Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Serum Lipid-Based Prognostic Model for Advanced Intrahepatic Cholangiocarcinoma Under Chemo-Immunotherapy
Authors Jiang C, Long K ![]() , Fang T, Li W, Yang L, Chai P, Tao J
, Fang T, Li W, Yang L, Chai P, Tao J ![]() , Long K
, Long K
Received 13 October 2025
Accepted for publication 30 December 2025
Published 13 January 2026 Volume 2026:13 569963
DOI https://doi.org/10.2147/JHC.S569963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Chengzhi Jiang,1,2,* Kaijun Long,1,* Tianyuan Fang,2 Wen Li,2 Liu Yang,2 Pengcheng Chai,2 Ji Tao,2 Kaiguo Long1
1Department of Breast and Thyroid Surgery, The Second Affiliated Hospital of Zunyi Medical University, Zunyi City, Guizhou Province, People’s Republic of China; 2Department of Gastrointestinal Medical Oncology, Harbin Medical University Cancer Hospital, Harbin, Heilongjiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kaiguo Long, Email [email protected] Ji Tao, Email [email protected]
Background: Serum lipid levels have been associated with the prognosis of various malignancies.
Aim: To develop a novel nomogram based on serum lipid parameters to predict overall survival in patients with intrahepatic cholangiocarcinoma.
Methods: Serum lipid profiles and survival data were collected prior to the initiation of chemotherapy combined with immunotherapy. Survival analysis was performed to identify prognostic factors associated with ICC. Independent prognostic factors were used to construct a nomogram. The predictive performance of the nomogram was evaluated. External validation of the survival analysis and nomogram for serum lipids was conducted using a validation cohort.
Results: Low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and apolipoprotein A1 were selected for further analysis. Survival analysis demonstrated that patients with low LDL-C, high HDL-C, and high ApoA1 levels exhibited significantly longer OS and PFS. A nomogram incorporating LDL-C and HDL-C was constructed to predict 1-, 2-, and 3-year survival probabilities. The nomogram exhibited favorable predictive performance.
Discussion: Pre-treatment serum levels of LDL-C, HDL-C, and ApoA1 exhibited significant prognostic value for advanced ICC. The nomogram constructed based on LDL-C and HDL-C effectively predicted survival outcomes, providing a theoretical basis to support treatment decision-making and individualized prognostic assessment in clinical practice.
Keywords: Serum lipid levels, Intrahepatic Cholangiocarcinoma, Immunotherapy, Nomogram
Introduction
Intrahepatic cholangiocarcinoma (ICC) is the second most common primary liver malignancy after hepatocellular carcinoma. Although various therapeutic strategies, including chemotherapy, targeted therapy, and chemotherapy combined with immunotherapy, are currently available for advanced ICC, the overall clinical outcomes remain unsatisfactory, with a 5-year survival rate of less than 20% in most patients.1 Notably, patients receiving chemoimmunotherapy exhibit longer overall survival (OS) compared to those receiving chemotherapy alone; however, the overall survival rates remain suboptimal, indicating substantial challenges in the immunotherapeutic management of advanced ICC.2,3 Owing to factors such as low expression of immune checkpoints and intrinsic resistance of tumor cells, immune checkpoint inhibitors (ICIs) demonstrate limited efficacy in a subset of patients. Therefore, the identification of reliable biomarkers to stratify patients who are more likely to benefit from ICIs is essential for optimizing treatment strategies and guiding future therapeutic development.4
Lipid metabolic reprogramming plays a pivotal role in various biological processes of tumor cells, including proliferation, migration, invasion, and metastasis.5–12 Compared to monolayer-cultured ICC cells, ICC stem-like cells exhibit enhanced de novo fatty acid synthesis activity and higher expression levels of key enzymes involved in fatty acid biosynthesis, such as fatty acid synthase (FASN). Clinically, ICC patients with high FASN expression are associated with poorer long-term survival outcomes.13 Correspondingly, inhibition of the mTOR signaling pathway can suppress FASN-mediated fatty acid synthesis, thereby reducing fatty acid oxidation in tumor-associated macrophages and promoting antitumor immune responses.14 Additionally, treatment with fatty acid oxidation (FAO) inhibitors led to suppressed proliferation in several cancer cell types, including cholangiocarcinoma, suggesting that blockade of fatty acid catabolism may effectively inhibit tumor growth.15 Moreover, lipid metabolic reprogramming is closely associated with the efficacy of tumor immunotherapy. For example, cPLA2α activity driven by tumor cells and regulatory T cells (Tregs) can induce lipid droplet accumulation in effector T cells, resulting in T cell senescence. Inhibition of cPLA2α has been shown to prevent effector T cell exhaustion and enhance the efficacy of immunotherapy.16 CXCL6 can induce metabolic reprogramming in cholangiocarcinoma (CCA) by regulating the CXCR1/2-JAK-STAT/PI3K signaling axis. This, in turn, activates the neutrophil RAS/MAPK pathway, promoting the formation of Neutrophil Extracellular Traps (NETs). These events lead to reduced CD8+ T cell infiltration in the tumor microenvironment, contributing to immune evasion and resistance to immunotherapy.17 Additionally, URKB promotes phosphorylation of H3K9me3/serine 10, which reduces H3K9me3 enrichment at the NCEH1 promoter. This alteration increases overall NCEH1 expression and cholesterol levels in CCA cells, resulting in resistance to neoadjuvant chemoimmunotherapy in CCA patients. Targeting URKB with inhibitors or using statin drugs can enhance sensitivity to chemoimmunotherapy.18 Similarly, PD-L1-containing tumor-derived extracellular vesicles can also promote lipid droplet accumulation in T cells, leading to senescence and resistance to immunotherapy.19 Thus, lipid metabolic reprogramming may exert critical regulatory effects on tumor immunotherapy by modulating the immune microenvironment.20
With the widespread application of metabolomics, an increasing number of studies have revealed significant associations between alterations in serum lipid levels and the prognosis of various malignancies.21 Serum lipids are essential components involved in energy storage, metabolism, and cellular signal transduction. Changes in serum lipid levels can indirectly reflect lipid alterations within the tumor microenvironment, thereby representing potential biomarkers for predicting the efficacy of immunotherapy. A retrospective study reported that low levels of triglycerides and high-density lipoprotein cholesterol (HDL-C) were strongly associated with recurrence in patients with thyroid cancer.22 Earlier research also suggested that serum triglyceride and HDL-C levels were correlated with prostate cancer severity.23 Sun et al identified a causal association between elevated low-density lipoprotein cholesterol (LDL-C) and gastric cancer. Furthermore, triglyceride levels ≥2.2 mmol/L were found to increase the risk of gallbladder cancer in men over the age of 60.9 However, studies exploring the prognostic value and predictive significance of serum lipid levels in relation to immunotherapeutic outcomes in ICC remain scarce.
