")
Back to Journals » Clinical Epidemiology » Volume 15
Screening History and 7-Year Survival in 32,099 Colorectal Cancer Patients: A Population-Based Cohort Study
Authors Hsiao BY , Chiang CJ, Yang YW , Lin LJ, Hsu TH , Lee WC
Received 28 June 2023
Accepted for publication 26 September 2023
Published 3 October 2023 Volume 2023:15 Pages 1009—1025
DOI https://doi.org/10.2147/CLEP.S424918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Vera Ehrenstein
Bo-Yu Hsiao,1 Chun-Ju Chiang,1,2 Ya-Wen Yang,1,2 Li-Ju Lin,3 Tsui-Hsia Hsu,3 Wen-Chung Lee1,2,4
1Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan; 2Taiwan Cancer Registry, Taipei, Taiwan; 3Health Promotion Administration, Ministry of Health and Welfare, Taipei, Taiwan; 4Institute of Health Data Analytics and Statistics, College of Public Health, National Taiwan University, Taipei, Taiwan
Correspondence: Wen-Chung Lee, Institute of Health Data Analytics and Statistics, College of Public Health, National Taiwan University, Rm. 536, No. 17, Xuzhou Road, Taipei, 100, Taiwan, Tel +886-2-23511955, Email [email protected]
Background: It is unclear whether colorectal cancer screening history, regardless of stage, is an independent predictor of survival, and if the screening advantage persists after diagnosis. 32 099 patients with colorectal cancer were enrolled in this population-based cohort study.
Methods: We used data from the Taiwan Cancer Registry on patients with a first-time diagnosis of colorectal cancer between 2013 and 2015. In addition, we utilized data from a nationwide database of colorectal cancer screening programs to evaluate patients’ screening histories, and sourced outcome data from the National Death Registry, tracking patients up to the last day of 2019.
Results: Compared with fecal immunochemical testing (FIT)-positive patients with a follow-up examination, the adjusted hazard ratios (95% confidence intervals) for death from colorectal cancer were 1.40 (1.26– 1.56) for FIT-positive patients without a follow-up examination, 1.63 (1.48– 1.78) for FIT-negative patients, and 1.76 (1.65– 1.89) for never screened patients. The adjusted hazard ratios for the FIT-positive patients with a follow-up examination increased when diagnosis was delayed by more than 12 months and were 1.2 after a 2-year delay. The adjusted hazard ratios for FIT-negative patients were approximately 2.0, decreased rapidly to 1.6, and stabilized after the 9th time-to-diagnosis month.
Conclusion: In colorectal cancer patients, screening history prior to diagnosis is an independent prognostic factor, regardless of cancer stage or other variables. This study recommends that physicians take screening history into account during diagnosis to optimize follow-up and management for patients at higher risk.
Keywords: cancer registry, cancer screening, cohort study, colorectal cancer, prognosis
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Wardoyo has been published for this article.
Introduction
Colorectal cancer is the third most common cancer worldwide in terms of incidence and mortality.1 The age-standardized incidence and mortality rate for colorectal cancer in Taiwan, which were 38.1 and 12.4 (per 105) in 2019, respectively, are higher than those in Japan and Korea, and both rates have been increasing.2,3 Screening, a crucial intervention in the prevention of colorectal cancer that is typically performed in countries where colorectal cancer is prevalent, has been implemented in Taiwan since 2004.
Screening effectively reduces the incidence of and mortality from colorectal cancer.4–6 Previous studies have noted that a significant proportion of individuals who undergo screening are diagnosed with early-stage cancer, in contrast to those who are not screened.7–9 As the detection of cancer at an earlier stage is linked to lower mortality rates,10 prompt intervention subsequent to identifying preinvasive or early-stage colorectal cancer through screening becomes pivotal in curbing colorectal cancer-related mortality. Nevertheless, the enduring presence of survival advantages from screening post-diagnosis, even within the same cancer stage, remains uncertain.
Previous studies have compared two types of colorectal cancer cases considering stage matching: the “screen-detected” cases identified through screening methods and the “symptomatically diagnosed” cases detected based on the appearance of symptoms.11–13 The research findings indicate that individuals who underwent colorectal cancer screening using methods such as colonoscopy or the traditional fecal occult blood testing (FOBT), also known as guaiac-based FOBT, showed significant survival advantages when diagnosed at more advanced stages.11–13 However, discrepancies have arisen in their findings concerning early-stage colorectal cancer. The limited sample sizes (less than 2500 patients) in these studies may account for the significant divergence in their outcomes. Additionally, the applicability of these studies to the screened population in their respective countries might be compromised due to their hospital-based and regional study designs. Recently, a Korean population-based cohort study using national screening data compared survival outcomes between patients at the same stage of cancer who had been screened using the newer fecal immunochemical testing (FIT) and those who had never undergone screening.14 The study included approximately 35 000 patients with colorectal cancer and found that ever-screened patients had a significantly higher rate of survival than never-screened patients at every stage (including early stages). However, the study did not consider a colonoscopy examination, and patients with negative and positive results of FIT were not distinguished in their analysis. We hypothesized that FIT-positive and FIT-negative patients would differ in their prognosis and should thus be distinguished in studies.
This study aimed to evaluate the impact of colorectal cancer screening on survival outcomes based on the patient’s screening history. Additionally, the study sought to determine whether the patient’s screening history could serve as an independent predictor of survival, regardless of the stage of cancer.
Methods
Colorectal Cancer Screening Program and Dataset
Launched in 2004, Taiwan has a nationwide colorectal cancer screening program that provides a biennial single-sample FIT to residents aged 50 to 69 years.15 As part of this program, FIT screening kits are delivered through regional health centers and health bureaus in 25 municipalities, and 1501 hospitals and clinics were enrolled to participate in this program in 2010. In 2013, the program was expanded to cover individuals up to 74 years old, and the number of participating hospitals and clinics was doubled from its initial figure in 2010.16 Two FIT kit systems (OC-Sensor, Eiken Chemical, Tokyo, Japan; HM-Jack, Kyowa Medex, Tokyo, Japan) were utilized in this program. The choice of kit was determined by the procurement processes of individual municipalities. Both kits had a cutoff concentration of 20 µg of hemoglobin per gram of feces to define a positive result. This decision was based on a cost-effectiveness analysis from a community-based pilot study that confirmed the kits’ accuracy.17 Participants were randomly assigned to use one of the different FIT kits. After screening, the FIT results were sent to the screenees through mail or by a physician in the outpatient clinics. Screenees with a positive FIT result were then referred to within 3 months for their diagnosis to be confirmed through colonoscopy. Screenees who were not suitable for a colonoscopy were offered alternative diagnostic methods, such as a double-contrast barium enema and a flexible sigmoidoscopy. Screenees with a negative FIT result or who completed a diagnostic test were asked to undergo screening again biennially. We observed the data of approximately 5 million screenees from 2010 to 2019, including their FIT results and the follow-up examination results of individuals with a positive FIT result.
