduction
A stroke is a serious clinical condition of rapidly manifesting symptoms of a focal neurological impairment in the brain function that lasts >24 hours or may even result in death and of presumed vascular origin.1 In other words, stroke occurs when anything prevents a part of the brain from receiving blood or when an artery in the brain bursts or blocks.2,3 Estimates of stroke may vary by country and by year. For instance, according to the 2022 Global Stroke Factsheet, the lifetime risk of having a stroke has increased by 50% over the previous 17 years, with an estimated 1 in 4 persons expected to experience a stroke in their lifetime.4 On the other hand, another recent study predicted that by the year 2030, the age-standardized incidence rate of ischemic stroke would rise to 89.32 per 100,000 people worldwide.5 In Saudi Arabia, a prevalence of 7.3 million stroke cases was reported in the Middle East and North Africa region (MENA) region in 2019,6 while another systematic review and meta-analysis of stroke incidence among the Saudi population reported that there are 29 stroke cases for every 100,000 people annually for individuals residing Saudi Arabia.7
The human brain is a complex and essential organ that regulates numerous bodily functions, including thinking, memory retention, emotion, appetite, and many others.2 When the brain receives insufficient blood or when something blocks oxygen-rich blood from accessing the brain, brain cells begin to die within minutes, resulting in a stroke.2 All areas of the brain receive blood rich in oxygen from the arteries, which provides the oxygen the brain needs to function effectively and sufficiently.2 There are two primary types of strokes: ischemic strokes, which are more prevalent, are caused by blood clots that obstruct blood veins in the brain.8 In contrast, hemorrhagic strokes occur when a brain artery bursts or leaks blood.8 A transient ischemic attack (TIA), which is regarded as a tiny stroke and lasts no longer than five minutes, happens when the blood flow to the brain is momentarily stopped.9 On the other hand, a TIA is seen as a precursor to a future stroke, and it is estimated that more than one-third of TIA sufferers globally who do not receive treatment at the time go on to have a severe stroke within a year.9 The most common risk factors for stroke were diabetes, hypertension, atrial fibrillation, smoking, binge drinking, abusing drugs, and being sedentary especially inactivity.3,10,11 On the other hand, the most commonly identified warning signs of the stroke include loss of balance, dizziness, and difficulty speaking, followed by slurred speech.3 The World Stroke Association adopted the acronym FAST to distinguish four stroke warning symptoms, where the letters “F” stand for the face, “A” for the arm, “S” for speech, and “T” for time.12,13
In addition, the literature suggested that stroke is more prevalent among the elderly aged between 15–49 years with 47% of incidence in men and 53% of them in women.14 The burden of stroke is substantial, but it can be largely prevented because numerous risk factors are known to be modifiable. The Saudi Public Health Authority, with assistance from the World Bank Group, has done initiatives for the prevention of public health burden by, offering the strategic direction required to reduce both the health and economic impact of disorders, such as CVD, so that life expectancy can be increased15 However, this is only possible if people are aware of these factors. Additionally, because many treatment options depend on time, early detection and hospital presentation are crucial for minimizing death and disability. To obtain an appropriate diagnosis and course of therapy, it is necessary to be aware of the condition and its symptoms. Posing sufficient knowledge regarding the illness may also be beneficial to them if they or their families come into real phenomena.3,16,17 Many studies have shown that people’s failure to recognize the early warning signs and symptoms of a stroke delays the hospitalization of stroke patients.16,17 There have been several reports published previously from around the world to study the prevalence and incidence of strokes.10,11,13,14,17 Although those earlier studies were published in different population.13,16 As per our knowledge, no such research has been conducted so far among the Saudi population to examine the knowledge of stroke warning signs and risk factors among the Saudi population. Therefore, the goal of this study was to assess knowledge of the risk factors, and warning signs, of stroke and to determine associated demographic factors among individuals living in Riyadh, Saudi Arabia.
Methods
Study Design, Population, and Respondents’ Recruitment
A cross-sectional online survey was conducted between June and August 2023, using electronic questionnaires. Any individual who is currently residing in Riyadh, Saudi Arabia, and is at least 20 years old made up the study’s population. The questionnaire link was disseminated via social media websites. The study sample followed a convenience sampling technique. The aims and inclusion criteria for the study were described in the cover letter, and the beginning of the study questionnaires. Other than Saudi citizens, those who lived other countries and gave partial answers to the questionnaires were not included in the study. Furthermore, before carrying out the study the study protocol and questionnaires were reviewed and approved by the ethics committee at the College of Medicine, King Saud University, Riyadh, Saudi Arabia (IRB Project No. E-23-8115). In addition, informed consent was obtained from the participants, before completing the questionnaires. This study followed the guidelines outlined in the Declaration of Helsinki, for the research involves humans.
Sample Size
Similar to many studies18–26 the sample size was calculated using the Raosoft sample size calculator by considering the 2023 Riyadh population (n= 7,682,430)27 of Saudi Arabia, at a 5% margin of error (ME) and 95% confidence interval (CI), the required sample size for this study was calculated to be 385. To account for nonresponse and reduce any data collection error, the projected sample size was further raised to 500. Thus, n= 500 individuals were included in this study.