This study analyzed the association between pre-treatment serum lipid levels and prognosis in patients with advanced ICC undergoing chemotherapy combined with immunotherapy. Independent prognostic risk factors were identified, and a nomogram-based prognostic model was constructed to provide a potential reference for clinical decision-making and prognostic assessment (Figure 1).
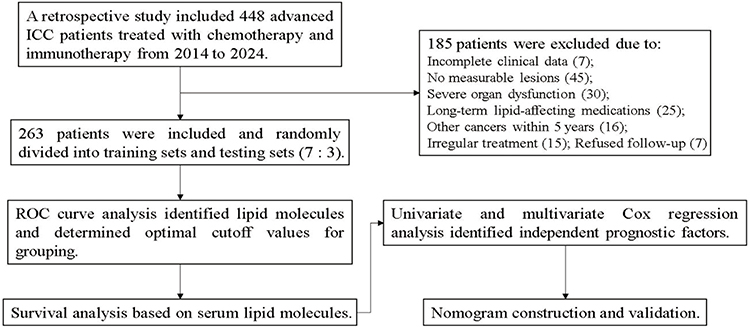 |
Figure 1 Work flow of this study. |
Methods
Study Population
This study enrolled 263 patients diagnosed with unresectable advanced ICC at the Harbin Medical University Cancer Hospital between January 2014 and January 2024. Inclusion criteria were as follows: (1) Histopathological confirmation of ICC; (2) Presence of measurable lesions according to the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1); (3) Effective radiological assessments performed prior to treatment and after every 2–3 treatment cycles; (4) Treatment regimen consisting exclusively of chemotherapy combined with immune checkpoint inhibitors (ICIs); (5) Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2; and (6) Patient age between 18 and 80 years.
Exclusion criteria were as follows: (1) Incomplete clinical data; (2) Absence of measurable lesions; (3) History of other histologically confirmed malignancies within the past five years; (4) Presence of severe organ dysfunction; (5) Diagnosis of autoimmune deficiency disorders; (6) Use of medications known to affect serum lipid levels during the treatment period, such as statins or fibrates; (7) History of prior locoregional liver therapies, including surgery, interventional procedures (eg, ablation, embolization, or brachytherapy).
The follow-up deadline for all patients was June 2024, and the median follow-up time was 20.1 months.
Clinical Data Collection
Clinical records were retrospectively reviewed to collect baseline clinical data from patients. The collected variables included sex, age, smoking history, alcohol history, ECOG, performance status, American Joint Committee on Cancer (AJCC) staging, histological differentiation, Child–Pugh classification, and primary tumor size.
In a fasting state, serum lipid profiles were collected within one week prior to the initiation of systemic therapy, including LDL-C, HDL-C, total cholesterol, triglycerides (TG), apolipoprotein B (APOB), apolipoprotein A1 (APOA1), and lipoprotein alpha (Lpα).
Efficacy Evaluation and Follow-Up
Computed tomography (CT) and other imaging modalities were performed prior to treatment and subsequently every 2–3 treatment cycles to monitor and evaluate therapeutic response. Treatment efficacy was assessed according to the RECIST version 1.1 and categorized as complete remission (CR), partial remission (PR), stable disease (SD), or progressive disease (PD). The objective response rate (ORR) and disease control rate (DCR) were used as short-term efficacy endpoints. ORR was defined as the proportion of patients achieving CR or PR, while DCR was defined as the proportion of patients achieving CR, PR, or SD.
OS was used as the primary indicator for evaluating long-term treatment efficacy. PFS was defined as the time from initiation of chemotherapy combined with immunotherapy for advanced disease to either documented disease progression or death from any cause. OS was defined as the time from initial diagnosis of ICC to death from any cause or the date of last follow-up. The primary endpoint was OS, while secondary endpoints included PFS, DCR, and ORR.
Survival Analysis
Receiver operating characteristic (ROC) curve analysis was performed to calculate the area under the curve (AUC) for serum lipid levels, including LDL-C, HDL-C, CHOL, TG, ApoB, ApoA-1, and Lpα. Parameters with AUC values greater than 0.7 were retained for subsequent analyses. The dataset was randomly divided into a training cohort and a testing cohort at a 7:3 ratio. The prognostic model was constructed using the training cohort and validated in the testing cohort. Serum lipid levels were then dichotomized into high and low groups based on these cut-off points. ROC curve analysis was conducted using the “pROC” package in R software to determine optimal cut-off values and corresponding AUCs. Clinical characteristics and short-term therapeutic efficacy between groups were compared using Fisher’s exact test. Survival curves for patients with high versus low serum lipid levels were generated using the “survival” package in R. A value of P < 0.05 is considered to indicate statistically significant differences.
Nomogram
Univariate and multivariate Cox regression analyses were performed using the “survival” package in R to identify independent prognostic factors among patients’ clinical characteristics and serum lipid levels. Forest plots were generated using the “ggplot2” package. Independent prognostic factors were incorporated into a nomogram constructed with the “nomogram” package. Calibration curves were established using the “rms” package, and the concordance index (C-index) was calculated for internal validation of the nomogram. The predictive performance of the nomogram-based prognostic model was further assessed using ROC curves and decision curve analysis (DCA), generated via the “timeROC” and “Dcurves” packages, respectively. External validation was conducted using data from the testing cohort.
Statistical Methods
Data organization, statistical analyses, tabulation, and visualization were performed using R software version 4.3.2. Categorical variables were presented as counts (percentages). Normally distributed continuous variables were summarized as mean ± standard deviation, while non-normally distributed continuous variables were expressed as median (interquartile range). Comparisons of categorical variables between two groups were conducted using Fisher’s exact test.
Ethics
The study was conducted in accordance with the Declaration of Helsinki (6th revision, 2008). The study protocol was approved by the Ethics Committee of Cancer Hospital of Harbin Medical University (protocol number KY2023-18, approved on 01/11/2023).
Results
Clinical Characteristics
A total of 263 patients meeting the criteria were ultimately enrolled in this study (Table 1). All patients received first-line chemotherapy regimens consisting of GC, GS, or GEMOX. Upon disease progression, second-line chemotherapy consisted of mFOLFOX. Immunotherapy agents included camrelizumab.