Study Design and Data Linkage
This population-based cohort study analyzed data from the Taiwan Cancer Registry on patients with a first-time diagnosis of colorectal cancer between 2013 and 2015. The Taiwan Cancer Registry is a comprehensive, nationwide, population-based database. Its completeness is calculated by comparing registered cancer cases to potential cases derived from death certificates, National Health Insurance-designated catastrophic illnesses, and major cancer screening programs; it has a completeness rate exceeding 98%. The registry also maintains a high level of timeliness, with less than a 14-month interval between diagnosis and reporting to the central cancer registry system. Furthermore, it has a morphologically verified rate of 93%, meaning that cancer diagnoses are confirmed through histological or cytological methods. Cases solely registered through death certificates make up less than 1% of the total.18,19 Patients with only precancerous lesions or a diagnosis of colorectal cancer without indication of the stage (6%) were excluded. The patients who lacked stage information were slightly older and had undergone less chemotherapy, while other characteristics were similar to those who had stage information. We restricted the analysis to 32 099 patients aged ≧50 years in 2010 (the target population of the colorectal cancer screening program). We used the data obtained from a nationwide colorectal cancer screening program database to assess the screening history of patients and the data from the National Death Registry to follow up on patient outcomes until the last day of 2019.
The incidence of colorectal cancer (ICD-O-3: C18-21) and associated mortality (ICD-10: C18-21) were identified on the basis of the International Classification of Diseases. The colorectal cancer stages were classified as stage 0 (carcinoma in situ) to stage IV in accordance with the American Joint Committee on Cancer Staging Manual (AJCC). Level of urbanization for the place of residence of the patients were coded from the highest to the lowest, with each level corresponding to a metropolis, city, growing town, town, old town, agricultural town, and village, respectively.20 The hospitals where patients had a diagnosis and were treated were categorized into medical centers, regional hospitals, and local community hospitals. The site of colorectal cancer was grouped into 4 locations: the distal colon (ie, the splenic flexure, descending, sigmoid colon, and rectosigmoid junction), the proximal colon (ie, the cecum, ascending, hepatic flexure, and transverse colon), the rectum and anus (ie, the rectum, anus, canal, and their overlapping sites), and others or unspecified (ie, the appendix, unspecified, and overlapping sites of the colon). We also examined the treatment methods of patients with colorectal cancer, especially chemotherapy. Patients with at least one FIT record from 1 January 2010 to the date of the diagnosis of colorectal cancer were referred to as the ever-screened patients. The ever-screened patients were categorized into FIT-positive or FIT-negative patients according to their latest FIT results before the diagnosis. The FIT-positive patients were further divided into 2 groups according to whether a follow-up examination (eg, a colonoscopy, a double-contrast barium enema, and a flexible sigmoidoscopy) was performed before the diagnosis of colorectal cancer.
Statistical Analysis
After diagnosis, the cumulative probability curves of death from colorectal cancer between the FIT-positive with/without a follow-up examination, the FIT-negative, and the never-screened patients were compared using the log rank test. We used a Cox regression model to evaluate the association between screening history and prognosis (death from colorectal cancer after diagnosis) with adjustment for various confounding factors (eg, age at diagnosis, sex, urbanization level, hospital type, treatment, cancer sites, and cancer stage). We also used a Cox regression model for the ever-screened patients to explore the association between time to diagnosis (ie, from the last FIT) and death from colorectal cancer after diagnosis. Because the association might be nonlinear, we used a restricted cubic spline (knots placed at the 3rd, 6th, and 12th months) to fit the dose-response curve.
We conducted sensitivity analyses to assess the stability of our results, adjusting for other colorectal cancer staging systems (including more detailed AJCC, Dukes’, and SEER staging), and for several prognosis-related clinicopathological variables (including tumor grading, tumor size, lymph node ratio, circumferential resection margin, perineural invasion, bowel obstruction, and bowel perforation). Additionally, we took steps to mitigate common biases in screening impact studies, including competing risks, lead-time bias, and length bias. To account for competing risks, we utilized the Fine-Gray model.21 To address lead-time and length biases, we implemented correction methods suggested by Duffy et al’s study.21
All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Ethical Approval and Data Availability
The study protocol was approved by the National Taiwan University Research Ethics Committee (NTU-REC No.202101HM030) and the Data Release Review Board of the Health Promotion Administration, Ministry of Health and Welfare in Taiwan. The National Taiwan University Research Ethics Committee waived the requirement for informed consent due to the lack of personal information and secondary data in the study. All methods were performed in accordance with the relevant guidelines and regulations. Due to legal restrictions imposed by the government of Taiwan in relation to the “Personal Information Protection Act”, data cannot be made publicly available.
Results
The characteristics and follow-up outcomes of 32 099 patients with a diagnosis of colorectal cancer for the first time between 2013 and 2015 are shown in Table 1. The majority of patients were 60 to 64 years old (17.1%), men (58%), living in areas with higher (metropolis and city) urbanization levels (54.1%), having a diagnosis in medical centers (54.1%), having cancer at the distal colon (41.3%), and having received treatment (95%) after the diagnosis. According to the AJCC staging classification (stage 0 to IV), most patients in this study had a diagnosis of stage III cancer (28.5%). We examined the past screening history for each colorectal cancer patient before their diagnosis up until 2010. Individuals who participated in screening at least once were classified as “ever-screened”. A total of 13 559 individuals met this criterion, accounting for 42.2% of the total patient population. Of these patients, 8 797 patients had a positive FIT result with a follow-up examination at the last screening, 1 826 patients had a positive FIT result without a follow-up examination and the remaining 2 936 patients had negative FIT results at the last screening. In the follow-up period until the end of 2019, 17 711 (55.2%) patients were alive, 10 190 (31.8%) patients died from colorectal cancer, and 4 198 (13.1%) died from other causes. Patients who tested FIT-positive and underwent a follow-up examination had higher proportions of stage 0 (19.0%) and stage I (30.9%) colorectal cancer diagnoses. Conversely, those who tested FIT-positive but did not undergo follow-up examination, as well as those who tested FIT-negative and those who were never-screened, had higher proportions of stage III (25.7% to 30.7%) and stage IV (18.8% to 26.0%) colorectal cancer diagnoses. Additionally, among those tested FIT-positive and received a follow-up examination, 78.8% remained alive during the follow-up period, while among the never-screened group, 41.5% died from colorectal cancer and 17.0% from other causes.