Questionnaire
This study included a questionnaire to assess the study respondents’ current level of knowledge of stroke risk factors, warning symptoms, and associated factors. To fulfill the objectives of the study, a questionnaire was developed from a previously published study (Appendix 1).3,13,16 The respondents’ knowledge of stroke was evaluated, including their comprehension of its risk factors, warning indications, early treatment options, and information sources. Age, sex, education level, occupation, and other demographic data about the respondents were gathered in the questionnaire’s first section. Additionally, the respondents were questioned in this area regarding the purpose and window of thrombolysis. Using 19 questions in a three-point scale (Yes /No/I do not know) style, the respondents’ knowledge of risk factors and warning signs was assessed, and the fourth component covers information sources for managing a stroke assessed using multiple choice answers.
The original survey was written in English. We used the forward and backward translational techniques to translate the survey into Arabic. Instead of translating words by word, this translation method used conceptual translation. Two experienced healthcare experts and academics reviewed the Arabic form of the questionnaire for clarity and comprehensibility and concluded that respondents would not have any trouble understanding it. The questionnaire was then pretested on 20 individuals who were eventually dropped from the study population. Respondents were questioned about the questionnaire’s readability and clarity as well as whether any of the questions were difficult to comprehend. Utilizing Cronbach’s alpha, data were used to evaluate the reliability of internal consistency. The results showed adequate internal consistency reliability for the risk factor knowledge and warning signs questionnaires (with Cronbach’s alpha = 0.72).
The data was gathered under the direction of a senior researcher from the College of Pharmacy through the use of online questionnaires using a convincing sampling technique. First, an invitation link comprising electronic questions was delivered to the participants via social media, which served as the primary platform. The questionnaires were limited to Saudi citizens; non-residents were not permitted to respond to them. We also gave the surveys to friends and coworkers and advised them to send or bring referrals to the study to increase the response rate (snowball technique).
The risk factors and warning signs knowledge scores were calculated. Each right response received a score of “one”, while each incorrect response received a score of “zero” to calculate the knowledge scores for risk factors. Each of the twelve knowledge surveys was computed to determine the overall knowledge score for the risk variables. Moreover, the total knowledge score was split into two categories: good, who received more than 50% of the total score, and poor, who received less than 50% of the whole score. The same concept was used to gauge people’s Knowledge of stroke warning signs.
Analysis
Descriptive statistics such as frequency (n) and percentages (%) were used to describe the respondent’s demographic information. Continuous data were described using the mean (M) and standard deviation (Std). To find out the association between variables Chi-square or Fisher exact test, a p-value of <0.05 was used to establish the statistical significance difference between the variables. The data were analyzed using the Statistical Package for Social Science (SPSS) version 27.
Results
Four hundred and sixty-two individuals completed the survey. Most of them were aged between 20–24 years (n=133, 28.8%), and were Saudi nationals (98.3%). More than half of the respondents (56.9%) had a university level of education while most of the respondents were employed (46.3%) respectively. Nearly two-thirds of respondent’s parents will not work in a healthcare setting. Most of the respondents (n=396, 85.7%) knew A stroke or brain attack happens when blood flow to your brain is stopped. In addition, 79.9% of the respondents thought that a stroke affects the ability to move eat, and other body functions. Furthermore, 23.4% of the respondents answered that 0–4.5 hours was the window period of thrombolysis, while 28.4% of the respondents believed that 4.5–6 hours’ respondents’ demographic characteristics and professional information are summarized in Table 1.
 |
Table 1 Socio-Demographic Characteristics and Some Basic Knowledge of the Study Respondents Towards Stroke (n=462) |
The respondents’ awareness of stroke risk factors is shown in Table 2. The “most recognized” risk factors of stroke, according to respondents, were drinking alcohol (77.3%), having high blood pressure (69.5%), having had a stroke in the past (n=292; 63.2%), smoking (56.5%), slightly more than half of respondents 236 (51.1%) also believed that being sedentary, and taking birth control pills (45.2%), having hyperlipidemia (42.9%), having heart disease (44.8%), or are risk factors for stroke.
 |
Table 2 Respondents Knowledge of Risk Factors of Strokes (n=462) |
We examined respondent’s knowledge of stroke warning signs in the third component of the survey. The “most recognized” warning signs of stroke were numbness or weakness in the face or limbs of the body (n = 332, 71.9%), followed by severe headaches of unclear origin 302 (65.4%) and blurred vision (n = 293, 63.4%). Additionally, 27.3% (n=126) of the respondents believed that heart palpitations or chest pain is a warning sign of stroke. However, fewer than half of respondents (n=214; 46.3%) believed that difficulty in speaking and understanding. Table 3 summarizes respondents’ understanding of the “most recognized” warning signs of stroke.
 |
Table 3 Respondents’ Knowledge of Warning Signs of Stroke |
In this study majority (n=249; 73.5%) of the respondents agreed that if they saw individual suffering from stroke, they would like to take the patient to hospital immediately, while 64.9% (n=2020) of them revealed that they will call to ambulance, 6.8% (n=23) revealed to give home remedies, 1.8% (n=6) like to give painkillers to control the pain and 123 (26.6%) of the respondents answered that they do not know what to do in that situation as shown in Figure 1. With regards to the source of information for the stroke, the majority of them revealed physicians, (n=265;78.2%), followed by relatives or friends (n=232; 68.4%), textbooks and internet (n=227; 67%), pharmacists (n=162; 47.8%) and Nurse (n=61; 18%) as shown in Figure 2.
