Back to Journals » Patient Preference and Adherence » Volume 16
Interventions to Improve Medication Adherence in People with Schizophrenia: A Systematic Review
Authors Cahaya N, Kristina SA, Widayanti AW ![]() , Green J
, Green J ![]()
Received 17 June 2022
Accepted for publication 17 August 2022
Published 1 September 2022 Volume 2022:16 Pages 2431—2449
DOI https://doi.org/10.2147/PPA.S378951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Noor Cahaya,1,2 Susi Ari Kristina,3 Anna Wahyuni Widayanti,3 James Green4
1Doctoral Program in Pharmacy, Faculty of Pharmacy, Universitas Gadjah Mada, Yogyakarta, Indonesia; 2Department of Pharmacy, Faculty of Mathematics and Science, Universitas Lambung Mangkurat, Banjarbaru, Indonesia; 3Department of Pharmaceutics, Faculty of Pharmacy, Universitas Gadjah Mada, Yogyakarta, Indonesia; 4School of Allied Health and Physical Activity for Health, Health Research Institute (HRI), University of Limerick, Limerick, Ireland
Correspondence: Susi Ari Kristina, Department of Pharmaceutics, Faculty of Pharmacy, Universitas Gadjah Mada, Sekip Utara, Yogyakarta, 55281, Indonesia, Email [email protected]
Abstract: Nonadherence to medications is very common in people with schizophrenia. Numerous methods have been implemented to improve medication adherence. The study aimed to determine what interventions have been used and to assess the effectiveness of these in improving medication adherence in people with schizophrenia. Two electronic databases (PubMed and Science Direct) and a manual search were used to locate RCT studies that examined interventions in medication adherence for schizophrenia, published between 2011 and 2022. The search was conducted using the terms (schizophrenia OR schizophrenic) AND (interventions OR adherence therapy) AND (medication adherence OR medication compliance). Sixteen studies were included, and relevant data were extracted and selected. Sixteen studies used interventions that involve family, health professionals (psychiatrists, psychologists, nurses, and pharmacists), SMS, and smart electronic reminders. Medication adherence was measured using medication refill records from hospital dispensing records or claim databases, electronic devices, plasma blood concentration, and participant self-reporting. Thirteen out of 15 studies showed significant improvements in adherence compared to routine care. The other three studies did not result in improved medication adherence. Interventions with diverse strategies delivered to individuals with schizophrenia showed the potential to reduce medication non-adherence in people with schizophrenia so that they can be utilized as an alternative to support treatment in people with schizophrenia in addition to antipsychotic medication. In future research strategies, it will be necessary to identify the main problems regarding nonadherence in people with schizophrenia individually and also identify the patient’s perception of medication, illness, and behavior when taking medication in order to determine the next intervention that will be appropriate based on the patient’s needs to improve adherence.
Keywords: adherence, schizophrenia, strategies, medication, interventions, systematic review
Introduction
According to the 2017 Global Burden Disease report, 20 million people, or nearly 1% of the global population, suffer from schizophrenia.1 Schizophrenia is a mental illness characterized by a wide range of symptoms. Positive symptoms (hallucinations, delusions, poor concentration), negative symptoms (apathy, lack of sense, poor or inadequate social functioning), and cognitive symptoms (disorganized thoughts, drowsiness, difficulty performing tasks, memory problems) symptoms are common in people with schizophrenia.2 Current guidelines for schizophrenia care recommend antipsychotics as an essential part of long-term maintenance treatment for people with schizophrenia.3 However, nonadherence to antipsychotic medication is more prevalent in people with schizophrenia, which may increase the risk of relapse, rehospitalization, suicide, and death.4–6 Nonadherence to treatment has an impact on disease progression, leading to disease complications, disruption of physical and social functioning of the people with schizophrenia, and decreased quality of life.7
Nonadherence to antipsychotic treatments remains an enormous challenge for clinicians and pharmacists in treating people with schizophrenia.8,9 Many factors contribute to partial and full nonadherence to medicines for schizophrenia, including poor insight,10 a negative attitude towards medication,11 chronicity of illness,12 complicated treatment regimens, side effects of medications, cost of medication,13 and poor social functioning. Furthermore, non-adherence among patients with schizophrenia and schizoaffective disorders has been associated with cognitive impairment, depression, substance abuse, inadequate or fragmentation of care, lack of family support,14 cultural influences, and lower socioeconomic status.15
In the literature, “adherence” or “compliance” refers to the degree to which a person accepts advice from a healthcare professional or follows the instructions for their medicine.16 According to the consensus definition, people with schizophrenia are considered adherent if they take more than 80% of their prescribed medication, have partial adherence if the person takes only 50% of the prescribed medication, and are nonadherent if they do not take the drug for 1 week.17 Adherence to medication is a critical problem across all disease states but can be especially difficult for people with mental illness.
Various strategies have been used to improve medication adherence in people with schizophrenia, including patient and family education,18 motivational interviewing, cognitive and behavioral approaches, and other combinations of strategies.19,47 A Several strategies could be considered complex interventions: these were multifaceted and involved case management and collaborative care interventions. Some previous studies have also described various interventions to improve compliance with schizophrenia and other mental disorders, such as bipolar disorders.20 Other reviews evaluated the effectiveness of interventions only in certain populations in the country21 or focused on specific methods.22,23 This study differs from the previous another in that it focuses on people with schizophrenia receiving both inpatient and outpatient treatment, only uses oral antipsychotic medication, and focuses on adherence as the primary outcome.
Therefore, the objective of this review is to determine intervention methods that have been used in people with schizophrenia and to assess the effectiveness of these interventions in improving medication adherence in people with schizophrenia.
Materials and Methods
Search Strategy
We conducted a digital search of the PubMed database for studies that contained the following keywords: (schizophrenia*) AND (intervention* OR adherence therapy) AND (medication adherence OR medication compliance) and the Science Direct database that contained the keywords: (schizophrenia OR schizophrenic) AND (interventions OR adherence therapy) AND (medication adherence OR medication compliance). Furthermore, a hand search was conducted to identify additional relevant studies. To report the results of this systematic review, we use the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.24 The electronic search results were transferred to Mendeley; duplicates were automatically removed. Two authors (NC and SAK) used a three-step process to select relevant articles. First, titles and abstracts were screened independently to determine whether they met the eligibility criteria. Then, independently read the full text of the remaining articles to complete the final selection of relevant articles. Second, A.W.W reviewed all of the extracted data for the articles.