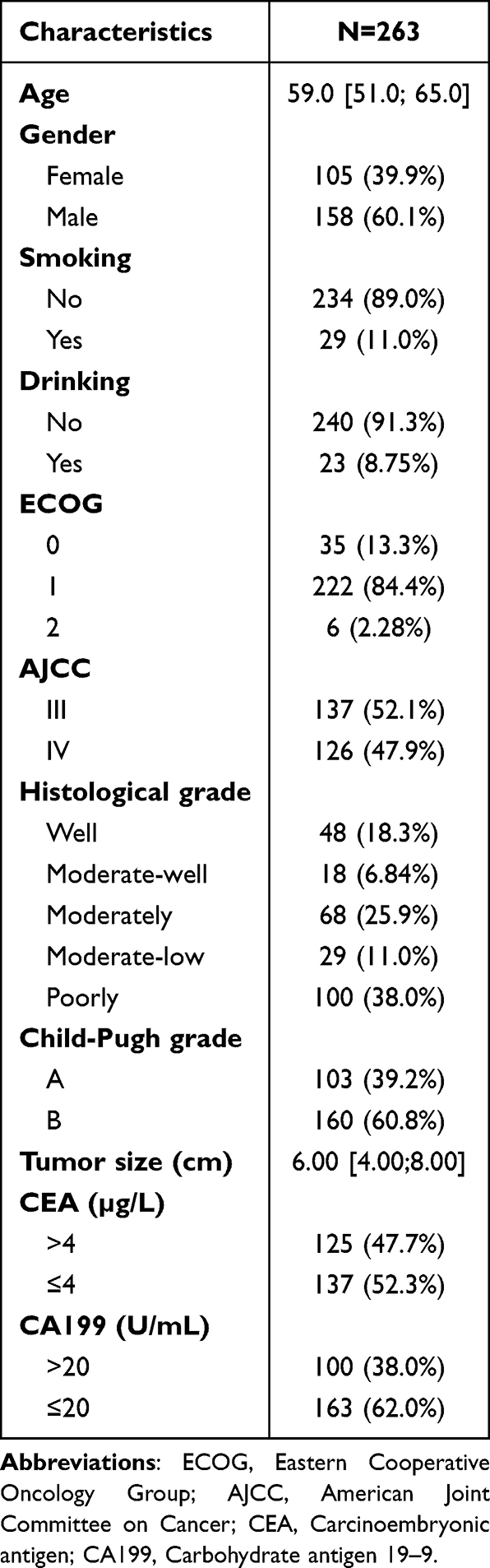 |
Table 1 Clinical Characteristics of the 263 Patients with Advanced ICC |
All patients were randomly divided into a training cohort and a testing cohort at a 7:3 ratio, including 184 patients in the training cohort and 79 patients in the testing cohort. Baseline characteristics between the training and testing cohorts showed no statistically significant differences except for primary tumor size (p = 0.022) (Table S1).
Determination of Optimal Cutoff Values for Serum Lipid Levels
To elucidate the relationship between serum lipid levels and prognosis, ROC curve analysis was employed to determine the optimal cutoff values for serum lipid parameters—including LDL-C, HDL-C, TC, TG, ApoB, ApoA1, and Lpα—in order to stratify patients into high- and low-level groups.
In the training cohort, the optimal cutoff value for LDL-C was 3.050 mmol/L. Based on this cutoff, patients were stratified into a high LDL-C group (n = 85) and a low LDL-C group (n = 99) (Figure 2A). For HDL-C, the optimal cutoff was 1.290 mmol/L. Patients were divided into high HDL-C (n = 96) and low HDL-C (n = 88) groups accordingly (Figure 2B). The optimal cutoff for ApoA1 was 1.435 g/L. Patients were categorized into high ApoA1 (n = 70) and low ApoA1 (n = 114) groups (Figure 2C). Similar results were observed in the validation cohort.
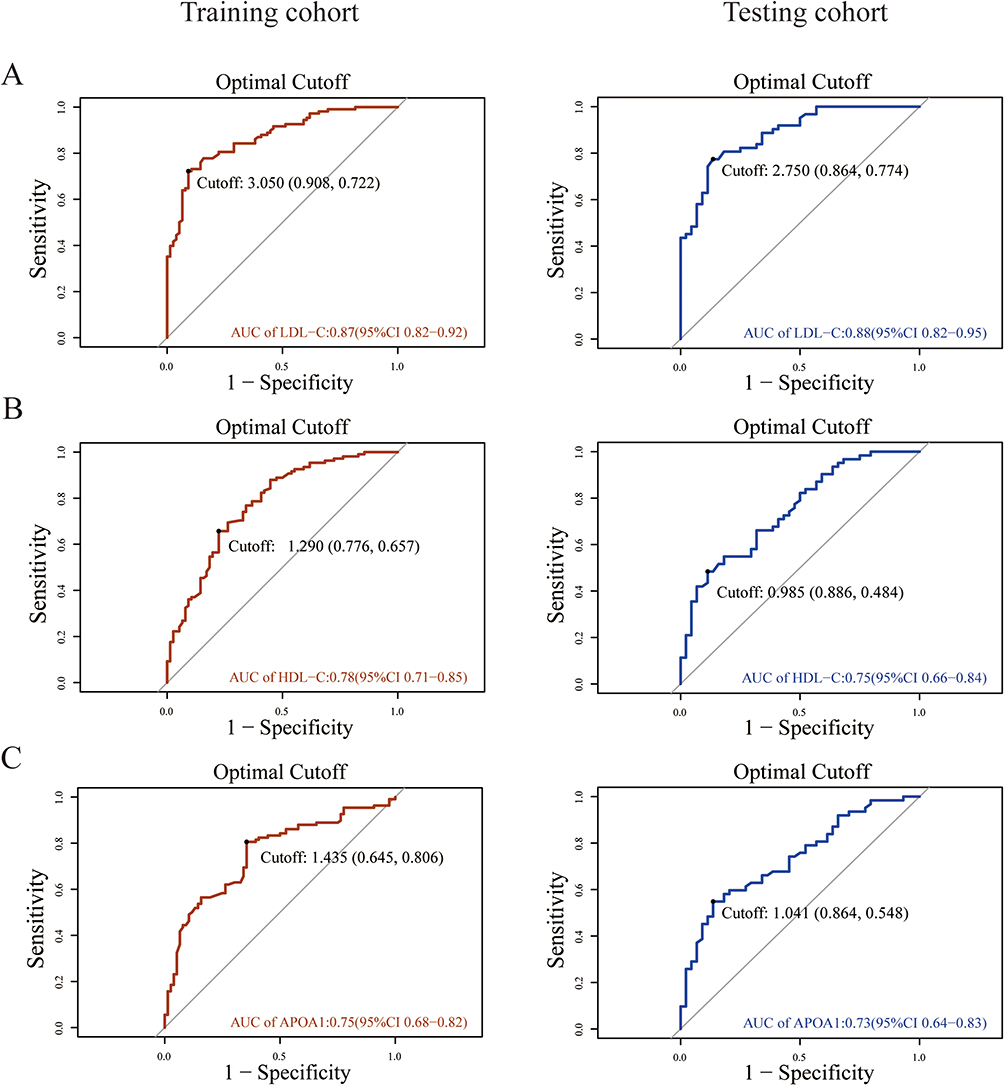 |
Figure 2 The ROC curve of LDL-C, HDL-C and APOA1. (A) The ROC curve of LDL-C. (B) The ROC curve of HDL-C. (C) The ROC curve of APOA1. Abbreviations: ROC, Receiver operating characteristic; LDL-C, Low-Density Lipoprotein Cholesterol; HDL-C, High-Density Lipoprotein Cholesterol; APOA1, Apolipoprotein A1. |
The remaining indicators were excluded from further analysis due to AUC values below 0.7 and were therefore not grouped based on optimal cutoff values (Figure S1).