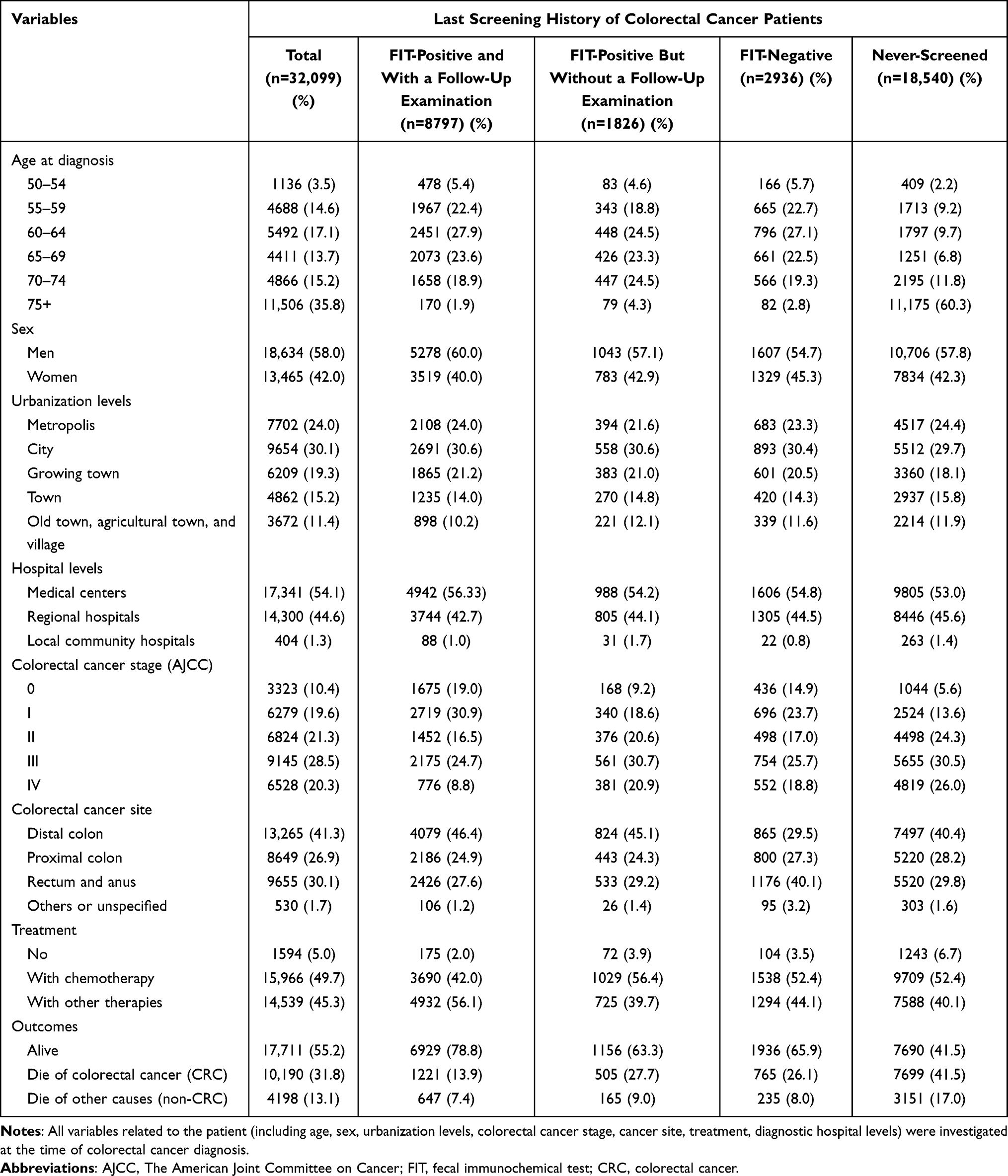 |
Table 1 Baseline Characteristics and Outcomes for Patients Diagnosed with Colorectal Cancer Between 2013 and 2015 |
The cumulative probabilities of death from colorectal cancer for all patients with stages are shown in Figure 1. For all patients, regardless of stage, the 7-year (since diagnosis) cumulative probability of death from colorectal cancer in patients who had never been screened was 47.8%, which was significantly higher than those who were FIT-negative (29.2%), FIT-positive without a follow-up examination (31.5%), and FIT-positive with a follow-up examination (16.4%). For every stage (ie, stage 0 to stage IV), the cumulative probabilities of death from colorectal cancer were significantly different among patients with 4 screening histories. For patients who were never-screened, FIT-negative, FIT-positive without a follow-up examination, and FIT-positive with a follow-up examination, the 7-year cumulative probabilities of death from colorectal cancer were 8.9%, 1.8%, 1.9%, and 1.2% for stage 0, 15.4%, 5.5%, 7.7%, and 4.9% for stage I, 29.6%, 18.4%, 18.0%, and 11.0% for stage II, 47.9%, 33.4%, 27.2%, and 22.5% for stage III, 91.4%, 86.9%, 87.2%, and 84.5% for stage IV, respectively. We also provide a comparison of survival rates between colorectal cancer patients who were ever-screened and those who were never-screened (Supplementary Figure S1). The results show that, overall, patients who were ever-screened had better 7-year survival rates than those who were never screened.