Eligibility Criteria
We considered all possible designs for clinical trials, including single group trials, randomised control trials, control clinical trial, pilot, or feasibility study. Studies published in English between 2011 and 2022 were included. We excluded editorials, letters, practice recommendations, other guidelines, conference abstracts, conference reports, systematic reviews, and meta-analyses, as well as studies with an unclear procedure or intervention. Articles were included if they involved participants with a formal diagnosis of schizophrenia, schizoaffective or schizophreniform disorders, according to the criteria of the Diagnostic and Statistical Manual, DSM-V-TR25 or International Statistical Classification of Disease, Tenth Revision (ICD-10),26 and used oral antipsychotic medication in therapy. We excluded articles that involved participants with a diagnosis of organic disorders, ICD-10 mental retardation, long-acting or depot antipsychotic medication use, homelessness, a suicide attempt, drug or substance abuse, and alcohol dependence.
Risk of Bias Assessment
NC and SAK assessed the risk of bias in selected studies independently using a tool adapted from a Cochrane Collaborative tool for assessing the risk of bias in randomized trials. There were six criteria were used in this bias risk assessment: random sequence generation (selection bias); allocation concealment (selection bias); blinding of participants, personnel, and outcome assessment (information bias); incomplete outcome data (attrition bias); selective outcome reporting (reporting bias); and other bias (eg, confounding bias). Each criterion was rated as having a low risk of bias, being unclear (inadequate information for judgment), or having a high risk of bias.27 Disagreements between N.C and S.A.K were resolved by consensus after discussion or by A.W.W when necessary. Details on the assessment of the risk of bias are presented in Figure 1.
 |
Figure 1 Summary of quality assessment of studies. |
Results
Study Selection
Figure 2. shows the PRISMA flow diagram for the literature search process. Initially, 708 studies were identified. After removing duplicates (n=8), we screened the articles according to eligibility criteria by reading the abstracts and titles. This resulted in 39 potential studies to be included. Of these, twenty-three were excluded; The reasons for excluding studies were: no medication adherence assessment (n=10), using depot antipsychotic (n = 7), and protocol (n = 6). Sixteen studies met the inclusion criteria for this review.
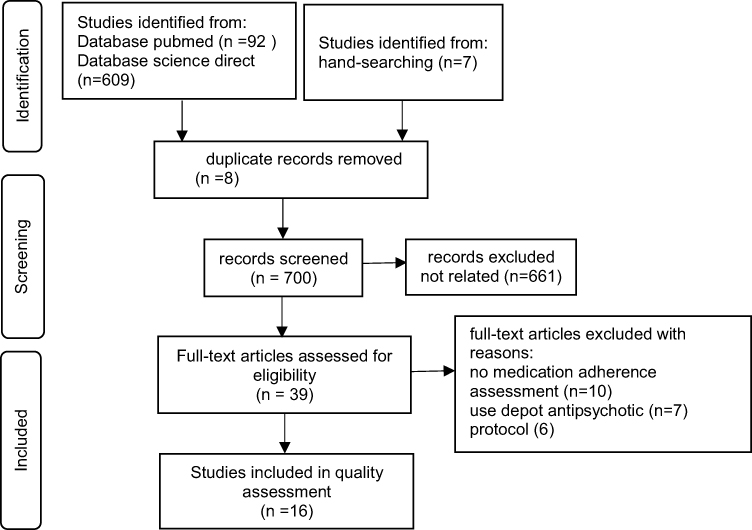 |
Figure 2 PRISMA diagram of this review. |
Characteristics of Included Study
All sixteen studies included in this review were randomized controlled trials. Eleven studies were at low risk of bias and five studies were at high risk of bias. The main characteristics of the included studies are presented in Table 1. The oldest studies were published in 201128,29 and the most recent study was published in 2020.30,31 Fifteen studies used a randomized controlled trial design with two arms,28–42 and one study used a randomized controlled trial design with three arms.43 The studies were conducted in the United States,29,43 several countries in East, West and South Asia such as China,31,36 HongKong,35,40,41 Japan;34 Turkey,33 Pakistan,28 India,32 and Vietnam;42 as well as European countries such as Spain,37 the Netherlands,38 and Germany.30,39
 |  |  |  |
Table 1 Summary Characteristics of Included Studies |
Types of Intervention and Personnel Who Delivered the Intervention
The Supervised Treatment in Outpatients for Schizophrenia (STOPS) program employs a drug supervisor who is appointed by the patient’s family or close relatives. The drug supervisor is responsible for administering drugs from health facilities to patients in the correct dose and supervising treatment and recording patient medication adherence. STOPS, used an educational intervention for caregivers (key care supervisors) to administer and supervise the medication provided free of charge as part of a treatment program.28
In five studies, motivational interviews were used as an intervention, while normal treatment (TAU) and routine care were used as controls.33,35,38,40,41 Motivational interviewing (MI) is a client-centered consultation method, supported by a series of phases, that is, engaging, focusing, evoking, and planning. Patients participate in discussions with therapists about their concerns and problems with medication. The overall objective is to increase the patient’s personal motivation to change.
One study applied adherence therapy intervention.39 Adherence therapy (AT) is a treatment-based, patient-centered that aims to reduce psychiatric symptoms in patients by increasing treatment adherence. The four cornerstones of AT are keeping the patient engaged and minimizing resistance to change, providing the patient with the information required by the patient about medications and side effects, and generating discrepancies in the patients’ beliefs about treatment.44 The patients in the intervention group received eight sessions of AT in addition to TAU.39 Adherence therapy is based on the concept that patient beliefs have an impact on medication adherence.16,45,46
Montes et al37 used an SMS reminder strategy. Patients received SMS reminders every day for more than 3 months to take their antipsychotic medication. The intervention group was compared with the control group who received standard therapy.37 Velligan et al,43 used PharmCAT and Med-eMonitor (MM) interventions for patients. PharmCAT is a component of the Full-CAT program, which consists of a series of intervention strategies aimed at compensating for the cognitive impairment associated with schizophrenia and improving adaptive functioning, but the interventions are only aimed at patient compliance issues. A Med-eMonitor (MM) is a smart pill container or electronic device in the home of a patient that helps remind patients to take medication, provides warnings in the case of the wrong medication, records side effects experienced by patients, and follows up if the patient does not adhere via telephone.