Comparison of Clinical Characteristics Among Different Levels of LDL-C, HDL-C, and APOA1
ROC analysis identified LDL-C, HDL-C, and ApoA1 as candidates for further stratified analysis. Subsequently, baseline clinical characteristics were compared among patient groups with different levels of LDL-C, HDL-C, and ApoA1.
No significant differences were observed between the high and low LDL-C groups of advanced ICC patients with clinical characteristics (Table S2). Whereas, for HDL-C, a statistically significant difference was observed in histological differentiation between the high group and low group (p = 0.028, Table S3). Similarly, in high and low APOA1 groups, a statistically significant difference was found in primary tumor size (p = 0.01), with the median tumor size in the low ApoA1 group being larger than that in the high ApoA1 group (Table S4).
Relationship Between LDL-C, HDL-C, and APOA1 and Short-Term Treatment Efficacy
To investigate the relationship between LDL-C, HDL-C, and ApoA1 levels and patients’ short-term therapeutic responses, this study analyzed DCR and ORR, with the results as follows:
The DCR were 50.59% and 47.22% for the low- and high-LDL-C groups, respectively (p = 0.889); the ORR were 12.94% and 5.56%, respectively (p = 0.182) (Table S5). For HDL-C, the DCRs were 45.13% and 59.09% for the low- and high-HDL-C groups, respectively (p = 0.367); the ORRs were 9.73% and 9.09%, respectively (p = 1) (Table S5). Regarding ApoA1, the DCRs were 46.39% and 53.33% for the low- and high-ApoA1 groups, respectively (p = 0.67); the ORRs were 7.22% and 13.33%, respectively (p = 0.278) (Table S5).
In summary, patients with low LDL-C, high HDL-C, and high ApoA1 levels exhibited better short-term therapeutic responses; however, none of these three indicators showed statistically significant differences in DCR or ORR.
Relationship Between LDL-C, HDL-C, and ApoA1 and Long-Term Therapeutic Outcomes
Subsequently, OS and PFS were compared among advanced ICC patients stratified by LDL-C, HDL-C, and ApoA1 levels. In the training cohort, The low LDL-C group exhibited significantly longer mOS and mPFS compared to the high LDL-C group, with mOS extended by 22.1 months (p < 0.001, HR = 3.968, 95% CI 2.698–5.835) (Figure 3A) and mPFS extended by 2.3 months (p = 0.027, HR = 1.549, 95% CI 1.021–2.348) (Figure S2A). For HDL-C, the training cohort’s low HDL-C group had a shorter mOS and mPFS than the high HDL-C group by 17.5 months (p < 0.001, HR = 0.364, 95% CI 0.248–0.533) (Figure 3B) and 3.07 months (p = 0.025, HR = 0.642, 95% CI 0.426–0.967) (Figure S2B), respectively. Regarding ApoA1, the low ApoA1 group in the training cohort showed a longer mOS than the high ApoA1 group by 4.62 months (p < 0.001, HR = 0.463, 95% CI 0.311–0.689) (Figure 3C) and a significantly shorter mPFS by 6.8 months (p = 0.004, HR = 0.395, 95% CI 0.183–0.851) (Figure S2C).
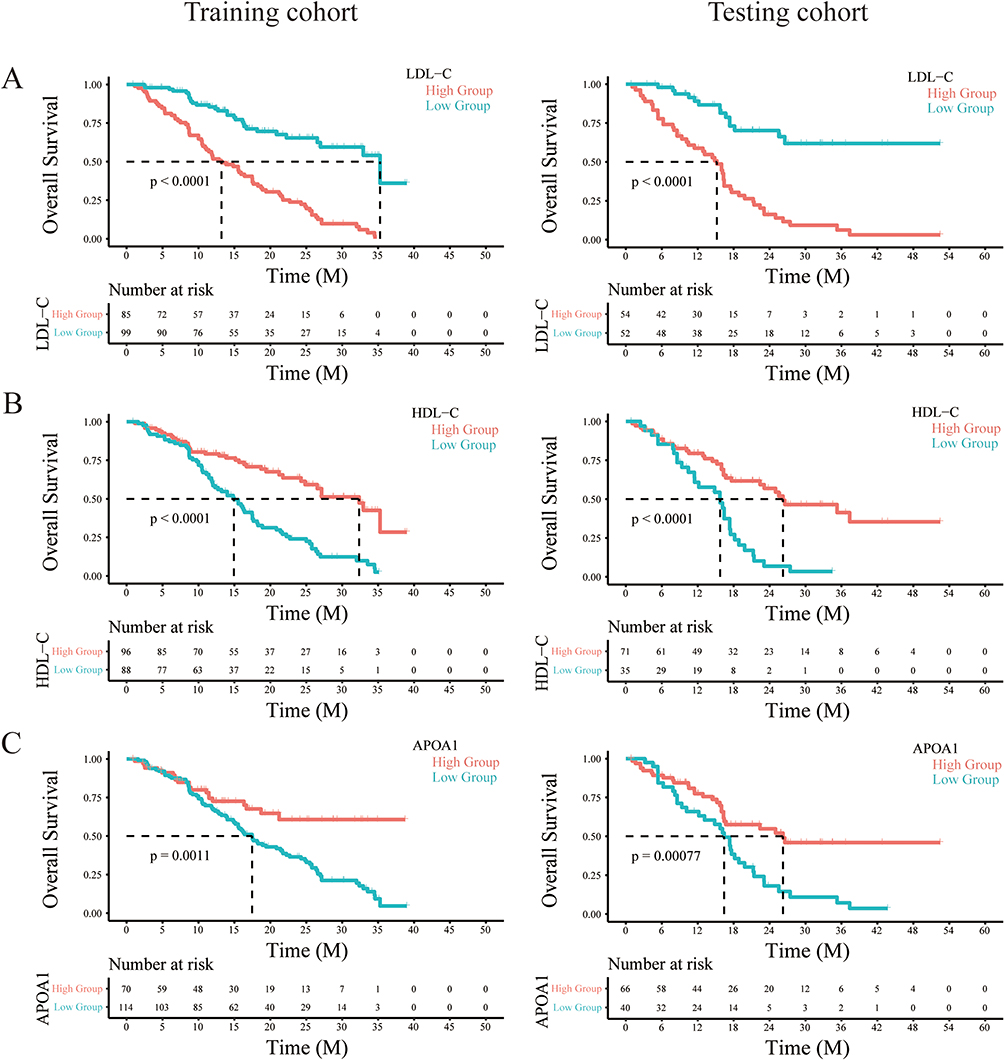 |
Figure 3 Comparison of Kaplan-Meier curves of OS between different levels of LDL-C, HDL-C and APOA1 for training cohort and testing cohort. (A) Kaplan-Meier curves of OS with LDL-C. (B) Kaplan-Meier curves of OS with HDL-C. (C) Kaplan-Meier curves of OS with APOA1. Abbreviations: LDL-C, Low-Density Lipoprotein Cholesterol; HDL-C, High-Density Lipoprotein Cholesterol; APOA1, Apolipoprotein A1; OS, overall survival. |
Additionally, in testing cohort, the mOS of different levels for LDL-C (p<0.0001), HDL-C (p<0.0001) and ApoA1 (p<0.0001) all showed statisticantly differences (Figure 3). For mPFS, there demonstrated no significance except for ApoA1 (p=0.0049) (Figure S2).
