Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Second-Generation Long-Acting Injectable Antipsychotics: A Comprehensive Assessment of Effectiveness, Safety, and Cost
Authors Ifteni P ![]() , Petric PS
, Petric PS ![]() , Popa AV, Teodorescu A
, Popa AV, Teodorescu A ![]() , Georgescu R, Manea MC
, Georgescu R, Manea MC
Received 16 March 2026
Accepted for publication 27 May 2026
Published 20 June 2026 Volume 2026:22 606817
DOI https://doi.org/10.2147/NDT.S606817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Taro Kishi
Petru Ifteni,1,2 Paula-Simina Petric,1,2 Andreea Violeta Popa,1,2 Andreea Teodorescu,1,2 Radu Georgescu,3 Mihnea Costin Manea4,5
1Faculty of Medicine, Transilvania University of Brașov, Brașov, Romania; 2Clinical Hospital of Psychiatry and Neurology in Brașov, Brașov, Romania; 3Faculty of Medicine, “Iuliu Hațieganu” University of Medicine and Pharmacy of Cluj-Napoca, Cluj-Napoca, Romania; 4Faculty of Medicine, “Carol Davila” University of Medicine and Pharmacy of Bucharest, Bucharest, Romania; 5“Prof. Dr. Alexandru Obregia” Clinical Psychiatry Hospital, Bucharest, Romania
Correspondence: Paula-Simina Petric, Faculty of Medicine, Transilvania University of Brașov, Brașov, Romania, Email [email protected]
Background: Second-generation long-acting injectable antipsychotics (SG-LAIs) improve adherence, reduce relapse, and enhance outcomes in schizophrenia, yet remain underused. In Romania, data on psychiatrists’ views is limited.
Objective: To assess Romanian psychiatrists’ attitudes and prescribing behaviors regarding SG-LAIs, and identify key drivers and barriers to their use.
Methods: We conducted a cross-sectional questionnaire survey among psychiatrists in urban hospital, outpatient, and private settings, treating more than 1,000 patients with schizophrenia. The survey rated the four SG-LAIs available in Romania (aripiprazole, olanzapine, paliperidone, and risperidone) on efficacy, tolerability, dosing flexibility, monitoring needs, prescribing frequency, and perceived obstacles/facilitators.
Results: 80 psychiatrists participated. Aripiprazole LAI received the most favorable ratings, ranking highest for efficacy, safety, patient functioning, ease of administration, guideline alignment, side-effect profile, monitoring requirements, and overall preference. Paliperidone and risperidone were also positively evaluated for dosing versatility, whereas olanzapine generally scored lowest. Main factors encouraging LAI prescription were improved adherence (96.3%) and reduced relapse risk (96.3%), followed by a favorable clinical profile (66.3%). Key barriers included lack of patient trust (57.5%), lack of hospital supply (43.8%), absence of LAI formulations for certain antipsychotics (43.8%), and limited experience (36.3%).
Conclusion: Romanian psychiatrists show a strong preference for aripiprazole LAI, with decisions driven mainly by clinical benefits. Reducing patient concerns and system-level limitations—especially availability, indications, and communication— may support increased use of SG-LAIs in everyday clinical care.
Keywords: schizophrenia, adherence, relapse, long-acting injectable antipsychotics, efficacy, safety
Background
Schizophrenia is a chronic psychiatric illness characterized by recurrent psychotic episodes and functional decline when untreated. Antipsychotic medication represents the primary therapeutic approach, and sustained adherence contributes to long-term clinical stability and relapse prevention.1 Long-acting injectable antipsychotics (LAIs) were developed in the 1960s as a strategy to improve adherence by providing a slow, sustained release of medication, thereby reducing the need for oral drugs.2 In the early 2000s, second-generation (atypical) LAIs became available, including depot formulations of risperidone, paliperidone, olanzapine, and aripiprazole.3 By ensuring continuous drug delivery, LAIs can achieve more consistent therapeutic levels. Real-world studies have linked LAI use with greater treatment adherence and lower rates of relapse and hospitalization compared to oral antipsychotics.4 LAI-treated patients also show reduced mortality and fewer emergency visits, reflecting the benefits of sustained adherence.5
Despite these advantages, LAIs remain underutilized in clinical practice worldwide. In the United States of America, fewer than 15% of patients with schizophrenia receive an LAI prescription,4 and across Europe the proportion of patients on LAIs generally remains below 30%.1 This under-prescription of LAIs has multiple contributing factors, often centered around prescriber attitudes.6 Surveys indicate that many clinicians viewed LAIs as a last resort option – reserving them for patients with very severe illness or those with established nonadherence to oral medication.7 Such practice is at odds with expert recommendations and treatment guidelines, which advocate for broader and earlier use of LAIs when appropriate. The gap between evidence-based benefits of LAIs and their real-world prescribing frequency suggests that attitudinal and systemic barriers play a significant role.8
Research efforts have sought to understand why clinicians do not prescribe LAIs more frequently. Common barriers identified include limited clinician experience or lack of confidence in managing LAI treatments, concerns about the logistics of administering injectables (such as medication storage and the need for staff to give injections), and an expectation that patients will be unwilling or fearful to receive injections.9 Some prescribers also think that LAIs are more costly or produce more side effects than oral antipsychotics.10 These reservations reflect a combination of clinician-, system-, and patient-related factors: limited prescriber familiarity, restricted availability or reimbursement policies, and patient concerns about cost, understanding of treatment, or negative attitudes toward injections. Together, these influences help explain the persistent hesitation to use LAIs despite their proven clinical benefits.1,4
At the same time, not all clinicians are hesitant to use LAIs. Attitudes toward LAI antipsychotics vary widely across practitioners. For example, a recent survey from USA found that roughly one-third actively use LAIs as early as possible in appropriate patients, whereas about 15% remain generally hesitant to use LAIs at all.4,11 The remaining clinicians tended to fall in between – often preferring to initiate LAIs only for patients with more severe courses of illness or clear nonadherence issues.11 These findings underscore that prescriber mindsets range from very proactive to quite cautious regarding LAI use. Understanding where a given group of clinicians stands on this spectrum is important, as their mindset can impact patient access to LAI therapy and ultimately patient outcomes.12
In Romania, the use of long-acting injectable antipsychotics (LAIs) in psychiatric practice has not been extensively investigated, even though similar implementation challenges are likely present. Available data indicate that the utilization of depot antipsychotics has increased steadily in recent years, with national consumption of long-acting formulations approximately doubling between 2015 and 2018.13 Although structural and policy-related factors can, in some contexts, limit wider adoption, the Romanian healthcare system provides full reimbursement for LAIs for insured patients with schizophrenia—representing over 80% of all individuals with this diagnosis—meaning that, in most cases, cost does not represent a barrier to access.
Despite this favorable reimbursement framework, the absence of widely disseminated national guidelines specifically addressing LAI prescribing may contribute to variability in clinical practice. Clinicians may therefore rely on international recommendations or personal clinical experience, making individual attitudes and levels of confidence with LAIs particularly influential.14–16 This gap is reflected in the limited research examining Romanian psychiatrists’ perspectives on the use of LAIs, aligning with a broader lack of data on prescriber attitudes in Eastern Europe.16
Given the substantial clinical benefits associated with second-generation LAIs—including improved adherence,17 reduced relapse rates,18 and more favorable long-term outcomes19—their earlier and broader use is increasingly emphasized in international treatment guidelines. Nevertheless, real-world implementation remains inconsistent and appears to be shaped as much by clinician perceptions and local healthcare system dynamics as by the available evidence base.20,21 In countries like Romania, where treatment access is largely ensured and financial barriers are minimal, exploring psychiatrists’ attitudes is particularly relevant for identifying the remaining facilitators and obstacles that influence the integration of LAIs into routine clinical practice.
This aim of this study is to contribute to the limited literature on clinician perspectives in Eastern Europe by examining the attitudes of Romanian psychiatrists toward second-generation LAIs. By doing so, it aims to inform targeted strategies for optimizing the use of these treatment options in psychiatric practice.
Methods
Study Design
This is a cross-sectional, questionnaire-based study conducted among Romanian psychiatrists to assess their attitudes toward second-generation long-acting injectable antipsychotics. The data collection was carried out between January 1st, 2025, to July 31st, 2025. Participation in the study was voluntary and anonymous.
Study Population
A total of 100 psychiatrists were invited to participate in the study. Of these, 20 responses were excluded because the completed questionnaires were not submitted within the required timeframe (1 month). The final sample consisted of 80 psychiatrists whose responses met the inclusion criteria and were included in the analysis.
Participants represented all major clinical settings, including psychiatric hospitals, general hospitals with psychiatric wards, outpatient mental health centers, and private practice. All respondents were board-certified psychiatrists actively involved in the prescription and management of antipsychotic treatments for adult patients, each overseeing a caseload of more than 100 patients per month.
