")
Back to Journals » International Journal of General Medicine » Volume 16
The Prognostic Significance of Postoperative Adjuvant Chemotherapy in the Population Aged 75 Years and Older with Stage II–III Colorectal Cancer: A Retrospective Multi-Center Cohort Study
Authors Liu L, Pang X, Zhao K, Chen Y, Li Y, You R, Xu T, Liu M, Wu L, Li Z , Pu H
Received 5 May 2023
Accepted for publication 24 July 2023
Published 3 August 2023 Volume 2023:16 Pages 3311—3322
DOI https://doi.org/10.2147/IJGM.S420024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lizhu Liu,1,* Xiaolin Pang,2,* Ke Zhao,3,* Yaxue Chen,4 Yanli Li,1 Ruimin You,1 Tingting Xu,5 Mengmei Liu,6 Lin Wu,7 Zhenhui Li,1 Hongjiang Pu8
1Department of Radiology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Centre, Kunming, 650118, People’s Republic of China; 2Department of Radiotherapy, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510655, People’s Republic of China; 3Department of Radiology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, 510080, People’s Republic of China; 4Department of Nursing, Dazhou Vocational and Technical College, Dazhou, Sichuan, 635000, People’s Republic of China; 5Department of Oncology, The People’s Hospital of Chuxiong Yi Autonomous Prefecture, Chuxiong, 675000, People’s Republic of China; 6School of Public Health, Kunming Medical University, Kunming, 650000, People’s Republic of China; 7Department of Pathology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Center, Kunming, 650118, People’s Republic of China; 8Department of Oncology, Dazhou Central Hospital, Dazhou, Sichuan, 635000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenhui Li, Department of Radiology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Centre, Kunming, 650118, People’s Republic of China, Tel/Fax +86 87168179549, Email [email protected] Hongjiang Pu, Department of Oncology, Dazhou Central Hospital, Dazhou, Sichuan, 635000, People’s Republic of China, Tel/Fax +86 87168179549, Email [email protected]
Background: It is common for elderly patients to be underrepresented in clinical trials for cancer, which can result in a lack of efficacy data and unclear criteria to guide treatment decisions for clinical doctors. Therefore, one of the common challenges in oncology treatment is determining the extent to which patients aged 75 and older have benefited from postoperative chemotherapy.
Purpose: The study aimed to explore the effect of adjuvant chemotherapy (AC) on 3-year recurrence-free survival (RFS) after curative resection in patients aged 75 years and older with stage II–III colorectal cancer (CRC).
Methods: The retrospective cohort analysis was performed on patients with stage II–III CRC who received curative resection at three cancer centers in China between 2008 and 2017. Kaplan-Meier curves and Multivariable Cox regression models were used to analyze the impact of AC on RFS in patients. Finally, propensity-score matching was used to reduce selection bias and confounding factors in patients aged 75 years and older with stage II–III CRC.
Results: A total of 2885 patients were included (1729 (59.9%) male; 1312 (61.5%) received AC). The pre-matching cohort was comprised of 151 patients aged 75 years and older (median age (IQR)77.00 (76.00, 79.00); 97 (64.2%) male, 51 (72.9%) received AC). Age (P=0.001), postoperative carcinoembryonic antigen (CEA)(P=0.02) level were associated with prognosis. But AC was not associated with 3-year RFS (HR, 1.27; 95% CI, 0.80– 2.0; log-rank P=0.37). After a predisposition 1: 1 match (with or without AC, n = 42), AC remains uncorrelated with 3-year RFS (HR, 1.39; 95% CI, 0.52– 3.70; log-rank P=0.66).
Conclusion: Patients over the age of 75 with stage II–III CRC who receive AC or do not face the same risk of postoperative recurrence. As a result, patients with stage II–III postoperative adjuvant chemotherapy can make an informed decision regarding whether they want to undergo chemotherapy based on their age and reduce the unnecessary side effects of chemotherapy.
Keywords: colorectal cancer, adjuvant chemotherapy, recurrence-free survival, prognosis
Introduction
Colorectal cancer is the world’s third most prevalent cause of death from cancer.1
Since 2000–2016, the incidence and mortality of CRC have shown an upward trend. The incidence rate of CRC in China knotting jumped to the second and the mortality rate ranked fourth.2 Patients over the age of 65 made up 54% of the 147,950 people in the United States who received a CRC diagnosis in 2020, and they also accounted for 68% of CRC fatalities.1
Currently, the primary treatment for CRC involves the removal of the primary tumor and regional lymph nodes.3 Cancers detected at early stages have an excellent 5-year survival rate of approximately 92%.3 However, this rate significantly decreases during stage III CRC, which is characterized by lymph node metastasis.3 To improve prognosis and reduce the risk of recurrence, several guidelines suggest that patients with locally advanced CRC should undergo adjuvant chemotherapy (AC) after curative resection.4–6 Age, physical condition, and underlying disease must all be carefully considered when choosing a particular adjuvant chemotherapy plan. There is no proof that patients 70 years of age or older will benefit from adding oxaliplatin to 5-FU/LV regimens.7,8 It is common for elderly patients to be underrepresented in clinical trials for cancer, which can result in a lack of efficacy data and unclear criteria to guide treatment decisions for clinical doctors.