Independent Prognostic Factors Affecting Outcomes in Advanced Intrahepatic Cholangiocarcinoma Patients
To further investigate independent prognostic factors, Cox proportional hazards regression models were employed. General clinical characteristics, along with varying levels of LDL-C, HDL-C, and ApoA1, were included in both univariate and multivariate analyses based on OS and PFS.
Univariate Cox regression analysis based on the training cohort revealed that low levels of HDL-C, low levels of ApoA1, and larger primary tumor size were significantly associated with poor OS in ICC patients, whereas low LDL-C levels were correlated with favorable prognosis (p < 0.05) (Figure 4A). Similarly, univariate Cox analysis in the validation cohort demonstrated that low HDL-C and low ApoA1 levels were adverse prognostic factors, while low LDL-C levels and well to moderately differentiated histology were associated with improved prognosis in ICC patients (p < 0.05) (Figure 4B).
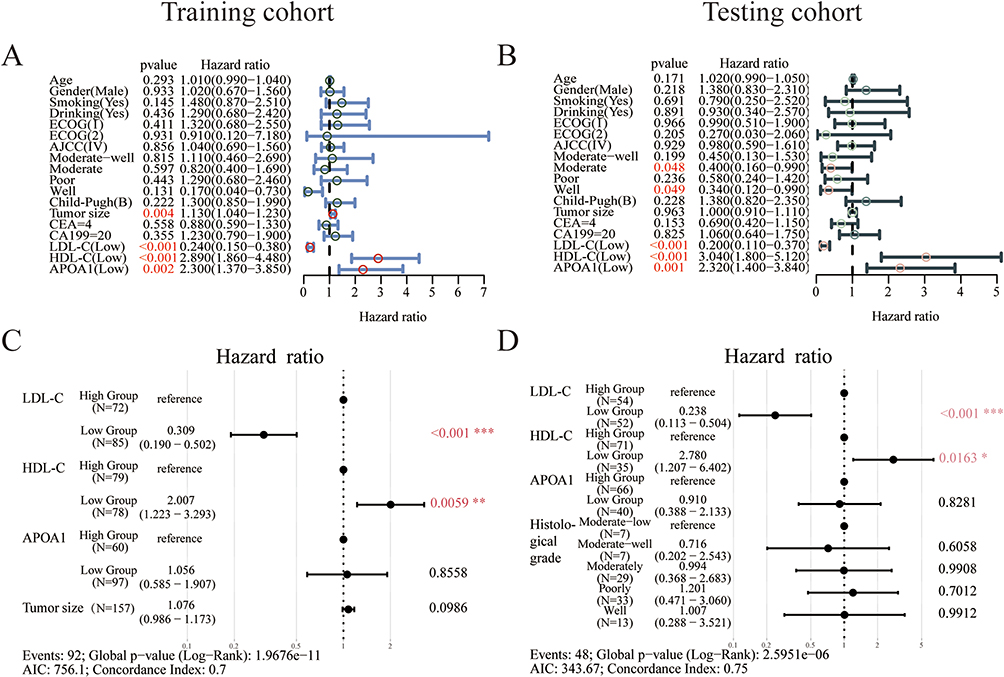 |
Figure 4 COX regression analysis of OS with advanced ICC for training cohort and testing cohort. (A) Univariate analysis of OS for training cohort. (B) Univariate analysis of OS for testing cohort. (C) Multivariate analysis of OS for training cohort. (D) Multivariate analysis of OS for testing cohort. Colored text and *, p<0.05; **, p<0.05; ***, p<0.001. Abbreviations: LDL-C, Low-Density Lipoprotein Cholesterol; HDL-C, High-Density Lipoprotein Cholesterol; APOA1, Apolipoprotein A1; OS, overall survival. |
Multivariate Cox regression analyses in both the training and validation cohorts demonstrated that low levels of LDL-C and HDL-C were independent prognostic factors for ICC patients (p < 0.05). Specifically, low LDL-C was identified as an independent protective factor, whereas low HDL-C was an independent risk factor for poor prognosis in ICC patients (Figure 4C and D).
Subsequently, Cox regression analysis was performed to evaluate the impact of LDL-C, HDL-C, and ApoA1 on PFS in ICC patients. Univariate Cox analysis in the training cohort demonstrated that well-differentiated tumors and low LDL-C levels were favorable prognostic factors for PFS, whereas low HDL-C was also identified as a favorable prognostic factor for PFS (p < 0.05) (Figure S3A). In the validation cohort, the trends for all three markers were consistent with those observed in the training cohort; however,only the association with ApoA1 reached statistical significance (Figure S3B).
Multivariate Cox regression analysis based on the training cohort indicated that low LDL-C was a protective factor for PFS in ICC patients, whereas low HDL-C was a risk factor; however, these results did not reach statistical significance (Figure S3C). In the validation cohort, multivariate Cox regression identified low ApoA1 as an adverse prognostic factor for PFS in ICC patients (p < 0.05) (Figure S3D).
Construction and Validation of the Nomogram Prediction Model
Given the stronger association between the aforementioned serum molecules and OS in ICC patients, we focused exclusively on developing a predictive model for OS to forecast the prognosis of advanced ICC patients receiving chemotherapy combined with immunotherapy. Based on the results of the multivariate Cox regression analysis, LDL-C and HDL-C were selected as variables to construct a nomogram for predicting 1-, 2-, and 3-year survival probabilities. Patients with low HDL-C and high LDL-C scores exhibited higher risk scores, indicating poorer survival rates at 1, 2, and 3 years (Figure 5A).