Meds-Help is a pharmacy-based intervention. The intervention is in the form of prescribing treatment packages followed by education and medication counseling by pharmacists for people with schizophrenia.29 Similarly, collaborative care32 is a pharmacy-based intervention. Mishra et al,32 used collaborative care with pharmacists and psychiatrists working together as a team to improve patient drug compliance and patient clinical outcomes.
The Family Schizophrenia Psychoeducation Program (FSPP) is a program offered to people with schizophrenia and their families to provide comprehensive information on schizophrenia through direct discussions with psychiatrists, psychologists, and nurses in a hospital with the ultimate goal of improving medication adherence and improving the quality of life of patients with schizophrenia.42
Individualized occupational therapy (IOT) strategies are tailored to enhance cognitive functioning and prompt adaptive behaviors to maximize functional outcomes for patients with schizophrenia. It consists of a combination of effective psychosocial treatment programs, including motivational interviewing, self-monitoring, individualized visits, handicraft activities, individualized psychoeducation, and discharge planning.34
An intervention called LEAN (Lay Health supporters, E-platform, Award, and integration) involved the recruitment of lay health supporters; an electronic platform with mobile texting/SMS for medication reminders, health, education, and monitoring; the awarding of token gifts for positive behavioral improvement; and integration of texting with the health system.31,36 In this review, two studies were using the LEAN strategy. The first study conducted by Xu et al, used a 2-arm randomized controlled trial design, while the study conducted by Cai et al, was a randomized controlled trial of a step-by-step wait list design, which is a follow-up implementation of LEAN from previous trials.
SDM-PLUS is an intervention with an approach to increase patient motivation through special communication techniques provided by trained health workers so that patients are allowed to be directly involved in discussions with health workers regarding their treatment.30
The involvement of the healthcare professional providing the intervention can be seen in all the studies included in this review. Interventions in the form of motivational interview techniques,33,35,38,40,41 adherence therapy,39 IOT,34 and SDM-PLUS30 were provided by therapists (psychologists, psychiatrists, or mental health nurses), while the STOPS (Supervised Treatment in Outpatients for Schizophrenia),28 FSPP (Family Schizophrenia Psychoeducation Program),42 and LEAN (Lay Health supporters, E-platform, Award and iNtegration)31,36 programs were delivered by family members. Two interventions involved pharmacists, which were Meds Help29 and Collaborative Care.32
Participants Characteristic
The total number of participants in each study ranged from 23 to 322 participants. Based on the characteristics of participants in thirteen studies, data on the age of participants ranged from 14–65 years, while the remaining three studies were unknown.29,31,36 The mean age of the participants in fifteen studies ranged from 16.2 to 50.2 years, but in Mishra et al32 studies it was not stated. In all studies, the majority of the participants involved were male (range between 50% and 97%). Five studies involved only male participants37–39,42,43 and two studies only female participants,31,36 the rest included both male and female participants.25–27,32–35,40,41
Inpatients and outpatients with schizophrenia or related psychoses, such as schizoaffective disorder, who were receiving treatment in a hospital or community service department, were enrolled in the 16 studies included in this systematic review. Farooq et al,28 Valenstein et al29 Cai et al,31 Montes et al,37 Chien et al,35,40,41 Mishra et al,32 Ertem and Duman,33 and Xu et al36 included out-patients. Hamann et al,30 Velligan et al,43 Schulz et al,39 Ngoc et al,42 and Shimada et al,34 included inpatients and only one study included inpatients and outpatients.38
Medication Adherence Measurements
Three approaches were used to measure adherence in sixteen studies, including: (1) participants’ response to a questionnaire via researcher interview or participants’ self-reporting, (2) electronic compilation of participants’ dosing history, and (3) analysis of medication refill record from hospital dispensing record or claim database. Self-report measures were the Medication Adherence Questionnaire (MAQ),37,38 Drug Attitude Inventory (DAI),31,36–39 Medication Adherence Rating Scale (MARS),30,39 Morisky Medication Adherence Scale (MMAS),34 Adherence Rating Scale (ARS and BARS).31,35,36,40,41 Other studies used self-ratings by patients or relatives or healthworkers,28,42 pill count,31,36,43 and blood plasma level.39 Adherence rates were reported as mean or median percentages or percentages of complete doses taken, or assessment tool scores.
Three studies29,37,38 used the MAQ questionnaire. The MAQ is also known as the 4-item Morisky Medication Scale (MMAS-4) and Morisky Scale.48 The MAQ is a self-assessment questionnaire consisting of four questions with yes-or-no answers. When the answer indicates a negative adherence issue, a score of 1 is recorded.49 The total score ranges from 0 (good adherence) to 4 (poor adherence).49 In Barkhof et al,38 measurements of adherence using MAQ were carried out at the beginning of participant recruitment, post-treatment, and six months of follow-up, but in Montes et al,37 measurements of adherence were carried out at the beginning of participant recruitment, 3 months after the intervention, and 3 months after the intervention was stopped. The total MAQ score in the intervention group was compared with the control group.37,38
The MMAS-8 is an updated version of the previous Morisky scale, consisting of 8 items with dichotomous answers “Yes or No”. The total score ranged from 0 to 8, with higher scores indicating better adherence to prescribed medication. In a study by Shimada et al,34 assessments were conducted by trained evaluators before assignment (baseline assessment) and at discharge or 3 months following hospitalization (post-assessment).
The DAI is a questionnaire consisting of a self-assessment scale developed to measure subjective responses and attitudes of chronic people with schizophrenia to treatment. A positive total score means a positive subjective attitude. The DAI questionnaire was used to assess attitudes toward treatment.50,51 The DAI is available in 30-item and 10-item versions. The 10-item version (DAI-10) consists of a subset of DAI-30 items.52
The Medication Adherence Rating Scale (MARS) is a 10-item self-report instrument in which a yes or no response is given to questions asked. The total scores range from 0 (low likelihood of medication adherence) to 10 (high likelihood). Assessment of patient medication adherence was measured from follow-up 1 to follow-up 2 and follow-up 2 to follow-up 3. The average improvement in medication adherence in the intervention and control groups was assessed.32
The single-item ARS developed by Staring et al,53 is a self-report measurement to measure medication adherence. ARS items were assessed on a 5-point Likert scale (1 = total non-adherence, 2 = poor compliance, 3 = inadequate compliance, 4 = moderate compliance, and 5 = good compliance).