An analysis of patients aged 70 years and older who underwent adjuvant 5-FU therapy revealed no evidence of a diminished effect of chemotherapy on cancer recurrences or deaths with increasing age. However, this study predates the oxaliplatin era.9 According to more recent research, older patients had less incremental benefit from oxaliplatin than younger patients.10 When assessing poor response to medication, it is important to consider whether insufficient dosage may be the cause. Older patients have a higher likelihood of discontinuing oxaliplatin early, resulting in a 25% reduction in cumulative dosage compared to younger patients.11 However, the two main trials demonstrating the efficacy of oxaliplatin included only 25 (1%) and 131 (5%) patients aged 75 years and older (D.J. Sargent, personal communication, November 2009).12,13 Therefore, one of the common challenges in oncology treatment is determining the extent to which patients aged 75 and older have benefited from postoperative chemotherapy. To explore the practical practice patterns and outcomes, we assessed the effectiveness of postoperative adjuvant chemotherapy in patients over 75 years old with stage II–III CRC.
Methods
Ethics Statement
This retrospective study was performed in accordance with the Declaration of Helsinki. The Ethics Committee approved this study of Yunnan Cancer Hospital (KY2019141), the Ethics Committee of the Sixth Affiliated Hospital of Sun Yat-sen University (2021ZSLYEC-051) and the Research Ethics Committee of Guangdong Provincial People’s Hospital (GDREC2020011H). The research design verified the model by tracking the patients’ postoperative follow-up, calculating the use of postoperative AC, collecting their clinical data, understanding the risk factors of postoperative AC in CRC patients, and building a prediction model according to each risk factor index clinically.14 Due to the study’s retrospective nature, the ethics committee waived the informed consent requirement. All patient data were anonymous during the survey.
Study Population
A total of 4214 patients with stage II–III CRC confirmed by pathological diagnosis between 2008 and 2017 were retrospectively selected at Yunnan Provincial Cancer Hospital, the Sixth Affiliated Hospital of Sun Yat-sen University, and Guangdong Provincial People’s Hospital, all of whom directly underwent curative resection. The following patients were excluded: synchronous colon cancer, metastatic disease, underwent emergency surgery, received preoperative treatment, or only stoma construction.
Variables
The following variables were analyzed: age at diagnosis, body mass index, sex, preoperative and postoperative CEA level, surgical modality, primary tumor location, tumor differentiation, pathological type, T stage, N stage, the 8th AJCC stage, number of lymph node dissection, lymphovascular invasion (LVI) (yes/no), perineural invasion (yes/no), tumor deposition (yes/no).
Our primary observation is 3-year RFS. In this study, the RFS was defined as the number of months since surgery before the first recurrence. Patients were followed up every three months during the first three years. After that, patients were followed up every six months until they died. During each follow-up, patients underwent physical examinations and blood tests that included measuring CEA levels. CT scans of the chest and abdomen were performed every six months. In this study, patients received chemotherapy within 3 weeks to 2 months postoperatively, with chemotherapy regimens including FOLFOX (fluorouracil, leucovorin, oxaliplatin) for 6 cycles, Cape OX (capecitabine and oxaliplatin) for 3 cycles, Capecitabine for 6 cycles, or 5-FU/leucovorin for 3 cycles,15,16 as determined by the surgeon according to the patient’s general circumstances and wishes.
Statistical Analysis
The use of AC after curative resection and its survival benefits were studied in patients of different ages (mainly in elderly patients aged 75 years and older). The Wilcoxon Mann–Whitney test, Fisher’s exact test, or Chi-square test was used to compare the use of AC with patients who did not receive it, regardless of whether data was categorical or continuous. Kaplan-Meier survival curves and multivariable Cox proportional risk regression models are used in survival analysis.
In subgroup analysis, the association between AC acceptance or non-reception and 3-year RFS was investigated in elderly, middle-aged, and young groups using Kaplan-Meier analysis.
Propensity score matching was performed to assess selection bias resulting from potential confounders.17 Clinical factors in the model include age at diagnosis, sex, body mass index, T stage, N stage, the 8th AJCC stage. Patients receiving AC are matched to those not receiving AC in a 1:1 ratio using a greedy nearest neighbor matching algorithm without substitution, the caliper value was 5%.18 The Kruskal–Wallis analysis was used to compare patient characteristics between matching groups of propensity scores. Analyze the data using R 4.2.2 (R Project). All P-values < 0.05 were considered significant. This study follows comprehensive standard reporting guidelines for reporting trials.14
Results
Recruitment Process
In this study, 2885 patients with stage II–III CRC who underwent radical surgery were collected directly from Yunnan Provincial Cancer Hospital, the Sixth Affiliated Hospital of Sun Yat-sen University, and Guangdong Provincial People’s Hospital from 2008 to 2017. Out of the total number of patients studied, 2132 patients received AC after surgery. Patients were divided into three groups based on age: the elderly group (age ≥ 75, n=224), the middle-aged group (age 41–74, n=2446), and the younger group (age ≤40, n=215). Finally, using propensity matching in the elder group: before matching (n=151), after matching (with AC n=42, without AC n=42) (Figure 1).