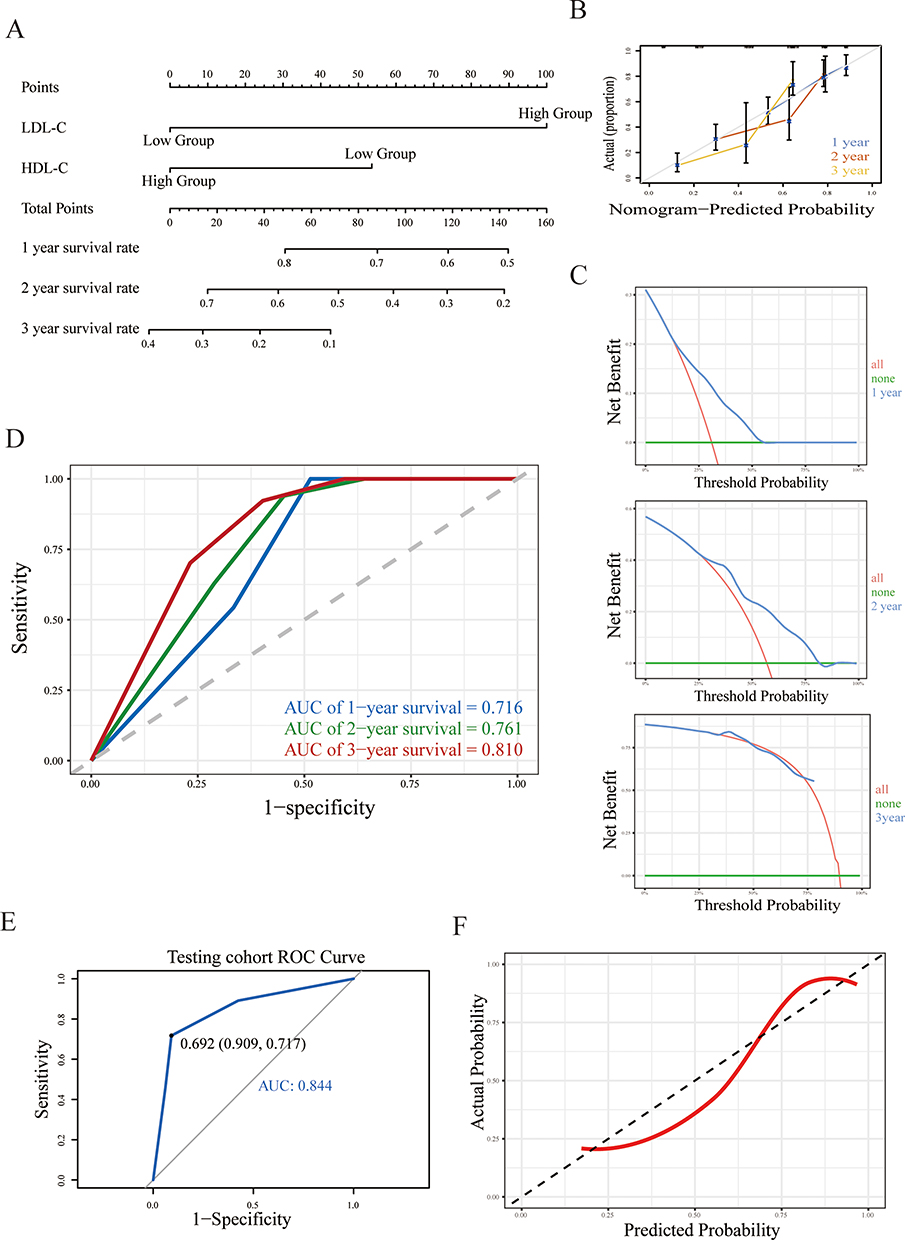 |
Figure 5 Nomogram construction and verification. (A) The nomogram model of OS. (B) Calibration of the model. (C) DCA of the model at 1-year, 2-year and 3-year. (D) A time-ROC curve of the model. (E) A ROC curve of testing cohort. (F) Calibration of the model by testing cohort. Abbreviations: LDL-C, Low-Density Lipoprotein Cholesterol; HDL-C, High-Density Lipoprotein Cholesterol; APOA1, Apolipoprotein A1. |
Subsequently, the nomogram prediction model was validated using calibration curves. Internal validation demonstrated that the C-index for predicting the prognosis of advanced ICC patients receiving immunotherapy was 0.68. The calibration curves for 1-, 2-, and 3-year survival closely approximated the ideal diagonal line (Figure 5B). DCA was performed to evaluate the clinical net benefit, revealing that the DCA models at 1-, 2-, and 3 years remained within the optimal range across certain threshold probabilities, indicating that the prediction model provides meaningful clinical net benefit and has practical clinical utility (Figure 5C). Time-dependent ROC analysis yielded AUCs of 0.716, 0.761, and 0.810 at 1-, 2-, and 3 years, respectively, further supporting the model’s predictive capability (Figure 5D). Moreover, the Hosmer-Leme show goodness-of-fit test resulted in a p-value of 0.1083 (Table S6), indicating no significant systematic bias and an acceptable model fit.
To further validate the clinical utility of the prognostic model, external validation was performed using the testing cohort. Calibration of the model in the testing cohort demonstrated that the calibration curve closely approximated the ideal reference line (Figure 5E). The model’s discriminative ability for external data was assessed by ROC analysis, yielding an AUC of 0.844 with a 95% CI of 0.757–0.931 (Figure 5F). These results indicate that the model possesses robust predictive performance in external datasets.
Discussion
Various biomarkers have been widely applied for prognostic assessment in cancer patients. However, due to high costs and hard in testing, there remains a need to identify biomarkers that are more easily detectable while maintaining high specificity and sensitivity. Lipids play crucial roles in cellular activities.24 Studies have demonstrated that cancer cells within the tumor microenvironment require abundant nutrients to sustain tumor growth. Energy generated solely through glycolysis is insufficient, therefore lipid metabolism is utilized to support rapid proliferation, survival, and metastasis of tumor cells.25 Liquid biopsy-based assessment of peripheral blood lipid profiles has been applied in malignancies such as lung adenocarcinoma and breast cancer. Related investigations have also been conducted in intrahepatic cholangiocarcinoma.14,20,26,27
This study utilized ROC curve analysis to select LDL-C, HDL-C, and ApoA1 as prognostic factors for patients with advanced ICC. Survival analyses based on the training and validation cohorts demonstrated that patients with low LDL-C, high HDL-C, and elevated ApoA1 levels had significantly longer mOS. Regarding PFS, the training cohort showed that patients with low LDL-C and high HDL-C exhibited prolonged mPFS. Although the validation cohort results did not reach statistical significance, the overall trends for these two markers were consistent with the training cohort, likely due to the smaller sample size of the validation cohort. Consistent with our findings, Shu et al reported that postoperative ICC patients with high serum HDL-C derived greater clinical benefit.28 Additionally, Lin et al found that cervical cancer patients exhibited higher LDL-C and lower HDL-C levels compared to healthy controls, and that elevated LDL-C and decreased HDL-C were adverse prognostic factors in this population.29 These findings align with our results, suggesting that increased cancer risk and poor prognosis are associated with low HDL-C and high LDL-C levels. Conversely, another study observed that head and neck squamous cell carcinoma patients with high LDL-C and low ApoA1 levels experienced better PFS.30 This discrepancy may reflect metabolic heterogeneity among different tumor types.