 |
Figure 1 What the respondents should do when they observe a stroke patient (More than one answer able to be selected). |
 |
Figure 2 Source of information for the stroke (More than one answer able to be selected). |
There was no significant difference between respondents’ knowledge, about the window period of thrombolysis and occupation (p = 0.427), (Figure 3a). Similarly, 12.5% (n=58) of the male respondents identified 0–4.5 hours as the window period for the thrombolysis, while 10.8% (n=50) of the female-identified correctly (p = 0.005). However, there indicated no significant association between gender and the window period of thrombolysis as shown in Figure 3b. In addition, there was a significant association between education and knowledge of thrombolysis, for example, respondents with university degrees answered more correctly than other education, indicating a significant difference between them (p = 0.001) as shown in Figure 3c.
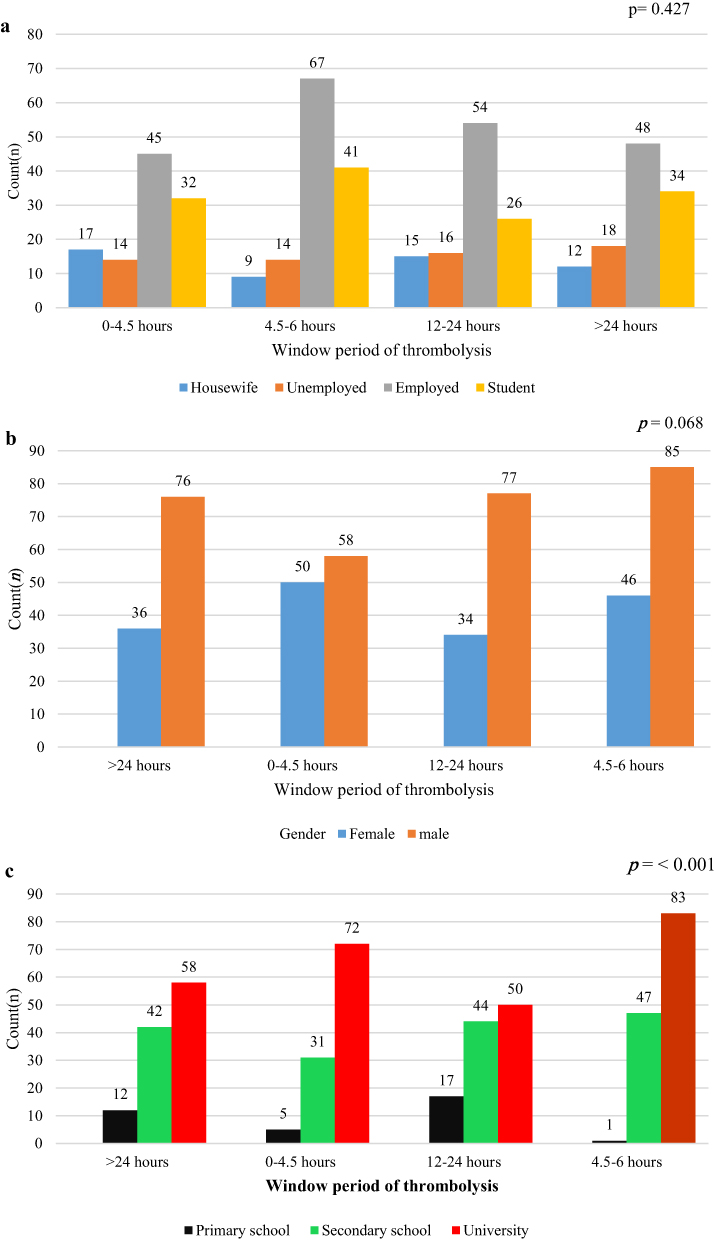 |
Figure 3 (a) Window period of thrombolysis according to gender. (b) Window period of thrombolysis according to education. (c) Window period of thrombolysis according to occupation. |
Furthermore, the findings of this study revealed a significant difference regarding age group and source of information for the stroke, for instances individuals aged between 20–30 years were preferred to textbooks and internet as the main source of information for their stroke (Figure 4) comparing to other age groups, indicating statistically significant difference (p=0.001) (Figure 4).