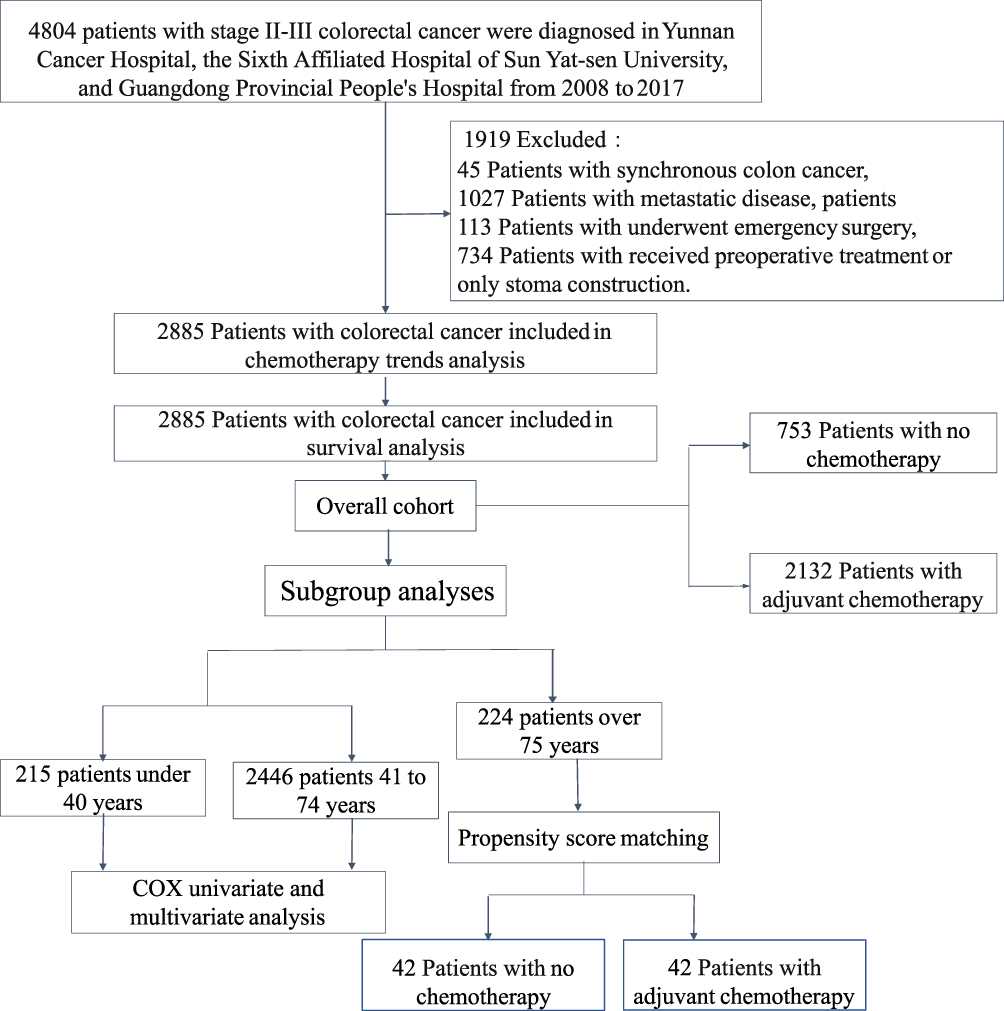 |
Figure 1 Consort Diagram of the Study Population. Notes: Schulz KF, Altman DG, Moher D, CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.19 |
Clinical Features of the General Population
A total of 2885 patients (median age (IQR), 60 (50.00–67.00); 1729 (59.9%) males; 1312 (61.5%) accepted AC) were enrolled. The median survival time of patients aged 75 years and above is 4 years (95% CI, 3.66, 4.47). AC was related to age, sex, BMI, surgical approach, tumor location, tumor differentiation, pathological type, T stage, N stage, the 8th AJCC pathological stage, the number of lymph node dissection, LVI, PNI, tumor deposition, preoperative CEA and age group (P <0.05) (Table 1).
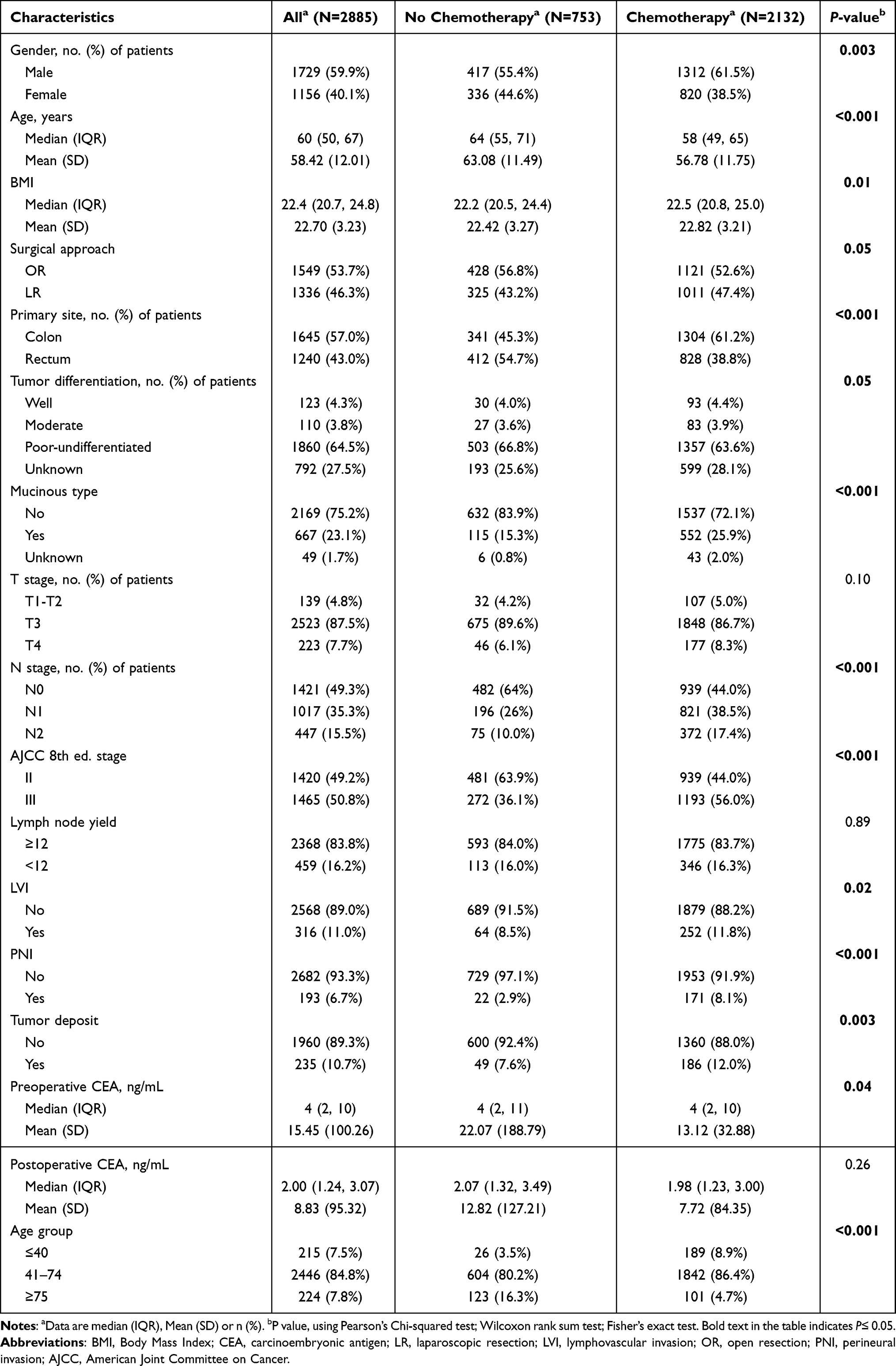 |
Table 1 Patient and Tumor Characteristics |
Univariate and Multifactorial Analysis of the Total Population to Study the Relationship Between AC and Prognosis
In univariate analysis, surgical approach, tumor location, pathological type, N1/N2, LVI, PNI, tumor deposition, AC, preoperative and postoperative CEA were associated with prognosis (P<0.001). After