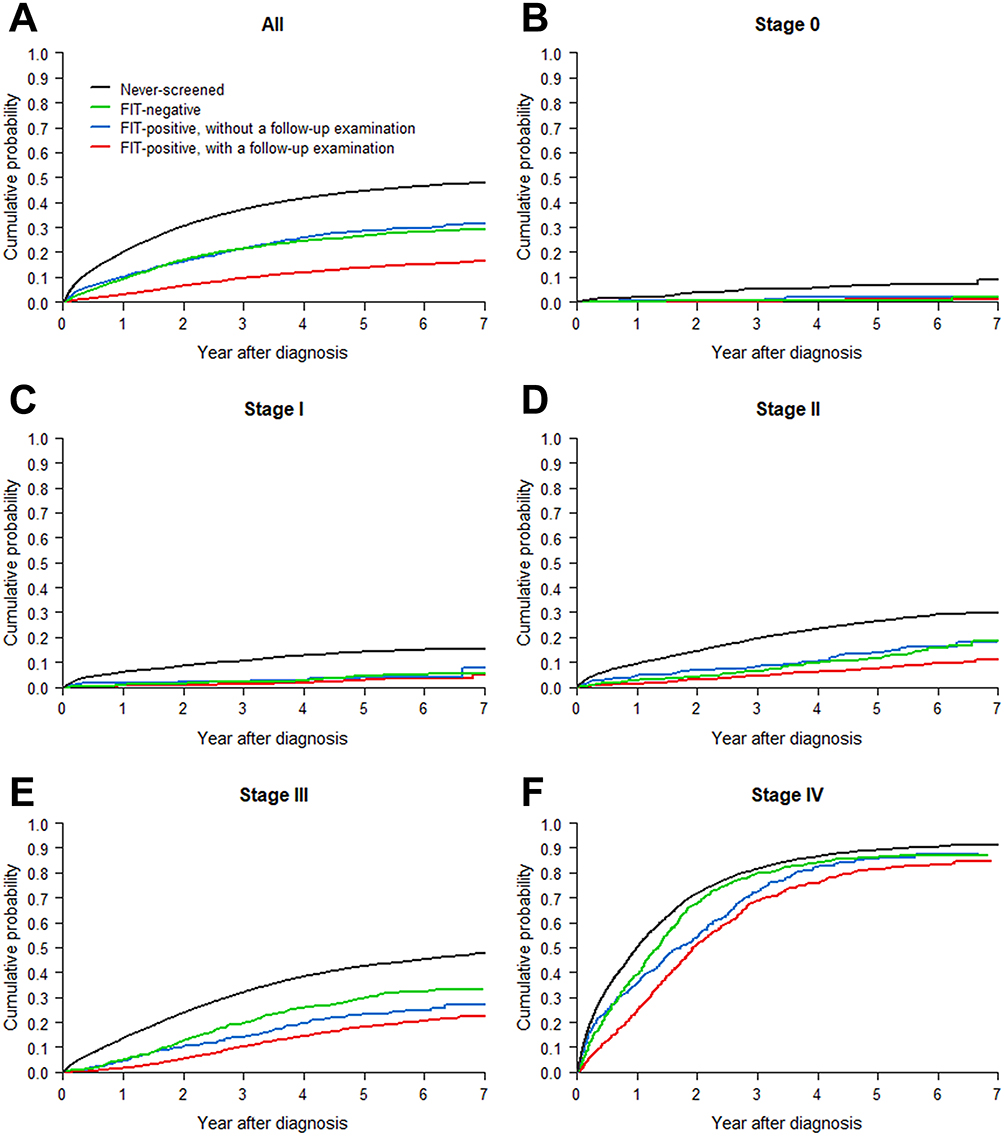 |
Figure 1 Cumulative Probability of Colorectal Cancer Death by Screening History and Colorectal Cancer Stages. Notes: (A) All Patients Regardless of Stages; (B) Stage 0; (C) Stage I; (D) Stage II; (E) Stage III; (F) Stage IV. |
Table 2 presents the hazard rates and hazard ratios for deaths from colorectal cancer. Patients who were never screened, patients having a diagnosis in local community hospitals, patients with advanced-stage colorectal cancer, patients with cancer at the proximal colon, patients not receiving treatment after diagnosis, older patients, men, and patients living in lower urbanization levels had a higher risk of death from colorectal cancer. Compared with FIT-positive patients with a follow-up examination, the crude hazard ratios (crude-HRs) and rate differences (RDs, per 100 person-year) of death from colorectal cancer for the patients who were never-screened were 4.06 and 9.8, that for patients who were FIT-negative were 2.09 and 3.3, and that for patients who were FIT-positive without a follow-up examination were 2.24 and 3.8. After adjustment for other variables (ie, cancer stage, cancer site, hospital for diagnosis, treatment, age at diagnosis, sex, and urbanization levels), the adjusted hazard ratios (Adj-HRs) decreased but were significantly higher than 1. The Adj-HRs were 1.76 for never-screened patients, 1.63 for FIT-negative patients, and 1.40 for FIT-positive patients without a follow-up examination. Overall, colorectal cancer mortality hazard for ever-screened patients was 0.68 times that of never-screened patients, and the RD was −8.7 (per 100 person-year) (Supplementary Table S1). Similar results were obtained when different colorectal cancer staging systems were used for adjustment (Supplementary Table S2).
 |
Table 2 Hazard Rates and Hazard Ratios for Death Due to Colorectal Cancer |
Table 3 presents the results of the stratified analysis by cancer stage. With or without adjusting for other variables, we found that the risk of death from colorectal cancer in never-screened patients was significantly higher than that in FIT-positive patients with colonoscopy examination at every stage (stage 0 to IV, Crude-HRs: 6.96, 5.13, 3.75, 2.84 and 1.61; Adj-HRs: 3.62, 1.83, 2.06, 1.93, and 1.36). The risk of death from colorectal cancer in the FIT-negative patients were also higher (for stage I or above) or significantly higher (for stage II or above) than that in the FIT-positive patients with a follow-up examination (stage 0 to IV, Crude-HRs: 0.92, 1.48 1.65, 1.74, and 1.36; Adj-HRs: 0.87, 1.26, 1.49, 1.70, and 1.40). In addition, FIT-positive patients without a follow-up examination had an increased risk of death from colorectal cancer (stage 0 to IV, Crude-HRs: 1.79, 1.42 1.86, 1.31, and 1.20; Adj-HRs: 1.48, 1.28, 1.79, 1.22, and 1.24). The comparison results between ever-screened and never-screened patients by cancer stages are presented in Supplementary Table S1.