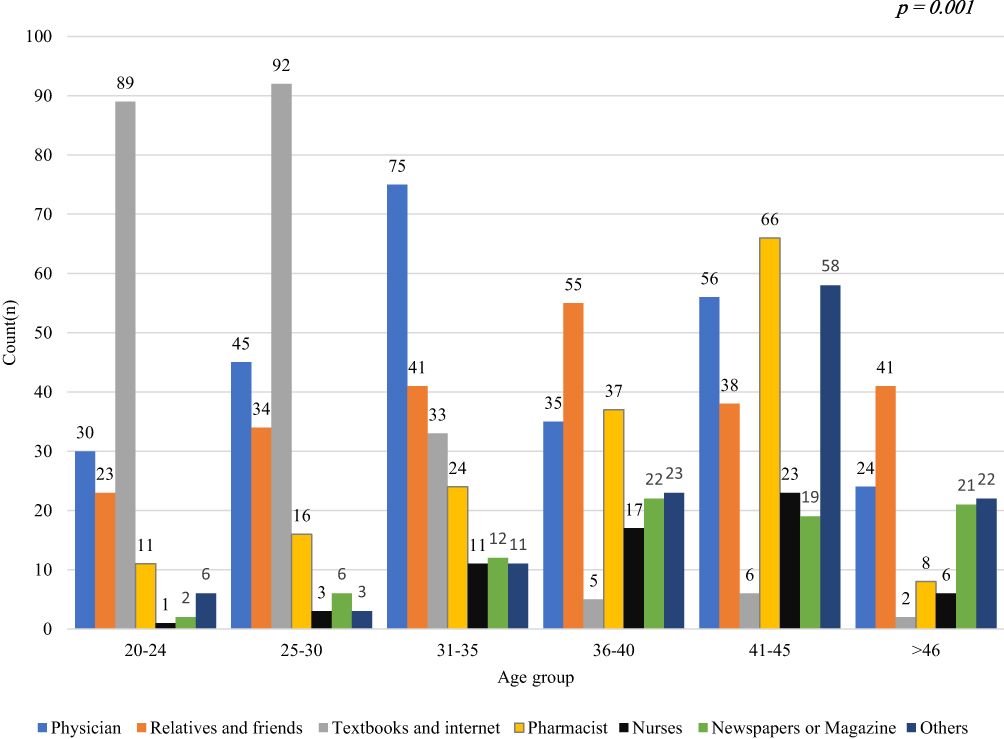 |
Figure 4 Source of information for the stroke according to age group. |
Table 4 displays the statistically significant difference between the respondents’ knowledge scores of stroke risk factors and their demographic variables. Gender (p=0.428) age (p = 0.064) and knowledge score of stroke risk factors were not significantly associated. Similarly, there was no significant difference between respondents’ knowledge score of occupation and the risk factor for stroke (p = 0.895). As indicated in Table 4, there was a significant difference between respondents’ knowledge of the risk factor for stroke and educational level (p = 0.011) and parents who worked in healthcare settings (p = 0.015). Similarly, the Table 5 illustrates the relationship between demographic characteristics and knowledge of stroke warning signs. According to the data presented, the knowledge scores regarding stroke warning signs were not significantly associated with gender (p= 0.328), age (p=0.318), education (p=0.062), occupation (p=0.279), and parent working status (p=0.174).
 |
Table 4 Association Between Knowledge Score of the Risk Factor of Stroke of the Respondents Concerning Demographics |
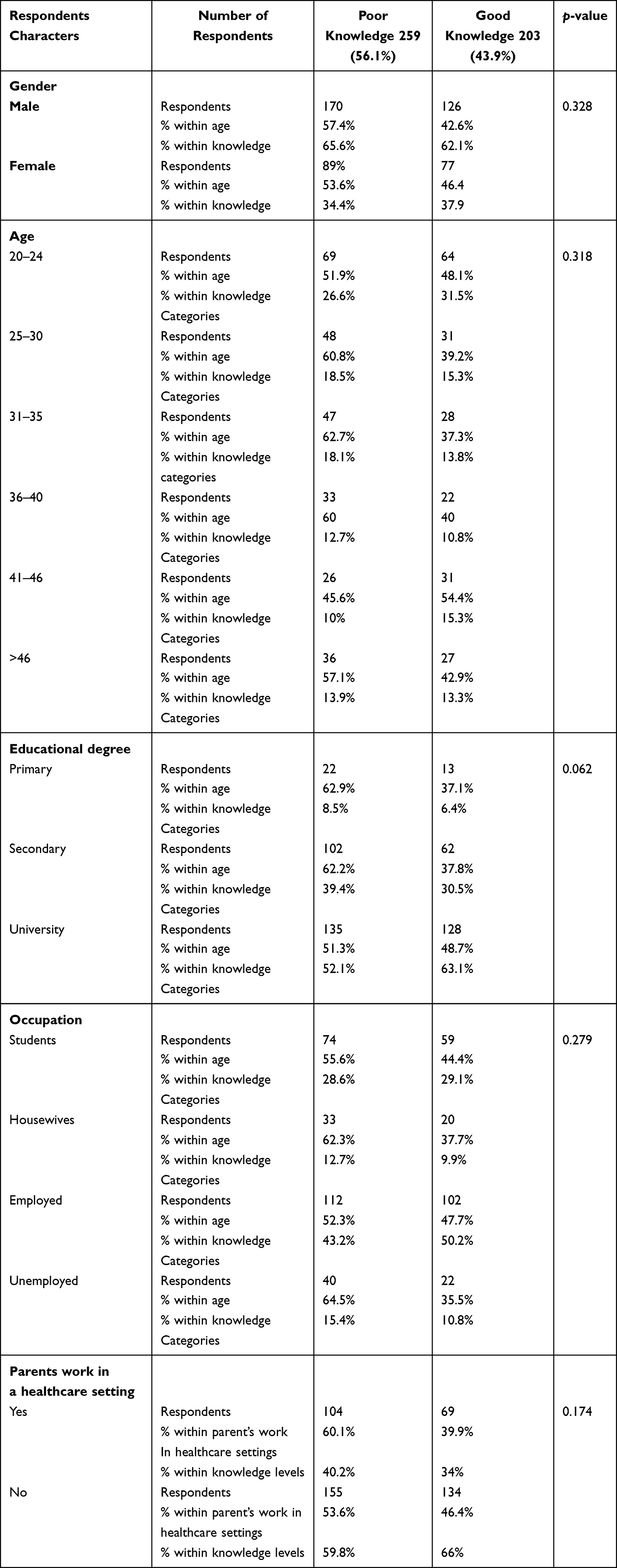 |
Table 5 Association Between Knowledge Score of Warning Signs of Stroke of the Respondents Concerning Demographics |
Discussion
Despite all implemented and ongoing initiatives, the incidence of CVDs is still an international problem. Identifying any CVDs varied based on the signs and symptoms and type. In the case of stroke, for example, different symptoms such as numbness in the face, arm, or leg, trouble speaking or understanding, and dizziness, can help in identifying the disease and preventing harm by rushing to the hospital with the patient. These symptoms do not appear in most patients or sometimes it’s difficult to understand or the incidence of stroke may occur suddenly without any specific symptoms. In addition, many individuals might not be aware of the symptoms or they may have delayed the visit to physicians. The lack of knowledge about the signs, symptoms, and early prevention in the community of the general public has a serious impact on an individual’s health, and safety and is difficult to recover. Therefore, most of these disease identifications and symptoms recognition are carried out by individual’s knowledge, and attitudes towards the diseases only. In the literature, studies evaluating the health care professional’s awareness and knowledge of risk factors of stroke are common. However, there are only a few studies on stroke knowledge of risk factors and warning signs among Saudi individuals and the public. Therefore, it would be speculated that our study is the first to assess the awareness/ knowledge of stroke risk factors and warning signs among adults living in Riyadh Saudi Arabia.
In this study, 64.7% of the respondents were found to have an adequate knowledge of the risk factors for stroke. These findings were comparable to previous findings, where 67.2% of the patients were found to have good knowledge of the risk factors.28 Similarly, another recent study revealed a 45.81% of the respondents had adequate knowledge of stroke risk factors.13 On the other hand, another study among teenagers in Spain reported poor knowledge of cerebrovascular disease was observed in a sample of teenagers. Therefore, this knowledge should be integrated into the school curriculum school curriculum.29 In this study, the most recognized risk factors for strokes were drinking alcohol (77.3%), having high blood pressure (69.5%), having had a stroke in the past (n=292; 63.2%), and smoking (56.5%), 51.1% also believed that being sedentary are the risk factors for the