multivariate analysis, surgical approach (HR, 0.53; 95% CI, 0.4–0.71; P<0.001), N1 (HR, 2.22; 95% CI, 1.64–3.01; P<0.001), N2 (HR, 4.07; 95% CI, 2.93–5.66; P<0.001), LVI (HR, 1.66; 95% CI, 1.17–2.35; P<0.001), PNI (HR, 2.01; 95% CI, 1.2–3.37; P=0.01), elevated preoperative CEA (HR, 1.44; 95% CI, 1.13–1.85; P<0.001) and postoperative CEA (HR, 2.56; 95% CI, 1.92–3.42; P<0.001) remained significantly associated with prognosis. Age ≥ 75 years old (HR, 1.05; 95% CI, 0.61–1.81; P = 0.85), AC was unrelated with prognosis (HR, 0.77; 95% CI, 0.58–1.01; P=0.06) (Table 2).
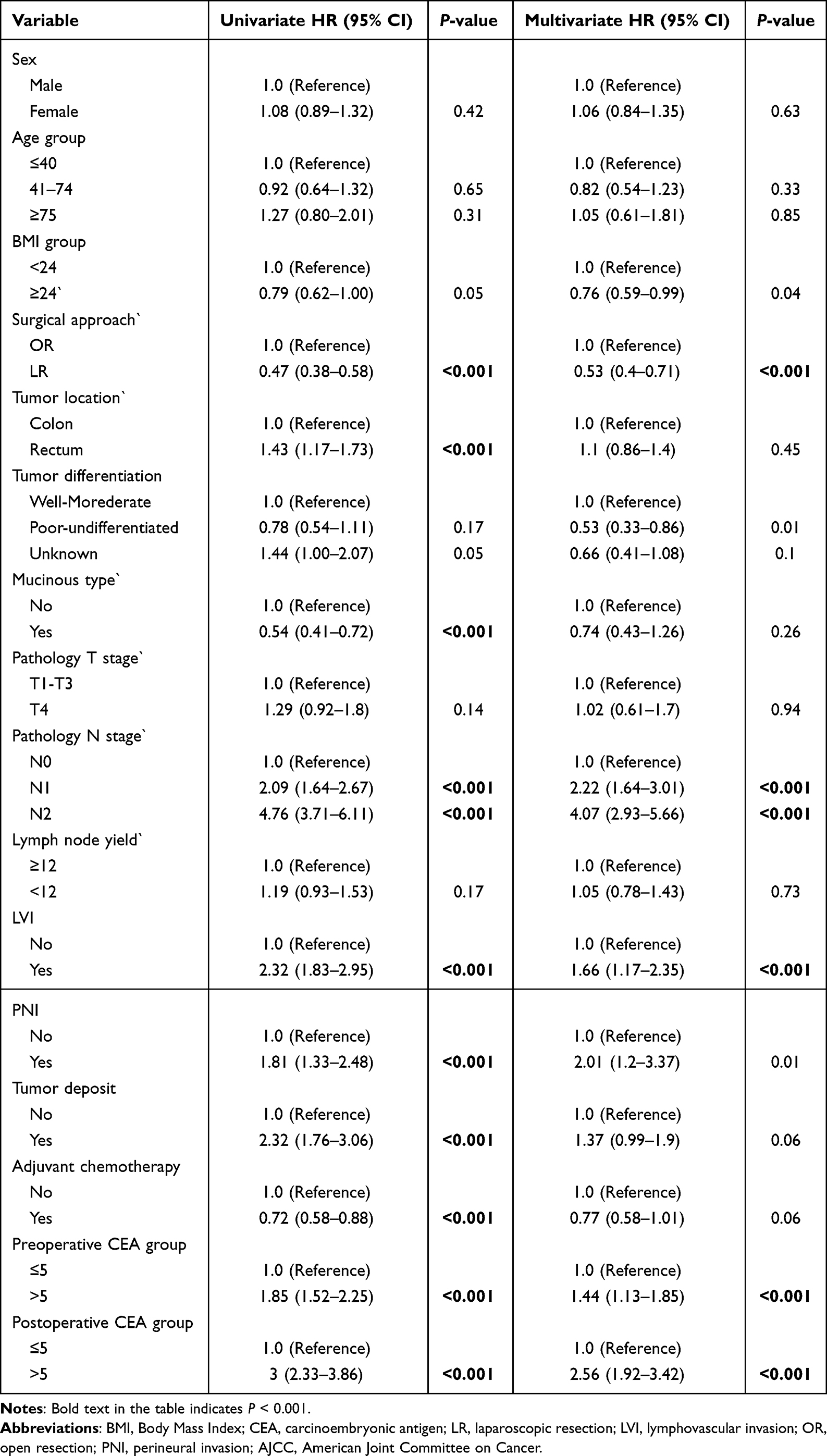 |
Table 2 Univariate and Multivariate Analyses of Overall Cohort |
Kaplan-Meier Curves and Multivariable Cox Regression Models Shows the Relationship Between AC and 3-Year RFS in Different Age Groups
In the total population (HR, 0.72; 95% CI, 0.58–0.88; log-rank P=0.0017) (Figure 2a) and middle-aged group (HR, 0.92; 95% CI, 0.64–1.32; log-rank P =0.012) (Figure 2c), which has a longer 3-year RFS than patients who did not receive AC. In the young group (HR, 1.06; 95% CI, 0.74–1.51; log-rank P=0.26) (Figure 