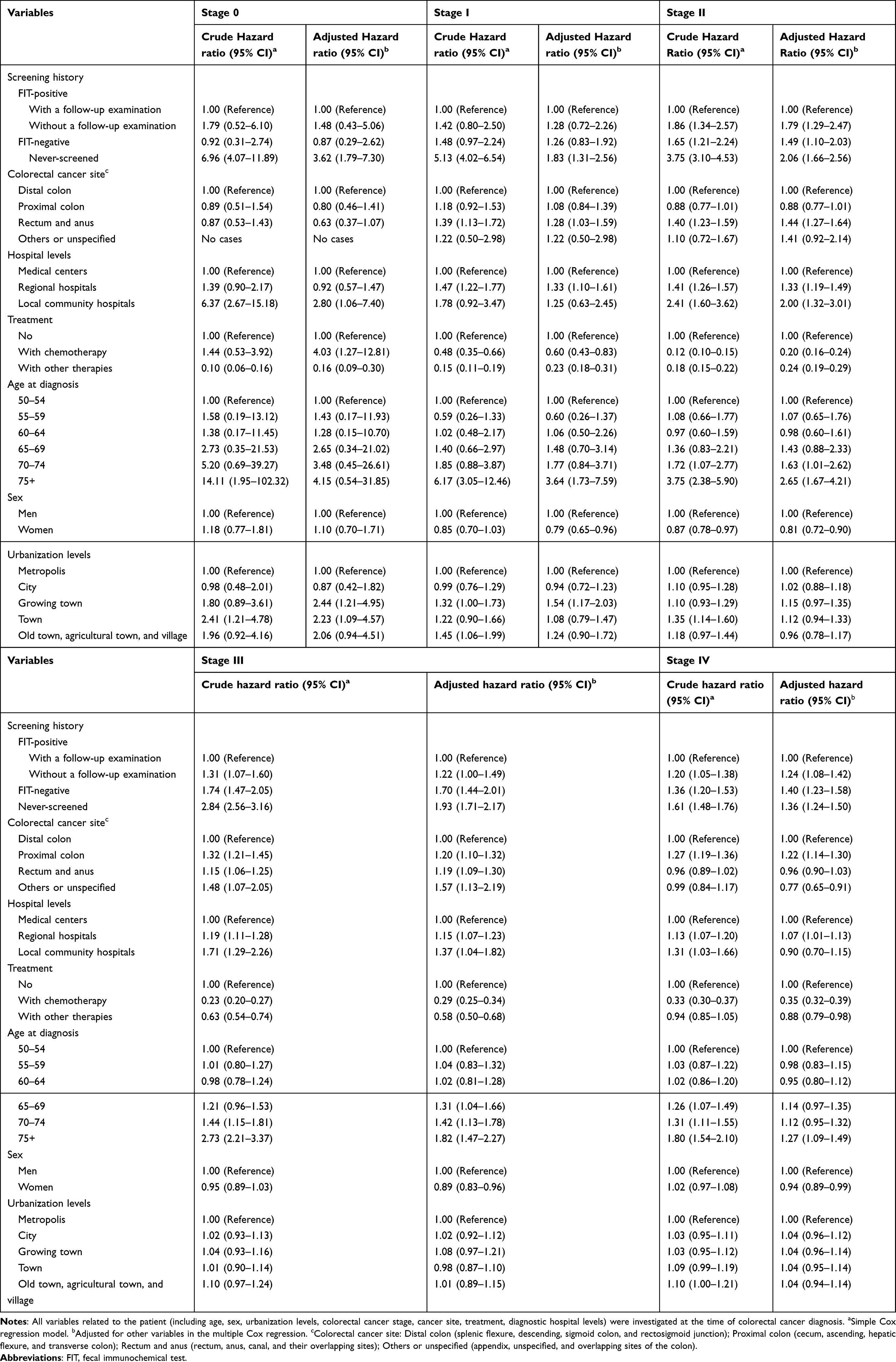 |
Table 3 Hazard Ratios for Death Due to Colorectal Cancer by Colorectal Cancer Stage |
Supplementary Table S3 presents hazard rates and hazard ratios for death from colorectal cancer in different categories of time to diagnosis (ie, from the last FIT). Figure 2 shows the dose-response curves of the time to diagnosis and death from colorectal cancer. The Adj-HR of death from colorectal cancer among FIT-positive patients with a follow-up examination was approximately 1.0. However, the Adj-HR increased when the diagnosis was delayed by more than 12 months and was 1.2 after a 2-year delay. The Adj-HR of death from colorectal cancer in FIT-positive patients without a follow-up examination remains relatively stable, ranging from 1.3 to 1.4. The Adj-HRs of FIT-negative patients were approximately at 2.0, decreased rapidly to 1.6, and stabilized after 9 months.
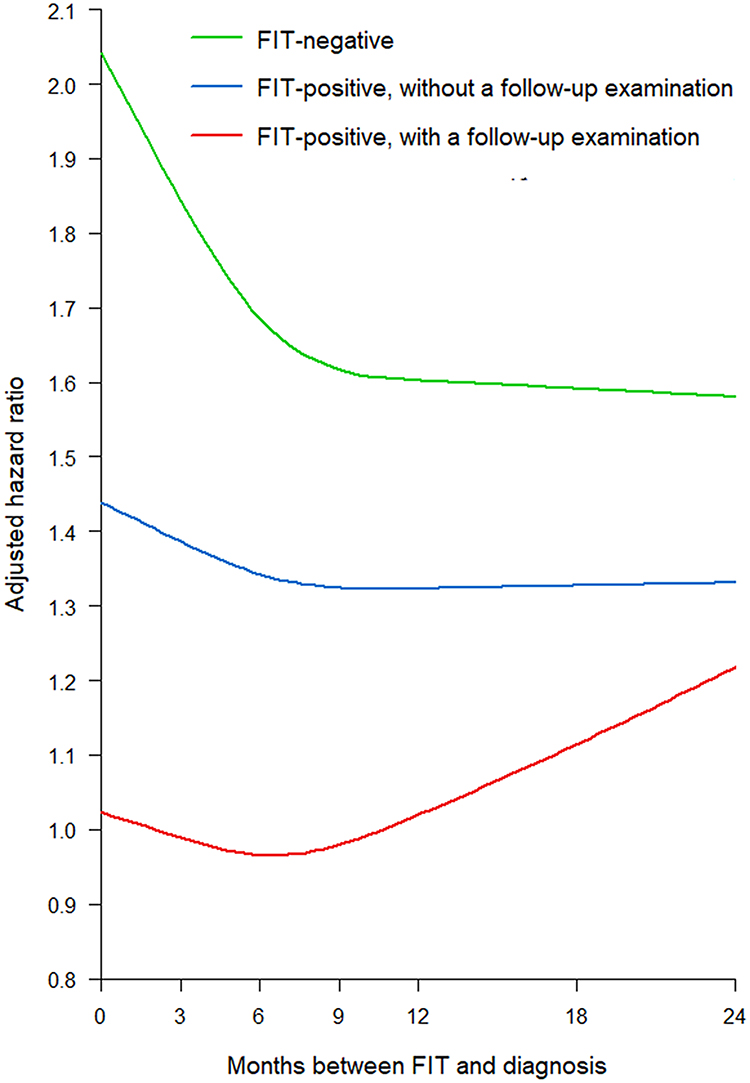 |
Figure 2 Dose-response Curves of the Time to Diagnosis (from the Last Fecal Immunochemical Testing) and Colorectal Cancer Death. |
We detailed the results of accounting for competing risks, lead-time bias correction, and length bias adjustment in Supplementary Table S4. Relative to FIT-positive patients who underwent a follow-up examination, the Adj-HRs for colorectal cancer death—after accounting for competing risks (Model 2)—were 1.38, 1.55, and 1.69 for FIT-positive patients without follow-up, FIT-negative patients, and those who were never screened, respectively. After lead-time bias correction (Model 3), these Adj-HRs decreased to 1.10, 1.26, and 1.37, respectively. Similarly, the crude hazard ratios (Crude-HRs) also saw a decline after correcting for length bias (Model 4), settling at 1.87, 1.83, and 3.53, in contrast to the initial Cox model (Model 1). Supplementary Figure S2 illustrates the overall impact of lead-time bias correction for patients who have ever been screened, and the potential estimation ranges for length bias correction are provided in Supplementary Tables S5–S7.