stroke. These results concurred with earlier research that had been published locally as well as internationally. For instance, a prior study in India found that the most prevalent risk factor was hypertension, which was then followed by poor diet, hyperlipidemia, smoking, alcohol usage, and cigarette use.10 Similar findings were found in a recent survey of the general public conducted by Mubarak et al, which indicated that an unhealthy lifestyle was followed by hypertension (72.5%), hyperlipidemia, being elderly, and heart disease.30 Similarly, a recent study among Egyptians found that stress, obesity, high serum cholesterol, and hypertension were the most common risk factors for stroke, accounting for 92.2% of cases.31 Smoking was also a significant risk factor, accounting for 72.6% of cases.31 These findings are far greater than ours. These differences in current and previous findings could be attributed to data collection methods, for example, in the current study self-administered questionnaires were used, whereas in the Osama et al, 2019 study researcher collected data using face-to-face interviews; additionally, there may be educational differences among respondents.31
Similar to the previous study, another one of individuals with cardiovascular disorders found that physical inactivity was the leading cause of stroke risk, followed by hypertension (55.5%).13 While previous research by Boehme et al in 2017 reported that hypertension, smoking, diet, and physical inactivity are some of the more frequently reported modifiable risk factors for ischemic and hemorrhagic stroke, age, sex, and race/ethnicity are no modifiable risk factors.32 The differences in the outcomes of the current and previous studies might be attributable population studied, cultural and economic factors, although in the current study, most of them identified alcohol as one of the risk factors, which might be due to the cultural factor, since in Arabic countries individual believes that alcohol and other abused drugs had adverse effects on the health and therefore its consumption is prohibited.32–34 Furthermore, the use of alcohol is associated with elevation of blood pressure,32,34 some studies revealed that alcohol consumption is associated with liver damage, which in turn stops the liver from producing a substance that helps blood to clot which can raise the risk of ischemic stroke.35
Similar results were found in Ethiopia, where the most prevalent risk factors were hypertension (74.9%), followed by family history (33.6%), alcohol consumption (22.4%), smoking (17.2%), and heart failure (17.2%).36 According to a prior study by Zhang et al in 2023, hypertension was the main risk factor for stroke in the Chinese population, followed by age, lifestyle habits, body mass index, diabetes, and dwelling area.37 The discrepancies in understanding of stroke between the current and previous findings could be attributed to the study’s samples, design, questionnaires used, and individuals’ home countries. Furthermore, in previous studies, the respondents were diabetes, heart disease, and stroke unit patients, which may have affected knowledge, because it is believed that patients with specific diseases may have attended health care professionals counseling about the diseases, and been exposed to medication use, thereby posing adequate knowledge. Furthermore, some of the risk factors identified in this study, such as alcohol consumption, tobacco use, birth control pill use, and lack of exercise, were modifiable by changing one’s lifestyle or using medicine, thereby helping to control the frequency of strokes and other diseases. These findings imply that to live a healthy life, people must be aware of and knowledgeable about several modifiable risk factors.