2b), matching the pre-senior group (HR, 1.27; 95% CI, 0.80–2.00; log-rank P = 0.37) (Figure 2d) and the post-matched senior group (HR, 1.39; 95% CI, 0.52–3.70; log-rank P = 0.66) (Figure 2e), AC was not associated with 3-year RFS.
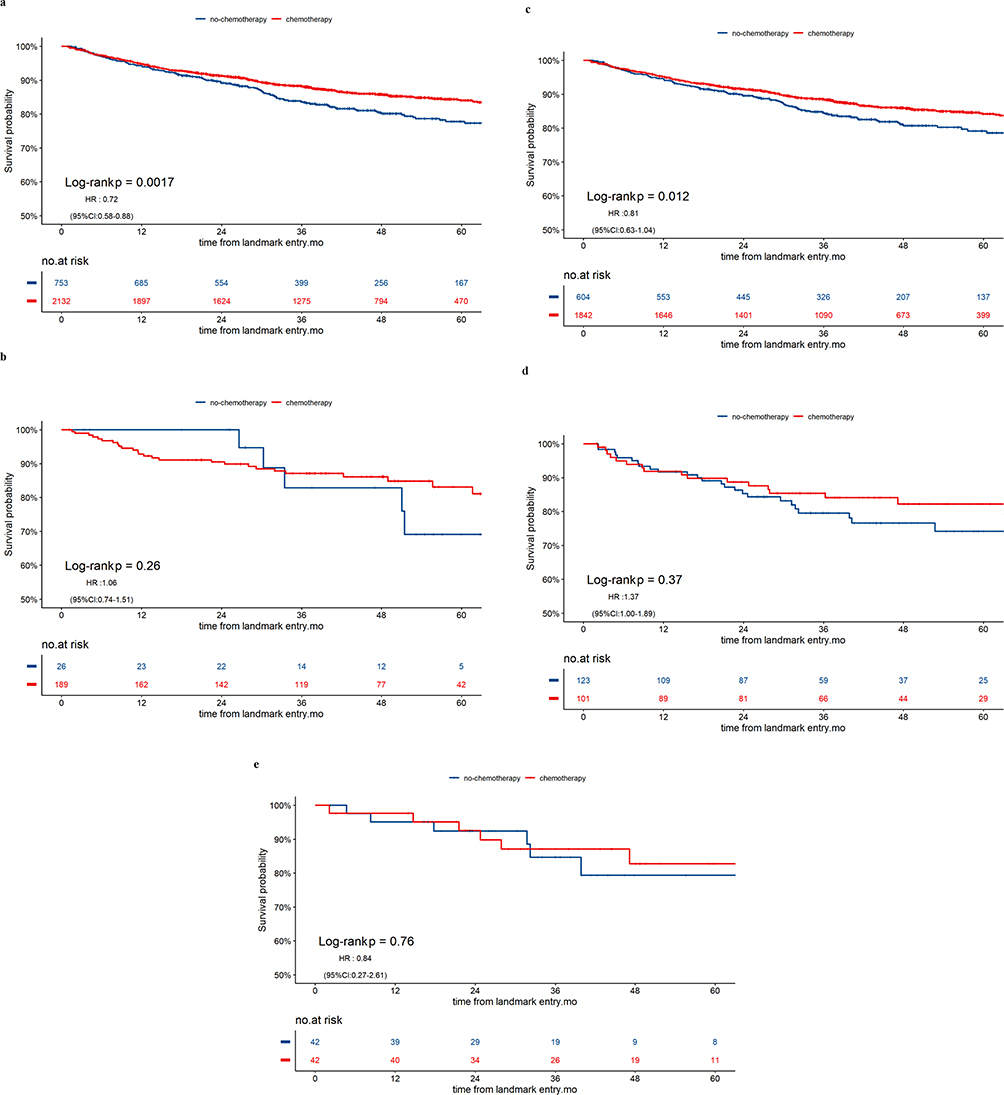 |
Figure 2 Kaplan-Meier curves for recurrence-free survival that Associated with the Use of Adjuvant Chemotherapy in Overall cohort (a), young group (b), middle-aged group (c), pre-matched senior group (d) post-matched senior group (e). |
Propensity-Matching Cohort for Elderly Patients with CRC Aged 75 Years and Older
The pre-matching cohort was comprised of 151 patients aged 75 years and older (median age (SD) 77.96 (2.96), 97 (64.2%) males, 51 (72.9%) received AC). Where age, tumor type, postoperative CEA level was associated with prognosis. After a predisposition 1:1 match, there was no received AC group (n=42), received AC group (n=42), none of these factors correlated with prognosis (Table 3). After adjusting for multivariate analysis after matching (Table S1), chemotherapy was still not statistically significant in the 75 years and older.