Notably, this study did not involve patients or patient-level clinical data but was based exclusively on the opinions of practicing psychiatrists. Participation consisted of completing an anonymous questionnaire designed to explore clinicians’ perspectives on the use of second-generation long-acting injectable antipsychotics. Invitations to participate were distributed through professional networks, and respondents completed the survey voluntarily. No personal identifiers were collected, and the investigators did not have access to participants’ personal contact information. All responses were recorded anonymously and analyzed only in aggregated form. The study was conducted in accordance with applicable data protection regulations and ethical standards for survey-based research involving healthcare professionals.
Inclusion and Exclusion Criteria
Inclusion criteria were: certified psychiatrists currently practicing in Romania, actively involved in treating patients with schizophrenia or other psychotic disorders. Exclusion criteria included incomplete questionnaire responses or professionals not involved in prescribing antipsychotic medication.
Data Collected
Data were collected using a structured questionnaire developed specifically for the purpose of this research. The instrument comprised both single/multiple-choice items and rating-scale questions. The single/multiple-choice items explored domains such as:
- Frequency and context of prescribing LAIs
- Reasons for choosing LAIs in clinical practice
- Perceived obstacles and facilitators influencing the use of LAIs
In the rating-scale section, participants were asked to evaluate and compare the four second-generation long-acting injectable antipsychotics currently available in Romania—aripiprazole LAI, olanzapine LAI, paliperidone LAI, and risperidone LAI—across several dimensions, including:
- Perceived efficacy
- Safety profile
- Patient functionality outcomes
- Ease of administration
- Number and severity of side effects
- Versatility in dosing
- Monitoring requirements post-administration
- Alignment with treatment guidelines and prescribing protocols
Each of these attributes was rated on a structured scale (from 1 to 4, where 1 = most favorable, 2 = somewhat favorable, 3 = somewhat unfavorable, 4 = least favorable), allowing for comparative analysis of clinician preferences. An overall ranking of the four antipsychotics was also requested. Additionally, the questionnaire gathered demographic and professional information such as clinical experience and primary workplace (eg., hospital, outpatient unit, private practice).
Statistical Analysis
Data were analyzed using SPSS version 20.00. Descriptive statistics were used to summarize participant characteristics and response frequencies. For categorical variables, results were presented as absolute numbers and percentages. For continuous variables, means and standard deviations were reported. A significance threshold of p < 0.05 was used throughout. Qualitative responses to open-ended questions were categorized thematically and analyzed using basic content analysis techniques.
Results
Participant Characteristics
The study sample included a total of 80 psychiatrists practicing in urban areas across Romania. As shown in Table 1, the majority were senior psychiatrists (n = 56; 70%), while the remaining 24 (30%) were specialist psychiatrists. Regarding workplace distribution, most respondents were affiliated with psychiatric hospitals (n = 37; 46.25%), followed by outpatient clinics (n = 21; 26.25%), psychiatric wards within general hospitals (n = 12; 15%), and private practices (n = 10; 12.5%). Several participants reported working in more than one clinical setting.
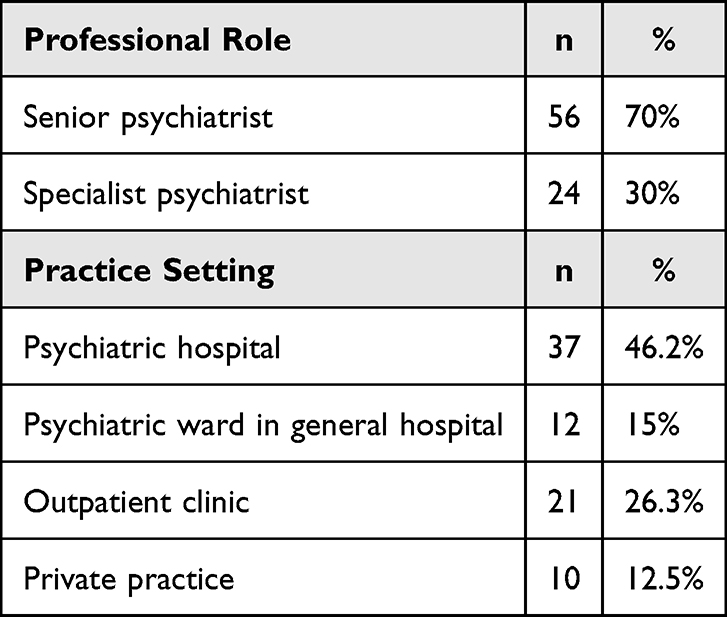 |
Table 1 Participant Characteristics (N = 80) |
Frequency of LAI Prescription
As illustrated in Figure 1, nearly half of the respondents (45%) reported prescribing long-acting injectable antipsychotics frequently, defined as administering them on a daily basis in their clinical practice. A similar proportion (43.75%) indicated occasional use, referring to prescription of LAIs approximately one to two times per month. Only a small minority (10%) reported rare use, defined as prescribing LAIs once or twice every six months. These findings indicate that while LAIs are integrated into the regular practice of many Romanian psychiatrists, a substantial proportion still limits their use to more occasional contexts.
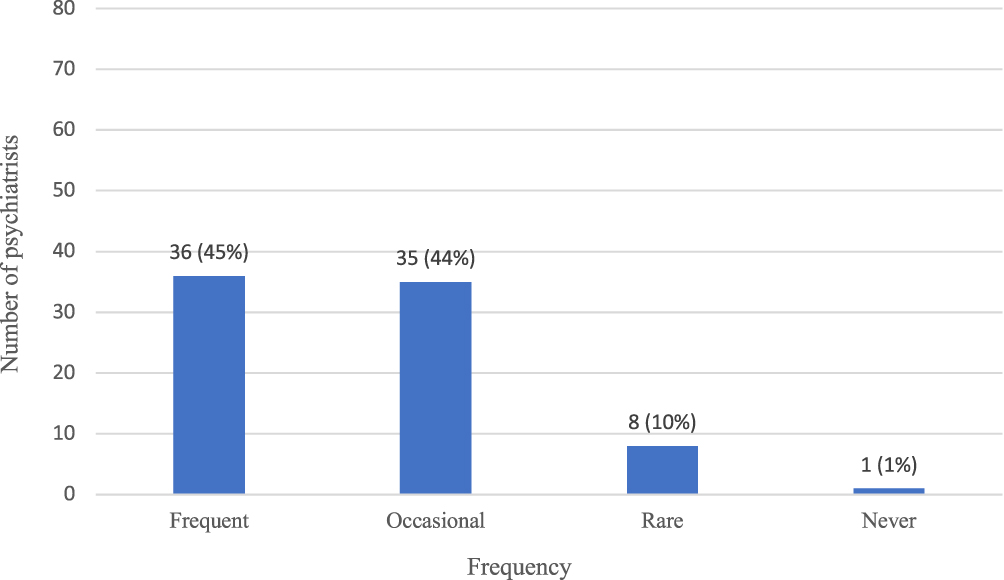 |
Figure 1 Frequency of LAI prescription. |
Psychiatrists’ Perceptions of SG-LAIs
Statistically significant differences were found in the perceived efficacy of the four SG-LAIs (Table 2). Aripiprazole received the most favorable efficacy rating (Mean = 2.06, SD = 1.14), being rated significantly better than olanzapine (Mean = 2.78, SD = 1.17; p < 0.001), paliperidone (Mean = 2.76, SD = 1.02; p < 0.001), and risperidone (Mean = 2.40, SD = 1.00; p < 0.05). No significant difference was observed between olanzapine and paliperidone (p = 0.91), indicating similar perceived efficacy. However, risperidone was rated significantly more favorable than both olanzapine and paliperidone (p < 0.05). In summary, aripiprazole was perceived as the most effective, followed by risperidone, while olanzapine and paliperidone received the least favorable efficacy ratings.