With regards to respondent’s knowledge related to warning signs of stroke 43.9% of the respondents reported good knowledge of warning signs of stroke, suggesting that Saudi adults lack adequate knowledge of warning signs of stroke. Although the current knowledge of Saudi adults about the warning signs was lower than the previous study among Ethiopians the author reported 63.9% of the total good knowledge of warning signs of stroke.28 In this study, most of the respondents recognized that numbness or weakness of the face and/or limbs (71.9%), followed by, severe headache with unknown cause (71.9%), blurred vision (63.4%), 27.3% of the respondents thought that chest pain or heart palpitations are a most recognized warning signs of stroke. However, less than half of the respondents (46.3%) thought that difficulty in speaking and understanding was a warning sign of stroke. On the other hand, a previous study by Workina et al, 2021 identified that sudden unilateral weakness (62.6%) was the main warning sign of stroke.13 Similarly, another recent study among the Egyptian population identified that paralysis of one side of the body (81.8%), numbness of one side of the body (79.2%), loss of consciousness (74.6%), mouth deviation (70.7%), and speech disturbance (69.7%) were the most frequent warning symptoms of stroke.31
The majority of respondents to this survey agreed that they would take people with strokes to the hospital right away, and 64.9% said they would call an ambulance if they spotted someone suffering from a stroke. These results were in line with earlier research by Osama et al among the Egyptian population, where 86% of respondents said they would transport the patient right to the hospital, followed by 45.4% who would visit a neurologist.31 In a similar vein, a survey of the Indian population found that 15.7% said they would give the patient morphine first to ease the pain while 34.6% preferred to call an ambulance when they realized the patient was having a stroke attack.10
With regards to the source of information of the stroke, Saudi adults reported a physician, followed by family and friends, a pharmacist, and nurses. These findings suggested a greater role of physicians and other healthcare professionals in the management of CVD. These findings were similar to previous findings by Chhabra et al, 2019, who reported that pharmacists are the primary source of the community’s information on stroke followed by physicians and nurses, respectively.10 On the other hand, Getu et al study 59.8% of the respondents heard about the stroke from friends and relatives,28 which is similar to our findings. Similarly, another recent study reported that textbooks and other educational material were the most common source of information, reported by 38.3% of the respondents, while familiar and friends were reported by 26.9%.38 Similarly, another study among individuals living in Egyptian revealed that 87.5% of the respondent’s sources of knowledge of stroke were heard or read about it.31 Family and friends can also help spread information in society because they are more socialized with the community, have seen or read about the diseases on social media, have had a real-life incident or previous experience with the patients, or have an educated person in their family.39 Furthermore, it is believed that reading textbooks on various topics is a habit of individuals, which helps to become more knowledgeable and aware; additionally, visiting health care providers is time-consuming and may require appointments,40,41 so many prefer to self-source, such as reading textbooks or using internet resources, which might be the reason of respondents use of textbooks as resource of their stroke.
Furthermore, one-fourth of the respondents preferred a pharmacist, which might be because pharmacists are available easily without any prior consultation, in addition in Saudi Arabia one must qualify for the Saudi licensing exam which is a combination of multiple subjects, that helps in gaining additional knowledge towards various diseases and may help the pharmacist in providing adequate, evidence-based medical advice. Furthermore, pharmacists have the right to prescribe over-The-counter medication, in addition to counseling and dispensing. This study has some limitations Firstly this study investigated the knowledge of stroke risk factors, warning signs, and treatment strategies among Saudis aged between 20–46 years only. Since the previous research has shown that middle-aged adults are more susceptible to stroke and other CVDs,3 these individuals are the upcoming generation, and their knowledge and awareness may help educate their children and family members. The respondents were limited to central region, preventing the generalizability of the findings by regionally and internationally. In addition, the study also employed a self-administered form of data collection, which may have increased the recall bias. According to the current findings, education programs on the prevention and awareness of a variety of risk factors for stroke and other diseases are critical to enhancing their knowledge and, as a result, their self-confidence and ability to help others in the community. The findings revealed that individuals require simple access and acceptability of resources, as well as counseling and educational campaigns with the assistance of health care experts. Furthermore, the findings demonstrate that some risk factors can be modified through lifestyle changes to improve people’s health and wellness. It is recommended that this study be repeated using a larger representative samples from other regions of Saudi Arabia to give a higher level of evidence.
Conclusion
In conclusion, it was discovered that 64.7% of the respondents had sufficient knowledge about the risk factors for stroke. This study has the potential to inform wider educational campaigns about stroke, to benefit primary prevention and early management/outcomes. On the other hand, knowledge of warning signs of stroke suggested that more work needs to raise people’s awareness of diseases and their symptoms through various educational activities and campaigns to increase people’s knowledge of diseases. Therefore, it is important to spread knowledge using a variety of means, such as social media, posters, brochures, and flyers. The planning of stroke prevention can benefit from this information. Knowing that raising individuals’ knowledge about the risk of stroke and other diseases would significantly improve the outcome of diseases.