Farooq et al study28 adapted the Herz et al54 methods of measuring medication adherence, which is measured during the interview using a questionnaire with a 5-point scale (where 1 is always and 5 is never). Medication adherence assessments were performed every three months beginning at baseline, using the information provided by participants and relatives. If available, drugs calculated from the previous prescription add to this information. Participants were considered to be in full adherence to treatment if they took their medication as prescribed without missing a dose during the assessment period. Non-adherence was defined as missing medication for more than a week at a time. Partial adherence occurs when participants take some medications but do not take them every day of the week.28
The Ngoc et al42 study used a medication adherence inventory scale to assess nonadherence that was adapted for Vietnam, and this instrument consists of 8 items rated on a frequency scale of 0–2, with higher scores indicating higher non-compliance.55
Concentration to dose Ratio (CDR) is a measurement of compliance using the calculation of the ratio of concentration to serum dose, namely the higher the CDR, the more patients are adherent. If a patient is taking more than one antipsychotic drug the psychiatrist is asked to specify the primary antipsychotic drug used for analysis. All blood samples were collected between 8 and 10 am by the nurse or psychiatrist working on the ward. For follow-up testing, subjects are invited to the clinic for blood collection. If patients are unable to attend, blood is drawn at their homes.39
Xu et al36 and Cai et al31 used pill counts to measure adherence. The number of undeclared home pills as a proportion of the doses taken in the previous month (number of first counts – number of second counts + number of additional pills taken – number of pills discarded) /(the number of pills determined). If two or more types of antipsychotic drugs were taken, adherence was calculated by combining the number of tablets of the drug required by the prescription as the denominator and the actual number of pills taken as the numerator. However, pill counts were not performed at baseline. Instead, refill records and 2 rating scales were used at baseline i.e Brief Adherence Rating Scale (BARS) and Drug Attitude Inventory-10 (DAI-10). Adherence by refill record was calculated as a cumulative medication possession ratio (0–100%) over 1 year, ie, the number of days medication obtained over 365 days divided by 365 days. DAI-10 adherence was originally from −10 to +10 (highest score equals more positive attitude toward medication), which was rescaled to be 0 to 1. BARS adherence is the self-reported percentage of dosages taken over the past month.31,36
An electronic monitor was used to measure compliance in a study conducted by Velligan et al43 The med-monitor is calculated by comparing the number of doses that the patient is supposed to take with the number of times the container is opened in a certain dose window and the patient indicates that the pill was consumed. In addition to adherence to the electronic monitor, participants’ homes were visited monthly for unannounced pill counts.
Duration of Follow-Up
The duration of follow-up varied between all studies. The duration ranged from 3 months to 18 months. One study started follow-up after 1 week of intervention, followed by 6 months and 12 months.35 In Chien et al study,41 had the longest follow-up, first at 2 weeks, continued for 6 months and 18 months. One study did not report the duration of the intervention.32
Effectiveness of Interventions on Medication Adherence
Summary study results is summarized in Table 2. Motivational interviewing interventions were performed in five studies. The intervention was based on motivational interviewing conducted in approximately 5–8 sessions during the 6-month to 18-month program. Four studies33,35,40,41 showed significant improvement in medication adherence; one study38 did not. The same results were also shown in the adherence therapy intervention,39 which showed a change in the mean score of adherence that was not significant in the intervention group compared to the control group.
 |
Table 2 Summary of Study Results |
The remaining ten studies with more heterogeneous interventions — STOPS (Supervised Treatment in Outpatients for Schizophrenia),28 Meds-Help,29 SMS-based interventions,37 Pharm-CAT and Med-eMonitor,43 FSPP (Family Schizophrenia Psychoeducation Program),42 collaborative care,32 IOT (Individualized Occupational Therapy),34 and the last one, LEAN (Lay Health supporters, E-platform, Award, and integration),31,36 mostly showed positive results on medication adherence. The intervention SDM-PLUS (Shared Decision-Making PLUS)30 did not show a significant improvement in adherence.
Effectiveness of Interventions on Other Outcomes
In these studies, other outcome measures such as symptom and clinical severity,27,28,35–37,39–41,43 Global Functioning and Psychosocial Functioning,28,30,35,37,40,41,43, Quality of Life (QoL),29,32,37,42 hospitalization rates or rehospitalisation,31,34–36,38,40,41 insight into illness,33,35,40,41 stigma,42 and intrinsic motivation34 were also measured.
Some of the measurements showed positive effects, while others did not. The effects appear to depend on the interventions and characteristics of participants, which are different in each study.
Discussion
This systematic review summarises the evidence available on interventions designed to improve medication adherence in patients with schizophrenia. The majority of interventions found positive improvements in adherence, across a range of intervention types, including motivational interviewing, technology-enhanced/mHealth interventions, collaborative care and complex interventions. Included studies were all randomized trials and were mostly judged to be at low risk of bias.