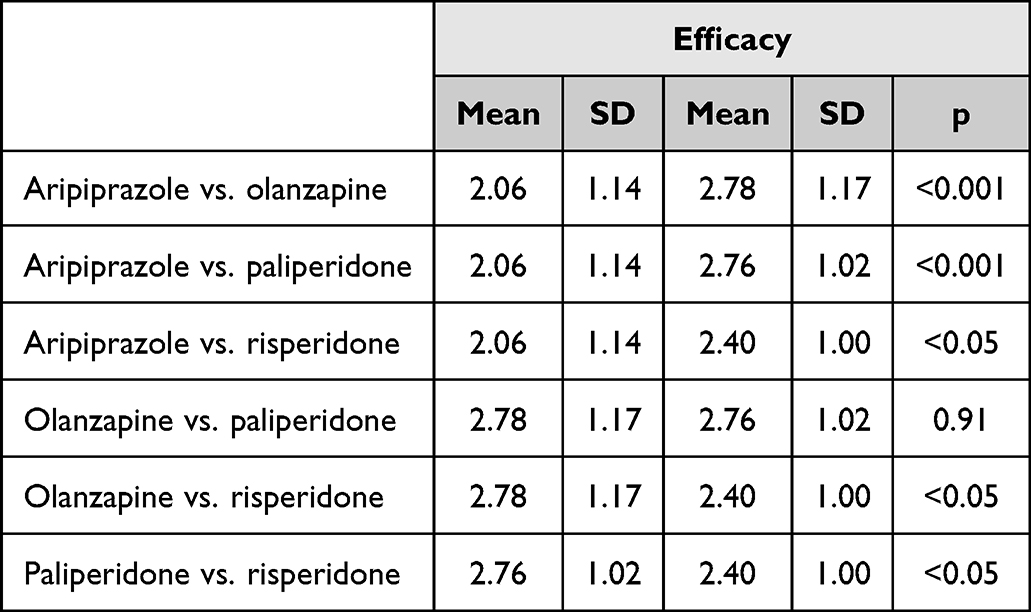 |
Table 2 Perceived Efficacy of SG-LAIs |
Clear differences emerged in psychiatrists’ perceptions of safety across the evaluated SG-LAIs (Table 3). Aripiprazole was rated as the safest formulation, receiving the lowest (most favorable) mean safety score (Mean = 1.51, SD = 0.99). This score was significantly better than those for olanzapine (Mean = 3.25, SD = 1.11; p < 0.001), paliperidone (Mean = 2.43, SD = 0.74; p < 0.001), and risperidone (Mean = 2.81, SD = 0.80; p < 0.001). Among the remaining LAIs, paliperidone was perceived as significantly safer than olanzapine (p < 0.001), but less safe than risperidone (p < 0.001). Additionally, risperidone was perceived as safer than olanzapine (p < 0.01). In summary, aripiprazole was considered the safest LAI, while olanzapine received the least favorable safety ratings.
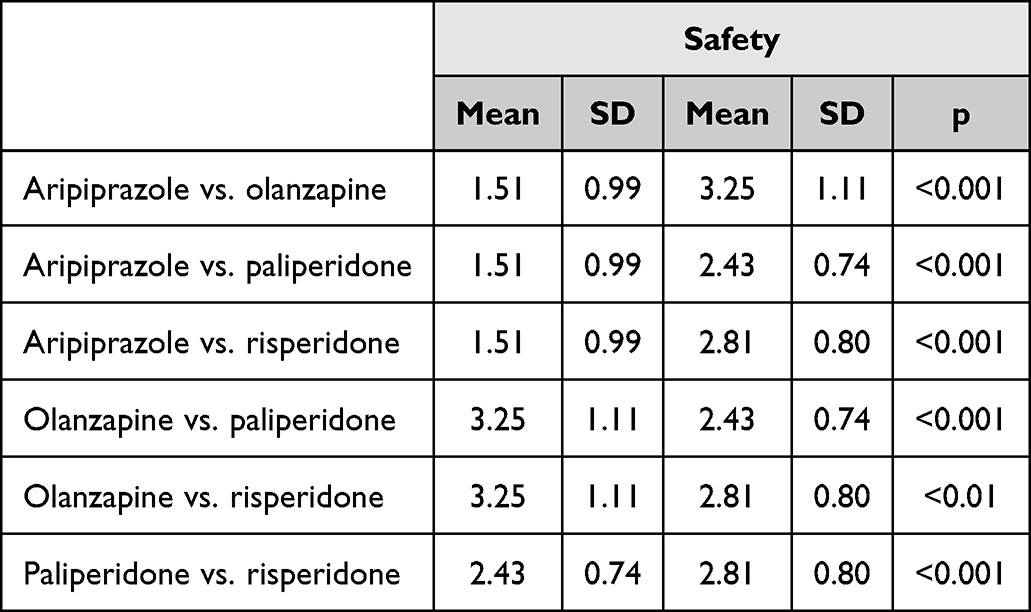 |
Table 3 Perceived Safety of SG-LAIs |
Statistically significant differences were observed in the perceived ability of SG-LAIs to support patient functionality (Table 4). Aripiprazole received the most favorable ratings (Mean = 1.64, SD = 1.08), significantly outperforming olanzapine (Mean = 2.91, SD = 1.00; p < 0.001), paliperidone (Mean = 2.58, SD = 0.94; p < 0.001), and risperidone (Mean = 2.88, SD = 0.97; p < 0.001). Between the other formulations, paliperidone was rated more favorably than olanzapine (p < 0.05) and risperidone (p < 0.05), while olanzapine and risperidone showed no significant difference. Overall, aripiprazole was perceived as the most beneficial for maintaining or improving patient functionality, followed by paliperidone, with olanzapine and risperidone receiving less favorable evaluations.
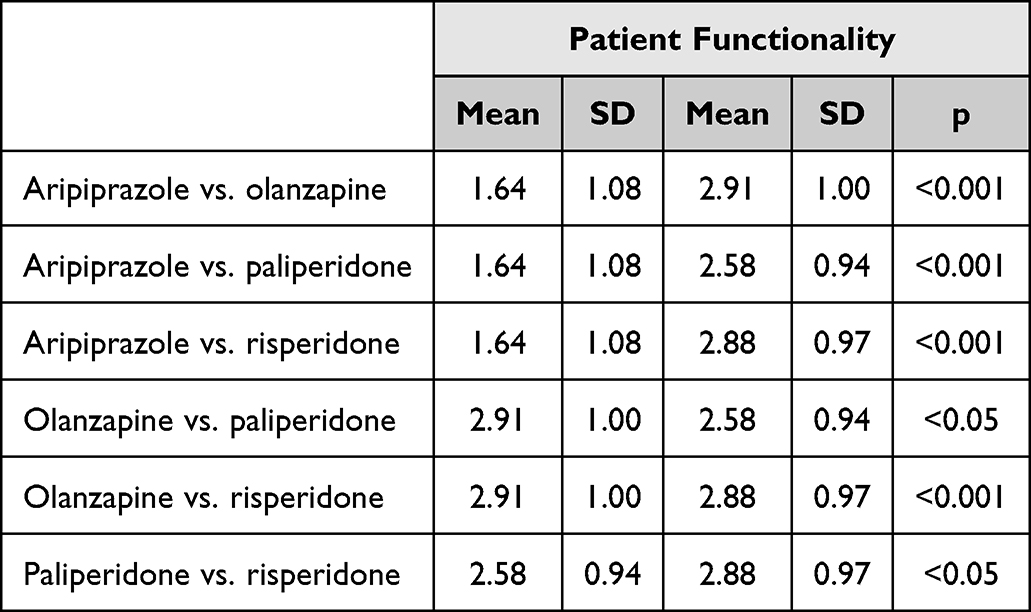 |
Table 4 Perceived Ability of SG-LAIs to Support Patient Functionality |
There were statistically significant differences in psychiatrists’ ratings of ease of administration across the four SG-LAIs (Table 5). Aripiprazole was rated as the easiest to administer, with the lowest (most favorable) mean score (Mean = 1.61, SD = 0.92). This rating was significantly better than those for olanzapine (Mean = 3.29, SD = 1.09; p < 0.001), paliperidone (Mean = 2.38, SD = 0.93; p < 0.001), and risperidone (Mean = 2.73, SD = 0.83; p < 0.001). Among the remaining LAIs, paliperidone was rated easier to administer than olanzapine (p < 0.001) and risperidone (p < 0.001), while risperidone was also rated easier to administer than olanzapine (p = 0.0003). Overall, aripiprazole emerged as the most favorably perceived in terms of ease of administration, while olanzapine received the least favorable evaluations.