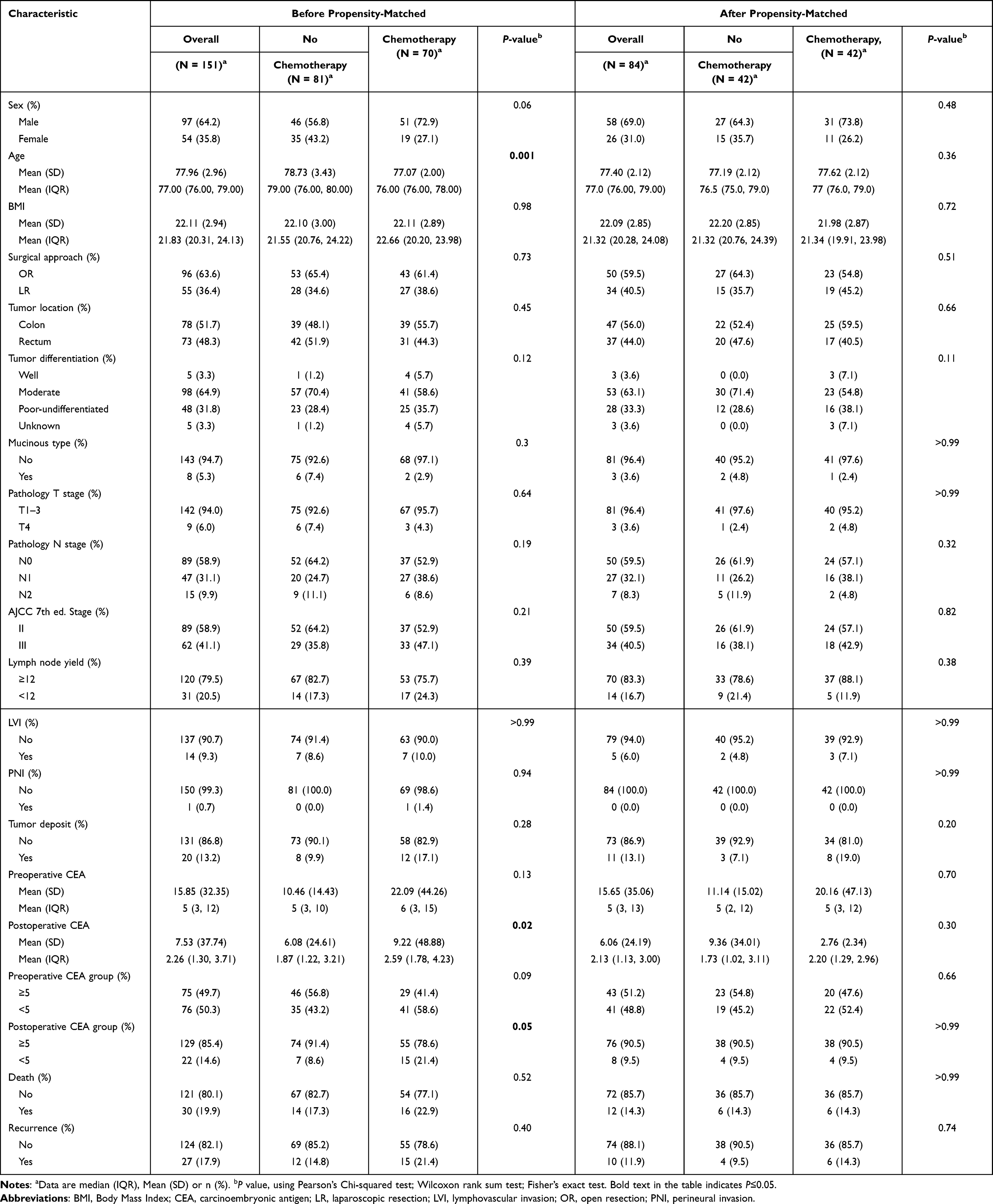 |
Table 3 Characteristics of Patients 75 Years and Older Who Underwent Surgery for Colorectal Cancer Before and After Matching |
Discussion
This analysis investigates the association between adjuvant chemotherapy after curative surgery and prognosis in patients with stage II–III colorectal cancer of different age groups. In the univariate analysis of the total population from 2008 to 2017, it was observed that patients with CRC who received AC after surgery had a 3-year extended RFS, which indicates AC can reduce the risk of postoperative death and improve prognosis. However, multivariate analyses revealed inconsistent results, suggesting that chemotherapy was not an independent risk factor for prognosis. In the propensity-matching cohort of elderly patients with CRC aged 75 years and older, postoperative AC was not associated with 3-year RFS. In subgroup analysis, postoperative acceptance of AC by patients with CRC in the middle-aged group and postoperative acceptance or non-acceptance of AC in the younger and elderly groups were not associated with 3-years RFS. These experimental results showed that elderly patients with CRC aged 75 years and older may not benefit from chemotherapy, and further validation is needed for younger patients.