Three of the included studies, all using patient-therapist interactions, did not find evidence that the intervention improved the adherence of people with schizophrenia.30,38,39 Hamann et al30, reported on the SDM-PLUS intervention, which used an approach to increase motivation through communication between patients and health workers. This method is similar to motivational interviewing which also emphasizes communication techniques to increase motivation. Two studies38,39 using adherence therapy interventions based on motivational interviews also failed to find evidence of improved adherence. However, the remaining four motivational interviewing studies did find positive effects.33,35,40,41
Based on a review of the literature, it was found that one of the six studies reviewed showed a relationship between motivational interviewing (MI) and medication adherence. While the other five studies did not. They found association between MI and other outcomes such as improved psychotic symptoms and decreased re-hospitalization rates.23 Motivational interviews may be beneficial for some patients with schizophrenia, but they should not be used as first-line therapy. Instead, they can be used as an adjunct treatment to improve patient outcomes, particularly for patients on a treatment program. Motivational interviews can assist in motivating patients and involving them in their treatment.56 Motivational Interview is an opportunity to promote health patients are not motivated, but otherwise may be able to respond to interventions. Motivational interviews are useful tools for clinicians to encourage patients to seek help for mental health problems.57
According to intervention guidelines, Motivational Interview is divided into four phases (8 sessions).23,56 In several studies in this review, there were differences in the number of Motivational Interview sessions given to participants. In the study of Chien et al40 Motivational Interview was divided into 8 sessions, and 6 sessions in Chien et al41 and Chien et al35 But in Barkhof et al, patients were offered 8 sessions with a minimum of 5 sessions. A review and meta-analysis conducted by Gray et al44 also showed evidence that AT was significantly able to reduce psychiatric symptoms compared to TAU in a follow-up period of less than 1 year, while the effect on adherence behavior and attitudes was not significant. Based on one study, it was found that the MI intervention provided a more dominant advantage over mental disorders patients with conditions who did not seek treatment, and from the study it was also found that the intensity of the MI intervention in short duration was as effective as a longer intervention, while two sessions of MI for 15 minutes was effective in increasing treatment attendance.57
The systematic review and meta-analysis of Loots et al20 also explained that the significant effect of medication adherence could be achieved when the intervention was adequate and provided extended follow-up duration. Each duration selected in the intervention will have an effect size value. Motivational interviewing that focuses on medication and changes in medication used, achieving beneficial outcomes in adherence at six months of follow-up with moderate effect size.40 Studies that include proper and extended follow-up periods are important, as researchers need to assess the impacts of the intervention on adherence to immediate, intermediate and long-term effects.20 Based on the evidence, it is necessary to pay attention to several factors such as the patient’s condition, how the patient seeks treatment, and the duration of follow-up in order to achieve the optimal outcomes for improving medication adherence.
Several studies used daily SMS as a reminder intervention, which increased medication adherence in people with schizophrenia.37 Another study that also uses text messages for reminders of medication, called LEAN, was the study conducted by Xu et al36 and Cai et al31 Many studies have shown that text message interventions were effective in increasing the rate of medication adherence for people with HIV, asthma, diabetes, schizophrenia, and heart disease. The intervention period ranged from 1 week to 14 months. These studies were mostly conducted in developed countries, and applied a randomized controlled trial (RCT) design with intervening periods ranging from 1 week to 14 months.58 The results of the narrative literature review59 showed almost all studies suggest that SMS reminders help improve patient medication compliance and appointment reminders. In addition, it also reported the many benefits of using SMS reminders, including ease of use, relative cost, and fast and automated message delivery. The minimal risk was reported, and most participants found repeated reminders acceptable Text messaging appears to be an effective reminder mechanism to promote better medication compliance.
Another form of intervention that is also carried out was Meds Help, which is a pharmacy-based intervention that includes prescribing unit doses of drugs for psychiatric and medical conditions, education on packaged drugs, and refill reminders sent 2 weeks earlier for 6 and 12 months. This intervention has significantly increased medication possession ratios (MPR).29 Results of meta-analysis showed that pharmacist intervention had a statistically significant effect on medication adherence in patients with schizophrenia. The mean score of medication adherence of patients in the pharmacist intervention group was higher than in the control group (SMD = 0.60, 95% CI 0.41, 0.79) and the pooled relative risk for medication adherence was 1.13 (95% CI 1.07, 1.19).60 The study conducted by Mishra et al32 is also a pharmacy-based intervention. Patients are educated using Patient Information Leaflets (PIL). Based on these two studies, we can provide evidence that pharmacists’ involvement in the care for patients with schizophrenia has an influential effect on increasing patient medication adherence. Evidence can be used as an example of an intervention that can be used or for the development of intervention models by pharmacists in the future, so that there will be more interventions that can be used to improve pharmaceutical services for patients with mental disorders, especially schizophrenia.
In another study conducted by Velligan et al,43 used environmental support through home visits (Pharm CAT) and reminders to adhere to medication (Med-eMonitor). The intervention carried out in this study is a behavioral intervention. This intervention benefits individual patients, improves independent living skills, and improves cognitive abilities by training patients to adapt by providing education about treatment and providing support through medication reminders to improve patient compliance. The results showed an increase in patient compliance through measurement of the number of pills and electronic monitors in the measurement periods of 3, 6, and 9 months. Another study is in the form of a psychoeducational program (FSPP)42 aimed at patients and their families. This intervention educates patients and their families about schizophrenia, including symptoms, and how to treat them, as well as the prognosis of schizophrenia if properly treated. In the end, it is hoped that after participating in this program, patients and their families will improve their stigma against schizophrenia, families will fully assist and support patients’ treatment, medication adherence will increase and quality of life will also improve. This program consists of three sessions with a duration of approximately 1.5 h, which take place in the hospital. The sessions are interactive, with hospital staff providing information, but also facilitating discussion with families and patients. Sessions were conducted by a hospital psychiatrist, two psychologists, and two nurses. Sessions are usually provided for one and a half weeks. The FSPP program showed results that were able to significantly improve adherence to treatment adherence compared to controls.