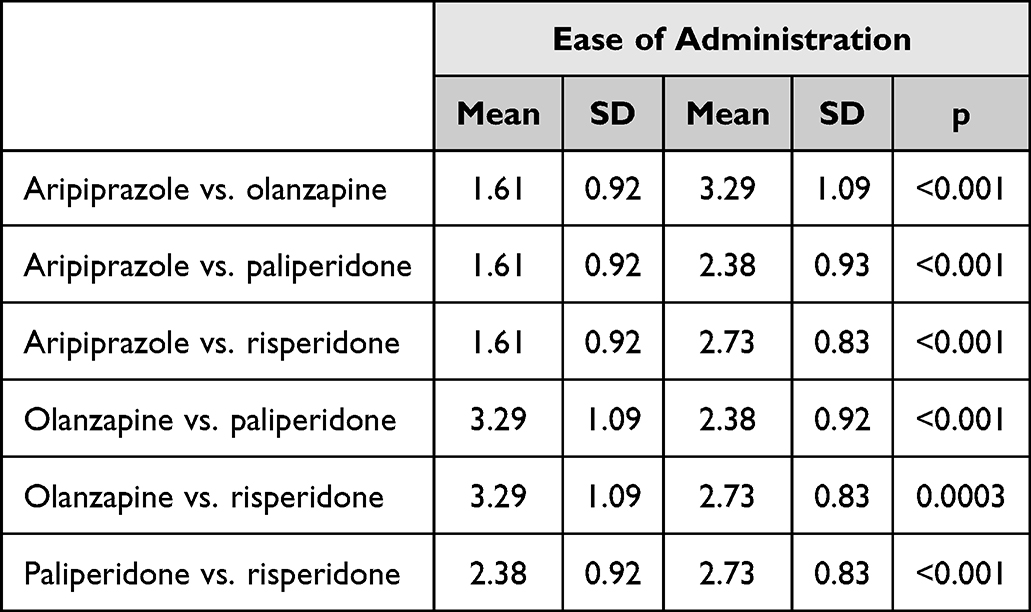 |
Table 5 Perceived Ease of Administration |
Psychiatrists’ perceptions of cost varied significantly between the evaluated SG-LAIs (Table 6). Risperidone was perceived as the most cost-favorable option, with the lowest mean score (Mean = 1.91, SD = 1.08). It was rated significantly better than aripiprazole (Mean = 2.29, SD = 1.09; p = 0.02), olanzapine (Mean = 2.68, SD = 1.04; p < 0.001), and paliperidone (Mean = 3.13, SD = 0.89; p < 0.001). Aripiprazole was perceived as significantly more cost-favorable than olanzapine (Mean = 2.68, SD = 1.04; p = 0.02) and paliperidone (p < 0.001). Olanzapine was rated more favorably in terms of cost than paliperidone (p = 0.005). Overall, risperidone was considered the most affordable, followed by aripiprazole, with paliperidone receiving the least favorable cost ratings.
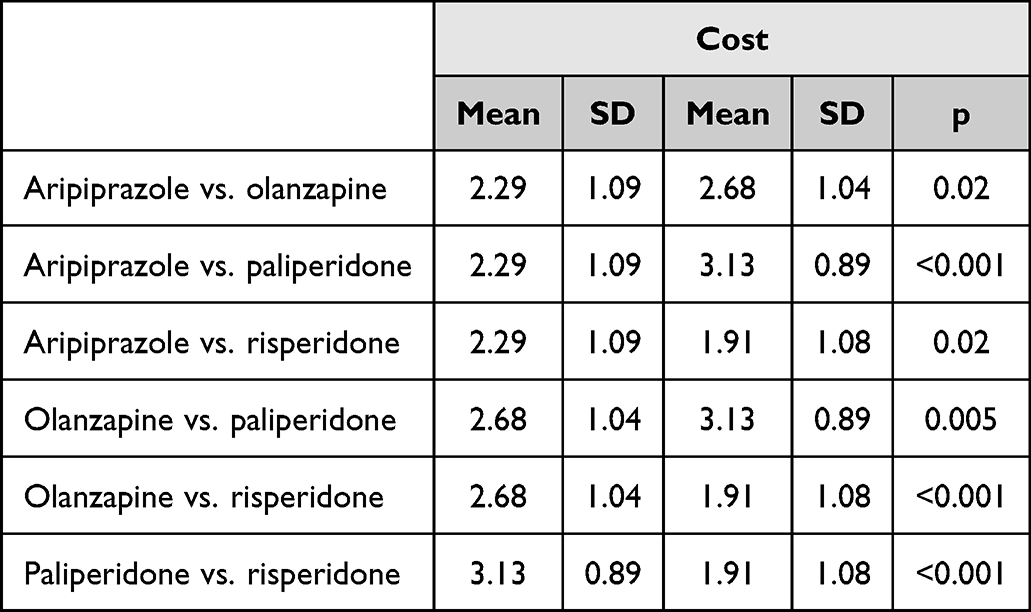 |
Table 6 Perceived Cost |
Ratings of guideline alignment showed statistically significant differences between several SG-LAIs (Table 7). Aripiprazole was perceived as the most favorably included in prescribing protocols, with the lowest mean score (Mean = 1.70, SD = 1.04), significantly outperforming olanzapine (Mean = 2.70, SD = 1.06; p < 0.001), paliperidone (Mean = 2.98, SD = 0.98; p < 0.001), and risperidone (Mean = 2.63, SD = 0.99; p < 0.001). No significant difference was found between olanzapine and paliperidone (p = 0.08) or between olanzapine and risperidone (p = 0.66). However, risperidone was rated more favorably than paliperidone (p = 0.0260). Overall, aripiprazole was viewed as having the strongest alignment with prescribing protocols, while paliperidone was perceived least favorably in this regard.
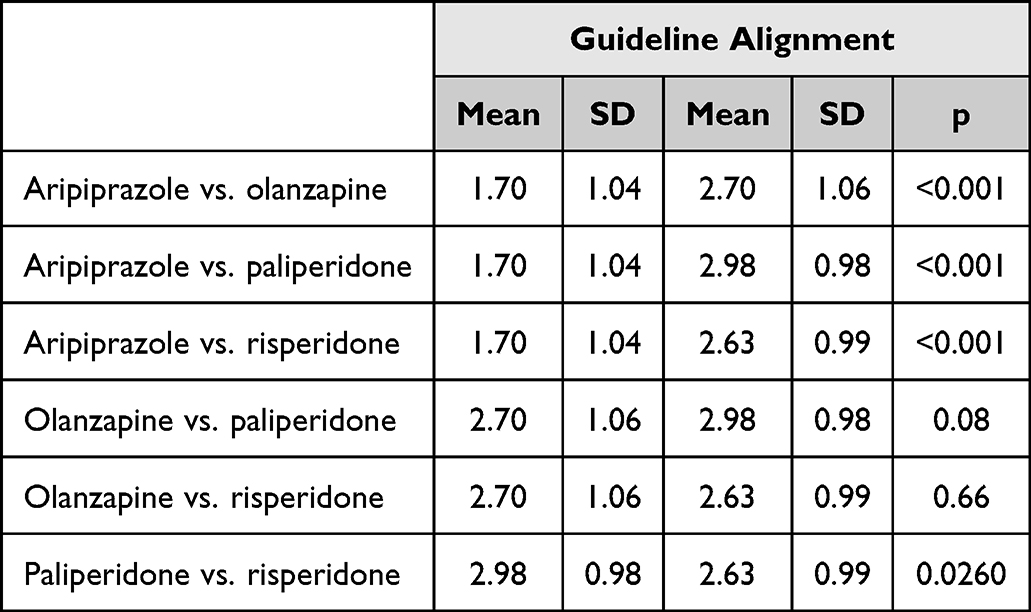 |
Table 7 Perceived Inclusion in Prescribing Protocols |
There were significant differences in psychiatrists’ ratings of the side effect burden among SG-LAIs (Table 8). Aripiprazole received the most favorable evaluation, with the lowest mean score (Mean = 1.28, SD = 0.69), indicating it was perceived as having the fewest side effects. This rating was significantly better than those for olanzapine (Mean = 3.39, SD = 0.88; p < 0.001), paliperidone (Mean = 2.35, SD = 0.71; p < 0.001), and risperidone (Mean = 2.99, SD = 0.85; p < 0.001). Among the other formulations, paliperidone was rated more favorably than olanzapine (p < 0.001) and risperidone (p < 0.001), while risperidone was perceived as having fewer side effects than olanzapine (p = 0.004). Overall, aripiprazole was viewed as the most tolerable, whereas olanzapine received the least favorable ratings in terms of side effect profile.