According to the results of three large-scale trials, the use of fluorouracil (FU/LV or capecitabine) and oxaliplatin as adjuvant chemotherapy for six months is the standard care for stage III CRC patients.20 Older patients did not receive too much postoperative AC may be the following reasons: lack of randomized clinical trials in older adults, coupled with concerns about their limited life expectancy, their fitness for radical treatment, and increased toxic complications due to age-related changes in chemotherapeutic pharmacokinetics,21 which resulting in a smaller study size. A previous study has shown that older patients with stage III CRC with a pathological diagnosis often do not receive appropriate AC due to concerns about side effects and tolerance.22 San et al studied the effects of AC on patients with stage III CRC aged 75 years or older and reported that AC use declines with age.23 On the other hand, several previous studies have reported that oxaliplatin treatment did not affect the prognosis of stage III CRC patients over 70 years of age.11,24,25 Yothers et al investigated the additional effects of oxaliplatin on patients over 70 years of age in a newer NSABP C-07 trial.11 McCleary et al examined the impact of age on CRC recurrence after receiving AC using the ACCENT database, with patients aged 70 years or older having a reduced benefit from the addition of oxaliplatin to 5-FU in adjuvant therapy.10
Age, on the other hand, is not related to physiological age. In randomized trials, oxaliplatin appeared surprisingly effective in patients over 75 years of age in the community compared to patients over 70 years of age.23 A detailed assessment of the patient’s general condition and appropriate AC indications is essential to obtain the maximum benefit of AC, especially for older patients. A previous study reported that selected patients with CRC could derive the same benefits from adjuvant fluorouracil-based therapy without significantly increasing toxic effects and supported the proposition that even the oldest patients with CRC should consider treatment.10 The result suggests that older patients, particularly high-risk patients, could derive a survival benefit from AC to control cancer properly. What’s more, clinicians should not hesitate to implement aggressive cancer treatment for older patients in the same manner as they would in younger patients.
Our study has the advantage of being relatively large overall, with detailed identification of CRC risk factors when collecting data retrospectively. We also used propensity score matching to reduce the effect of confounding factors, which improve the accuracy and credibility of the results. At the same time, this study also has some limitations. For one, it is a retrospective cohort study and may have some selection bias. More generally, it was a multi-center study, and the surgeon determined the types of indications and chemotherapy regimens for AC. Patients may have received differences in their treatment regimen, including dose, course and drug combination, which can cause difficulties in the interpretation and comparison of the study results. Finally, the number of elderly CRC patients aged 75 years and older is still quite limited, which limits the accuracy of the study’s analysis. In summary, although retrospective studies provide useful information about the postoperative effects of AC in curative resection for patients aged 75 and older with stage II–III CRC, the results need to be further confirmed and validated, typically through more prospective randomized controlled trials to obtain more reliable evidence. Physicians should carefully weigh various pieces of evidence and consider individualized decision-making based on the specific circumstances of each patient when formulating treatment plans.
Conclusions
In conclusion, we have studied the application of AC after curative resection in patients of different age groups and their survival benefits. In the total population and middle-aged group, which has a longer 3-year RFS than patients who did not receive AC. In the young group, matching the pre-senior group and the post-matched senior group, AC was not associated with 3-year RFS. Patients over the age of 75 with stage I–III CRC receive AC or do not, facing the same risk of postoperative recurrence. Therefore, patients aged 75 years and older with stage II–III postoperative AC can choose whether to undergo chemotherapy according to their age to reduce unnecessary chemotherapy side effects. Moreover, there is potential for further research to examine whether young patients diagnosed with CRC are receiving excessive chemotherapy. The objective of such research would be to optimize chemotherapy protocols and prolong the survival period for these patients.
Data Sharing Statement
Original data are available on request to the corresponding author, PU HJ.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Yunnan Digitalization, Development and Application of Biotic Resource [202002AA100007], the National Natural Scientific Foundation of China [82001986], the Outstanding Youth Science Foundation of Yunnan Basic Research Project [202101AW070001], the Yunnan Basic Research Project [202201AT070010], and Innovation Team of Kunming Medical University [CXTD202110].
Disclosure
The authors have declared that there is no conflict of interest.