Discussion
This study revealed that, after adjusting for cancer stage and other variables, the mortality risks for colorectal cancer patients are ranked as follows: FIT-positive patients with follow-up examinations have the lowest risk, followed by FIT-positive patients without follow-up, then FIT-negative patients, and finally, patients who were never screened have the highest risk. Unlike previous studies that compared prognoses between only two categories of patients—either screen-detected versus symptomatically-diagnosed11–13 or ever-screened versus never-screened14 our research offers a more detailed stratification of patients’ mortality risks. Specifically, we observed that patients who underwent screening, irrespective of their FIT results, consistently demonstrated lower mortality risks compared to those who were never screened. The results remained consistent when adjusted for cancer stage using various staging systems (Supplementary Table S2), and they were stable across different demographics and clinical variables such as age, sex, cancer site, treatment, and clinicopathological status,22 (Supplementary Table S8). This suggests that a patient’s screening history prior to diagnosis serves as an independent prognostic factor23 irrespective of cancer stage or other influencing variables.
Furthermore, we found that screening had survival benefits with respect to other causes of death (Supplementary Table S9). A plausible reason could be that individuals who participate in the screening program are generally more health-conscious. Additionally, we observed that the primary causes of death were malignant neoplasms (31%) and circulatory system diseases (19%). Previous studies have shown that approximately 25% to 30% of patients with colorectal cancer had liver metastases within 6 months of diagnosis and nearly 50% throughout their lives.24,25 In addition, patients with colorectal cancer had an increased risk of cardiovascular diseases.26,27 Additional studies are warranted to examine whether colorectal cancer screening can reduce metastases to the liver (or other sites) and prevent cardiovascular diseases by reducing the incidence of colorectal cancer and associated mortality. On the other hand, we utilized a competing risk model (Fine and Gray model) to evaluate the relationship between screening history and colorectal cancer mortality (Model 2 in Supplementary Table S4). Our analysis revealed a slight reduction in the effect of screening history, but the relationship remained significant.
This study revealed that colorectal cancer patients who were FIT-positive and had follow-up examinations exhibited the best survival outcomes. This is primarily attributed to the fact that this group mainly consists of asymptomatic screen-detected colorectal cancer patients. Early treatment in asymptomatic FIT-positive patients with a follow-up examination can yield better survival.28 A previous study also observed this phenomenon.11 However, patients without a follow-up examination may have developed symptoms at the diagnosis and lose the full benefit of screening, which resulted in poorer survival (Adj-HR = 1.40 compared with those with a follow-up examination). The risk of postponed diagnostic examination increases, a trend also substantiated by our observation that FIT-positive patients, even with follow-up examinations, faced an amplified risk of succumbing to colorectal cancer if their diagnosis occurred more than 1 year after their screening results, subsequent to adjustments for cancer stage and other confounding factors (Figure 2). Previous analyses of time-to-diagnosis primarily focused on FIT-positive patients, revealing that individuals who underwent colonoscopy more than 6 months after a FIT-positive result exhibited a notably elevated risk of advanced-stage colorectal cancer.29 The delay in diagnostic examination can be attributed to a variety of factors, including limited colonoscopy capacity following the expansion of FIT screenings after 2010,30 lack of patient awareness about the significance of positive FIT results, limitations in healthcare services, extended waiting times that result in patient drop-off, and financial constraints that make examinations unaffordable for some individuals.31 A recent study also assessed the time to diagnosis among those who had undergone screening.14 However, it is important to emphasize that the study focused on individuals who had participated in screening previously, without distinguishing between different FIT results or evaluating whether follow-up examinations were conducted.
In this study, we observed that FIT-negative patients diagnosed early with colorectal cancer faced a higher risk of mortality compared to those diagnosed later (Figure 2). These early-diagnosed patients received their cancer diagnosis shortly after obtaining a negative FIT result. There are two plausible explanations for this outcome. First, the negative FIT results could be false negatives. Second, these patients’ diseases might have progressed rapidly from the initial emergence of cancer cells to requiring medical intervention,32,33 potentially resulting in a worse prognosis. Furthermore, as a group, the FIT-negative patients had even poorer survival compared to those who were FIT-positive. The majority of these FIT-negative patients fell under the category of interval cancer cases.34 These patients already showed symptoms at the time of their diagnosis, leading to a poorer prognosis compared to FIT-positive patients, irrespective of whether or not they had undergone follow-up examinations. In this context, we also conducted a comparative analysis of colorectal cancer mortality risk among three categories of patients: screen-detected patients (those diagnosed through a positive FIT result and a follow-up examination), symptomatic interval cancer patients (those diagnosed within 2 years following their most recent negative FIT result), and never-screened patients (Supplementary Table S10). Consistent with prior study, screen-detected patients exhibited higher survival rates than interval cancer patients.13 However, a notable departure from previous research was our observation of interval cancer patients demonstrating a more favorable survival trend compared to never-screened patients. This could potentially be attributed to heightened symptom awareness or overall health consciousness among FIT-negative patients.
Nevertheless, the apparent survival benefit of screening should still be interpreted cautiously. First, while the screening effect refers to the scenario in which screened patients are diagnosed earlier in the disease progression compared to their never-screened counterparts, the comparison of survival rates between these groups is frequently influenced by the argument that screened patients have effectively advanced the starting point for measuring survival—a phenomenon known as the lead-time bias. To address this bias, we referred to a study that evaluated transition rates of every colorectal cancer stage based on this Taiwanese population-based screening.35 Using that transition rates, we adjusted for possible lead time in screen detection among FIT-positive patients with follow-up examinations.21 After lead-time correction, there remains a significant difference in crude hazard rates between FIT-positive patients with a follow-up examination and never-screened patients (Model 3 in Supplementary Table S4); the time to diagnosis within 12 months among FIT-positive patients with a follow-up examination showed the lowest risk of colorectal cancer mortality (Supplementary Table S11), and ever-screened patients exhibited a significant survival advantage over never-screened patients (Supplementary Figure S2). Second, length time bias may also be present in our results. Slow-growing tumors were more likely to be detected through screening than fast-growing tumors; therefore, a survival benefit was present among the screened patients. We corrected length bias and performed sensitivity analyses.21 After the correction, the screening effect slightly decreased but still remained significantly different from those who were never-screened (Model 4 in Supplementary Table S4). Finally, compared with patients who were never-screened, patients who had been screened were usually more health-conscious and had better compliance to treatment once they had a disease, which may result in better survival. However, in this study, we found that screened patients differed in their prognosis with respect to their FIT results and whether they underwent a follow-up examination.
This study has several limitations. First, we only obtained screening data after 2010. The never-screened patients in this study might have participated in screening or underwent the endoscopy before 2010. If so, we underestimated the effect of screening. Second, several crucial prognostic factors for colorectal cancer were not adjusted for in this study, such as family history of colorectal cancer and a patient’s socioeconomic status. Unfortunately, this information was unavailable in the databases.