Subsequent Cox regression analyses based on the training and validation cohorts revealed that low LDL-C and low HDL-C as independent protective and risk factors for OS, respectively. Similarly, Shu et al reported that low HDL-C was an independent risk factor for postoperative ICC patients,24 supporting the role of low HDL-C as an independent prognostic indicator in ICC. Additionally, Chen et al identified LDL-C as an independent prognostic factor in non-esophageal squamous cell carcinoma, further confirming the prognostic value of LDL-C in cancer.31 In another study on cervical cancer, patients exhibited elevated LDL-C levels and decreased HDL-C levels compared to healthy controls.29 Conversely, a study on head and neck squamous cell carcinoma found that high LDL-C and low ApoA1 were protective factors.30 These findings suggest heterogeneity in lipid metabolism among different cancer types, with the same serum lipid markers having distinct prognostic implications depending on the tumor context.
Subsequently, LDL-C and HDL-C identified as predictive factors were used to construct a nomogram for predicting 1-, 2-, and 3-year survival rates in advanced ICC patients receiving chemotherapy combined with immunotherapy. The nomogram was internally and externally validated using the training and validation cohorts, respectively, demonstrating robust predictive performance and clinical utility. These findings are consistent with previous studies in thyroid cancer, which also suggest that HDL-C can serve as a prognostic biomarker for cancer.22 Zhu et al constructed a model for predicting the postoperative prognosis of ICC using PIIN, gender, grading, CA19-9, N stage, and tumor quantity.32 By integrating the PIIN score and other clinical risk factors, the PIIN diagram is helpful for personalized prognosis assessment of ICC patients. Ding et al also predicted the postoperative prognosis of ICC through the three-level lymph node structure.33 Similar to our study, the factors used in the aforementioned studies for building the prognosis model are all easily obtainable in clinical practice, but they lack metabolites as building factors, and there is scarce research on prognosis models for advanced ICC treatment. Our study further supplements this aspect of research. In summary, LDL-C and HDL-C may serve as reliable biomarkers for predicting prognosis in patients with advanced ICC.
We envision that in the future, this model could be applied in clinical practice. By measuring the serum lipid profiles of patients prior to chemoimmunotherapy and incorporating these into the nomogram, we could calculate the 1-year, 3-year, and 5-year survival rates. For patients identified as high-risk (ie, those with lower survival rates), lipid-lowering therapy could be administered alongside tumor treatment, with the goal of extending patient survival. The findings of Liu et al also support this approach.18
However, this study has several limitations. First, as a single-center study with a relatively small sample size due to the rarity of cholangiocarcinoma, the conclusions may not fully represent the broader population of advanced ICC patients in China. Future multicenter studies with larger cohorts are needed to validate these findings. Second, serum lipid levels can be influenced by factors such as patient age, sex, hormonal status, and underlying comorbidities; therefore, stricter study controls are required to minimize confounding effects. Third, this study did not investigate the metabolic reprogramming mechanisms underlying the observed alterations in serum lipid profiles, and the causes of lipid level changes remain unclear. Further research will be conducted to explore these underlying mechanisms.
Conclusion
In summary, we successfully constructed and validated a prognostic model to predict the OS of patients with advanced ICC, which provides a more accurate basis for the immunotherapy decision of such patients. The strategy of chemotherapy in combination with immunotherapy dominates in advanced ICC patients, and it is suggested that immunotherapy should be incorporated into clinical treatment protocols more frequently.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author JT.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki (6th revision, 2008). The study protocol was approved by the Ethics Committee of Cancer Hospital of Harbin Medical University (protocol number KY2023-18, approved on 01/11/2023).
Consent to Participate
We have informed all participants why the research is being conducted, whether or not anonymity is assured, and how the data they are collecting is being stored. All of participants have written informed consent for participation.
Acknowledgments
We would like to thank all the infotainment and records rooms for their assistance with this study.
Author Contributions
Chengzhi Jiang and Kaijun Long share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential competing of interest.
This paper has been uploaded to [Sciety-labs] as a preprint: [https://scietylabs.elifesciences.org/articles/by?article_doi=10.21203/rs.3.rs-7803902/v1].
References
1. Qurashi M, Vithayathil M, Khan S. Epidemiology of cholangiocarcinoma. EJSO. 2025;51. doi:10.1016/j.ejso.2023.107064
2. Piha-Paul SA, Oh D-Y, Ueno M, et al. Efficacy and safety of pembrolizumab for the treatment of advanced biliary cancer: results from the KEYNOTE-158 and KEYNOTE-028 studies. Int J Cancer. 2020;147:2190–13. doi:10.1002/ijc.33013
3. Kelley R, Bridgewater J, Gores G, et al. Systemic therapies for intrahepatic cholangiocarcinoma. J Hepatol. 2020;72:353–363. doi:10.1016/j.jhep.2019.10.009
4. Rui R, Zhou L, He S. Cancer immunotherapies: advances and bottlenecks. Front Immunol. 2023;14:1212476. doi:10.3389/fimmu.2023.1212476
5. Raggi C, Taddei ML, Rae C, et al. Metabolic reprogramming in cholangiocarcinoma. J Hepatol. 2022;77:849–864. doi:10.1016/j.jhep.2022.04.038
6. Maurya SK, Chaudhri S, Kumar S, et al. Repurposing of metabolic drugs metformin and simvastatin as an emerging class of cancer therapeutics. Pharm Res. 2025;42:49–67. doi:10.1007/s11095-024-03811-1
7. Ruze R, Liu T, Zou X, et al. Obesity and type 2 diabetes mellitus: connections in epidemiology, pathogenesis, and treatments. Front Endocrinol. 2023;14:1161521. doi:10.3389/fendo.2023.1161521
8. Tang H-Y, Chen A-Q, Zhang H, et al. Vascular smooth muscle cells phenotypic switching in cardiovascular diseases. Cells. 2022;12:11. doi:10.3390/cells11244060