Acknowledgments
The authors would like to extend their appreciation to King Saud University, Riyadh, Saudi Arabia for supporting this work through the Researcher Supporting Project (RSPD2023R1099).
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research Supporting Project, number (RSPD2023R1099), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Manual WS. The WHO STEPwise Approach to Stroke Surveillance. Vol. 96. Geneva: World Health Organization; 2006.
2. Centers for disease control and prevention. About stroke. Available from: https://www.cdc.gov/stroke/about.htm#:~:text=A%20stroke%2C%20sometimes%20called%20a,term%20disability%2C%20or%20even%20death. Accessed August 14, 2023.
3. Syed W, Qadhi OA, Barasheed A, AlZahrani E, Al-Rawi BA. Evaluation of knowledge of risk factors and warning signs of stroke–an observational study among future health care professionals. Front Public Health. 2023;11:1131110. doi:10.3389/fpubh.2023.1131110
4. World Health Organization. World Stroke Day; 2022. Available from: https://www.who.int/srilanka/news/detail/29-10-2022-world-stroke-day-2022#:~:text=The%20Global%20Stroke%20Factsheet%20released,a%20stroke%20in%20their%20lifetime.
5. Pu L, Wang L, Zhang R, Zhao T, Jiang Y, Han L. Projected global trends in ischemic stroke incidence, deaths and disability-adjusted life years from 2020 to 2030. Stroke. 2023;54(5):1330–1339. doi:10.1161/STROKEAHA.122.040073
6. Jaberinezhad M, Farhoudi M, Nejadghaderi SA, et al. The burden of stroke and its attributable risk factors in the middle east and north Africa region, 1990–2019. Sci Rep. 2022;12(1):2700. doi:10.1038/s41598-022-06418-x
7. Alqahtani BA, Alenazi AM, Hoover JC, et al. Incidence of stroke among Saudi population: a systematic review and meta-analysis. Neurol Sci. 2020;41(11):3099–3104. doi:10.1007/s10072-020-04520-4
8. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2023 update: a report from the American heart association. Circulation. 2023;147:e93–e621. doi:10.1161/CIR.0000000000001123
9. American Heart Association/American Stroke Association. TIA (transient ischemic attack); 2016.
10. Chhabra M, Gudi SK, Rashid M, Sharma P, Sharma S, Khan H. Assessment of knowledge on risk factors, warning signs, and early treatment approaches of stroke among community adults in north India: a telephone interview survey. J Neurosci Rural Pract. 2019;10(3):417–422. doi:10.1055/s-0039-1697561
11. El-Hajj M, Salameh P, Rachidi S, Al-Hajje A, Hosseini H.Development of a diagnosis score for stroke in the Lebanese population. Clin Epidemiol Glob Health. 2018;07:79–87.
12. Fisher M, Iadecola C, Sacco R. Introduction to the stroke compendium. Circ Res. 2017;120(3):437–438. doi:10.1161/CIRCRESAHA.116.310453
13. Workina A, Kebede S, Fekadu C, Wubetie Snr A. Knowledge of risk factors and warning signs of stroke among patients with heart disease at tikur anbessa specialized hospital. Open Access Emerg Med. 2021;13:57–66. doi:10.2147/OAEM.S291648
14. Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization (WSO): global stroke fact sheet 2022. Int J Stroke. 2022;17(1):18–29. doi:10.1177/17474930211065917
15. Alqunaibet A, Herbst C, El-Sharty S, et al. Noncommunicable diseases in Saudi Arabia: toward effective interventions for prevention. IBRD. 2021;10:1–20.
16. Nansseu JR, Atangana CP, Petnga SN, Kamtchum-Tatuene J, Noubiap JJ. Assessment of the general public’s knowledge of stroke: a cross-sectional study in Yaoundé. Cameroon J Neurol Sci. 2017;378:123–129.
17. Zeina H, Mona O, Reem H. Primary care physicians’ awareness and perceptions on adherence to primary cardiovascular disease prevention guidelines in Lebanon; 2021. Available from: https://journals.sagepub.com/doi/full/10.1177/1742395320983879.