In recent years, stool deoxyribonucleic acid (sDNA) testing has shown greater sensitivity in detecting colorectal cancer and advanced adenomas compared to the FIT, offering potential as a promising alternative for non-invasive screening.36,37 This method could address the limitations associated with FIT’s false-negative outcomes that can occur with a single non-bleeding stool sample.38 While sDNA testing has not yet been definitively proven as an effective screening tool for colorectal cancer,39 it has been adopted for screening purposes in countries like the United States,40 the United Kingdom,41 Canada,42 and Australia.43 Future research could explore survival outcomes for patients detected via sDNA testing, comparing these with outcomes for patients detected using FIT and subsequent colonoscopy. If sDNA testing is found to produce better outcomes, it may serve as an alternative to invasive colonoscopy in screening protocols.
In conclusion, this 7-year follow-up of 32 099 patients with colorectal cancer showed that screening using FIT has benefits in addition to stage shift: patients in the same stage of colorectal cancer who were screened had better survival than those who were not. However, patients with a negative FIT result and patients with a positive FIT result without a follow-up examination were at higher risk of death from colorectal cancer. FIT-negative interval cancer patients are often symptomatic at diagnosis, resulting in a poorer prognosis. The risk of death also increased for patients with colorectal cancer with a positive FIT result and a follow-up examination but with delayed diagnosis by more than 12 months. In colorectal cancer patients, screening history prior to diagnosis is an independent prognostic factor, regardless of cancer stage or other variables. This study recommends that physicians take screening history into account during diagnosis to optimize follow-up and management for patients at higher risk.
Acknowledgment
The content of this research may not represent the opinion of the Taiwan Health Promotion Administration, Ministry of Health and Welfare. This study originated from the doctoral dissertation of Bo-Yu Hsiao, the first author of this paper, which was conducted at the National Taiwan University under the supervision of Professor Wen-Chung Lee, the corresponding author. This article was subsidized for English editing by National Taiwan University under the Excellence Improvement Program for Doctoral Students (grant number 108-2926-I-002-002-MY4), sponsored by the National Science and Technology Council, Taiwan.
Funding
This work is supported by grants from the Health Promotion Administration, the Ministry of Health and Welfare in Taiwan (A1111010; Tobacco Health and Welfare Taxation), and the National Science and Technology Council in Taiwan (MOST 111-2314-B-002-089-MY3). The funders had no role in study design, data collection, and analysis, the decision to publish, or preparation of the manuscript.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019;14(2):89–103. doi:10.5114/pg.2018.81072
2. Taiwan cancer registry. Incidence and mortality rates for top 10 cancers in Taiwan; 2019. Available from: https://twcr.tw/wp-content/uploads/2022/02/Top-10-cancers-in-Taiwan-2019.pdf.
3. Chiu HM, Chang LC, Hsu WF, et al. Non-invasive screening for colorectal cancer in Asia. Best Pract Res Clin Gastroenterol. 2015;29(6):953–965. doi:10.1016/j.bpg.2015.09.015
4. Breekveldt ECH, Lansdorp-Vogelaar I, Toes-Zoutendijk E, et al. Colorectal cancer incidence, mortality, tumour characteristics, and treatment before and after introduction of the faecal immunochemical testing-based screening programme in the Netherlands: a population-based study. Lancet Gastroenterol Hepatol. 2022;7(1):60–68. doi:10.1016/S2468-1253(21)00368-X
5. Brenner H, Stock C, Hoffmeister M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ. 2014;348:g2467. doi:10.1136/bmj.g2467
6. Hamza S, Cottet V, Touillon N, et al. Long-term effect of faecal occult blood screening on incidence and mortality from colorectal cancer. Dig Liver Dis. 2014;46(12):1121–1125. doi:10.1016/j.dld.2014.08.041
7. Law CC, Wong CHN, Chong PSK, et al. Effectiveness of population-based colorectal cancer screening programme in down-staging. Cancer Epidemiol. 2022;79:102184. doi:10.1016/j.canep.2022.102184
8. Larsen MB, Njor S, Ingeholm P, et al. Effectiveness of colorectal cancer screening in detecting earlier-stage disease-a nationwide cohort study in Denmark. Gastroenterology. 2018;155(1):99–106. doi:10.1053/j.gastro.2018.03.062
9. McClements PL, Madurasinghe V, Thomson CS, et al. Impact of the UK colorectal cancer screening pilot studies on incidence, stage distribution and mortality trends. Cancer Epidemiol. 2012;36(4):e232–242. doi:10.1016/j.canep.2012.02.006
10. O’Connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American joint committee on cancer sixth edition staging. J Natl Cancer Inst. 2004;96(19):1420–1425. doi:10.1093/jnci/djh275
11. Brenner H, Jansen L, Ulrich A, et al. Survival of patients with symptom- and screening-detected colorectal cancer. Oncotarget. 2016;7(28):44695–44704. doi:10.18632/oncotarget.9412
12. Cienfuegos JA, Baixauli J, Martinez Ortega P, et al. Screening-detected colorectal cancers show better long-term survival compared with stage-matched symptomatic cancers. Rev Esp Enferm Dig. 2018;110(11):684–690. doi:10.17235/reed.2018.5509/2018
13. Gill MD, Bramble MG, Hull MA, et al. Screen-detected colorectal cancers are associated with an improved outcome compared with stage-matched interval cancers. Br J Cancer. 2014;111(11):2076–2081. doi:10.1038/bjc.2014.498
14. Luu XQ, Lee K, Jun JK, et al. Effect of colorectal cancer screening on long-term survival of colorectal cancer patients: results of the Korea national cancer screening program. Int J Cancer. 2022;150(12):1958–1967. doi:10.1002/ijc.33953
15. Chiu HM, Chen SL, Yen AM, et al. Effectiveness of fecal immunochemical testing in reducing colorectal cancer mortality from the one million Taiwanese screening program. Cancer Am Cancer Soc. 2015;121(18):3221–3229.