9. Yang J, Shay C, Saba NF, et al. Cancer metabolism and carcinogenesis. Exp Hematol Oncol. 2024;13:10. doi:10.1186/s40164-024-00482-x
10. Sun Y, Cao D, Zhang Y, et al. Appraising associations between signature lipidomic biomarkers and digestive system cancer risk: novel evidences from a prospective cohort study of UK Biobank and Mendelian randomization analyses. Lipids Health Dis. 2024;23:61. doi:10.1186/s12944-024-02053-9
11. Wang S, Huang X, Zhao S, et al. Progressions of the correlation between lipid metabolism and immune infiltration characteristics in gastric cancer and identification of BCHE as a potential biomarker. Front Immunol. 2024;15:1327565. doi:10.3389/fimmu.2024.1327565
12. Duan Y, Deng M, Liu B, et al. Mitochondria targeted drug delivery system overcoming drug resistance in intrahepatic cholangiocarcinoma by reprogramming lipid metabolism. Biomaterials. 2024;309:122609. doi:10.1016/j.biomaterials.2024.122609
13. Qian L, Wang G, Li B, et al. Regulation of lipid metabolism by APOE4 in intrahepatic cholangiocarcinoma via the enhancement of ABCA1 membrane expression. PeerJ. 2024:
14. Lori G, Pastore M, Navari N, et al. Altered fatty acid metabolism rewires cholangiocarcinoma stemness features. JHEP Rep Innov Hepatol. 2024;6:101182. doi:10.1016/j.jhepr.2024.101182
15. Chen Y, Zhou Y, Ren R, et al. Harnessing lipid metabolism modulation for improved immunotherapy outcomes in lung adenocarcinoma. J ImmunoTher Cancer. 2024:12. doi:10.1136/jitc-2024-008811
16. de Gauna M R, Biancaniello F, González-Romero F, et al. Cholangiocarcinoma progression depends on the uptake and metabolization of extracellular lipids. Hepatology. 2022;76:1617–1633. doi:10.1002/hep.32344
17. He T, Wang Z-Y, Xu B, et al. CXCL6 reshapes lipid metabolism and induces neutrophil extracellular trap formation in cholangiocarcinoma progression and immunotherapy resistance. Adv Sci Weinh Baden-Wurtt Ger. 2025:
18. Liu F, Chen W, Zhang Z, et al. Targeting Aurora kinase B regulates cholesterol metabolism and enhances chemoimmunotherapy in cholangiocarcinoma. Gut. 2025:gutjnl–2025–335291. doi:10.1136/gutjnl-2025-335291
19. Liu X, Hartman CL, Li L, et al. Reprogramming lipid metabolism prevents effector T cell senescence and enhances tumor immunotherapy. Sci Transl Med. 2021:13. doi:10.1126/scitranslmed.aaz6314
20. Ma F, Liu X, Zhang Y, et al. Tumor extracellular vesicle-derived PD-L1 promotes T cell senescence through lipid metabolism reprogramming. Sci Transl Med. 2025:17. doi:10.1126/scitranslmed.adm7269
21. Yang K, Wang X, Song C, et al. The role of lipid metabolic reprogramming in tumor microenvironment. Theranostics. 2023;13:1774–1808. doi:10.7150/thno.82920
22. Yuan J, Chen Z, Zhang J, et al. Preoperative serum lipids as novel predictors of survival in 3575 patients with papillary thyroid cancer. J Clin Endocrinol Metab. 2024;110:668–676. doi:10.1210/clinem/dgae601
23. Salgado-Montilla J, Soto Salgado M, Surillo trautmann B, et al. Association of serum lipid levels and prostate cancer severity among Hispanic Puerto Rican men. Lipids Health Dis. 2015;14:111. doi:10.1186/s12944-015-0096-0
24. Yu S-M, Chang X-J, Gu -Y-Y, et al. Serum high-density lipoprotein cholesterol levels predict early recurrence and prognosis of intrahepatic cholangiocarcinoma after surgical resection. Heliyon. 2024:
25. Li X, Jia Y, Li Y, et al. Crosstalk between metabolic reprogramming and microbiota: implications for cancer progression and novel therapeutic opportunities. Front Immunol. 2025. doi:10.3389/fimmu.2025.1582166
26. Bian X, Liu R, Meng Y, et al. Lipid metabolism and cancer. J Exp Med. 2021;218. doi:10.1084/jem.20201606
27. Yu X, Tong H, Chen J, et al. CircRNA MBOAT2 promotes intrahepatic cholangiocarcinoma progression and lipid metabolism reprogramming by stabilizing PTBP1 to facilitate FASN mRNA cytoplasmic export. Cell Death Dis. 2023;14:20. doi:10.1038/s41419-022-05540-y
28. Zhu H, Hu H, Hao B, et al. Insights into a machine learning-based palmitoylation-related gene model for predicting the prognosis and treatment response of breast cancer patients. Technol Cancer Res Treat. 2024;23:15330338241263434. doi:10.1177/15330338241263434
29. Cheng L, Li Z, Zheng Q, et al. Correlation study of serum lipid levels and lipid metabolism-related genes in cervical cancer. Front Oncol. 2024:14. doi:10.3389/fonc.2024.1384778
30. Wang S, Wang L, Li H, et al. Correlation analysis of plasma lipid profiles and the prognosis of head and neck squamous cell carcinoma. Oral Dis. 2024;30:329–341. doi:10.1111/odi.14456
31. Chen S, Li X, Wen X, et al. Prognostic nomogram integrated baseline serum lipids for patients with non-esophageal squamous cell carcinoma. Ann Transl Med. 2019;7:548. doi:10.21037/atm.2019.09.86
32. Zhu J, Wang D, Liu C, et al. Development and validation of a new prognostic immune-inflammatory-nutritional score for predicting outcomes after curative resection for intrahepatic cholangiocarcinoma: a multicenter study. Front Immunol. 2023;14:1165510. doi:10.3389/fimmu.2023.1165510
33. Ding G-Y, Ma J-Q, Yun J-P, et al. Distribution and density of tertiary lymphoid structures predict clinical outcome in intrahepatic cholangiocarcinoma. J Hepatol. 2022;76:608–618. doi:10.1016/j.jhep.2021.10.030
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Construction and Validation of TACE Therapeutic Efficacy by ALR Score and Nomogram: A Large, Multicenter Study
Li H, Guo L, Su K, Li C, Jiang Y, Wang P, Chen J, Wu Z, Xu K, Gu T, Zeng H, He K, Chi H, Zhao W, Han L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:1009-1017
Published Date: 29 June 2023
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024
Clinical Significance and Molecular Annotation for PD-L1 Negative Advanced Non-Small Cell Lung Cancer with Sensitivity to Responsive to Dual PD-1/CTLA-4 Blockade
Wang L, Liu L, Zhao J, Yu X, Su C
ImmunoTargets and Therapy 2024, 13:435-445
Published Date: 6 September 2024
Prognostic Value of Inflammatory and Nutritional Markers in Advanced Esophageal Squamous Cell Carcinoma Treated with Immunotherapy: A Retrospective Cohort Study
Liu X, Ren S, Li X, Cheng X, Fang Y, Zhang S, Zhao Y, Ma W, Zhang T
Journal of Inflammation Research 2025, 18:15393-15408
Published Date: 4 November 2025
Prognostic Nomogram for Hepatocellular Carcinoma Patients with High Systemic Immune-Inflammation Index: Validation in Surgical and Immunotherapy Cohorts and Exploration of Immune Microenvironment Mechanisms
Wang X, Hu Z, Ding J, Zheng S, Wei B, Zhou Y, Wang S
Journal of Hepatocellular Carcinoma 2026, 13:588390
Published Date: 30 March 2026