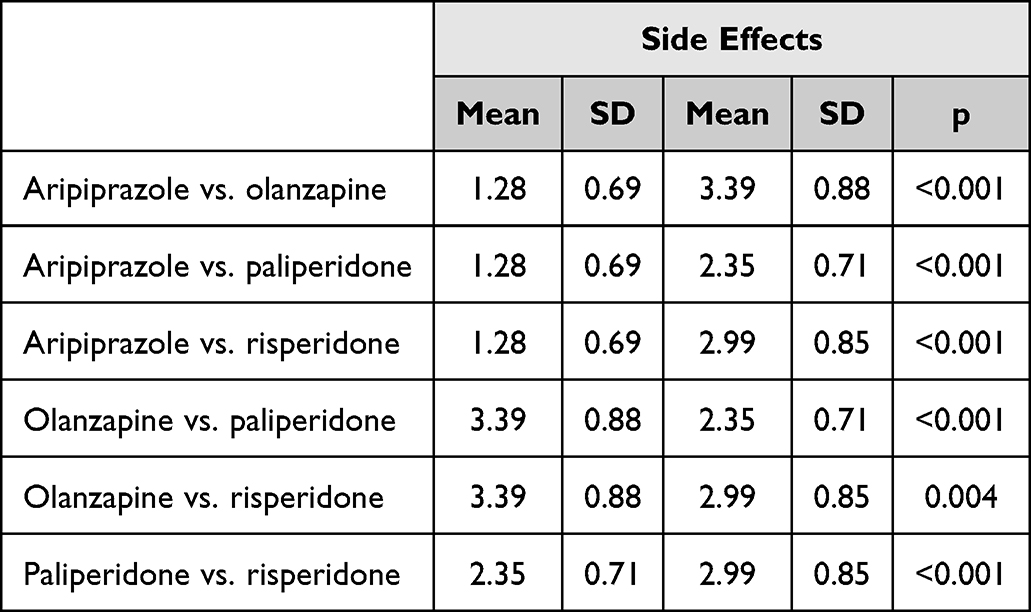 |
Table 8 Perceived Side Effect Profile |
Significant differences were observed between SG-LAIs regarding the amount of monitoring required after administration (Table 9). Aripiprazole received the most favorable rating, with the lowest mean score (Mean = 1.26, SD = 0.65), indicating it was perceived as requiring the least post-administration monitoring. This score was significantly better than those for olanzapine (Mean = 3.60, SD = 0.76; p < 0.001), paliperidone (Mean = 2.31, SD = 0.82; p < 0.001), and risperidone (Mean = 2.83, SD = 0.69; p < 0.001). Among the remaining agents, paliperidone was perceived as requiring less monitoring than olanzapine (p < 0.001) and risperidone (p < 0.001), while risperidone was also rated more favorably than olanzapine (p < 0.001). Overall, aripiprazole was viewed as the easiest to manage in terms of monitoring requirements, whereas olanzapine was perceived as the most demanding in this regard.
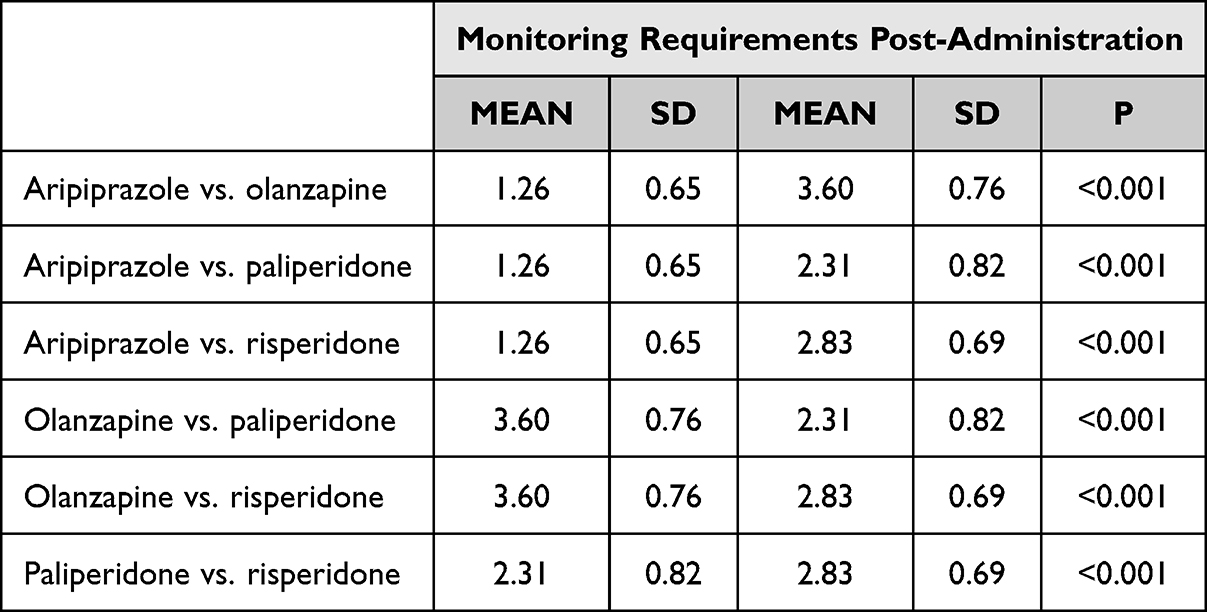 |
Table 9 Perceived Monitoring Requirements Post-Administration |
Psychiatrists’ ratings of dosing versatility revealed several statistically significant differences between SG-LAIs (Table 10). Paliperidone and risperidone were perceived as the most versatile, each receiving a mean score of 2.39 (SD = 1.14 and SD = 0.97, respectively), with no significant difference between them (p = 1). Both were rated significantly better than olanzapine (Mean = 2.96, SD = 1.07; p = 0.0014 and p = 0.0005, respectively). Aripiprazole received a mean score of 2.26 (SD = 1.17), which was significantly more favorable than olanzapine (p < 0.001) but not significantly different from paliperidone (p = 0.47) or risperidone (p = 0.44). Overall, paliperidone, risperidone, and aripiprazole were rated similarly and more favorably for dosing versatility, while olanzapine received the least favorable evaluation in this category.
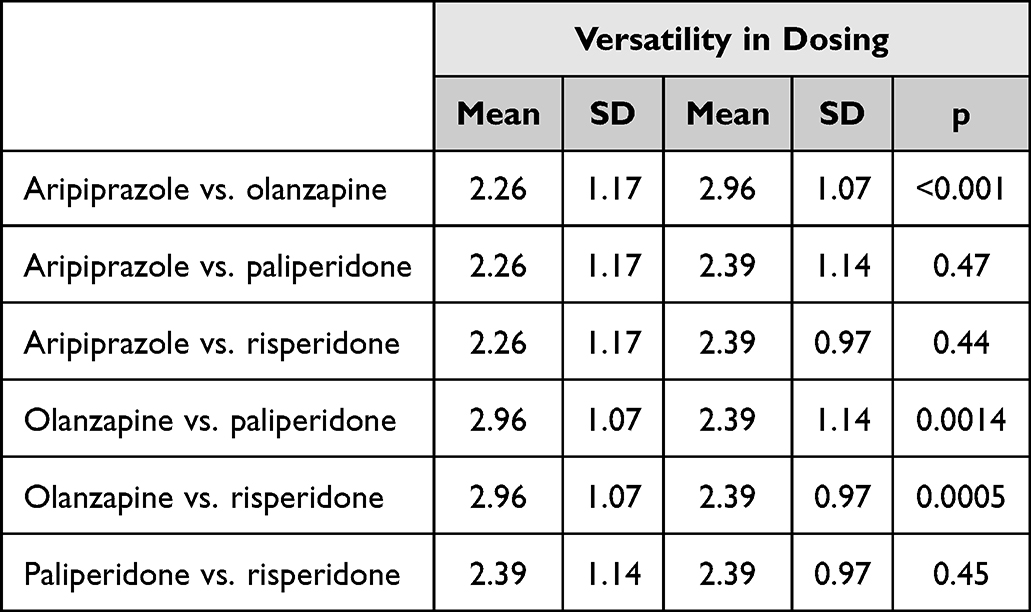 |
Table 10 Perceived Versatility in Dosing |
In the overall ranking, statistically significant differences emerged between the SG-LAIs (Table 11). Aripiprazole achieved the most favorable position, with the lowest mean score (Mean = 1.44, SD = 0.78), outperforming olanzapine (Mean = 3.01, SD = 1.02; p < 0.001), paliperidone (Mean = 2.76, SD = 0.98; p < 0.001), and risperidone (Mean = 2.79, SD = 0.94; p < 0.001). No statistically significant differences were found among olanzapine, paliperidone, and risperidone in their overall scores (p > 0.05). Aripiprazole was the top choice among respondents, while the remaining three formulations were rated similarly and less favorably.
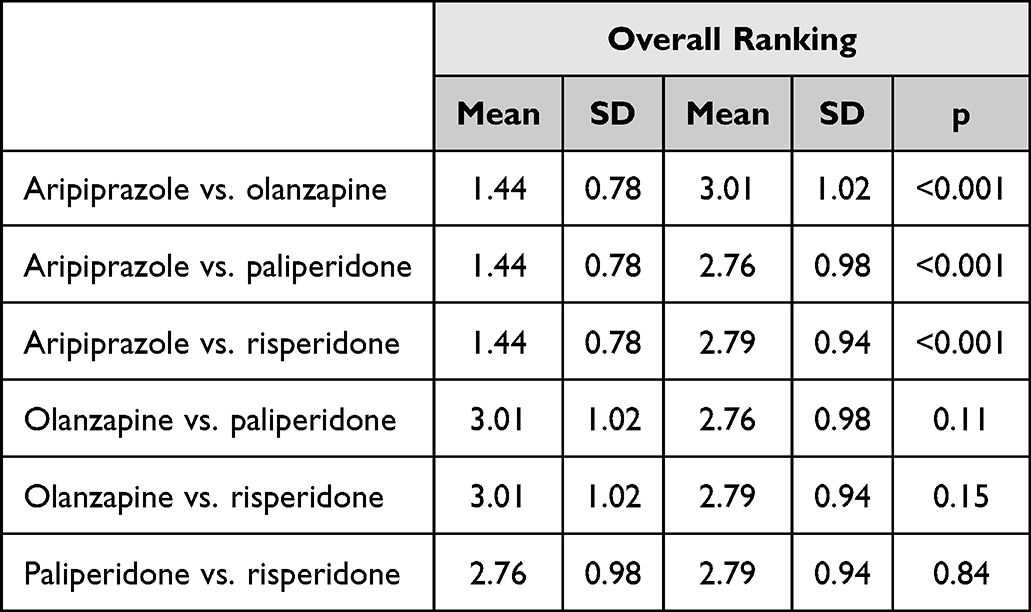 |
Table 11 Overall Ranking of SG-LAIs |
As shown in Figure 2, aripiprazole LAI consistently received the most favorable ratings across nearly all domains, particularly in efficacy, safety, ease of administration, and overall preference. Risperidone LAI scored favorably for cost, while paliperidone LAI occupied intermediate positions across most parameters. In contrast, olanzapine LAI was rated least favorably overall, primarily due to safety concerns, metabolic side effects, and post-injection monitoring requirements.