18. Iqbal A, Azhar S, Murtaza G, et al. Navigating thyroid dysfunction and comorbidities among university students in Abbottabad, Pakistan - a cross-sectional evaluation of screening tool for thyroid dysfunction. Int J Gen Med. 2023;16:4193–4205. doi:10.2147/IJGM.S415311
19. Bashatah A, Syed W, Al-Rawi MBA. Knowledge of cardiovascular disease risk factors and its primary prevention practices among the Saudi public - a questionnaire-based cross-sectional study. Int J Gen Med. 2023;16:4745–4756. doi:10.2147/IJGM.S433472
20. Alobaid AM, Syed W, Al-Rawi MBA. Factors associated with sedentary behavior and physical activity among people living in Saudi Arabia - a cross-sectional study. Risk Manag Healthc Policy. 2023;16:1985–1997. doi:10.2147/RMHP.S427792
21. Syed W, Al-Rawi MBA. Community pharmacists awareness, perceptions, and opinions of artificial intelligence: a cross-sectional study in Riyadh, Saudi Arabia. Technol Health Care. 2023:1–13. doi:10.3233/THC-230784
22. Bashatah A, Qadhi OA, Al Sadoun A, Syed W, Al-Rawi MBA. Evaluation of young adults’ physical activity status and perceived barriers in the Riyadh region of Saudi Arabia. J Multidiscip Healthc. 2023;16:557–569. doi:10.2147/JMDH.S397341
23. Alobaid AM, Syed W, Al-Rawi MBAMBA. Evaluation of headache trends among undergraduate first responders for medical emergencies at Saudi University in Riyadh, Saudi Arabia. Medicina. 2023;59(9):1522. doi:10.3390/medicina59091522
24. Syed W, Alharbi MK, Samarkandi OA, et al. Evaluation of knowledge, awareness, and factors associated with diabetes: a cross-sectional community-based Study. Int J Endocrinol. 2022:1921010. doi:10.1155/2022/1921010
25. Samreen S, Siddiqui NA, Wajid S, Mothana RA, Almarfadi OM. Prevalence and use of dietary supplements among pharmacy students in Saudi Arabia. Risk Manag Healthc Policy. 2020;13:1523–1531. doi:10.2147/RMHP.S256656
26. Syed W, Iqbal A, Siddiqui NA, Mothana RA, Noman O. Attitudes and associated demographic factors contributing towards the abuse of illicit drugs: a cross-sectional study from health care students in Saudi Arabia. Medicina. 2022;58(2):322. doi:10.3390/medicina58020322
27. World population review. Riyadh population; 2023. Available from: https://worldpopulationreview.com/world-cities/riyadh-population.
28. Getu RA, Aga F, Badada T, Workie SG, Belew MA, MekonnenRN K. Knowledge of stroke risk factors and warning symptoms among adults with type 2 diabetes in Addis Ababa, Ethiopia, 2021: an institution-based cross-sectional study. BMC Cardiovasc Disord. 2023;23:21. doi:10.1186/s12872-022-03031-8
29. Arboix A, Arboix-Alió A, Hernández-Arrieta M.Escaso conocimiento de la enfermedad vascular cerebral en una muestra de jovenes adolescentes [Scant knowledge about cerebrovascular disease in a sample of teenagers]. Rev Neurol. 2003;37(5):500.
30. Mubaraki AA, Alqahtani AS, Almalki AA, et al. Public knowledge and awareness of stroke among adult population in Taif city, Saudi Arabia. Neurosci J. 2021;26:339–345. doi:10.17712/nsj.2021.4.20210057
31. Osama A, Ashour Y, El-Razek RA, Mostafa I. Public knowledge of warning signs and risk factors of cerebrovascular stroke in Ismailia Governorate, Egypt. Egypt J Neurol Psychiatr Neurosurg. 2019;55(1):1–6. doi:10.1186/s41983-019-0079-6
32. Boehme AK, Esenwa C, Elkind MS. Stroke risk factors, genetics, and prevention. Circ Res. 2017;120(3):472–495. doi:10.1161/CIRCRESAHA.116.308398
33. Alhashimi FH, Khabour OF, Alzoubi KH, Al-Shatnawi SF. Attitudes and beliefs related to reporting alcohol consumption in research studies: a case from Jordan. Pragmat Obs Res. 2018;9:55–61. doi:10.2147/POR.S172613
34. Kuo SH, Lee YT, Li CR, et al. Mortality in emergency department sepsis score as a prognostic indicator in patients with pyogenic liver abscess. Am J Emerg Med . 2013;31:916–921.
35. Smyth A, O’Donnell M, Rangarajan S, et al. Alcohol intake as a risk factor for acute stroke: the INTERSTROKE study. Neurology. 2023;100(2):e142–e153. doi:10.1212/WNL.0000000000201388
36. Fekadu G, Chelkeba L, Kebede A. Risk factors, clinical presentations and predictors of stroke among adult patients admitted to stroke unit of Jimma University Medical Center, south west Ethiopia: prospective observational study. BMC Neurol. 2019;19(1):187. doi:10.1186/s12883-019-1409-0
37. Zhang X, Dai J, Li W, Yang Y. High-risk population and factors of stroke has changed among middle-aged and elderly Chinese—evidence from 1989 to 2015. Front Public Health. 2023;11:1090298. doi:10.3389/fpubh.2023.1090298
38. Elshebiny A, Almuhanna M, AlRamadan M, Aldawood M, Aljomeah Z. Awareness of stroke risk factors, warning signs, and preventive behaviour among diabetic patients in Al-Ahsa, Saudi Arabia. Cureus. 2023;15(2):e35337. doi:10.7759/cureus.35337
39. Pew Rsearch Center. Friends and family – important drivers of news. Available from: https://www.pewresearch.org/journalism/2013/03/17/friends-and-family-important-drivers-of-news/.
40. Paterick TE, Patel N, Tajik AJ, Chandrasekaran K. Improving health outcomes through patient education and partnerships with patients. Proc. 2017;30(1):112–113. doi:10.1080/08998280.2017.11929552
41. Bashatah AS, Syed W, Al-Rawi MB. perceptions of peoples towards health care seeking behavior from health care professionals–findings from Saudi community perspective. Farmacia. 2023;71:1095–1102. doi:10.31925/farmacia.2023.5.24
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.