The study conducted by Farooq et al used intervention in the form of a program called STOPS. This program is an adoption of the DOTS program for tuberculosis patients. This program focuses on the importance of the supervisor’s role for patients during treatment, so the ultimate goal is to increase adherence to medication adherence and improve clinical outcomes.28
The study conducted by Shimada et al used a complex intervention. An individualized occupational therapy (IOT) program is a psychosocial program developed to facilitate proactive participation in treatment and improve cognitive function and other outcomes for hospitalized patients with acute schizophrenia. The program consists of motivational interviews, self-monitoring, individual visits, craft activities, individual psychoeducation, and discharge planning.34
In this review, several interventions to improve adherence have been described in patients with schizophrenia, although some of these interventions have not been successful in improving adherence to medications. Several problems arose in the studies included in this review, including those related to the reluctance of patients to participate in the study, dropouts that occurred during the study, and the unstable condition of patients who occasionally relapsed. Based on this review, there is also evidence that a single intervention or combination of interventions can improve adherence in patients with schizophrenia. The success of the intervention carried out is also influenced by the duration of the intervention given. Several studies in this review showed that the duration of the intervention differs from one another, adjusting to the type of intervention administered. In general, the duration of the intervention given is at least 3 months. The previous review found that interventions of a purely educational nature were the least successful in improving antipsychotic adherence, while those that employed combinations of education, behavioral, and affective strategies were the most successful in terms of adherence and secondary outcomes. Furthermore, interventions that reported improvements in adherence tended to be longer in duration and involved a larger number of participants, highlighting the importance of appropriate intensity and duration of therapy, along with the need to have a sample size large enough to determine the effectiveness of an intervention’s effectiveness.61
A recent qualitative systematic review study found the conclusion that the strength of social attachment and the potential for joint decision-making programs in deciding treatment programs for people with schizophrenia are necessary so that patients are can rebuild perceptions to be able to live normally.62 Therefore, in an intervention that is given, it is very necessary to have a relationship of trust between the therapist and the patient, education in the form of education to the patient or the patient’s family about the disease and treatment, and motivation that must be continuously instilled in the patient to take treatment and return to normal life.
In all studies in this review, it was found that various health care professionals, such as psychiatrists, psychologists, mental nurses, and pharmacists, were found to act as people who provide interventions to people with schizophrenia. Most of the health care professionals who are heavily involved are psychiatrists, psychologists, and mental nurses. There is little direct involvement of pharmacists in the intervention. In general, pharmacists are only involved in the process of prescribing, procuring, and managing antipsychotic drugs.
Non-adherence in people with schizophrenia is influenced by a number of factors, including the disease, the patient, the treatment, environmental factors, and the patient’s relationship with the physician.14 These factors must be considered by the clinician when determining the appropriate intervention for the patient’s needs, both individually and in groups. Furthermore, the active engagement and collaboration of health professionals such as psychiatrists, psychologists, psychiatric nurses, and pharmacists helps to improve the treatment of people with schizophrenia. The various interventions provided have benefits and weaknesses, and these interventions can be used as adjunctive therapy to antipsychotic therapy, which is still the mainstay of schizophrenia treatment. Furthermore, the variability in the research methodology applied, the intervention used, the definition of adherence, and the outcome measure of adherence chosen, becomes a problem in drawing conclusions regarding which intervention is most effective in improving medication adherence in people with schizophrenia.
Limitations
This systematic review has some limitations. One limitation of this study was that it used a small number of databases and did not use large Embase databases. In addition, this review is limited to research published in English, research related to the discussed themes that were published in languages other than English may have been overlooked. This review concentrates on studies that used a randomized trial or randomized controlled trial design. As a result, the possibility of intervention using designs developed by others, such as a quasi-experimental or nonrandomized study, is not covered in this review. In the future, it is hoped that there will be not only quantitative research but also research with qualitative study designs to evaluate the evaluation of the interventions that have been given.
Conclusion
Of the 15 studies, 2 have no significant effect on increasing adherence in people with schizophrenia. Interventions using various strategies have the potential to reduce medication nonadherence in schizophrenic patients, enables them to be used as adjunctive therapy to the main antipsychotic treatment to support people with schizophrenia. No intervention is superior or inferior because each has both benefits and drawbacks. Recent research will need to explore the major problems potentially causing patient nonadherence before developing intervention strategies, so that the interventions provided are based on the patient’s needs to improve medication adherence.
Acknowledgments
This study is a part of a doctoral dissertation and the author expresses gratitude to Universitas Gadjah Mada and Universitas Lambung Mangkurat.
Disclosure
The authors report that they have no conflicts of interest in this work.
References
1. Collaborators, G. 2017 D. and I. I. and P. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392. doi:10.1016/S0140-6736(18)32279-7
2. Kahn RS. Schizophrenia. Nat Rev Dis Prim. 2015;1:1–23.
3. Fatani BZ, Aldawod RA, Alhawaj FA. Schizophrenia: etiology, pathophysiology and management: a review. Egypt J Hosp Med. 2017;69:2640–2646. doi:10.12816/0042241
4. Hiwot S, Henock A. A study to assess the prevalence of antipsychotics non-adherence and it’s associated factors among patients with schizophrenia in. JOJ Nurse Heal Care. 2018;6:001–005.
5. Conti V, Lora A, Cipriani A, et al. Persistence with pharmacological treatment in the specialist mental healthcare of patients with severe mental disorders. Eur. J. Clin. Pharmacol. 2012;68:1647–1655. doi:10.1007/s00228-012-1298-2
6. Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr. Bull. 2018;44:1195–1203. doi:10.1093/schbul/sby058
7. Lee KC; American Pharmacists Association. Improving medication adherence in patients with severe mental illness. Pharm Today. 2013;19:69–80. doi:10.1016/S1042-0991(15)31317-7
8. Anderson KH, Ford S, Robson D, et al. An exploratory, randomized controlled trial of adherence therapy for people with schizophrenia. Int. J. Ment. Health Nurs. 2010;19:340–349. doi:10.1111/j.1447-0349.2010.00681.x
9. Yalçin N, Ak S, Gürel ŞC, Çeliker A. Compliance in schizophrenia spectrum disorders: the role of clinical pharmacist. Int Clin Psychopharmacol. 2019;30:1–8.
10. Lysaker PH, Vohs J, Hillis JD, et al. Poor insight into schizophrenia: contributing factors, consequences and emerging treatment approaches. Expert Rev. Neurother. 2013;13:785–793. doi:10.1586/14737175.2013.811150
11. Uhlmann C, Kaehler J, Harris MA, et al. Negative impact of self-stigmatization on attitude toward medication adherence in patients with psychosis. J. Psychiatr. Pract. 2014;20:405–410. doi:10.1097/01.pra.0000454787.75106.ae
12. Sajatovic M, Mbwambo J, Lema I, et al. Correlates of poor medication adherence in chronic psychotic disorders. BJPsych Open. 2021;7:1–7. doi:10.1192/bjo.2020.141
13. Lizer MH. The impact of a pharmacist assisted clinic upon medication adherence and quality of life in mental health patients. Ment Heal Clin. 2013;2:236–239. doi:10.9740/mhc.n133114
14. Higashi K, Medic G, Littlewood KJ, et al. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther. Adv. Psychopharmacol. 2013;3:200–218. doi:10.1177/2045125312474019
15. Phan SV. Medication adherence in patients with schizophrenia. Int J Psychiatry Med. 2016;51:211–219. doi:10.1177/0091217416636601
16. World Health Organisation. Adherence to long -term therapies evidence for action. Appl Mech Mater. 2003. doi:10.4028/www.scientific.net/AMM.321-324.1779
17. Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry. 2009;70:1–48. doi:10.4088/JCP.7090su1cj
18. Saber E, Kader NMA, Mohammed A. Effect of psycho educational program on improving of medication adherence among schizophrenic patients. J Nurs Heal Sci. 2018;7:69–79.