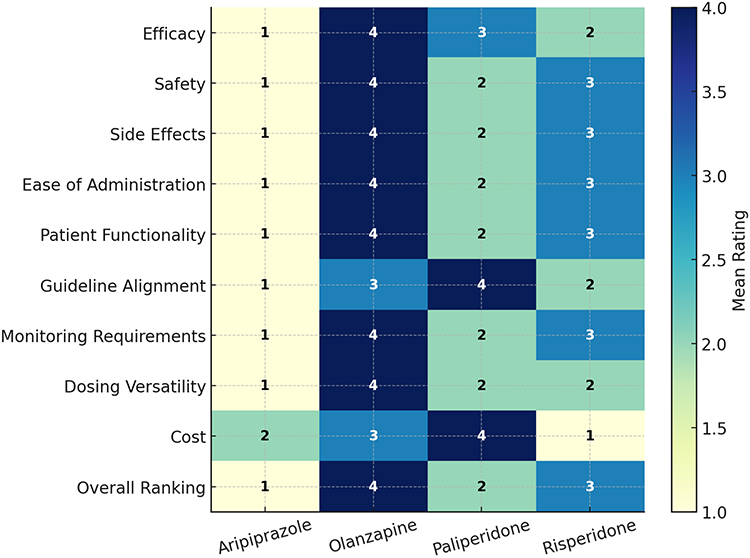 |
Figure 2 Overall ratings of SG-LAIs across key domains (1 = most favorable, 4 = least favorable). |
Factors Influencing the Prescription of SG-LAIs
When asked about factors that encourage the prescription of SG-LAIs, participants could select multiple answers. The most frequently reported factors were increased patient adherence and reduced risk of relapse, each cited by 77 respondents (96.3%). A favorable clinical profile was mentioned by 53 respondents (66.3%). Factors related to patient or caregiver input, such as patient/caregiver preference, were reported by 28 respondents (35.0%), while compliance with clinical guidelines was noted by 29 respondents (36.3%). Availability of treatment through the national health program was selected by 27 respondents (33.8%). These results indicate that clinical considerations—particularly adherence and relapse prevention—are the primary motivators for prescribing LAIs, whereas logistical aspects and patient preference, although relevant, are less frequently prioritized. (Figure 3).
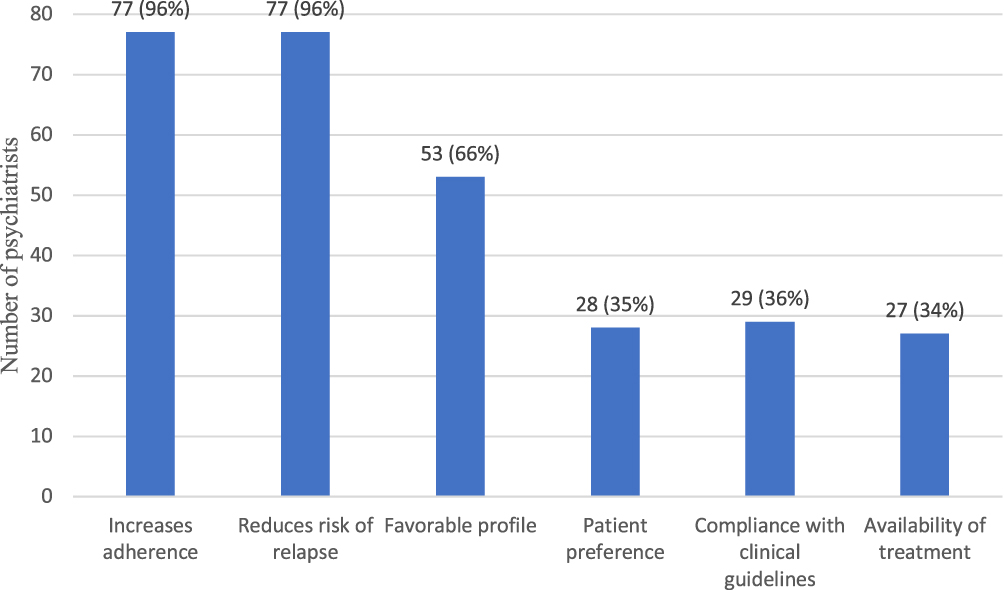 |
Figure 3 Factors encouraging the prescription of SG-LAIs. |
Participants could select multiple options when identifying barriers to prescribing SG-LAIs. The most frequently reported obstacle was lack of patient trust, cited by 46 respondents (57.5%). Absence from hospital supply and lack of LAI formulations for certain antipsychotics were each mentioned by 35 respondents (43.8%). Lack of experience in use was reported by 29 respondents (36.3%). These findings suggest that, beyond logistical limitations such as hospital availability and formulation range, perceptual and experiential factors—particularly patient acceptance—remain key challenges in the broader implementation of SG-LAIs in clinical practice (Figure 4).
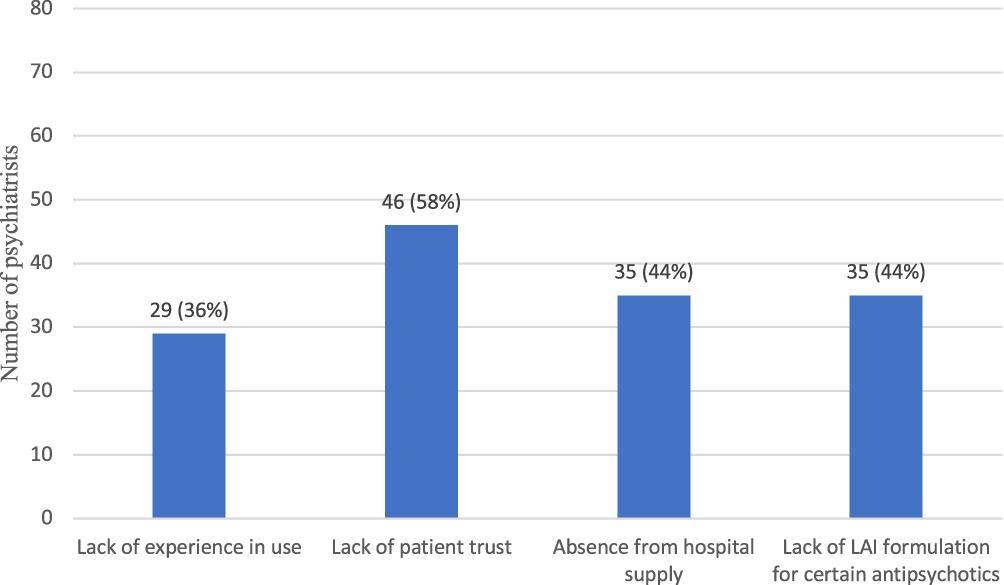 |
Figure 4 Obstacles to prescribing SG-LAIs. |
When asked about additional measures that could encourage the prescription of SG-LAIs, respondents could choose more than one option. The most frequently selected factor was broadening indications to include other diagnoses, chosen by 63 respondents (78.8%). Increased availability in hospitals was cited by 39 respondents (48.8%), while standardized tools for assessing the need for initiation were noted by 31 respondents (38.8%). The least frequently mentioned factor was more clinical data on efficacy an safety, selected by 9 respondents (11.3%). These results suggest that prescribers see expansion of approved indications and improving access within hospital settings as the most impactful strategies for increasing LAI utilization, whereas the demand for additional efficacy data is comparatively low (Figure 5).