References
1. Siegel RL, Miller KD, Sauer AG, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–164. doi:10.3322/caac.21601
2. Zheng R, Zhang S, Zeng H, et al. Cancer incidence and mortality in China, 2016. J Natl Cancer Center. 2022;2(1):1–9. doi:10.1016/j.jncc.2022.02.002
3. Dienstmann R, Mason MJ, Sinicrope FA, et al. Prediction of overall survival in stage II and III colon cancer beyond TNM system: a retrospective, pooled biomarker study. Ann Oncol. 2017;28(5):1023–1031. doi:10.1093/annonc/mdx052
4. Watanabe T, Muro K, Ajioka Y, Hashiguchi Y, Ito Y. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. Int J Clin Oncol. 2017;23(1):1–34. doi:10.1007/s10147-017-1101-6
5. Benson AB, Venook AP, Cederquist L, et al. Colon cancer, Version 1.2017, NCCN clinical practice guidelines in oncology. J Natl Comprehen Cancer Netw. 2017;15(3):370. doi:10.6004/jnccn.2017.0036
6. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27(8):1386–1422. doi:10.1093/annonc/mdw235
7. Christophe T, Thierry A, Franck B, et al. Adjuvant therapy with fluorouracil and oxaliplatin in stage II and elderly patients (between ages 70 and 75 years) with colon cancer: subgroup analyses of the Multicenter International Study of Oxaliplatin, Fluorouracil, and Leucovorin in the Adjuvant Treatment of Colon Cancer trial. J Clin Oncol. 2012;30(27):3353–3360. doi:10.1200/JCO.2012.42.5645
8. Tan K-Y, Konishi F, Suzuki K. The evidence for adjuvant treatment of elderly patients (age > or = 70) with stage III colon cancer is inconclusive. Surg Today. 2010;40(4):385–387. doi:10.1007/s00595-009-4047-0
9. Sargent DJ, Goldberg RM, Jacobson SD, Macdonald JS, Labianca R. A pooled analysis of adjuvant chemotherapy for resected colon cancer in elderly patients. N Engl J Med. 2001;345(15):1091–1097. doi:10.1056/NEJMoa010957
10. McCleary NJ, Meyerhardt JA, Green E, Yothers G, de Gramont A. Impact of age on the efficacy of newer adjuvant therapies in patients with stage II/III colon cancer: findings from the ACCENT database. J Clin Oncol. 2013;31(20):2600–2606. doi:10.1200/JCO.2013.49.6638
11. Yothers G, O’Connell MJ, Allegra CJ, Kuebler JP, Colangelo LH. Oxaliplatin as adjuvant therapy for colon cancer: updated results of NSABP C-07 trial, including survival and subset analyses. J Clin Oncol. 2011;29(28):3768–3774. doi:10.1200/JCO.2011.36.4539
12. Andre T. Oxialiplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350(23):2343–2351 doi:10.1056/NEJMOA032709
13. Philip KJ, Samuel WH, Michael J O, et al. Oxaliplatin combined with weekly bolus fluorouracil and leucovorin as surgical adjuvant chemotherapy for stage II and III colon cancer: results from NSABP C-07. J Clin Oncol. 2007;25(16):2198–2204. doi:10.1200/JCO.2006.08.2974
14. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
15. Benson AB, Venook AP, Al-Hawary MM, Cederquist L, et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J Natl Compr Canc Netw. 2018;16(4):359–369. doi:10.6004/jnccn.2018.0021
16. Benson AB, Venook AP, Al-Hawary MM, et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018;16(7):874–901. doi:10.6004/jnccn.2018.0061
17. Renehan AG, Malcomson L, Emsley R, Gollins S, Maw A. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol. 2015;17(2):174–183. doi:10.1016/S1470-2045(15)00467-2
18. Xiao L, Zhang C, Sun Z, Yang F, Xiao R. Propensity-matched analysis of adjuvant chemotherapy for completely resected Stage IB non-small-cell lung cancer patients. Lung Cancer. 2019;133:75–82. doi:10.1016/j.lungcan.2019.04.024
19. Schulz KF, Altman DG, Moher D. CONSORT Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3):e1000251.
20. Tominaga T, Nonaka T, Oyama S, Shiraishi T, Takeshita H. Effect of oxaliplatin in elderly colon cancer patients with pathological T4 and/or N2 disease: a multicenter, propensity score-matched analysis. Int J Colorectal Dis. 2022;37(5):1181–1188. doi:10.1007/s00384-022-04159-x
21. André T, de Gramont A, Vernerey D. Adjuvant fluorouracil, leucovorin, and oxaliplatin in stage II to III colon cancer: updated 10-year survival and outcomes according to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J Clin Oncol. 2015;33(35):4176–4187. doi:10.1200/JCO.2015.63.4238
22. Hurria A, Lichtman SM. Clinical pharmacology of cancer therapies in older adults. Br J Cancer. 2008;98(3):517–522. doi:10.1038/sj.bjc.6604201
23. Tominaga T, Nonaka T, Sumida Y, Hidaka S, Sawai T, Nagayasu T. Effectiveness of adjuvant chemotherapy for elderly patients with lymph node-positive colorectal cancer. World J Surg Oncol. 2016;14(1):197. doi:10.1186/s12957-016-0959-5
24. Sanoff HK, Carpenter WR, Stürmer T, Goldberg RM, Martin CF. Effect of adjuvant chemotherapy on survival of patients with stage III colon cancer diagn osed after age 75 years. J Clin Oncol. 2012;30(21):2624–2634. doi:10.1200/JCO.2011.41.1140
25. André T, Meyerhardt J, Iveson T, Sobrero A, Yoshino T. Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): final results from a prospective, pooled analysis of six randomised, Phase 3 trials. Lancet Oncol. 2020;21(12):1620–1629. doi:10.1016/S1470-2045(20)30527-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.