16. Chou CK, Chen SL, Yen AM, et al. Outreach and inreach organized service screening programs for colorectal cancer. PLoS One. 2016;11(5):e0155276. doi:10.1371/journal.pone.0155276
17. Chen LS, Liao CS, Chang SH, et al. Cost-effectiveness analysis for determining optimal cut-off of immunochemical faecal occult blood test for population-based colorectal cancer screening (kcis 16). J Med Screen. 2007;14(4):191–199. doi:10.1258/096914107782912022
18. Chiang CJ, Wang YW, Lee WC. Taiwan’s nationwide cancer registry system of 40 years: past, present, and future. J Formos Med Assoc. 2019;118(5):856–858. doi:10.1016/j.jfma.2019.01.012
19. Chiang CJ, You SL, Chen CJ, et al. Quality assessment and improvement of nationwide cancer registration system in Taiwan: a review. Jpn J Clin Oncol. 2015;45(3):291–296. doi:10.1093/jjco/hyu211
20. Liu CYH, Chuang YT, Chen YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manage. 2006;4(1):1–22.
21. Duffy SW, Nagtegaal ID, Wallis M, et al. Correcting for lead time and length bias in estimating the effect of screen detection on cancer survival. Am J Epidemiol. 2008;168(1):98–104. doi:10.1093/aje/kwn120
22. Chan HC, Huang CC, Huang CC, et al. Predicting colon cancer-specific survival for the asian population using national cancer registry data from Taiwan. Ann Surg Oncol. 2022;29(2):853–863. doi:10.1245/s10434-021-10646-2
23. Chan YM, MacKay C, Ritchie DT, et al. Screen detection is a survival predictor independent of pathological grade in colorectal cancer. A prospective cohort study. Surgeon. 2021;19(1):20–26. doi:10.1016/j.surge.2020.02.004
24. Hackl C, Neumann P, Gerken M, et al. Treatment of colorectal liver metastases in Germany: a ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer. 2014;14:810. doi:10.1186/1471-2407-14-810
25. Pan Z, Peng J, Lin J, et al. Is there a survival benefit from adjuvant chemotherapy for patients with liver oligometastases from colorectal cancer after curative resection? Cancer Commun. 2018;38(1):29. doi:10.1186/s40880-018-0298-8
26. Hee YJ, Bang CS, Baik GH, et al. Association between ischemic heart disease and colorectal neoplasm: a systematic review and meta-analysis. Springerplus. 2016;5(1):1664. doi:10.1186/s40064-016-3349-0
27. Jeong S, Lee G, Choi S, et al. Estimating risk of cardiovascular disease among long-term colorectal cancer survivors: a nationwide cohort study. Front Cardiovasc Med. 2021;8:721107. doi:10.3389/fcvm.2021.721107
28. Shida H, Ban K, Matsumoto M, et al. Asymptomatic colorectal cancer detected by screening. Dis Colon Rectum. 1996;39(10):1130–1135. doi:10.1007/BF02081414
29. Lee YC, Fann JC, Chiang TH, et al. Time to colonoscopy and risk of colorectal cancer in patients with positive results from fecal immunochemical tests. Clin Gastroenterol Hepatol. 2019;17(7):1332–1340 e1333. doi:10.1016/j.cgh.2018.10.041
30. Jen HH, Hsu CY, Chen SL, et al. Rolling-out screening volume affecting compliance rate and waiting time of fit-based colonoscopy. J Clin Gastroenterol. 2018;52(9):821–827. doi:10.1097/MCG.0000000000000955
31. Wang YW, Chen HH, Wu MS, et al. Current status and future challenge of population-based organized colorectal cancer screening: lesson from the first decade of Taiwanese program. J Formos Med Assoc. 2018;117(5):358–364. doi:10.1016/j.jfma.2017.09.010
32. Oono Y, Fu K, Nakamura H, et al. Progression of a sessile serrated adenoma to an early invasive cancer within 8 months. Dig Dis Sci. 2009;54(4):906–909. doi:10.1007/s10620-008-0407-7
33. Lee KW, Park SK, Yang HJ, et al. Microsatellite instability status of interval colorectal cancers in a Korean population. Gut Liver. 2016;10(5):781–785. doi:10.5009/gnl15376
34. Rutter MD, Beintaris I, Valori R, et al. World endoscopy organization consensus statements on post-colonoscopy and post-imaging colorectal cancer. Gastroenterology. 2018;155(3):909–925 e903. doi:10.1053/j.gastro.2018.05.038
35. Jen HH. Consolidated Coxian Phase-Type-Based Stochastic Model for Evaluation of Effectiveness of Population-Based Screening [Unpublished doctoral dissertation]: National Taiwan University; 2019.
36. Imperiale TF, Ransohoff DF, Itzkowitz SH. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med. 2014;371(2):187–188. doi:10.1056/NEJMc1405215
37. Sturzlinger H, Conrads-Frank A, Eisenmann A, et al. Stool DNA testing for early detection of colorectal cancer: systematic review using the hta core model((r)) for rapid relative effectiveness assessment. Ger Med Sci. 2023;21:Doc06. doi:10.3205/000320
38. Chang PY, Chen CC, Chiang JM, et al. A simple and highly specific massarray-based stool DNA assay to prioritize follow-up decisions in fecal immunochemical test-positive individuals. Cancers. 2019;11(3). doi:10.3390/cancers11030423
39. Collins JF, Lieberman DA, Durbin TE, et al. Accuracy of screening for fecal occult blood on a single stool sample obtained by digital rectal examination: a comparison with recommended sampling practice. Ann Intern Med. 2005;142(2):81–85. doi:10.7326/0003-4819-142-2-200501180-00006
40. Force US, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: us preventive services task force recommendation statement. JAMA. 2021;325(19):1965–1977. doi:10.1001/jama.2021.6238
41. Tepus M, Yau TO. Non-invasive colorectal cancer screening: an overview. Gastrointest Tumors. 2020;7(3):62–73. doi:10.1159/000507701
42. Anand S, Liang PS. A practical overview of the stool DNA test for colorectal cancer screening. Clin Transl Gastroenterol. 2022;13(4):e00464. doi:10.14309/ctg.0000000000000464
43. Parkin CJ, Bell SW, Mirbagheri N. Colorectal cancer screening in Australia: an update. Aust J Gen Pract. 2018;47(12):859–863. doi:10.31128/AJGP-01-18-4472
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
IGFBP5 is Upregulated and Associated with Poor Prognosis in Colorectal Cancer
Deng Y, Yang X, Hua H, Zhang C
International Journal of General Medicine 2022, 15:6485-6497
Published Date: 6 August 2022
Upregulation of Long Noncoding RNA MALAT1 in Colorectal Cancer Promotes Radioresistance and Aggressive Malignance
Shen W, Yu Q, Pu Y, Xing C
International Journal of General Medicine 2022, 15:8365-8380
Published Date: 28 November 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
The Prognostic Significance of Postoperative Adjuvant Chemotherapy in the Population Aged 75 Years and Older with Stage II–III Colorectal Cancer: A Retrospective Multi-Center Cohort Study
Liu L, Pang X, Zhao K, Chen Y, Li Y, You R, Xu T, Liu M, Wu L, Li Z, Pu H
International Journal of General Medicine 2023, 16:3311-3322
Published Date: 3 August 2023
BICDL1 Predicts Poor Prognosis and is Correlated with Methylation and Immune Infiltration in Colorectal Cancer
Luo H, Luo J, Ding N, Zhang T, He Y
Pharmacogenomics and Personalized Medicine 2023, 16:1109-1126
Published Date: 22 December 2023