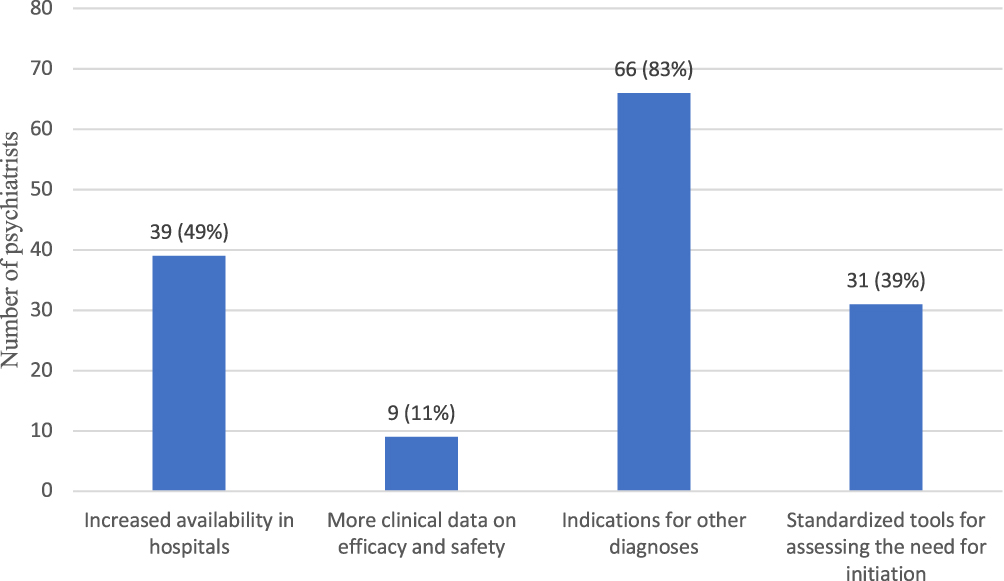 |
Figure 5 Factors that could encourage the prescription of SG-LAIs. |
Discussion
This study provides the first systematic assessment of Romanian psychiatrists’ attitudes toward second-generation long-acting injectable antipsychotics. Aripiprazole LAI emerged as the most favorably rated formulation across the majority of evaluated domains, including efficacy, safety, side effect profile, patient functionality, ease of administration, protocol inclusion, monitoring requirements, and overall preference. Paliperidone and risperidone also received favorable evaluations in certain areas, particularly dosing versatility, while olanzapine was consistently rated least favorably, largely due to its perceived safety profile, side effect burden, and high monitoring requirements.
When considering factors that encourage the prescription of SG-LAIs, respondents highlighted clinical benefits—particularly increased adherence and reduced risk of relapse—as the most influential motivators. In contrast, the main barriers to prescribing were lack of patient trust, limited hospital availability, absence of formulations for certain antipsychotics, and lack of clinician experience. Additional measures identified as potentially increasing LAI use included expanding indications to other diagnoses, improving hospital access, and implementing standardized tools for assessing the need for initiation.
The findings of this study align with international literature indicating that clinical outcomes—especially adherence and relapse prevention—are the dominant drivers of LAI prescription.21 Studies conducted in Western Europe, North America, and Asia have similarly identified these factors as primary motivators, while barriers such as patient reluctance, limited availability, and prescriber familiarity are consistently reported across settings.22,23
Our result that aripiprazole LAI is the preferred option in Romania is in line with recent surveys from Italy and Spain, where aripiprazole was also highly rated for tolerability, safety, and patient acceptability.24,25 This preference may be explained by its favorable metabolic profile, lower risk of extrapyramidal symptoms compared to other formulations, and flexible dosing schedule. In contrast, olanzapine’s lower rankings in this study are consistent with previous research linking its use to significant metabolic side effects and the requirement for post-injection monitoring, both of which can be perceived as barriers by clinicians.26
Paliperidone’s and risperidone’s intermediate ratings in our sample also mirror observations from other European studies, where they are valued for efficacy and availability in multiple dosing intervals but may be limited by side effect profiles or injection-site reactions.27 These results align with prior research identifying formulary and reimbursement restrictions as major drivers of LAI prescribing behavior.28
Our findings regarding psychiatrists’ perceptions of the relative safety, efficacy, and ease of administration of different SG-LAIs are also consistent with considerations highlighted by Citrome et al29 While efficacy among second-generation LAIs is broadly comparable, tolerability and logistical issues influence clinical decision-making. For example, olanzapine LAI requires a mandatory three-hour post-injection monitoring period due to the risk of post-injection delirium/sedation syndrome, which may discourage its use in routine practice. Conversely, paliperidone and newer risperidone formulations are often viewed more favorably because of their simplified initiation and extended dosing intervals. These practical concerns align closely with our observation that prescribing preferences are shaped not only by perceptions of clinical outcomes but also by structural and administrative barriers.
The consistently favorable ratings for aripiprazole LAI suggest that psychiatrists value formulations that combine efficacy with a favorable tolerability profile, flexible dosing options, and minimal post-administration requirements. These characteristics likely contribute to perceptions of improved patient adherence and overall treatment satisfaction. Additionally, the metabolic neutrality and low incidence of sedation associated with aripiprazole may further enhance its appeal in clinical practice.30
Olanzapine’s consistently low ratings in this study can be attributed to two key factors: the significant post-injection monitoring requirements mandated by its risk of post-injection delirium/sedation syndrome, and its well-documented metabolic side effects.31 These challenges may limit its utility in high-volume clinical settings and among patients with comorbidities such as obesity or metabolic syndrome.32
The mid-range ratings for paliperidone and risperidone reflect a balance between perceived efficacy and practical considerations. While both agents are widely available and supported by substantial clinical evidence, factors such as injection-site discomfort, prolactin elevation, or dosing inflexibility may limit their perceived utility compared to aripiprazole.33,34
The involvement of 80 psychiatrists with substantial clinical experience and cumulative patient pools exceeding 1,000 individuals with schizophrenia constitutes an important source of strength and representativeness for this study. Working across all major psychiatric care settings, these clinicians offer a diverse and ecologically valid perspective on current prescribing practices. Prescribing decisions were primarily influenced by the perceived benefits of long-acting injectable antipsychotics, particularly improved adherence and reduced relapse risk, while key barriers included patient distrust, limited hospital availability, absence of certain formulations, and insufficient prescriber experience. Participants also identified several measures likely to enhance LAI utilization, such as expanding approved indications, improving hospital access to a broader range of formulations, and implementing standardized initiation tools. These findings underscore the importance of aligning prescribing practices with international evidence demonstrating the value of second-generation LAIs in improving treatment continuity and outcomes in schizophrenia and related disorders. Addressing both patient-level and system-level barriers—alongside targeted educational initiatives aimed at increasing clinicians’ familiarity and confidence with LAIs—may facilitate more consistent and evidence-based integration of these formulations into routine psychiatric care in Romania.
This study has several limitations. Its cross-sectional design captures psychiatrists’ attitudes only at one moment in time, which may not reflect changes in prescribing practices. Self-reported data may introduce response bias, and the questionnaire’s structured format limits deeper qualitative insights into clinicians’ reasoning.
Conclusion
This study offers the first systematic insight into the attitudes of Romanian psychiatrists toward second-generation long-acting injectable antipsychotics. Aripiprazole LAI emerged as the most favorably rated option across most clinical and practical domains, while olanzapine LAI was consistently ranked lowest, largely due to safety concerns and high monitoring requirements. Paliperidone and risperidone LAIs held an intermediate position, with specific strengths in dosing versatility.
Institutional Review Board Statement
Ethical approval from the Ethics Committee of the Clinical Hospital of Psychiatry and Neurology in Brașov was not required, as the study did not involve human subjects or the use of patient data from hospitals.
Data Sharing Statement
The data supporting the findings of this study are not publicly available due to privacy and confidentiality considerations. An anonymized dataset may be provided by the corresponding author upon reasonable request and subject to approval by the local ethics committee.
Ethics Approval and Consent to Participate
Participation in the survey was voluntary, and all respondents were informed about the purpose of the study before completing the questionnaire. The survey collected only anonymized responses, and no personal or identifiable information was recorded. As the study involved only the opinions of practicing psychiatrists and did not include patients, clinical data, or any interventions involving human subjects, formal approval from a local ethics committee was not required according to applicable regulations.
Informed Consent Statement
Participation in this study was entirely voluntary. All respondents were informed about the purpose of the research, the anonymous and confidential nature of their responses, and their right to withdraw at any time without providing a reason. Participants were informed that by completing and returning the questionnaire, they provided informed consent to participate in the study.