19. El-Mallakh P, Findlay J. Strategies to improve medication adherence in patients with schizophrenia: the role of support services. Neuropsychiatr Dis Treat. 2015;11:1077–1090. doi:10.2147/NDT.S56107
20. Loots E, Goossens E, Vanwesemael T, et al. Interventions to improve medication adherence in patients with schizophrenia or bipolar disorders: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18:1–22. doi:10.3390/ijerph181910213
21. Inwanna S, Duangchan C, Mathews AK. Effectiveness of interventions to promote medication adherence in schizophrenic populations in Thailand: a systematic review. Int J Environ Res Public Health. 2022;19:1–18. doi:10.3390/ijerph19052887
22. Hegedüs A, Kozel B. Does adherence therapy improve medication adherence among patients with schizophrenia? A systematic review. Int J Ment Health Nurs. 2014;23:490–497. doi:10.1111/inm.12089
23. Vanderwaal FM. Impact of motivational interviewing on medication adherence in schizophrenia. Issues Ment Health Nurs. 2015;36:900–904. doi:10.3109/01612840.2015.1058445
24. Page MJ, Moher D, Bossuyt PM, et al. Research methods and reporting PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews review findings. BMJ. 2021:n160. doi10.1136/bmj.n160
25. APA. Diagnostic and Statistical Manual of Mental Disorders DSM-5.
26. World Health Organisation. The ICD-10 classification of mental and behavioural disorders; (1992).
27. Higgins JPT, Altman DG, Gotzsche PC, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:1–9. doi:10.1136/bmj.d5928
28. Farooq S, Nazar Z, Irfan M, et al. Schizophrenia medication adherence in a resource-poor setting: randomised controlled trial of supervised treatment in out-patients for schizophrenia (STOPS). Br J Psychiatry. 2011;199:467–472. doi:10.1192/bjp.bp.110.085340
29. Valenstein M, Kavanagh J, Lee T, et al. Using a pharmacy-based intervention to improve antipsychotic adherence among patients with serious mental illness. Schizophr. Bull. 2011;37:727–736. doi:10.1093/schbul/sbp121
30. Hamann J, Holzhüter F, Blakaj S, et al. Implementing shared decision-making on acute psychiatric wards: a cluster-randomized trial with inpatients suffering from schizophrenia (SDM-PLUS). Epidemiol. Psychiatr. Sci. 2020;29(e137). doi:10.1017/S2045796020000505
31. Cai Y, Gong W, He H, et al. Mobile texting and lay health supporters to improve schizophrenia care in a resource-poor community in rural China (LEAN trial): randomized controlled trial extended implementation. J. Med. Internet Res. 2020;22:e22631. doi:10.2196/22631
32. Mishra A, Sai Krishna G, Sravani A, et al. Impact of pharmacist-led collaborative patient education on medication adherence and quality of life of schizophrenia patients in a tertiary care setting. Bull. Fac. Pharmacy, Cairo Univ. 2017;55:345–349. doi:10.1016/j.bfopcu.2017.08.001
33. Ertem MY, Duman ZÇ. The effect of motivational interviews on treatment adherence and insight levels of patients with schizophrenia: a randomized controlled study. Perspect Psychiatr Care. 2019;55:75–86. doi:10.1111/ppc.12301
34. Shimada T, Ohori M, Inagaki Y, et al. A multicenter, randomized controlled trial of individualized occupational therapy for patients with schizophrenia in Japan. PLoS One. 2018;13:e0193869. doi:10.1371/journal.pone.0193869
35. Chien WT, Cheung EFC, Mui JHC, Gray R, Ip G. Adherence therapy for schizophrenia: a randomised controlled trial. Hong Kong Med J. 2019;25(Suppl 2):4–9.
36. Xu D, Xiao S, He H, et al. Lay health supporters aided by mobile text messaging to improve adherence, symptoms, and functioning among people with schizophrenia in a resource-poor community in rural China (LEAN): a randomized controlled trial. PLoS Med. 2019;16:1–21. doi:10.1371/journal.pmed.1002785
37. Montes JM, Medina E, Gomez-Beneyto M, Maurino J. A short message service (SMS)-based strategy for enhancing adherence to antipsychotic medication in schizophrenia. Psychiatry Res. 2012;200:89–95. doi:10.1016/j.psychres.2012.07.034
38. Barkhof E, Meijer CJ, De Sonneville LMJ, Linszen DH, De Haan L. The effect of motivational interviewing on medication adherence and hospitalization rates in nonadherent patients with multi-episode schizophrenia. Schizophr Bull. 2013;39:1242–1251. doi:10.1093/schbul/sbt138
39. Schulz M, Gray R, Spiekermann A, et al. Adherence therapy following an acute episode of schizophrenia: a multi-centre randomised controlled trial. Schizophr. Res. 2013;146:59–63. doi:10.1016/j.schres.2013.01.028
40. Chien WT, Mui JHC, Cheung EFC, Gray R. Effects of motivational interviewing-based adherence therapy for schizophrenia spectrum disorders: a randomized controlled trial. Trials. 2015;16(270). doi:10.1186/s13063-015-0785-z
41. Chien WT, Mui J, Gray R, Cheung E. Adherence therapy versus routine psychiatric care for people with schizophrenia spectrum disorders: a randomised controlled trial. BMC Psychiatry. 2016;16. doi:10.1186/s12888-016-0744-6
42. Ngoc TN, Weiss B, Trung LT. Effects of the family schizophrenia psychoeducation program for individuals with recent onset schizophrenia in Viet Nam. Asian J Psychiatr. 2016;22:162–166. doi:10.1016/j.ajp.2016.06.001
43. Velligan D, Mintz J, Maples N, et al. A randomized trial comparing in person and electronic interventions for improving adherence to oral medications in schizophrenia. Schizophr. Bull. 2013;39:999–1007. doi:10.1093/schbul/sbs116
44. Gray R, Bressington D, Ivanecka A, et al. Is adherence therapy an effective adjunct treatment for patients with schizophrenia spectrum disorders? A systematic review and meta-analysis. BMC Psychiatry. 2016;16. doi10.1186/s12888-016-0801-1
45. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Heal. 1999;14:1–24. doi:10.1080/08870449908407311
46. Nunes V, Neilson JO. Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence full guideline January 2009 National Collaborating Centre for Primary. Clin Guidel Evid Rev. 2009;364:1–364.