Acknowledgments
The authors would like to express their gratitude to all participating psychiatrists for their time and valuable insights. We also wish to acknowledge the support of our colleagues from the Clinical Hospital of Psychiatry and Neurology in Brașov and from the “Prof. Dr. Alexandru Obregia” Psychiatry Hospital for their assistance in facilitating the distribution of the questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Patel MX, Bent-Ennakhil N, Sapin C, et al. Attitudes of European physicians towards the use of long-acting injectable antipsychotics. BMC Psychiatry. 2020;20(1):123. doi:10.1186/s12888-020-02530-2
2. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psych. 2016;77(suppl 3):21984. doi:10.4088/JCP.15032su1
3. Pappa S, Emsley R. The evolution of long-acting antipsychotic treatments. Therapeutic Adv Psychopharmacol. 2024;14:20451253241305610. doi:10.1177/20451253241305610
4. Tiihonen J. The use of long-acting injectables in early-phase schizophrenia. Lancet Psychiatry. 2023;10(7):481–16. doi:10.1016/S2215-0366(23)00180-3
5. Kishimoto T, Robenzadeh A, Leucht C, et al. Long-acting injectable vs oral antipsychotics for relapse prevention in schizophrenia: a meta-analysis of randomized trials. Schizophrenia Bulletin. 2014;40(1):192–213. doi:10.1093/schbul/sbs150
6. Kane JM, McEvoy JP, Correll CU, Llorca P-M. Controversies surrounding the use of long-acting injectable antipsychotic medications for the treatment of patients with schizophrenia. CNS Drugs. 2021;35(11):1189–1205. doi:10.1007/s40263-021-00861-6
7. Verdoux H, Pambrun E, Tournier M, Bezin J, Pariente A. Antipsychotic long-acting injections: a community-based study from 2007 to 2014 of prescribing trends and characteristics associated with initiation. Schizophr Res. 2016;178(1–3):58–63. doi:10.1016/j.schres.2016.09.014
8. Citrome L, Belcher E, Stacy S, Suett M, Mychaskiw M, Salinas GD. Management of schizophrenia with long-acting injectable antipsychotic medications: an assessment of the educational needs of clinicians. Neuropsychiatric Dis Treatment. 2022;18:111. doi:10.2147/NDT.S326299
9. Kane JM, Schooler NR, Marcy P, et al. Effect of long-acting injectable antipsychotics vs usual care on time to first hospitalization in early-phase schizophrenia: a randomized clinical trial. JAMA psychiatry. 2020;77(12):1217–1224. doi:10.1001/jamapsychiatry.2020.2076
10. Kane JM, Garcia-Ribera C. Clinical guideline recommendations for antipsychotic long-acting injections. Br J Psychiatry. 2009;195(S52):s63–s67. doi:10.1192/bjp.195.52.s63
11. Correll CU. Long-acting injectable antipsychotics for patients with first-episode and early-phase schizophrenia: still not considered often enough. CNS Spectrums. 2025;30(1):e66. doi:10.1017/S1092852925100503
12. Iaru I, Bucsa C, Farcas A, et al. Utilization of psychotropic medicines in Romania during 1998–2018. Front Pharmacol. 2023;14:1157231. doi:10.3389/fphar.2023.1157231
13. Miron AA, Ifteni PI, Teodorescu A, Petric PS. Long-acting injectable antipsychotics (LAIs) prescribing trends during the COVID-19 Pandemic in Romania. Healthcare. 2022;10(7):1265. doi:10.3390/healthcare10071265
14. Kaplan G, Casoy J, Zummo J. Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Preference Adher. 2013;1171–1180. doi:10.2147/PPA.S53795
15. García-Carmona JA, Barnett J, Campos-Navarro MP, Mason K, Valdivia-Muñoz F, Pappa S. Comparative effectiveness of long-acting injectable antipsychotics in a large naturalistic cohort across two European centers: findings from the long-acting injectable antipsychotics collaborative (LAICO) study. Neurosci Appl. 2022;1:100111. doi:10.1016/j.nsa.2022.100111
16. Haddad PM, Correll CU. Long-acting antipsychotics in the treatment of schizophrenia: opportunities and challenges. Expert Opinion Pharmacotherapy. 2023;24(4):473–493. doi:10.1080/14656566.2023.2181073
17. Alphs L, Nasrallah HA, Bossie CA, et al. Factors associated with relapse in schizophrenia despite adherence to long-acting injectable antipsychotic therapy. Int Clin Psychopharmacol. 2016;31(4):202–209. doi:10.1097/YIC.0000000000000125
18. Petric PS, Teodorescu A, Miron AA, Manea MC, Ifteni P. Cognitive outcomes in nonacute patients with schizophrenia treated with long-acting injectable antipsychotics versus oral antipsychotics. Ame J Therapeutics. 2024;31(3):e219–e228. doi:10.1097/MJT.0000000000001729
19. Ifteni P, Petric P-S, Teodorescu A. Rating opportunity for long-acting injectable antipsychotic initiation index (ROLIN). Front Psychiatry. 2021;12:767756. doi:10.3389/fpsyt.2021.767756
20. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(Suppl 3):1–24.
21. Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74(10):957–965. doi:10.4088/JCP.13r08440
22. Schneider-Thoma J, Chalkou K, Dörries C, et al. Comparative efficacy and tolerability of 32 oral and long-acting injectable antipsychotics for the maintenance treatment of adults with schizophrenia: a systematic review and network meta-analysis. Lancet. 2022;399(10327):824–836. doi:10.1016/S0140-6736(21)01997-8
23. García-Carmona JA, Simal-Aguado J, Campos-Navarro MP, Valdivia-Muñoz F, Galindo-Tovar A. Long-acting injectable antipsychotics: analysis of prescription patterns and patient characteristics in mental health from a Spanish real-world study. Clin Drug Invest. 2020;40(5):459–468. doi:10.1007/s40261-020-00913-7
24. Wang D, Schneider-Thoma J, Siafis S, et al. Long-acting injectable second-generation antipsychotics vs placebo and their oral formulations in acute schizophrenia: a systematic review and meta-analysis of randomized-controlled-trials. Schizophrenia Bulletin. 2024;50(1):132–144. doi:10.1093/schbul/sbad089
25. Nguyen TTK, McDonald C, Hallahan B. The association of metabolic syndrome and long acting injectable antipsychotics: a systematic review. Eur J Psych. 2022;36(3):163–175. doi:10.1016/j.ejpsy.2022.01.002
26. Manchado Perero S, Rodríguez Lorente A, García-Pérez A, et al. Long-term effectiveness, adherence and safety of twice-yearly paliperidone-palmitate long acting-injectable in patients with schizophrenia in Europe: 2-year mirror-image data from the paliperdone-2 per year study (P2Y). Front Psychiatry. 2025;16:1540213. doi:10.3389/fpsyt.2025.1540213
27. Lindenmayer J-P, Glick ID, Talreja H, Underriner M. Persistent barriers to the use of long-acting injectable antipsychotics for the treatment of schizophrenia. J Clin Psychopharmacol. 2020;40(4):346–349. doi:10.1097/JCP.0000000000001225
28. Citrome L. Choosing amongst the long-acting injectable antipsychotics: an evidence-based pragmatic guide. CNS Spectrums. 2025;1–48.
29. Citrome L. Aripiprazole long-acting injectable formulations for schizophrenia: aripiprazole monohydrate and aripiprazole lauroxil. Expert Rev Clin Pharmacol. 2016;9(2):169–186. doi:10.1586/17512433.2016.1121809
30. Ventriglio A, Baldessarini RJ, Vitrani G, et al. Metabolic syndrome in psychotic disorder patients treated with oral and long-acting injected antipsychotics. Front Psychiatry. 2019;9:744. doi:10.3389/fpsyt.2018.00744
31. McDonnell DP, Andersen SW, Detke HC, Zhao F, Watson SB. Long-term safety and tolerability of open-label olanzapine long-acting injection in the treatment of schizophrenia: 190-week interim results. Clin Med Insights. 2011;3:CMPsy–S6659.
32. Nasrallah HA, Gopal S, Gassmann-Mayer C, et al. A controlled, evidence-based trial of paliperidone palmitate, a long-acting injectable antipsychotic, in schizophrenia. Neuropsychopharmacology. 2010;35(10):2072–2082. doi:10.1038/npp.2010.79
33. Kane JM, Agid O, Castle DJ, et al. The use of long-acting injectables for people with schizophrenia: consensus panel recommendations for overcoming barriers and implementing treatment. Neurol Therapy. 2025;1–31.
34. Kishimoto T, Sanghani S, Russ MJ, et al. Indications for and use of long-acting injectable antipsychotics: consideration from an inpatient setting. Int Clin Psychopharmacol. 2017;32(3):161–168. doi:10.1097/YIC.0000000000000165
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Interventions to Improve Medication Adherence in People with Schizophrenia: A Systematic Review
Cahaya N, Kristina SA, Widayanti AW, Green J
Patient Preference and Adherence 2022, 16:2431-2449
Published Date: 1 September 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023
The Effect of Longer Dosing Intervals for Long-Acting Injectable Antipsychotics on Outcomes in Schizophrenia
Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, Wang S, Richarz U, Gopal S, Kane JM
Neuropsychiatric Disease and Treatment 2023, 19:531-545
Published Date: 7 March 2023