47. Morrison AP, Pyle M, Maughan D, et al. Antipsychotic medication versus psychological intervention versus a combination of both in adolescents with first-episode psychosis (MAPS): a multicentre, three-arm, randomised controlled pilot and feasibility study. Lancet Psychiatry. 2020;7:788–800. doi:10.1016/S2215-0366(20)30248-0
48. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74. doi:10.1097/00005650-198601000-00007
49. Tan XI, Patel I, Chang J. Review of the four item Morisky Medication Adherence Scale (MMAS-4) and eight item Morisky Medication Adherence Scale (MMAS-8). Innov Pharm Pharm. 2014;5(165):5.
50. Hogan TP, Awad AG. Subjective response to neuroleptics and outcome in schizophrenia: a re-examination comparing two measures. Psychol Med. 1992;22:347–352. doi:10.1017/S0033291700030282
51. Robles García R, Salazar Alvarado V, Páez Agraz F, Ramírez Barreto F. Assessment of drug attitudes in patients with schizophrenia: psychometric properties of the DAI Spanish version. Actas Esp Psiquiatr. 2004;32:138–142.
52. Nielsen RE, Lindström E, Nielsen J, Levander S. DAI-10 is as good as DAI-30 in schizophrenia. Eur Neuropsychopharmacol J Eur Coll Neuropsychopharmacol. 2012;22:747–750. doi:10.1016/j.euroneuro.2012.02.008
53. Staring ABP, Van der Gaag M, Koopmans GT, et al. Treatment adherence therapy in people with psychotic disorders: randomised controlled trial. Br J Psychiatry. 2010;197:448–455. doi:10.1192/bjp.bp.110.077289
54. Herz MI, Lamberti JS, Mintz J, et al. A program for relapse prevention in schizophrenia: a controlled study. Arch Gen Psychiatry. 2000;57:277–283. doi:10.1001/archpsyc.57.3.277
55. Dunja D, Požgain I, Grgic M, Filakovic P. Psychoeducation and compliance in the treatment of the patients with schizophrenia. Coll Antropol. 2007;31:1111–1115.
56. Romano M, Peters L. Evaluating the mechanisms of change in motivational interviewing in the treatment of mental health problems: a review and meta-analysis. Clin Psychol Rev. 2015;38:1–12. doi:10.1016/j.cpr.2015.02.008
57. Lawrence RN, Fullbrook P, Somerset S, Schulz P. Motivational interviewing to enhance treatment attendance in mental motivational interviewing to enhance treatment attendance in mental health settings: a systematic review and meta- - analysis. J Psychiatry Ment Heal Nurs. 2017;1–20. doi:10.1111/jpm.12420
58. Sarabi RE, Sadoughi F, Orak RJ, Bahaadinbeigy K. The effectiveness of mobile phone text messaging in improving medication adherence for patients with chronic diseases: a systematic review. Iran Red Crescent Med J. 2016;18:1–8.
59. Schwebel FJ, Larimer ME. Using text message reminders in health care services: a narrative literature review. Internet Interv. 2018;13:82–104. doi:10.1016/j.invent.2018.06.002
60. Samprasit N, Bunchuailua W, Kapol N. Outcomes of pharmacist intervention in schizophrenic patients: a systematic review and meta-analysis of randomized controlled trials. Srinagarind Med J. 2020;35:576–583.
61. Dolder CR, Lacro JP, Leckband S, Jeste DV. Interventions to improve antipsychotic medication adherence: review of recent literature. J Clin Psychopharmacol. 2003;23:389–399. doi:10.1097/01.jcp.0000085413.08426.41
62. Pothimas N, Tungpunkom P, Kanungpiarn T, Hannes K. Experiences of medication adherence among people with schizophrenia: a qualitative systematic review. Pacific Rim Int J Nurs Res. 2021;25:229–241.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of COVID-19 Pandemic on Prescribing of Long-Acting Injectable Antipsychotics for Schizophrenia: Results from a United States Prescriber Survey
Zhdanava M, Starr HL, Totev TI, Lefebvre P, Shah A, Sheng K, Pilon D
Neuropsychiatric Disease and Treatment 2022, 18:2003-2019
Published Date: 7 September 2022
The Development of Schematics to Illustrate Women’s Experiences with Adjuvant Hormone Therapy in the Treatment of Breast Cancer
AlOmeir O, Patel N, Donyai P
Patient Preference and Adherence 2022, 16:2639-2647
Published Date: 23 September 2022
Perceptions with Type 2 Diabetes Mellitus of the Value of Prescribed Medications Among Malaysian Adults: A Qualitative Study
Lim MC, Hatah E, Lai KC, Buang A, Koay TJ, Sim WJY, Ng SC
Patient Preference and Adherence 2022, 16:3133-3142
Published Date: 29 November 2022
The Effect of Longer Dosing Intervals for Long-Acting Injectable Antipsychotics on Outcomes in Schizophrenia
Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, Wang S, Richarz U, Gopal S, Kane JM
Neuropsychiatric Disease and Treatment 2023, 19:531-545
Published Date: 7 March 2023
Investigating the Effect of Adherence to Antipsychotic Therapy on the Length of Stay and Number of Hospitalizations in Patients with Schizophrenia – A Descriptive Analysis
Barliana MI, Ramdini DA, Afifah NN, Alfian SD, Sumiwi SA
Patient Preference and Adherence 2023, 17:2737-2747
Published Date: 1 November 2023